

Abstract
Eosinophilic cystitis is a rare inflammatory disorder of the bladder, characterized by eosinophilic infiltration of the bladder wall, fibrosis of the mucosa, and muscle necrosis. Ultrasonography, when performed, shows a pseudotumoral mass that can be mistaken for malignancy. We report a case of a woman referred to our department in which an ultrasound showed a bladder mass and the biopsy demonstrated the presence of eosinophilic cystitis. The patient was treated with medical treatment and the outcome was favorable with the disappearance of symptoms and no recurrence at controls. We carry a literature review of cystitis eosinophilic, the ultrasound appearance, and therapeutic modalities.
Keywords: Eosinophilic cystitis, Bladder tumor, Diagnosis, Treatment
Introduction
Eosinophilic cystitis is a rare inflammatory disorder of the bladder, first described independently by Brown [1] and Palubinskas [2] in 1960. Eosinophilic cystitis is a histological diagnosis characterized by eosinophilic infiltration of the bladder wall, fibrosis of the mucosa, and muscle necrosis. The incidence is not known and it is present in all ages, without prevalence of sex and ethnicity. The aetiology is not clear. Van den Ouden reported a mild prevalence of allergy, asthma, and transitional cell carcinoma of the bladder between the most reported aetiological factors [3]. The most common symptoms of presentation are dysuria, hematuria, and pain. Ultrasonography, when performed, can show a pseudotumoral mass that can be mistaken for malignancy. [4] Cystoscopy with bladder biopsy is the most important procedure for its diagnosis. Diagnosis is confirmed via biopsy with histologic examination [5]. Therapy often involves corticosteroids, antihistamines, and nonsteroidal anti-inflammatory drugs [6], but sometimes it requires surgical treatment [7].
Case report
A 77-year-old woman was referred to our ultrasound laboratory from the emergency room for haematuria. She had a history of stroke and carotid stenosis. Laboratory showed anemia (RG 3.36 × 106 mL, Hb 9.1 g/dL) with normal coagulation. Urine cytology showed no malignant cells. Ultrasound showed a thickened bladder wall with a 22 mm tumor on the left side of the wall (Fig. 1). There was no hydronephrosis. Cystoscopy under anesthesia was then performed, showing diffuse urothelial erythema, with a mass in the posterior bladder wall. At biopsy pathological examination described an edematous and erythematous urothelial mucosa with a prominent eosinophilic infiltrate mixed with lymphocytes and neutrophilic granulocytes deep within the muscolaris propria (Fig. 2). The final diagnosis was eosinophilic cystitis. The outcome was favorable with no symptoms. A computed tomography scan performed 6 months after as control showed the absence of tumoral mass.
Fig. 1.
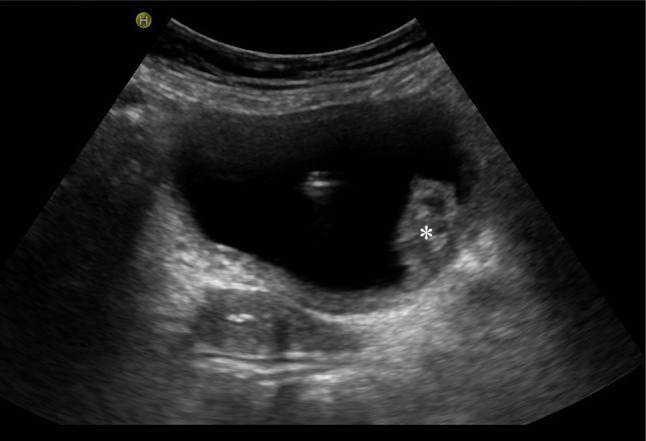
US transverse scan of the bladder shows a thickened bladder wall with a 22 mm parietal mass on the left side (asterisk). A catheter is present
Fig. 2.

Histologic specimen shows a prominent eosinophilic infiltrate mixed with lymphocytes and neutrophilic granulocytes deep within the muscularis propria, resulting in a diagnosis of eosinophilic cystitis
Discussion
Eosinophilic cystitis is a rare inflammatory condition of the bladder. Although no clear cause has been determined, previous reports have associated eosinophilic cystitis with allergenic status, bacterial infections, parasites, medications, and other medical conditions [8, 9]. The most common clinical symptoms include dysuria, hematuria, urinary frequency, urgency, and suprapubic pain. Investigations include ultrasound and cystoscopy.
Ultrasound is often nonspecific, showing marked thickening of the bladder wall, eventually with a focal pseudotumoral mass, leading to a diagnosis of bladder cancer. Cystoscopy showed an inflamed mucosa with ulceration and necrosis. In the case of polypoid mass, a malignant tumor is considered and a biopsy is performed. The diagnosis is made by histopathologic confirmation of diffuse, transmural infiltration of eosinophils throughout the bladder wall. The patient in this case presented with gross hematuria. Initial ultrasound showed a bladder tumor, confirmed by cystoscopy. Bladder biopsy revealed up to 80 eosinophils per HPF, consistent with severe eosinophilic cystitis.
No standard therapeutic protocol has been established for eosinophilic cystitis. A wide variety of medical regimens have been reported, including antibiotics, antihistamines, corticosteroids (oral and intravesical), and nonsteroidal anti-inflammatory drugs. Although eosinophilic cystitis is a benign disease, it may progress to a diffuse and aggressive form [10] that does not respond to medical management and may impair both lower and upper urinary tract functions requiring surgical treatment, with a partial or total cystectomy [7].
In this particular case, treatment with oral fluconazole resulted not only in symptomatic relief but also in resolution of the underlying eosinophilic cystitis upon post-treatment bladder biopsy.
Conclusion
Pseudotumoral eosinophilic cystitis is a challenging pathology that mimics bladder cancer. The diagnosis is possible only after the histological examination. Eosinophilic cystitis is equally distributed among the sexes with the main presenting symptoms of frequency, dysuria, hematuria, suprapubic pain, and urinary retention. In the majority of patients, the course of eosinophilic cystitis is usually benign and accompanied by a successful outcome with conservative therapy, however, cases of aggressive behavior with extension to the whole of the bladder or to the adjacent structures are also reported. The frequency of recurrence and the tendency to chronicity require close monitoring. Medical treatment is the first line (corticosteroids, NSAIDs, cotrimoxazole, DMSO, or immunosuppressants), combined with transurethral resection of the lesions. In case of failure, cystectomy seems a preferable alternative to partial surgery.
Funding
The authors have no relevant financial or non-financial interests to disclose.
Declarations
Conflicts of interest
The authors declare that they have no conflicts of interest related to this article.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Brown EW. Eosinophilic granuloma of the bladder. J Urol. 1960;83:665–668. doi: 10.1016/S0022-5347(17)65773-2. [DOI] [PubMed] [Google Scholar]
- 2.Palubinskas AJ. Eosinophilic cystitis. Case report of eosinophilic infiltration of the urinary bladder. Radiology. 1960;75:589–91. doi: 10.1148/75.4.589. [DOI] [PubMed] [Google Scholar]
- 3.van den Ouden D. Diagnosis and management of Eosinophilic cystitis: a pooled analysis of 135 cases. Eur Urol. 2000;37(4):386–394. doi: 10.1159/000020183. [DOI] [PubMed] [Google Scholar]
- 4.Saadi A, Bouzouita A, Ayed H, Kerkeni W, Cherif M, Ben Slama RM, Derouiche A, Chebil M. Pseudotumoral Eosinophilic cystitis. Urol Case Rep. 2015;3(3):65–67. doi: 10.1016/j.eucr.2015.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Popescu OE, Landas SK, Haas GP. The spectrum of Eosinophilic cystitis in males: case series and literature review. Arch Pathol Lab Med. 2009;133(2):289–294. doi: 10.5858/133.2.289. [DOI] [PubMed] [Google Scholar]
- 6.Zaman SR, Vermeulen TL, Parry J. Eosinophilic cystitis: treatment with intravesical steroids and oral antihistamines. BMJ Case Rep. 2013 doi: 10.1136/bcr-2013-009327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rossanese M, Palumbo V, Sioletic S, Crestani A, Giannarini G, Ficarra V. Surgical treatment of Eosinophilic cystitis in adults: a report of two cases and a literature review. Urol Int. 2019;102(1):122–124. doi: 10.1159/000485257. [DOI] [PubMed] [Google Scholar]
- 8.Hellstrom HR, Davis BK, Shonnard JW. Eosinophilic cystitis. A study of 16 cases. Am J Clin Pathol. 1979;72(5):777–84. doi: 10.1093/ajcp/72.5.777. [DOI] [PubMed] [Google Scholar]
- 9.Mosholt KS, Dahl C, Azawi NH. Eosinophilic cystitis: three cases, and a review over 10 years. BMJ Case Rep. 2014 doi: 10.1136/bcr-2014-205708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Itano NM, Malek RS. Eosinophilic cystitis in adults. J Urol. 2001;65(3):805–807. doi: 10.1016/S0022-5347(05)66531-7. [DOI] [PubMed] [Google Scholar]