
Figure 4. Subgroup Analysis of the Primary End Point (Primary Analysis Population).
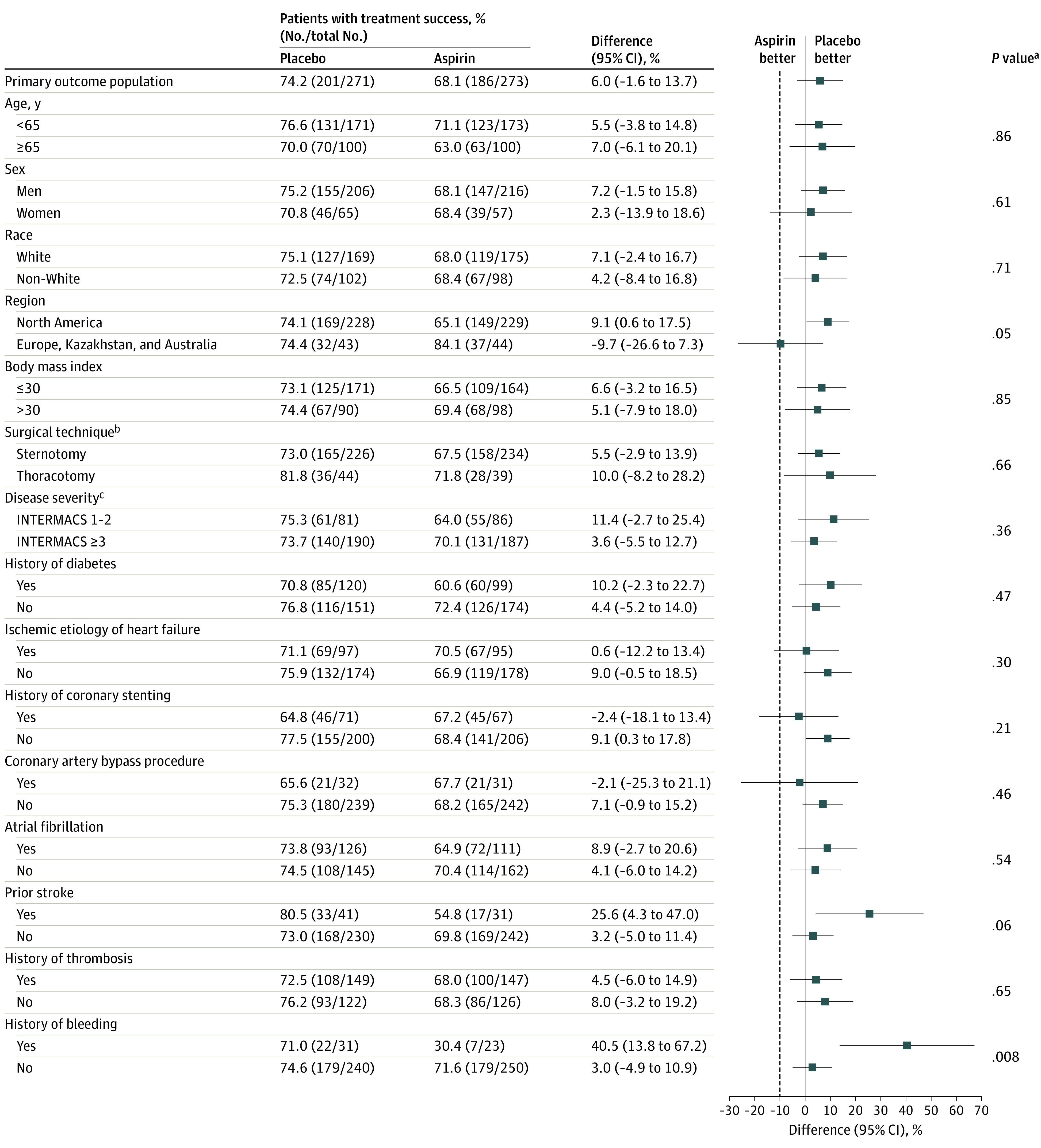
There were no significant interactions on the primary end point for most subgroups, including age, sex, race and ethnicity, obesity, disease severity, history of diabetes, ischemic etiology of heart failure, history of coronary stenting, thrombosis history, history of atrial fibrillation, coronary artery bypass surgery, or left ventricular assist device (LVAD) surgical implant method. Patients with a history of bleeding or stroke were noted to experience more benefit from aspirin avoidance. The dashed line represents the noninferiority margin of −10% for the success difference.
aInteraction testing of primary end point subgroups was completed by general linearized modeling with terms for treatment group, subgroup, and their interaction.
bSurgical techniques include sternotomy, referring to full median sternotomy, and thoracotomy, referring to left thoracotomy combined with right thoracotomy or hemisternotomy.
cDisease severity defined by Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) profiles, which range from 1 to 7; a profile of 1 represents the most severe illness and a profile of 7 the least severe illness.