

Abstract
Objective
While generally considered a safe sport, archery injuries are often the result of overuse or penetration and largely affect the upper extremities. Studies have shown that during training periods the average risk of injury is 4.4%. By studying mechanisms of injury and their prevalence nationally, this study aims to educate coaches, athletes, and equipment manufacturers on ways the sport can be safer from a clinical perspective.
Methods and Materials
The National Electronic Injury Surveillance System Database was queried to analyze archery-related musculoskeletal injuries that occurred between 2013 and 2022.
Results
Approximately 43,083 injuries were recorded over a 10-year span, of which 8,038 were women and 35,367 were men. Men were thus 4.4 times more likely to experience injury during archery. Injury sites in men included the finger (66.2%), hand (17.1%), face (6.2%), shoulder (5.4%), and foot (5.1%). All reported injuries in women were finger-related. The most common diagnoses for men were lacerations (58.1%), fractures (12.7%), contusions and abrasions (7.5%), foreign body (5.9%), punctures (4.9%), and strains/sprains (4.9%). Women exclusively experienced lacerations, accounting for 100% of their injuries.
Conclusion
The study identifies that lacerations were the most common archery-related injury that was treated in the ED. Additionally, the fingers were the most common site of injury. Findings from this study suggest that improved safety equipment, such as reinforced gloves, finger tabs, and forearm braces should be used by athletes to practice the sport more safely. Future research could involve studying injury rates in archers who use each combination of these safety precautions to investigate which gear is most protective.
Keywords: archery, National Electronic Injury Surveillance System
Introduction
Archery is a constantly developing sport that has become increasingly popular among a variety of age groups. Archery is composed of different phases including aiming, release, and follow through.1 From drawing to releasing, an archer is constantly pulling against an enormous amount of pressure from the tension of the string (9-18 kgs) as they extend their non-dominant hand to the target while the dominant hand engages in a dynamic pulling and releasing of the bowstring.2 Depending on the different types of bows such as olympic, recurve, and compound, the site of injury tends to vary. For example, for archers using an olympic bow, hypertrophy of the finger flexor tendons is common, whereas the upper arm and shoulder are prone to injuries when using the compound bow.3,4 For a well-balanced performance, an archer must focus on the strength and endurance of their forearm and shoulder girdle muscles as they are key to executing the technique properly.5
Despite being a non-contact sport, archery commonly results in injuries with the impingement of soft tissues. Tendons, ligaments, and nerves are most prone to such injuries.6 Soft tissue injuries may cause chronic pain and inflammation, and can contribute to the development of bone spurs, which cause further microtrauma to tissue.7 Acute injuries may also include lacerations, typically in cases where an arrow pierces the forearm and causes severe bruising or desensitization of the affected area if severe.6 Both of these injuries are common even in archers who take precautions such as wearing a finger tab, or a forearm brace due to the continuous and rapid act of extending and releasing the bowstring to the target.
Due to the overuse of shoulder and rotator cuff muscles, shoulder and back injuries are also common in archers. However, wrist and hand injuries have also been becoming more common due to the misuse and mishandling of the equipment. While shoulder injuries have been previously studied, current literature does not include a large segment of injuries, including the fingers, wrists, and hands. This retrospective study aims to characterize archery injuries and report on their epidemiology over the past ten years.
Methods and Materials
Study Design
National Electronic Injury Surveillance System (NEISS), an electronic, publicly available database, was queried and analyzed to perform a retrospective study of musculoskeletal injuries resulting from archery. The NEISS database is formulated by the United States Consumer Product Safety Commission, which closely tracks and records various traumatic injuries that have occurred due to consumer products and have resulted in emergency department visits. In this study, archery was chosen from the Sports and Recreation Equipment section of the product group to analyze all injuries that resulted in emergency department visits.
Study Population
The NEISS database has transcribed and recorded data from approximately ~100 emergency departments throughout the United States In this study, NEISS data over a ten-year span from 2013 to 2022 was queried. The patient population was not filtered by age, sex, or race. Participants were required to have experienced an archery-related injury in the aforementioned time interval to meet the inclusion criteria.
To analyze injuries specifically related to archery, products in the sports and recreation equipment group with archery as the subgroup were searched. In the archery subgroup, all equipment, apparel, and activity-related injuries were included in the study (code 1235). All body parts were searched in the study including head/neck injuries: the head (code 75), face (code 76), eyeball (code 77), mouth (code 88), neck (code 89), and ear (code 94). Upper extremity body parts including the shoulder (code 30), the elbow (code 32), the lower arm (code 33), the wrist (code 34), the upper arm (code 80), the hand (code 82), and the finger (code 92) were searched in the study. Lower trunk/pubic region body parts including: the pubic region (code 38) and the lower trunk (code 79) were also searched in the study. Lower extremity body parts including: the knee (code 35), the lower leg (code 36), the ankle (code 37), the upper leg (code 81), the foot (code 83), and the toe (code 93) were all queried in the study.
In terms of diagnosis codes, all codes were queried, but only diagnoses that had numerical data were used for analysis. These diagnoses included contusions (code 53), foreign bodies (code 53), fractures (code 57), lacerations (code 59), punctures (code 63), strains/sprains (code 64), and other (code 71). Patients’ dispositions were also analyzed to determine if they were admitted to the hospital, treated and released (code 1), treated and transferred (code 2), treated and admitted for hospitalization (code 4), or left without observation (code 6).
Statistical Analysis
Gender, anatomic locations, age groups, and diagnoses related to archery injuries were assessed in this study. Anatomic locations were also grouped into 6 broad categories for subanalysis: (1) head/neck, (2) upper extremities, (3) lower trunk/pubic region, (4) lower extremities, (5) 25% or more of body, and (6) upper trunk. NEISS database outputs were analyzed using JMP Pro 15. Through this study, the authors examined whether males or females were more prone to archery injuries, how injuries were distributed among various age groups, the types of injuries that were most common in affected individuals, and the necessity of follow-up care for affected individuals.
Results
A total of 43,083 archery-related injuries were identified through the NEISS database over a ten-year span. Males incurred 82% of the injuries (n=35,367), an injury rate 4.4 times higher than in females (n=8,038).
Figure 1 depicts the frequency distribution of archers among different age groups suffering from archery-related injuries. Injury rates peaked at ages 10-19 years in males and 30-39 years in females, with a peak incidence at age 15 in men and a peak incidence at age 36 in women. Injury rates declined as individuals grew from adolescence until middle age in their fifties, where numbers peaked again for both genders. Thereafter, the number of injuries declined with age where reported cases were less than 1,200 for both males and females in their 80s.
Figure 1. Number of archery-related injuries by 10-year age groups from the NEISS database.

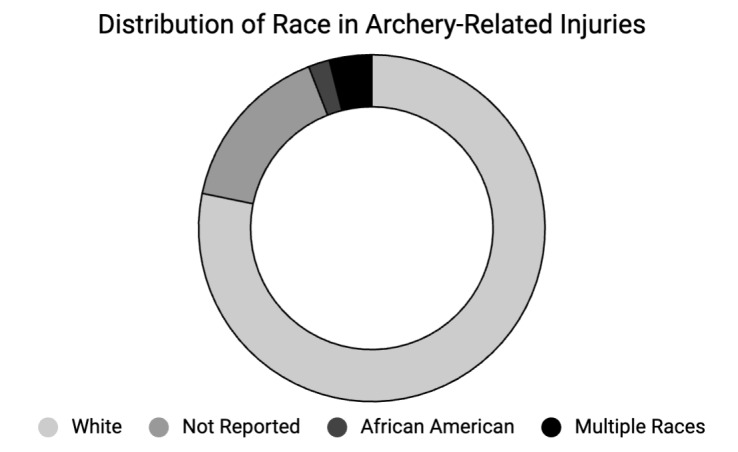
This cohort was also analyzed by race. White patients (~78%) were the most affected by archery-related injuries. Additionally, the graph shows that the Black population made up a small percentage (~2%), while some patients did not report their race. Additionally, some patients were recorded as identifying with multiple races, indicating that they did not identify into a single category presented to them. This category made up approximately 4% of the injured population.
Figure 2. Distribution of race in archery related injuries from the NEISS database.
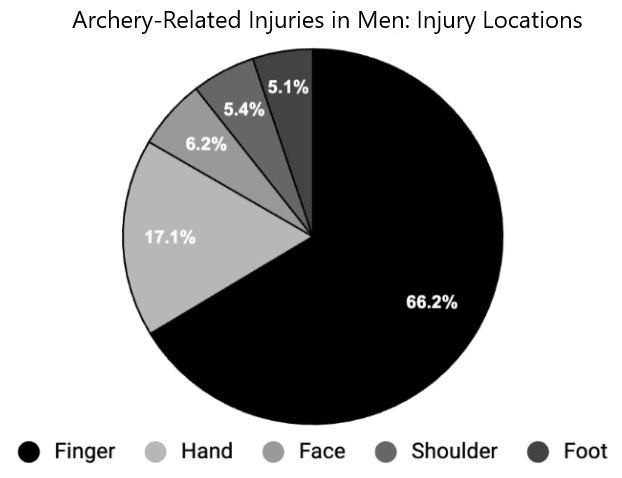
With regards to anatomic location, archery-related injuries most commonly affected the fingers. Injuries were distributed as follows in men: 66.2% finger (n=23,342), 17.1% hand (n=6,012), 6.2% face (n=2,122), 5.4% shoulder (n=1,909), and 5.1% foot (n=1,803). In contrast, in women, 100% of all reported injuries were of the finger. Figure 3 represents the distribution of anatomic injuries in men.
Figure 3. Distribution of archery-related injuries by the affected body part in men.
In men, the most common diagnosis was lacerations (58.1%). Other frequently encountered diagnoses include fracture (12.7%), contusions/abrasions (7.5%), foreign body (5.9%), puncture (4.9%), and strains/sprains (4.9%), while the remaining injuries were classified as other (6%) as represented in Figure 4. In women, all archery injuries in the database were reported as lacerations (100%).
Figure 4. Most common diagnoses of archery-related injuries in emergency departments in men.

In terms of disposition, all individuals who suffered from archery-related injuries and went to the ED were treated, examined, and then released. Additional hospitalization was not needed for the reported visits. By the data queried from the database, 33,769 males were treated/examined, and then released, while 7,692 females were treated/examined, and then released.
Discussion
While partly understated, archery-related visits to the emergency department are relatively common. After a review of the NEISS database, approximately 43,083 archery-related injuries resulted in ED visits between 2013 and 2022. This represents an average annual incidence of 4,308 injuries. Based on the National Safety Council, 3.2 million people were treated in the ED for sports and recreational activities annually.8 This data suggests that about 1 in every 670 sports injuries in the United States are archery-related injuries. Given this frequency, expanding on risk prevention and mitigation strategies in archery is worthwhile.
With over 23 million Americans aged 18 and older participating in archery, the United States is a leading country where archery is increasingly popular; this is due to the variety of training facilities and programs available.9 In the United States, archery participants are more often males than females by a 3:1 margin.10 Most archers come from rural backgrounds, usually from the Midwest, and begin their archery journey from a young age.10 As participation gradually increased in males throughout the years, participation rates for females are declining.10 Overall, young males, ages 15-29, make up more than 55% of all archers.10 Efforts to dispel the gender disparity and provide an opportunity for the sport to be available to all, regardless of gender, can be beneficial to counter this trend.
Analysis of the database corroborates previous epidemiological findings that males suffer significantly higher rates of archery-related injuries than women.11 Specifically, it was determined that males suffer archery-related injuries 4.4 times more than women. Therefore, there are more recorded cases of males visiting the ED for archery-related injuries than women.12 Thus, in terms of injuries, although males suffer higher rates of injuries, it can not be concluded that men are more susceptible to injuries than women because archery is a sport predominantly played by males.
The highest frequency of injuries occurred during adolescence in both men and women. These occurred at the highest rates in the 10-19 year age group in men, peaking at 15 years, suggesting that male archers are most susceptible to injury during this stage of life. Most archers begin their archery experience with no past experience and therefore, need to be thoroughly trained to handle the heavy bow and arrow. With just a slip of the finger, the position of the arrow can be drastically altered, allowing more room for injuries to occur. Since most of the injuries in both genders occurred during the adolescent period, these findings suggest that more focus should be given to properly training and accurately guiding novice archers to prevent injuries.
The most common injury site was the finger in both genders with lacerations being the most common diagnosis. Although safety gear is worn by archers to protect the finger, it is still extremely vulnerable to injuries due to the continuous and excessive pressure inflicted on it as the archer shoots the arrow. By misplacing the arrow or bending the finger in an improper manner, an archer is prone to being injured even with the finger brace, leading to lacerations of the skin. Traumatic lacerations to the skin, which are often painful and occur near the joints, remain a common reason for patients to seek emergency care.13
In addition to traumatic lacerations, fractures such as open metacarpal fractures are common diagnoses in archers. During the aiming phase, fractures due to improper placement of the hand are predominant, given the extensive amount of stress placed on the upper extremities.14 Other chronic injuries included bilateral medial epicondylitis and median nerve compression, affecting the wrist in most archers.15,16 As tension is concentrated at the wrist and fingers when pulling the bowstring, prolonging the time of exposure with the string, even after the release of the arrow, can cause these chronic injuries, in addition to tendonitis, blistering, and bruising.17 Overuse type of tendon injuries and strains such as de Quervain’s tenosynovitis, extensor tendon tenosynovitis are among the most common musculoskeletal injuries in competitive archers and occur when the tendons and rotator cuff muscles are overused with repetitive load bearing, putting enormous amounts of stress on the body and leads to early degenerative changes.18,19 As most of these injuries are caused by poor technique, overuse, and limited recovery time, it is important to provide archers with comprehensive training to prevent further injuries.20
This study has limitations worth noting. The total number of archery-related injuries is likely to be underreported in the NEISS database as it only includes individuals who reported to the ED for treatment, and excludes individuals who have been injured but did not seek emergency care. As archery is a sport that is predominantly played by males, there is limited data for women. In the NEISS database, all reported injuries for women were lacerations of the finger - not accounting for a variety of injuries that likely affect women. This limits the ability to further analyze gender as it relates to archery injuries by location and wound type.
In the NEISS database, there is limited data on geographical location of where archery-related injuries occurred. The database includes information regarding the specific incident sites of injuries such as home, farm/ranch, school, and industrial place but does not have records of the distribution of injuries among the states/territories in the United States. This limits the ability to further analyze if location, rural or urban, has an effect on archery-related injuries and visits to the ED. Further research should focus on considering location as a component of analysis to establish if differences in geographic location has an effect on training methods or the use of safety gear to help prevent further injuries.
Additionally, a portion of injury types in the NEISS database were recorded as “other”. The “other” category limited our analysis as the mechanism of injury could not be concretely stated. In the NEISS database, race is categorized as White, Black/African American, and other. This other category is a combination of cases where the ED record indicates more than one race or where none of the above applies. Due to this characterization, the database fails to capture the full diversity of the US population and cannot provide an accurate representation of injuries associated by race. Additionally, while diagnoses of injuries were provided, the severity of each injury was not taken into consideration in the database and therefore, could not be analyzed. Finally, as this is a retrospective study, the study design limits the ability to draw causative conclusions, but rather suggests correlations.
This study’s objectives were to provide an overview of archery-related injuries and their trends in demographics, diagnosis, and disposition. Future studies may include better characterizing archery injuries in both genders and injury rates in athletes with various protective gear in use. This work would help contribute to the growing body of literature that advocates for the implementation and use of protective gear in the sport.
References
- The Characteristics of Shoulder Muscles in Archery Athletes. Kim Ri Na, Lee Jin Hyuck, Hong Seok Ha, Jeon Jin Ho, Jeong Woong Kyo. Sep 1;2018 Clinics in shoulder and elbow. 21(3):145–150. doi: 10.5397/cise.2018.21.3.145. doi: 10.5397/cise.2018.21.3.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biomechanical study of the final push-pull in archery. Leroyer P., Van Hoecke J., Helal J.N. Feb;1993 Journal of sports sciences. 11(1):63–69. doi: 10.1080/02640419308729965. doi: 10.1080/02640419308729965. [DOI] [PubMed] [Google Scholar]
- Sonographic assessment of finger flexor tendons in olympic archers. Bayram K., Levent Ö., Hayri E., Ýsmail K., Ayþen A. 2012Turk J Phys Med Rehabil. 58:85–7. [Google Scholar]
- Bow Hunterʼs Stroke. Sorensen Bruce F. May;1978 Neurosurgery. 2(3):259–261. doi: 10.1227/00006123-197805000-00013. doi: 10.1227/00006123-197805000-00013. [DOI] [PubMed] [Google Scholar]
- Shoulder injuries in archery. Mann D.L., Littke N. 1989Canadian journal of sport sciences = Journal canadien des sciences du sport. 14(2):85–92. [PubMed] [Google Scholar]
- Injuries in archers. Singh AnantKumar, Lhee Sang-Hoon. 2016Saudi Journal of Sports Medicine. 16(3):168. doi: 10.4103/1319-6308.187554. doi: 10.4103/1319-6308.187554. [DOI] [Google Scholar]
- Incidence and severity of reported acute sports injuries in 35 sports using insurance registry data. Åman M., Forssblad M., Henriksson-Larsén K. Apr 8;2015 Scandinavian Journal of Medicine & Science in Sports. 26(4):451–462. doi: 10.1111/sms.12462. doi: 10.1111/sms.12462. [DOI] [PubMed] [Google Scholar]
- Sports and recreational injuries. https://injuryfacts.nsc.org/home-and-community/safety-topics/sports-and-recreational-injuries
- The Adoption of the Bow and Arrow in Eastern North America: A View from Central Arkansas. Nassaney Michael S., Pyle Kendra. Apr;1999 American Antiquity. 64(2):243–263. doi: 10.2307/2694277. doi: 10.2307/2694277. [DOI] [Google Scholar]
- Responsive Management: Archery Participation Among Adult United States Residents in 2014. http://archerytrade.org/wp-content/uploads/2018/01/ATA_Participation_2015_Report_final.pdf
- Crossbow injuries to the thumb. Vogels E., Mahajan A., Klena J. 2015The Journal of sports medicine and physical fitness. 55(7-8):756–760. [PubMed] [Google Scholar]
- Archer demographics and statistics [2023]: Number of archers in the US. https://www.zippia.com/archer-jobs/demographics/
- Laceration Management. Mankowitz Scott L. Sep;2017 The Journal of emergency medicine. 53(3):369–382. doi: 10.1016/j.jemermed.2017.05.026. doi: 10.1016/j.jemermed.2017.05.026. [DOI] [PubMed] [Google Scholar]
- Metacarpal fracture from archery: a case report. Vogel R.B., Rayan G.M. 2003The Journal of the Oklahoma State Medical Association. 96(2):79–80. [PubMed] [Google Scholar]
- Archery-related injuries of the hand, forearm, and elbow. Rayan GHAZI M. Oct;1992 Southern medical journal. 85(10):961–964. doi: 10.1097/00007611-199210000-00007. doi: 10.1097/00007611-199210000-00007. [DOI] [PubMed] [Google Scholar]
- Is archery a strength or endurance sport? Androlia A. 2013Archery Focus. 17:28–29. [Google Scholar]
- Ultrasound features of trigger finger: Review of the literature. Bianchi Stefano, Gitto Salvatore, Draghi Ferdinando. May 20;2019 Journal of Ultrasound in Medicine. 38(12):3141–3154. doi: 10.1002/jum.15025. doi: 10.1002/jum.15025. [DOI] [PubMed] [Google Scholar]
- Subject characteristics and low back pain in young athletes and nonathletes. Kujala URHO M., Salminen JOUKO J., Taimela SIMO, Oksanen AIRI, Jaakkola LAURA. Jun;1992 Medicine & Science in Sports & Exercise. 24(6):627–632. doi: 10.1249/00005768-199206000-00003. doi: 10.1249/00005768-199206000-00003. [DOI] [PubMed] [Google Scholar]
- Overuse injuries in sport: a comprehensive overview. Aicale R., Tarantino D., Maffulli N. Dec;2018 Journal of Orthopaedic Surgery and Research. 13(1):30910118613018–018. doi: 10.1186/s13018-018-1017-5. doi: 10.1186/s13018-018-1017-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arrow head wounds: major stimulus in the history of surgery. Karger Bernd, Sudhues Hubert, Brinkmann Bernd. Oct 25;2001 World Journal of Surgery. 25(12):1550–1555. doi: 10.1007/s00268-001-0168-3. doi: 10.1007/s00268-001-0168-3. [DOI] [PubMed] [Google Scholar]