

Abstract
Helicobacter pylori remains a major health problem worldwide, causing considerable morbidity and mortality due to peptic ulcer disease and gastric cancer. These guidelines constitute an update of the previous “Recommendations on the diagnosis and management of Helicobacter pylori infection” issued in 2014. They have been developed by a Task Force organized by the Governing Board of the Polish Society of Gastroenterology. They discuss, with particular emphasis on new scientific data covering papers published since 2014: the epidemiology, clinical presentation, diagnostic principles and criteria for the diagnosis, and recommendations for the treatment of H. pylori infection. The guidelines in particular determine which patients need to be tested and treated for infection. The Task Force also discussed recommended treatment algorithms. Accordingly, a combination of available evidence and consensus-based expert opinion were used to develop these best practice advice statements. It is worth noting that guidelines are not mandatory to implement but they offer advice for pragmatic, relevant and achievable diagnostic and treatment pathways based on established key treatment principles and using local knowledge and available resources to guide regional practice.
Keywords: Helicobacter pylori, H. pylori, eradication, gastritis, gastric cancer, atrophy, quatriple therapy
1. Methodology of recommendation
The following paper presents the latest recommendations and the diagnostic and therapeutic guidelines on Helicabacter pylori (H. pylori) infection by the Working Group of the Polish Society of Gastroenterology. The recommendations concern: current methods of diagnosis and treating H. pylori infection in people over 18 years of age.
They include the applicability of international guidelines and available epidemiological data and are adapted for the specifics of the Polish health care system. It should be emphasised that the Polish recommendations are not a faithful copy of the European guidelines. This is due to differences in antibiotic sensitivity and the regional incidence of gastric cancer. Therefore, according to experts, it is necessary to optimise and adapt the recommendations for the population they are dedicated for.
1.1. Scope and purpose of recommendations
1.1.1. Objectives
The aim of the guideline is to improve physicians’ knowledge of the prevalence and clinical significance of H. pylori infection, to identify diagnostic methods, and to present the appropriate management of infected people according to the current state of knowledge. We expect that the application of these recommendations will translate into an increased disease diagnosis with reduced diagnosis costs, as well as an impact on the appropriate treatment of patients, especially in cases of first-line treatment failure.
1.1.2. Health issues addressed in the recommendations
The recommendations discuss in detail the health problems related to the H. pylori infection:
Have the epidemiological data on H. pylori infection changed significantly in recent years?
How does H. pylori infection occur?
What are the clinical consequences of chronic H. pylori infection?
What are the clinical manifestations (symptoms) of H. pylori infection?
When and how to test patients for H. pylori infection?
Which drugs and for how long should be used for H. pylori eradication?
How to evaluate the effectiveness of the treatment provided?
How to manage the eradication failure?
1.1.3. Target population of patients to whom the recommendations apply
The recommendations address the management of male and female adult patients (over 18 years of age) with both symptomatic and asymptomatic H. pylori infection.
1.1.4. Target audience
The guidelines are developed for all physicians, especially specialists in gastroenterology, internal medicine and infectious diseases.
1.2. How recommendations are developed?
The source data was searched in electronic databases: PubMed, NCBI, Cochrane Library, ResearchGate, Google Scholar, as well as in guidelines published on the websites of international scientific societies (US, UK, European: AGA, ACG, USNGC, NICE, UEG).
Only original studies (optimally prospective, randomised, double-blind, controlled trials) and, in the absence of such studies: studies with a lower rank of evidence quality, up to observational and retrospective studies, excluding case series and case reports) and statistical reviews and meta-analyses were used to create recommendations. Studies published in languages other than Polish and English were excluded. Recommendations were developed in accordance with the recommendations of the Health Technology Protection Agency, the AGREE II methodology and the GRADE recommendation evaluation system were used to evaluate and describe a recommendation. Patient management questions were developed according to the PICO protocol [1, 2].
Recommendations were allocated a strength of recommendation with an additional assessment of the evidence level (discussed in Tables I and II). The method of making the final decisions involved a Delphi voting system [3]. In addition, the acceptance of each statement was discussed by a panel of experts (agreement level, Table III).
Table I.
| Strenght of recommendation | |
|---|---|
| Strong | The benefits clearly outweigh the risks and burden, or vice versa. Usually in guidelines the recommendation formulated as: “we recommend”. |
| Weak | Benefits closely balanced with risks and burdens. Usually in guidelines the recommendation formulated as: “we suggest”. |
Table II.
| Evidence level (quality of evidence) | |
|---|---|
| High | One or more high-quality, well-conducted randomised controlled trials (RCTs) that provide consistent and directly usable results. This means that further research is very unlikely to affect the estimated effect. |
| Moderate | RCTs but with important limitations (i.e. biased assessment of treatment effect, high patient loss during follow-up, lack of blinding, unexplained heterogeneity), indirect evidence from similar (but not identical) study populations and studies with very small numbers of patients or observed events (endpoints). In addition, there is evidence from well-designed non-randomised controlled studies, well-designed analytical cohort studies or from case-control studies, and from multiple case series with or without intervention. This means that further research is likely to have an important impact on the estimated effect and could alter it. |
| Low | Observational studies, typically of low quality due to error risk. This means that further research will almost certainly have a significant impact on the estimated effect and will most likely alter it. |
| Very low | The evidence is contradictory, of poor quality or lacking in results, so that the benefits and risks ratio cannot be determined. This means that any estimated effect is very uncertain as evidence or is unavailable or does not allow to formulate any conclusions. |
Table III.
Scale determining the agreement level (rating scale) for the recommendations used in the vote [1]
| Category | Agreement level |
|---|---|
| A | Full acceptance |
| B | Acceptance with some objection |
| C | Acceptance with serious objection |
| D | Rejection with some objection |
| E | Full rejection |
If at least 80% of voters had chosen categories A or B, then the agreement level is high, otherwise it is low.
Each recommendation is discussed on the basis of the scientific evidence used in its development (the link between recommendations and scientific data).
1.2.1. Interpretation of recommendations
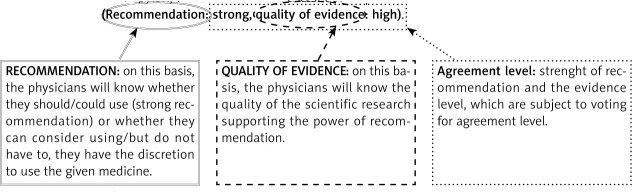
A graphical interpretation of an example recommendation is shown below.
Each recommendation is accompanied by three information:
– the strenght of the recommendation is defined in the document as strong or weak and based on GRADE,
– quality of the evidence is defined in the document as high, moderate, weak, very weak and is based on GRADE,
– agreement level (rating scale).
Example:
4.1. Recommendation 1
For the eradication of H. pylori, we recommend the use of quadruple therapy with bismuth for 14 days in the first line of treatment. (Recommendation: strong, quality of evidence: high).
4.1.1. Voting: Agreement level ← the result of the experts’ work on the given recommendation)
A – %; B – %; C – %; D – %; E – % ← percentage of experts voting in favour of a recommendation (according to Table III).
Agreement level: ← if > 80% of experts have voted for A and B then the agreement level is high, otherwise it is low.
2. Introduction
Helicobacter pylori is a Gram-negative micro-aerophilic bacillus. To live, it requires oxygen in concentrations less than atmospheric (around 20%). In a hostile environment (low pH), it transforms into a cocci form (not a spore form but a coccoid form, in which case the bacterium does not multiply and is more difficult to damage). It primarily resides on the surface of the gastric mucosa, under the layer of mucus covering the cells, where the conditions are more favourable. It gets underneath this layer using the flagellate-covered cilia. Mucinase, produced by the bacterium, liquefies mucus, facilitating its movement. Helicobacter pylori also produces urease, an enzyme that breaks down urea to carbon dioxide and ammonia, causing the neutralisation of hydrochloric acid and an increase in pH in the immediate vicinity of the bacterium, allowing it to survive in an acidic environment. Due to outer proteins and lipopolysaccharides, it stably adheres to host cells and, thanks to its complex antioxidant system, it defends itself against attack by neutralising the oxygen free radicals produced by neutrophils. If damage to the bacterial DNA occurs, H. pylori is equipped with an efficient repair system. Vacuolising toxins and cytotoxic proteins are responsible for the actual damage to host cells. The first one (VacA) has the ability to form huge intracellular vacuoles, leading to cell damage. The expression of VacA, with varying degrees of activity, is shown by 40–60% of H. pylori strains. The activity of different alleles of VacA toxin influences its cytotoxicity, leading directly and indirectly to the initiation of apoptosis in host cells. By inducing the production of inflammatory mediators, the CagA cytotoxic protein damages the cytoskeleton, increasing further the ability of bacteria to adhere to damaged cells. The most important role of CagA is to interfere with the complex processes of cell growth and differentiation and disrupt intracellular signalling leading to cell transformation, making CagA one of the best known oncogenes of bacterial origin. To date, two subtypes of the protein have been described, 1a and 2 a. The former, East Asian, is considered more virulent, giving a stronger inflammatory response and associated with greater likelihood of malignant transformation. In Europe, including Poland, the less virulent, western subtype is predominant [4–8].
2.1. Epidemiology
The main reservoir of bacteria is human. Helicobacter pylori infection is common. It is estimated that 50% of the world’s general population is infected, although of course geographical and demographic differences are observed. A recent systematic review and meta-analysis published in Gastroenterology by Hooi et al. proved that in Europe, the prevalence of infection ranges from less than 40% of the population in Scandinavian countries and Germany, to more than 70% in Portugal. In Poland, the prevalence of infection is estimated to be between 50% and 69% with age variation [9]. Recent data published by Łaszewicz et al. in 2002–2003, showed that approximately 84% of adults and 32% of children are infected, while Szaflarska-Popławska and Soroczyńska-Wrzyszcz using a breath test found infection in 23.6% of young people aged 13–17 years (data for 2008–2015) [10, 11].
Infection usually occurs in childhood or adolescence via oral route. It is believed that the infection is usually lifelong. Although the dominant belief is that transmission is most often from mother to child (or within the family), there are no studies of sufficient quality to justify, for example, family eradication or prevention of infection [12].
2.2. Spectrum of symptoms and complications of infection
The different virulence of different proteins and toxins from different strains translates into a different clinical picture of infection. An overwhelming proportion (up to 80%) of infected people have no symptoms or, importantly, no disease complications. Also, there are no pathognomonic signs of infection. The most common diseases that may or may not be associated with H. pylori infection include:
a) Dyspepsia
Dyspepsia is defined as epigastric pain, usually postprandial or meal-related, early satiety, postprandial fullness. It affects up to 20% of the general population. There are many reasons for the phenomenon, and in countries with H. pylori infection rates > 15% of the population, the infection is thought to be such a common cause of symptoms (20–50% of dyspepsia patients) that every patient requires its exclusion [13].
b) Gastritis
Generally, H. pylori always causes an acute phase of inflammation by damaging the gastric mucosa. However, most often (in about 80% of cases) there are no clear, acute or chronic disease symptoms. It is known that most often the infection progresses to the chronic phase, which is latent in up to 90% of patients. Only 10–20% of people are symptomatic, due to inflammation in the pre-pyloric stomach area, gastrin overproduction and the development of ulcers area (due to its separation from the parietal cells). Approximately 5% of people develop extensive atrophic inflammation. It is a particular form of inflammation that significantly increases the risk of gastric cancer development based on cell atrophy and the occurrence of intestinal metaplasia followed by dysplasia (Correa’s cascade) [14, 15].
c) Peptic ulcer disease
An ulcer, i.e. a full-thickness defect in the mucosa, exceeding the muscle layer and extending to the submucosa or even deeper, is the consequence of an imbalance between irritants (hydrochloric acid, pepsin) and protective factors (a properly vascularized and mucus-covered mucosa), the production and function of which is affected by infection. The H. pylori infection is responsible for about 75–90% of duodenal ulcers and about 70% of gastric ulcers. It results in hypergastrinemia, excessive production of hydrochloric acid, damage to the mucus layer and mucosa (development of a local inflammatory response) and, finally, weakened defence processes. All this leads to the development of ulcers [5, 14].
d) Stomach cancer
Thanks to numerous epidemiological, molecular and animal studies and a wealth of data on the reduction of gastric cancer incidence in populations undergoing eradication of H. pylori infection, it is now recognised as a major aetiological factor of gastric cancer. It is estimated that up to 90% of cases may be caused by infection, which is considered both intestinal and diffused types [16, 17].
e) Gastric MALT lymphoma
Long-term immune system stimulation due to infection is capable of leading to uncontrolled monoclonal proliferation and the development of gastric MALT lymphoma. Approximately 90% of these arise from infection (particularly with high VacA virulence strains) and, interestingly, the first line of therapy for malignant tumours is the treatment of H. pylori infection.
f) Other diseases
Helicobacter pylori infection is associated with many other diseases of different organs and systems. Although many of these relationships still remain hypothetical, a correlation between infection and spontaneous thrombocytopenic purpura, iron and/or vitamin B12 deficiency anaemia, as well as between certain cancers (e.g. hepatocellular carcinoma), myocardial infarction or asthma has been proven to date. In 2020, the first review of meta-analyses and systematic reviews on the association between H. pylori infection and various diseases was published in the British Medical Journal. 88 publications were meticulously analysed (out of a baseline of more than 3,000 considered), discussing both the harmful and protective role of infection. Those areas where controversy still exists (e.g. cardiology) were analysed [17]. Most such associations have been proven in Asian studies, but there is also good evidence of the association between the infection and diseases of various systems (such as cancer, diabetes, cirrhosis, Parkinson’s disease, myocardial infarction, COPD or glaucoma), in Europe and in the Western countries.
3. Indications for Helicobacter pylori testing
3.1. Statement 1
| Gastritis caused by Helicobacter pylori is infectious disease regardless of the symptoms and complications. |
| Quality of evidence: high. Recommendation: not applicable. |
3.1.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.1.2. Discussion
Helicobacter pylori cannot be considered as a commensal microbiota, as its presence in the stomach induces inflammatory response of varying severity irrespective of the presence of ailments [18].
Indeed, the spectrum of symptoms and disease consequences varies between patients and ranges from asymptomatic forms to peptic ulcer disease and gastric cancer, most often untreatable at the time of diagnosis. Inflammation is caused by multiple mechanisms, induced both in gastric epithelial cells, which are the site of first contact with the pathogen, and in circulating immune cells recruited to the site of infection. Helicobacter pylori stimulates the production of pro-inflammatory cytokines such as: IL-1, IL-6, IL-8, TNF and RANTES [19]. On microscopic examination, chronic active inflammation with infiltration of neutrophils and mononuclear cells is observed. It has been shown that the cure of H. pylori infection leads to withdrawal of inflammatory lesions and restoration of normal mucosa, provided irreversible changes have not occurred. It is thought that some forms of mucosal atrophy may even withdraw [20].
3.2. Statement 2
| As all people infected with H. pylori should be offered a treatment, it is crucial to establish clear indications for testing for infections for which there is proven benefit from treatment. |
| Quality of evidence: high. Recommendation: not applicable. |
3.2.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.2.2. Discussion
In real world, it is most important to distinguish between indications for the diagnosis of infection and indications for its eradication. Until recently, tests were only performed for clinical indications (disease symptoms) and treatment was recommended for all those found to be infected. Several guidelines with the status of international recommendations have emerged between 2014 and 2022, including a report by the International Agency for Research on Cancer (IARC), the WHO opinion, the so-called Kyoto consensus or the Maastricht recommendations (fifth and sixth editions), which include world-known experts in the field among their authors, in which the approach to mass testing and eradication is changing [16, 21, 22]. While in countries with a high risk of gastric cancer, it should be recommended, for countries with an average or low incidence (including Poland), unequivocal evidence for the validity of such a procedure is lacking. Helicobacter pylori infection is necessary but not sufficient for the development of gastric cancer. In addition, the infection has a protective effect in isolated but civilisation-relevant diseases such as childhood obesity and asthma. In the US, there are even stricter recommendations, issued in 2017, where testing is not offered to patients with vitamin B12 deficiency, with a family history of gastric cancer or with hyperplastic polyps [23].
At stake in mass eradication, as mentioned, is a reduction in the incidence of gastric cancer (46–51% reduction in Asian populations). In 2020, the results of two studies prospectively evaluating the effectiveness of eradication were published. A study published in Gut involving more than 85% of the population of the Matsu Islands (China), in which the incidence of post-interventional infection decreased from 64.2% to 15% between 2004 and 2018, showed that the incidence of gastric cancer decreased by 53%. In a prospective randomised, placebo-controlled study evaluating the effectiveness of H. pylori eradication in first-degree relatives of people with gastric cancer, from South Korea (New England Journal of Medicine), eradication was shown to significantly reduce the risk of cancer (by 45%) [24, 25]. The evidence for reductions in incidence and mortality does not only extend to high-risk countries. In an US retrospective cohort study, the effectiveness of eradication in the prevention of gastric cancer was proven, but again, the greatest benefit was for non-white races. A Markov model developed in this country to assess the cost and effectiveness of gastric cancer screening confirmed these observations. Screening and surveillance for abnormalities was only cost-effective in black, Latin American and Asian individuals.
It should therefore be considered that, under Polish conditions, patients with symptoms or diseases with a proven link to infection should be tested (Table IV) and, most likely, all patients undergoing gastroscopy (most indications include diseases that may be related, even indirectly, to infection, although further studies are needed to support this hypothesis). If infection due to other causes is detected, the decision to eradicate should be taken individually after discussion with the patient.
Table IV.
Indications for testing and eradication of H. pylori – a summary
| Undiagnosed dyspepsia (“test and treat” strategy) |
| Dyspepsia – differential diagnosis |
| Atrophic gastritis |
| Gastric and/or duodenal peptic ulcer disease (also in medical history) |
| After gastrectomy due to cancer |
| First-degree relatives of gastric cancer patients |
| Gastric lymphoma |
| Planned long-term treatment with non-steroidal anti-inflammatory drugs including aspirin |
| Long-term PPI treatment* |
| Idiopathic thrombocytopenic purpura (ITP) |
| Unexplained iron deficiency anaemia |
| Deficiency of vitamin B12 |
| Differential diagnosis of other diseases (coeliac disease, Crohn’s) |
| Patient’s request* |
| Post-treatment infection follow-up |
No proven beneficial population effect in this indication. PPI – proton pump inhibitors.
At this stage, there is insufficient evidence for testing the general population in Poland and Europe [24–28].
3.3. Statement 3
| Given the most common indications for gastroscopy and the prevalence and universality of risk factors and complications of H. pylori infection, a rapid urease test is suggested for every patient undergoing gastroscopy. In patients treated with PPIs, the decision to perform the test should be individualised. |
| Quality of evidence: very low. Recommendation: weak. |
3.3.1. Voting
A – 40%; B – 60%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.3.2. Discussion
The H. pylori infection is a potentially curable cause of dyspepsia, peptic ulcer disease or gastric cancer. Indications for endoscopic diagnosis of infection vary according to the risk of malignancy and previous therapies and include older age (> 50 yrs), male sex, the presence of gastric cancer in first-degree relatives, a pepsinogen I/III ratio < 3 or smoking [22, 29]. This means that the majority of subjects with a suspected infection have an indication for gastroscopy. On the other hand, the main indications for gastroscopy are epigastric pain, dyspepsia, nausea and vomiting, anaemia and overt gastrointestinal bleeding, followed by reflux disease and cirrhosis surveillance. Thus, in more than 80% of indications for gastroscopy, there are, by definition, indications for a test for H. pylori. Despite the lack of formal studies, many recommendations consider gastroscopy to be generally associated with testing for infection and, according to European experts, the procedure is incomplete without a test [30]. Due to the possibility of false-negative results during treatment with proton pump inhibitors (PPIs), the indications for testing during therapy should be determined on an individual basis.
3.4. Statement 4
| In the diagnosis of undiagnosed or functional dyspepsia, first H. pylori infection should be excluded. |
| Quality of evidence: high. Recommendation: strong. |
3.4.1. Voting
A – 60%; B – 30%; C – 10%; D – 0%; E – 0%.
Agreement level: high.
3.4.2. Discussion
A ‘test and treat’ strategy based on non-invasive diagnostic testing for H. pylori infection, and treatment in the event of a positive result, in countries with high rates of H. pylori infection is considered a safe and cost-effective strategy for managing patients with symptoms of undiagnosed dyspepsia [31, 32]. A detailed discussion on the management of dyspepsia is the subject of separate recommendations and is beyond the scope of this publication. However, it should be emphasised that more than a dozen large, good-quality prospective randomised controlled studies have confirmed the validity of such a management. A 2019 network meta-analysis by Eusebi et al. which included 15 randomised trials (6,162 patients), showed that the strategy in question was the best among all competing management strategies. It significantly reduces the need for gastroscopy (23% of patients in this group required endoscopy) [33]. In simulation modelling of different strategies, Beresniak et al. proved that the ‘test and treat’ strategy is twice as cheap as an endoscopy-based strategy and 12.5% cheaper than a symptomatic treatment strategy (treat symptoms first, test for H. pylori later) [34].
3.5. Statement 5
| In patients under 45 years of age with symptoms of dyspepsia, without alarming symptoms, a non-invasive diagnosis for H. pylori infection is recommended. |
| Quality of evidence: moderate. Recommendation: weak. |
3.5.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.6. Statement 6
| Upper gastrointestinal endoscopy with simultaneous testing for H. pylori infection is indicated in patients with alarming symptoms and in patients over 45 years of age with dyspeptic symptoms, as well as in cases where the ‘test and treat’ strategy has failed. |
| Quality of evidence: moderate. Recommendation: weak. |
3.6.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.6.2. Discussion
Discussion of statements 5 and 6.
In clinical practice for the diagnosis of dyspepsia, we can use non-invasive tests for the detection of H. pylori infection with proven and acceptable effectiveness. The need for the test alone is not an indication for gastroscopy. Depending on the geographical region, the prevalence of gastric cancer in the population and the epidemiology of other risk factors for organic upper gastrointestinal disease, the age at which endoscopic examination is recommended for patients with dyspepsia symptoms ranges from 45 to 60 years [22, 31–34].
Poland is one of the countries with a low incidence of gastric cancer. According to the 2019 National Cancer Registry (NCR), 5,100 new cases were detected in Poland (standardised incidence rate – 22/100,000), and year-on-year the incidence is decreasing [35]. Still, gastric cancer is diagnosed at advanced stages, when treatment options are limited. Recent Polish data from a nationwide study by Januszewicz et al. showed that up to 6% of gastric cancers are missed (undiagnosed) during the first diagnostic gastroscopy [36]. Although the mean age at diagnosis of cancer in this study was about 68 years, and the incidence is known to increase with age, KRN data indicate that the first noticeable increase in gastric cancer incidence is observed from 45 years of age onwards both in males and females [35]. These data are consistent with recent large population-based studies published in 2022 in Nature and Lancet analysing trends in gastric cancer incidence and mortality from the ‘90s to estimated figures in 2040. An increase in incidence is seen from 45 years of age onwards, particularly in females (the variation in age groups is not as clear) [37, 38]. Therefore, given the lack of population-based screening in Poland, the prevalence of H. pylori infection and the high prevalence of other risk factors for gastric cancer in patients with upper gastrointestinal symptoms, despite the lack of scientific studies, we maintain our previous recommendation to perform gastroscopy after 45 years of age [39, 40].
3.7. Statement 7
| Suspicion and/or diagnosis of atrophic gastritis is an indication for diagnosis of H. pylori infection. |
| Quality of evidence: high. Recommendation: strong. |
3.7.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.7.2. Discussion
Helicobacter pylori infection is a predisposing factor for the development of chronic atrophic gastritis. This, in turn, is a recognised risk factor for gastric cancer [7, 14]. It has been shown that eradication of the infection is most effective in terms of cancer prevention if carried out before chronic atrophic inflammation develops [41]. Even when atrophy occurs, eradication can reverse the process and, at least to some extent, also stop the progression from intestinal metaplasia into neoplastic lesions [42]. For a detailed discussion of the relationship between H. pylori and cancers arising from atrophic gastritis, see ‘Prevention and public health’.
3.8. Statement 8
| The indication for the diagnosis of H. pylori infection is gastric and/or duodenal ulcer disease – active, inactive and complicated. |
| Quality of evidence: high. Recommendation: strong. |
3.8.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.8.2. Discussion
The first references to a potentially pathogenic bacterium detected in mammalian stomachs appeared as early as the end of the 19th century in Germany, Italy and Poland (Walery Jaworowski, 1899) [43]. However, it was not until the 1980s that B.J Marshall and J.R. Warren proved the link between Helicobacter infection and gastritis symptoms, for which they were awarded the Nobel Prize in Medicine in 2005, it became clear that the aetiology of peptic ulcer disease is overwhelmingly infectious and contagious [44]. The research from the late second decade of the 21st century confirms the epidemiology of gastric and duodenal ulcer disease. It is estimated that around 70–80% of gastric ulcers and up to 90% of duodenal ulcers are caused by infection. Eradication of H. pylori reduces the risk of their development and, if they do occur, shortens healing time and reduces the risk of recurrence [45, 46].
3.9. Statement 9
| In patients diagnosed with gastric cancer or lymphoma, after gastrectomy for cancer and among first-degree relatives of gastric cancer patients, a diagnosis for H. pylori should be performed. |
| Quality of evidence: high. Recommendation: strong. |
3.9.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.9.2. Discussion
Helicobacter pylori is a recognised risk factor for gastric cancer and lymphoma. Detailed relationships between infection and carcinogenesis are presented in the discussion of steatment 2 and in the chapters ‘Introduction’, ‘Prevention’ and ‘Public health’. In this discussion, it is worth citing the results of three good-quality studies published in the New England Journal of Medicine, Gut and Gastroenterology. The first study, by Choi et al. 2020, looked at first-degree relatives of gastric cancer patients [25]. In this single-centre, double-blind, placebo-controlled study, H. pylori-infected relatives were subjected to eradication or followed up (after placebo administration). After a mean follow-up of 9.2 years, eradication was shown to more than double (HR = 0.45, p = 0.03) the risk of gastric cancer. Furthermore, half of the cancer patients were found to have a chronic infection. In a study, Chiang et al. assessed the impact of mass eradication on gastric cancer incidence and mortality [24]. Eradication began throughout the study area in 2004 and continued until 2018. During this time, six rounds of eradication took place. Again, this study showed a reduction of more than half (53% reduction, p < 0.001) in cancer incidence compared to pre-eradication data. The mortality rates have decreased by 25%. The most recent study, Yan et al. 2022, was an update after more than 26 years of a study evaluating the effect of eradication on gastric cancer prevention [47]. Patients were originally subjected to eradication in 1994 and their fate was now analysed after several decades of regular follow-up and endoscopic surveillance. The eradication group had a 43% lower risk of cancer, and when those without pre-cancerous lesions on index gastroscopy were assessed, the risk was lower by 63%. These findings are consistent with previous research.
3.10. Statement 10
| Chronic use of non-steroidal anti-inflammatory drugs (NSAIDs) including aspirin and other antiplatelet drugs with coexisting H. pylori infection promotes the development of gastric ulcers. Patients starting therapy with these drugs, or undergoing treatment, should have a diagnosis for H. pylori performed. |
| Quality of evidence: high. Recommendation: strong. |
3.10.1. Voting
A – 80%; B – 10%; C – 10%; D – 0%; E – 0%.
Agreement level: high.
3.10.2. Discussion
Non-steroidal anti-inflammatory drugs (NSAIDs) including aspirin (ASA) still are an independent risk factors for peptic ulcer disease and its complications [48]. Some studies have also shown that patients with H. pylori infection using NSAIDs have a higher risk of developing the disease than uninfected patients, and the risk of ulcer bleeding is even several times higher in these patients [49]. The greatest benefit of eradication was shown in the group of patients prior to starting long-term NSAIDs treatment, whereas in those already treated, the risk of developing peptic ulcer disease was comparable to that of patients not subjected to eradication [50]. Nevertheless, in recent years, eradication has also been shown to reduce the risk of ulcer recurrence in NSAIDs-treated patients [51]. Therefore, eradication is indicated in patients with a history of gastric and duodenal ulcers and using NSAIDs. In 2022, the results of the HEAT study, which evaluated the effect of H. pylori eradication in the primary prevention of upper gastrointestinal ulcer bleeding, were published in Lancet [52]. This was a prospective, randomised, placebo-controlled study in patients over 60 years of age. Eradication has been shown to reduce the risk of bleeding by 2.5 times in the first 2.5 years post eradication, and then this effect disappears. This is the first observation of its kind, shedding completely new light on the seemingly familiar and certain issue of reducing the risk of ulcer complications through H. pylori eradication. This may partly explain the observations of clinicians who encounter a high number of complications in daily practice, although of course the findings need to be confirmed.
Antiplatelets other than aspirin are unlikely to increase the risk of ulcer bleeding in patients without H. pylori infection, whereas the risk of ulcer bleeding in patients with H. pylori infection was significantly increased in patients on combination therapy: ASA + NSAID (OR = 5.85). Thus, prior to the initiation of anticoagulant and/or antiplatelet treatment, as a general rule the diagnosis for H. pylori and prior eradication should always be considered.
It should also be mentioned that there is growing evidence of adverse effects of serotonin reuptake inhibitors on the gastrointestinal mucosa manifested by peptic ulcer disease and bleeding, particularly in patients already taking NSAIDs. In 2022, a meta-analysis on this question was published in Nature and proved that the risk of bleeding was 75% higher in the group using drugs from both classes concomitantly [53].
3.11. Statement 11
| Helicobacter pylori infection plays an important role in the etiopathogenesis of: iron deficiency anaemia, vitamin B12 deficiency anaemia and idiopathic thrombocytopenic purpura. During diagnosis for these diseases, tests should be carried out to exclude H. pylori infection. |
| Quality of evidence: moderate. Recommendation: strong. |
3.11.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.11.2. Discussion
In 2020 The American Gastroenterology Association (AGA) has published recommendations for the management of iron deficiency anaemia, in which, based on the available scientific evidence, it recommends the early H. pylori eradication as a potential reason [54]. Meanwhile, the UK guidance (BSG) issued in 2021 mentions this possibility, but makes it clear that the data are limited and/or contradictory [55]. However, it is worth noting that we have results from studies showing that iron supplementation in patients with iron deficiency anaemia and H. pylori infection is effective, while combination therapy (iron supplementation and eradication) is statistically significantly better.
We do not have good quality studies linking eradication to the resolution of vitamin B12 deficiency anaemia. However, given the potential mechanism of its formation (atrophy due to infection, resulting in impaired absorption), it is worth considering eradication in this group of patients.
In adults with idiopathic thrombocytopenic purpura, H. pylori eradication gives a sustained improvement by increasing platelet counts, as shown in a systematic review of 25 studies published in Blood [56]. Also, haematology recommendations recommend testing and, if infection is confirmed, treatment of H. pylori infection as part of the management of thrombocytopenic purpura [57].
3.12. Statement 12
| When taking duodenal biopsy samples as part of the diagnosis of coeliac disease or Crohn’s disease, we suggest taking biopsy samples for concurrent H. pylori infection, as this infection may interfere with the picture of other diseases. |
| Quality of evidence: low. Recommendation: weak. |
3.12.1. Voting
A – 40%; B – 50%; C – 0%; D – 0%; E – 10%.
Agreement level: high.
3.12.2. Discussion
Helicobacter pylori infection causes not only macroscopic but also microscopic duodenitis. If biopsy samples need to be taken, in the differential diagnosis of diseases with an inflammatory infiltrate (visceral disease, Crohn’s disease, etc.), sections should be taken for urease testing concomitantly with taking sections for histopathological examination [58].
3.13. Statement 13
| There is insufficient evidence of a correlation between the occurrence of hyperplastic polyps or lymphocytic inflammation and H. pylori infection. |
| Quality of evidence: very low. Recommendation: weak. |
3.13.1. Voting
A – 70%; B – 30%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.13.2. Discussion
Several retrospective observational studies have suggested a possible relationship between the development of hyperplastic polyps and H. pylori infection. However, to date there is insufficient evidence to support this relationship, and recent work even suggests that the incidence of hyperplastic polyps is increasing, even though the incidence of H. pylori infection is decreasing [59]. There is even less data linking lymphocytic gastritis to infection, and in 2014 Nielsen et al. published the results of a study in which this relationship was not confirmed [60].
3.14. Statement 14
| After completion of treatment for H. pylori infection, it is advisable to assess the treatment effectiveness. |
| Quality of evidence: low. Recommendation: weak. |
3.14.1. Voting
A – 70%; B – 30%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.14.2. Discussion
For a detailed discussion of this question, see statement 24. This statement was kept for consistency in the recommendation and discussion of indications for testing for H. pylori infection. Due to the prevalence of the infection and the potential for increasing bacterial resistance to the eradication regimens used, it is advisable to monitor the treatment effectiveness. Patients who have not been cured have an increasing risk of complications. The common availability of cheap and effective diagnostic tests makes it easy to monitor the therapeutic effect. To date, there is no good scientific evidence of the cost-effectiveness of such management (with the exception of bleeding ulcers, which used to be one of the few indications for cure assessment). The need to maintain the optimal eradication regimen in a specific population also supports the assessment of treatment effectiveness, which would not be possible without systematic confirmation of its effectiveness.
3.15. Statement 15
| The mass introduction of screening and subsequent treatment of all infected individuals is currently not recommended, as it leads to increasing antibiotic resistance of H. pylori and other bacteria. The ideal prevention against complications associated with H. pylori infection would be the introduction of a vaccine. |
| Quality of evidence: moderate. Recommendation: weak. |
3.15.1. Voting
A – 80%; B – 20%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
3.15.2. Discussion
As mentioned before, no benefit for mass screening and eradication has been demonstrated in countries with a low risk of gastric cancer. More information can be found in the ‘Introduction’ section and in the ‘Prevention and Public Health’ chapter. However, it should be remembered that Poland is one of the countries with a low and decreasing risk of gastric cancer. No epidemiological studies have yet been carried out to estimate the dependence of this trend on the introduction of universal testing and treatment of infection. In countries with a high risk of gastric cancer, the evidence for the effectiveness of eradication in preventing gastric cancer is growing, and it is strong enough that, in general, screening is taking effect. In mid-November 2022, the WHO International Agency for Research on Cancer (IARC) launched a new pan-European project to accelerate the reduction of gastric cancer in Europe through the eradication of H. pylori infection: EUROHELICAN). The project co-funded by the European Union and is intended to introduce population-based screening (‘test and treat’ strategy) to prevent the development of gastric cancer in Europe [61]. A multicentre study has also been initiated in European countries with regions at highest risk of gastric cancer, which is designed to evaluate the effect of H. pylori eradication on cancer mortality in people between 40 and 64 years of age (GISTAR study) [62]. The study is planned to include 30,000 participants and results can be expected after 15 years.
4. Diagnostic methods
4.1. Statement 16
| If there is no indication for gastroscopy, it is recommended to first of all perform a test to detect H. pylori antigens in faeces using laboratory immunochemical methods (ELISA, CLIA) with automatic measurement reading or a 13C-urea breath test (UBT). |
| Quality of evidence: high. Recommendation: strong. |
4.1.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
4.1.2. Discussion
Diagnosis of H. pylori infection is recommended only for planned treatment. It is not recommended to start eradication therapy without confirmation of current infection by suitably reliable methods [22, 23]. The available diagnostic methods can be classified as invasive and non-invasive.
For all gastroscopy-based invasive tests and non-invasive tests that confirm active H. pylori infection (faecal H. pylori antigens and breath test) proton pump inhibitors (PPIs) should be discontinued for 14 days prior to testing, and bismuth and antibiotics should be discontinued for 4 weeks prior to testing [22, 34, 39, 63]. Failure to follow these recommendations may reduce the sensitivity of the tests performed.
The choice of diagnostic method depends on the patient’s current clinical situation and the need for gastroscopy [22, 63, 64]. If there is no indication for gastroscopy then a test to detect H. pylori antigens in faeces or a breath test is the recommended exam [22]. Helicobacter pylori antigens in faeces are detected using immunochemical methods – immunoenzymatic and immunochemiluminescent test using monoclonal antibodies and automated analysers [64]. The so-called rapid tests, requiring no measurement device, based on immunochromatographic methods with monoclonal or polyclonal antibodies are also available – these are not recommended due to their variable diagnostic accuracy [64]. The detection of H. pylori antigen in faeces is indicative of ongoing infection. Faecal antigen testing can therefore be used to establish an initial diagnosis of H. pylori and to confirm eradication [64, 65]. Of the available tests, faecal antigen testing is most cost-effective in regions with low to moderate H. pylori prevalence [65]. Active H. pylori infection in the stomach is manifested by the presence of bacterial antigens in faeces. Many tests can detect H. pylori-specific antigens (e.g. catalase) in faeces, providing a convenient, non-invasive diagnostic tool [66, 67]. Newer tests using monoclonal antibodies perform better in comparative studies [68–70]. The sensitivity and specificity of the laboratory immunoassay using monoclonal antibodies (94% and 97%) are comparable to the urea breath test (UBT) [70–72]. In cases of active bleeding in peptic ulcer disease, the specificity of H. pylori faecal antigen testing may be reduced. However, the sensitivity of the immunoassay with monoclonal antibodies remains high in cases of recent bleeding due to peptic ulcer disease [73]. Faeces antigen testing using a polyclonal enzyme immunoassay is no longer used due to its low sensitivity. Rapid, in-office monoclonal immunochromatographic tests for faecal antigens have high specificity, but their use has been limited by low sensitivity (96 and 50%, respectively) [74].
The urea breath test is a highly researched and widely recommended non-invasive test as part of an ‘test and treat’ strategy [22]. This test is based on the hydrolysis of urea by H. pylori urease to NH3 and CO2. The patient ingests urea labelled with non-radioactive 13C (preferred) or radioactive 14C (rarely used; radiation dose is minimal [approximately 1 µCi], contraindicated in children and pregnant women) [64]. The resulting 13CO2 or 14CO2 is expelled through the lungs with the expired air. An increase in 13CO2 concentration after urea ingestion relative to baseline or a positive 14CO2 assay (undetectable under normal conditions) indicate urease activity in the stomach, indicating the presence of H. pylori). The 13C-UBT test has a high diagnostic value, as it has a sensitivity of 88–95% and a specificity of 95–100% [75, 76]. False-positive results are rare. False-negative results can be observed, among others, in patients taking PPIs, bismuth or antibiotics and in the situation of active bleeding from a peptic ulcer [22, 64]. To improve the diagnostic value of UBT, the use of citric acid in the test meal is suggested. Citric acid helps to slow gastric emptying and improves the distribution of gastric contents by increasing the contact time with H. pylori urease [22, 76]. Whether H2 blockers affect the sensitivity of UBT is controversial [77].
4.2. Statement 17
| The use of antibody-based tests (IgG, IgA) for the detection of H. pylori in serum, whole blood, urine and saliva in clinical settings is discouraged. Exceptions are patients on PPIs, preparations of bismuth or antibiotic therapy, in whom treatment cannot be interrupted and diagnosis requires exclusion of H. pylori infection. |
| Quality of evidence: high. Recommendation: strong. |
4.2.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
4.2.2. Discussion
The sensitivity and specificity of IgG antibody assays in detecting H. pylori infection is low (approximately 80%) [22, 39, 64]. With simultaneous IgG and IgA assays, the diagnostic value increases slightly. Serological tests require validation at the local level, as H. pylori strains are diverse and it is virtually impossible to achieve it in routine practice [22]. Guidelines recommend that serological tests should not be used in low-prevalence populations, as their low diagnostic value may result in inappropriate treatment in a significant number of patients [22, 39].
A positive result is not indicative of current infection, as the presence of antibodies is observed for many months after cure. For this reason, serological tests are not suitable for the assessment of effectiveness of eradication. Serum IgG against H. pylori assays can serve as a screening test in specific clinical situations: a) during treatment with PPIs and antibiotics, b) in patients with other factors reducing the sensitivity of the other tests, e.g. active or recent gastric ulcer bleeding, atrophic gastritis or cancer (if the patient has not received prior eradication treatment) [22, 64]. The determination of antibodies against H. pylori can be used for screening when other diagnostic methods are unavailable or upper gastrointestinal endoscopy cannot be performed [22, 39]. In the event of a positive serology test, infection should be confirmed using another method (faecal H. pylori antigens or urea breath test) before eradication treatment is introduced.
4.3. Statement 18
| Most H. pylori infections can be diagnosed using a histopathological examination with histochemical staining alone. In cases of chronic (active) gastritis in which H. pylori is not found by histochemical staining, an immunohistochemical study may additionally be performed. |
| Quality of evidence: moderate. Recommendation: strong. |
4.3.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
4.3.2. Discussion
Histological examination of gastric mucosal sections is a commonly used method with a high diagnostic value (sensitivity 95%, specificity 98%) [78]. The section is stained with haematoxylin and eosin and additionally with special stains (e.g. Giemsa or Warthin and Starry) [78]. Most H. pylori infections can be diagnosed using a histological examination with histochemical staining alone. In cases of chronic (active) gastritis in which H. pylori bacteria is not found by histochemical staining, an immunohistochemical study may additionally be performed. If the image of the examined section is normal, there is no need to deepen the diagnosis. Histological examination also makes it possible to assess lesions in the gastric mucosa. For the assessment of gastritis caused by H. pylori, at least 2 sections should be taken during gastroscopy from the pre-pyloric part of the stomach (from the greater and lesser curvature 3 cm proximal to the pyloric duct) and 2 sections from the middle part of the gastric body [22]. Consideration should also be given to taking additional sections from the angular notch to detect precancerous lesions. The sections should be put in separate containers. If gastric sections are taken correctly (according to the guidelines), it is not necessary to perform a urease test. The sensitivity of histological examination may be reduced in patients with bleeding ulcers and in patients using PPIs, due to migration of H. pylori into the proximal part of the gastric body [79] (Table V).
Table V.
Diagnostic methods used in the diagnosis of H. pylori infection
| Test name | Sensitivity | Specificity | Comments | |
|---|---|---|---|---|
| Invasive tests: | ||||
| Urease test (CLO – test) Recommended |
90% | 95% | Cheap and quick, simple. False-negative result e.g. due to bleeding, post PPIs and antibiotics. PPIs should be discontinued 14 days before the test, and antibiotics and bismuth should be discontinued for 4 weeks. | |
| Histological examination | 95% | 98% | An expensive and time-consuming study. Assesses mucosal lesions. 14 days before the test, do not administer PPIs. | |
| Microbiological examination (bacterial culture) | 40–70% | 100% | Assesses the sensitivity of H. pylori to antibiotics. An expensive and time-consuming study. Difficult culture conditions. 14 days before the test, discontinue PPIs. | |
| Non-invasive tests: | ||||
|
H. pylori antigens in faeces Recommended |
94% | 97% | Cheap, simple and readily available. Confirms current infection and assesses the effectiveness of eradication. 14 days before the test, do not administer PPIs, and discontinue antibiotics and bismuth for 4 weeks. | |
| Breath test (using 13C or 14C-urea) | 88–95% | 95–100% | Confirms current infection and assesses the effectiveness of eradication. Difficult access. 14 days before the test, do not administer PPIs, and discontinue antibiotics and bismuth for 4 weeks. | |
| Serology (IgG or IgG + IgA) | 85% | 79% | Cheap, fast and useful for screening. Unsuitable for confirmation of current infection and eradication. | |
5. Treatment
5.1. Statement 19
| A key role in H. pylori eradication is played by the doctor-patient agreement, informing the patient of the possible side effects of the drugs used and adapting the treatment to the patient’s financial capabilities. Information should be obtained from the patient about previous antibiotic exposures so that they are not taken into account when choosing H. pylori treatment. |
| Quality of evidence: very low. Recommendation: weak. |
5.1.1. Voting
A – 100%; B – 0%; C – 0%; D – %; E – 0%.
Agreement level: high.
5.1.2. Discussion
The consensus of experts is that optimal H. pylori eradication treatment should be effective from the first treatment attempt and have at least 90% success rate [22, 23, 80]. Consequences of ineffective eradication include clinical complications associated with persistent H. pylori infection, repeated exposures to antibiotics and gastric acid inhibitors, generation of antibiotic resistance among the bacteria, and increased direct and indirect healthcare costs. The most important factors responsible for treatment failure are bacterial resistance to antibiotics and non-compliance. Therefore, the doctor should carefully discuss the treatment regimen, the benefits of eradication and possible side effects with the patient before prescribing the therapy. The results of the European Registry on H. pylori management (Hp-EuReg) confirmed that patient’s compliance significantly increased the effectiveness of eradication (87%), compared with non-compliance (56%) [81]. The patient should be warned about the adverse effects of smoking on the treatment effectiveness [82]. Smoking increases gastric acid secretion, impairs mucus secretion and reduces submucosal blood flow in the stomach, thereby reducing the local penetration of antibiotics.
Current European guidelines suggest determining the sensitivity of H. pylori to antibiotics (culture, molecular testing) even before using first-line therapy [22]. If the antibiotic sensitivity profile of H. pylori is unknown (as in the vast majority of cases), a thorough history of the patient’s previous exposure to antibiotics should be taken before prescribing eradication treatment. This recommendation is particularly relevant for further attempts to use clarithromycin and levofloxacin, as resistance rates to clarithromycin have been shown to reach 15–67% and 19–30% to levofloxacin in these situations [83]. A survey for the eradication treatment prescribers showed that only 38% had collected information from patients regarding previously used antibiotics [84].
5.2. Statement 20
| Poland belongs to countries with a high rate of clarithromycin resistance (> 15%), therefore the recommended first-line treatment in Poland is quadruple therapy with bismuth (PPI, bismuth, tetracycline, nitroimidazole) or quadruple therapy without bismuth (PPI, amoxicillin, clarithromycin, nitroimidazole), given their high effectiveness and lower complexity compared to sequential or hybrid treatment. |
| Quality of evidence: moderate. Recommendation: strong. |
Table VI.
First-line treatment in H. pylori eradication
| Regime | Dosage | Treatment duration |
|---|---|---|
| Quadruple therapy with bismuth | • PPIa BID • Bismuth 120 mg QID • Metronidazole 500 mg TID or QID • Tetracycline 500 mg TID or QID |
10–14 days |
| Quadruple therapy without bismuth | • PPIa BID • Amoxicillin 1000 mg BID • Metronidazole 500 mg BID • Clarithromycin 500 mg BID |
14 days |
Standard proton pump inhibitor (PPI) doses: omeprazole 20 mg, esomeprazole 20 mg, rabeprazole 20 mg, lansoprazole 30 mg, pantoprazole 40 mg.
5.2.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
5.2.2. Discussion
The increasing resistance of H. pylori to antibiotics is the reason for constantly changing treatment regimes. The World Health Organization (WHO) has identified H. pylori as one of the 12 highest priority pathogens for the development of new, effective antibiotics [85]. In a meta-analysis of 50,000 patients from 45 countries, primary resistance to clarithromycin ranged from 10% to 34% and to metronidazole from 23% to 56% [83]. In a Polish study of paediatric and adult populations, H. pylori resistance to clarithromycin was 28% and to metronidazole 46%, with combined resistance to both antibiotics as high as 20% [86]. The analysis of the population of south-western Poland confirmed resistance to clarithromycin and metronidazole of 46% and 56% respectively [87]. The use of triple therapy with clarithromycin, in the case of bacterial resistance to this antibiotic, resulted in a very low cure rate of only 43% [88]. Therefore, classic triple therapy (PPI + clarithromycin + amoxicillin or metronidazole), should not be used in Poland currently.
Quadruple therapy with bismuth has high effectiveness and reduces the issue of clarithromycin resistance [89–91]. Resistance to metronidazole can be overcome by acting synergistically with bismuth and increasing its daily dose to 1.5–2 g [92]. An analysis of 21,533 patients from the Hp-EuReg registry showed that quadruple therapy with bismuth had over 90% effectiveness in the first-line eradication treatment [93]. The use of this treatment in regions with high clarithromycin resistance had no effect on the high percentage of successful eradication – 94.4% [91]. A multicentre, prospective study with 2,100 patients with H. pylori infection showed the effectiveness of quadruple therapy with bismuth in first-, second- and subsequent-lines to be 95%, 89% and 92%, respectively, based on the modified intention-to-treat (m-ITT) analysis [94]. Two bismuth-containing preparations are currently available in Poland: Pylera (a combination drug, one capsule contains 140 mg of bismuth tripotassium dicitrate, i.e. 40 mg of bismuth oxide, 125 mg of metronidazole and 125 mg of tetracycline hydrochloride), and Ulcamed, which contains bismuth only (one tablet contains 120 mg of bismuth oxide as bismuth tripotassium dicitrate).
In the absence of availability or intolerance of bismuth preparations, an alternative form of first-line treatment is bismuth-free quadruple therapy, with a high eradication success rate of more than 90% [93]. It is important to remember that if there is a high (> 15%) proportion of H. pylori strains resistant to both clarithromycin and metronidazole in a given area, the effectiveness of quadruple therapy without bismuth is significantly lower, i.e. 79% [95]. Despite initially encouraging results, sequential or hybrid treatments are currently not recommended for the treatment of H. pylori infection due to their complicated administration and lower effectiveness than bismuth-free quadruple therapy [22, 80, 95].
5.3. Statement 21
| The recommended duration of quadruple therapy with bismuth is 14 days. The recommended durations of bismuth-free quadruple therapy is 14 days. |
| Quality of evidence: very low. Recommendation: weak. |
5.3.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
5.3.2. Discussion
The results of a meta-analysis evaluating the effectiveness, safety and compliance rates showed ≥ 85% effectiveness of quadruple therapy with bismuth administered for 10–14 days, compared to a shorter treatment duration [96]. Given the high prevalence of metronidazole resistance in many countries, also in Poland, the recommended eradication period is 14 days [22, 80]. Alternatively, quadruple therapy with bismuth for 10 days can be used if its effectiveness has been confirmed in the given region [22]. A meta-analysis of 30 studies involving nearly 6,500 patients confirmed the high, 90% effectiveness of 10-day treatment using a combination bismuth preparation (Pylera) in an intention-to-treat (ITT) analysis, regardless of dose or type of PPI [89]. The results of the Hp-EuReg registry, reflecting the real-world data, showed the effectiveness of 10-day therapy in first-, second- and subsequent lines treatment to be 94%, 90% and 86%, respectively [94]. In a retrospective analysis in north-eastern Poland, the effectiveness of 10-day treatment using a combined bismuth preparation was 89.4% [97]. Currently, there are no studies directly comparing classic quadruple therapy with bismuth with a combination preparation for 10 or 14 days.
For bismuth-free quadruple therapy, the recommended treatment duration is 14 days [22]. A real-life study conducted in Italy found a statistically significant superiority for 14-day therapy over 10-day therapy (ITT 96.1% vs. 80%, p = 0.001) [98]. In an analysis of 4,164 patients from the Hp-EuReg registry treated empirically with bismuth-free quadruple therapy in the first-line setting, a 14-day eradication superiority was demonstrated over 10-day eradication (m-ITT 92.1% vs. 88.3%) [93].
Helicabacter pylori is most sensitive to antibiotics when the stomach pH remains between 6 and 8, as this is the optimal environment for bacterial replication. In addition to the bactericidal effect found in vitro, proton pump inhibitors, by increasing gastric pH, enhance the penetration of antibiotics into the mucosa and increase their stability and antimicrobial activity. The level of inhibition of gastric acid secretion by PPIs is strongly dependent on the patient’s ability to metabolise the drug, which is determined by the polymorphism of cytochrome 2C19 (CYP2C19). In individuals with the CYP2C19 genetic polymorphism who metabolise drugs rapidly (56–81% of the Caucasian population), the use of older-generation PPIs (omeprazole, lansoprazole), which are mainly utilised by this cytochrome, is associated with a higher rate of eradication failure [99]. A meta-analysis evaluating the effect of PPIs on the effectiveness of 3-drug therapy with clarithromycin showed that the use of high versus standard doses of PPIs, improved eradication rates by 8% (82% vs. 74%, RR = 1.09, 95% CI: 1.01–1.17) [100]. This effect was particularly obvious when esomeprazole 40 mg was compared to omeprazole (20 mg) or pantoprazole (40 mg) – an 11% improvement in eradication effectiveness. Quadruple therapy with bismuth showed no difference in treatment effectiveness between low, standard and high doses of PPIs [16]. In contrast, the superiority of high over low doses of PPIs was found for quadruple therapy without bismuth [93].
Vonoprazan is a drug that inhibits the ATP-H+/K+ pump in gastric lining cells in a competitive, potassium-dependent manner. Compared to PPIs, the effect of vonoprazan is more rapid, lasts longer, produces a stronger inhibition of gastric acid secretion, and is independent of food intake and CYP2C19 polymorphism [101]. In a meta-analysis of trials on triple therapy with clarithromycin, replacing PPIs with vonoprazan increased eradication effectiveness by 20% [102]. Preliminary results also indicate a high, 90-95% effectiveness of vonoprazan in dual therapy with amoxicillin (as first and second-line treatment) [103].
5.4. Statement 22
| If H. pylori eradication fails, the choice of second-line treatment should be based on the data on local antimicrobial resistance and the patient’s previous exposure to antibiotics. The recommended second-line treatment in Poland are triple therapy with levofloxacin, quadruple therapy with bismuth and double therapy with high doses of PPI and amoxicillin. The recommended duration of second-line treatment is 14 days. |
| Quality of evidence: low. Recommendation: weak. |
| Regime | Dosage | Treatment duration |
|---|---|---|
| Triple therapy with levofloxacin | •PPIa BID •Amoxicillin 1000 mg BID •Levofloxacin 500 mg QD or 250 mg BID |
10–14 days |
| Quadruple therapy with bismuth | •PPIa BID •Bismuth 120 mg QID •Metronidazole 500 mg TID •Tetracycline 500 mg TID or QID |
10–14 days |
| Dual therapy | •PPIa 20 mg QID •Amoxicillin 750 mg QID |
10–14 days |
Standard proton pump inhibitor (PPI) doses: omeprazole 20 mg, esomeprazole 20 mg, rabeprazole 20 mg, lansoprazole 30 mg, pantoprazole 40 mg.
5.4.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
5.4.2. Discussion
Determining the antibiotic sensitivity profile of H. pylori enables the implementation of targeted treatment and prevents the build-up of antibiotic resistance. As obtaining this information requires, in most cases, the collection of microbiological material during endoscopy, such management is rare in everyday clinical practice. If the antibiotic sensitivity profile of H. pylori is not known, the type of second-line treatment should be made on the basis of previous antibiotic exposure or the known regional prevalence of resistance of the micro-organism. There are no literature data to support the superiority of targeted antibiotic therapy over empirical antibiotic therapy in patients after one or more unsuccessful eradication attempts [104, 105]. A meta-analysis of 13 studies (mostly second-line treatment) showed similar effectiveness of targeted and empirical therapy (RR = 1.09; 95% CI: 0.97 to 1.22) [106]. Close surveillance of the effectiveness of eradication and monitoring of local antibiotic resistance rates are crucial in choosing the optimal empirical therapy.
If quadruple therapy with bismuth fails as first-line treatment, the next regimen should include triple therapy with levofloxacin or double therapy with high doses of PPI and amoxicillin. A literature review with meta-analysis of 54 randomised clinical trials showed that levofloxacin used for a minimum of 10 days in triple therapy (PPI, levofloxacin, amoxicillin) or quadruple therapy (PPI, levofloxacin, bismuth, amoxicillin or tetracycline) was superior to quadruple therapy with bismuth in second-line settings [107]. When prescribing levofloxacin-containing eradication therapy, it is important to take into account the prevalence of resistance to this antibiotic, which is found in up to 31% of infected patients in the United States and 14% in Poland [108, 109]. The addition of bismuth to triple therapy with levofloxacin has been shown to have a beneficial effect. Comparing levofloxacin therapy (PPI, amoxicillin, levofloxacin) with and without bismuth showed a slight superiority for bismuth therapy (87% vs. 83%), particularly obvious in the case of concurrent levofloxacin resistance (71% vs. 37%) [110]. In patients following an unsuccessful eradication attempt, the use of quadruple therapy with bismuth, levofloxacin, amoxicillin and esomeprazole for 14 days showed a high effectiveness of 90% [111].
As H. pylori resistance to amoxicillin is occasional, using dual therapy with high doses of PPI and amoxicillin avoids the problems associated with common resistance to clarithromycin, metronidazole and levofloxacin. The administration of amoxicillin 3–4 times a day in a total dose of 2–3 g is effective in preventing the decrease of concentration below therapeutic values. A meta-analysis of 15 randomised clinical trials showed that the use of PPIs and amoxicillin 4 times a day significantly improved eradication effectiveness compared to lower doses (87% vs. 73%) [112].
Quadruple therapy with bismuth is considered an effective option for second-line treatment after previous failure of quadruple therapy without bismuth. A literature review with a meta-analysis of 30 comparative studies showed that quadruple therapy with bismuth, used as a second-line treatment, had 89% effectiveness [89]. The recommended duration of second-line treatment is 14 days [22, 23, 80].
5.5. Statement 23
| After ineffective first- and second-line treatment, in the absence of the possibility to determine the antibiotic sensitivity of the bacteria, the following are recommended for rescue therapy: dual therapy with high doses of PPI and amoxicillin, therapy with rifabutin, quadruple therapy with bismuth and other antibiotics. |
| Quality of evidence: low. Recommendation: weak. |
5.5.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
5.5.2. Discussion
After ineffective first- and second-line quadruple therapy with bismuth and therapy with levofloxacin, respectively, in the absence of an antibiotic sensitivity determination, the following are recommended for rescue therapy: double therapy with high doses of PPI and amoxicillin, therapy with rifabutin, quadruple therapy with bismuth and other antibiotics. The use of dual therapy with high doses of amoxicillin (4 × 750 mg) and a PPI (rabeprazole 4 × 20 mg) for 14 days as a rescue treatment had a high effectiveness (95.3%, 95% CI: 91.9–98.8%), surpassing the effects of therapy with levofloxacin or sequential treatment [113]. A meta-analysis of 12 randomised trials involving 2,249 patients confirmed that dual therapy with high-dose PPIs and amoxicillin had similar effectiveness to currently recommended regimens (83.2% vs 85.3%, RR = 1.00, 95% CI: 0.97–1.03), with a lower incidence of adverse effects (12.9% vs. 28.0%, RR = 0.53, 95% CI: 0.37–0.76) [114].
Due to the low resistance of H. pylori to rifabutin, determined to be approximately 0.13%, it can be an alternative in rescue therapy [115]. Treatment with rifabutin (2 × 150 mg or 1 × 300 mg), amoxicillin (2 × 1000 mg) and PPI (BID), as third- and fourth-line treatment, was shown to have effectiveness of 66% and 70%, respectively [116]. Based on an analysis of 3,052 patients treated with rifabutin, a successful eradication rate was confirmed in 73% of infected individuals [115]. The use of rifabutin at a daily dose of 300 mg appears to be superior over a daily dose of 150 mg. The incidence of myelotoxicity as a consequence of eradication therapy with the rifabutin regimen was less than 2%, was completely reversible and did not increase the risk of other infections [116]. In regions with an increased incidence of tuberculosis, it is important to remember that the widespread use of rifabutin may increase the risk of Mycobacterium tuberculosis resistance to this antibiotic. An alternative rescue regimen is to reuse quadruple therapy with bismuth using different antibiotics than during the previous therapy. In a Chinese study, the use of three different regimens of quadruple therapy with bismuth, based on prior antibiotic exposure, was associated with eradication effectiveness of 82.5–84% [117].
5.6. Statement 24
| Any eradication treatment should be followed by an assessment of its effectiveness using non-invasive tests at least 4 weeks after the discontinuation of treatment with antibiotics and bismuth and at least 2 weeks after PPI withdrawal. |
| Quality of evidence: high. Recommendation: high. |
5.6.1. Voting
A – 70%; B – 30%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
5.6.2. Discussion
Eradication failure is defined as a persistent positive non-serology test result for H. pylori at least 4 weeks after completion of eradication treatment according to current guidelines and after discontinuation of any medication that may affect the test sensitivity, such as proton pump inhibitors [118]. The most appropriate method for confirming H. pylori eradication is a breath test or detection of H. pylori antigens in faeces using monoclonal antibodies [22]. Determination of IgGs against H. pylori does not differentiate between active and past infection and should therefore not be used in determining the effectiveness of eradication. If an upper gastrointestinal endoscopy is planned, an alternative is to take a biopsy sample for a rapid urease test.
5.7. Statement 25
| In the case of penicillin allergy, the first-line treatment remains quadruple therapy with bismuth; for second-line treatment, it is triple therapy with a fluoroquinolone. |
| Quality of evidence: low. Recommendation: weak. |
5.7.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
5.7.2. Discussion
In patients reporting allergy to penicillins, allergy testing is the appropriate course of action, as allergy to this antibiotic is not confirmed in most of these individuals [119]. In cases of confirmed penicillin allergy, quadruple therapy with bismuth should be used as first-line treatment [120]. Second-line treatment may benefit from triple or quadruple therapy with levofloxacin, or quadruple therapy with bismuth if not previously used [120].
5.8. Statement 26
| Only specific strains of probiotics can reduce the incidence of side effects associated with H. pylori eradication therapy. |
| Quality of evidence: moderate. Recommendation: weak. |
5.8.1. Voting
A – 70%; B – 20%; C – 0%; D – 10%; E – 0%.
Agreement level: high.
5.8.2. Discussion
The results of meta-analyses indicate that specific probiotic strains, through their antimicrobial and immunomodulatory effects, can support the treatment of H. pylori infection, as well as reduce the side effects of eradication treatment. The mechanism of antimicrobial action of probiotics is multifactorial and includes secreting antimicrobial substances, attenuating urease activity, increasing mucus production, inhibiting adhesion of H. pylori to gastric epithelial cells and strengthening the mucosal barrier [121]. A meta-analysis including 5,792 patients showed that probiotic supplementation improved the eradication rate by approximately 10% compared to the control group (OR = 1.94) and reduced the incidence of antibiotic-related side effects (OR = 0.56) [122]. It is important to remember that the effectiveness of probiotics depends on the species of micro-organisms used, their dosage, as well as the duration of administration. Probiotics with proven effects on reducing the incidence of side effects of H. pylori eradication treatment include Lactobacillus spp. and Saccharomyces boulardii [22]. A randomised, double-blind study showed that the administration of Lactobacillus reuteri strain DSM17648 for 2 weeks during classic triple eradication treatment resulted in a significant reduction in gastrointestinal side effects compared to placebo [123]. Probiotics with proven beneficial effects on the effectiveness of H. pylori eradication include certain strains of Lactobacillus, Saccharomyces boulardii and Bifidobacterium [22]. The results of three meta-analyses showed that the addition of S. boulardii to eradication treatment improved treatment effectiveness (RR: 1.09–1.13) [22]. One probiotic preparation combining S. boulardii and Lactobacillus reuteri DSM17648 is available on the Polish market, which, due to the unique synergistic action of these two strains, can make a significant contribution to optimising eradication treatment.
| Probiotics with documented effects in reducing the incidence of side effects of H. pylori eradication |
|
Lactobacillus spp. (L. reuteri DSM17648) Saccharomyces boulardii |
| Probiotics documented effects that increase the effectiveness of H. pylori eradication |
|
Lactobacillus spp. Saccharomyces boulardii Bifidobacterium |
6. Prevention and public health
6.1. Statement 27
| Helicobacter pylori infection is a major etiological factor in gastric adenocarcinoma. |
| Quality of evidence: high. Recommendation: strong. |
6.1.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
6.1.2. Discussion
In 1994, Helicobacter pylori infection was recognised by the World Health Organisation International Agency for Research on Cancer as a Group I carcinogen, responsible for gastric cancer. Treatment of H. pylori infection has become the main method of gastric cancer prevention.
Other environmental factors for gastric cancer include Epstein-Barr virus (EBV) infection, smoking, frequent consumption of red and processed meat and high salt intake. Genetic conditions, autoimmune gastritis and status post partial gastrectomy are also factors predisposing for gastric cancer [124, 125].
6.2. Statement 28
| Helicobacter pylori infection is associated with the development of MALT gastric lymphoma. In MALT lymphoma confined to the stomach, H. pylori eradication is the first-line treatment. |
| Quality of evidence: high. Recommendation: strong. |
6.2.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
6.2.2. Discussion
The stomach is the most common site for non-Hodgkin’s lymphomas originating from B cells (> 95%). The predominant subtype is extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT). In 90% of MALT lymphoma cases, chronic gastritis caused by H. pylori infection is found. A t(11;18)(q21;q21) translocation may be present, which is responsible for disease progression independent of antigenic stimulation, i.e. resistance to H. pylori eradication. Only about 3% of patients are found to have bone marrow involvement. In recent years, there has been a trend towards an increase in the diagnosis of gastric MALT lymphomas without concomitant H. pylori infection (6–40%). These types are characterised by a greater degree of disease progression. If no spiral bacteria are found on histology, other methods should be used to assess H. pylori infection: serology, faecal H. pylori antigen and urea breath test [126].
The primary treatment for gastric MALT lymphoma is the eradication of H. pylori. Eradication is successful in approximately 75–80% of patients, although the optimal time to achieve a treatment response can take up to 24 months. Current guidelines recommend that patients responding to antibiotic therapy should not be qualified for other forms of treatment (radiotherapy, immunotherapy).
Eradication treatment should be used even in patients with MALT gastric lymphoma and no confirmation of H. pylori infection. In patients with no lymphoma regression after antibiotic therapy and who have localised disease, radiotherapy should be used.
Helicobacter pylori infection is also likely to play a role in the pathogenesis of diffuse large B-cell lymphoma (DLBCL) and Burkitt’s lymphoma (BL) [127].
6.3. Statement 29
| Diagnostic upper gastrointestinal endoscopy should include gastric mucosal biopsies both to identify Helicobacter pylori infection and to diagnose and assess the severity of atrophic gastritis using the OLGA and OLGIM histological risk stratification systems. |
| Quality of evidence: moderate. Recommendation: strong. |
6.3.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
6.3.2. Discussion
According to ESGE (European Society of Gastrointestinal Endoscopy) recommendations, in patients with suspected gastritis in the course of H. pylori infection, it is indicate to obtain two sections from the antrum and two sections from the gastric body. The need to take sections from two sites is due to the heterogeneous distribution of the bacteria and the frequent proximal location of gastritis associated with H. pylori infection, especially in the elderly. In addition, according to the recommendations for the management of gastric precancerous conditions (MAPS II), gastric mucosal biopsies should be performed to determine the extent of atrophy and intestinal metaplasia and to establish rules for endoscopic surveillance [128].
Chronic atrophic gastritis and intestinal metaplasia (IM) are considered as pre-cancerous conditions of gastric cancer. Histological risk stratification systems (OLGA (Operative Link for Gastritis Assessment) and OLGIM (Operative Link for Gastric Intestinal Metaplasia)) should be used to assess the severity of atrophic gastritis and intestinal metaplasia. The advanced stages of atrophic gastritis are considered to be significant (moderate to severe = grades III and IV) atrophy or intestinal metaplasia that involve both the mucosa of the antrum and gastric body. Histologically confirmed intestinal metaplasia is the most reliable marker of gastric mucosal atrophy. The risk of gastric cancer is increased in patients with OLGIM grades III and IV [129, 130].
High-resolution endoscopy with chromoendoscopy shows superiority in identifying pre-cancerous lesions and early gastric cancer compared to white-light endoscopy.
To assess the severity of chronic atrophic gastritis, it is advisable to take 5 sections according to the updated Sydney protocol: 2 sections from the antrum (greater and lesser curvature; 3 cm from the pylorus), 2 sections from the body (lesser curvature; 4 cm proximal to the gastric angle and halfway through the greater curvature) and 1 section from the gastric angle – into separate containers [29, 131].
6.4. Statement 30
| In patients with chronic atrophic gastritis and H. pylori infection, we recommend eradication to reduce the risk of gastric adenocarcinoma. |
| Quality of evidence: low. Recommendation: weak. |
6.4.1. Voting
A – 90%; B – 0%; C – 0%; D – 10%; E – 0%.
Agreement level: high.
6.4.2. Discussion
Eradication of H. pylori promotes healing of chronic non-atrophic gastritis and may lead to regression of atrophic gastritis and reduces the risk of gastric cancer in patients with non-atrophic and atrophic gastritis [128].
In patients with confirmed intestinal metaplasia, H. pylori eradication does not appear to significantly reduce the risk of gastric cancer, but reduces inflammation and atrophy, and should therefore be considered [128].
6.5. Statement 31
| The mode of endoscopic surveillance in patients with atrophic gastritis and intestinal metaplasia depends on the location of the lesions (body and/or antrum) and the following risk factors: family history of gastric cancer, persistent H. pylori infection, incomplete intestinal metaplasia and a diagnosis of autoimmune gastritis. |
| Quality of evidence: moderate. Recommendation: strong. |
6.5.1. Voting
A – 100%; B – 0%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
6.5.2. Discussion
Patients with atrophic gastritis (mild and moderate) located only in the pre-pyloric area and around the gastric angle, without metaplasia and without risk factors (family history of gastric cancer; persistent H. pylori infection) do not require endoscopic surveillance.
Patients with atrophic gastritis and metaplasia confined to the antrum or gastric body without risk factors do not require endoscopic surveillance. However, when risk factors are present (i.e. family history of gastric cancer; persistent H. pylori infection, autoimmune gastritis) they should have a gastroscopy every 3 years.
In patients with advanced atrophic gastritis, i.e. atrophy or metaplasia in the antrum and body, OLGA/OLGIM III/IV, without a family history of gastric cancer, endoscopic surveillance (gastroscopy + sections) every 3 years is indicated due to the increased risk of gastric cancer. On the other hand, in this group of patients when close relatives have developed gastric cancer, they are subject to endoscopic surveillance every 1–2 years.
In patients with dysplasia, repeat high-resolution endoscopy with chromoendoscopy should be performed at a reference centre, and if no endoscopic lesions are found, follow-up high-resolution gastroscopy with chromoendoscopy should be performed at 12 months (low-grade dysplasia) and 6 months (high-grade dysplasia), respectively [128, 131, 132]. The management algorithm for patients with atrophic gastritis is shown in Figure 1.
Figure 1.

The management algorithm for patients with atrophic gastritis, intestinal metaplasia or dysplasia
6.6. Statement 32
| In patients with autoimmune atrophic gastritis, follow-up endoscopies every 3-5 years are recommended regardless of H. pylori infection status. |
| Quality of evidence: low. Recommendation: weak. |
6.6.1. Voting
A – 60%; B – 20%; C – 20%; D – 0%; E – 0%.
Agreement level: high.
6.6.2. Discussion
Autoimmune gastritis is a chronic, progressive inflammatory condition in which antibodies are formed against the lining cells and against Castle’s intrinsic factor. During the course of inflammation, the glandular cells of the gastric mucosa are replaced by foci of intestinal metaplasia. The inflammatory process leads to a significant reduction in hydrochloric acid secretion and the development of achlorhydria. Treatment consists of parenteral vitamin B12 supplementation and, in the case of H. pylori infection, eradication is recommended [128].
6.7. Statement 33
| Establishing a link between the use of anticoagulants (coumarins, NOACs) in the coexistence of H. pylori infection and an increased risk of upper gastrointestinal bleeding requires further research. |
| Quality of evidence: low. Recommendation: weak. |
6.7.1. Voting
A – 90%; B – 10%; C – 0%; D – 0%; E – 0%.
Agreement level: high.
6.7.2. Discussion
Drugs belonging to the anticoagulants do not cause direct damage to the mucosa of the gastrointestinal tract. The mechanism of gastrointestinal bleeding is due to the disruption of the physiological haemostasis processes.
To date, few studies have been published that have assessed the association between H. pylori infection and oral anticoagulants, either vitamin K antagonists or new non-vitamin K antagonist oral anticoagulants (NOACs).
In a cohort study published in 2018, anticoagulant use was shown to increase the risk of ulcer bleeding (OR = 2.34), while no increased risk of ulcer bleeding was demonstrated in patients with H. pylori infection taking oral anticoagulants (OR = 0.95) [133].
A randomised study of a population with non-valvular atrial fibrillation using NOACs showed a 25% higher overall risk of major gastrointestinal haemorrhage complications compared to a population treated with warfarin for the same indication, with some differences between individual drugs [134]. No data available on H. pylori infection status.
As the most important risk factors for gastrointestinal bleeding in patients taking anticoagulants, most publications mark out: age over 65 years (VKAs) or over 75 years (NOACs), history of peptic ulcer disease with or without complications, concomitant use of antiplatelet drugs or NSAIDs. Confirmation of at least 1 risk factor is an indication for the use of PPI. In patients with a history of gastric or duodenal ulcers, testing for H. pylori infection is recommended before the initiation of anticoagulants [133, 135].
Conflict of interest
Professor PhD, MD Anita Gąsiorowska: a speaker for Urgo Polfa Lodz. Professor PhD, MD Jarosław Daniluk: a speaker for DiaSorin Poland. The other authors declare no conflict of interest.
References
- 1.Brouwers M, Kho M, Browman G, et al. for the AGREE Next Steps Consortium . AGREE II: advancing guideline development, reporting and evaluation in healthcare. CMAJ 2010; 182: E839-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Guyatt G, Oxman A, Akl A, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary findings tables. J Clin Epidemiol 2011; 64: 383-94. [DOI] [PubMed] [Google Scholar]
- 3.Dalkey N, Helmer O. An experimental application of the DELPHI method to the use of experts. Manag Sci 1963; 9: 458-67. [Google Scholar]
- 4.Kersulyte D, Mukhopadhyay AK, Velapatino B, et al. Differences in genotypes of Helicobacter pylori from different human populations. J Bacteriol 2000; 182: 3210-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Peek RM Jr. Events at the host-microbial interference of the gastrointestinal tract. IV. The pathogenesis of H. pylori persistence. Am J Physiol Gastrointest Liver Physiol 2005; 289: 8-12. [DOI] [PubMed] [Google Scholar]
- 6.Amieva MR, El-Omar EM. Host-bacterial interactions in Helicobacter pylori infection. Gastroenterology 2008; 134: 306-23. [DOI] [PubMed] [Google Scholar]
- 7.Correa P, Piazuelo MB. Natural history of Helicobacter pylori infection. Dig Liver Dis 2008; 40: 490-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yamaoka Y, Kodama T, Kita M, et al. Relationship of vacA genotypes of Helicobacter pylori to cagA status, cytotoxin production, and clinical outcome. Helicobacter 1998; 3: 241-53. [DOI] [PubMed] [Google Scholar]
- 9.Hooi JK, Lai WY, Ng WK, et al. Global prevalence of Helicobacter pylori infection: systematic review and meta-analysis. Gastroenterology 2017; 153: 420-9. [DOI] [PubMed] [Google Scholar]
- 10.Laszewicz W, Iwańczak F, Iwańczak B; Task Force of the Polish Society of Gastroenterology . Seroprevalence of Helicobacter pylori infection in Polish children and adults depending on socioeconomic status and living conditions. Adv Med Sci 2014; 59: 147-50. [DOI] [PubMed] [Google Scholar]
- 11.Szaflarska-Popławska A, Soroczyńska-Wrzyszcz A. Prevalence of Helicobacter pylori infection among junior high school students in Grudziadz, Poland. Helicobacter 2019; 24: e12552. [DOI] [PubMed] [Google Scholar]
- 12.Cave DR. Transmission and epidemiology of Helicobacter pylori. Am J Med 1996; S5: 12S-18S. [DOI] [PubMed] [Google Scholar]
- 13.Kim SE, Kim N, Lee JY, et al. Prevalence and risk factors of functional dyspepsia in health check-up population: a nationwide multicenter prospective study. J Neurogastroenterol Motil 2018; 24: 603-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Correa P, Houghton J. Carcinogenesis of Helicobacter pylori. Gastroenterology 2007; 133: 659-72. [DOI] [PubMed] [Google Scholar]
- 15.Tan P, Yeoh KG. Genetics and molecular pathogenesis of gastric adenocarcinoma. Gastroenterology 2015; 149: 1153-62. [DOI] [PubMed] [Google Scholar]
- 16.IARC/WHO . Helicobacter pylori eradication as a strategy for preventing gastric cancer. International Agency for Research on Cancer/ World Health Organisation, 2014. “http://www.iarc.fr/en/publications/pdfs-online/wrk8/” www.iarc.fr/en/publications/pdfs-online/wrk8/ (dostęp na listopad 2020).
- 17.Li L, Tan J, Liu L, et al. Association between H. pylori infection and health putcomes: an umbrella review of systematic reviews and meta-analyses. BMJ Open 2020; 10: e031951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.McGee DJ, Mobley HL. Pathogenesis of Helicobacter pylori infection. Curr Opin Gastroenterol 2000; 16: 24-31. [DOI] [PubMed] [Google Scholar]
- 19.Lamb A, Yamaguchi H, Chen LF. The many roads traveled by Helicobacter pylori to NF-kappaB activation. Gut Microbes 2010; 1: 109-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Niikura R, Hayakawa Y, Hirata Y, et al. he Reduction in gastric atrophy after Helicobacter pylori eradication is reduced by treatment with inhibitors of gastric acid secretion. Int J Mol Sci 2019; 20: 1913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sugano K, Tack J, Kuipers EJ, et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015; 64: 1353-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Malfertheiner P, Megraud F, Rokkas T, et al. European Helicobacter and Microbiota Study group . Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut 2022. doi: 10.1136/gutjnl-2022-327745. [DOI] [Google Scholar]
- 23.Chey WD, Leontiadis GI, Howden CW, et al. ACG clinical guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol 2017; 112: 212-39. [DOI] [PubMed] [Google Scholar]
- 24.Chiang TH, Chang WJ, Chen SL, et al. Mass eradication of Helicobacter pylori to reduce gastric cancer incidence and mortality: a long-term cohort study on Matsu Islands. Gut 2021; 70: 243-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Choi IJ, Kim CG, Lee JY, et al. Family history of gastric cancer and Helicobacter pylori treatment. N Engl J Med 2020; 382: 427-36. [DOI] [PubMed] [Google Scholar]
- 26.Ford AC, Yuan Y, Moayyedi P. Helicobacter pylori eradication therapy to prevent gastric cancer: systematic review and meta-analysis. Gut 2020; 69: 2113-21. [DOI] [PubMed] [Google Scholar]
- 27.Kumar S, Metz DC, Ellenberg S, et al. Risk factors and incidence of gastric cancer after detection of Helicobacter pylori infection: a large cohort study. Gastroenterology 2020; 158: 527-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Saumoy M, Schneider Y, Shen N, et al. Cost effectiveness of gastric cancer screening according to race and ethnicity. Gastroenterology 2018; 155: 648-60. [DOI] [PubMed] [Google Scholar]
- 29.Pouw R, Barret M, Biermann K, et al. Endoscopic tissue sampling–Part 1: Upper gastrointestinal and hepatopancreatobiliary tracts. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021; 53: 1174-88. [DOI] [PubMed] [Google Scholar]
- 30.O’Connor A, O’Morain C. Mistakes in the management of Helicobacter pylori infection and how to avoid them. UEG Education 2017; 17: 42-4. [Google Scholar]
- 31.Black CJ, Paine PA, Agrawal A, et al. British Society of Gastroenterology guidelines on the management of functional dyspepsia. Gut 2022; 71: 1697-723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wauters L, Dickman R, Drug V, et al. United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) consensus on functional dyspepsia. United European Gastroenterol J 2021; 9: 307-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Eusebi L, Black C, Howden C, et al. Effectiveness of management strategies for uninvestigated dyspepsia: systematic review and network meta-analysis. BMJ 2019; 367: 161136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Beresniak A, Malfertheiner P, Franceschi F, et al. Helicobacter pylori “Test-and-Treat” strategy with urea breath test: a cost-effective strategy for the management of dyspepsia and the prevention of ulcer and gastric cancer in Spain-Results of the Hp-Breath initiative. Helicobacter 2020; 25: e12693. [DOI] [PubMed] [Google Scholar]
- 35.https://onkologia.org.pl/pl/raporty dostęp na dzień 26.09.2022 [Google Scholar]
- 36.Januszewicz W, Witczak K, Wieszczy P, et al. Prevalence and risk factors of upper gastrointestinal cancers missed during endoscopy: a nationwide registry-based study. Endoscopy 2022; 54: 653-60. [DOI] [PubMed] [Google Scholar]
- 37.Song Y, Liu X, Cheng W, et al. The global, regional and national burden of stomach cancer and its attributable risk factors from 1990 to 2019. Sci Rep 2022; 12: 11542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Morgan E, Arnold M, Camargo MC, et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020-40: a population-based modelling study. EClinicalMedicine 2022; 47: 101404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bartnik W, Celinska-Cedro D, Dzieniszeski J, et al. Wytyczne Polskiego Towarzystwa Gastroenterologii dotyczące diagnostyki i leczenia zakażenia Helicobacter pylori. Gastroenterol Klin 2014; 6: 41-9. [Google Scholar]
- 40.Kurek K, Baniukiewicz A, Białek A, et al. Wskaźniki jakości w endoskopii górnego odcinka przewodu pokarmowego–wytyczne grupy roboczej Polskiego Towarzystwa Gastroenterologii. Gastroenterol Prakt 2014; 3: 30-48. [Google Scholar]
- 41.Rokkas T, Pistiolas D, Sechopoulos P, et al. The Long-term impact of Helicobacter pylori eradication on gastric histology: a systematic review and meta-analysis. Helicobacter 2007; 12: 32-8. [DOI] [PubMed] [Google Scholar]
- 42.Choi IJ, Kook M-C, Kim Y-I, et al. Helicobacter pylori therapy for the prevention of metachronous gastric cancer. N Engl J Med 2018; 378: 1085-95. [DOI] [PubMed] [Google Scholar]
- 43.Jaworski W. Podręcznik chorób żołądka i dietetyki szczegółowej. Wydawnictwo Dzieł Lekarskich Polskich, Kraków 1899; 30-47. [Google Scholar]
- 44.Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984; 8390: 1311-15. [DOI] [PubMed] [Google Scholar]
- 45.Kamada T, Satoh K, Itoh T, et al. Evidence-based clinical practice guidelines for peptic ulcer disease 2020. J Gastroenterol 2021; 56: 303-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Leodolter A, Kulig M, Brasch H, et al. A meta-analysis comparing eradication, healing and relapse rates in patients with Helicobacter pylori-associated gastric or duodenal ulcer. Aliment Pharmacol Ther 2001; 15: 1949-58. [DOI] [PubMed] [Google Scholar]
- 47.Yan L, Chen Y, Chen F. Effect of Helicobacter pylori eradication on gastric cancer prevention: updated report from a randomized controlled trial with 26.5 years of follow-up. Gastroenterology 2022; 163: 154-62. [DOI] [PubMed] [Google Scholar]
- 48.Kim TJ, Kim ER, Hong SN, et al. Effectiveness of acid suppressants and other mucoprotective agents in reducing the risk of occult gastrointestinal bleeding in nonsteroidal anti-inflammatory drug users. Sci Rep 2019; 9: 11696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Venerito M, Schneider C, Costanzo R, et al. Contribution of Helicobacter pylori infection to the risk of peptic ulcer bleeding in patients on nonsteroidal anti-inflammatory drugs, antiplatelet agents, anticoagulants, corticosteroids and selective serotonin reuptake inhibitors. Aliment Pharmacol Ther 2018; 47: 1464-71. [DOI] [PubMed] [Google Scholar]
- 50.Chan FK, Sung JJ, Chung SC, et al. Randomised trial of eradication of Helicobacter pylori before non-steroidal anti-inflammatory drug therapy to prevent peptic ulcers. Lancet 1997; 350: 975-79. [DOI] [PubMed] [Google Scholar]
- 51.Liang CM, Yang SC, Wu CK, et al. Risk of recurrent peptic ulcer disease in patients receiving cumulative defined daily dose of nonsteroidal anti-inflammatory drugs. J Clin Med 2019; 8: 1722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hawkey C, Avery A, Coupland C, et al. Helicobacter pylori eradication for primary prevention of peptic ulcer bleeding in older patients prescribed aspirin in primary care (HEAT): a randomised, double-blind, placebo-controlled trial. Lancet 2022; 400: 1597-606. [DOI] [PubMed] [Google Scholar]
- 53.Alam SM, Qasswal M, Ahsan MJ, et al. Selective serotonin reuptake inhibitors increase risk of upper gastrointestinal bleeding when used with NSAIDs: a systemic review and meta-analysis. Sci Rep 2022; 12: 14452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Rockey DC, Altayar O, Falck-Ytter Y, et al. AGA Technical Review on gastrointestinal evaluation of iron deficiency anemia. Gastroenterology 2020; 159: 1097-119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Snook J, Bhala N, Beales ILP, et al. British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults. Gut 2021; 70: 2030-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Stasi R, Sarpatwari A, Segal JB, et al. Effects of eradication of Helicobacter pylori infection in patients with immune thrombocytopenic purpura: a systematic review. Blood 2009; 113: 1231-40. [DOI] [PubMed] [Google Scholar]
- 57.Neunert C, Lim W, Crowther M, et al. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood 2011; 117: 4190-207. [DOI] [PubMed] [Google Scholar]
- 58.Hammer ST, Greenson JK. The clinical significance of duodenal lymphocytosis with normal villus architecture. Arch Pathol Lab Med 2013; 137: 1216-9. [DOI] [PubMed] [Google Scholar]
- 59.Yu X, Wang Z, Wang L, et al. Gastric hyperplastic polyps inversely associated with current Helicobacter pylori infection. Exp Ther Med 2020; 19: 3143-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Nielsen JA, Roberts CA, Lager DJ, et al. Lymphocytic gastritis is not associated with active Helicobacter pylori infection. Helicobacter 2014; 19: 349-55. [DOI] [PubMed] [Google Scholar]
- 61.https://www.iarc.who.int/news-events/iarc-and-partners-to-tackle-gastric-cancer-in-europe-through-h-pylori-eradication/ Available at 05.12.2022.
- 62.Leja M, Park JY, Murillo R, et al. Multicentric randomised study of Helicobacter pylori eradication and pepsinogen testing for prevention of gastric cancer mortality: the GISTAR study. BMJ Open 2017; 7: e016999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Adrych K. Czy każdy chory z zakażeniem Helicobacter pylori powinien być leczony? Aktualne stanowisko. Gastroenterol Klin 2018; 10: 23-31. [Google Scholar]
- 64.Adrych K, Solnica B. Diagnostyka zakażenia Helicobacter pylori. In: Interna Szczeklika. Gajewski P (ed.). MP 2021; 948-50. [Google Scholar]
- 65.Gisbert JP, de la Morena F, Abraira V. Accuracy of monoclonal stool antigen test for the diagnosis of H. pylori infection: a systematic review and meta-analysis. Am J Gastroenterol 2006; 101: 1921-23. [DOI] [PubMed] [Google Scholar]
- 66.Veijola L, Myllyluoma E, Korpela R, et al. Stool antigen tests in the diagnosis of Helicobacter pylori infection before and after eradication therapy. World J Gastroenterol 2005; 11: 7340-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Gisbert JP, Pajares JM. Stool antigen test for the diagnosis of Helicobacter pylori infection: a systematic review. Helicobacter 2004; 9: 347-68. [DOI] [PubMed] [Google Scholar]
- 68.Lario S, Ramírez-Lázaro MJ, Montserrat A, et al. Diagnostic accuracy of three monoclonal stool tests in a large series of untreated Helicobacter pylori infected patients. Clin Biochem 2016; 49: 682-7. [DOI] [PubMed] [Google Scholar]
- 69.Korkmaz H, Kesli R, Karabagli P, et al. Comparison of the diagnostic accuracy of five different stool antigen tests for the diagnosis of Helicobacter pylori infection. Helicobacter 2013; 18: 384-91. [DOI] [PubMed] [Google Scholar]
- 70.Braden B, Teuber G, Dietrich CF, et al. Comparison of new faecal antigen test with (13)C-urea breath test for detecting Helicobacter pylori infection and monitoring eradication treatment: prospective clinical evaluation. BMJ 2000; 320: 148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Calvet X, Lario S, Ramírez Lázaro MJ, et al. Comparative accuracy of 3 monoclonal stool tests for diagnosis of Helicobacter pylori infection among patients with dyspepsia. Clin Infect Dis 2010; 50: 323-8. [DOI] [PubMed] [Google Scholar]
- 72.Wu DC, Wu IC, Wang SW, et al. Comparison of stool enzyme immunoassay and immunochromatographic method for detecting Helicobacter pylori antigens before and after eradication. Diagn Microbiol Infect Dis 2006; 56: 373-8. [DOI] [PubMed] [Google Scholar]
- 73.Gisbert JP, Trapero M, Calvet X, et al. Evaluation of three different tests for the detection of stool antigens to diagnose Helicobacter pylori infection in patients with upper gastrointestinal bleeding. Aliment Pharmacol Ther 2004; 19: 923-8. [DOI] [PubMed] [Google Scholar]
- 74.Korkmaz H, Findik D, Ugurluoglu C, et al. Reliability of stool antigen tests: investigation of the diagnostic value of a new immunochromatographic Helicobacter pylori approach in dyspeptic patients. Asian Pac J Cancer Prev 2015; 16: 657-60. [DOI] [PubMed] [Google Scholar]
- 75.Ferwana M, Abdulmajeed I, Alhajiahmed A, et al. Accuracy of urea breath test in Helicobacter pylori infection: meta-analysis. World J Gastroenterol 2015; 21: 1305-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Shiotani A, Saeed A, Yamaoka Y, et al. Citric acid-enhanced Helicobacter pylori urease activity in vivo is unrelated to gastric emptying. Aliment Pharmacol Ther 2001; 15: 1763-7. [DOI] [PubMed] [Google Scholar]
- 77.Graham DY, Opekun AR, Jogi M, et al. False negative urea breath tests with H2-receptor antagonists: interactions between Helicobacter pylori density and pH. Helicobacter 2004; 9: 17-27. [DOI] [PubMed] [Google Scholar]
- 78.Wright CL, Kelly JK. The use of routine special stains for upper gastrointestinal biopsies. Am J Surg Pathol 2006; 30: 357-61. [DOI] [PubMed] [Google Scholar]
- 79.Genta RM, Graham DY. Comparison of biopsy sites for the histopathologic diagnosis of Helicobacter pylori: a topographic study of H. pylori density and distribution. Gastrointest Endosc 1994; 40: 342-5. [DOI] [PubMed] [Google Scholar]
- 80.Fallone CA, Chiba N, van Zanten SV, et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 2016; 151: 51-69. [DOI] [PubMed] [Google Scholar]
- 81.Nyssen OP, Vaira D, Tepes B, et al. Room for improvement in the treatment of Helicobacter pylori infection: lessons from the European registry on H. pylori management (HP-EUREG). J Clin Gastroenterol 2021; 56: e98-108. [DOI] [PubMed] [Google Scholar]
- 82.Yu J, Yang P, Qin X, et al. Impact of smoking on the eradication of Helicobacter pylori. Helicobacter 2021; 27: e12860. [DOI] [PubMed] [Google Scholar]
- 83.Savoldi A, Carrara E, Graham DJ, et al. Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in world health organization regions. Gastroenterology 2018; 155: 1372-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Murakami TT, Scranton RA, Brown HE, et al. Management of Helicobacter pylori in the united states: results from a national survey of gastroenterology physicians. Prev Med 2017; 100: 216-22. [DOI] [PubMed] [Google Scholar]
- 85.Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the who priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis 2018; 18: 318-27. [DOI] [PubMed] [Google Scholar]
- 86.Dzierzanowska-Fangrat K, Rozynek E, Celinska-Cedro E, et al. Antimicrobial resistance of Helicobacter pylori in Poland: a multicentre study. Int J Antimicrob Agents 2005; 26: 230-4. [DOI] [PubMed] [Google Scholar]
- 87.Binkowska A, Biernat MM, Laczmański L, et al. Molecular patterns of resistance among Helicobacter pylori strains in south-western Poland. Front Microbiol 2018; 9: 3154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Nyssen O, McNicholl PAG, Megraud F, et al. Sequential versus standard triple first-line therapy for Helicobacter pylori eradication. Cochrane Database Syst Rev 2016; 2016: CD009034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Nyssen O, McNicholl AG, Gisbert JP. Meta-analysis of three-in-one single capsule bismuth-containing quadruple therapy for the eradication of Helicobacter pylori. Helicobacter 2019; 24: e12570. [DOI] [PubMed] [Google Scholar]
- 90.Malfertheiner P, Bazzoli F, Delchier JC, et al. Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: a randomised, open-label, non-inferiority, phase 3 trial. Lancet 2011; 377: 905-13. [DOI] [PubMed] [Google Scholar]
- 91.Macías-García F, Bastón-Rey I, Iglesia-García D, et al. Bismuth-containing quadruple therapy versus concomitant quadruple therapy as first-line treatment for Helicobacter pylori infection in an area of high resistance to clarithromycin: a prospective, cross-sectional, comparative, open trial. Helicobacter 2019; 24: e12546. [DOI] [PubMed] [Google Scholar]
- 92.Ji Y, Lu H. Meta-analysis: High-dose vs. Low-dose metronidazole-containing therapies for Helicobacter pylori eradication treatment. PLoS One 2018; 13: e0189888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Nyssen O, Bordin D, Tepes B, et al. European registry on Helicobacter pylori management (HP-EUREG): patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21 533 patients. Gut 2021; 70: 40-54. [DOI] [PubMed] [Google Scholar]
- 94.Nyssen O, Perez-Aisa A, Castro-Fernandez M, et al. European registry on Helicobacter pylori management: single-capsule bismuth quadruple therapy is effective in real-world clinical practice. United European Gastroenterol J 2021; 9: 38-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Gisbert J, McNicholl A. Eradication of Helicobacter pylori infection with non-bismuth quadruple concomitant therapy. Front Anti-infective Drug Discov 2020; 1-34. DOI: 10.2174/9789811412387119080001. [DOI] [Google Scholar]
- 96.Fischbach LA, an Zanten S, Dickason J. Meta-analysis: the efficacy, adverse events, and adherence related to first-line anti-Helicobacter pylori quadruple therapies. Aliment Pharmacol Ther 2004; 20: 1071-82. [DOI] [PubMed] [Google Scholar]
- 97.Wasielica-Berger J, Gugnacki P, Mlynarczyk M, et al. Comparative effectiveness of various eradication regimens for Helicobacter pylori infection in the northeastern region of Poland. Int J Environ Res Public Health 2022; 19: 6921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Romano M, Gravina AG, Nardone G, et al. Non-bismuth and bismuth quadruple therapies based on previous clarithromycin exposure are as effective and safe in an area of high clarithromycin resistance: a real-life study. Helicobacter 2020; 25: e12694. [DOI] [PubMed] [Google Scholar]
- 99.Kuo CH, Lu CY, Shih HY, et al. Cyp2c19 polymorphism influences Helicobacter pylori eradication. World J Gastroenterol 2014; 20: 16029-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Villoria A, Garcia P, Calvet X, et al. Meta-analysis: high-dose proton pump inhibitors vs. standard dose in triple therapy for Helicobacter pylori eradication. Aliment Pharmacol Ther 2008; 28: 868-77. [DOI] [PubMed] [Google Scholar]
- 101.Ohkuma K, Iida H, Inoh Y, et al. Comparison of the early effects of vonoprazan, lansoprazole and famotidine on intragastric pH: a three-way crossover study. J Clin Biochem Nutr 2018; 63: 80-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Jung YS, Kim EH, Park CH. Systematic review with meta-analysis: the efficacy of vonoprazan-based triple therapy on Helicobacter pylori eradication. Aliment Pharmacol Ther 2017; 46: 106-14. [DOI] [PubMed] [Google Scholar]
- 103.Hunt RH, Scarpignato C. Potent acid suppression with ppis and p-cabs: What’s new? Curr Treat Options Gastroenterol 2018; 16: 570-90. [DOI] [PubMed] [Google Scholar]
- 104.López-Góngora S, Puig I, Calvet X, et al. Systematic review and meta-analysis: susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. J Antimicrob Chemother 2015; 70: 2447-55. [DOI] [PubMed] [Google Scholar]
- 105.Liou JM, Chen CC, Chang CY, et al. Efficacy of genotypic resistance-guided sequential therapy in the third-line treatment of refractory Helicobacter pylori infection: a multicentre clinical trial. J Antimicrob Chemother 2013; 68: 450-6. [DOI] [PubMed] [Google Scholar]
- 106.Espada M, Gisbert J. Non-bismuth quadruple concomitant treatment for H. pylori eradication: systematic review and meta-analysis. United European Gastroenterol J 2021; 9: 325. [Google Scholar]
- 107.Chang YL, Tung YC, Tu YK, et al. Efficacy of second-line regimens for Helicobacter pylori eradication treatment: a systemic review and network meta-analysis. BMJ Open Gastroenterol 2020; 7: e000472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Shiota S, Reddy R, Alsarraj A, et al. Antibiotic resistance of Helicobacter pylori among male united states veterans. Clin Gastroenterol Hepatol 2015; 13: 1616-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Megraud F, Coenen S, Versporten A, et al. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013; 62: 34-42. [DOI] [PubMed] [Google Scholar]
- 110.Liao J. Zheng Q, Liang X, et al. Effect of fluoroquinolone resistance on 14-day levofloxacin triple and triple plus bismuth quadruple therapy. Helicobacter 2013; 18: 373-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Gisbert JP, Romano M, Gravina AG, et al. Helicobacter pylori second-line rescue therapy with levofloxacin-and bismuth-containing quadruple therapy, after failure of standard triple or non-bismuth quadruple treatments. Aliment Pharmacol Ther 2015; 41: 768-75. [DOI] [PubMed] [Google Scholar]
- 112.Zhu YJ, Zhang Y, Wang TY, et al. High dose PPI-amoxicillin dual therapy for the treatment of of Helicobacter pylori infection: a systematic review with meta-analysis. Therap Adv Gastroenterol 2020; 13: 1756284820937115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Yang JC, Lin CH, Wang HL, et al. High-dose dual therapy is superior to standard first-line or rescue therapy for Helicobacter pylori infection. Clin Gastroenterol Hepatol 2015; 13: 895-905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Gao CP, Zhang D, Zhang T, et al. PPI-amoxicillin dual therapy for Helicobacter pylori infection: an update based on a systematic review and meta-analysis. Helicobacter 2020; 25: e12692. [DOI] [PubMed] [Google Scholar]
- 115.Gisbert JP. Rifabutin for the treatment of Helicobacter pylori infection: a review. Pathogens 2020; 10: 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Gisbert JP, Calvet X. Review article: rifabutin in the treatment of refractory Helicobacter pylori infection. Aliment Pharmacol Ther 2012; 35: 209-21. [DOI] [PubMed] [Google Scholar]
- 117.Zhou JJ, Shi X, Zheng SP, et al. Efficacy of bismuth-based quadruple therapy for eradication of Helicobacter pylori infection based on previous antibiotic exposure: a large-scale prospective, single-center clinical trial in China. Helicobacter 2020; 25: e12755. [DOI] [PubMed] [Google Scholar]
- 118.Shah SC, Iyer PG, Moss SF. AGA clinical practice update on the management of refractory Helicobacter pylori infection: expert review. Gastroenterology 2021; 160: 1831-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Macy E. Penicillin allergy: optimizing diagnostic protocols, public health implications, and future research needs. Curr Opin Allergy Clin Immunol 2015; 15: 308-13. [DOI] [PubMed] [Google Scholar]
- 120.Nyssen OP, Pérez-Aisa A, Tepes B, et al. , Helicobacter pylori first-line and rescue treatments in patients allergic to penicillin: experience from the European registry on H. pylori management (hp-eureg). Helicobacter 2020; 25: e12686. [DOI] [PubMed] [Google Scholar]
- 121.Compare D, Sgamato C, Nardone OM, et al. Probiotics in gastrointestinal diseases: all that glitters is not gold. Dig Dis 2022; 40: 123-32. [DOI] [PubMed] [Google Scholar]
- 122.Zhang M, Zhang C, Zhao J, et al. Meta-analysis of the efficacy of probiotic-supplemented therapy on the eradication of H. pylori and incidence of therapy-associated side effects. Microb Pathog 2020; 147: 104403. [DOI] [PubMed] [Google Scholar]
- 123.Yang C, Liang L, Lv P, et al. Effects of non-viable Lactobacillus reuteri combining with 14-day standard triple therapy on Helicobacter pylori eradication: a randomized double-blind placebo-controlled trial. Helicobacter 2021; 26: e12856. [DOI] [PubMed] [Google Scholar]
- 124.Thrift AP, El-Serag HB. Burden of gastric cancer. Clin Gastroenterol Hepatol 2020; 18: 534-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Kim J, Cragin Wang T. Helicobacter pylori and gastric cancer. Gastrointest Endoscopy Clin N Am 2021; 31: 451-65. [DOI] [PubMed] [Google Scholar]
- 126.Raderer M, Kiesewetter B. What you always wanted to know about gastric MALT-lymphoma: a focus on recent developments. Ther Adv Med Oncol 2021; 13: 17588359211033825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Ishikawa E, Nakamura M, Satou A, et al. Mucosa-associated lymphoid tissue (MALT) lymphoma on the gastrointestinal tract in the modern era. Cancer 2022; 14: 446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Pimentel-Nunes P, Libanio D, Marcos-Pinto R, et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019; 51: 365-88. [DOI] [PubMed] [Google Scholar]
- 129.Rugge M, Meggio A, Pennelli G, et al. Gastritis staging in clinical practice: the OLGA staging system. Gut 2007; 56: 631-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Capelle LG, de Vries AC, Haringsma J, et al. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest Endosc 2010; 71: 1150-8. [DOI] [PubMed] [Google Scholar]
- 131.Banks M, Graham D, Jansen M, et al. British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut 2019; 68: 1545-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Gupta S, Li D, El Serag HB, et al. AGA Clinical Practice Guidelines on Management of Gastric Intestinal Metaplasia. Gastroenterology 2020; 158: 693-702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Arbignani MG, Gatta L, Gabrielli D, et al. Gastroprotection in patients on antiplatelet and/or anticoagulant therapy: a position paper of National Association of Hospital Cardiologists (ANMCO) and the Italian Association of Hospital Gastroenterologists and Endoscopists (AIGO). Eur J Intern Med 2021; 85: 1-13. [DOI] [PubMed] [Google Scholar]
- 134.Radaelli F, Fuccio L, Paggi S, et al. What gastroenterologists should know about direct oral anticoagulants Dig Liver Dis 2020; 52: 1115-25. [DOI] [PubMed] [Google Scholar]
- 135.Sostres C, Gargallo CJ. Gastrointestinal lesions and complications of low-dose aspirin in the gastrointestinal tract. Best Pract Res Clin Gastroenterol 2012; 26: 141-51. [DOI] [PubMed] [Google Scholar]