

Abstract
Background:
Suture button fixation is frequently used to stabilize the distal tibiofibular syndesmosis in athletes sustaining an isolated ligamentous syndesmosis injury.
Purpose:
To report on a series of periprosthetic fibula fractures adjacent to the lateral suture button after a subsequent unrelated ankle injury or progressive stress injury after initial ankle syndesmosis stabilization using the knotless TightRope (Arthrex).
Study Design:
Case series; Level of evidence, 4.
Methods:
Eight elite athletes with periprosthetic fibula fractures and stress injuries around the lateral suture buttons were evaluated. In all athletes, the knotless TightRope had been used to stabilize an isolated ligamentous ankle syndesmotic injury, after which all patients recovered and returned to professional sports at their preinjury level. The athletes subsequently developed an acute fibula fracture or a fibula stress fracture related to the 3.7-mm drill hole in the fibula adjacent to the lateral suture buttons after a mean of 14.1 months (range, 5-29 months). The management of these complications was analyzed.
Results:
Five athletes sustained a periprosthetic fibula fracture in the form of undisplaced spiral Weber B injuries after a subsequent, unrelated injury. Poor healing response was noted with initial nonoperative treatment for the first 2 athletes, and surgical intervention was performed with successful union of the fracture and return to sports. The subsequent 3 athletes had early surgery with uneventful recovery. Another 3 athletes developed stress injuries adjacent to the fibula suture button without a history of acute trauma. In 2 of the 3 athletes, the position of lateral suture buttons was in the anterior third of the fibula. Initial nonoperative management yielded poor healing response, and subsequent surgical intervention was required to enable healing and return to sports.
Conclusion:
Nonoperative management of fractures adjacent to the fibula suture button of a knotless TightRope may lead to a delay in union. Therefore, early surgical intervention should be considered in elite athletes, whose return-to-sports time is critical. Care is needed to ensure that the fibula hole for the suture button is centrally located because the eccentric placement of the fibula hole in the anterior third of the fibula may contribute to the development of a stress reaction or stress fracture. Surgical intervention for a periprosthetic fibula stress fracture leads to satisfactory resolution of symptoms.
Keywords: periprosthetic fibula fracture, stress injury, suture button fixation, syndesmosis injury, TightRope
Ankle injuries account for 17% of all English Premier League soccer injuries, equating to a typical first team expecting 1 ankle injury in a player approximately every 10 games. 13 In the Premiership Rugby, ankle injuries have been reported to occur at an incidence of around 6 per 1000 player-hours. 2 It has been reported that ankle syndesmosis injury occurs in 1% to 18% of all ankle sprains in the general population,3,7,13,17 although it is a more commonly encountered injury in athletes.6,12 Ankle syndesmosis injuries are also more commonly associated with residual symptoms that can lead to prolonged dysfunction when compared with ankle lateral ligament sprains in an athletic population.6,12
Suture button syndesmotic fixation devices have gathered popularity over the last 15 years for the treatment of syndesmosis injuries.10,12,16,18,21 Reported advantages of the suture button device over screw fixation include dynamic stabilization that allows rotation of the fibula during ankle movements while maintaining accurate reduction of the syndesmosis.10,12,16,18,21 This, along with the low-profile design of the implant, is said to offer biomechanical superiority to screw fixation, reduce the need for implant removal, eliminate screw breakage, and avoid the risk of late diastasis.10,12,16,18,21 In addition, the newer suture button implant utilizes a fibula plate to distribute the forces along the fibula better when using 2 suture button devices (Dual Syndesmosis TightRope implant and Syndesmosis TightRope XP Buttress Plate implant; both by Arthrex) to protect against stress risers.
When originally introduced, the TightRope (Arthrex) came in a knotted design. The main complication recognized in the knotted suture button fixation was the presence of the prominent knot in the No. 5 FiberWire (Arthrex) beneath the thin subcutaneous layer of the lateral ankle, which could lead to skin and soft tissue irritation, wound infections, wound granuloma formation, and cases of osteomyelitis in the distal tibia.11,19,21 In 2012, it was changed to a knotless design to overcome this problem. 4
The 2 senior authors (J.C. and T.C.) treat ankle injuries in elite athletes and regularly use suture button fixation for isolated ligamentous ankle syndesmotic injuries (without fracture). Both surgeons independently recognized that some athletes developed a periprosthetic fibula fracture around the knotless suture button. This had not been seen with the knotted predecessor. There are no reported cases of periprosthetic fracture in the peer-reviewed or manufacturer's literature for either the knotted or the knotless suture button fixation. The aim of this study was to report this complication, provide advice on management options, and explore potential predisposing mechanisms that may help prevent its occurrence.
Methods
This was a retrospective case series of 8 elite athletes (professional football and rugby players) managed by the 2 senior authors (J.C. and T.C.) between 2014 and 2020. After an unrelated subsequent ankle injury, athletes with periprosthetic fibula fractures around the knotless suture buttons were included in this study. The exclusion criteria were ankle syndesmosis injuries with associated fractures. This study was determined to be exempt from institutional review board approval.
In this series, the knotless suture button TightRope was used in all athletes to stabilize isolated ligamentous ankle syndesmotic injuries without any associated fractures or dislocations (unstable grade 2 syndesmosis injuries). After surgical syndesmotic stabilization, all patients had returned to professional sports at their preinjury level and were asymptomatic. These athletes subsequently developed either an acute fracture after a further ankle injury or a stress fracture. Both were related to the 3.7-mm drill hole in the fibula adjacent to the lateral suture button device. All case notes and imaging were reviewed, detailing the initial injury fixation, duration before reinjury, reinjury mechanism, level of the periprosthetic fracture, associated injuries (deltoid or medial malleolar fracture), and the management details of this subsequent injury.
In the initial presentation for ankle syndesmotic injuries, all the included athletes had signs of unstable syndesmosis—including tenderness over the anterior inferior tibiofibular ligament (AiTFL) and the anterior interosseous membrane during palpation, a positive squeeze test, and a positive external rotation test. They also had preoperative magnetic resonance imaging (MRI) confirming injury to the AiTFL and syndesmosis. There were no cases with associated fractures, dislocations, or deltoid ligament ruptures requiring surgical repair. In terms of surgical procedures, all patients had a routine ankle diagnostic arthroscopy to assess the syndesmosis stability, during which direct visualization confirmed the ruptured AiTFL, the syndesmosis widening during the external rotation test and during insertion of the 4.5-mm shaver blade into the distal syndesmosis. The remnant AiTFL and synovitis were debrided as necessary. The TightRope fixation was then performed according to standard techniques under fluoroscopic guidance. The senior authors routinely insert the guidewire from the posterolateral cortical apex of the fibula aiming toward the anteromedial cortical apex of the tibia angled at 30° anterior to the coronal plane and placed 2 cm above the tibia plafond under fluoroscopic guidance.
Postoperatively, patients were placed in an Aircast XP Walker boot (DJO Global) for 3 weeks and mobilized nonweightbearing for 1 week, partial weightbearing for 1 week, and then allowed to full weightbearing. Ankle range of motion and proprioceptive exercises were commenced within the first 3 weeks. Heavy-impact activities were encouraged progressively from week 6 onward as tolerated.
Results
All 8 included athletes were male professional soccer and rugby players aged 19 to 31 years (mean, 23.4 years). All had undergone previous fixation of an isolated ligamentous ankle syndesmosis injury using a knotless TightRope device—7 athletes had a single suture button device and 1 athlete had 2 suture button devices inserted. All athletes had returned to full sports participation at the same preinjury level of competition at a mean of 13.5 weeks postoperatively (range, 12-16 weeks).
Five athletes sustained a periprosthetic fibula fracture after a subsequent, unrelated injury. The median time between initial syndesmotic injury requiring TightRope fixation and subsequent injury with periprosthetic fibula fracture was 23 months (range, 7-29 months). These 5 injuries were undisplaced spiral Weber B injuries, with the fracture propagating through the fibula suture button drill hole. These undisplaced fractures were all recognizable on plain radiographs, although some patients had computed tomography (CT) scans performed to evaluate the extent of the fracture. In the single player with 2 TightRope devices in situ, the fibula fracture occurred at the distal TightRope drill hole adjacent to the lateral suture button. The fracture displaced none of the fibula suture buttons from their positions. All the suture button positions were at the central or posterior third of the fibula (sagittal profile), except for 1 patient with suture button fixation at the anterior third of the fibula. Table 1 summarizes the athlete characteristics.
Table 1.
Characteristics of the Elite Athletes a
| Athlete | Age, y | Sport | Primary Procedure | Suture Button Placement | Secondary Injury | Time to Secondary Injury, mo | Injury Mechanism | Management |
|---|---|---|---|---|---|---|---|---|
| 1 | 19 | Rugby | Single TightRope | Anterior third of fibula | Undisplaced Weber B fibula fracture | 10 | External rotation | Initially nonoperative management, then removal of suture button and ORIF because of delayed healing at 8 wk |
| 2 | 20 | Soccer | Single TightRope | Central fibula | Undisplaced Weber B fibula fracture | 29 | External rotation | ORIF and replacement TightRope |
| 3 | 26 | Soccer | Single TightRope | Central fibula | Undisplaced Weber B fibula fracture | 23 | Collision during a tackle | Initially nonoperative management, then ORIF and replacement TightRope because of delayed healing at 10 wk |
| 4 | 20 | Soccer | Single TightRope | Central fibula | Undisplaced Weber B fibula fracture | 26 | Collision during a tackle | Removal of suture button and ORIF |
| 5 | 25 | Rugby | Double TightRope | Central fibula | Undisplaced Weber B fibula fracture at the distal drill hole | 7 | Fell during scrum | Removal of suture button and ORIF |
| 6 | 23 | Soccer | Single TightRope | Anterior third of fibula | Anterior cortical stress fracture | 6 | No direct injury but progressive pain and aches | Initially nonoperative management, then ORIF and bone graft because of no evidence of healing and continuing pain at 8 wk |
| 7 | 25 | Soccer | Single TightRope | Anterior third of fibula | Anterior cortical stress fracture | 7 | No direct injury but progressive pain and aches | ORIF and bone graft |
| 8 | 31 | Soccer | Single TightRope | Central fibula | Stress reaction to pain | 5 | No direct injury but progressive pain and aches | Removal of suture button |
ORIF, open reduction and internal fixation.
In terms of treatment, the first 2 players in this series were initially managed nonoperatively for 8 (athlete 1) and 10 (athlete 3) weeks, respectively, in a weightbearing Aircast XP Walker boot (DJO Global) using a bone stimulator (Exogen; Bioventus) but failed to show any progress to healing and thus underwent open reduction and internal fixation (ORIF) with fibula plate fixation and removal (athlete 1) or replacement (athlete 3) of the TightRope device (Table 1 and Figures 1 and 2). They subsequently went on to uncomplicated full union and returned to full sports after the surgery. All other players were subsequently managed with early ORIF of the fibula and had an uneventful recovery. They all returned to their sports at their preinjury level of competition at 12, 13, and 12 weeks, respectively. Of these 5 players, 3 had the TightRope completely removed, while 2 had a replacement TightRope inserted (Table 1). For all cases, the syndesmosis was tested after the initial TightRope was removed, and a new TightRope was inserted only if the syndesmosis tested unstable.
Figure 1.
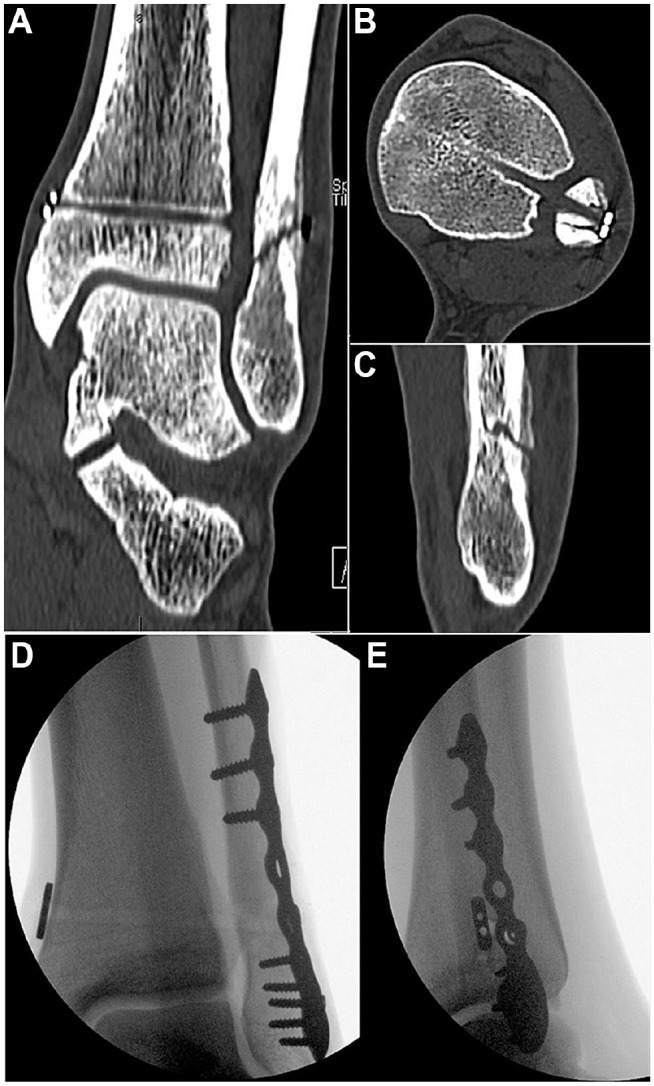
(A-C) CT scans from athlete 3, diagnosed with undisplaced Weber B fracture after an unrelated injury initially treated nonoperatively, with minimal to no healing response at 10 weeks. (D and E) Intraoperative imaging showed open reduction and internal fixation of the fibula with the replacement of the suture button device in a new position because the syndesmosis was noted to be unstable. CT, computed tomography.
Figure 2.

(A and B) Initial radiographs of undisplaced Weber B fibula fracture after an unrelated injury in athlete 1, with the lateral suture button located at the anterior third of the fibula. (C and D) Radiographs at 6 weeks after removal of the suture button device and open reduction and internal fixation of the fibula. The syndesmosis was tested intraoperatively to be stable, and no TightRope replacement was performed.
On the other hand, 3 other athletes developed pain adjacent to the fibula suture button during normal play and training without any specific injury (Table 1). Imaging modalities such as MRIs and CT scans confirmed that 2 of the 3 athletes had sustained a stress fracture, and the other one had a stress reaction of the fibula just next to the fibula suture button. The median time between initial syndesmotic fixation and subsequent stress injury was 6 months (range, 5-7 months). Contrary to the initial 5 athletes with acute fibula periprosthetic fracture, it was observed that the fibula suture buttons in the 2 athletes with stress fractures were in the anterior third of the fibula (sagittal profile) rather than being central or posteriorly located. The first athlete with fibula stress fracture was treated with an initial period of nonoperative management (off-loading and Exogen bone stimulator for 8 weeks) but failed to heal. He underwent fibula ORIF with plate fixation and autogenous bone grafting. CT scans at 10 weeks confirmed fracture healing, and he returned to full sports at 13 weeks. The second athlete with stress fracture was treated with fibula ORIF and bone grafting early due to initial experience. The TightRope devices were removed for these 2 athletes and were not replaced. In the case of stress reaction, the TightRope was removed without fixation, and he could return to sports uneventfully (Figures 3 and 4). Additionally, all 8 athletes had their serum calcium and 25-hydroxy vitamin D levels screened at the time of periprosthetic fibula fractures and stress injuries, with adequate levels noted.
Figure 3.

(A and B) Coronal and (C and D) axial MRI images of bone marrow edema and stress reaction at the fibula suture button drill hole in athlete 8. MRI, magnetic resonance imaging.
Figure 4.

(A-C) CT scans of stress reaction at the fibula suture button drill hole in athlete 8. (D-F) CT scans of healing response at the drill hole 6 weeks after removal of the suture button device. CT, computed tomography.
Discussion
The most important message in this case series is to recognize that acute fractures and stress-related injuries to the fibula may occur adjacent to the fibula suture button after subsequent unrelated ankle injury or via progressive stress injury and that nonoperative management may lead to a significant delay in fracture union. Therefore, early surgical intervention is recommended for elite athletes in such circumstances. Furthermore, an eccentrically placed (anterior) fibula drill hole for the lateral suture button may predispose to a stress-related injury in high-demand athletes.
In our experience, the 2 senior authors had independently initiated nonoperative management for each of their first cases. However, they noted a delay in fracture union clinically and on CT scanning at 8 to 10 weeks. This was deemed unacceptable for elite professional athletes, for whom early return to play is critical.1,3,5,12 Therefore, management was changed to removal of the TightRope device and plate fixation of the fracture. Subsequently, all cases were treated with the removal of the previous syndesmotic suture button device and primary surgical plate fixation. If there was any clinical evidence of syndesmosis instability during the ORIF fibula, a TightRope replacement would be inserted in a different position. It was difficult to comment whether the syndesmosis instability was from the initial injury or the subsequent injury, although the only 2 athletes who needed TightRope replacement were both in the acute periprosthetic fractures group. None of the stress fracture/injury cases required TightRope replacement. These fractures united with players returning to elite sports at their previous level. No player has had further ankle symptoms related to the fibula or syndesmosis.
We postulate that the No. 5 FiberWire suture material in the suture button drill hole may impede normal fracture callus formation with persistent micromotion at the fracture site, delaying fracture healing. This echoes the suggestion by Hohman et al, 9 when discussing a case report of a tibia and fibula fracture through a suture button tract, that the nonabsorbable sturdy nature of the suture material can result in repetitive disruption of bone healing at the drill hole. This was also illustrated by Leucht et al 15 in their histological analysis of a murine model on skeletal regeneration around implants, where they showed that bony encapsulation occurs when implant micromotion creates a low strain of 0.20 to 0.50; however, when effective strain exceeds 0.50, bone matrix deposition is inhibited and fibrous tissue occupies the site. 1 We also concur with Hohman et al 9 that the presence of the suture material in the drill hole may represent a region of high strain with constant loading interrupting bone healing. Removal of the suture material and plate fixation, by contrast, stabilizes the fracture sufficiently to allow the progression of normal callus formation, maturation, and healing.
Eccentric placement of the TightRope in the fibula at the time of initial syndesmosis stabilization may occur inadvertently while directing the guidewire/drill toward the anteromedial tibia. This likely occurs when the guidewire skives toward the anterior aspect of the fibula because of the anatomical curve anteriorly from the fibula ridge and may remain undetected on the intraoperative fluoroscopy. The eccentric placement of the lateral suture button may lead to increased stress at the bone and suture button interface, leading to a stress riser, while the nonabsorbable nature of the No. 5 FiberWire suture material prevents the drill hole from healing, as previously discussed. In this series, the 2 fibula stress fractures occurred when the TightRope was misplaced in the anterior third of the fibula and the drill hole was directed anteromedially toward the tibia. All 3 cases of stress injuries occurred without any acute trauma but during playing/training and presented with an insidious onset of pain. From a biomechanical perspective, Ho et al 8 have demonstrated in a porcine femur model that there is a significant reduction in peak torque bone strength under torsional loading when there is a 4-mm bicortical drill hole defect. By occluding this defect with a screw or plaster of paris, bone strength was improved in their specimens. Johnson and Fallat, 14 in their cadaveric study, reported that the mean load to failure of intact fibulas was 360.86 N, while the fibulas with one 3.5-mm drill hole had a significantly lower mean load to failure of 215.20 N in bending forces. In the present series, we suggest that the persistent stress riser under the eccentrically placed fibula suture button combined with the failure of bone healing in the No. 5 FiberWire track means that nonoperative management is unlikely to succeed, especially in elite athletes because of the nature of their training and high-demand sporting activities. Consequently, given that nonoperative management resulted in an unacceptable delay to the union, we advocate early surgical intervention. Despite that, the need for routine removal of the TightRope devices to prevent the occurrence of this complication is not necessary, as it appears to be limited to elite athletes only in small numbers based on our observations—as opposed to recreational athletes and the general population.
Augmentation of the TightRope construct with a fibula plate (Dual Syndesmosis TightRope implant and Syndesmosis TightRope XP Buttress Plate implant) has been developed to improve the distribution of the forces across the fibula and potentially protect the fibula from fracture when using 2 TightRopes. In a cadaveric study, Tsai et al 20 reported no significant difference in the maximum torque leading to fracture of the fibula between 2 TightRope constructs when compared with 1 TightRope and a plate construct. Nonetheless, they found greater rotation was required to fracture the fibula after fixation with the 1 TightRope and plate construct. They concluded that adding the plate may reduce stress risers and decrease the risk of failure, as demonstrated by the higher rotation to failure in the plate construct. A literature review has failed to demonstrate any reported cases of this complication with or without the plate augmentation; however, we suggest that if eccentric misplacement of the fibula suture button is recognized at the time of the original surgery, it may be appropriate to use a fibula plate to reduce the risk of a subsequent stress fracture.
Limitations
This case series was limited by the retrospective nature of the data collection, the lack of patient-reported outcomes, and the small number of cases. There was also a limited follow-up duration after the surgical management of the fibula fractures. Additionally, there is a potential criticism that these athletes may have residual syndesmosis instability that resulted in subsequent ankle injuries. However, the ability of these athletes to return to sports at their preinjury level without any complaints would suggest otherwise. We were also unable to provide a prevalence of this complication, as we do not have an exact denominator of how many isolated syndesmosis injuries were treated with this technique during this study period. Despite that, to our knowledge, this case series is the first to report this potential complication using the TightRope in elite athletes and offers recommendations on management options and preventative tips.
Conclusion
Nonoperative management of fractures adjacent to the fibula suture button of a knotless TightRope may lead to a delayed union. Therefore, early surgical intervention should be considered in elite athletes, whose return-to-sports time is critical. Care must be taken to ensure the fibula suture button hole is placed centrally in the fibula or even just posterior to the center point when directing the guidewire anteromedially, as the eccentric placement of the fibula hole in the anterior third of the fibula may contribute to the development of a stress reaction or stress fracture. If misplacement is recognized during the index surgery, surgeons should consider using a fibula plate to distribute forces along the fibula.
Footnotes
Final revision submitted May 12, 2023; accepted May 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.C. has received consulting fees from Arthrex, Orthosolutions, and Stryker. J.C. has received education payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the National Health Service Health Research Authority.
References
- 1. Ballal MS, Pearce CJ, Calder JD. Management of sports injuries of the foot and ankle: an update. Bone Joint J. 2016;98-B(7):874-883. [DOI] [PubMed] [Google Scholar]
- 2. Brooks JH, Fuller CW, Kemp SP, Reddin DB. Epidemiology of injuries in English professional rugby union: part 1 match injuries. Br J Sports Med. 2005;39(10):757-766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Calder JD, Bamford R, Petrie A, McCollum GA. Stable versus unstable grade II high ankle sprains: a prospective study predicting the need for surgical stabilization and time to return to sports. Arthroscopy. 2016;32(4):634-642. [DOI] [PubMed] [Google Scholar]
- 4. Colcuc C, Blank M, Stein T, et al. Lower complication rate and faster return to sports in patients with acute syndesmotic rupture treated with a new knotless suture button device. Knee Surg Sports Traumatol Arthrosc. 2018;26(10):3156-3164. [DOI] [PubMed] [Google Scholar]
- 5. D’Hooghe P, Grassi A, Alkhelaifi K, et al. Return to play after surgery for isolated unstable syndesmotic ankle injuries (West Point grade IIB and III) in 110 male professional football players: a retrospective cohort study. Br J Sports Med. 2020;54(19):1168-1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Gerber JP, Williams GN, Scoville CR, Arciero RA, Taylor DC. Persistent disability associated with ankle sprains: a prospective examination of an athletic population. Foot Ankle Int. 1998;19(10):653-660. [DOI] [PubMed] [Google Scholar]
- 7. Harper MC. Delayed reduction and stabilization of the tibiofibular syndesmosis. Foot Ankle Int. 2001;22(1):15-18. [DOI] [PubMed] [Google Scholar]
- 8. Ho KW, Gilbody J, Jameson T, Miles AW. The effect of 4 mm bicortical drill hole defect on bone strength in a pig femur model. Arch Orthop Trauma Surg. 2010;130(6):797-802. [DOI] [PubMed] [Google Scholar]
- 9. Hohman DW, Affonso J, Marzo JM, Ritter CA. Pathologic tibia/fibula fracture through a suture button screw tract: case report. Am J Sports Med. 2011;39(3):645-648. [DOI] [PubMed] [Google Scholar]
- 10. Honeycutt MW, Riehl JT. Effect of a dynamic fixation construct on syndesmosis reduction: a cadaveric study. J Orthop Trauma. 2019;33(9):460-464. [DOI] [PubMed] [Google Scholar]
- 11. Hong CC, Lee WT, Tan KJ. Osteomyelitis after TightRope fixation of the ankle syndesmosis: a case report and review of the literature. J Foot Ankle Surg. 2015;54(1):130-134. [DOI] [PubMed] [Google Scholar]
- 12. Hunt KJ, Phisitkul P, Pirolo J, Amendola A. High ankle sprains and syndesmotic injuries in athletes. J Am Acad Orthop Surg. 2015;23(11):661-673. [DOI] [PubMed] [Google Scholar]
- 13. Jain N, Murray D, Kemp S, Calder J. Frequency and trends in foot and ankle injuries within an English Premier League Football Club using a new impact factor of injury to identify a focus for injury prevention. Foot Ankle Surg. 2014;20(4):237-240. [DOI] [PubMed] [Google Scholar]
- 14. Johnson BA, Fallat LM. The effect of screw holes on bone strength. J Foot Ankle Surg. 1997;36(6):446-451. [DOI] [PubMed] [Google Scholar]
- 15. Leucht P, Kim JB, Wazen R, et al. Effect of mechanical stimuli on skeletal regeneration around implants. Bone. 2007;40(4):919-930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Naqvi GA, Cunningham P, Lynch B, Galvin R, Awan N. Fixation of ankle syndesmotic injuries: comparison of tightrope fixation and syndesmotic screw fixation for accuracy of syndesmotic reduction. Am J Sports Med. 2012;40(12):2828-2835. [DOI] [PubMed] [Google Scholar]
- 17. Rammelt S, Zwipp H, Grass R. Injuries to the distal tibiofibular syndesmosis: an evidence-based approach to acute and chronic lesions. Foot Ankle Clin. 2008;13(4):611-633. [DOI] [PubMed] [Google Scholar]
- 18. Schepers T. Acute distal tibiofibular syndesmosis injury: a systematic review of suture-button versus syndesmotic screw repair. Int Orthop. 2012;36(6):1199-1206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Storey P, Gadd RJ, Blundell C, Davies MB. Complications of suture button ankle syndesmosis stabilization with modifications of surgical technique. Foot Ankle Int. 2012;33(9):717-721. [DOI] [PubMed] [Google Scholar]
- 20. Tsai J, Pivec R, Jauregui JJ, et al. Strength of syndesmosis fixation: two TightRope versus one TightRope with plate-and-screw construct. J Long Term Eff Med Implants. 2016;26(2):161-165. [DOI] [PubMed] [Google Scholar]
- 21. Zhang P, Liang Y, He J, Fang Y, Chen P, Wang J. A systematic review of suture-button versus syndesmotic screw in the treatment of distal tibiofibular syndesmosis injury. BMC Musculoskelet Disord. 2017;18(1):286. [DOI] [PMC free article] [PubMed] [Google Scholar]