

Abstract
Research suggests that transportation is an important social determinant of health, because the ability to get around is consequential for accessing health care and nutritious food and for making social connections. We used an inductive mixed-methods approach and a quantitative k-means clustering approach to identify 5 categories of transportation insecurity using the validated 16-item Transportation Security Index. The resulting 5-category measure distinguished among respondents with qualitatively different experiences of transportation insecurity. Analyzing data from 2018 that were representative of the US adult population aged 25 years or older, we demonstrated a nonparametric association between transportation insecurity and 2 different health measures (self-rated health and depressive symptoms). There was a threshold relationship between self-rated health and any level of transportation insecurity. High transportation insecurity had a very strong relationship with depressive symptoms. The categorical Transportation Security Index will be useful for clinicians who wish to screen for transportation-related barriers to health care. It will also facilitate research investigating the influence of transportation insecurity on health outcomes and provide the basis for interventions designed to address health disparities.
Keywords: categorical measures, health-care access, health outcomes, screeners, social determinants of health, transportation, transportation insecurity, Transportation Security Index
Abbreviations
- CES-D
Center for Epidemiologic Studies Depression Scale
- CI
confidence interval
- FSI
Food Security Index
- TSI
Transportation Security Index
Transportation is an important social determinant of health (1), enabling people to access nutritious food (2, 3), seek medical care (4, 5), and obtain needed medication (6, 7), including the coronavirus disease 2019 (COVID-19) vaccine (8). Conversely, difficulties with transportation contribute to social isolation (9), with adverse consequences for mental and physical health (10, 11).
Despite the well-recognized interaction between transportation and health, research investigating this relationship has been stymied by the absence of a single concept and measure with which to compare findings across populations and health outcomes (for an overview, see Syed et al. (12)). Therefore, Gould-Werth et al. (13) developed and validated (14) the Transportation Security Index (TSI), a measure that captures transportation insecurity: a condition in which a person is unable to regularly move from place to place in a safe or timely manner due to the absence of resources for transportation. Modeled after the Food Security Index (FSI) (15), the TSI directly measures transportation insecurity at the individual level by asking respondents how often in the past 30 days they have experienced 16 different symptoms of transportation insecurity.
To date, the TSI has been used to document the prevalence of transportation insecurity nationwide and by subgroup. One in 4 adults in the United States experiences transportation insecurity, with the prevalence of insecurity being especially high among persons living below the poverty line (16) and those with disabilities (17). In a future clinical trial, Sung et al. (18) plan to use the TSI as an assessment tool to evaluate medication adherence among human immunodeficiency virus (HIV) patients who inject drugs.
The initial development of the TSI resulted in a continuous measure derived from the 16 items; however, a categorical measure would also be useful, for multiple reasons. First, categorical measures can assess nonparametric (i.e., noncontinuous) relationships between transportation insecurity and health outcomes. Second, a categorical measure can help clinicians who wish to screen for transportation barriers to health care and refer patients to supportive social services (19, 20). Screeners have become critical tools with which to identify and address social determinants of health in care settings, especially since policies have devoted funding and reimbursement for these tools (21, 22). Indeed, through its categorization into 4 qualitatively meaningful categories, the FSI has been used to great effect in precisely these ways (23, 24).
In this paper, we propose a categorization of the TSI with 5 categories. We evaluate categories using both inductive mixed-methods and k-means clustering approaches. The synthesis of these methods leads to a final 5-category categorization that is supported by both quantitative and qualitative evidence. We use this categorical measure to estimate associations between transportation insecurity and 2 health outcomes: self-rated health and depressive symptoms. Our results demonstrate that the categorical TSI can provide new insights into patterns of nonparametric associations that would be difficult to identify using continuous measures.
METHODS
We used data on transportation insecurity and health conditions from a module included in a nationally representative survey administered by GfK SE (Nuremberg, Germany) to their online panel (“KnowledgePanel”) in 2018. GfK is a global marketing research company (www.gfk.com) that recruits panel members using probability-based sampling and an address-based sampling frame; panel members are provided with access to the Internet and hardware if necessary. Panel members are assigned to specific study samples based on the study’s sampling design and then invited to complete the survey. GfK compensates participants using an ongoing incentive program which includes special raffles and sweepstakes with cash rewards.
Sample
The sampling frame was noninstitutionalized adults aged 25 years or over who resided in the United States; adults with a household income at or below 100% of the federal poverty level were oversampled. Although 2,447 panel members completed the survey (completion rate = 52.9%), only 2,011 met the study’s eligibility criteria (for a description, see Murphy et al. (14)), and another 12 were excluded from the final analysis (n = 1,999) because they did not complete all 16 items that comprise the TSI. To ensure a nationally representative analytical sample, GfK weighted the data to account for unequal probabilities of inclusion and differential nonresponse. As illustrated in Table 1, the weighted survey data aligned closely with the 2018 Current Population Survey.
Table 1.
Characteristics of Survey Respondents in a Study of Categories of Transportation Insecurity and Their Associations With Health Conditions (n = 1,999), United States, 2018a
| Characteristic | Unweighted % | Weighted % | No. of Persons | CPS Benchmark, % |
|---|---|---|---|---|
| Race/ethnicity | ||||
| White | 67.5 | 65.5 | 1,351 | 64.8 |
| Black | 12.3 | 11.5 | 246 | 11.6 |
| Hispanic | 12.4 | 14.9 | 249 | 15.4 |
| Other | 7.6 | 8.1 | 153 | 8.2 |
| Age group, years | ||||
| 25–39 | 29.3 | 28.9 | 585 | 30.0 |
| 40–64 | 49.4 | 50.2 | 987 | 46.6 |
| ≥65 | 21.4 | 20.9 | 427 | 23.4 |
| Sex | ||||
| Male | 48.6 | 47.7 | 971 | 48.2 |
| Female | 51.4 | 52.3 | 1,028 | 51.8 |
| Education | ||||
| Less than high school | 10.4 | 10.2 | 208 | 10.2 |
| High school | 31.2 | 29.0 | 623 | 28.5 |
| Some college | 31.9 | 26.6 | 638 | 26.3 |
| Bachelor’s degree or more | 26.5 | 34.2 | 530 | 34.9 |
| Household income, dollars/year | ||||
| ≤15,000 | 36.6 | 8.3 | 732 | 9.1 |
| 15,001–29,999 | 10.5 | 10.2 | 209 | 13.0 |
| 30,000–49,999 | 9.9 | 16.4 | 199 | 18.4 |
| 50,000–74,999 | 11.8 | 17.2 | 235 | 19.1 |
| ≥75,000 | 31.2 | 48.0 | 624 | 40.5 |
| FPL status | ||||
| ≤100% of FPL | 41.9 | 9.1 | 837 | 11.8 |
| 101%–200% of FPL | 11.2 | 19.3 | 223 | 17.6 |
| >200% of FPL | 46.9 | 71.6 | 939 | 70.6 |
| Children | ||||
| No | 70.7 | 69.7 | 1,414 | 69.7 |
| Yes | 29.3 | 30.3 | 585 | 30.3 |
Abbreviations: CPS, Current Population Survey; FPL, federal poverty level; TSI, Transportation Security Index.
a Mean TSI score = 3.823 (standard deviation, 6.488); possible range of TSI sum scores, 0–32.
Questionnaire
The questionnaire consisted of 136 items, including the 16-item TSI, and took respondents 23 minutes to complete, on average. The TSI asks respondents how often they have experienced 16 unique symptoms of transportation insecurity (see Web Table 1, available at https://doi.org/10.1093/aje/kwad145). Responses are given on a 3-point scale: never (0), sometimes (1), and often (2); thus, the simple sum score of the TSI ranges from 0 to 32. The questionnaire also included 2 items that provide further information about a respondent’s transportation situation: 1) a single-item self-report that asked how often the respondent experienced transportation insecurity and 2) an open-ended question about problems getting from place to place (see Web Table 1).
Additionally, the questionnaire included items measuring 2 different health conditions. The first variable was a single measure of self-rated health (“In general, how would you rate your health?”—excellent, very good, good, fair, or poor) that has been shown to be correlated with mortality and morbidity (25, 26). Responses were dichotomized into fair/poor versus excellent/very good/good. The second variable was a 7-item version of the validated Center for Epidemiologic Studies Depression Scale (CES-D) (27). Depressive symptoms may relate to transportation insecurity via restricted access to social support and greater social isolation (10, 11), a major predictor of depression (28). CES-D scores range from 0 to 21. Based on a standard cutoff, we dichotomized scores into depressive symptoms (CES-D score ≥9 = 1) versus no symptoms (CES-D score <9 = 0).
Analytical approach
There is no universally accepted method for determining category boundaries (see, for example, the 2002 US Department of Agriculture report (29)). Indeed, as Busch (30) illustrates, there are any number of approaches that can be taken to identify cutpoints. Therefore, following Busch’s advice (30), we sought to balance the tradeoff between losing information and gaining interpretability while keeping in mind the specific context within which the measure will be used. Although we used the FSI as our model to develop the TSI, unlike the FSI (31), the TSI does not exhibit Guttman-like properties such that items scale hierarchically by severity. Therefore, unli ke the FSI, we could not categorize the TSI based on item content alone. Instead, we used as our initial input the continuous scale defined as the sum of TSI item responses (i.e., TSI sum score).
To identify groups of respondents with similar response patterns (i.e., categorize the continuous TSI), we analyzed the unweighted data using 2 complementary approaches. Our first approach was inductive and involved triangulating between analyses of 4 sources of quantitative and qualitative data: 1) TSI sum scores, 2) responses to the 16 individual items in the TSI, and responses from 3) the self-report and 4) the open-ended item. We began by evaluating the distribution of self-responses within and across each of the 32 TSI sum scores to determine whether there were clusters (i.e., categories) of respondents who reported never, sometimes, or often experiencing transportation insecurity. Next, we sought to validate these preliminary categories. To do so, we first examined whether patterns of endorsement across the 16 items of the TSI were similar within categories and different between categories. We then assessed how respondents described their qualitative experiences with transportation insecurity in the open-ended item to confirm that experiences were similar within (and different between) categories.
Our second approach examined the data using k-means clustering. K-means clustering is a purely quantitative, nondeterministic partitional clustering method that clusters observations into k mutually exclusive and exhaustive categories (32). Using each observation’s unweighted continuous TSI sum score as input, the initial k group means are defined as the TSI sum score of k randomly selected observations. Each observation is then assigned to the group with the mean continuous 16-item TSI sum score closest to its own based on Euclidian (or Minkowski) distance. Once all of the observations have been assigned to a group, each group’s mean value is recalculated. The process repeats until group assignment does not change between iterations. We desired to identify a k that provided as much description of the population as could be generally reproduced; thus, we fitted each model 10 times and selected the solution that was generated a majority of the time. Cutpoints were then defined as the range of TSI sum scores within each of the k groups. These analyses were conducted in Stata 15.1 (33). See the Web Appendix for additional details.
After arriving at a final categorization scheme, we used logistic regression models to assess the associations with health conditions by transportation insecurity category, accounting for a standard set of demographic controls: age (<25, 25–39, 40–64, or ≥65 years), sex (male or female), race/ethnicity (Black non-Hispanic, Hispanic, White non-Hispanic, or other non-Hispanic), annual household income (≤$15,000, $15,001–$29,999, $30,000–$49,999, $50,000–$74,999, or ≥$75,000), level of educational attainment (less than high school, high school, some college, or bachelor’s degree or higher), and marital status (married, widowed, divorced, separated, never married, or living with a partner). All models were weighted to be nationally representative of the US adult population using the “survey” package in R software (34).
RESULTS
Inductive mixed-methods approach
We began by examining the distribution of transportation insecurity sum scores and considering how various scores correlated with the qualitative information provided by respondents and their direct self-reports of transportation insecurity. Using the single self-report measure of transportation insecurity, 77.95% of respondents reported never experiencing transportation insecurity, 16.17% reported experiencing it sometimes, and 5.88% reported experiencing it often. Among the 955 respondents (47.8%) with a TSI sum score greater than or equal to 1, 59.6% reported never experiencing transportation insecurity, 28.6% reported experiencing it sometimes, and 11.7% reported experiencing it often.
Figure 1 shows the unweighted distribution of self-reported transportation insecurity by a respondent’s TSI sum score for respondents with sum scores greater than 0 (less than 1% (0.7%) of respondents with sum scores of 0 or 1 reported experiencing insecurity). Just under 10% of all respondents (n = 181) had a score of 1, meaning they answered “sometimes” to a single item, and 5% of respondents (n = 106) had a sum score of 2, most of whom (91%) answered “sometimes” twice. Affirmative responses all related to time (items labeled as “late,” “took longer,” and “early” in Web Table 1), and no respondents with sum scores of 1 or 2 indicated that transportation was a barrier to getting where they need to go in open-ended responses. Most problems involved traffic (e.g., “The ONLY problem is horrendous traffic in Los Angeles!”). A small percentage (2%) expressed mild stress (e.g., “Traffic and long-distance driving are stressful to me”), but the stress did not prevent them from regularly moving between places in a safe or timely manner. Taken together, we felt confident categorizing respondents with scores of 0, 1, and 2 as being transportation-secure.
Figure 1.
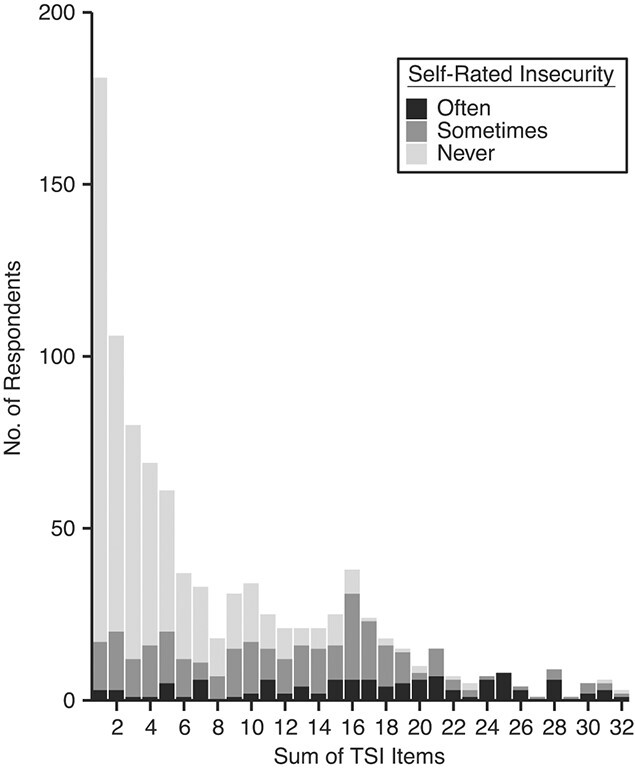
Self-rated level of transportation insecurity by Transportation Security Index (TSI) sum score, United States, 2018. The figure shows the unweighted distribution of respondents with self-reported transportation insecurity by respondent’s TSI sum score for persons with scores greater than 1 (n = 939) in the 2018 GfK KnowledgePanel (GfK SE, Nuremberg, Germany).
Among the 149 respondents with TSI sum scores of 3 or 4, 17.4% reported “sometimes” experiencing transportation insecurity, compared with 10% among those with scores of 1 or 2. Only 6% described worrying about car repairs and breakdowns or relying on backup transportation in their open-ended responses, and none indicated that transportation prevented them from getting around despite these problems. Only 2 respondents among those with a score of 3 (n = 80) or 4 (n = 69) reported experiencing transportation insecurity “often,” and, in open-ended responses, they both indicated that they could satisfactorily get where they needed to go. Thus, although respondents with scores of 3 or 4 were more likely to sometimes experience insecurity relative to those with scores of less than 3, they were still able to get around.
Among respondents with scores of 5 (n = 61), 13% reported “often” experiencing transportation insecurity and 25% reported “sometimes” experiencing insecurity. These values were higher than those from respondents with scores of 3 and 4, yet the open-ended responses indicated similar experiences with transportation: worrying about their car breaking down but still being able to access essential destinations, like work. As a result, we grouped respondents with scores of 5 with respondents with scores of 3 and 4. Respondents with scores of 3–5 were qualitatively different from those we categorized as “transportation-secure” because they were inconvenienced by transportation and experienced transportation-related worry, so we classified this group as experiencing marginal insecurity.
Respondents with scores of 6 or more clearly experienced transportation insecurity that affected their daily lives. We classified this next group of respondents, those having scores of 6–10, as experiencing low insecurity. Unlike respondents in the marginal insecurity group, respondents in the low insecurity group reported having constrained travel. For example, one respondent with a score of 6 wrote, “I don’t go out very much to save money, so I usually go to places close to me by walking. I only take public transportation a few times a month by depositing $20 to my half fare Metro Card.” Among persons in this low insecurity group, 34% reported that they “sometimes” experienced transportation insecurity in the self-report question, and only 6.5% reported “often” experiencing transportation insecurity.
We classified respondents with scores of 11–16 as experiencing moderate insecurity. Among persons in this group, 17% reported “often” experiencing transportation insecurity. Respondents with scores of 11 or greater were also more likely to affirm items that measured negative feelings about their transportation. For instance, whereas fewer than 1% (n = 9) of those experiencing low insecurity reported “often” feeling bad because of transportation, 17% of those with scores of 11–16 reported “often” having such feelings. Open-ended responses conveyed similar sentiments. One respondent with a score of 11 described feeling embarrassed because they drove a vehicle in need of repairs which they could not afford, writing, “I traveled less, felt embarrassed because of the noise and safety concern. I can’t afford a car payment plus full coverage insurance. Life is hard.”
Figure 1 shows a sizeable jump in respondents with a score of 16. Just over half (56%) of these respondents answered “sometimes” to all 16 questions Among the 22 respondents who answered “sometimes” to all 16 items, 5 reported “never” experiencing transportation insecurity, 15 reported “sometimes,” and 1 reported “often.” We suspect that some of these respondents may have “straightlined” answers and not considered them individually (35), especially those who reported “never” experiencing transportation insecurity in the single self-report item. At the same time, it was clear that respondents with scores of 16 did experience moderate problems with transportation. For instance, among the 17 respondents with scores of 16 who did not answer “sometimes” to all 16 items, 5 reported “often” experiencing transportation insecurity and 10 reported experiencing it “sometimes.” Similarly, their open-ended responses revealed difficulties accessing reliable transportation and constrained travel, with one person writing, “My car has serious problems, and I cannot afford to pay for them. I have no friends who drive. I use Medicaid-provided transportation for doctor’s visits.” Thus, while we interpreted values of 16 cautiously, we classified these respondents as experiencing moderate insecurity.
Finally, we determined that those with scores of 17 or greater experienced high insecurity. Among respondents in this group, 44% (n = 61) reported “often” experiencing transportation insecurity, more than double the share of respondents in the moderate-insecurity group. Furthermore, respondents with scores of 17 or greater were more likely to describe either not being able to go places at all or being severely limited in the places they could go in their open-ended responses. For example, one respondent (score of 24) wrote, “We have no vehicle here, so we all have to walk or ride the bus everywhere; it has really made getting a job difficult.” Another (score of 17) wrote, “There are many restrictions on when, where, and for how long I can get out.” Such difficulty getting to places was also evident in how this group endorsed items on the TSI that tap into constrained travel behavior compared with those with lower scores. For example, whereas only 8% (n = 12) of respondents with scores of 11–16 reported that they were “often” not able to leave the house, nearly half (49%) of respondents with scores of 17 or higher (n = 67) reported “often” having this experience.
In sum, this approach suggested the following 5-category categorization of TSI sum scores: no insecurity/secure = 0–2; marginal insecurity = 3–5; low insecurity = 6–10; moderate insecurity = 11–16; and high insecurity = 17–32.
K-means clustering approach
Table 2 illustrates the range of TSI sum scores observed for each of the 3, 4, 5, or 6 groups identified across each of the 10 iterations of the k-means clustering models. Because we used k-means clustering to identify internal consistency, we did not use weighted data for these analyses. For both the k = 6 and k = 5 models, among the 10 iterations, there were 5 unique solutions of which 3 and 4 of those solutions, respectively, occurred more than once. In the k = 4 model, one of the 10 solutions replicated 6 times (with 4 solutions appearing 1 time each), and in the k = 3 model, one solution replicated 8 times and a second replicated twice.
Table 2.
Transportation Security Index Sum Scores by K-Means Clustering Solution, United States, 2018a
| K-Means Clustering Solution | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| k = 6 | k = 5 | k = 4 | k = 3 | |||||||||||||||
|
Iteration
No. |
1 | 2 | 3 | 4 | 5 | 6 | 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 1 | 2 | 3 |
| 1 | 0–1 | 2–3 | 4–7 | 8–13 | 14–20 | ≥21 | 0 | 1–2 | 3–7 | 8–15 | ≥16 | 0–2 | 3–7 | 8–15 | ≥16 | 0–3 | 4–12 | ≥13 |
| 2 | 0–1 | 2–3 | 4–7 | 8–13 | 14–20 | ≥21 | 0 | 1–2 | 3–7 | 8–15 | ≥16 | 0–2 | 3–7 | 8–15 | ≥16 | 0–3 | 4–12 | ≥13 |
| 3 | 0–1 | 2–3 | 4–7 | 8–13 | 14–20 | ≥21 | 0 | 1–2 | 3–7 | 8–15 | ≥16 | 0–2 | 3–7 | 8–15 | ≥16 | 0–3 | 4–12 | ≥13 |
| 4 | 0 | 1–2 | 3–6 | 7–12 | 13–20 | ≥21 | 0 | 1–2 | 3–7 | 8–15 | ≥16 | 0–2 | 3–7 | 8–15 | ≥16 | 0–3 | 4–12 | ≥13 |
| 5 | 0 | 1–2 | 3–6 | 7–12 | 13–20 | ≥21 | 0–1 | 2–4 | 5–10 | 11–19 | ≥20 | 0–2 | 3–7 | 8–15 | ≥16 | 0–3 | 4–12 | ≥13 |
| 6 | 0 | 1–2 | 3–6 | 7–12 | 13–20 | ≥21 | 0–1 | 2–4 | 5–10 | 11–19 | ≥20 | 0–2 | 3–7 | 8–15 | ≥16 | 0–3 | 4–12 | ≥13 |
| 7 | 0 | 1 | 2–4 | 5–10 | 11–19 | ≥20 | 0–1 | 2–4 | 5–10 | 11–19 | ≥20 | 0–2 | 3–9 | 10–18 | ≥19 | 0–3 | 4–12 | ≥13 |
| 8 | 0 | 1 | 2–4 | 5–10 | 11–19 | ≥20 | 0–1 | 2–6 | 7–13 | 14–22 | ≥23 | 0–3 | 4–10 | 11–19 | ≥20 | 0–3 | 4–12 | ≥13 |
| 9 | 0 | 1–2 | 3–6 | 7–12 | 13–21 | ≥22 | 0–2 | 3–6 | 7–12 | 13–20 | ≥21 | 0–4 | 5–11 | 12–20 | ≥21 | 0–4 | 5–13 | ≥14 |
| 10 | 0–1 | 2–4 | 5–10 | 11–17 | 18–23 | ≥24 | 0–2 | 3–7 | 8–13 | 14–20 | ≥21 | 0–4 | 5–12 | 13–21 | ≥22 | 0–4 | 5–13 | ≥14 |
a For ease of interpretation, clustering solutions have been rearranged so that identical solutions are adjacent.
We ruled out k = 6 and k = 5 solutions because none were replicated across the majority of iterations. The k = 3 solution replicated 8 times but was less descriptive—especially at the most insecure end of the distribution—than the k = 4 solution, which still replicated across the majority (n = 6) of iterations. We thus identified the following categories of transportation insecurity with the k-means approach: no insecurity/secure = 0–2; low insecurity = 3–7; moderate insecurity = 8–15; and high insecurity = 16–32.
Selecting the final categorization
Table 3 shows that the 2 methods of categorizing transportation insecurity demonstrated similar patterns, especially in how they categorized the most extreme points (highest and lowest sum scores). Both approaches identified the most secure respondents as those with scores between 0 and 2, leading us to retain the category of secure/no insecurity for persons with these scores. However, the two approaches differed in terms of the number of categories identified (5 vs. 4) and the different distributions of sum scores across those categories.
Table 3.
Proposed Categorization of Transportation Insecurity Using the 16-Item Transportation Security Index
| Categorization Method | TSI Sum Score |
|---|---|
| Mixed methods | |
| Secure | 0–2 |
| Marginal insecurity | 3–5 |
| Low insecurity | 6–10 |
| Moderate insecurity | 11–16 |
| High insecurity | ≥17 |
| K-means clustering | |
| Secure | 0–2 |
| Marginal insecurity | |
| Low insecurity | 3–7 |
| Moderate insecurity | 8–15 |
| High insecurity | ≥16 |
| Final categorization | |
| Secure | 0–2 |
| Marginal insecurity | 3–5 |
| Low insecurity | 6–10 |
| Moderate insecurity | 11–16 |
| High insecurity | ≥17 |
Abbreviation: TSI, Transportation Security Index.
While one approach identified the least secure (high insecurity) respondents as those with scores greater than 16 (k-means clustering approach), the other identified the least secure respondents as those with scores greater than 17 (mixed-methods approach). Since the quantitative solution may have been influenced by “straightlining,” and because of a marked qualitative difference between persons with scores of 16 and those with scores of 17, we followed the recommendation of the mixed-methods approach and defined high insecurity as scores of 17 and above.
Table 3 shows that the other difference between the two solutions was the categorization of the intermediate points. Our mixed-methods approach categorized persons with scores between 3 and 16 into 3 groups (3–5, 6–10, and 11–16), whereas the k-means clustering approach separated those with scores between 3 and 15 into 2 groups (3–7 and 8–15). The mixed-methods approach provided compelling evidence that persons with scores of 3–5 were qualitatively different from those with scores of 6–10 in that while they worried about transportation, unlike those with scores of 6–10, they were able to regularly get to their destinations. The mixed-methods approach provided similarly compelling evidence that persons with scores of 6–10 were qualitatively different from those with scores of 11–16: Respondents with scores between 6 and 10 were much less likely to report “often” experiencing transportation insecurity and were less likely to endorse items suggesting that they experienced negative feelings because of their transportation insecurity—findings supported by their open-ended responses as well. Given the strength of the evidence that suggested that the marginal, low, and moderate insecurity categories held meaningful qualitative distinctions, we retained these 3 categories in our final TSI categorization. This led us to a final categorization of the TSI that included 5 categories, as recommended by the mixed-methods approach (illustrated in Table 3).
Associations between transportation insecurity and health conditions
Table 4 shows the predicted odds ratios for poor self-rated health and depressive symptoms for individuals experiencing transportation insecurity at marginal, low, moderate, and high levels compared with those who were not transportation-insecure. Models showed that the continuous TSI variable was associated with worse conditions for both outcome variables (see Web Table 2). Results using the categorical variable showed that modeling a linear association may be misleading. Results predicting poor health revealed a threshold effect: All 4 categories of transportation insecurity were associated with higher odds of being in poor health, with similar magnitudes. The odds ratios ranged between 1.94 (95% confidence interval (CI): 1.16, 3.24) and 2.71 (95% CI: 1.33, 5.53)—differences that cannot be distinguished from sampling variation. The results suggest a step function where poor health is higher among people with any amount of transportation insecurity than among those with no transportation insecurity, but there are no differences between people with different levels of transportation insecurity.
Table 4.
Odds Ratios for Associations Between Transportation Insecurity and Health Conditions, United States, 2018
| Health Measure | ||||
|---|---|---|---|---|
|
Poor Self-Rated Health
a
(n = 1,989 Observations) |
Depressive Symptoms
b
(n = 1,946 Observations) |
|||
| Variable | OR | 95% CI | OR | 95% CI |
| Level of transportation insecurity | ||||
| None/transportation-secure | 1.00 | Referent | 1.00 | Referent |
| Marginal | 1.94 | 1.16, 3.24 | 0.71 | 0.38, 1.32 |
| Low | 2.60 | 1.52, 4.47 | 1.89 | 0.99, 3.59 |
| Moderate | 1.97 | 1.06, 3.67 | 3.19 | 1.70, 5.97 |
| High | 2.71 | 1.33, 5.53 | 12.22 | 6.37, 23.45 |
| Household income, dollars/year | ||||
| ≤15,000 | 1.00 | Referent | 1.00 | Referent |
| 15,001–29,999 | 0.43 | 0.27, 0.70 | 0.71 | 0.40, 1.25 |
| 30,000–49,999 | 0.67 | 0.43, 1.07 | 0.79 | 0.45, 1.37 |
| 50,000–74,999 | 0.37 | 0.23, 0.61 | 0.51 | 0.28, 0.92 |
| ≥75,000 | 0.25 | 0.15, 0.40 | 0.49 | 0.29, 0.84 |
| Age group, years | ||||
| 25–39 | 1.00 | Referent | 1.00 | Referent |
| 40–64 | 1.48 | 0.97, 2.25 | 0.58 | 0.39, 0.85 |
| ≥65 | 2.17 | 1.35, 3.47 | 0.48 | 0.29, 0.79 |
| Highest level of education | ||||
| Less than high school | 1.00 | Referent | 1.00 | Referent |
| High school | 0.71 | 0.43, 1.16 | 0.97 | 0.53, 1.78 |
| Some college | 0.47 | 0.28, 0.81 | 0.85 | 0.46, 1.58 |
| Bachelor’s degree or higher | 0.40 | 0.23, 0.71 | 0.51 | 0.26, 0.99 |
| Race/ethnicity | ||||
| Black non-Hispanic | 1.00 | Referent | 1.00 | Referent |
| Hispanic | 0.89 | 0.47, 1.68 | 1.67 | 0.80, 3.50 |
| Other non-Hispanic | 0.81 | 0.34, 1.92 | 1.71 | 0.73, 4.02 |
| White non-Hispanic | 1.00 | 0.59, 1.68 | 1.38 | 0.71, 2.68 |
| Marital status | ||||
| Not married | 1.00 | Referent | 1.00 | Referent |
| Married | 0.65 | 0.45, 0.95 | 0.94 | 0.64, 1.38 |
| Sex | ||||
| Male | 1.00 | Referent | 1.00 | Referent |
| Female | 0.80 | 0.58, 1.11 | 1.41 | 0.99, 2.01 |
Abbreviations: AIC, Akaike information criterion; CI, confidence interval; OR, odds ratio.
a AIC = 1,602.
b AIC = 1,457.
The risk of depressive symptoms exhibited a nonlinear dose-response relationship with severity of transportation insecurity, with large variation in magnitudes across categories of transportation insecurity. Compared with transportation-secure individuals, the odds of experiencing depressive symptoms were 12.22 (95% CI: 6.37, 23.45) times higher among those with high transportation insecurity, 3.19 (95% CI: 1.70, 5.97) times higher among those with moderate insecurity, and 1.89 (95% CI: 0.99, 3.59) times higher among those with low insecurity. Persons with a marginal level of transportation insecurity were slightly less likely to experience depressive symptoms, but the result could not be distinguished from random sampling error (odds ratio = 0.71, 95% CI: 0.38, 1.32). These results reflect a sharp, nonlinear change in the influence of transportation insecurity on depressive symptoms.
DISCUSSION
We arrived at a 5-category TSI measure based on 2 distinct approaches: a mixed-methods approach and a quantitative k-means clustering approach. The categorical TSI distinguishes persons who experience no insecurity/are secure (sum scores ranging from 0 to 2), marginal insecurity (3–5), low insecurity (6–10), moderate insecurity (11–16), and high insecurity (17–32) from each other. These discrete categories distinguish qualitatively different degrees of transportation insecurity and have implications for understanding the relationship between transportation insecurity and health conditions. Indeed, we show sizeable, nonlinear associations between transportation insecurity and key health measures: poor self-rated health and depressive symptoms.
As with the findings derived from any survey, ours are dependent on a specific survey methodology and context, and their robustness hinges on their replicability in future studies. For example, although GfK takes care to provide its online panel members with access to the Internet and hardware if needed, future researchers might consider targeting hard-to-reach individuals, including those without Internet access or those lacking technological literacy. Future researchers might also try to replicate these findings using other modes of survey administration, such as paper or interview modes.
As discussed above, we expect that some degree of “straightlining” may have occurred in responses. However, we suspect that the number of respondents who straightlined answers was empirically small in our sample. Further, our multimethod approach allowed us to ward off potential straightlining bias. Specifically, our approach enabled us to observe that persons with scores of 16 were qualitatively different from those with scores of 17, something the k-means clustering method alone could not detect. Thus, to the extent that straightlining occurred, we do not believe this skewed our final categorization.
Finally, the practice of categorization is fundamentally one of data reduction that, by definition, results in the loss of information. However, that information is only useful if the continuous distributions are linear in their parameters to outcome variables of interest. We found that not to be the case. The log odds of both self-rated health and depressive symptoms were associated with categorical differences in transportation insecurity. Yet these were only 2 health measures. As health scholars continue to investigate the role that transportation plays as a social determinant of health, the categorical TSI will be a useful tool for exploring the association between categorical differences in transportation insecurity and additional health conditions, especially those that require a high level of management. Such research may be especially timely given the focus on equity in funding of federal infrastructure projects in the current US administration—projects which include investigations into interventions that reduce transportation insecurity (36).
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Department of Sociology, College of Literature, Science, and the Arts, University of Michigan, Ann Arbor, Michigan, United States (Karina McDonald-Lopez, Alexandra K. Murphy, Jamie Griffin); Washington Center for Equitable Growth, Washington, DC, United States (Alix Gould-Werth); Department of Sociology, Zanvyl Krieger School of Arts and Sciences, Johns Hopkins University, Baltimore, Maryland, United States (Michael D. M. Bader); and Gerald R. Ford School of Public Policy, University of Michigan, Ann Arbor, Michigan, United States (Nicole Kovski).
This work was supported by the National Science Foundation (grant OIA09936884); the Stanford Center on Poverty and Inequality (grant H79AE000101 from the US Department of Health and Human Services); and the University of Michigan’s Poverty Solutions and Mcity initiatives, College of Literature, Science, and the Arts, Office of Research, and Department of Sociology.
Data are not available to the public.
We thank Dr. David Pedulla for his feedback on an earlier draft of this paper and are grateful to Dr. Lydia Wileden for her assistance in gathering Current Population Survey benchmark data.
Any opinions, findings, and conclusions or recommendations expressed in this article are those of the author(s) and do not necessarily reflect the views or official policies of the National Science Foundation or the US Department of Health and Human Services.
Conflict of interest: none declared.
REFERENCES
- 1. Artiga S, Hinton E. Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity. Menlo Park, CA: Henry J. Kaiser Family Foundation; 2018. https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/. Accessed May 9, 2023. [Google Scholar]
- 2. Morland K, Wing S, Diez Roux AV, et al. Neighborhood characteristics associated with the location of food stores and food service places. Am J Prev Med. 2002;22(1):23–29. [DOI] [PubMed] [Google Scholar]
- 3. Walker RE, Keane CR, Burke JG. Disparities and access to healthy food in the United States: a review of food deserts literature. Health Place. 2010;16(5):876–884. [DOI] [PubMed] [Google Scholar]
- 4. Wallace R, Hughes-Cromwick P, Mull H, et al. Access to health care and nonemergency medical transportation: two missing links. Trans Res Rec. 2005;1924(1):76–84. [Google Scholar]
- 5. Chaiyachati KH, Hubbard RA, Yeager A, et al. Association of rideshare-based transportation services and missed primary care appointments: a clinical trial. JAMA Intern Med. 2018;178(3):383–389. [DOI] [PubMed] [Google Scholar]
- 6. Tierney WM, Harris LE, Gaskins DL, et al. Restricting Medicaid payments for transportation: effects on inner-city patients’ health care. Am J Med Sci. 2000;319(5):326–333. [DOI] [PubMed] [Google Scholar]
- 7. Kripalani S, Henderson LE, Jacobson TA, et al. Medication use among inner-city patients after hospital discharge: patient-reported barriers and solutions. Mayo Clin Proc. 2008;83(5):529–535. [DOI] [PubMed] [Google Scholar]
- 8. Liu D, Kwan MP, Kan Z, et al. Racial/ethnic inequity in transit-based spatial accessibility to COVID-19 vaccination sites. J Racial Ethn Health Disparities. 2023;10:1533–1541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Dobbs B, Hussey E, Pidborochynksi T. Transportation mobility and social isolation in community-dwelling older adults. Innov Aging. 2018;2(1):448. [Google Scholar]
- 10. Cacioppo JT, Cacioppo S. Social relationships and health: the toxic effects of perceived social isolation. Soc Personal Psychol Compass. 2014;8(2):58–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Alcaraz KI, Eddens KS, Blase JL, et al. Social isolation and mortality in US black and white men and women. Am J Epidemiol. 2018;188(1):102–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Syed ST, Gerber BS, Sharp LK. Traveling towards disease: transportation barriers to health care access. J Community Health. 2013;38(5):976–993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Gould-Werth A, Griffin J, Murphy AK. Developing a new measure of transportation insecurity: an exploratory factor analysis. Surv Pract. 2018;11(2):3706–3734. [Google Scholar]
- 14. Murphy AK, Gould-Werth A, Griffin J. Validating the sixteen-item Transportation Security Index in a nationally representative sample: a confirmatory factor analysis. Surv Pract. 2021;14(1):1–17. [Google Scholar]
- 15. Frongillo EA Jr. Validation of measures of food insecurity and hunger. J Nutr. 1999;129(2 suppl):506S–509S. [DOI] [PubMed] [Google Scholar]
- 16. Murphy AK, McDonald-Lopez K, Pilkauskas N, et al. Transportation insecurity in the United States: a descriptive portrait. Socius. 2022;8(10):23780231221121060. [Google Scholar]
- 17. Vallas R, Knackstedt K, Brown H, et al. Economic Justice Is Disability Justice. New York, NY: The Century Foundation; 2022. https://tcf.org/content/report/economic-justice-disability-justice/. Accessed May 9, 2023. [Google Scholar]
- 18. Sung ML, Viera A, Esserman D, et al. Contingency Management and Pre-Exposure Prophylaxis Adherence Support Services (CoMPASS): a hybrid type 1 effectiveness-implementation study to promote HIV risk reduction among people who inject drugs. Contemp Clin Trials. 2023;125:107037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Buitron de la Vega P, Losi S, Martinez LS, et al. Implementing an EHR-based screening and referral system to address social determinants of health in primary care. Med Care. 2019;57(suppl 2):S133–S139. [DOI] [PubMed] [Google Scholar]
- 20. Chaiyachati KH, Krause D, Sugalski J, et al. A survey of the National Comprehensive Cancer Network on approaches toward addressing patients’ transportation insecurity. J Natl Compr Canc Netw. 2023;21(1):21–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Beck AF, Cohen AJ, Colvin JD, et al. Perspectives from the Society for Pediatric Research: interventions targeting social needs in pediatric clinical care. Pediatr Res. 2018;84(1):10–21. [DOI] [PubMed] [Google Scholar]
- 22. Fraze TK, Brewster AL, Lewis VA, et al. Prevalence of screening for food insecurity, housing instability, utility needs, transportation needs, and interpersonal violence by US physician practices and hospitals. JAMA. 2019;2(9):e1911514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Seligman HK, Jacobs E, López A, et al. Food insecurity and glycemic control among low-income patients with type 2 diabetes. Diabetes Care. 2012;35(2):233–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Aff (Millwood). 2015;34(11):1830–1839. [DOI] [PubMed] [Google Scholar]
- 25. DeSalvo KB, Bloser N, Reynolds K, et al. Mortality prediction with a single general self-rated health question. J Gen Intern Med. 2006;21(3):267–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Latham K, Peek CW. Self-rated health and morbidity onset among late midlife U.S. adults. J Gerontol B Psychol Sci Soc Sci. 2013;68(1):107–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. [Google Scholar]
- 28. Choi H, Irwin MR, Cho HJ. Impact of social isolation on behavioral health in elderly: systematic review. World J Psychiatry. 2015;5(4):432–438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Nord M, Bickel G. Measuring Children's Food Security in U.S. Households, 1995-99. (Food Assistance and Nutrition Research Report no. 25). Washington, DC: Food and Rural Economics Division, Economic Research Service, US Department of Agriculture; 2002. https://www.ers.usda.gov/publications/pub-details/?pubid=46624. Accessed August 4, 2023. [Google Scholar]
- 30. Busch EL. Cut points and contexts. Cancer. 2021;127(23):4348–4355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Food and Consumer Service, US Department of Agriculture . Household Food Security in the United States in 1995: Summary Report of the Food Security Measurement Project .Alexandria, VA: US Department of Agriculture; 1997. https://www.fns.usda.gov/household-food-security-united-states-1995-summary-report-food-security-measurement-project. Accessed May 9, 2023. [Google Scholar]
- 32. MacQueen J. Some methods for classification and analysis of multivariate observations. In: Le Cam LM, ed. Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability. Berkeley, CA: University of California Press; 1967:281–297. [Google Scholar]
- 33. StataCorp LLC . Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC; 2017. [Google Scholar]
- 34. Lumley T. survey: Analysis of Complex Survey Samples. (Version 4.0). https://cran.r-project.org/web/packages/survey/index.html. Published 2020. Accessed January 2, 2023.
- 35. Krosnick JA, Narayan S, Smith WR. Satisficing in surveys: initial evidence. New Dir Eval. 1996;1996(70):29–44. [Google Scholar]
- 36. Federal Transit Administration, US Department of Transportation . Federal Transit Administration announces funding to explore transportation insecurity that leads to poverty. https://www.transit.dot.gov/about/news/federal-transit-administration-announces-funding-explore-transportation-insecurity-leads. Published February 8, 2023. Accessed May 9, 2023.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.