

Abstract
To strengthen the Nigeria polio eradication program at the operational level, the National Stop Transmission of Polio (N-STOP) program was established in July 2012 as a collaborative effort of the National Primary Health Care Development Agency, the Nigerian Field Epidemiology and Laboratory Training Program, and the US Centers for Disease Control and Prevention. Since its inception, N-STOP has recruited and trained 125 full-time staff, 50 residents in training, and 50 ad hoc officers. N-STOP officers, working at national, state, and district levels, have conducted enumeration outreaches in 46 437 nomadic and hard-to-reach settlements in 253 districts of 19 states, supported supplementary immunization activities in 236 districts, and strengthened routine immunization in 100 districts. Officers have also conducted surveillance assessments, outbreak response, and applied research as needs evolved. The N-STOP program has successfully enhanced Global Polio Eradication Initiative partnerships and outreach in Nigeria, providing an accessible, flexible, and culturally competent technical workforce at the front lines of public health. N-STOP will continue to respond to polio eradication program needs and remain a model for other healthcare initiatives in Nigeria and elsewhere.
Keywords: national stop transmission of polio, global polio eradication initiative, routine immunization, supplemental immunization activity, Nigeria
Fourteen years after the 2000 initial target date for the global eradication of polio, Nigeria remains one of 3 countries where poliomyelitis is endemic [1]. To interrupt wild poliovirus (WPV) transmission in any country, the Global Polio Eradication Initiative (GPEI) emphasizes 4 main strategies: (1) high polio vaccination coverage in the routine immunization (RI) program, (2) periodic national and subnational supplemental immunization activities (SIAs), (3) containment of localized poliovirus transmission through mop-up campaigns, and (4) enhanced surveillance for detection of acute flaccid paralysis (AFP) cases [2, 3]. In line with these strategies, in 2012 the Nigerian polio program developed a polio eradication emergency action plan, focusing on improving the quality of SIAs, improving vaccination team performance, and increasing accountability of polio eradication staff at all levels. During 2012–2013, the program made considerable progress in strengthening the implementation of polio eradication activities and overcoming some of the chronic barriers to reaching missed children [4].
Despite this progress, WPV transmission persists in a number of high-risk states in northern Nigeria, owing to poor quality campaigns, inadequate technical and managerial capacity at the operational level, suboptimal accountability, and insecurity [3]. To address these challenges, the 2012 Nigerian National Polio Eradication Emergency Plan identified management and technical surge capacity as key strategic priorities for the Nigerian polio program [5]. To strengthen the Nigeria polio eradication program at the operational level, the National Stop Transmission of Polio (N-STOP) program was established in July 2012 as a collaborative effort of the National Primary Health Care Development Agency, the Nigerian Field Epidemiology and Laboratory Training Program (NFELTP), and the US Centers for Disease Control and Prevention (CDC). Founded in 2008, the NFELTP is a 2-year applied epidemiology training program modeled after CDC’s Epidemic Intelligence Service. Like the Epidemic Intelligence Service, one of the main objectives of the NFELTP is to build the local public health workforce. The NFELTP is a collaborative effort among several institutions, including the Federal Ministry of Health, the Federal Ministry of Agriculture and Rural Development, the African Field Epidemiology Network, the University of Ibadan, Ahmadu Bello University, Zaria, and the CDC. Enrollment into the NFELTP program has been on the increase annually, with 38 residents enrolled in 2013.
In this article, we summarize the core activities and major achievements of the N-STOP program during the first year of implementation.
N-STOP PROGRAM OVERVIEW
Approach
The N-STOP program is modeled after the CDC–World Health Organization Stop Transmission of Polio (STOP) program [6, 7]. The N-STOP program provides highly qualified indigenous and culturally competent management and technical support at the most critical operational levels in high-risk districts.
Staffing
In July 2012, 70 Nigerian public health professionals were trained during the first N-STOP short course. Of the 70 medical, veterinary, and allied health professionals trained, 70% were NFELTP residents and graduates, and 30% were counterparts from the Federal Ministry of Health, the Federal Ministry of Agriculture and Rural Development, state governments, and 2 NFELTP-affiliated universities. The second training took place in June 2013 for a new cohort of 32 NFELTP residents and 23 other Nigerian public health professionals from NFELTP-affiliated institutions, yielding 125 trained officers at the national or state levels (Table 1). In 2013, at the request of the National Primary Health Care Development Agency to extend the geographic scope of its activities, the N-STOP program assigned officers to 100 high-risk districts (ie, local government areas [LGAs]) in northern Nigeria (Figure 1). As of November 2013, technical staffing includes 15 full-time officers who are NFELTP graduates, 100 full-time district or LGA-level officers known as N-STOP LGA officers (NSLOs), 50 NFELTP residents in training, and 50 ad hoc N-STOP officers from academic and government institutions. The 15 full-time graduate N-STOP officers work at the national polio eradication Emergency Operations Center (EOC), state EOCs, and state primary healthcare development agencies to support GPEI efforts as part of the state team. State-level N-STOP officers are assigned to each of the 11 northern Nigeria states at high risk for polio, including the federal capital territory, and they report to the director of primary healthcare services at the state ministry of health in their respective states.
Table 1.
National Stop Transmission of Polio (N-STOP) Program Human Resource Capacity Development in States at High Risk for Polio, July 2012–July 2013
| Type of Training | Individuals Trained, No. | States, No. | Trainee Categories |
|---|---|---|---|
| N-STOP short course: overview of GPEI (SIAs, surveillance) | 125 | 14 | NFELTP graduates and residents, FMoH and FMARD project officers, state GPEI officers and university faculty |
| Local capacity development | 17 | 9 | Veterinary officers, agricultural extension workers, public health officers |
| Field-based training (as enumerators) | 1976 | 18 | Agricultural extension and animal health officers, teachers, health workers |
| Strengthening RI | 500 | 11 | Veterinarians, public health officers, nurses, and other degree holders |
Abbreviations: FMARD, Federal Ministry of Agriculture and Rural Development; FMoH, Federal Ministry of Health; NFELTP, Nigeria Field Epidemiology and Laboratory Training Program; GPEI, Global Polio Eradication Initiative, Polio Eradication Initiative; RI, routine immunization; SIA, supplemental immunization activity.
Figure 1.
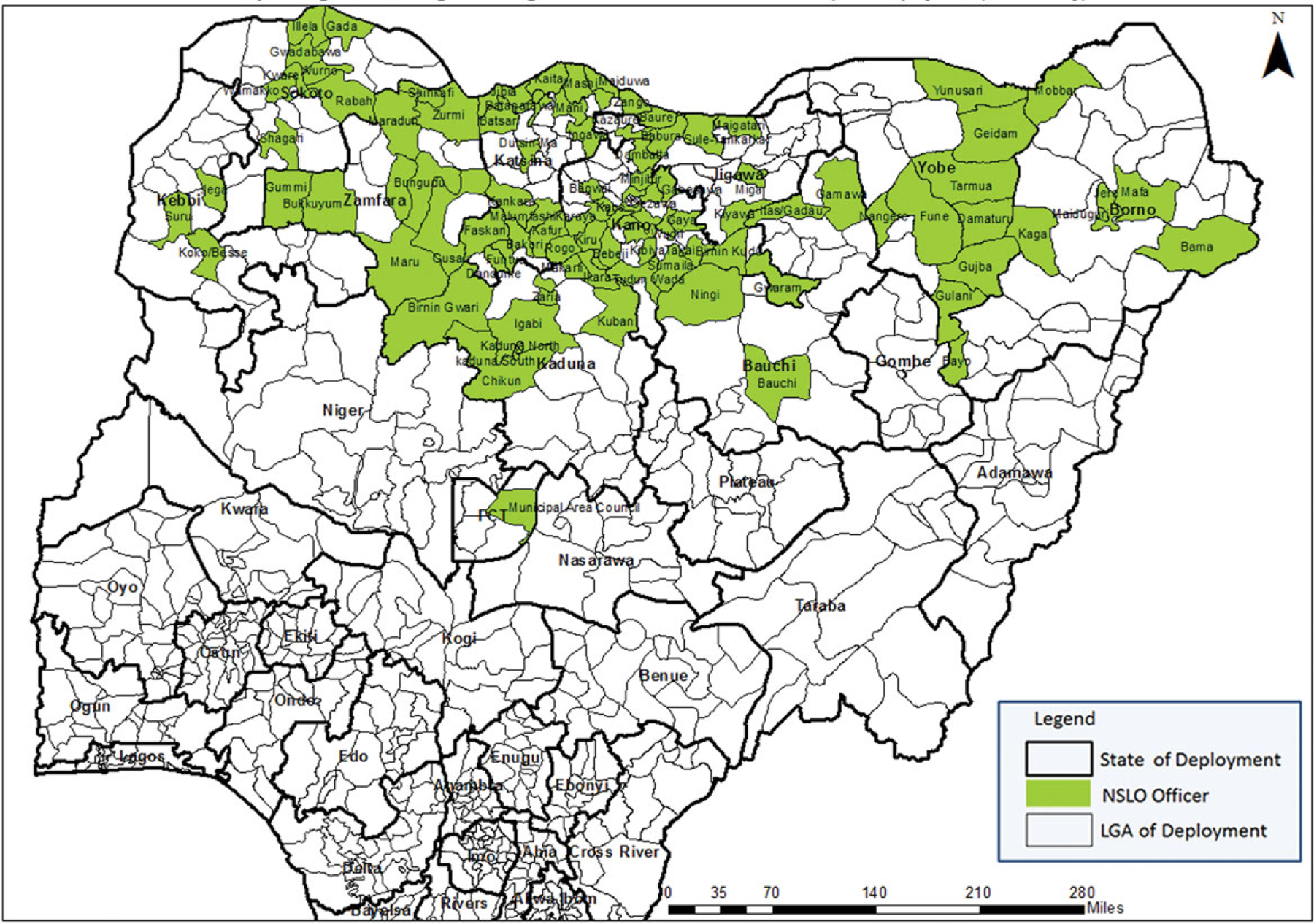
Geographic distribution of the assignment of National Stop Transmission of Polio (N-STOP) program local government area (LGA) officers in Nigeria, by LGA, as of July 2013.
Training
The N-STOP short-course training modules were adapted from the CDC–World Health Organization STOP program to include Nigeria-specific modules. The modules are based on adult learning principles and include participatory exercises, role-playing and development of interpersonal communication skills. Content includes technical aspects of poliomyelitis, GPEI, and the Expanded Program on Immunization (EPI), as well as good management and problem-solving practices. In addition to this basic central training, N-STOP uses an applied periodic modular training model to strengthen EPI at the district level in 100 LGAs.
Terms of Reference
The terms of reference for N-STOP officers varies on the basis of their assignments. To minimize duplication of efforts of other partners, the program focuses on providing a flexible workforce that can address diverse needs of the Nigeria polio eradication program at the national, state, and local levels. During its first year, N-STOP assisted in (1) strengthening overall program management, (2) conducting outreach to underserved populations, (3) providing targeted technical assistance at all levels, (4) strengthening routine immunization, (5) conducting applied research, and (6) training managers and developing management capacity.
RESULTS AND ACHIEVEMENTS
Strengthening Overall Management of the Polio Eradication Program
Since its inception, N-STOP officers have formed part of the management cadre of the polio program, through their membership in the polio eradication core group (a strategic and operational think-tank for the national polio program) and in the EOCs at both national and state levels. At the operational level, N-STOP officers have supported the planning, implementation, supervision, and monitoring of polio SIAs in 17 states and the Federal Capital Territory. Under the direction of the national EOC, N-STOP has supported deployment of senior level staff to serve as members of management support teams who are deployed before SIAs, to provide management and technical oversight of key activities and thereby ensure high-quality SIAs. Management support teams are assigned to the most challenging districts, and members work with the district GPEI team and community leaders to improve vaccination team performance, increase access to hard-to-reach, underserved and insecure settlements, and resolve noncompliance issues.
Outreach to Underserved Populations
A key challenge to polio eradication in Nigeria has been development of sustainable outreach strategies to nomadic, remote and scattered settlements [8]. In July 2012, N-STOP officers piloted an outreach strategy that included organizing meetings between leaders from underserved communities and primary healthcare and GPEI staff at the district level. The community leaders were requested to bring a list of all settlements in their jurisdiction. The settlement lists were harmonized with the lists provided by the district-level polio SIA planning teams. N-STOP officers observed that many nomadic, remote, and scattered settlements were left out of local microplans and that vaccination teams and independent campaign monitors tended to miss these settlements systematically. Major barriers to reaching these communities include the remoteness of the settlements, difficulty in accessing the settlements, lack of adequate resources to support outreach teams, and frequent seasonal movements of the nomads in some of these communities.
To address these barriers, N-STOP officers worked with community leaders to conduct outreach to these settlements, starting in August 2012. Teams were deployed to enumerate settlements and administer oral polio vaccine to unvaccinated children (so-called 0-dose children). During the enumeration, additional settlements were found that were not known either to local community leaders or to the district level polio teams. On the basis of the lessons learned from these exercises, N-STOP developed a standard operating procedure for outreach to underserved communities, which has been adopted by the national polio program. This standard operating procedure has been updated constantly on the basis of findings from the field and documentation of best practices. Using the standard operating procedure, the national program conducted subnational immunization campaigns during January and June 2013 that focused on underserved areas. The EOC also mandated the N-STOP to scale up efforts to further characterize and reach these communities during 2012–2013.
During August 2012–July 2013, N-STOP officers conducted enumeration and landscape analysis of nomadic, scattered, and hard-to-reach border settlements in 253 LGAs across 17 northern states and the federal capital territory (Figure 2). Local veterinarians, animal health and agricultural extension workers, teachers, and primary healthcare workers were trained for the enumeration outreach exercise and worked under the supervision of N-STOP state field coordinators. These field workers were selected because of their familiarity with the underserved communities, because they often interact regularly with the underserved populations or their animals. During the enumeration outreach activities, the program introduced the use of smart phones and geographic information system technology to map settlements, collect census data, and identify AFP cases. N-STOP officers trained field-based personnel at both the LGA and ward levels in the use of these technologies, thereby boosting local public health capacity.
Figure 2.
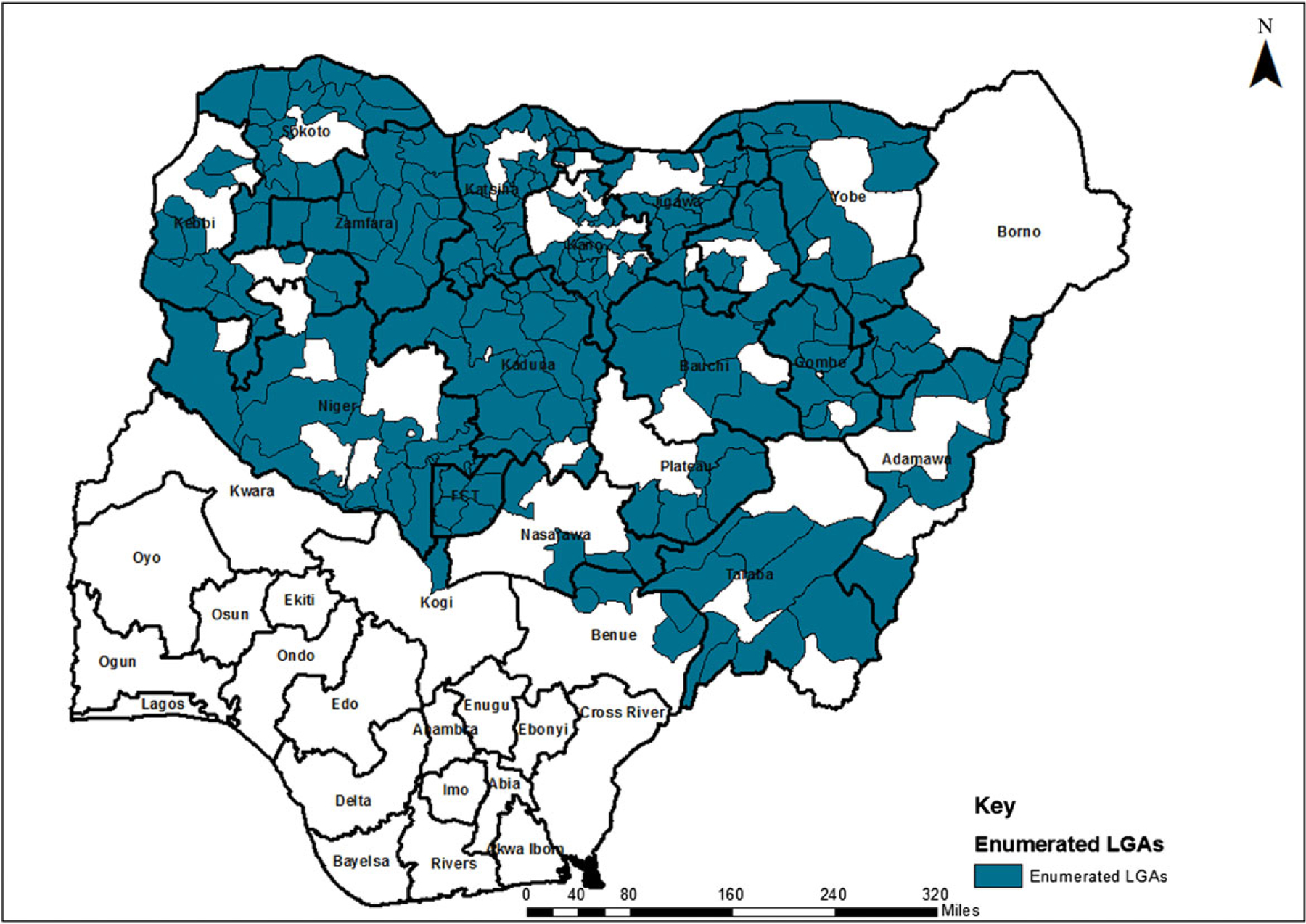
Geographic distribution of local government area (LGAs) enumerated by the National Stop Transmission of Polio (N-STOP) program in Nigeria during Immunization Plus Days from August 2012 to July 2013.
Over the 1-year implementation period of these outreach efforts, N-STOP teams have discovered up to 200 unreported suspected AFP cases that occurred within 6 months of the date of each outreach exercise, as well as numerous settlements naive to polio vaccination campaigns. Of the 46 437 settlements enumerated in the first 1-year period of activities, 5112 (11%) had never been included in previous SIAs or RI activities. In these 5112 settlements, 58 074 children <5 years of age had never received the first dose of any vaccine. In addition, N-STOP officers identified 8607 settlements (18.5%) that were not visited during the preceding SIA. A total of 63 850 0-dose children <5 years of age were identified, of which 36 773 (57.6%) were vaccinated by N-STOP officers during these activities. Eradication of polio from Nigeria depends on continuing to identify previously missed settlements and 0-dose children and ensuring that they are integrated into future vaccination campaigns and RI services.
Targeted Technical Assistance for Polio Eradication Activities
Surveillance Assessments, Outbreak Investigations, and Response
N-STOP officers have provided support during 11 polio case investigations and surveillance assessments in 5 states. Many of these outbreaks occurred in settlements close to nomadic and border communities; N-STOP has played an important role in ensuring that these communities are vaccinated as a part of the outbreak response. N-STOP officers have also responded to 29 outbreaks of other vaccine-preventable diseases, including 17 measles outbreaks and 1 suspected diphtheria outbreak across 15 states in Nigeria. In addition to providing highly skilled services, these activities allowed resident N-STOP officers to fulfill their NFELTP training requirements or core activities of learning.
Support of Immunization Plus Days
Conducting high-quality SIAs is vital for interrupting WPV transmission [9]. Since the establishment of the N-STOP program, officers have been deployed repeatedly to 236 LGAs in 17 northern states and the Federal Capital Territory to support Immunization Plus Days. Generally, officers provide support for microplan reviews and updates, with special focus on the inclusion of newly discovered underserved settlements in the updated microplan, selection and training of vaccination teams and independent monitors, strengthening coordination and supervision of immunization activities at the LGA level, and supporting the monitoring and supervision of vaccination teams during implementation. In April 2013, the EOC developed a more structured approach for providing technical and oversight support to high-risk districts and subdistricts through the deployment of multidisciplinary management support teams, including N-STOP officers as team members; the N-STOP officers focus on coordinating outreach to underserved communities.
RI Strengthening
Strengthening the routine infant and childhood immunization program is a key component of the overall strategy for polio eradication [2, 3]. In June 2012, the national polio EOC identified 107 polio high-risk LGAs across 14 northern Nigerian states, based on the CDC–Global Good risk analysis algorithm. To help increase RI coverage, the N-STOP program recruited, trained, and deployed 100 NSLOs to 100 (93%) of 107 districts in 11 of 14 states (including the federal capital territory) classified as high risk (Figure 1). The NSLOs work under the supervision of the district directors of primary healthcare services and N-STOP state team leads. The NSLOs are contracted for a 1-year period, renewable every 3 months, to help implement an applied training program for district level staff on RI-specific modules (Table 2). The thematic modules cover all aspects of RI and are linked with structured applied follow-up field or service exercises to implement what is learned in the training using a systematic work plan. Tools and operational funding support are provided to execute these assignments, with oversight provided by the N-STOP state team leads. Participants report on the implementation of the applied assignments in the follow-up courses, to ensure that training activities are applied successfully. This applied training model has been successful in improving RI planning and service delivery at the ward and settlement levels, especially among underserved populations. On the basis of the successful implementation of this model of training, N-STOP has been requested to expand the training to all districts in a number of northern states where the risk of polio is high.
Table 2.
Thematic Training of District-Level Team on Routine Immunization (RI) and Post-Training Assignments in 2013
| Thematic Area of Training | Participants | Post-Training Assignment |
|---|---|---|
| Overview of RI | LIO, NSLO, partners | Baseline assessment |
| RI microplanning | LIO, NSLO, partners | Reach every ward microplanning |
| Vaccine and cold chain management | LIO, cold chain officer, NSLO, partners | Cold chain assessment, implementation of vaccine management standard operating procedures |
| Service delivery and supportive supervision | LIO, health educator, NSLO, partners | Cascade training on best practices to health facility personnel, supervisory plan |
| Data management | LIO, M&E officer, NSLO, partners | Use of DHIS for district |
| Monitoring and evaluation | LIO, M&E officer, NSLO, partners | Coverage survey |
| Campaign management | LIO, health educator, NSLO, partners | Vaccinator training |
| Community demand | LIO, health educator, NSLO, partners | Community engagement |
| Surveillance for VPD | LIO, NSLO, partners | AFP surveillance assessment |
Abbreviations: DHIS, District Health Information System; LIO, local immunization officer; M&E, monitoring and evaluation; NSLO, National Stop Transmission of Polio program local government area officer; VPD, vaccine-preventable disease;
Epidemiological Studies and Applied Research
As programmatic needs evolve, N-STOP officers have designed and conducted epidemiological and operational research to support priority polio eradication activities. Often, these needs develop quickly, based on emerging issues, and timely results are expected with minimal delay. N-STOP has provided the capacity and flexibility to execute this type of work efficiently. Studies performed during July 2012–April 2013 are summarized in Table 3. Findings of these studies have been presented to the national polio EOC team, as well as at the 24th and 25th national polio/routine immunization expert review committee meetings. The findings have been useful for informing critical strategic decision making, including (1) the expert review committee’s recommendation to place greater attention on reaching underserved populations, (2) the United Nations Children’s Fund’s intensification of grass-roots social mobilization and community engagement strategies to resolve oral polio vaccine refusal issues, (3) the EOC’s decision to delay plans for expansion of the oral polio vaccine target age group for vaccination during a combined oral polio vaccine–MenAfriVac campaign, and (4) the decision to delay the scale up of the new vaccination team training modules.
Table 3.
Epidemiological and Programmatic Research Studies Performed to Improve Polio Eradication Initiative Activities by the National Stop Transmission of Polio (N-STOP) Program, Nigeria, 2012–2013
| Study | Description | Scale | Key Findings | Outcome |
|---|---|---|---|---|
| 1 | Oral polio vaccination knowledge, attitude and practices among nomadic Fulani populations | 10 LGAs in 7 states | Poor knowledge about OPV, low access to OPV, and high willingness to accept the vaccine if offered | Scale-up of the outreach to underserved populations in all LGAs in high-risk states |
| 2 | Assessing the acceptability of expanding the eligible age group for OPV and acceptance of a proposed combined OPV and MenAfriVac (cerebrospinal meningitis vaccine) | Kumbotso LGA, Kano State | Focus group participants expressed strong reservations about expanding the age group for polio immunization | Expansion of the age group was delayed until better social mobilization strategies are in place |
| 3 | Baseline assessment of routine infant immunization services in 8 high-priority LGAs with cVDPV outbreaks | Kano, Bauchi, Jigawa, Katsina, Sokoto, Zamfara, and Niger states | A high burden of vaccine-preventable diseases, poor RI coverage with high dropout rates. Very limited human resource capacity, inadequate cold chain and service delivery logistics, and poor and outdated RI microplans | LGA level scale-up of N-STOP, BMGF RI intensification project, and other partner efforts to strengthen RI at the ward and settlement levels |
| 4 | Evaluation of why children are missed during IPDs | 8 LGAs in 6 states | Some of the major reasons included low polio risk perception, more concerns about other health issues, lack of awareness, teams not visiting homes or child being absent during team visits, and lack of access to OPV | Improved social mobilization activities before and during IPD campaigns and provision of incentives targeting communities with a high proportion of missed children |
| 5 | Evaluation of the nomads outreach strategy | 10 LGAs in 4 states | 95% of children who received 0 doses of polio vaccine and were identified during the nomads outreach during August 2012–March 2013 have received at least 2 doses of OPV | Scale-up of the outreach strategy to other states and adoption of the N-STOP approach by the national EOC |
| 6 | Evaluation of the efficacy and acceptability of a new vaccination team training package developed by the national program | 15 LGAs in 8 states | Most participants preferred the new package, but there was no significant difference in team performance between those who received the new training package and those who received the old training package | Old training package was maintained; some states rolled out the new package because of its better visual aid and interactive design |
| 7 | Evaluation of unreported or missed AFP cases | 2 LGAs in 1 state | One of 5 AFP cases was confirmed as due to WPV1 and was epidemiologically linked to the others | LGA polio program officers were made aware of the need for enhanced AFP surveillance in nomadic settlements |
| 8 | Evaluation of AFP surveillance systems | 4 LGAs in 4 states | The surveillance systems were useful but suboptimal in efficiency, with opportunities for capacity and management improvements | Improved local case-investigation process and documentation of the identified gaps for resolution |
Abbreviations: AFP, acute flaccid paralysis; BMGF, Bill and Melinda Gates Foundation; cVDPV, circulating vaccine-derived poliovirus; EOC, emergency operations center; IPD, Immunization Plus Day; LGA, local government area; OPV, oral polio vaccine; WPV1, wild poliovirus type 1.
DISCUSSION
The rapid scale up and implementation of the N-STOP program has significantly enhanced GPEI partnerships in Nigeria and reflects the successful collaboration among several organizations, including NPHCDA, NFELTP, the Federal Ministry of Health, the Federal Ministry of Agriculture and Rural Development, leading universities, the CDC, and other GPEI partners. Through its networking, the program provides targeted technical assistance in several areas of polio eradication activities at the national, state, and district levels. Documented evidence confirms the value of intersectorial (animal, human, and environment) collaboration in the surveillance and control of emerging infectious diseases, food safety, and zoonoses [5, 10–13]. The N-STOP program has taken advantage of its wide network across these sectors to enhance collaborations between the animal and human health sectors, with the objective to improve community linkages. Such linkages are aimed at identifying underserved nomadic communities and reaching them with basic primary healthcare services. The adoption of standard operating procedures for outreach to underserved populations and the applied training in RI are helping to transform service delivery at the local level.
The use of indigenous Nigerian epidemiologists to solve the unique problems faced by the polio program ensures the availability of culturally competent and technically sound staff members who are well equipped to tackle the programmatic issues facing the program. This approach should be extended beyond vaccination activities and the healthcare system to other sectors of the Nigerian society. Building local capacity is key to the sustainability of any development work.
The N-STOP program has benefited from a structured supervisory approach for monitoring and accountability of local officers. In addition, through research activities, N-STOP officers are providing data for evidence-based decision making. Going forward, N-STOP will continue to respond to emerging issues of the Nigerian polio program. Future opportunities to leverage the N-STOP approach should be further explored, including using current relationships and networks to expand the reach of other primary healthcare services and enhance community-based disease surveillance activities. It is hoped that when polio has finally been eradicated, the N-STOP model will be a framework to boost provision of other primary healthcare services, especially with respect to other vaccine-preventable diseases, and also serve as a significant source for future public health leadership in Nigeria.
Financial support.
This work was supported by the Centers for Disease Control and Prevention.
Footnotes
Presented in part: African Field Epidemiology Network Conference, Addis Ababa, Ethiopia, November 2013.
Supplement sponsorship. This article is part of a supplement entitled “The Final Phase of Polio Eradication and Endgame Strategies for the Post-Eradication Era,” which was sponsored by the Centers for Disease Control and Prevention.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed
References
- 1.Global Polio Eradication Initiative. Infected countries Geneva: GPEI, 2013. http://www.polioeradication.org/Infectedcountries.aspx. Accessed 21 May 2013. [Google Scholar]
- 2.Global Polio Eradication Initiative. Strategy Geneva: GPEI, 2010. http://www.polioeradication.org/Aboutus/Strategy.aspx. Accessed 21 May 2013. [Google Scholar]
- 3.Independent Monitoring Board of the Global Polio Eradication Initiative: report, May 2013. Geneva: Global Polio Eradication Initiative, 2013. http://www.polioeradication.org/Aboutus/Governance/IndependentMonitoringBoard.aspx. Accessed 30 June 2013. [Google Scholar]
- 4.Nigeria National Polio Eradication Emergency Plan (NPEP) 2012. http://www.polioeradication.org/Portals/0/Document/Aboutus/Governance/IMB/7IMBMeeting/7.3_7IMB.pdf. Accessed 28 June 2013. [Google Scholar]
- 5.Schelling E, Bechir M, Ahmed MA, Wyss K, Randolph TF, Zinsstag J . Human and animal vaccination delivery to remote nomadic families, Chad. Emerg Infect Dis 2007; 13:373–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention (CDC). History of the Stop Transmission of Polio (STOP) Program Atlanta, GA: US Department of Health and Human Services, CDC, 2012. http://www.cdc.gov/polio/stop/about.htm. Accessed 9 December 2013. [Google Scholar]
- 7.Centers for Disease Control and Prevention (CDC). The Global Polio Eradication Initiative Stop Transmission of Polio (STOP) Program—1999–2013. MMWR Morb Mortal Wkly Rep 2013; 62:501–3. [PMC free article] [PubMed] [Google Scholar]
- 8.Centers for Disease Control and Prevention (CDC). Polio field census and vaccination of underserved populations—northern Nigeria, 2012– 2013. MMWR Morb Mortal Wkly Rep 2013; 62:663–5. [PMC free article] [PubMed] [Google Scholar]
- 9.Malhotra V Lessons from observation of supplementary immunization activity in India. Online J Health Allied Scs 2012; 11:11. http://www.ojhas.org/issue41/2012-1-11.htm. Accessed 21 May 2013. [Google Scholar]
- 10.Kahn LH. Confronting zoonoses, linking human and veterinary medicine. Emerg Infect Dis 2006; 12:556–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Khan LH, Kaplan B, Steele JH. Confronting zoonoses through closer collaboration between medicine and veterinary medicine (as ‘one medicine’). Vet Ital 2007; 43:5–19. [PubMed] [Google Scholar]
- 12.Schelling E, Wyss K, Béchir M, Daugla D, Zinsstag J. Synergy between public health and veterinary services to deliver human and animal health interventions in rural low income settings. Br Med J 2005; 331:1264–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Graham JP, Leibler JH, Price LB, et al. The animal-human interface and infectious disease in industrial food animal production: rethinking biosecurity and biocontainment. Public Health Rep 2008; 123:282–99. [DOI] [PMC free article] [PubMed] [Google Scholar]