

INTRODUCTION
Distal femur fractures account for 4%–6% of all femur fractures.[1,2] These fractures have a bimodal age distribution pattern, most commonly affecting elderly osteoporotic women from low-energy trauma, followed by young men from high-energy trauma.[2] Although distal femur fractures have not been as well described as hip fractures, the mortality and morbidity associated with distal femur fractures are similar to those associated with hip fractures, and should not be underestimated.[3-5] Hence, it is important to aim for a quick return to pre-injury functional status with minimal reoperation rates.
The current practice in managing displaced distal femur fractures would involve surgical fixation using extramedullary fixed-angle locking plate or intramedullary fixation with a retrograde nail if the patient is fit enough to undergo surgery.[6-9] However, distal femur fractures are notoriously difficult to treat, as they often present with bone loss from metaphyseal comminution, poor bone quality from osteoporosis and a short distal fragment that is difficult to stabilise.[7-9] Extramedullary fixation with lateral locking plates is the main workhorse, because they allow multiple locking screw fixation into the distal fragment with good stability and stiffness as inherent to fixed-angle construct. Nonetheless, they are load-bearing devices and can lead to complications related to excessive construct stiffness such as implant fracture or non-union with rates ranging from 19% to 22%.[8-14] Retrograde intramedullary nails have seen increasing use with good outcomes, but they are associated with increased micro-motion at the fracture site in osteoporotic comminuted fractures and are difficult to use in very distal fractures with inadequate bone purchase.[8-11]
The need for more stable fixations have resulted in the use of supplemental fixations such as dual plating and nail-plate construct for distal femur fractures in recent years.[15-23] Reports from multiple authors using these supplemental fixations in native, periprosthetic and revision distal femur fracture fixations have shown good results.[15-23] To date, there is a paucity of data to show the collective outcomes of such supplemental fixation techniques focused at increasing stability in the fixation construct to allow shared load bearing across the fracture site for improved healing and early weight-bearing.
Hence, we aimed to review our experience with augmented fixation and its outcomes in treating distal femur fractures using combinations of nail, plate and/or cable cerclage wiring construct.
METHODS
This is a retrospective review of all patients with distal femur fractures admitted to our institution and treated with augmented fixation from 1 January 2013 to 31 October 2017. The inclusion criteria were fractures treated with augmented fixation and a minimum age of 21 years. Decision for augmented fixation was based on the experience of the senior author (AG) on the predicted risk of failure of fixation with early weight-bearing. Some prognostic factors for augmented fixation include extensive distal femur metaphyseal comminution and bone loss, poor bone stock, low fracture line or short distal fragment insufficient for single implant stabilisation. Patients with open fracture, pathological fractures (oncology and infection), revision fixation and skeletally immature patients were excluded.
Pertinent demographic data (age, gender, weight), pre-injury ambulatory status, presence of comorbidities, 25-hydroxy vitamin D level, American Society of Anesthesiology (ASA) grade, mechanism of injury, fracture pattern, types of augmented fixation, estimated blood loss (EBL), duration of surgery, radiation dosage from image intensifier (II), immediate postoperative weight-bearing status, final follow-up ambulatory status, union rates and complications were analysed statistically. The institutional review board approved this study.
Preoperative radiographs were reviewed and classified according to Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification system. The assessment of bone mineral density (BMD) was based on the dual energy X-ray absorptiometry tool and WHO classifications. The ASA grading was used to assess the overall health status of a patient and their fitness for surgery.
Postoperative radiographs were reviewed, and union was defined as complete cortical bridging with no visible fracture line. All surgeries were performed by the senior surgeon (AG) who is a fellowship trained traumatologist and specialist registrars. Surgeries were performed under fluoroscopic guidance and, in most cases, a large femoral distractor was applied initially to achieve length and provisional alignment of the fracture. Postoperative rehabilitation was standardised where early ambulatory exercises with a walking aid together with a physiotherapist was commenced at postoperative Day 1, as tolerated. All patients were reviewed at two and six weeks, and at three, six and 12 months with clinical examinations and radiographic monitoring.
Data entry was performed using a spreadsheet application (Excel 2003, Microsoft Corp., Redmond, WA, USA). Frequency tables and descriptive statistics (mean, standard deviation or median where appropriate) were presented for all variables. Categorical variables were presented as proportions and continuous variables were presented as means.
RESULTS
A total of 20 patients who met the inclusion criteria. These patients had an average age of 68.7 (range 27–85) years. 16 (80%) of them were aged 60 years and older, and 18 (90%) patients were female. The majority of our patients were ASA grade 2 (45%, n = 9), followed by 6 (30%) with ASA grade 3 and 5 (25%) with ASA grade 1. In terms of pre-injury ambulatory status, 17 (85%) patients were independent ambulators and only three patients required walking aids (one with walking stick and two with walking frame). All the 18 (90%) female patients sustained low-velocity injury (fall from a standing height), while the only two male patients in the cohort had high-velocity injuries. Within available numbers, the average duration of surgery (18 patients) was 172.8 (range 105–240) minutes, average EBL (13 patients) was 276.9 (range 50–600) mL, average radiation dose from II (18 patients) was 238.1 (range 74.59–460.46) cGy cm2, mean 25-hydroxy vitamin D level (19 patients) was 17.6 (range 5–29) ng/mL, and the BMD scan showed that five out of 11 patients were osteoporotic, with a mean T score of − 3.5 (−2.5 to − 3.6). The remaining six were in the osteopenic range. Table 1 shows the demographics of the patients.
Table 1.
Demographics of patients treated with augmented fixation for distal femur fractures (N=20).
| Characteristic | n (%) |
|---|---|
| Agea (yr) | 68.7 (27–85) |
|
| |
| Gender | |
| Male | 2 (10) |
| Female | 18 (90) |
|
| |
| Weighta (kg) (n=17) | 61 (39.9–120.0) |
|
| |
| ASA grade | |
| 1 | 5 (25) |
| 2 | 9 (45) |
| 3 | 6 (30) |
| 4 | 0 (0) |
|
| |
| Pre-injury ambulatory status | |
| Independent | 17 (85) |
| Walking aids | 3 (15) |
|
| |
| Hypertension | |
| Yes | 14 (70) |
| No | 6 (30) |
|
| |
| Diabetes mellitus | |
| Yes | 10 (50) |
| No | 10 (50) |
|
| |
| Hyperlipidaemia | |
| Yes | 12 (60) |
| No | 8 (40) |
|
| |
| Ischaemic heart disease | |
| Yes | 3 (15) |
| No | 17 (85) |
|
| |
| Renal impairment | |
| Yes | 3 (15) |
| No | 17 (85) |
|
| |
| AO classification | |
| A1 | 5 (25) |
| A2 | 3 (15) |
| A3 | 1 (5) |
| C1 | 1 (5) |
| C2 | 7 (35) |
| C3 | 2 (10) |
|
| |
| Duration of surgerya (n=18) | 172.8 (105–240) |
|
| |
| Estimated blood lossa (mL) (n=13) | 276.9 (50–600) |
|
| |
| Radiation dosea,b (cGy cm2) (n=18) | 238.1 (74.59–460.46) |
|
| |
| Vitamin D levela (n=19) | 17.6 (5–29) |
|
| |
| Osteoporosis (n=11) | |
| Yes | 5 (45.5) |
| No | 6 (54.5) |
|
| |
| T score for osteoporotic patientsa (n=5) | −3.5 (−2.5 to−3.6) |
aData presented as mean (range). bFrom image intensifier usage. AO: Arbeitsgemeinschaft für Osteosynthesefragen
The distal femur fractures treated with augmented fixation were mainly AO type A and C, where there was a discontinuity between the articular block and the diaphysis [Table 1]. There were six types of augmented fixation constructs, with the most common being nail and cable construct, followed by dual plating construct, dual plating and cable construct, nail plate and cable construct, nail dual plate and cable construct, with the least common being the plate and cable construct [Figures 1 and 2]. Only one patient had periprosthetic distal femur fracture involving the femur component. It was a Lewis and Rorabeck type II fracture, where the fracture is displaced but the femoral component is still stable. Table 2 shows the types of fractures treated with their corresponding augmented fixation constructs.
Figure 1.

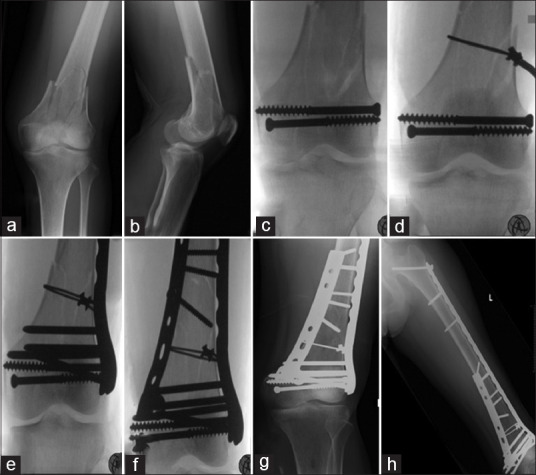
Nail cable cerclage wiring construct. Radiographs show (a and b) distal femur fracture AO type C2 fracture; and (c-h) reduction and fixation with cable cerclage wiring construct and Poller blocking screw followed by retrograde femur nailing. (i-l) postoperative radiographs show complete union.
Figure 2.
Dual plating with cable cerclage wiring construct. Radiographs show (a and b) distal femur fracture AO type C2 fracture; and (c-f) reduction and fixation with cable cerclage wiring construct and dual plating (lateral locking plate in bridge-plating mode spanning the entire femur and medial buttress plating). (g and h) Postoperative radiographs show complete union.
Table 2.
AO classification of distal femur fractures with their corresponding augmented fixation constructs.
| AO classification | Types of augmented fixation constructs | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| Nail, cable cerclage | Nail, lateral plate, cable cerclage | Nail, dual plate, cable cerclage | Lateral plate, cable cerclage | Dual plate | Dual plate, cable cerclage | |
| A1 | 4 | 0 | 0 | 0 | 0 | 1 |
| A2 | 1 | 1 | 0 | 0 | 0 | 1 |
| A3 | 0 | 0 | 0 | 0 | 1 | 0 |
| C1 | 0 | 0 | 1 | 0 | 0 | 0 |
| C2 | 3 | 0 | 0 | 1 | 2 | 1 |
| C3 | 1 | 0 | 1 | 0 | 0 | 0 |
| Periprosthetic | 0 | 1 | 0 | 0 | 0 | 0 |
AO: Arbeitsgemeinschaft für Osteosynthesefragen
All patients were allowed early weight-bearing as tolerated with walking aids postoperatively. However, three patients were allowed only toe-touch weight-bearing with walking frame owing to additional injuries on the same limb. These three patients had other concomitant injuries on the ipsilateral limb, such as two cases of vascular injuries (both requiring vascular intervention preoperatively) and one case of calcaneum fracture (concurrently fixed).
In this series, all our patients were ambulant as of their last follow-up visit, although only 9 (45%) out of 20 patients were able to retain their pre-injury independent ambulatory status, while 3 (15%) patients retained their pre-injury ambulatory status with walking aids. The remaining 8 (40%) patients who were independent ambulators prior to injury needed walking aids after surgery. No wound complications, loss of fracture reduction post-fixation, removal of implants or revision surgery were required as per last review. All patients except one achieved fracture union. The patient with non-union was on renal dialysis, with multiple co-morbidities including peripheral vascular disease. She was able to weight-bear with a walking stick as of her last follow-up visit (13 months after surgery) and refused revision surgery as she was asymptomatic. In addition, there was a case of postoperative pulseless limb due to popliteal artery intimal injury, for which an urgent angiogram and stenting were performed. This patient had an AO A2 type fracture that was uneventfully treated with nail and cable construct. We postulate that the popliteal artery intimal injury could be due to intraoperative reduction manoeuvres. No in-hospital death was reported, but one death occurred at four months postoperatively owing to an unrelated cause. The average follow-up duration was 12.6 (range 4–34) months.
DISCUSSION
With the increasing life expectancy and aging population, distal femur fractures are becoming more common.[2-5] Common concerns when dealing with distal femur fractures regardless of age are similar owing to the extensive metaphyseal comminution, which can lead to bone loss, inadequate bony purchase, and very commonly, a low fracture line resulting in a short distal fragment that is difficult to stabilise.[7-9] These are further compounded in elderly patients when poor bone quality from osteoporosis predisposes to complications such as implant cut out and post-fixation articular fragment displacement.
Combination treatment to augment distal femur fracture fixation is not new. Dual plating with the addition of medial plate to supplement a deficient medial buttress in distal femur fractures had been described in native, periprosthetic and revision fracture fixation by multiple authors.[8,9,15,16,23] Holzman et al. added a medial locking plate to treat distal femur fracture non-union that was previously fixed with an in situ lateral locking plate placed during the initial surgery. In their study, 20 out of 21 non-unions progressed to union successfully.[16] Nail plate construct was also gaining popularity as it was able to produce a more stable construct, with more reports showing good outcomes in the recent years.[17-22] Birjandinejad et al. showed that the addition of a 4.5-mm compression plate to a series of femur and tibial non-unions primarily treated with intramedullary nails resulted in union for all the 25 femur non-unions and 11 out of 13 tibial non-unions at a mean of 4.78 months.[17]
In our experience, while lateral locking plates are very good for most distal femur fractures, many have residual motion at the fracture site, leading to non-union and implant failure. This is associated with comminution and bone loss, especially over the medial column, poor bone quality from osteoporosis and a short distal fragment that is difficult to stabilise. Similarly, Salas et al. in their two-part study,[11,12] used biomechanical data from fracture fixation constructs on synthetic osteoporotic distal femur bone to generate a finite element analysis model. They found that an osteoporotic distal femoral model fixed with a lateral locking plate versus intramedullary nail produced different stresses on the implant and surrounding bone upon weight-bearing. The lateral locking plate behaves like a load-bearing device during weight-bearing while the bone does not experience much stress, especially medially. Conversely, the intramedullary nail does not take much of the load, while the surrounding bone experiences more stress. The authors noted that during ramped-up analysis, the probability of implant fracture was greater for the lateral locking plate than it was for the intramedullary nail, although catastrophic failure of the surrounding cortex was more likely to occur surrounding the nail.[11,12] Moreover, Chen et al.[12] used a finite element method to evaluate the differences between a retrograde intramedullary nail and lateral locking plate with and without an intramedullary allograft for osteoporotic periprosthetic distal femur fractures.[13] They found that the lateral locking plate with intramedullary allograft construct provided both lateral and middle supports to the distal femur fracture while the lateral locking plate and retrograde intramedullary nail constructs respectively transmit loads through the lateral and middle path separately, resulting in high stresses on the implants and the construct individually. The lateral locking plate with intramedullary allograft was the most stable construct with least micromotion, because the allograft could partially transmit load to the proximal femur and reduce the moment arm between the allograft and the condyles, while the lateral locking plate alone was most unstable in the middle and medial side of the fracture owing to the longer moment arm of lateral fixation.[13]
A notable proportion of patients in our cohort, most of whom were elderly patients (16 out of 20 patients >60 years old) with multiple comorbidities and low vitamin D levels, had osteoporosis/osteopenia. We found that augmented fixation using combinations of nail, plate and/or cable cerclage wiring construct were able to provide the additional stability for a reliable bony union. The shared load-bearing across the fracture site allowed a stable environment for bone healing.[13] Another principle practiced during augmented fixation was dissection without excessive soft tissue disruption and periosteal stripping. All the augmented fixation constructs were performed via minimally invasive surgery (MIS) techniques such as minimally invasive plating osteosynthesis technique for a bridge plating construct or cable cerclage wiring inserted via MIS wire passer. In combination, these techniques led to an augmented fixation construct that was imbued with additional stability at the fracture site while preserving biology, which was necessary to allow for optimal healing and early weight-bearing. In addition, the supplemental implants in augmented fixation allowed us to render them as assistive reduction tools. For example, in selected cases, we used cable cerclage wiring to reduce the metaphyseal and/or diaphyseal butterfly fragments of the distal femur fracture or a combination of cable cerclage wiring and lateral locking plate for indirect reduction of the fracture fragment, followed by buttress plating [Figures 1 and 2]. Cable cerclage wiring has, in many instances, provided the much-needed initial reduction and stability, followed by subsequently fixation with nail or plates in our series. It has also been reported recently by Lee et al. that percutaneous cerclage wiring resulted in better reduction of the fracture, maintenance of the alignment and shorter time to union.[24]
Weight-bearing status after fixation of distal femur fractures is not well described. Generally, most patients, especially those with comminution and poor bone stock, will be placed on a period of protected weight-bearing or non-weight-bearing, which can limit their mobility, increase the length of hospital stay and delay return to function.[6,8] In our own experience, elderly patients found it hard to adhere to limited weight-bearing such as toe touch weight-bearing or partial weight-bearing, as they often have concomitant gait instability and limited reserves/degenerative joint conditions in the contralateral limb that preclude them from offloading the newly fixed distal femur fracture site. With the additional stability conferred by augmented fixation, all patients in our series were allowed early weight-bearing, with no implant complications or revision surgeries required, even though a large majority of patients were elderly, with poor bone stock. Similarly, Hussain et al. reported about nine patients with interprosthetic distal femur fractures treated with a combined retrograde intramedullary nail and lateral locking plate who were allowed immediate weight-bearing and achieved good union rates.[20] Liporace and Yoon reported on a series of 15 patients (nine periprosthetic and six native) treated with nail plate construct and allowed immediate weight-bearing owing to the increased stability provided by the supplemental fixation; all these patients achieved successful fracture union.[21]
It is well known that a large majority of patients have poor functional and ambulatory status after hip fracture surgery owing to being non-ambulant.[3-5,25] However, ambulatory status after distal femur fracture surgery is not well known. Very few studies have reported regarding ambulatory status after native distal femur fracture surgery. Kammerlander et al.’s study on geriatric distal femoral fractures demonstrated that at least 23% of patients were totally housebound, 26% were unable to perform any social activities and only 18% were able to walk unaided after lateral locking plate fixation.[26] Hart et al. found that at one year, all patients who underwent distal femoral replacement were ambulatory, while in the lateral locking plate cohort, only 27% (6/22) of patients were able to ambulate independently at one year.[27] In the present study, we found that all patients were able to stay ambulant at an average of 12.6 months after the surgery, although not at their pre-injury level. After surgery, 60% of our patients who could ambulate independently or with walking aids prior to their surgery managed to retain their ambulatory status, and 40% of our patients who were previously independent ambulators had to use walking aids after the surgery. None were wheelchair dependent. We postulate that the ability to maintain ambulatory status was likely attributable to the early weight-bearing regime that was started after augmented fixation. The benefits of early weight-bearing are numerous, including accelerated functional recovery and reduced burden on healthcare resources. While our study is limited by small numbers and no comparison cohort, we strongly believe that with the additional stability provided by augmented fixation, early weight-bearing was not only achievable but also sustainable in the long term.
The other limitations of this study include its retrospective nature, lack of a longer-term follow-up and that the results generated were from a single centre. As the choices of the implants were based on the surgeons’ preference, selection bias may have been present. We were also limited by the number of patients with available 25-hydroxy vitamin D levels and BMD scans to make a conclusive analysis. Despite the aforementioned limitations, the strengths of the study are its inclusion of postoperative ambulatory status for all patients and it being the first study to report the collective outcomes of augmented fixation in distal femur fractures.
In conclusion, augmented fixation for distal femur fractures is an effective method to treat various types of distal femur fractures, especially those with bone loss from comminution and poor bone stock. It should be considered as an option for a single intervention focused at increasing stability in the fixation construct to allow shared load-bearing across the fracture site for improved healing and early weight-bearing. A notable proportion of the patients were able to maintain pre-injury ambulation status at one year following augmented fixation and none were rendered non-ambulatory.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury. 2006;37:691–7. doi: 10.1016/j.injury.2006.04.130. [DOI] [PubMed] [Google Scholar]
- 2.Martinet O, Cordey J, Harder Y, Maier A, Bühler M, Barraud GE. The epidemiology of fractures of the distal femur. Injury. 2000;31(Suppl 3):C62–3. doi: 10.1016/s0020-1383(00)80034-0. [DOI] [PubMed] [Google Scholar]
- 3.Streubel PN, Ricci WM, Wong A, Gardner MJ. Mortality after distal femur fractures in elderly patients. Clin Orthop Relat Res. 2011;469:1188–96. doi: 10.1007/s11999-010-1530-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moloney GB, Pan T, Van Eck CF, Patel D, Tarkin I. Geriatric distal femur fracture: Are we underestimating the rate of local and systemic complications? Injury. 2016;47:1732–6. doi: 10.1016/j.injury.2016.05.024. [DOI] [PubMed] [Google Scholar]
- 5.Jennison T, Divekar M. Geriatric distal femoral fractures: A retrospective study of 30 day mortality. Injury. 2019;50:444–7. doi: 10.1016/j.injury.2018.10.035. [DOI] [PubMed] [Google Scholar]
- 6.Smith JR, Halliday R, Aquilina AL, Morrison RJ, Yip GC, McArthur J, et al. Distal femoral fractures: The need to review the standard of care. Injury. 2015;46:1084–8. doi: 10.1016/j.injury.2015.02.016. [DOI] [PubMed] [Google Scholar]
- 7.Hoskins W, Sheehy R, Edwards ER, Hau RC, Bucknill A, Parsons N, et al. Nails or plates for fracture of the distal femur?Data from the Victoria Orthopaedic Trauma Outcomes Registry. Bone Joint J. 2016;98-B:846–50. doi: 10.1302/0301-620X.98B6.36826. [DOI] [PubMed] [Google Scholar]
- 8.Beltran MJ, Gary JL, Collinge CA. Management of distal femur fractures with modern plates and nails: State of the art. J Orthop Trauma. 2015;29:165–72. doi: 10.1097/BOT.0000000000000302. [DOI] [PubMed] [Google Scholar]
- 9.Hake ME, Davis ME, Perdue AM, Goulet JA. Modern implant options for the treatment of distal femur fractures. J Am Acad Orthop Surg. 2019;27:e867–75. doi: 10.5435/JAAOS-D-17-00706. [DOI] [PubMed] [Google Scholar]
- 10.Salas C, Mercer D, DeCoster TA, Reda Taha MM. Experimental and probabilistic analysis of distal femoral periprosthetic fracture: A comparison of locking plate and intramedullary nail fixation. Part A: Experimental investigation. Comput Methods Biomech Biomed Engin. 2011;14:157–64. doi: 10.1080/10255842.2010.535816. [DOI] [PubMed] [Google Scholar]
- 11.Salas C, Mercer D, DeCoster TA, Reda Taha MM. Experimental and probabilistic analysis of distal femoral periprosthetic fracture: A comparison of locking plate and intramedullary nail fixation. Part B: Probabilistic investigation. Comput Methods Biomech Biomed Engin. 2011;14:175–82. doi: 10.1080/10255842.2010.539207. [DOI] [PubMed] [Google Scholar]
- 12.Chen SH, Chiang MC, Hung CH, Lin SC, Chang HW. Finite element comparison of retrograde intramedullary nailing and locking plate fixation with/without an intramedullary allograft for distal femur fracture following total knee arthroplasty. Knee. 2014;21:224–31. doi: 10.1016/j.knee.2013.03.006. [DOI] [PubMed] [Google Scholar]
- 13.Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh JL. Locking plates for distal femur fractures: Is there a problem with fracture healing? J Orthop Trauma. 2011;25(Suppl 1):S8–14. doi: 10.1097/BOT.0b013e3182070127. [DOI] [PubMed] [Google Scholar]
- 14.Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ. Risk factors for failure of locked plate fixation of distal femur fractures: An analysis of 335 cases. J Orthop Trauma. 2014;28:83–9. doi: 10.1097/BOT.0b013e31829e6dd0. [DOI] [PubMed] [Google Scholar]
- 15.Steinberg EL, Elis J, Steinberg Y, Salai M, Ben-Tov T. A double-plating approach to distal femur fracture: A clinical study. Injury. 2017;48:2260–5. doi: 10.1016/j.injury.2017.07.025. [DOI] [PubMed] [Google Scholar]
- 16.Holzman MA, Hanus BD, Munz JW, O’Connor DP, Brinker MR. Addition of a medial locking plate to an in situ lateral locking plate results in healing of distal femoral nonunions. Clin Orthop Relat Res. 2016;474:1498–505. doi: 10.1007/s11999-016-4709-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Birjandinejad A, Ebrahimzadeh MH, Ahmadzadeh-Chabock H. Augmentation plate fixation for the treatment of femoral and tibial non-union after intramedullary nailing. Orthopedics. 2009;32:409. doi: 10.3928/01477447-20090511-12. [DOI] [PubMed] [Google Scholar]
- 18.Attum B, Douleh D, Whiting PS, White-Dzuro GA, Dodd AC, Shen MS, et al. Outcomes of distal femur nonunions treated with a combination nail/plate construct and autogenous bonegrafting. J Orthop Trauma. 2017;31:e301–4. doi: 10.1097/BOT.0000000000000926. [DOI] [PubMed] [Google Scholar]
- 19.Kanabur P, Sandilands SM, Whitmer KK, Owen TM, Coniglione FM, Shuler TE. Nail and locking plate for periprosthetic fractures. J Orthop Trauma. 2017;31:e425–31. doi: 10.1097/BOT.0000000000000939. [DOI] [PubMed] [Google Scholar]
- 20.Hussain MS, Dailey SK, Avilucea FR. Stable fixation and immediate weight-bearing after combined retrograde intramedullary nailing and open reduction internal fixation of noncomminuted distal interprosthetic femur fractures. J Orthop Trauma. 2018;32:e237–40. doi: 10.1097/BOT.0000000000001154. [DOI] [PubMed] [Google Scholar]
- 21.Liporace FA, Yoon RS. Nail plate combination technique for native and periprosthetic distal femur fractures. J Orthop Trauma. 2019;33:e64–8. doi: 10.1097/BOT.0000000000001332. [DOI] [PubMed] [Google Scholar]
- 22.Mirick Mueller GE. Nail-plate constructs for periprosthetic distal femur fractures. J Knee Surg. 2019;32:403–6. doi: 10.1055/s-0039-1683444. [DOI] [PubMed] [Google Scholar]
- 23.Park KH, Oh CW, Park IH, Kim JW, Lee JH, Kim HJ. Additional fixation of medial plate over the unstable lateral locked plating of distal femur fractures: A biomechanical study. Injury. 2019;50:1593–8. doi: 10.1016/j.injury.2019.06.032. [DOI] [PubMed] [Google Scholar]
- 24.Lee JH, Park KC, Lim SJ, Kwon KB, Kim JW. Surgical outcomes of simple distal femur fractures in elderly patients treated with the minimally invasive plate osteosynthesis technique: Can percutaneous cerclage wiring reduce the fracture healing time? Arch Orthop Trauma Surg. 2020;140:1403–12. doi: 10.1007/s00402-020-03385-8. [DOI] [PubMed] [Google Scholar]
- 25.Tay YW, Hong CC, Murphy D. Functional outcome and mortality in nonagenarians following hip fracture surgery. Arch Orthop Trauma Surg. 2014;134:765–72. doi: 10.1007/s00402-014-1982-z. [DOI] [PubMed] [Google Scholar]
- 26.Kammerlander C, Riedmüller P, Gosch M, Zegg M, Kammerlander-Knauer U, Schmid R, et al. Functional outcome and mortality in geriatric distal femoral fractures. Injury. 2012;43:1096–101. doi: 10.1016/j.injury.2012.02.014. [DOI] [PubMed] [Google Scholar]
- 27.Hart GP, Kneisl JS, Springer BD, Patt JC, Karunakar MA. Open reduction vs distal femoral replacement arthroplasty for comminuted distal femur fractures in the patients 70 years and older. J Arthroplasty. 2017;32:202–6. doi: 10.1016/j.arth.2016.06.006. [DOI] [PubMed] [Google Scholar]