

Abstract
BACKGROUND:
Long QT syndrome (LQTS) is a heterogeneous syndrome that may be congenital or, more frequently, acquired. The real-world prevalence of acquired LQTS (aLQTS) in the emergency department (ED) remains to be determined. The aim of this study was to determine prevalence of aLQTS and its impact on symptoms on ED admissions.
METHODS:
Electrocardiograms (ECG) of 5,056 consecutively patients admitted in the ED of a tertiary hospital between January 28th and March 17th of 2020 were reviewed. All patients with aLQTS were included. Clinical data with a focus on QT prolonging drugs and clinical factors were recorded. Statistical comparison was made between the groups with and without corrected QT (QTc) interval greater than 500 ms (value that is considered severely increased).
RESULTS:
A total of 383 ECGs with prolonged QTc were recognized, corresponding to a prevalence of aLQTS at admission of 7.82%. Patients with aLQTS were more commonly men (53.3%) with an age of (73.49±14.79) years old and QTc interval of (505.3±32.4) ms. Only 20.4% of these patients with aLQTS were symptomatic. No ventricular arrhythmias were recorded. Patients with QT interval greater than 500 ms were more frequently female (59.5%; P<0.001) and were more frequently on QT prolonging drugs (77.3%; P=0.025). Main contributing factor was intake of antibiotics (odds ratio [OR] 4.680) followed by female gender (OR 2.473) and intake of antipsychotics (OR 1.925).
CONCLUSION:
aLQTS is particularly prevalent in the ED. Female patients on antibiotics and antipsychotics are at particularly high risk. Efforts must be made to avoid, detect and treat aLQTS as early as possible.
Keywords: Long QT syndrome, Epidemiology, Drug interactions, Emergency department
INTRODUCTION
Long QT syndrome (LQTS) is a heterogeneous syndrome that may be congenital or acquired,[1] the latter being more common.[2] It is defined as a prolonged corrected QT (QTc) interval in the electrocardiogram (ECG) with values greater than 470 ms in men and 480 ms in women.[3] Values higher than 500 ms are considered severe for both sexes and indicate a particularly high risk for torsades de pointes (TdP) or polymorphic ventricular tachycardia (pVT).[3,4] An increase >60 ms from the QTc baseline is also considered an alarming sign.[5] pVT and TdP may present with syncope, cardiac arrest or sudden cardiac death (SCD). Timely diagnosis and treatment are crucial to prevent them.[4,6]
Risk factors for acquired LQTS (aLQTS) include female sex, advanced age, metabolic disorders, electrolyte imbalances and cardiac diseases (acute coronary syndromes and myocarditis).[7-9] The most common cause of prolongation of the QT interval is drug-related. A wide range of different drug classes influence repolarization, including class IA antiarrhythmics,[8] class III antiarrhythmics,[7] fluoroquinolones, macrolides, antifungals, antipsychotics, antidepressants, H1 antihistamine and anticholinergics.[8,10-16]
The real-world prevalence of aLQTS remains to be determined, and specific data regarding its prevalence in the emergency department (ED) is largely unknown. Additionally, this syndrome includes a heterogeneous group of patients who lacks better analysis.
Previous studies reported a prevalence between 28.5%–35% in the ED for QT prolongation, both acquired and hereditary.[17-20] Also, approximately 25% of the patients admitted to cardiac intensive care units (ICUs) had prolonged QTc intervals at admission[3] and 20%–24% had severely prolonged QTc intervals when admitted to any ICU.[21,22] The prevalence of QTc interval greater than 500 ms in other hospital wards was 0.7%–0.9%.[23,24]
Our aim was to determine the prevalence of aLQTS in patients admitted to the ED and to characterize the subset of patients at particularly high risk of TdP (patients with QTc>500 ms).
METHODS
Study design and patient selection
We performed a retrospective study of consecutive patients admitted to the ED of a tertiary hospital between the 28th of January and 17th of March 2020 (prepandemic period in Portugal).
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Local Ethics Committee (OBS.SF.23/2021). Due to the observational aspect of this study, informed consent was waived.
Patient eligibility criteria
Patients were eligible for inclusion if they had an ECG with a prolonged QTc interval using Bazett’s formula (greater than 470 ms in men and 480 ms in women as defined by the American Heart Association and American College of Cardiology Foundation).[3]
Exclusion criteria were the following: 1) congenital LQTS or known relative with LQTS; 2) repeated ED admissions; 3) bad ECG quality; 4) atrial fibrillation (AF) /atrial flutter; and 5) pacemaker rhythm.
Data collection
Variables retrieved were age, sex, clinical presentation (palpitations, presyncope, syncope, seizure or cardiac arrest) and QT prolonging drugs or with known risk of TdP and risk factors contributing to prolonged QT interval as determined by CredibleMeds® (an online resource that promotes the safe use of medicines).[8] QTc was determined using the Bazett’s formula and uncorrected QT interval as measured manually by the main researchers using the average of three measurements.
Drugs were grouped according to drug class: antiarrhythmics, antibiotics, antihistamines, antiemetics, antifungal, immunomodulators, opioids, antipsychotics, antidepressants, diuretics, anti-migraine, bronchodilators, hormones, proton-pump inhibitors (PPIs) and others.
Study endpoints
The primary endpoint was to determine the prevalence of aLQTS and its impact on symptoms at admission to the ED.
The secondary endpoints focused on determining risk factors for a severely prolonged QT interval defined as values greater than 500 ms. [3]
Data analysis
Statistical analysis was performed using IBM SPSS Statistics version 26. Categorical variables are presented as frequencies and percentages, and continuous variables as means and standard deviations if normally distributed, or as medians and interquartile ranges for variables with skewed distributions. Normal distribution was verified through the Kolmogorov-Smirnov test or skewness and kurtosis (maximum tolerated interval of -1 to 1).
Bivariate analysis was performed by using Chi-square test (or Fisher exact test as appropriate) for categorical variables with a Bonferroni correction for multiple analyses and independent t-test for continuous variables. Using logistic regression, odds ratio (OR) were determined for the variables with P <0.100. All reported P values are two-tailed with values less than 0.05 indicating statistical significance. The authors had full access to data and take full responsibility for its integrity.
RESULTS
A total of 6,280 ECGs were identified. These ECGs belonged to 5,056 patients. A total of 1,380 ECGs were subsequently excluded. No patients with a prior diagnosis of LQTS were identified. The final sample comprised 2,573 women and 2,327 men. A total of 383 ECGs with prolonged QTc were recognized (Figure 1). The total prevalence of aLQTS was 7.82%.
Figure 1.

Flowchart of ECG selection. ECG: electrocardiogram; AF: atrial fibrillation.
Patients with aLQTS were more commonly men (n=204; 53.3%) with an average age of 73.49 ± 14.79 years old (range 19–95 years) and average QTc interval of 505.3 ± 32.4 ms (range 470–680 ms). The majority of patients were asymptomatic (79.6%) and the most common symptom was syncope (39/78) followed by presyncope (22/78). No TdP or pVT were documented. Baseline characteristics and risk factors are shown in Table 1. Diuretics, PPIs, antidepressants, and antipsychotics were among the classes most frequently present in patients with prolonged QT (Table 2).
Table 1.
Baseline characteristics and risk factors of the studied population
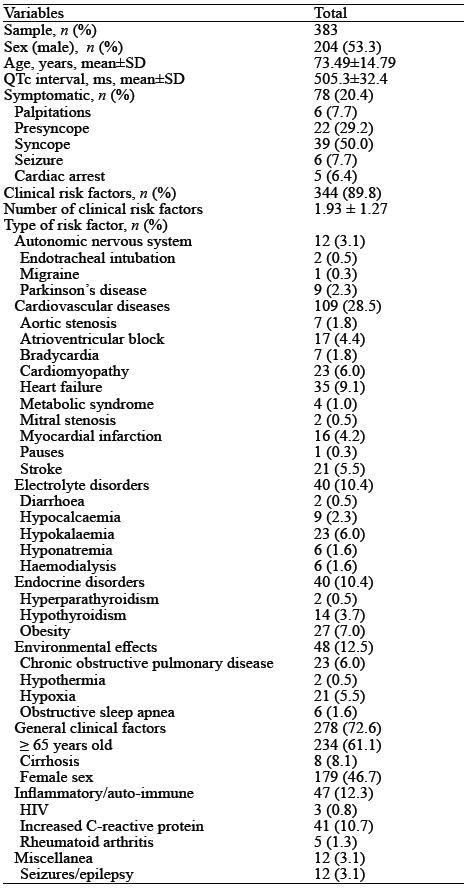
Table 2.
Patients on QT prolonging drugs

Subgroup analysis of patients with severely prolonged QTc interval (>500 ms)
There were 163 patients with severely prolonged QTc intervals (> 500 ms), corresponding to a prevalence of 3.3% (and 42.6% of the overall aLQTS group).
Female patients (59.5%; P<0.001) and patients on QT prolonging drugs (77.3%; P=0.025) were more likely to have a severely prolonged QTc interval (Table 3). Additionally, the use of a greater number of drugs and particularly, intake of antibiotics (P=0.004), antipsychotics (P=0.014) or antidepressants (P=0.028) were associated with severely prolonged QTc interval (Table 3). There was also a trend for prolonged QTc intervals in patients on diuretics (P=0.051) (Table 3). Of note, although the mean number of risk factors was greater in the population with severely prolonged QTc intervals, the difference was not statistically significant (P=0.055) (Table 3). No statistically significant differences were found regarding age, clinical presentation or type of risk factors present.
Table 3.
Comparison between patients with and without severely prolonged QTc interval

Using logistic regression, patients on antibiotics had the greatest odds of severely prolonged QTc interval (OR 4.860; 95% confidence interval (95% CI) 1.497–14.631; P=0.008). Female patients had almost 2.5 times greater odds of severely prolonged QTc (OR 2.473; 95% CI 1.663–3.747; P< 0.001). The remaining ORs are shown on Table 4.
Table 4.
Logistic analysis of the risk factors of severely prolonged QTc interval

DISCUSSION
Acquired LQTS is an often-overlooked entity that lacks better understanding and study. Previous studies estimate that the prevalence of LQTS in the ED is 30%–40%.[17–20] Our results show that this syndrome is particularly common in this setting, even when accounting only for patients with a severely prolonged QTc. Similar to other studies, we detected that these were mainly older patients (73.49±14.79 years).[2,25] Of note, the great majority of patients in this study had no symptoms that could draw attention to LQTS. As such, careful evaluation of the QT interval is key, even in asymptomatic patients, as it may be the only sign detected before a dysrhythmic event and death.
Regarding drugs contributing to this syndrome, most interact with the hERG gene and the IKr channel.[26] In this study, and in contrast to previous studies where antiarrhythmics had the spotlight,[2,25] diuretics (and in particular, furosemide) were the drugs most commonly associated with LQTS in our emergency population. In addition to contributing to ionic imbalance, furosemide may lead to QT prolongation even when corrected for low serum levels of calcium and potassium.[27] We hypothesize that the high prevalence of these drugs in our population reflects advanced age and the fact that heart failure and hypertension are particularly frequent in the ED setting.
The second most prescribed drug class in this population was PPIs, mainly pantoprazole. Its impact is mainly due to decreased absorption of magnesium and consequent hypomagnesaemia and not by directly prolonging QT.[28,29] This effect is particularly magnified in the presence of diuretics.[28]
Antipsychotropic medication also plays a crucial role in a large subset of patients.[30] Antidepressants (selective serotonin reuptake inhibitor [SSRI] but also tricyclic drugs) are increasingly prescribed and used chronically.[31] The main mechanism for QT prolongation appears to be Na+ channel blockage in tricyclic agents and inhibition of the IKr channel in SSRIs.[14] Their impact on the QT interval demands a careful risk-benefit analysis prior to their initiation and in every hospital appointment, [32,33] as excessive dosage or co-administration with other drugs such as K+ channel blockers may lead to a devastating effect.[14,34] Regarding antipsychotics, their impact has long been studied and is mainly mediated by hERG channel blockade.[35] Nearly all antipsychotics cause QT prolongation[32] but particular attention needs to be given to patients on haloperidol, thioridazine, pimozide, ziprasidone, risperidone, melperone, and quetiapine, as they are known to prolong QT the most.[34]
Also of note are antibiotics. Macrolides and fluoroquinolones are increasingly utilized in clinical practice as beta-lactam resistance surges. Similar to SSRIs, blockade of the IKr channel is the main contributor to QT prolongation.[14,30,36] In addition, CYP3A4 inhibition by macrolides can also increase the half-life and concentration of other QT prolonging drugs and dramatically increase QTc.[14]
Classically regarded as the main culprits of prolonged QT, antiarrhythmics were found in only a small proportion of our sample. Nonetheless, the same channel blocking capabilities responsible for their antiarrhythmic effect contribute to QT prolongation and TdP.[14,30,37] As such, careful ECG monitoring, especially in class IA (quinidine, procainamide and disopyramide) and class III agents (such as amiodarone and sotalol), is needed to maintain a tight control of the clinical status.[14]
Regarding clinical risk factors, our study showed that patients with elevated C-reactive protein more frequently had LQTS in the ED. Recent studies have shown that the inflammatory pathway affects the electrophysiological properties of cardiomyocytes, contributing to changes in repolarization and consequent QT prolongation.[38] Heart failure was also particularly prevalent in our study population. Multiple mechanisms have also been hypothesized to contribute to QT prolongation in heart failure, including structural changes and heterogeneous depolarization, in addition to the effect of drug iatrogenesis.[39,40] Hypokalemia is also a determinant factor in prolonging QT. Its impact on the functioning of potassium channels leads to synergy with the inhibiting properties of QT prolonging drugs and a marked increase in the risk of ventricular fibrillation (VF) and TdP.[41]
A QT interval greater than 500 ms has been linked to an increased risk of ventricular arrhythmias and complications.[3,24] Our study demonstrated that female patients on antibiotics were at an increased risk of severely prolonged QT interval. Other particularly relevant contributors to this severely prolonged QTc were the number of QT prolonging drugs, clinical risk factors, and the use of antipsychotics and antidepressants. Studies have shown that antipsychotics and antidepressants are being prescribed at a particularly high and increasing rate in recent years, particularly in elderly patients.[42–44] In fact, most recent national studies found an increasing trend for overall polypharmacy in the elderly, reaching in some cases a general prevalence of 8%–29%.[45–48] This fact leads not only to increased direct costs in healthcare systems, but also to a greater risk of drug and clinical factor interactions. Accordingly, careful monitoring of baseline and follow-up ECG in this therapeutic setting is crucial to avoid severe QT prolongation.
Despite the increased risk of TdP, the direct correlation between QT prolongation and clinical presentation remains to be fully determined.[7,24] Our study showed no link between a severely prolonged QT interval and symptoms.
Limitations
Our study was retrospective and unicentric which may have led to bias in the sample selection and increased the probability of the presence of confounders. Other factors contributing to QT prolongation such as race and socioeconomic status were not evaluated due to the lack of reporting on the clinical data used. Additionally, it was impossible to ascertain the prognostic influence of aLQTS during follow-up and correction using Bazett’s formula may overcorrect the QT interval at higher heart rates.
CONCLUSION
In conclusion, aLQTS is particularly prevalent in the ED setting. The complex interaction of clinical factors and drug iatrogenesis and the unpredictability of its manifestations render its management and recognition difficult but essential. Efforts must be made to raise clinicians’ awareness to avoid, detect and treat aLQTS as early as possible.
Footnotes
Funding: The authors did not receive support from any organization for the submitted work.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee of Centro Hospitalar e Universitário de Coimbra (OBS.SF.23/2021).
Conflicts of interest: The authors have no relevant financial or non-financial interests to disclose.
Author contribution: DAF and GC contributed equally to the work and are co-first authors. Conception and design of study: DAF, GC, DMF, CQ; Acquisition of data: DAF, GC, DMF, CQ; Analysis and/or interpretation of data: DAF, GC, DMF, CQ; Drafting the manuscript: DAF, GC, DMF, CQ; Revising the manuscript critically for important intellectual content: CFR, LG, RP, NA; Approval of the version of the manuscript to be published: DAF, GC, DMF, CQ, CFR, LG, RP, NA.
REFERENCES
- 1.Aerssens J, Paulussen AD. Pharmacogenomics and acquired long QT syndrome. Pharmacogenomics. 2005;6(3):259–70. doi: 10.1517/14622416.6.3.259. [DOI] [PubMed] [Google Scholar]
- 2.Sarganas G, Garbe E, Klimpel A, Hering RC, Bronder E, Haverkamp W. Epidemiology of symptomatic drug-induced long QT syndrome and torsade de pointes in Germany. Europace. 2014;16(1):101–8. doi: 10.1093/europace/eut214. [DOI] [PubMed] [Google Scholar]
- 3.Drew BJ, Ackerman MJ, Funk M, Gibler WB, Kligfield P, Menon V, et al. Prevention of torsade de pointes in hospital settings:a scientific statement from the American Heart Association and the American College of Cardiology Foundation. J Am Coll Cardiol. 2010;55(9):934–47. doi: 10.1016/j.jacc.2010.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Barra S, Agarwal S, Begley D, Providência R. Post-acute management of the acquired long QT syndrome. Postgrad Med J. 2014;90(1064):348–58. doi: 10.1136/postgradmedj-2013-132398. [DOI] [PubMed] [Google Scholar]
- 5.Ramalho D, Freitas J. Drug-induced life-threatening arrhythmias and sudden cardiac death:A clinical perspective of long QT, short QT and Brugada syndromes. Rev Port Cardiol (Engl Ed) 2018;37(5):435–46. doi: 10.1016/j.repc.2017.07.010. [DOI] [PubMed] [Google Scholar]
- 6.Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death:the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by:association for European Paediatric and Congenital Cardiology (AEPC) Eur Heart J. 2015;36(41):2793–867. doi: 10.1093/eurheartj/ehv316. [DOI] [PubMed] [Google Scholar]
- 7.Khan IA. Clinical and therapeutic aspects of congenital and acquired long QT syndrome. Am J Med. 2002;112(1):58–66. doi: 10.1016/s0002-9343(01)01011-7. [DOI] [PubMed] [Google Scholar]
- 8.QTdrugs List. Available at: www.CredibleMeds.org .
- 9.Rabkin SW. Impact of age and sex on QT prolongation in patients receiving psychotropics. Can J Psychiatry. 2015;60(5):206–14. doi: 10.1177/070674371506000502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jackman WM, Friday KJ, Anderson JL, Aliot EM, Clark M, Lazzara R. The long QT syndromes:a critical review, new clinical observations and a unifying hypothesis. Prog Cardiovasc Dis. 1988;31(2):115–72. doi: 10.1016/0033-0620(88)90014-x. [DOI] [PubMed] [Google Scholar]
- 11.Beitland S, Platou ES, Sunde K. Drug-induced long QT syndrome and fatal arrhythmias in the intensive care unit. Acta Anaesthesiol Scand. 2014;58(3):266–72. doi: 10.1111/aas.12257. [DOI] [PubMed] [Google Scholar]
- 12.Redfern WS, Carlsson L, Davis AS, Lynch WG, MacKenzie I, Palethorpe S, et al. Relationships between preclinical cardiac electrophysiology, clinical QT interval prolongation and torsade de pointes for a broad range of drugs:evidence for a provisional safety margin in drug development. Cardiovasc Res. 2003;58(1):32–45. doi: 10.1016/s0008-6363(02)00846-5. [DOI] [PubMed] [Google Scholar]
- 13.Thompson JL, Crossman RR. Drug-induced QT prolongation. US Pharmacist. 2007;32(2) [Google Scholar]
- 14.Nachimuthu S, Assar MD, Schussler JM. Drug-induced QT interval prolongation:mechanisms and clinical management. Ther Adv Drug Saf. 2012;3(5):241–53. doi: 10.1177/2042098612454283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Roden DM, Woosley RL, Primm RK. Incidence and clinical features of the quinidine-associated long QT syndrome:implications for patient care. Am Heart J. 1986;111(6):1088–93. doi: 10.1016/0002-8703(86)90010-4. [DOI] [PubMed] [Google Scholar]
- 16.Haverkamp W, Breithardt G, Camm AJ, Janse MJ, Rosen MR, Antzelevitch C, et al. The potential for QT prolongation and proarrhythmia by non-antiarrhythmic drugs:clinical and regulatory implications. Report on a policy conference of the European Society of Cardiology. Eur Heart J. 2000;21(15):1216–31. doi: 10.1053/euhj.2000.2249. [DOI] [PubMed] [Google Scholar]
- 17.Scheuermeyer FX, Innes G, Grafstein E, Chard R, Vandenberg S, Cheyne J, et al. Emergency department patients with a prolonged corrected QT interval do not have increased thirty-day mortality. Acad Emerg Med. 2019;26(7):818–22. doi: 10.1111/acem.13702. [DOI] [PubMed] [Google Scholar]
- 18.Seftchick MW, Adler PH, Hsieh M, Wolfson AB, Chan ST, Webster BW, et al. The prevalence and factors associated with QTc prolongation among emergency department patients. Ann Emerg Med. 2009;54(6):763–8. doi: 10.1016/j.annemergmed.2009.03.021. [DOI] [PubMed] [Google Scholar]
- 19.Vandenberk B, Siau C, Vandael E, Puype L, Branders J, Dewolf P, et al. A prolonged QTc-interval at the emergency department:should we always be prepared for the worst? J Cardiovasc Electrophysiol. 2019;30(10):2041–50. doi: 10.1111/jce.14114. [DOI] [PubMed] [Google Scholar]
- 20.Birda CL, Kumar S, Bhalla A, Sharma N, Kumari S. Prevalence and prognostic significance of prolonged QTc interval in emergency medical patients:a prospective observational study. Int J Crit Illn Inj Sci. 2018;8(1):28–35. doi: 10.4103/IJCIIS.IJCIIS_59_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tisdale JE, Wroblewski HA, Overholser BR, Kingery JR, Trujillo TN, Kovacs RJ. Prevalence of QT interval prolongation in patients admitted to cardiac care units and frequency of subsequent administration of QT interval-prolonging drugs:a prospective, observational study in a large urban academic medical center in the US. Drug Saf. 2012;35(6):459–70. doi: 10.2165/11598160-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 22.Pickham D, Helfenbein E, Shinn JA, Chan G, Funk M, Weinacker A, et al. High prevalence of corrected QT interval prolongation in acutely ill patients is associated with mortality:results of the QT in Practice (QTIP) Study. Crit Care Med. 2012;40(2):394–9. doi: 10.1097/CCM.0b013e318232db4a. [DOI] [PubMed] [Google Scholar]
- 23.Yu HX, Zhang L, Liu JQ, Liu Y, Kowey PR, Zhang YL, et al. Acquired long QT syndrome in hospitalized patients. Heart Rhythm. 2017;14(7):974–8. doi: 10.1016/j.hrthm.2017.03.014. [DOI] [PubMed] [Google Scholar]
- 24.Haugaa KH, Bos JM, Tarrell RF, Morlan BW, Caraballo PJ, Ackerman MJ. Institution-wide QT alert system identifies patients with a high risk of mortality. Mayo Clin Proc. 2013;88(4):315–25. doi: 10.1016/j.mayocp.2013.01.013. [DOI] [PubMed] [Google Scholar]
- 25.Molokhia M, Pathak A, Lapeyre-Mestre M, Caturla L, Montastruc JL, et al. L'Association Française des Centres Régionaux de Pharmacovigilance (CRPV). Case ascertainment and estimated incidence of drug-induced long-QT syndrome:study in Southwest France. Br J Clin Pharmacol. 2008;66(3):386–95. doi: 10.1111/j.1365-2125.2008.03229.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.El-Sherif N, Turitto G, Boutjdir M. Acquired long QT syndrome and electrophysiology of torsade de pointes. Arrhythm Electrophysiol Rev. 2019;8(2):122–30. doi: 10.15420/aer.2019.8.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Snitker S, Doerfler RM, Soliman EZ, Deo R, St Peter WL, Kramlik S, et al. Association of QT-prolonging medication use in CKD with electrocardiographic manifestations. Clin J Am Soc Nephrol. 2017;12(9):1409–17. doi: 10.2215/CJN.12991216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kieboom BCT, Kiefte-de Jong JC, Eijgelsheim M, Franco OH, Kuipers EJ, Hofman A, et al. Proton pump inhibitors and hypomagnesemia in the general population:a population-based cohort study. Am J Kidney Dis. 2015;66(5):775–82. doi: 10.1053/j.ajkd.2015.05.012. [DOI] [PubMed] [Google Scholar]
- 29.Hoorn EJ, van der Hoek J, de Man RA, Kuipers EJ, Bolwerk C, Zietse R. A case series of proton pump inhibitor-induced hypomagnesemia. Am J Kidney Dis. 2010;56(1):112–6. doi: 10.1053/j.ajkd.2009.11.019. [DOI] [PubMed] [Google Scholar]
- 30.Pourmand A, Mazer-Amirshahi M, Chistov S, Sabha Y, Vukomanovic D, Almulhim M. Emergency department approach to QTc prolongation. Am J Emerg Med. 2017;35(12):1928–33. doi: 10.1016/j.ajem.2017.08.044. [DOI] [PubMed] [Google Scholar]
- 31.Mars B, Heron J, Kessler D, Davies NM, Martin RM, Thomas KH, et al. Influences on antidepressant prescribing trends in the UK:1995-2011. Soc Psychiatry Psychiatr Epidemiol. 2017;52(2):193–200. doi: 10.1007/s00127-016-1306-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Beach SR, Celano CM, Sugrue AM, Adams C, Ackerman MJ, Noseworthy PA, et al. QT prolongation, torsades de pointes, and psychotropic medications:a 5-year update. Psychosomatics. 2018;59(2):105–22. doi: 10.1016/j.psym.2017.10.009. [DOI] [PubMed] [Google Scholar]
- 33.Beach SR, Kostis WJ, Celano CM, Januzzi JL, Ruskin JN, Noseworthy PA, et al. Meta-analysis of selective serotonin reuptake inhibitor-associated QTc prolongation. J Clin Psychiatry. 2014;75(5):e441–9. doi: 10.4088/JCP.13r08672. [DOI] [PubMed] [Google Scholar]
- 34.Wenzel-Seifert K, Wittmann M, Haen E. QTc prolongation by psychotropic drugs and the risk of torsade de pointes. Dtsch Arztebl Int. 2011;108(41):687–93. doi: 10.3238/arztebl.2011.0687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hasnain M, Vieweg WV, Howland RH, Kogut C, Breden Crouse EL, Koneru JN, et al. Quetiapine, QTc interval prolongation, and torsade de pointes:a review of case reports. Ther Adv Psychopharmacol. 2014;4(3):130–8. doi: 10.1177/2045125313510194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Volberg WA, Koci BJ, Su WG, Lin J, Zhou J. Blockade of human cardiac potassium channel human Ether-a-go-go-Related gene (HERG) by macrolide antibiotics. J Pharmacol Exp Ther. 2002;302(1):320–7. doi: 10.1124/jpet.302.1.320. [DOI] [PubMed] [Google Scholar]
- 37.Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart. 2003;89(11):1363–72. doi: 10.1136/heart.89.11.1363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lazzerini PE, Capecchi PL, Laghi-Pasini F. Long QT syndrome:an emerging role for inflammation and immunity. Front Cardiovasc Med. 2015;2:26. doi: 10.3389/fcvm.2015.00026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Davey PP, Bateman J, Mulligan IP, Forfar C, Barlow C, Hart G. QT interval dispersion in chronic heart failure and left ventricular hypertrophy:relation to autonomic nervous system and Holter tape abnormalities. Br Heart J. 1994;71(3):268–73. doi: 10.1136/hrt.71.3.268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Breidthardt T, Christ M, Matti M, Schrafl D, Laule K, Noveanu M, et al. QRS and QTc interval prolongation in the prediction of long-term mortality of patients with acute destabilised heart failure. Heart. 2007;93(9):1093–7. doi: 10.1136/hrt.2006.102319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.El-Sherif N, Turitto G. Electrolyte disorders and arrhythmogenesis. Cardiol J. 2011;18(3):233–45. [PubMed] [Google Scholar]
- 42.Luo Y, Kataoka Y, Ostinelli EG, Cipriani A, Furukawa TA. National prescription patterns of antidepressants in the treatment of adults with major depression in the US between 1996 and 2015:a population representative survey based analysis. Front Psychiatry. 2020;11:35. doi: 10.3389/fpsyt.2020.00035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jonson M, Sigström R, Hedna K, Rydberg Sterner T, Falk Erhag H, Wetterberg H, et al. Time trends in depression prevalence among Swedish 85-year-olds:repeated cross-sectional population-based studies in 1986, 2008, and 2015. Psychol Med. 2023;53(6):2456–65. doi: 10.1017/S0033291721004335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hálfdánarson Ó, Zoëga H, Aagaard L, Bernardo M, Brandt L, Fusté AC, et al. International trends in antipsychotic use:a study in 16 countries, 2005-2014. Eur Neuropsychopharmacol. 2017;27(10):1064–76. doi: 10.1016/j.euroneuro.2017.07.001. [DOI] [PubMed] [Google Scholar]
- 45.Oktora MP, Denig P, Bos JHJ, Schuiling-Veninga CCM, Hak E. Trends in polypharmacy and dispensed drugs among adults in the Netherlands as compared to the United States. PLoS One. 2019;14(3):e0214240. doi: 10.1371/journal.pone.0214240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Moriarty F, Hardy C, Bennett K, Smith SM, Fahey T. Trends and interaction of polypharmacy and potentially inappropriate prescribing in primary care over 15 years in Ireland:a repeated cross-sectional study. BMJ Open. 2015;5(9):e008656. doi: 10.1136/bmjopen-2015-008656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Nishtala PS, Salahudeen MS. Temporal trends in polypharmacy and hyperpolypharmacy in older New Zealanders over a 9-year period:2005-2013. Gerontology. 2015;61(3):195–202. doi: 10.1159/000368191. [DOI] [PubMed] [Google Scholar]
- 48.Onoue H, Koyama T, Zamami Y, Hagiya H, Tatebe Y, Mikami N, et al. Trends in polypharmacy in Japan:a nationwide retrospective study. J Am Geriatr Soc. 2018;66(12):2267–73. doi: 10.1111/jgs.15569. [DOI] [PubMed] [Google Scholar]