

This prespecified analysis of the Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure (DELIVER) randomized clinical trial investigates the association of initial changes in estimated glomerular filtration rate with cardiovascular and kidney outcomes in patients with heart failure and mildly reduced or preserved ejection fraction.
Key Points
Question
What is the association of initial changes in estimated glomerular filtration rate (eGFR) with cardiovascular and kidney outcomes among patients with heart failure and mildly reduced ejection fraction (HFmrEF) or preserved ejection fraction (HFpEF)?
Findings
Among 5788 participants of the Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure (DELIVER) trial, an initial eGFR decline of greater than 10% (vs ≤10%) was frequent and associated with a higher risk of the primary cardiovascular outcome among those randomized to placebo but not among those randomized to dapagliflozin. An initial eGFR decline greater than 10% was not associated with adverse kidney outcomes among dapagliflozin-treated patients.
Meaning
These data suggest, among patients with HFmrEF or HFpEF, that sodium-glucose cotransporter-2 inhibitors should not be discontinued in response to an initial eGFR decline.
Abstract
Importance
An initial decline in estimated glomerular filtration rate (eGFR) is expected after initiating a sodium-glucose cotransporter-2 inhibitor (SGLT2i) and has been observed across patients with diabetes, chronic kidney disease, and heart failure.
Objective
To examine the implications of initial changes in eGFR among patients with heart failure with mildly reduced ejection fraction (HFmrEF) or preserved ejection fraction (HFpEF) enrolled in the Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure (DELIVER) trial.
Design, Setting, and Participants
This was a prespecified analysis of the results of the DELIVER randomized clinical trial, which was an international multicenter study of patients with EF greater than 40% and eGFR greater than or equal to 25. The DELIVER trial took place from August 2018 to March 2022. Data for the current prespecified study were analyzed from February to October 2023.
Intervention
Dapagliflozin, 10 mg per day, or placebo.
Main Outcomes and Measures
In this prespecified analysis, the frequency of an initial eGFR decline (baseline to month 1) was compared between dapagliflozin and placebo. Cox models adjusted for baseline eGFR and established prognostic factors were fit to estimate the association of an initial eGFR decline with cardiovascular (cardiovascular death or heart failure event) and kidney (≥50% eGFR decline, eGFR<15 or dialysis, death from kidney causes) outcomes, landmarked at month 1, stratified by diabetes.
Results
Study data from 5788 participants (mean [SD] age, 72 [10] years; 3253 male [56%]) were analyzed. The median (IQR) change in eGFR level from baseline to month 1 was −1 (−6 to 5) with placebo and −4 (−9 to 1) with dapagliflozin (difference, −3; P < .001). A higher proportion of patients assigned to dapagliflozin developed an initial eGFR decline greater than 10% vs placebo (1144 of 2892 [40%] vs 737 of 2896 [25%]; odds ratio, 1.9; 95% CI, 1.7-2.1; P difference <.001). An initial eGFR decline of greater than 10% (vs ≤10%) was associated with a higher risk of the primary cardiovascular outcome among those randomized to placebo (adjusted hazard ratio [aHR], 1.33; 95% CI, 1.10-1.62) but not among those randomized to dapagliflozin (aHR, 0.90; 95% CI, 0.74-1.09; P for interaction = .01). Similar associations were observed when alternative thresholds of initial eGFR decline were considered and when analyzed as a continuous measure. An initial eGFR decline of greater than 10% was not associated with adverse subsequent kidney composite outcomes in dapagliflozin-treated patients (aHR, 0.94; 95% CI, 0.49-1.82).
Conclusions and Relevance
Among patients with HFmrEF or HFpEF treated with dapagliflozin, an initial eGFR decline was frequent but not associated with subsequent risk of cardiovascular or kidney events. These data reinforce clinical guidance that SGLT2is should not be interrupted or discontinued in response to an initial eGFR decline.
Trial Registration
ClinicalTrials.gov Identifier: NCT03619213
Introduction
Over the past several years, the sodium-glucose cotransporter-2 inhibitors (SGLT2is) have significantly altered the clinical treatment of patients with type 2 diabetes (T2D),1,2 chronic kidney disease (CKD),1,3,4,5 and heart failure,6,7,8,9,10 with large outcomes trials demonstrating major risk reductions in cardiovascular and kidney outcomes and, in some circumstances, death.
The major pharmacologic action of SGLT2is involves the inhibition of sodium and glucose reabsorption in proximal tubule cells of the kidney, leading to glycosuria, natriuresis, and reduction of intraglomerular pressure.11,12 As such, and similar to that observed with renin-angiotensin system inhibitors, the initiation of SGLT2is is often accompanied by an acute initial decline in estimated glomerular filtration rate (eGFR) that may be observed clinically. Although this has been shown to be reversible upon SGLT2i withdrawal in some studies,13,14 concerns remain that such acute functional changes in eGFR may lead to inappropriate drug cessation, thus preventing patients from benefiting from long-term risk reduction.15
Among those randomly assigned to SGLT2i treatment, post hoc analyses of patients with CKD have observed similar slowing of long-term kidney function decline in those with or without an initial eGFR decline,16,17,18 and analyses from the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG Outcome) program reported that the risk reduction in cardiovascular outcomes with empagliflozin was not modified by the initial eGFR decline.16 In the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) trial of patients with heart failure and reduced ejection fraction, the development of an eGFR decline greater than 10% was associated with a lower risk of cardiovascular outcomes among those assigned to dapagliflozin, compared with those with a similar decline assigned to placebo.19
In this prespecified analysis of the Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure (DELIVER) trial, we evaluated the magnitude and frequency of an initial decline in eGFR, its predictors, and its association with clinical outcomes.
Methods
Data Sharing, Trial Design, and Oversight
Data underlying the findings described in this article may be obtained following AstraZeneca’s data sharing policy.20 The design, statistical analysis plan, and primary outcomes of the DELIVER trial have been published.21,22 Local ethics committees approved the trial, and all patients provided written informed consent. The trial was reviewed by an independent data and safety monitoring committee. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines.
Study Patients
The DELIVER trial enrolled adults 40 years or older with symptomatic heart failure and left ventricular ejection fraction greater than 40%, elevated N-terminal pro–brain natriuretic peptide (NT-proBNP) concentrations, and structural heart disease (left ventricular hypertrophy or left atrial enlargement within 12 months). Patients were randomly assigned in a 1:1 fashion to dapagliflozin, 10 mg once daily, or a matching placebo. Notable exclusion criteria included an eGFR level less than 25 at visit 1 (enrollment) and systolic BP lower than 95 mm Hg on 2 consecutive readings at visit 1 or 2 (randomization). Race was captured on a dedicated demographics case report form and included the following categories: Asian, Black or African American, White, or other race designation (including American Indian or Alaska Native and Native Hawaiian or Other Pacific Islander).
Definitions of Changes in eGFR and Serum Creatinine Level
For this prespecified secondary analysis of initial changes in biomarkers of kidney function, only patients with baseline and 1-month measurements of serum creatinine were included (eTable 1 in Supplement 1). The changes in eGFR level between baseline and month 1, as calculated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (2009),23 were categorized as follows: less than 0% (no decline or increase), 0% to 10% decline, or greater than 10% decline. In sensitivity analyses, additional changes in eGFR level (>25% decline) and serum creatinine (increase ≥0.3 mg/dL; increase ≥0.5 mg/dL; to convert to micromoles per liter, multiply by 88.4) were considered.
Cardiovascular and Kidney Outcomes
The primary outcome was the composite of cardiovascular death or a worsening heart failure event (hospitalization or urgent visit). For clinical kidney outcomes, owing to the infrequent occurrence of sustained declines in eGFR level in this trial,24 we evaluated a post hoc kidney composite outcome consisting of either the first occurrence of (1) 50% or greater decline in eGFR level relative to the month 1 value (as the initial decline in eGFR level was calculated from baseline to month 1); (2) development of end-stage kidney disease (from adverse event [AE] reporting or decline in eGFR level to <15); or (3) death due to kidney causes. Prespecified exploratory outcomes included the effect of dapagliflozin on change in eGFR (calculated by the CKD-EPI equation [2009]23 using serum creatinine measurements from visits at baseline and months 1, 4, 12, 24, and 36).
Safety Outcomes
The DELIVER trial collected data on serious AEs, AEs that led to discontinuation of dapagliflozin or placebo, and select other AEs (including kidney-related AEs).9 The frequency of safety events was compared according to categories of eGFR decline (≤10% vs >10%) among patients who received at least 1 dose of randomized treatment. The occurrence of AEs was examined separately in those assigned to placebo and those assigned to dapagliflozin, and according to timing in relation to the calculation of the eGFR decline at month 1 (≤1 month and >1 month).
Statistical Analysis
Data were reported as mean (SD) when normally distributed, as median (IQR) when nonnormally distributed, and as frequencies and percentages for categorical variables. Differences in baseline characteristics were assessed by tests for trend across categories of eGFR decline (<0%, 0%-10%, >10%) using linear regression, the Cuzick nonparametric trend test, and the χ2 test for trend for continuous normal, continuous nonnormal, and categorical data, respectively.
The odds of developing an initial decline in eGFR (>10% vs ≤10% and 25% vs ≤25%) or an increase in serum creatinine (≥0.3 vs <0.3 mg/dL and ≥0.5 vs <0.5 mg/dL) for dapagliflozin vs placebo were initially assessed using unadjusted logistic regression. Subsequently, to examine for potential effect modification by other baseline variables, logistic regression models that adjusted for baseline factors and their corresponding treatment interaction terms were fit (eGFR level, age, sex, race, body mass index [BMI], history of hypertension, history of diabetes, left ventricular ejection fraction, NT-proBNP level, systolic blood pressure, use of a loop diuretic, mineralocorticoid receptor antagonist, angiotensin-converting enzyme inhibitor [ACEi]/angiotensin receptor blocker [ARB], or angiotensin receptor–neprilysin inhibitor). Those with P value interaction terms of <.10 (eGFR level, use of a mineralocorticoid receptor antagonist, or use of an ACEi/ARB) were selected for inclusion in a multivariable-adjusted model.
For the time-to-event outcomes, incidence rates and 95% CIs were calculated per 100 patient-years of follow-up. Unadjusted and adjusted Cox proportional hazards models, landmarked at month 1, were fit to assess the association of eGFR decline greater than 10% (vs ≤10%) with cardiovascular and kidney outcomes. The multivariable model adjusted for the following baseline variables: age, sex, race, eGFR level, BMI), hypertension, left ventricular ejection fraction, log-transformed NT-proBNP level, systolic blood pressure, mineralocorticoid receptor antagonist, ACEi/ARB, and change in systolic blood pressure from baseline to month 1. All Cox models were stratified by the presence or absence of diabetes at baseline. Interaction terms were included to assess if the association of eGFR decline (>10% vs ≤10% from baseline to month 1) with cardiovascular and kidney composite outcomes differed according to randomized treatment assignment. In subgroup analyses, models were fit separately among those assigned to dapagliflozin and those assigned to placebo. The association of eGFR decline as a continuous variable with incidence rates of clinical outcomes was estimated using Poisson regression, with potential nonlinearity accommodated by using restricted cubic splines with 3 knots.
Multivariable mixed-effects models were used to assess for changes in eGFR over time (chronic slope, from month 4 through month 36) according to the presence or absence of an eGFR decline greater than 10% between baseline and month 1. Month 4 was chosen as the starting point for the examination of the chronic slope due to the observed pattern of initial change from baseline to month 1, followed by a rebound from month 1 to month 4. Models included terms for eGFR decline greater than 10%, trial visit, interaction between eGFR decline and trial visit, treatment assignment, the interaction between treatment assignment and visit, age, sex, race, eGFR level, BMI, diabetes, hypertension, left ventricular ejection fraction, log-transformed NT-proBNP level, systolic blood pressure, mineralocorticoid receptor antagonist use, ACEi/ARB use, and change in systolic blood pressure from baseline to month 1. Intercepts and slopes over time were allowed to vary randomly between patients via the inclusion of patient and time as random effects. In subgroup analyses, models were fit separately among those assigned to dapagliflozin and those assigned to placebo.
All analyses were performed at an α level of .05, without correction for multiple hypothesis testing, using Stata/MP, version 16.0 (StataCorp). All P values were 2-sided, and P < .05 was considered statistically significant. Data for the current study were analyzed from February to October 2023.
Results
Patient Characteristics
Overall, 5788 of 6263 patients (92%; mean [SD] age, 72 [10] years; 3255 male [56%]; 2535 female [44%]) had paired measurements of serum creatinine and eGFR level at both baseline and month 1, allowing the initial change in eGFR level to be calculated. Comparisons of patients where an initial eGFR decline was possible vs not possible to calculate are provided in eTable 1 in Supplement 1. Patients self-identified with the following race categories: 171 American Indian or Alaska Native (3%), 1225 Asian (21%), 142 Black or African American (2%), 4068 White (70%), or 182 other race (3%).
During the first month of treatment, 2408 patients (42%) did not have any decline in eGFR level, of which 977 (41%) were assigned to dapagliflozin, and 1431 (59%) were assigned to placebo. A total of 1499 patients (26%) had 0% to 10% decline, of which 771 (51%) were assigned to dapagliflozin, and 728 (49%) were assigned to placebo. A total of 1881 patients (32%) had a decline of greater than 10%, of which 1144 (61%) were assigned to dapagliflozin, and 737 (39%) were assigned to placebo. At baseline, those experiencing higher initial declines vs those experiencing an increase in eGFR were more likely to be older (mean [SD] age, 72 [9] years vs 71 [10] years), have higher systolic blood pressure (mean [SD], 129 [16] mm Hg vs 128 [15] mm Hg), BMI level (mean [SD], 30.2 [6.3] vs 29.6 [6.0]; calculated as weight in kilograms divided by height in meters squared), ejection fraction (mean [SD], 55% [9%] vs 54% [9%]), and eGFR level (mean [SD], 61 [18] vs 58 [19]). They were more likely to have a history of hypertension and diabetes, to be taking an ACEi or ARB, and to be assigned to dapagliflozin (Table 1). Comparisons of baseline characteristics among those who developed an initial decline in eGFR level greater than 10% vs less than or equal to 10% are presented by randomized treatment arm in eTable 2 in Supplement 1.
Table 1. Baseline Characteristics According to Categories of Estimated Glomerular Filtration Rate (eGFR) Decline From Baseline to Month 1.
| Characteristica | eGFR decline | P value for trend | ||
|---|---|---|---|---|
| <0% (n = 2408) | 0%-10% (n = 1499) | >10% (n = 1881) | ||
| Age, mean (SD), y | 71 (10) | 71 (10) | 72 (9) | .04 |
| Sex, No. (%) | ||||
| Female | 1072 (45) | 603 (40) | 860 (46) | .56 |
| Male | 1336 (55) | 896 (60) | 1021 (54) | |
| Race, No. (%) | ||||
| American Indian or Alaska Native | 72 (3) | 50 (3) | 49 (3) | .26 |
| Asian | 533 (22) | 340 (23) | 352 (19) | |
| Black or African American | 51 (2) | 41 (3) | 50 (3) | |
| White | 1685 (70) | 1023 (68) | 1360 (72) | |
| Otherb | 67 (3) | 45 (3) | 70 (4) | |
| Geographic region, No. (%) | ||||
| Europe and Saudi Arabia | 1174 (49) | 693 (46) | 907 (48) | .09 |
| Asia | 512 (21) | 332 (22) | 340 (18) | |
| Latin America | 431 (18) | 286 (19) | 353 (19) | |
| North America | 291 (12) | 188 (13) | 281 (15) | |
| Systolic blood pressure, mean (SD), mm Hg | 128 (15) | 128 (16) | 129 (16) | .02 |
| Heart rate, mean (SD), beats/min | 71 (12) | 71 (11) | 72 (11) | .53 |
| BMI, mean (SD)c | 29.6 (6.0) | 29.7 (6.0) | 30.2 (6.3) | .003 |
| Serum creatinine, mean (SD), mg/dL | 1.2 (0.4) | 1.1 (0.3) | 1.1 (0.3) | <.001 |
| eGFR, mean (SD)d | 58 (19) | 66 (20) | 61 (18) | <.001 |
| Coronary artery disease, No. (%) | 746 (31) | 435 (29) | 587 (31) | .95 |
| Left ventricular ejection fraction, mean (SD), % | 54 (9) | 54 (9) | 55 (9) | .03 |
| NT-proBNP, median (IQR), pg/mL | 1007 (627-1741) | 972 (599-1619) | 1022 (637-1800) | .54 |
| NYHA classification, No. (%) | ||||
| I | 0 | 0 | 1 (0) | .47 |
| II | 1822 (76) | 1157 (77) | 1402 (75) | |
| III | 580 (24) | 340 (23) | 470 (25) | |
| IV | 6 (0) | 2 (0) | 8 (0) | |
| Hypertension, No. (%) | 2110 (88) | 1316 (88) | 1704 (91) | .003 |
| Diabetes, No. (%) | 1028 (43) | 637 (42) | 933 (50) | <.001 |
| Atrial fibrillation or flutter, No. (%) | 1385 (58) | 826 (55) | 1076 (57) | .76 |
| Stroke, No. (%) | 233 (10) | 130 (9) | 185 (10) | .92 |
| Hospitalization for heart failure, No. (%) | 988 (41) | 580 (39) | 772 (41) | .93 |
| Myocardial infarction, No. (%) | 648 (27) | 383 (26) | 487 (26) | .43 |
| Loop diuretic at randomization, No. (%) | 1870 (78) | 1089 (73) | 1478 (79) | .66 |
| ACE inhibitor or ARB at randomization, No. (%) | 1719 (71) | 1114 (74) | 1393 (74) | .04 |
| Mineralocorticoid-receptor antagonist at randomization, No. (%) | 1034 (43) | 631 (42) | 825 (44) | .58 |
| β-Blocker at randomization, No. (%) | 1985 (82) | 1220 (81) | 1578 (84) | .25 |
| ARNI, No. (%) | 113 (5) | 81 (5) | 83 (4) | .73 |
| Dapagliflozin, No. (%) | 977 (41) | 771 (51) | 1144 (61) | <.001 |
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; ARNI, angiotensin-neprilysin inhibitor; BMI, body mass index; NT-proBNP, N-terminal pro–brain natriuretic peptide; NYHA, New York Heart Association.
SI conversion factor: To convert serum creatinine to micromoles per liter, multiply by 88.4.
Plus-minus values are mean (SD).
Other race included American or Alaska Native and Native Hawaiian or Other Pacific Islander.
The BMI is the weight in kilograms divided by the square of the height in meters.
The eGFR at baseline was estimated according to the Chronic Kidney Disease Epidemiology Collaboration (2009) formula.
Initial eGFR Decline From Baseline to Month 1
The median (IQR) change in eGFR level from baseline to month 1 was −4 (−9 to 1) in those assigned to dapagliflozin and −1 (−6 to 5) in those assigned to placebo, with a placebo-corrected difference of −3 (P < .001). The median (IQR) percentage change in eGFR level from baseline to month 1 was −6% (−16% to 3%) in those assigned to dapagliflozin and −1% (−10% to 8%) in those assigned to placebo, with a placebo-corrected difference of −5% (P < .001).
A higher proportion of patients assigned to dapagliflozin experienced a decline in eGFR level of greater than 10% vs those assigned to placebo (1144 of 2892 [40%] vs 737 of 2896 [25%]; odds ratio, 1.9; 95% CI, 1.7-2.1; P difference <.001). Similar patterns were noted in analyses that examined alternative thresholds of changes in eGFR level or serum creatinine from baseline to month 1 (Table 2).
Table 2. Frequency of Threshold-Based Changes in Estimated Glomerular Filtration Rate (eGFR) and Serum Creatinine From Baseline to Month 1.
| Definition of dip event | Mean (SD) eGFR change | Mean (SD) serum creatinine change, mg/dL | No. of dip events in placebo arm (%) | No. of dip events in dapagliflozin arm (%) | Dip events in dapagliflozin vs placebo, odds ratio (95% CI) |
|---|---|---|---|---|---|
| eGFR dip >10% | −12 (6) | 0.3 (0.2) | 737 (25) | 1144 (40) | 1.9 (1.7-2.1)a 1.9 (1.7-2.1)b |
| eGFR dip >25% | −20 (8) | 0.5 (0.4) | 140 (5) | 262 (9) | 2.0 (1.6-2.4)a 2.0 (1.6-2.4)b |
| Delta serum creatinine ≥0.3 mg/dL | −17 (9) | 0.5 (0.4) | 167 (6) | 293 (10) | 1.8 (1.5-2.2)a 1.9 (1.6-2.3)b |
| Delta serum creatinine ≥0.5 mg/dL | −20 (10) | 0.8 (0.5) | 57 (2) | 101 (3) | 1.9 (1.3-2.6)a 1.9 (1.3-2.6)b |
SI conversion factor: To convert serum creatinine to micromoles per liter, multiply by 88.4.
Unadjusted.
Adjusted for baseline eGFR, mineralocorticoid use, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use.
Dapagliflozin and Initial eGFR Decline Greater Than 10% According to Baseline Characteristics
A series of logistic regression models were fit to examine if the treatment effect on the initial decline in eGFR differed according to baseline characteristics (adjusted for the randomized treatment, the variable of interest, and a corresponding interaction term). Although dapagliflozin was consistently associated with higher risk of an initial eGFR decline across the baseline characteristics considered, the risk of an eGFR decline greater than 10% for dapagliflozin (vs placebo) appeared to be higher for those with baseline eGFR level less than or equal to 60, those not taking an ACEi or ARB, and those not taking a mineralocorticoid receptor antagonist at baseline (eFigure 1 in Supplement 1). The effect estimates for dapagliflozin vs placebo for the development of an eGFR decline greater than 10% from models that adjusted for these variables were similar to those obtained from unadjusted models (Table 2).
Initial eGFR Decline and Risk of Cardiovascular Outcomes
In landmark analyses (beginning at-risk time at 1 month), among those assigned to placebo, the primary cardiovascular outcome occurred in 156 of 720 patients (22%) who experienced an eGFR decline greater than 10% and in 357 of 2140 patients (17%) who did not (adjusted hazard ratio [aHR], 1.33; 95% CI, 1.10-1.62). Among those assigned to dapagliflozin, the primary cardiovascular outcome occurred in 175 of 1135 patients (15%) who experienced an eGFR decline greater than 10% and in 274 of 1739 patients (16%) who did not (aHR, 0.90; 95% CI, 0.74-1.09; P for interaction = .01). The relevant Kaplan-Meier curves examining the risk of the primary cardiovascular outcome according to the presence or absence of an initial eGFR decline greater than 10% and assignment to dapagliflozin vs placebo are shown in Figure 1. Similar patterns of association were noted using other definitions of eGFR decline or increase in serum creatinine (Table 3). The incidence rate for the primary cardiovascular outcome according to the initial decline in continuous eGFR level from baseline to month 1 (both absolute and percentage) according to treatment arms are displayed graphically in Figure 2.
Figure 1. Risk of Primary Cardiovascular Outcome.

Kaplan-Meier curve showing the risk of the primary cardiovascular outcome according to the presence or absence of an initial decline in estimated glomerular filtration rate greater than 10% vs not and assignment to dapagliflozin vs placebo.
Table 3. Event Rates and Association of Thresholds of Change in Estimated Glomerular Filtration Rate (eGFR) or Serum Creatinine With Cardiovascular and Kidney Outcomesa.
| Definition of dip | Cardiovascular composite outcome | P value for interaction | |||||
|---|---|---|---|---|---|---|---|
| Placebo No. of events/No. of patients (%) event rate (95% CI) per 100 patient years |
Dapagliflozin No. of events/No. of patients (%) event rate (95% CI) per 100 patient-years |
Adjusted HR (95% CI) | |||||
| No dip | Dip | No dip | Dip | Placebo | Dapagliflozin | ||
| eGFR dip >10% | 357/2140 (17) 8.3 (7.4-9.2) |
156/720 (22) 11.2 (9.5-13.0) |
274/1739 (16) 7.8 (6.9-8.8) |
175/1135 (15) 7.5 (6.4-8.6) |
1.33 (1.10-1.62) | 0.90 (0.74-1.09) | .01 |
| eGFR dip >25% | 472/2727 (17) 8.6 (7.9-9.4) |
41/133 (31) 17.9 (13.2-24.3) |
396/2615 (15) 7.4 (6.7-8.2) |
53/259 (20) 10.3 (7.8-13.4) |
1.68 (1.21-2.33) | 1.22 (0.91-1.64) | .12 |
| Delta serum creatinine ≥0.3 mg/dL | 459/2701 (17) 8.4 (7.7-9.2) |
54/159 (34) 19.6 (15.0-25.5) |
387/2585 (15) 7.3 (6.6-8.1) |
62/289 (21) 11.0 (8.6-14.1) |
1.70 (1.27-2.28) | 1.19 (0.90-1.58) | .07 |
| Delta serum creatinine ≥0.5 mg/dL | 499/2806 (18) 8.9 (8.1-9.7) |
14/54 (26) 14.9 (8.8-25.1) |
429/2775 (15) 7.5 (6.9-8.3) |
20/99 (20) 11.0 (7.1-17.0) |
1.14 (0.67-1.95) | 1.16 (0.73-1.83) | .97 |
| Post hoc kidney composite outcome b | |||||||
| eGFR dip >10% | 38/2150 (1.8) 0.8 (0.6-1.1) |
17/734 (2.3) 1.1 (0.7-1.8) |
23/1744 (1.3) 0.6 (0.4-0.9) |
15/1143 (1.3) 6 (0.4-1.0) |
1.62 (0.90-2.89) | 0.94 (0.49-1.82) | .35 |
| eGFR dip >25% | 49/2747 (1.8) 0.8 (0.6-1.1) |
6/137 (4.4) 2.3 (1.0-5.1) |
36/2626 (1.4) 0.6 (0.5-0.9) |
2/261 (0.8) 0.4 (0.1-1.5) |
3.54 (1.45-8.61) | 0.45 (0.11-1.90) | .05 |
| Delta serum creatinine ≥0.3 mg/dL | 44/2720 (1.6) 0.8 (0.6-1.0) |
11/164 (6.7) 3.2 (1.9-6.3) |
34/2595 (1.3) 0.6 (0.4-0.9) |
4/292 (1.4) 6.1 (0.2-1.8) |
4.60 (2.24-9.41) | 0.67 (0.23-1.94) | .02 |
| Delta serum creatinine ≥0.5 mg/dL | 50/2830 (1.8) 0.8 (0.6-1.1) |
5/54 (9.3) 5.0 (2.1-12.0) |
36/2787 (1.3) 0.6 (0.4-0.8) |
2/100 (2.0) 1.0 (0.3-4.0) |
5.93 (2.22-15.83) | 0.97 (0.22-4.20) | .11 |
Abbreviation: HR, hazard ratio.
SI conversion factor: To convert serum creatinine to micromoles per liter, multiply by 88.4.
All models were landmarked for at-risk time to start at the month 1 visit.
For the renal composite, the threshold of 50% decline in eGFR was calculated relative to the month 1 measurement.
Figure 2. Incidence Rates of the Primary Outcome.
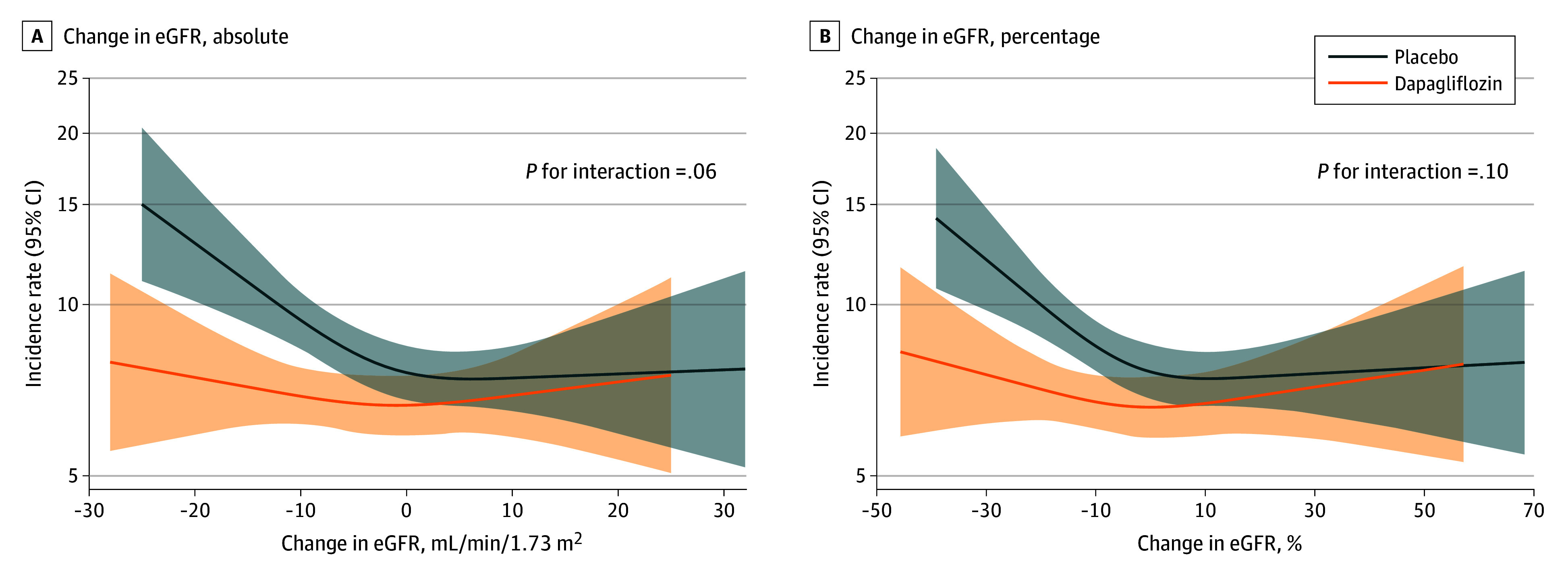
Adjusted incidence rates of the primary outcome occurring after 1 month (landmark analysis) according to change in estimated glomerular filtration rate (eGFR) from baseline to month 1 within randomized treatment groups. A, Absolute change in eGFR. B, Percentage change in eGFR. The shaded regions represent 95% CIs.
Initial eGFR Decline and Risk of Kidney Outcomes
Beginning at-risk time at 1 month, among those assigned to placebo, the post hoc kidney outcome occurred in 17 of 734 patients (2.3%) who experienced an eGFR decline greater than 10% and in 38 of 2150 patients (1.8%) who did not (aHR, 1.62; 95% CI, 0.90-2.89). Among those assigned to dapagliflozin, the post hoc kidney outcome occurred in 15 of 1143 patients (1.3%) who experienced an eGFR decline greater than 10% and in 23 of 1744 patients (1.3%) who did not (aHR, 0.94; 95% CI, 0.49-1.82; P for interaction = .35). Similar patterns of association were noted with other thresholds of changes in eGFR and serum creatinine level, although these analyses were limited by small numbers of events and wide CIs (Table 3).
Initial eGFR Decline and Longer-Term eGFR Slope
Among patients who developed an initial eGFR decline greater than 10%, the average adjusted change (IQR) in kidney function from month 4 was −1.2 (−1.6 to −0.8) per year; the corresponding value in those who did not develop an initial eGFR decline was −0.9 (−1.4 to −0.4) per year, with a difference of 0.3 (−0.2 to 0.8) per year. Although the overall rate of eGFR decline was faster among those assigned to placebo (compared with those assigned to dapagliflozin), the randomized treatment did not appear to modify the association of an initial eGFR decline vs no decline with longer-term eGFR slope (P for interaction = .68) (eFigure 2 in Supplement 1).
Initial eGFR Decline and AEs
The overall frequency of AEs was higher among those who experienced an initial eGFR decline greater than 10%, compared with those without this decline, in both early (≤1 month) and later (>1 month) periods. These findings were generally similar according to the randomized treatment assignment. The only exception was any serious AE from baseline to month 1, where the frequency of events among those with an eGFR decline greater than 10% (vs ≤10%) was higher in the placebo arm, as opposed to the dapagliflozin arm (eTable 3 in Supplement 1).
Discussion
Among patients with heart failure and mildly reduced or preserved ejection fraction enrolled in the DELIVER trial, the development of an initial decline in eGFR greater than 10% was more common among patients randomized to dapagliflozin than placebo. However, among those assigned to dapagliflozin, the presence of an initial eGFR decline was not associated with a higher risk of the primary cardiovascular outcome, nor with a difference in the longer-term rate of eGFR decline, compared with patients who did not develop an initial decline. Although AEs were overall more common among those with vs those without an initial eGFR decline, most were similar between dapagliflozin and placebo.
Initially used as a therapy to lower blood glucose in patients with diabetes, early experience with SGLT2is noted a propensity for these medications to cause modest acute elevations in serum creatinine level. Confirmation of these patterns (and reciprocal changes in eGFR level) were obtained in subsequent large clinical outcomes trials. More importantly, these trials also observed that the eGFR decline was reversible after drug discontinuation,13,14 and despite the initial decline, these medications slowed the longer-term decline in kidney function, compared with placebo.4,25 The acute decline in eGFR is felt to be a result of a reduction in intraglomerular pressure, via mechanism(s) that are still to be fully elucidated.11,12 Notably, some smaller mechanistic reports have shown that the acute decline in eGFR level with dapagliflozin occurs without evidence of kidney damage, as assessed by urine kidney injury biomarkers.26,27
However, despite these findings, real-world practice concerns remain regarding the underutilization of SGLT2i therapy across broad populations of patients where there are proven clinical indications.28 With respect to an initial decline in eGFR level, several studies have now examined the association of this phenomenon with clinical outcomes. For example, post hoc analyses of the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) study (T2D and CKD)17 and the EMPA-REG Outcome study (T2D and established cardiovascular disease)16 reported similar rates of longer-term eGFR decline in patients assigned to active therapy with vs without an initial decline in eGFR, whereas a post hoc analysis of the Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS CV; T2D and atherosclerotic cardiovascular disease) reported that patients in the largest (vs lowest) tertile of initial eGFR decline with ertugliflozin actually experienced the slowest rate of decline in longer-term eGFR slope.18 Real-world observational data from the Veterans Affairs database is consistent with these findings. In adjusted analyses, SGLT2i use was associated with a lower risk of cardiovascular and kidney outcomes in those with a higher-than-average probability of eGFR dip greater than 10% or greater than30%. Using inverse probability-weighted models, continued use of SGLT2is vs discontinuation at 6 months was associated with a lower risk of cardiovascular and kidney outcomes, across the categories of initial eGFR decline.15
In analyses from DAPA-HF, an initial decline in eGFR level of greater than 10% between baseline and 2 weeks occurred in 38% of patients assigned to dapagliflozin and 21% assigned to placebo. The association of a dip of greater than 10% with the primary cardiovascular outcome differed by treatment arms (HR, 1.45; 95% CI, 1.19-1.78 among those assigned to placebo and HR, 0.73; 95% CI, 0.59-0.91 among those assigned to dapagliflozin; P for interaction <.001).19 In the present analyses, we expand the knowledge base to those with heart failure and mildly reduced or preserved ejection fraction. We reported similar evidence for effect modification of the association of an initial eGFR decline with the primary cardiovascular outcome, according to randomized treatment arm, with an initial decline only being associated with a higher cardiovascular risk among those assigned to placebo. With respect to the kidney composite outcome, we observed the absence of a higher risk for those assigned to dapagliflozin who experienced an initial eGFR decline. This was largely in contrast to those assigned to placebo, where an initial decline was generally associated with a higher risk of the kidney outcome. Further, when chronic eGFR slope was examined (after month 4), the rate of eGFR decline appeared similar among those who did and did not develop an initial decline in eGFR in the dapagliflozin arm.
Strengths and Limitations
The strengths of our study include the large number of patients with the availability of repeated creatinine measurements, inclusion of patients to a lower eGFR threshold of 25, and detailed follow-up for adjudicated outcomes. However, limitations include some loss of patients without repeated kidney function measurements, generalizing results beyond a predominantly Asian and White population, potential residual confounding due to the consideration of a postrandomization exposure, and the relatively infrequent occurrence of post hoc defined kidney composite outcomes.
Conclusions
In conclusion, results of this prespecified analysis of the DELIVER trial showed that although an initial decline in eGFR level on initiation of dapagliflozin among participants of DELIVER was frequent, it was not associated with adverse cardiovascular outcomes and did not appear to alter the long-term trajectory of eGFR decline, compared with those without an initial eGFR decline. This is in contrast to the adverse cardiovascular and kidney prognostic implications of an initial eGFR decline with placebo. These data will be informative to clinicians and patients and, with appropriate monitoring, should provide reassurance for continuation of these medications in the majority of patients.
eFigure 1. Odds Ratio for Decline in eGFR >10% for Dapagliflozin vs Placebo in Subgroups
eFigure 2. Kaplan-Meier Curve Showing the Risk of the Primary Cardiovascular Outcome According to the Presence or Absence of an Initial Decline in eGFR >10% vs Not and Assignment to Dapagliflozin vs Placebo
eTable 1. Baseline Characteristics Among Those With and Without Available Data to Calculate the Difference on eGFR From Baseline to Month 1
eTable 2. Baseline Characteristics of Patients With an Initial eGFR Decline >10% From Baseline to Month 1, According to Randomized Treatment Arms
eTable 3. Adverse Events According to eGFR Decline >10% vs ≤10% and Relative to Month 1 Visit (Safety Population)
Data Sharing Statement.
References
- 1.Wanner C, Inzucchi SE, Lachin JM, et al. ; EMPA-REG OUTCOME Investigators . Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323-334. doi: 10.1056/NEJMoa1515920 [DOI] [PubMed] [Google Scholar]
- 2.Neal B, Perkovic V, Mahaffey KW, et al. ; CANVAS Program Collaborative Group . Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644-657. doi: 10.1056/NEJMoa1611925 [DOI] [PubMed] [Google Scholar]
- 3.Bhatt DL, Szarek M, Pitt B, et al. ; SCORED Investigators . Sotagliflozin in patients with diabetes and chronic kidney disease. N Engl J Med. 2021;384(2):129-139. doi: 10.1056/NEJMoa2030186 [DOI] [PubMed] [Google Scholar]
- 4.Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. ; DAPA-CKD Trial Committees and Investigators . Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436-1446. doi: 10.1056/NEJMoa2024816 [DOI] [PubMed] [Google Scholar]
- 5.Perkovic V, Jardine MJ, Neal B, et al. ; CREDENCE Trial Investigators . Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295-2306. doi: 10.1056/NEJMoa1811744 [DOI] [PubMed] [Google Scholar]
- 6.Packer M, Anker SD, Butler J, et al. ; EMPEROR-Reduced Trial Investigators . Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413-1424. doi: 10.1056/NEJMoa2022190 [DOI] [PubMed] [Google Scholar]
- 7.Anker SD, Butler J, Filippatos G, et al. ; EMPEROR-Preserved Trial Investigators . Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451-1461. doi: 10.1056/NEJMoa2107038 [DOI] [PubMed] [Google Scholar]
- 8.McMurray JJV, Solomon SD, Inzucchi SE, et al. ; DAPA-HF Trial Committees and Investigators . Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008. doi: 10.1056/NEJMoa1911303 [DOI] [PubMed] [Google Scholar]
- 9.Solomon SD, McMurray JJV, Claggett B, et al. ; DELIVER Trial Committees and Investigators . Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387(12):1089-1098. doi: 10.1056/NEJMoa2206286 [DOI] [PubMed] [Google Scholar]
- 10.Bhatt DL, Szarek M, Steg PG, et al. ; SOLOIST-WHF Trial Investigators . Sotagliflozin in patients with diabetes and recent worsening heart failure. N Engl J Med. 2021;384(2):117-128. doi: 10.1056/NEJMoa2030183 [DOI] [PubMed] [Google Scholar]
- 11.Kidokoro K, Cherney DZI, Bozovic A, et al. Evaluation of glomerular hemodynamic function by empagliflozin in diabetic mice using in vivo imaging. Circulation. 2019;140(4):303-315. doi: 10.1161/CIRCULATIONAHA.118.037418 [DOI] [PubMed] [Google Scholar]
- 12.van Bommel EJM, Muskiet MHA, van Baar MJB, et al. The renal hemodynamic effects of the SGLT2 inhibitor dapagliflozin are caused by post-glomerular vasodilatation rather than preglomerular vasoconstriction in metformin-treated patients with type 2 diabetes in the randomized, double-blind RED trial. Kidney Int. 2020;97(1):202-212. doi: 10.1016/j.kint.2019.09.013 [DOI] [PubMed] [Google Scholar]
- 13.Wanner C, Heerspink HJL, Zinman B, et al. ; EMPA-REG OUTCOME Investigators . Empagliflozin and kidney function decline in patients with type 2 diabetes: a slope analysis from the EMPA-REG OUTCOME trial. J Am Soc Nephrol. 2018;29(11):2755-2769. doi: 10.1681/ASN.2018010103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cherney DZI, Ferrannini E, Umpierrez GE, et al. Efficacy and safety of sotagliflozin in patients with type 2 diabetes and severe renal impairment. Diabetes Obes Metab. 2021;23(12):2632-2642. doi: 10.1111/dom.14513 [DOI] [PubMed] [Google Scholar]
- 15.Xie Y, Bowe B, Gibson AK, McGill JB, Maddukuri G, Al-Aly Z. Clinical implications of estimated glomerular filtration rate dip following sodium-glucose cotransporter-2 inhibitor initiation on cardiovascular and kidney outcomes. J Am Heart Assoc. 2021;10(11):e020237. doi: 10.1161/JAHA.120.020237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kraus BJ, Weir MR, Bakris GL, et al. Characterization and implications of the initial estimated glomerular filtration rate dip upon sodium-glucose cotransporter-2 inhibition with empagliflozin in the EMPA-REG OUTCOME trial. Kidney Int. 2021;99(3):750-762. doi: 10.1016/j.kint.2020.10.031 [DOI] [PubMed] [Google Scholar]
- 17.Oshima M, Jardine MJ, Agarwal R, et al. Insights from CREDENCE trial indicate an acute drop in estimated glomerular filtration rate during treatment with canagliflozin with implications for clinical practice. Kidney Int. 2021;99(4):999-1009. doi: 10.1016/j.kint.2020.10.042 [DOI] [PubMed] [Google Scholar]
- 18.Cherney DZI, Cosentino F, Dagogo-Jack S, et al. ; VERTIS CV Investigators . Initial eGFR changes with ertugliflozin and associations with clinical parameters: analyses from the VERTIS CV Trial. Am J Nephrol. 2022;53(7):516-525. doi: 10.1159/000524889 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Adamson C, Docherty KF, Heerspink HJL, et al. Initial decline (dip) in estimated glomerular filtration rate after initiation of dapagliflozin in patients with heart failure and reduced ejection fraction: insights from DAPA-HF. Circulation. 2022;146(6):438-449. doi: 10.1161/CIRCULATIONAHA.121.058910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.AstraZeneca . Our transparency commitments. Accessed October 1, 2023. https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure
- 21.Solomon SD, Vaduganathan M, Claggett BL, et al. Baseline characteristics of patients with HF with mildly reduced and preserved ejection fraction: DELIVER trial. JACC Heart Fail. 2022;10(3):184-197. doi: 10.1016/j.jchf.2021.11.006 [DOI] [PubMed] [Google Scholar]
- 22.Solomon SD, McMurray JJV, Claggett B, et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N Engl J Med. 2022;387(12):1089-1098. doi: 10.1056/NEJMoa2206286 [DOI] [PubMed] [Google Scholar]
- 23.Levey AS, Stevens LA, Schmid CH, et al. ; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) . A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-612. doi: 10.7326/0003-4819-150-9-200905050-00006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mc Causland FR, Claggett BL, Vaduganathan M, et al. Dapagliflozin and kidney outcomes in patients with heart failure with mildly reduced or preserved ejection fraction: a prespecified analysis of the DELIVER randomized clinical trial. JAMA Cardiol. 2023;8(1):56-65. doi: 10.1001/jamacardio.2022.4210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Herrington WG, Staplin N, Wanner C, et al. ; The EMPA-KIDNEY Collaborative Group . Empagliflozin in patients with chronic kidney disease. N Engl J Med. 2023;388(2):117-127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dekkers CCJ, Petrykiv S, Laverman GD, Cherney DZ, Gansevoort RT, Heerspink HJL. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obes Metab. 2018;20(8):1988-1993. doi: 10.1111/dom.13301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sen T, Li J, Neuen BL, et al. Effects of the SGLT2 inhibitor canagliflozin on plasma biomarkers TNFR-1, TNFR-2 and KIM-1 in the CANVAS trial. Diabetologia. 2021;64(10):2147-2158. doi: 10.1007/s00125-021-05512-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schernthaner G, Shehadeh N, Ametov AS, et al. Worldwide inertia to the use of cardiorenal protective glucose-lowering drugs (SGLT2i and GLP-1 RA) in high-risk patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19(1):185. doi: 10.1186/s12933-020-01154-w [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Odds Ratio for Decline in eGFR >10% for Dapagliflozin vs Placebo in Subgroups
eFigure 2. Kaplan-Meier Curve Showing the Risk of the Primary Cardiovascular Outcome According to the Presence or Absence of an Initial Decline in eGFR >10% vs Not and Assignment to Dapagliflozin vs Placebo
eTable 1. Baseline Characteristics Among Those With and Without Available Data to Calculate the Difference on eGFR From Baseline to Month 1
eTable 2. Baseline Characteristics of Patients With an Initial eGFR Decline >10% From Baseline to Month 1, According to Randomized Treatment Arms
eTable 3. Adverse Events According to eGFR Decline >10% vs ≤10% and Relative to Month 1 Visit (Safety Population)
Data Sharing Statement.