

Abstract
Extensive evidence has been found for the associations between personality traits and health. However, it remains unknown whether the relationships between personality and health show differential patterns across different life stages. The current research examined how the associations between the level of and changes in the Big Five personality traits and different types of health outcomes (self-rated, physical, and physiological health outcomes) differ across ages over the lifespan (Sample 1, age range: 15-100) and during the aging process (Sample 2, age range: 50-109) in particular. Using data from the two large longitudinal studies - the Household, Income and Labor Dynamics in Australia Survey (HILDA) and the Health and Retirement Study (HRS), we observed three important patterns. First, levels of and changes in personality traits were significantly associated with health across different life phases, and these effects were observed even in very old ages. Second, overall, the prospective relations between personality traits/changes in personality traits and health outcomes increased in strength in mid adulthood and/or early stages of late adulthood; however, the strength of their connections diminished in very old ages. Finally, there were some trait-specific and health outcome-specific patterns in the age-differential associations between personality and health. Findings from the current study contribute to enhancing our understanding of the personality-health link from a developmental perspective and provide critical information for the design and implementation of screening and interventions targeting health promotion.
Keywords: Personality, Health, Lifespan development, Aging, Longitudinal
It has been widely recognized that personality traits play crucial roles in health (Hill & Roberts, 2016; Murray & Booth, 2015; Smith, 2006) throughout adulthood until old age (Atherton et al., 2014; Graham et al., 2017; Mueller et al., 2018; Weston et al., 2015). Also, a general agreement has been reached that personality traits change across the life course (Graham et al., 2020; Roberts et al., 2006; Roberts & DelVecchio, 2000), and changes in personality also exert impacts on health (Hill & Roberts, 2016; Luo et al., 2022). However, it remains unknown to what degree personality traits are differentially connected to health at different ages. The current study addressed the following questions: First, are the associations between personality traits and health stable (in the same direction and of similar strength) over time? Second, if not, at what point in the adult lifespan are personality and health most strongly associated, and when does the personality-health link attenuate? Third, to what extent does the pattern for the possible age-differential associations between personality and health differ across different trait domains and different types of health outcomes? Answers to these questions will greatly enhance our understanding of how individual differences in health vary across the adult lifespan, and better uncover the role of dispositional factors in health from a lifespan perspective. Extending the investigation to changes in personality traits further tests the personality-health connection from a developmental perspective. Moreover, examining the differential associations between personality traits and health across ages may inform the prediction of health status among individuals in different life phases and provide critical information for the design and implementation of screening and interventions targeting health promotion. Therefore, the present research investigated the potential linear and quadratic moderating effects of age on the prospective associations between the Big Five personality traits (level and change) and different health outcomes (self-rated health, general disease level, and physiological health) in two samples from large longitudinal panel studies. Specifically, in Sample 1, we examined the age-differential relations between personality traits and health from a lifespan developmental perspective. Also, considering the importance of health challenges and rapid health changes during aging, in Sample 2, we zoomed in on individuals aged 50 and older to better scrutinize the age-related changes in the associations between personality traits and health outcomes in the aging population.
Theoretical Perspectives on Age Differences in the Personality-Health Associations
Personality-Health Associations across the Lifespan
Several theoretical frameworks have suggested that the connections between personality traits and health outcomes may become increasingly strong as people enter middle adulthood and/or late adulthood. For example, according to the theory of selective optimization with compensation (SOC; Baltes, 1997; Baltes & Smith, 2003), developmental processes include both gains and losses, and there is an age-associated loss in biological potential. Due to the decline in biological potentials, there is an age-related increase in the need for culture-based compensations to generate and maintain high levels of functioning, suggesting a moderating effect of age on the culture-health link such that the impact of culture becomes increasingly salient to health among older people. According to the Baltes (1997), culture refers to the entirety of psychological, social, material, and symbolic resources. Although the SOC theory was proposed for culture in general, as the author of the SOC theory indicated (Baltes, 1997), the predicted developmental pattern could be applied to a wide range of physical, psychological, and social resources. Therefore, it may be well applied to the link between personality traits and health outcomes as personality has been demonstrated as powerful psychological resources to health, both theoretically and empirically (Friedman et al., 2010; Goodwin & Engstrom, 2002; Goodwin & Friedman, 2006; Murray & Booth, 2015; Smith, 2006). Moreover, personality traits may increasingly function as compensatory resources as biological resources decline with age. For example, high conscientiousness may display compensatory effects by promoting health behavior engagement and medical adherence (Bogg & Roberts, 2004; Hill & Roberts, 2011), while low neuroticism contributes to health by protecting people from stressful experiences and feelings of distress as they age (Luo et al., 2023; Shackman et al., 2016). Higher levels of extraversion and agreeableness may also compensate for decreases in biological potentials by benefiting interpersonal relationships, resulting in more social support and resources (Graziano & Habashi, 2015; Wilkowski & Ferguson, 2014).
A similar pattern is also implied by the resource substitution hypothesis (Mirowsky & Ross, 2003), which states that the beneficial effects of resources on health are more salient among individuals with fewer alternatives. The resource substitution hypothesis indicates that personal education has more substantial influences on individuals’ health among those with less educated parents (Mirowsky & Ross, 2003; Ross & Mirowsky, 2011). Although originally formulated with reference to education, recent research has shown that personality traits can also show compensatory effects when alternative resources are limited. For example, personality traits have been found to show compensatory effects to background disadvantage in predicting status attainment such as annual income (Damian et al., 2015). As discussed above, as people age, personality traits may compensate for biological declines because of their connections to health-promoting behaviors and experiences, leading to stronger connections between personality and health in older ages.
More recently, the Life Course of Personality Model (LCP Model; Shanahan et al., 2014) was proposed for the association between the personality trait, conscientiousness, and health across different stages of life course in particular. The LCP model suggests that conscientiousness plays a crucial role in the promotion of health and avoidance of diseases throughout the life course, spanning from childhood, adolescence to adulthood. However, conscientiousness may become increasingly consequential to different health processes as people enter middle adulthood and/or early stage of late adulthood, given that aging processes introduce new challenges and the maintenance of health becomes more and more important during those life stages. In addition, conscientiousness is likely to increasingly distinguish people based on their health status over time because individuals who differ in conscientiousness engage in different behaviors (e.g., individuals high on conscientiousness are more likely to engage in health behaviors that are beneficial for health) on a day-to-day basis, the cumulative effects of which gives rise to diverging pathways of health. Therefore, consistent with the pattern predicted by the SOC theory and the resource substitution hypothesis, the LCP model also suggests a moderating role of age in the conscientiousness-health association such that there are increases in the strength of the connections between conscientiousness and health outcomes as people enter middle adulthood and/or early stage of late adulthood.
In sum, the theoretical notions suggest that there may be age-differential patterns in the personality-health link such that personality and health are increasingly tied to each other as people enter middle and/or late adulthood. However, while the LCP model proposes the age-differential associations between personality and health for the trait domain of conscientiousness in particular, other theoretical frameworks (e.g., the SOC theory) have hypotheses for cultural factors (including personality) in general. Thus, it remains to be examined to what extent the hypotheses can be applied to personality traits in different trait domains. In addition, there is also a lack of understanding of whether the patterns can be applied to different types of health outcomes (e.g., self-rated health, disease level).
Personality-Health Associations during the Aging Process
While the theoretical frameworks typically depict an amplifying importance of personality to health as people age, there has also been a clear call to further distinguish between the young-old (a period roughly from 65 to 85, also referred as the Third Age) and the oldest-old (starting approximately from the mid 80’s, also referred as the Fourth Age) age in late adulthood (Baltes & Smith, 2003; Mueller et al., 2018). The importance of differentiating the young-old and oldest-old age was also emphasized by the SOC theory and the LCP model as the two aging phases are qualitatively different from each other (Baltes, 1997; Baltes & Smith, 2003; Mueller et al., 2018; Shanahan et al., 2014). Specifically, according to previous research, in the young-old age, despite decreases in biological potentials, individuals still possess remarkable plasticity such that it is possible for compensatory resources, such as personality traits, to offset the biological losses and provide support to maintain adequate levels of functioning. In contrast, the oldest-old age is characterized by decrements across multiple domains of functioning and compared to those in the young-old ages, individuals in the oldest-old age are at a substantially higher risk of severe functional impairments (Baltes, 1997; Baltes & Smith, 2003; Mueller et al., 2018; Smith & Ryan, 2016). Based on the SOC theory and the LCP model (Baltes & Smith, 2003; Shanahan et al., 2014), the oldest-old age is highly vulnerable and change-resistant. Therefore, the effects of compensatory resources are likely to dissipate in this life stage because of the sharply decreased biological plasticity that limits their effectiveness and the overpowering force of biological processes of aging. Thus, scrutinizing the late adulthood, age may show moderating effects in a pattern that personality traits display increases in the strength of their associations with health outcomes in the young-old age due to their growing compensatory roles; however, the strength of the association decreases when people progress to the oldest-old age.
Taken together, different theoretical frameworks unanimously suggested the possibility that the associations between personality traits and health outcomes vary across different phases of the life course. Overall, we expected U-shaped relations (or inverted U-shaped relations depending on valence of the personality and health variables) between personality traits and health outcomes across ages over the lifespan and aging process such that the strength of their associations was strongest in midlife/young-old ages but diminished in the oldest-old phase. Identifying such an age-differential pattern requires sufficiently large sample sizes at different life phases. Most previous studies that sampled participants at different ages have a relatively smaller number of participants in late adulthood, especially in the oldest-old stage, leading to reduced power to detect the potential discrepancy between the young-old and oldest-old phases. Thus, in the current study, in addition to Sample 1 which included participants across different life stages, we also used data from an aging sample in which large sample sizes were available for both the young-old and the oldest-old age to afford us higher statistical power to detect potential decline in the associations between personality traits and health outcomes in the oldest-old age.
Empirical Findings on Age Differences in the Personality-Health Associations
According to previous research, some evidence was provided for the moderating effects of age on the personality-health link. For example, Canada et al. (2016) found that the associations between neuroticism and difficulties in performing daily physical activities were stronger in older adults (age 65 and older) compared to those in their young or middle-aged life phases. Mueller (2018) also reported that in a sample of older adults, the predictive effects of neuroticism on functional health (indexed by measures of handgrip strength and close visual acuity) were stronger in the group of subjects aged from 70 to 84 than the group of subjects who were 85 years or older. However, no difference in the predictive effects of extraversion was found between the two groups. When different age ranges were used to group participants, the effects of neuroticism and extraversion on perceived health and functional status were reported to be stronger in participants aged 75 and older than those aged between 60 and 74 (Duberstein et al., 2003). In contrast, other studies found relatively stable effects of personality traits, such as conscientiousness, dispositional forgiveness and gratitude, on self-rated health across adulthood (Hill & Allemand, 2011; Hill & Roberts, 2011; Hill et al., 2013).
In addition to the levels of personality traits assessed at certain time points, research has started to paying attention to changes in personality traits. Extensive evidence has suggested that personality traits change over the adult life span, with changes occurring even in late adulthood (Berg & Johansson, 2014; Graham et al., 2020; Kandler et al., 2015). Moreover, changes in personality traits have been shown to predict various health outcomes. For example, increases in neuroticism were related to higher mortality rates at a given age in older adults (Mroczek & Spiro, 2007). Other studies consistently reported evidence that increases in negative traits (e.g., neuroticism and impulsivity) and decreases in positive traits (e.g., conscientiousness and extraversion) were associated with higher risks of developing disease, having poorer self-perceived mental and physical health, and experiencing increases in work reduction due to physical health problems (Magee et al., 2013; Sutin et al., 2013; Turiano et al., 2012). However, very few studies have been conducted to examine the moderating effects of age on the links between changes in personality traits and health. One exception is Magee et al. (2013) who found that the effects of changes in personality traits over 4 years (measured on 2 occasions) on self-perceived physical health were generally found to be more salient in younger than older adults (participants were categorized into different age groups).
In sum, previous studies provided some preliminary evidence for the age-differential patterns in the personality-health associations. However, inconsistencies in the findings suggested that more research is needed.
Theoretical and Methodological Considerations for the Personality-Health Link across Ages
Several limitations have prevented researchers from drawing confident conclusions from prior work. First, only a limited number of personality trait domains and health outcomes were tested in previous studies. It is possible that there are trait-specific and/or health outcome-specific patterns that lead to the inconsistent findings. As we discussed, it remains to be examined to what extent the hypotheses can be applied across different personality trait domains and different types of health outcomes.
Second, most of the previous studies modeled age in a categorical rather than continuous way or only examined the linear moderating effects of age on the personality-health link. Such designs may obscure important patterns and lead to inaccurate conclusions. The SOC theory (Baltes, 1997) and the LCP Model (Shanahan et al., 2014) suggest that personality and health are likely to be increasingly tied to each other as people enter midlife or early stages of late adulthood but show attenuating connections in very old ages. Thus, there may be curvilinear patterns in their associations. It is essential that both linear and curvilinear effects of age are tested to better uncover the nuances in the personality-health link across the life course.
Third, different age ranges were used by each of these previous studies and most of them were restricted to certain life stages. To better examine the patterns of the personality-health associations, a wide range of ages (e.g., different phases across the life course) should be covered. Furthermore, previous research usually treated the young-old and oldest-old stages as a homogeneous group and rarely differentiated the two aging stages from each other. According to the SOC theory, it is crucial to distinguish between the young-old and oldest-old ages in late adulthood due to the potential differential importance of psychological factors to health. Relatedly, as the moderating effects of age are likely to be small (Hill & Roberts, 2016), it is important to have adequate sample sizes in ages in each life stage to detect the effects with sufficient power. Therefore, compared to previous work, in the present study, we used data from larger samples, including data from an aging sample with sufficient participants in both the young-old and the oldest-old phases, to ensure greater power to detect the effects.
Fourth, there is still a lack of understanding of how changes in personality traits and health are also contingent upon age. Research has shown changes in personality traits across different life phases (Bleidorn et al., 2019; Lucas & Donnellan, 2011; Roberts et al., 2006), with changes observed even in very old ages (Graham et al., 2020; Kandler et al., 2015; Mõttus et al., 2012). Thus, it is important to examine whether the patterns of the age-differential personality-health links proposed by previous theories are also applicable to changes in personality traits. Meanwhile, for personality-based interventions that target health prevention and promotion through triggering positive changes in personality traits (Chapman et al., 2014), understanding the degree of relevance of changes in personality traits to health is key to improving efficacy of the interventions.
The Current Study
The current study aimed to test the moderating effects of age (linear and quadratic effects) on the associations between the Big Five personality traits and health outcomes (self-rated health, general disease level, and physiological health indicator) in two samples using Moderated Nonlinear Factor Analysis (MNLFA; Bauer, 2017). Specifically, given the broad range of age across different life stages covered, we examined how the associations between the Big Five personality traits and health outcomes vary across ages over the life course (Age 19 - Age 97) using data from the Household, Income and Labor Dynamics in Australia Survey (HILDA). We also used data from the Health and Retirement Study (HRS, 2006-2016; the HRS is sponsored by the National Institute on Aging and is conducted by the University of Michigan) to zoom into the possible age-related differential associations between the Big Five personality traits and health outcomes during aging (Age 50 and older) in particular. This is because of the increasing salience of health challenges as people age, identifying factors that may be risky or protective to health becomes particularly important. Furthermore, the theoretical frameworks (e.g., SOC theory, LCP model) posit the importance of differentiating between the young-old and oldest-old age in late adulthood and suggest that the relations between personality traits and health are likely to vary across these stages (Baltes & Smith, 2003; Mueller et al., 2018; Shanahan et al., 2014). Compared to HILDA, much larger sample sizes were available in HRS for individuals in the young-old and oldest-old phases of late adulthood across ages, allowing us to better scrutinize the nuances of the personality-health association during the aging process. Rather than comparing and replicating results in two samples, the findings from the two samples served the aims of the present study in a complimentary way. By integrating their results, our approach of using these two samples allowed us to investigate the increasing salience of health challenges as people age, helping identify the particular importance of personality trait domains that may be deleterious to or protective of health across different stages of adulthood.
In both samples, analyzed separately, we first examined the concurrent (personality traits and health outcomes measured in the same wave) and prospective (personality traits measured in one wave and health outcomes measured 4 years later) associations between personality traits and health outcomes across ages. Compared to concurrent analyses, the prospective design allows researchers to obtain more accurate estimates of the personality-health relationship because it is likely that the effects of personality on health are better manifested after accumulating over time and the biasing impact of common method bias can be reduced substantially, thus laying stronger groundwork for future research to examine the causal relations between personality traits and health across ages. From a practical perspective, prospective design can better inform the implementation of early screening and prevention for potential health problems. Thus, in the subsequent sections, we focus on the prospective analyses. Details about the concurrent analyses and results can be found in the online supplemental material. Although personality traits are generally considered predisposing factors in the theoretical models reviewed, we note that the current study did not aim to make any causal inferences (more in the Discussion section). Next, given the availability of longitudinal assessments of personality traits, we conducted longitudinal analyses to test the moderating effects of age on the associations between changes in the Big Five personality traits across multiple waves and health outcomes measured together with the last-wave assessment of personality traits. Based on previous theoretical frameworks on the personality-health link across the life course, we hypothesized that, overall, the strength of the prospective associations between personality traits and health would increase with age in middle-aged and young-old life stages but decrease in very old age.
Method
Transparency and Openness
Data from HILDA and HRS are available via request/publicly available and the use of which is declared by Northwestern University as exempt IRB review. Data request/data of HILDA and HRS and prior publications used the data can be found at the websites of the studies (HILDA: https://melbourneinstitute.unimelb.edu.au/hilda; HRS: https://hrs.isr.umich.edu/about). All the analyses scripts can be found at https://osf.io/582ek/?view_only=3c106e1812b143e09b0674be85e55bf2.
Participants
Household Income and Labour Dynamics in Australia (HILDA).
The HILDA is an Australian household-based panel study that collects data on health, personal well-being, education, employment, and family life over the life course. Data collection began in 2001, and new measurement occasions occur every four years. In total, four waves of personality assessment were available in HILDA. In the prospective analyses, a sample of 16,063 participants (53.1% female) who provided data on the Big Five personality traits and at least one of the health outcomes (self-rated health and general disease level) was included. Personality traits were measured in the fifth (2005), ninth (2009), and thirteenth (2013) waves of assessment and were paired with self-rated health and general disease level assessed in the ninth (2009), thirteenth (2013), and seventeenth (2017) waves of assessment, resulting in a 4-year interval between personality measures and physical health assessments. For participants who provided assessments in multiple waves, we used participants’ first available personality measures and their health measured 4 years later (thus each participant’s personality responses were included in the analyses only once despite that many provided multiple waves). Timelines for assessments of personality and health outcomes used in the prospective analyses for HILDA are presented in Figures S1a. The mean age of the sample was 44.91 (SD = 18.17, Range: 19-97) at the time of health assessment (see Figure S2a for the distribution of age). 74% of the sample received at least 12 years of education or Certificate III or IV (courses require the completion of Year 10 and Year 11 education, respectively).
In the longitudinal analyses (in which changes in personality traits were tested), a sample of 16,788 participants (52.9% female) who provided data on personality traits in at least one of the four waves and at least one of the health outcomes (self-rated health and general disease level) was included. For physical health outcomes, personality traits measured in the fifth (2005), ninth (2009), thirteenth (2013), and seventeenth (2017) waves (6,468 participants provided data in all 4 waves) and self-rated health and general disease level assessed in the seventeenth (2017) wave of assessment were used. Timelines for assessments of personality and health outcomes used in the longitudinal analyses for HILDA are presented in Figures S1b.The mean age of the sample was 45.65 (SD = 19.08, Range: 15-100) at the time of the last available health assessment (see Figure S2b for the distribution of age). 74.6% of the sample received at least 12 years of education or Certificate III or IV.
The Health and Retirement Study (HRS).
The HRS is a longitudinal study of a representative American sample of participants (and their spouses) aged 50 years and older (Burkhauser & Gertler, 1995), aiming to investigate the challenges and opportunities of aging. In the prospective analyses, a sample of 16,404 participants (59.4% female) who had data on the Big Five personality traits and at least one of the health outcomes (self-rated health, general disease level, and allostatic load) was included. Specifically, personality data drawn from the eighth to the eleventh (measured in 2006, 2008, 2010, and 2012) waves were paired with health outcomes assessed 4 years later (from the tenth to the thirteenth waves in 2010, 2012, 2014, and 2016) (Health and Retirement Study, 2013a, 2013b, 2014, 2015a, 2015b, 2017a, 2017b, 2020a, 2020b, 2021a, 2021b, 2022). To maximize the sample size, for participants who provided assessments in multiple waves, we used participants’ first available personality measures and their health measured 4 years later. Timelines for assessments of personality and health outcomes used in the prospective analyses for HRS are presented in Figures S3a.The mean age of the sample was 69.13 (SD = 10.23, Range: 50-109) at the time of health assessment (see Figure S2c for the distribution of age). On average, the participants reported 12.73 (SD = 3.15) years of education.
In the longitudinal analyses, a sample of 15,322 participants (59.7% female) who provided data on personality traits in at least one of the three waves and on at least one of the health outcomes at Time 3 were included. In HRS, half of the participants completed psychosocial measures in 2006, 2010, and 2014, and the other half completed the measures in 2008, 2012, and 2016. The two samples were combined to maximize sample size in the longitudinal analyses such that personality traits were assessed every 4 years at 3 time points. A total of 7,313 participants had personality data at all 3 time points. Timelines for assessments of personality and health outcomes used in the longitudinal analyses for HRS are presented in Figures S3b.The mean age of the sample was 69.67 (SD = 10.52, Range: 50-104) at the time of health assessment (Time 3; see Figure S2d for the distribution of age). On average, the participants reported 12.79 (SD = 3.19) years of education.
We ran a series of attrition analyses to test whether dropouts resulted in unrepresentative longitudinal samples among participants who had usable personality data at Time 1 in both HILDA and HRS. Details can be found in the online supplemental material. In general, compared to participants who had personality at some (but not all) of the time points, those who provided data on all waves of the assessments had slightly lower scores on neuroticism and higher scores on conscientiousness (t = −4.50, p < .001, d = −.13 for neuroticism and t = 8.38, p < .001, d = .24 for conscientiousness in HILDA; t = −6.70, p < .001, d = −.16 for neuroticism and t = 7.90, p < .001, d = .19 for conscientiousness in HRS). Differences on other variables (e.g., education, gender, extraversion) were generally small.
Measures
Personality.
HILDA. The Big Five personality traits were measured by 28 adjectives derived based on a brief version of the Goldberg’s Big Five Markers Scale (Saucier, 1994). Each adjective was rated on a seven-point scale with 1 as “does not describe me at all” and 7 as “describes me very well”. Across the 4 waves used in the current study, Cronbach alphas ranged from 0.80 to 0.81 for neuroticism, 0.75 for extraversion across waves, from 0.78 to 0.79 for conscientiousness, from 0.77 to 0.78 for agreeableness, and from 0.74 to 0.75 for openness. HRS. The Big Five personality traits were measured by 26 adjectives using the MIDUS Big Five Adjectival scale (Lachman & Bertrand, 2001). Each adjective was rated on a four-point scale with 1 as “a lot” and 4 as “not at all”. Across the 3 waves, Cronbach alphas ranged from 0.71 to 0.72 for neuroticism, 0.75 for extraversion across waves, from 0.65 to 0.66 for conscientiousness, from 0.78 to 0.79 for agreeableness, and from 0.79 to 0.81 for openness.
Self-Rated Health.
In both HILDA and HRS, Self-rated health was measured by a single item asking participants to rate their general health status as poor, fair, good, very good, or excellent. The item was coded such that higher scores represented better perceived health states.
General Disease Level.
HILDA. General disease level was estimated as the sum of participants’ endorsement on items about diagnoses of different types of conditions that had persisted or were likely to persist for 6 months or more, including heart/coronary disease, high blood pressure/hypertension, Type 1 and Type 2 diabetes, any type of cancer, arthritis, lung conditions (asthma, chronic bronchitis, or emphysema), and other circulatory conditions. The total score ranged from 0 to 9. HRS. General disease level was computed as the total scores of participants’ endorsement on items about diagnoses of different conditions, including heart condition, high blood pressure, diabetes, any type of cancer, arthritis, lung disease, and stroke. The total score ranged from 0 to 7.
Allostatic Load.
Allostatic load was examined only in HRS. Physiological measures and biomarkers were used to index allostatic load. Cardiovascular functioning was assessed by systolic and diastolic blood pressure. The functioning of metabolic systems was measured by waist circumference, hemoglobin A1C (HbA1C), high density lipoprotein cholesterol (HDL), total cholesterol (TC), and cystatin C. C-reactive protein (CRP) was used as a marker of inflammatory reactions. Consistent with previous studies (McEwen, 2000; Seeman et al., 1997; Stephan et al., 2016), allostatic load index was computed by averaging z-scores of the 8 indicators, and higher values indicate higher dysregulation of the physiological systems.
Statistical Analysis
All the analyses were conducted using Mplus 8.5 (Muthen & Muthen, 1998-2017). Full information maximum likelihood (FIML) was used for estimation due to missing data across waves. Measurement invariance for each Big Five personality trait across waves was tested in each sample. Details about the analyses and results (see Table S1) can be found in online supplementary materials. Overall, consistent with previous research using these data (e.g., Chereches et al., 2022), measurement invariance was confirmed for all traits in both samples at the configural, metric, and scalar levels of analyses.
To examine the moderating effects of age on the prospective associations between each of the Big Five personality traits and health outcomes (self-rated health, general disease level, and allostatic load), the moderated nonlinear factor analysis (MNLFA) models were fitted for each pair of personality traits and health outcomes. Figure 1a displays the conceptual illustration of the model tested for the prospective personality-health link. In general, the MNLFA models allow model parameters, including latent means, latent variances, factor loadings, and covariances and correlations, to differ as a function of other variables on a continuous scale (Bauer, 2017). Researchers can regress these parameters on moderators to examine how the parameters change with moderators. Conceptually speaking, the moderation part is a regression model where parameter of interests is the Y (e.g., covariance) and the moderator variable is the X. If the regression slope is statistically significant, then we conclude that there is a significant moderation effect. The MNLFA model serves the purpose of the current study well to examine the moderating role of age by testing the degree to which the covariances between personality traits and health outcomes are variant/invariant across ages. Contrasting to the traditional moderation test (e.g., creating interaction terms of predictors and moderators) in which predictors and moderators are statistically indistinguishable from each other, the MNLFA model allows for direct translation of our research question into statistical models by using age to predict the covariance between personality and health. In addition, compared to the traditional moderation test, the MNLFA better facilitates modeling and interpreting quadratic moderating effects of age (testing whether there were U-shaped/inverted U-shaped patterns in the covariances between personality traits and health outcomes across ages). In the current analyses, personality traits were modeled as latent variables with the items assessing the traits used as manifest indicators. To test the possible quadratic moderating effects of age on the prospective associations between personality traits and health outcomes, in each model, age (at the time of health assessment) and the squared age (age^2) were included as moderators of the means and variances of the personality trait and the health outcome and the covariance between the personality trait and the health outcome. If the quadratic moderating effects of age were found to be nonsignificant, models were refitted to test the linear moderating effects of age only (with age included as the only moderator). As recommended for modelling in Mplus, age (and age in the calculation for squared age) was centered around 50 and then divided by 10 to reduce the variance of age for better convergence (Muthen & Muthen, 1998-2017). To ensure that model-implied correlations between personality and health across ages do not exceed −1 and 1, we followed the recommendation by Bauer (2017) and tested the linear and quadratic effect of age on the Fisher’s z transformed correlation. To facilitate results interpretation, we transformed all Fisher’s zs back to the correlation metric in the Results section. The moderating effects of the quadratic or linear term of age on the prospective covariance between personality traits and health outcomes were the focus in this step of the analyses. Model fit indices (such as CFI, RMSEA) were not available for MNLFA models yet.
Figure 1a & 1b.
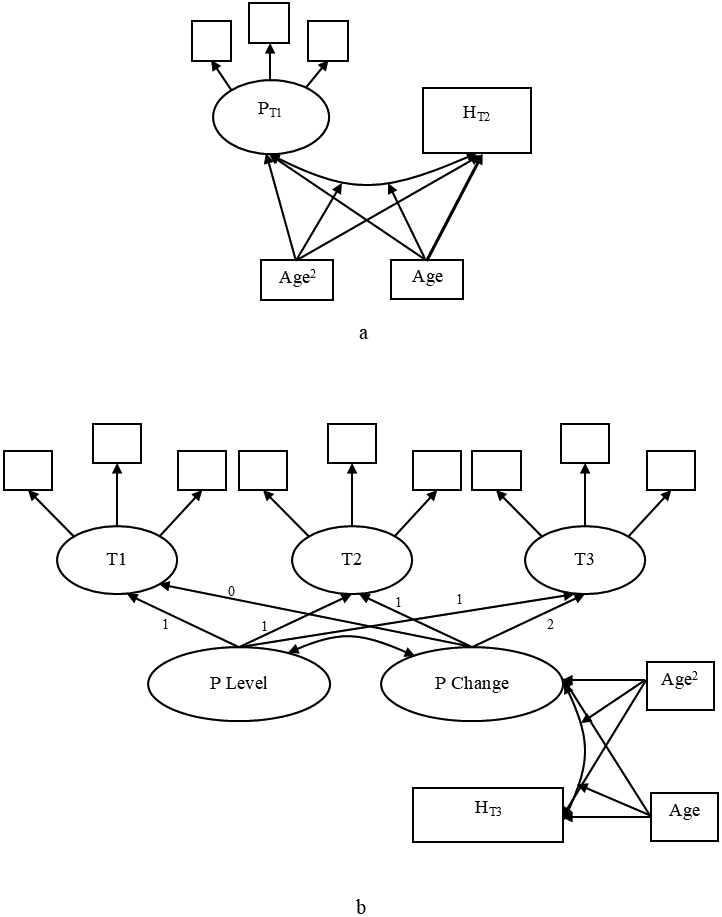
Conceptual overview of the moderated nonlinear factor analysis model to test the quadratic and/or linear moderating effects of age on the prospective association between personality traits/changes in personality traits and health outcomes. P = personality; H = health.
To test the moderating effects of age on the associations between changes in personality traits and health outcomes, in both the HILDA and the HRS samples (Figure 1b displays the conceptual illustration of the model tested for the link between changes in personality traits and health outcomes), latent growth models were fitted and the estimated slopes were then used to represent linear changes (only linear changes were modeled in the current study due to the limited number of time points) in personality traits across waves (see Table S2 for the means and variances of the slopes in the two samples). In each model, the latent variables for each of the Big Five personality traits were specified at each time point of assessment, and the latent variables were used to estimate the latent intercept and slope for each of the five personality traits. The intercept and slope parameters of the variables were set to correlate with each other. All the loadings and residual variance of the same item were fixed to be equivalent across waves. In the MNLFA models, the quadratic moderating effects of age on the covariance between changes in personality traits and health outcomes were tested by including both age and age^2 as moderators. Age was rescaled in the same way as discussed above. If nonsignificant effects were observed for the quadratic (age^2) term, models with only the linear moderating effects of age were refitted.
Results
Descriptive Results
The overall prospective correlations between the Big Five personality traits and the health outcomes tested in the two samples without considering the moderating effect of age are presented in Table 1. In general, high neuroticism was related to negative health outcomes (e.g., low self-rated health and high general disease level), whereas high extraversion, conscientiousness, agreeableness, and openness were related to positive health outcomes (e.g., high self-rated health, low general disease level and allostatic load). However, unexpectedly, in the models without age, neuroticism displayed a negative prospective association with general disease level, whereas conscientiousness and agreeableness were positively correlated with general disease level in HILDA.
Table 1.
Correlation coefficients and 95% confidence intervals for the prospective associations between the Big Five personality traits and health outcomes and the associations between changes in personality and health outcomes in the HILDA and the HRS samples (age as a moderator was not added).
| N | E | C | A | O | |
|---|---|---|---|---|---|
| Prospective Personality-Health Associations | |||||
| HILDA | |||||
| SRH | −.13* [−.15, −.11] | .13* [.11, .15] | .11* [.09, .13] | .05* [.03, .07] | .04* [.02, .06] |
| GDL | −.09* [−.11, −.07] | −.05* [−.08, −.03] | .04* [.02, .06] | .07* [.05, .09] | −.05* [−.07, −.03] |
| HRS | |||||
| SRH | −.26* [−.28, −.24] | .23* [.22, .25] | .29* [.27, .31] | .11* [.09, .13] | .20* [.19, .22] |
| GDL | .12* [.10, .14] | −.10* [−.11, −.08] | −.17* [−.19, −.16] | −.02 [−.04, .00] | −.10* [−.12, −.08] |
| AL | −.01 [−.03, .01] | −.06* [−.08, −.04] | −.13* [−.15, −.11] | −.05* [−.07, −.03] | −.04* [−.06, −.02] |
| Personality Change-Health Associations | |||||
| HILDA | |||||
| SRH | −.07* [−.11, −.03] | .09* [.05, .13] | .20* [.16, .24] | .14* [.09, .18] | .07* [.03, .12] |
| GDL | −.11* [−.17, −.06] | .09* [.03, .15] | −.08* [−.13, −.03] | −.16* [−.22, −.10] | −.14* [−.20, −.08] |
| HRS | |||||
| SRH | −.13* [−.18, −.09] | .25* [.20, .31] | .23* [.17, .28] | .20* [.14, .27] | .25* [.22, .28] |
| GDL | .06* [.02, .09] | −.17* [−.21, −.12] | −.17* [−.22, −.12] | −.13* [−.18, −.07] | −.22* [−.32, −.13] |
| AL | .01 [−.04, .05] | −.11* [−.16, −.05] | −.09* [−.13, −.04] | −.10* [−.16, −.04] | −.09* [−.16, −.01] |
Note. N = neuroticism; E = extraversion; C = conscientiousness; A = agreeableness; O = openness; SRH = self-rated health; GDL = general disease level; AL = allostatic load. *p ≤ .05.
Table 1 also presents the overall correlations between Big Five personality trait change (operationalized as slopes in the latent growth models) and health outcomes in the HILDA and the HRS samples without considering the moderating effect of age. Overall, increases in neuroticism were correlated with negative health outcomes (e.g., low self-rated health and high general disease level), while increases in extraversion, conscientiousness, agreeableness, and openness were correlated with positive health outcomes (e.g., high self-rated health, low general disease level and allostatic load). Unexpectedly, in HILDA, increases in neuroticism were linked to lower general disease level, whereas increases in extraversion were related to higher general disease level.
Personality and Health across the Lifespan (HILDA)
Self-Rated Health
We tested the moderating effects of age on the concurrent and prospective associations between the Big Five personality traits and health outcomes. Results for concurrent analyses are presented in the online supplement (see the section for “sample information and results for the concurrent analyses”, Tables S3-S5, and Figures S4-S5). Table 2 presents the unstandardized parameter estimates for the quadratic (age2 in quadratic effect test) and/or linear (age in linear effect test) moderating effects of age on the prospective associations between the Big Five personality traits and self-rated health and the relations between changes in personality traits and self-rated health in the HILDA sample (baseline estimates refer to the relations between personality traits and self-rated health at age 50). Figure 2 displays the model-implied prospective correlations between personality traits, changes in personality traits and self-rated health across ages plotted based on parameters estimated from the MNLFA model in HILDA. As shown in Table 3 and Figure 2, when examined across the life course, age showed significant quadratic moderating effects on the prospective links between neuroticism and openness and self-rated health. Specifically, a U-shaped prospective association was observed between neuroticism and self-rated health across ages such that the strength of their negative association was strongest in midlife and decreased during old ages. Across the lifespan, the positive prospective link between openness and self-rated health was weak at earlier ages but became stronger as individuals aged (after age 60). Age demonstrated a linear moderating effect on the prospective connection between conscientiousness and self-rated health. As shown in Figure 2, the positive association between conscientiousness and self-rated health weakened across ages. No significant moderating effects of age were found for extraversion and agreeableness such that the two trait domains exhibited stable prospective relations to self-rated health over time.
Table 2.
Parameter estimates and 95% confidence intervals for the quadratic and linear moderating effects of age on the prospective covariances between personality traits and self-rated health and general disease level and the covariance between changes in personality traits and self-rated health and general disease level in HILDA.
| Quadratic Effect Test | Linear Effect Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Age2 | 95% CI | p-value | Age | 95% CI | p-value | Baseline | Age | 95% CI | p-value | |
| Self-Rated Health | |||||||||||
| HILDA: prospective | |||||||||||
| Neuroticism | −.228* | .006* | [.001, .011] | .026 | .005 | [−.005, .015] | .300 | / | / | / | / |
| Extraversion | .108* | .000 | [−.005, .006] | .875 | .008 | [−.002, .018] | .125 | .109* | .008 | [−.002, .018] | .127 |
| Conscientiousness | .177* | −.002 | [−.007, .003] | .450 | −.012* | [−.022, −.002] | .022 | .172* | −.010* | [−.020, −.001] | .037 |
| Agreeableness | .071* | .002 | [−.003, .007] | .501 | −.005 | [−.015, .005] | .299 | .078* | −.006 | [−.015, .004] | .248 |
| Openness | .010 | .006* | [.000, .011] | .040 | .020* | [.010, .030] | <.001 | / | / | / | / |
| HILDA: change | |||||||||||
| Neuroticism | −.028* | −.002 | [−.006, .003] | .440 | .020* | [.011, .028] | <.001 | −.039* | .019* | [.011, .027] | / |
| Extraversion | .045* | .010* | [.004, .016] | .001 | −.020* | [−.032, −.009] | .001 | / | / | / | / |
| Conscientiousness | .101* | −.002 | [−.007, .003] | .420 | −.025* | [−.035, −.015] | <.001 | .095* | −.023* | [−.033, −.014] | .019 |
| Agreeableness | .051* | .005* | [.000, .009] | .047 | −.009 | [−.018, .000] | .053 | / | / | / | .395 |
| Openness | .029 | .004 | [−.001, .009] | .164 | .008 | [−.002, .018] | .123 | .043* | .007 | [−.003, .017] | .106 |
| General Disease Level | |||||||||||
| HILDA: prospective | |||||||||||
| Neuroticism | .112* | −.007* | [−.014, −.001] | .033 | .016* | [.004, .028] | .011 | / | / | / | / |
| Extraversion | −.031* | .007* | [.000, .013] | .040 | −.005 | [−.017, .007] | .437 | / | / | / | / |
| Conscientiousness | −.087* | .003 | [−.003, .009] | .348 | −.020* | [−.032, −.008] | .001 | −.094* | −.016* | [−.029, −.003] | .019 |
| Agreeableness | .034* | −.001 | [−.007, .006] | .825 | −.009 | [−.020, .003] | .162 | .021 | −.006 | [−.018, .007] | .395 |
| Openness | .015 | −.001 | [−.008, .005] | .734 | −.006 | [−.018, .006] | .337 | .010 | −.011 | [−.024, .002] | .106 |
| HILDA: change | |||||||||||
| Neuroticism | .008 | −.013* | [−.019, −.007] | <.001 | .045* | [.033, .057] | <.001 | / | / | / | / |
| Extraversion | .014 | .005 | [−.003, .013] | .190 | −.031* | [−.048, −.015] | <.001 | .033 | −.037* | [−.056, −.018] | <.001 |
| Conscientiousness | −.027 | .003 | [−.004, .009] | .399 | −.031* | [−.044, −.017] | <.001 | −.011 | −.026* | [−.041, −.011] | .001 |
| Agreeableness | −.069* | −.004 | [−.010, .002] | .200 | .001 | [−.012, .014] | .903 | −.094* | .004 | [−.010, .018] | .593 |
| Openness | −.055* | −.003 | [−.009, .004] | .404 | .010 | [−.004, .024] | .173 | −.073* | .012 | [−.003, .028] | .125 |
Note. *p ≤ .05. “ / ” indicates that models aiming to test the linear moderating effects of age only were not fitted as the quadratic moderating effects of age were found to be significant.
Figure 2.

The prospective correlations between the Big Five personality traits and self-rated health and general disease level and the correlations between changes in the Big Five personality traits and self-rated health and general disease level across ages in the HILDA sample. N = neuroticism; E = extraversion; C = conscientiousness; A = agreeableness; O = openness. Dashed lines represent statistically nonsignificant moderating effect of age (neither linear nor quadratic).
Table 3.
Summary of results for the prospective associations between the Big Five personality traits and changes in personality traits and health outcomes in HILDA.
| HILDA | |||
|---|---|---|---|
| Age2 | Age | Pattern Summary | |
| Self-Rated Health | |||
| N prospective | √ | negative relations increased in midlife but decreased in old ages | |
| N change | √ | negative relations decreased over the lifespan | |
| E prospective | positive relations were stable over the lifespan | ||
| E change | √ | positive relations decreased across ages but increased in old ages | |
| C prospective | √ | positive relations decreased over the lifespan | |
| C change | √ | positive relations decreased over the lifespan | |
| A prospective | positive relations were stable over the lifespan | ||
| A change | √ | positive relations decreased across ages but increased in old ages | |
| O prospective | √ | positive relations increased after 60’s | |
| O change | weak positive relations were stable over the lifespan | ||
| General Disease Level | |||
| N prospective | √ | positive relations increased over time but decreased after 60’s | |
| N change | √ | negative relations decreased before midlife and flattened | |
| E prospective | √ | weak relations over the lifespan despite a significant quadratic effect | |
| E change | √ | positive relations decreased and weak negative relations emerged and increased since midlife | |
| C prospective | √ | negative relations increased over the lifespan | |
| C change | √ | weak negative relations emerged and increased since midlife | |
| A prospective | weak and stable relations over the lifespan | ||
| A change | stable negative relations over the lifespan | ||
| O prospective | weak and stable relations over the lifespan | ||
| O change | stable negative relations over the lifespan | ||
Note. “Age2” is marked when significant quadratic moderating effects of age were found; “Age” is marked when significant linear moderating effects of age were found (with nonsignificant quadratic moderating effects). The strength of the relation is identified as weak when the magnitude is smaller than .05 most of the time over the lifespan. Relations smaller than .05 in strength were reported to be ranked below the 20th percentile in psychological research (Bosco et al., 2015). N = neuroticism; E = extraversion; C = conscientiousness; A = agreeableness; O = openness.
As Table 2 shows, when examined across the life span in HILDA for changes in personality traits, age demonstrated significant quadratic effects on the links between changes in extraversion and changes in agreeableness and self-rated health. As shown in Figure 2, after decreasing across younger and middle adulthood, the strength of the associations between changes in extraversion and changes in agreeableness and self-rated health went up in old ages such that the beneficial effects of elevation in extraversion and agreeableness on self-rated health were increasingly salient as people aged. In contrast, age exhibited significant linear effects on the relations between changes in neuroticism and changes in conscientiousness and self-rated health. As plotted in Figure 2, relative to young ages, the strength of the association between increases in neuroticism and lower levels of self-rated health, as well as the association between increases in conscientiousness and higher levels of self-rated health, diminished across ages. Increases in openness showed stable but weak relations to better self-related health across ages.
General Disease Level
As shown in Table 2, overall, the strength of the prospective associations between personality traits and general disease level were weaker than that for self-rated health. We detected significant quadratic effects of age on the prospective relations between neuroticism and extraversion and general disease level over the life course. The positive relation between neuroticism and general disease level increased in magnitude over time but decreased after 60’s (See Figure 2). The prospective relation between extraversion and general disease level was generally weak despite the significant quadratic effect of age. Additionally, we found that the negative prospective association between conscientiousness and general disease level became stronger (more negative) in a linear way as age goes up. Generally, stable but very weak associations were found for openness or agreeableness across ages.
Regarding change in personality traits, in HILDA, age demonstrated a significant quadratic effect on the association between changes in neuroticism and general disease level (see Table 2). According to the pattern displayed in Figure 2, contrary to our expectation, changes in neuroticism were associated with general disease level in young adulthood, meaning that increasing neuroticism was associated with less disease; however, the magnitude of this association approached zero as people entered the midlife stage. Age also displayed significant linear effects on the relations between changes in extraversion and changes in conscientiousness and general disease level across the life course. As expected, increases in extraversion and conscientiousness were related to lower general disease level after midlife, and the strength of their association increased linearly from midlife through older adulthood. No significant moderating effects of age were found for changes in agreeableness and openness as increases in agreeableness and openness displayed stable associations with lower general disease level during aging.
Table 3 provides a summary of the age-differential patterns for the prospective associations between the Big Five personality traits and health outcomes, as well as the associations between changes in the Big Five personality traits and health outcomes, across the life course in HILDA.
Personality and Health in the Aging Process (HRS)
Self-Rated Health
Age demonstrated quadratic moderating effects on the prospective associations between neuroticism, conscientiousness, and openness and self-rated health in HRS. As Table 4 and Figure 3 present, starting from age 50, the strength of the prospective associations between the three personality traits (negative association for neuroticism and positive associations for conscientiousness and openness) and self-rated health increased and peaked around 70’s; however, the strength of the links decreased when individuals entered their 80’s. No significant moderating effects of age were observed for extraversion and agreeableness. The prospective connections between higher extraversion and agreeableness and better self-rated health remained stable as people aged.
Table 4.
Parameter estimates and 95% confidence intervals for the quadratic and linear moderating effects of age on the prospective covariances between personality traits and self-rated health, general disease level, and allostatic load and the covariance between changes in personality traits and self-rated health, general disease level, and allostatic load in HRS.
| Quadratic Effect Test | Linear Effect Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Age2 | 95% CI | p-value | Age | 95% CI | p-value | Baseline | Age | 95% CI | p-value | |
| Self-Rated Health | |||||||||||
| HRS: prospective | |||||||||||
| Neuroticism | −.266* | .018* | [.004, .033] | .014 | −.052 | [−.115, .011] | .107 | / | / | / | / |
| Extraversion | .206* | −.009 | [−.023, .006] | .238 | .038 | [−.026, .101] | .250 | .229* | .003 | [−.014, .020] | .589 |
| Conscientiousness | .307* | −.018* | [−.033, −.003] | .019 | .038 | [−.029, .106] | .261 | / | / | / | / |
| Agreeableness | .108* | −.002 | [−.016, .012] | .767 | .007 | [−.056, .070] | .823 | .112* | .000 | [−.017, .016] | .968 |
| Openness | .116* | −.025* | [−.039, −.011] | .001 | .102* | [.040, .165] | .001 | / | / | / | / |
| HRS: change | |||||||||||
| Neuroticism | −.130* | −.013 | [−.030, .003] | .110 | .065 | [−.006, .137] | .073 | −.088* | .010 | [−.009, .028] | .301 |
| Extraversion | .115* | −.013 | [−.030, .004] | .141 | .048 | [−.027, .123] | .209 | .156* | −.006 | [−.025, .014] | .569 |
| Conscientiousness | .100* | −.022* | [−.040, −.003] | .023 | .076 | [−.009, .160] | .081 | / | / | / | / |
| Agreeableness | .076* | −.013 | [−.030, .005] | .154 | .044 | [−.032, .121] | .254 | .118* | −.008 | [−.028, .011] | .396 |
| Openness | .139* | −.002 | [−.018, .014] | .836 | −.016 | [−.087, .055] | .666 | .140* | −.021* | [−.040, −.003] | .020 |
| General Disease Level | |||||||||||
| HRS: prospective | |||||||||||
| Neuroticism | .211* | −.003 | [−.017, .011] | .673 | −.018 | [−.080, .043] | .561 | .202* | −.027* | [−.045, −.010] | .002 |
| Extraversion | −.075* | .017* | [.002, .031] | .021 | −.057 | [−.119, .005] | .073 | / | / | / | / |
| Conscientiousness | −.169* | .026* | [.011, .041] | <.001 | −.064 | [−.129, .001] | .053 | / | / | / | / |
| Agreeableness | .025 | .016* | [.002, .030] | .022 | −.064* | [−.125, −.003] | .040 | / | / | / | / |
| Openness | −.024 | .023* | [.010, .037] | .001 | −.084* | [−.144, −.023] | .007 | / | / | / | / |
| HRS: change | |||||||||||
| Neuroticism | .073* | .003 | [−.013, .018] | .717 | −.039 | [−.108, .030] | .268 | .034 | −.017 | [−.037, .002] | .079 |
| Extraversion | −.026 | .016 | [.000, .031] | .057 | −.063 | [−.135, .009] | .085 | −.058* | −.003 | [−.023, .017] | .748 |
| Conscientiousness | −.060 | .020* | [.003, .038] | .021 | −.063 | [−.143, .018] | .127 | / | / | / | / |
| Agreeableness | .018 | .025* | [.009, .041] | .002 | −.097* | [−.168, −.026] | .008 | / | / | / | / |
| Openness | −.042 | .019* | [.004, .034] | .014 | −.060 | [−.128, .007] | .081 | / | / | / | / |
| Allostatic Load | |||||||||||
| HRS: prospective | |||||||||||
| Neuroticism | .020 | −.005 | [−.029, .018] | .660 | .000 | [−.101, .101] | .998 | .019 | −.012 | [−.035, .010] | .274 |
| Extraversion | −.149* | −.014 | [−.038, .010] | .242 | .075 | [−.026, .177] | .147 | −.124* | .023* | [.001, .044] | .036 |
| Conscientiousness | −.330* | −.017 | [−.043, .008] | .190 | .139* | [.032, .247] | .011 | −.328* | .082* | [.060, .105] | <.001 |
| Agreeableness | −.054 | .014 | [−.010, .038] | .247 | −.031 | [−.134, .071] | .547 | −.127* | .034* | [.012, .055] | .002 |
| Openness | .011 | .022 | [−.001, .046] | .060 | −.078 | [−.177, .021] | .122 | −.088* | .022* | [.001, .043] | .039 |
| HRS: change | |||||||||||
| Neuroticism | .034 | .014 | [−.011, .040] | .273 | −.051 | [−.165, .062] | .377 | −.037 | .018 | [−.006, .043] | .144 |
| Extraversion | −.051 | .027 | [.000, .055] | .054 | −.075 | [−.197, .047] | .227 | −.225* | .064* | [.039, .089] | <.001 |
| Conscientiousness | −.320* | −.038* | [−.069, −.006] | .019 | .211* | [.071, .352] | .003 | / | / | / | / |
| Agreeableness | −.121* | .002 | [−.025, .029] | .885 | .027 | [−.093, .147] | .655 | −.166* | .043* | [.019, .068] | .001 |
| Openness | −.011 | .017 | [−.009, .043] | .202 | −.053 | [−.168, .061] | .362 | −.116* | .033* | [.009, .056] | .008 |
Note. *p ≤ .05. “ / ” indicates that models aiming to test the linear moderating effects of age only were not fitted as the quadratic moderating effects of age were found to be significant.
Figure 3.

The prospective correlations between the Big Five personality traits and self-rated health, general disease level, and allostatic load and the correlations between changes in the Big Five personality traits and self-rated health, general disease level, and allostatic load across ages in the HRS sample. N = neuroticism; E = extraversion; C = conscientiousness; A = agreeableness; O = openness. Dashed lines represent statistically nonsignificant moderating effect of age (neither linear nor quadratic).
When the relations between changes in personality traits and health were examined after age 50 in HRS, there was a significant quadratic effect of age on the connection between changes in conscientiousness and self-rated health (Table 4). As can be seen from Figure 3, the relation between increases in conscientiousness and better self-rated health increased in strength from 50 to 70 but declined after age 70. Also, there was a significant linear effect of age on the link between changes in openness and self-rated health, with the association between increases in openness and better self-rated health decreased across time in the aging process. Age did not show significant moderating effects on the links between changes in neuroticism, extraversion, and agreeableness and general disease level. Decreases in neuroticism and increases in extraversion and agreeableness displayed stable relations to better self-rated health during age.
General Disease Level
We detected significant quadratic effects of age on the prospective relations between extraversion, conscientiousness, agreeableness, and openness and general disease level in aging (Table 4). Specifically, there was a U-shaped prospective link between conscientiousness and general disease level (See Figure 3). The strength of their negative connection increased in early phases of late adulthood but diminished around age 80. However, despite the significant quadratic effects of age on the prospective relation between extraversion, agreeableness, and openness and general disease level, as Figure 3 presents, the associations were generally weak during aging process. We found a linear age pattern for neuroticism, such that the strength of the prospective positive association between neuroticism and general disease level declined in a linear manner across ages.
As presented in Table 4, during the aging process, age showed significant quadratic effects on the relations between changes in conscientiousness, changes in agreeableness, and changes in openness and general disease level in HRS. When examined from the pattern plotted in Figure 3, though generally weak, the strength of the associations between increases in conscientiousness, agreeableness, and openness and lower general disease level got slightly stronger in young-old ages but approached zero as individuals entered very old ages. Age did not display significant moderating effects on the associations between changes in neuroticism and changes in extraversion and general disease level during the aging process.
Allostatic Load
Significant linear effects of age on the prospective relations between extraversion, conscientiousness, agreeableness, and openness and allostatic load were found in HRS (Table 4). As shown in Figure 3, there was a decreasing strength in the prospective negative link between conscientiousness and allostatic load across ages. When compared to conscientiousness, the associations between extraversion, agreeableness and openness and allostatic load were generally weaker and decreased in strength across time in aging. No significant moderating effects of age were found for neuroticism.
As displayed in Table 4, for changes in personality traits, in HRS, age exhibited a significant quadratic effect on the link between changes in conscientiousness and allostatic load. As shown in Figure 3, an inverted U-shape pattern was observed in the strength of the association between increases in conscientiousness and lower levels of allostatic load. Their negative connection decreased in strength and approached zero around 70’s, after which, the strength of their connection showed slight increases again. In addition, there were also significant linear effects of age on the relations between increases in extraversion, agreeableness, and openness and lower levels of allostatic load during aging. In general, the connections between increases in extraversion, agreeableness, and openness and lower levels of allostatic load diminished in magnitude across time during the aging process. No significant moderating effects of age was observed for change in neuroticism.
Table 5 provides a summary of the age-differential patterns for the prospective associations between the Big Five personality traits and health outcomes, as well as the associations between changes in the Big Five personality traits and health outcomes, during the aging process in HRS.
Table 5.
Summary of results for the prospective associations between the Big Five personality traits and changes in personality traits and health outcomes in HRS.
| HRS | |||
|---|---|---|---|
| Age2 | Age | Pattern Summary | |
| Self-Rated Health | |||
| N prospective | √ | negative relations increased in young-old ages but decreased after 80’s | |
| N change | weak negative relations were stable in aging. | ||
| E prospective | positive relations were stable in aging | ||
| E change | positive relations were stable in aging | ||
| C prospective | √ | positive relations increased in young-old ages but decreased after 80’s | |
| C change | √ | positive relations increased from 50 to 70 but decreased after 70’s | |
| A prospective | positive relations were stable in aging | ||
| A change | positive relations were stable in aging | ||
| O prospective | √ | positive relations increased from 50 to 70 but decreased after 70’s | |
| O change | √ | positive relations decreased in aging | |
| General Disease Level | |||
| N prospective | √ | positive relations decreased in aging | |
| N change | weak and stable relations in aging | ||
| E prospective | √ | weak relations increased in aging but decreased after 80’s | |
| E change | weak and stable relations in aging | ||
| C prospective | √ | negative relations increased in aging but decreased after 70’s | |
| C change | √ | negative relations increased in aging but decreased after 80’s | |
| A prospective | √ | weak negative relations in aging | |
| A change | √ | weak negative relations in aging | |
| O prospective | √ | weak negative relations increased in aging but decreased after 80’s | |
| O change | √ | weak negative relations increased in aging but decreased after 80’s | |
| Allostatic Load | |||
| N prospective | weak and stable relations in aging | ||
| N change | weak and stable relations in aging | ||
| E prospective | √ | negative relations decreased in aging | |
| E change | √ | negative relations decreased in aging | |
| C prospective | √ | negative relations decreased in aging | |
| C change | √ | negative relations decreased in aging but increased in very old ages | |
| A prospective | √ | negative relations decreased in aging | |
| A change | √ | negative relations decreased in aging | |
| O prospective | √ | weak negative relations decreased in aging | |
| O change | √ | weak negative relations decreased in aging | |
Note. “Age2” is marked when significant quadratic moderating effects of age were found; “Age” is marked when significant linear moderating effects of age were found (with nonsignificant quadratic moderating effects). The strength of the relation is identified as weak when the magnitude is smaller than .05 most of the time over the lifespan. Relations smaller than .05 in strength were reported to be ranked below the 20th percentile in psychological research (Bosco et al., 2015). N = neuroticism; E = extraversion; C = conscientiousness; A = agreeableness; O = openness.
Discussion
The present study examined whether the prospective associations between the Big Five personality traits and different types of health outcomes (self-rated health, general disease level, and physiological health indicators) and the associations between changes in the personality traits and health outcomes demonstrated age-differential patterns across the lifespan and during the aging process in particular. Using data from large samples with participants at different life phases allowed us to detect the potential moderating effects of age with sufficient power. Modeling age continuously also enabled us to scrutinize the nuanced moderating effects of age on the personality-health link. According to the current results, when examined from the life-span and aging perspectives, both the prospective personality-health and the personality change-health links displayed differential associations across ages in terms of strength and/or direction of the relations. The results of the current study reveal three main findings. First, the results supported the importance of personality traits/changes in personality traits to health outcomes across different life stages. Second, overall, the strength of the prospective relations between the personality traits and health outcomes, as well as the connections between changes in personality traits and health outcomes, increased in midlife or early stages of late adulthood and decreased in very old ages. Third, despite the general pattern, trait-specific and health outcome-specific patterns of associations across ages were also observed.
Integration of the Information from the Two Samples
As we note that results from the two samples should not be considered as replicating each other as the two samples differ in the span and distribution of age. Rather, they should be interpreted as complimentary of each other. Jointly interpreting the results from the two samples can provide a more complete picture of the age-differential relation between personality and health across different life phases. Thus, before discussing the implications of the findings, we provide an integration of the results from the two samples to facilitate further discussion.
For self-rated health, overall, evidence was found that the associations between personality traits/changes in personality traits and self-rated health displayed the strongest associations in middle adulthood and/or early phases of late adulthood, and these associations diminished in very old age. Specifically, when the findings from the two samples were jointly considered, the above-mentioned pattern was found for the prospective associations between neuroticism, conscientiousness, and openness, as well as changes in conscientiousness, and self-rated health. However, the prospective relations between extraversion and agreeableness and self-rated health were generally stable in strength both across the lifespan and during the aging process. After decreasing in strength in young and middle adulthood, the relations between increases in extraversion and agreeableness and better self-rated health stayed stable in late adulthood. Regarding general disease level, across the two samples, we also observed that neuroticism and conscientiousness, as well as changes in conscientiousness over time, demonstrated strengthening associations with general disease level in midlife and young-old ages, but the strength of these connections decreased in very old ages (e.g., after age 80). Generally, the levels of and changes in extraversion, agreeableness, and openness exhibited weak relations to general disease level across time. In terms of allostatic load, according to the findings from HRS, in general, the prospective link between extraversion, conscientiousness, agreeableness, and openness and allostatic load decreased during aging. Similarly, the relations between changes in personality traits and allostatic load were also found to decline in magnitude as people aged in late adulthood.
Theoretical Implications
Relevance of Personality to Health across the Lifespan
It has been widely acknowledged that personality traits and changes in personality traits play essential roles in impacting individuals’ health status (Ferguson, 2013; Hill & Roberts, 2016; Kern & Friedman, 2011; Luo et al., 2022; Murray & Booth, 2015; Smith, 2006). By incorporating the moderating effects of age, findings from the current study contributes to the theoretical frameworks on the connections between personality traits and health by further supporting the importance of personality traits to health. According to our results, personality traits were substantially related to health outcomes across different life phases, with the associations observed even in very old ages (e.g., in 80’s). Moreover, the results further underscored the relevance of personality traits to health by demonstrating that the effects went beyond self-perception of health: the relations between personality and health were also observable in health outcomes assessed in a relatively objective way, including disease level and physiological health indicators, across different phases of the life course and aging process.
General Pattern of the Personality-Health Link across Ages
Results from the present study also highlight the developmental nature of the personality-health association. In general, our results suggest that the pattern predicted by the SOC theory and the LCP model can be applied to the prospective relations between neuroticism, conscientiousness, and openness and self-rated health. Similarly, the prospective relations between neuroticism and conscientiousness and general disease level displayed strengthening associations in midlife and young-old ages before declining in very old ages. As the SOC theory depicts, in early phases of the aging process, there is substantial self-plasticity such that individuals still possess psychological capacity to regulate the subjective impact of health-related losses (Baltes & Smith, 2003). Findings from the current study illustrate that low levels of neuroticism and high levels of conscientiousness and openness may act as compensatory resources to facilitate the adjustment as individuals age, and the efficacy of these trait domains do not diminish until individuals enter the oldest-old ages. In addition, the compensatory role of low neuroticism and high conscientiousness applies not only to subjective health perceptions but also contributes to reducing disease burden.
The findings from the two samples also reveal that the hypotheses proposed in the LCP model for the level of conscientiousness measured at a specific time point were also applicable to the relations between changes in conscientiousness and health outcomes. As we observed, the strength of the associations between increases in conscientiousness and higher self-rated health and lower general disease level elevated in midlife/young-old age but decreased in very old ages. Such pattern reveals that, during the early stages of aging, positive development in personality traits, increases in conscientiousness in particular, may provide resources for psychological adaptions to the changed health conditions and maintaining healthy functioning. Our results support and extend the LCP model by demonstrating that both the level of conscientiousness and changes in conscientiousness play important roles in health. The level of conscientiousness and changes in conscientiousness were found to display more consistent and more potent relations to self-rated health and general disease level across the life course and aging process when compared to other trait domains, especially in middle adulthood and young-old ages. Conscientiousness is closely tied to goal-directed behaviors, planning, and impulse control (Roberts et al., 2009). The SOC theory has posited that optimizing positive health change requires in concert the application of a set of behavior-enhancing factors, including physical status, goal commitment, practice, and efforts. Thus, conscientiousness contributes to desirable physical health outcomes as it promotes effective responses to health challenges (Shanahan et al., 2014). Meanwhile, conscientiousness has consistently been shown to be tied to an array of health behaviors and adherence (Bogg & Roberts, 2004; Hill & Roberts, 2011), which may also function as compensatory resources that exert beneficial effects on individual’s physical health.
Patterns Specific to Certain Trait Domains and Health Outcomes
Different from the general pattern in which the links between personality traits and health outcomes diminished in strength in very old ages, the level of and changes in extraversion and agreeableness demonstrated substantial stable relations to self-rated health throughout the aging process. Extraversion is closely related to positive social interactions because of its social core (Wilkowski & Ferguson, 2014). Similarly, agreeableness is also suggested to be related to the motivation to maintain harmonious interpersonal relationships (Graziano & Habashi, 2010, 2015). The current findings indicated the importance of positive social experiences to individuals’ subjective health evaluation for successful aging, even in very old ages during which individuals have to face considerable health declines and the lack of other compensatory resources.
In addition, for allostatic load, contrary to our expectations, neuroticism was only weakly linked to allostatic load throughout the aging process. Meanwhile, other than showing stronger connections with health outcomes during the young-old stage, the prospective connections between the positive trait domains and allostatic load diminished in strength in a linear manner across the aging process. Similarly, for changes in personality traits, while changes in neuroticism only showed a weak relation to allostatic load in aging, the links between changes in extraversion, agreeableness, and openness and allostatic load decreased in strength as individuals aged. The strength of the association between changes in conscientiousness and allostatic load declined over time but showed an increasing pattern after 80’s, suggesting a growing importance of conscientiousness to physiological health in the oldest-old phase. Compared to other types of health outcomes, allostatic load is influenced by biological functioning to a greater extent, which declines as individuals enter late adulthood. The pattern of current findings suggests that the compensatory power provided by personality traits to allostatic load decreases with biological declines over time. More research is needed to uncover the mechanisms underlying the strengthening association between changes in conscientiousness and allostatic load in the oldest-old ages.
Overall, as the first large-scale systematic investigation of the age-differential personality-health link, our findings contribute to refining the theories by specifying the patterns for the age-differential connections between personality and health for different trait domains and different types of health outcomes. Furthermore, the present study also extends the theoretical frameworks and empirical research on the personality-health link by investigating the age-differential associations for changes in personality traits.
Practical Implications
Understanding the age-differential associations between personality traits and health outcomes also has practical implications. As evidence has been shown for the importance of personality traits in influencing health outcomes, there are growing interests in developing personality-based interventions (Bleidorn et al., 2019; Chapman et al., 2014; Magidson et al., 2014) as research has demonstrated that personality traits are amenable to intervention (Roberts et al., 2017). Results from the present study adds support for the utility of the personality-based interventions by showing that personality traits, particularly changes in personality traits, are substantially related to different types of health outcomes in a prospective way across different life phases. In addition, the current findings contribute to identifying the critical period for implementing the personality-based interventions to help with disease prevention and health management. According to our results, in general, it is likely that the interventions will be most effective if they are administered in midlife stage or in early stages of late adulthood (around 50’s and 60’s). Furthermore, findings from the present study provide trait-specific and health-outcome-specific information that can be useful for improving the precision and efficacy of the interventions. For example, despite the general pattern, our results suggest that interventions designed to increase extraversion may lead to better subjective perception of health throughout the life course and aging process. Similarly, interventions aimed to increase conscientiousness may contribute to better physiological health after the 80’s. However, it is worth noting that findings from the present study can only be viewed as preliminary evidence for the potential use of the personality-based interventions. The assumption of applying the personality-based interventions for prevention/health promotion is that personality is a leading indicator and influences health through a downstream process (Chapman et al., 2014; Mroczek, 2014). In the current study, we did not attempt to examine the causal relation between personality traits/changes in personality traits and health. Previous work has demonstrated the reciprocal associations between changes in personality traits and changes in health outcomes (Luo et al., 2022). Factors, such as people’s socioeconomic status, that are related to both personality and health (Chen & Miller, 2013; Hughes et al., 2021) are likely to play roles in driving the observed associations between personality and health. More work is needed to establish the causal link between personality and health.
Limitations and Future Directions
The current study has many strengths such as using two large samples to examine the moderating effects of age from both the life-span and aging perspectives and conducting analyses for the dynamic changes in personality traits and different types of health outcomes. However, there are qualifications that need to be considered when interpreting the study findings. First, we only examined the Big Five personality traits and changes in the personality traits at the domain level. Recent research has suggested that there may be better predictive validity for facets and nuances (items used to measure personality traits) than domain-level traits (Stewart et al., 2022). Also, compared to domain-level traits, facets and nuances were found to better capture age-related differences in specific behaviors, thoughts, and feelings (Mottus & Rozgonjuk, 2021). It’s possible that the domain level traits are too broad and mask the underlying characteristics that are driving the observed associations. Thus, future research is needed to test the age-differential associations between personality traits/changes in personality traits and health at the facet- and nuance-level of personality traits. Second, only the Big Five were tested for personality. Previous work has shown that trait domains other than the Big Five, such as optimism, contribute to health outcomes and longevity during the aging process (Chopik et al., 2015; Lee et al., 2019). Moreover, in addition to personality traits, other domains of personality, such as goals and narrative identity, have been shown to be related to health outcomes and well-being and provide incremental information above and beyond the Big Five personality traits (Adler et al., 2016; McKnight & Kashdan, 2009). Thus, future studies should examine the possible age-differential associations between other trait domains and other domains of personality and health outcomes. Third, recent research has suggested that the structure of personality changes over time, with the structure for older adults differing from that for younger adults (Beck et al., 2023). Structural changes in personality traits should be taken into account in future work on the relations between personality traits and health. Fourth, the current study focused on the general levels of health outcomes in different types (e.g., general levels of subjective health perception, diseases, and physiological functioning). Future work is needed to examine if the patterns can be applied to specific health outcomes within each type (e.g., specific diseases). Fifth, in the present study, only self-report measures were used to assess personality traits. Aggregation of friend-rated personality traits has been reported to be a better predictor of longevity when compared with self-ratings (Jackson et al., 2015). Future research should use different sources to assess personality traits (e.g., other-report measures, behavioral measures). The information obtained from different rating methods can better inform how personality traits and health are connected at different life stages. Finally, it has been suggested that the mechanisms (e.g., stress exposure, health behaviors) underlying the personality-health link may differ across ages (Mroczek et al., 2020; Shanahan et al., 2014), with some mechanisms being more important in certain life phases than others. Future research will benefit from examining the potential age-differential mediating effects of various mechanisms to better uncover the personality-health association, contributing to improving the precision and efficacy of the personality-based intervention.
Conclusion
In summary, the current study investigated the age-differential prospective associations between the Big Five personality traits and changes in the personality traits and different types of health outcomes. Using data from two large longitudinal samples, we examined the moderating effects of age on the prospective relations between personality traits and health outcomes and the links between changes in personality traits and health outcomes from both life-span developmental and aging perspectives. Overall, the strength of the associations increased in midlife or early stages of late adulthood. However, the relations decreased in magnitude in very old ages. There were trait-specific and health outcome-specific patterns for the personality-health links across ages. Results from the current study provide insights into how personality traits and health are interconnected in different ages across the life course and during the aging process. Future research should examine the age-differential relations between personality and health at the facet- and nuance-level, use different sources for personality ratings, and consider the differential roles of different mechanisms across ages.
Supplementary Material
Acknowledgments
This research was supported by grants from the National Institute on Aging, R01-AG018436: Personality & Well-being Trajectories in Adulthood, R01- AG067622: Personality and Non-Cognitive Factors in the Risk of Dementia Progression and Physical Health, & R01-AG064006: Boston Early Adversity and Mortality Study: Linking administrative data to long-term longitudinal studies.
Footnotes
We were not authorized to share the data used in the current study in an open-access repository. Data used from the Household, Income and Labor Dynamics in Australia Survey (HILDA) are available upon request from the original data sources. Data used from the Health and Retirement Study (HRS) are available at https://hrs.isr.umich.edu/about.
The scripts for the analyses can be found at https://osf.io/582ek/?view_only=3c106e1812b143e09b0674be85e55bf2.
References
- Adler JM, Lodi-Smith J, Philippe FL, & Houle I (2016). The Incremental Validity of Narrative Identity in Predicting Well-Being: A Review of the Field and Recommendations for the Future. Personality and Social Psychology Review, 20(2), 142–175. doi.org/ 10.1177/1088868315585068 [DOI] [PubMed] [Google Scholar]
- Atherton OE, Robins RW, Rentfrow PJ, & Lamb ME (2014). Personality correlates of risky health outcomes: Findings from a large internet study. Journal of Research in Personality, 50, 56–60. doi.org/ 10.1016/j.jrp.2014.03.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baltes PB (1997). On the incomplete architecture of human ontogeny: Selection, optimization, and compensation as foundation of developmental theory. American Psychologist, 52(4), 366–380. doi: 10.1037/0003-066X.52.4.366 [DOI] [PubMed] [Google Scholar]
- Baltes PB, & Smith J (2003). New frontiers in the future of aging: From successful aging of the young old to the dilemmas of the fourth age. Gerontology, 49, 123–135. doi.org/ 10.1159/000067946 [DOI] [PubMed] [Google Scholar]
- Bauer DJ (2017). A more general model for testing measurement invariance and differential item functioning. Psychological Methods, 22(3), 507–526. doi: 10.1037/met0000077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck ED, Condon D, & Jackson J (2023). Interindividual age differences in personality structure. European Journal of Personality, 37(3), 257–275. 10.1177/08902070221084862 [DOI] [Google Scholar]
- Berg AI, & Johansson B (2014). Personality change in the oldest-old: Is it a matter of compromised health and functioning? Journal of Personality, 82(1), 25–31. doi: 10.1111/jopy.12030 [DOI] [PubMed] [Google Scholar]
- Bleidorn W, Hill PL, Back MD, Denissen JJA, Hennecke M, Hopwood CJ, … Roberts B (2019). The policy relevance of personality traits. American Psychologist, 74(9), 1056–1067. doi: 10.1037/amp0000503 [DOI] [PubMed] [Google Scholar]
- Bogg T, & Roberts BW (2004). Conscientiousness and health-related behaviors: a meta-analysis of the leading behavioral contributors to mortality. Psychological Bulletin, 130(6), 887. doi.org/ 10.1037/0033-2909.130.6.887 [DOI] [PubMed] [Google Scholar]
- Bosco FA, Aguinis H, Singh K, Field JG, & Pierce CA (2015). Correlational effect size benchmarks. Journal of Applied Psychology, 100(2), 431–449. doi.org/ 10.1037/a0038047 [DOI] [PubMed] [Google Scholar]
- Burkhauser RV, & Gertler PJ (1995). Introduction to special issue on the Health and Retirement Survey/data quality and early results. Journal of Human Resources, 30, S1–S6. https://www.jstor.org/stable/146276 [Google Scholar]
- Canada B, Stephan Y, Jaconelli A, & Duberstein PR (2016). The moderating effect of chronological age on the relation between neuroticism and physical functioning: Cross-sectional evidence from two French samples. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 71(1), 35–40. doi.org/ 10.1093/geronb/gbu083 [DOI] [PubMed] [Google Scholar]
- Chapman BP, Hampson S, & Clarkin J (2014). Personality-informed interventions for healthy aging: Conclusions from a national institute on aging work group. Developmental Psychology, 50(5), 1426–1441. doi: 10.1037/a0034135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chereches FS, Brehmer Y, & Olaru G (2022). Personality and limitations in instrumental activities of daily living in old age: Reciprocal associations across 12 years. European Journal of Personality, 0(0). doi.org/ 10.1177/08902070221111856 [DOI] [Google Scholar]
- Chen E, & Miller GE (2013). Socioeconomic status and health: mediating and moderating factors. Annual Review of Clinical Psychology, 9(1), 723–749. 10.1146/annurev-clinpsy-050212-185634 [DOI] [PubMed] [Google Scholar]
- Cheung GW, & Rensvold RB (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255. doi.org/ 10.1207/S15328007SEM0902_5 [DOI] [Google Scholar]
- Chopik WJ, Kim ES, & Smith J (2015). Changes in optimism are associated with changes in health over time among older adults. Social Psychological and Personality Science, 6(7), 814–822. doi.org/ 10.1177/1948550615590199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Damian RI, Su R, Shanahan M, Trautwein U, & Roberts BW (2015). Can personality traits and intelligence compensate for background disadvantage? Predicting status attainment in adulthood. Journal of Personality and Social Psychology, 109(3), 473. doi: 10.1037/pspp0000024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duberstein PR, Sörensen S, Lyness JM, King DA, Conwell Y, Seidlitz L, & Caine ED (2003). Personality is associated with perceived health and functional status in older primary care patients. Psychology and Aging, 18(1), 25–37. doi: 10.1037/0882-7974.18.1.25 [DOI] [PubMed] [Google Scholar]
- Ferguson E (2013). Personality is of central concern to understand health: Towards a theoretical model for health psychology. Health Psychology Review, 7(sup1), S32–S70. doi: 10.1080/17437199.2010.547985 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman HS, Kern ML, & Reynolds CA (2010). Personality and health, subjective well-being, and longevity. Journal of Personality, 78(1), 179–216. doi: 10.1111/j.1467-6494.2009.00613.x [DOI] [PubMed] [Google Scholar]
- Goodwin R, & Engstrom G (2002). Personality and the perception of health in the general population. Psychological Medicine, 32(2), 325–32. doi.org/ 10.1017/S0033291701005104 [DOI] [PubMed] [Google Scholar]
- Goodwin RD, & Friedman HS (2006). Health status and the five-factor personality traits in a nationally representative sample. Journal of Health Psychology, 11(5), 643–654. doi: 10.1177/1359105306066610 [DOI] [PubMed] [Google Scholar]
- Graham EK, Rutsohn JP, Turiano NA, Bendayan R, Batterham PJ, Gerstorf D, … Mroczek DK (2017). Personality predicts mortality risk: An integrative data analysis of 15 international longitudinal studies. Journal of Research in Personality, 70, 174–186. doi.org/ 10.1016/j.jrp.2017.07.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham EK, Weston SJ, Gerstorf D, Yoneda TB, Booth T, Beam CR, … Mroczek DK (2020). Trajectories of big five personality traits: A coordinated analysis of 16 longitudinal samples. European Journal of Personality, 34(3), 301–321. doi: 10.1002/per.2259 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graziano WG, & Habashi MM (2010). Motivational processes underlying both prejudice and helping. Personality and Social Psychology Review, 14(3), 313–331. doi.org/ 10.1177/1088868310361239 [DOI] [PubMed] [Google Scholar]
- Graziano WG, & Habashi MM (2015). Searching for the prosocial personality. In The Oxford handbook of prosocial behavior (pp. 231–255). Oxford University Press. 10.1093/oxfordhb/9780195399813.013.017 [DOI] [Google Scholar]
- Health and Retirement Study, (2006 HRS Core) public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2021). [Google Scholar]
- Health and Retirement Study, (2006 Biomarker Data) sensitive dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2013). [Google Scholar]
- Health and Retirement Study, (2008 HRS Core) public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2014). [Google Scholar]
- Health and Retirement Study, (2008 Biomarker Data) sensitive dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2013). [Google Scholar]
- Health and Retirement Study, (2010 HRS Core) public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2021). [Google Scholar]
- Health and Retirement Study, (2010 Biomarker Data) sensitive dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2015). [Google Scholar]
- Health and Retirement Study, (2012 HRS Core) public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2020). [Google Scholar]
- Health and Retirement Study, (2012 Biomarker Data) sensitive dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2015). [Google Scholar]
- Health and Retirement Study, (2014 HRS Core) public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2017). [Google Scholar]
- Health and Retirement Study, (2014 Biomarker Data) sensitive dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2017). [Google Scholar]
- Health and Retirement Study, (2016 HRS Core) public use dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2022). [Google Scholar]
- Health and Retirement Study, (2016 Biomarker Data) sensitive dataset. Produced and distributed by the University of Michigan with funding from the National Institute on Aging (grant number NIA U01AG009740). Ann Arbor, MI, (2020). [Google Scholar]
- Hill PL, & Allemand M (2011). Gratitude, forgivingness, and well-being in adulthood: Tests of moderation and incremental prediction. The Journal of Positive Psychology,6(5), 397–407. doi: 10.1080/17439760.2011.602099 [DOI] [Google Scholar]
- Hill PL, Allemand M, & Roberts BW (2013). Examining the pathways between gratitude and self-rated physical health across adulthood. Personality and Individual Differences, 54(1), 92–96. doi.org/ 10.1016/j.paid.2012.08.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill PL, & Roberts BW (2011). The role of adherence in the relationship between conscientiousness and perceived health. Health Psychology, 30(6), 797–804. doi: 10.1037/a0023860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill PL, & Roberts BW (2016). Personality and health: Reviewing recent research and setting a directive for the future. In Schaie KW, & Willis SL (Eds.), Handbook of the psychology of aging (eighth edition) (pp. 205–218). San Diego: Academic Press. doi.org/ 10.1016/B978-0-12-411469-2.00011-X [DOI] [Google Scholar]
- Horn JL, & McArdle JJ (1992). A practical and theoretical guide to measurement invariance in aging research. Experimental Aging Research, 18(3), 117–144. doi.org/ 10.1080/03610739208253916 [DOI] [PubMed] [Google Scholar]
- Hughes BT, Costello CK, Pearman J, Razavi P, Bedford-Petersen C, Ludwig RM, & Srivastava S (2021). The Big Five Across Socioeconomic Status: Measurement Invariance, Relationships, and Age Trends. Collabra: Psychology, 7(1), 24431. doi.org/ 10.1525/collabra.24431 [DOI] [Google Scholar]
- Jackson JJ, Connolly JJ, Garrison SM, Leveille MM, & Connolly SL (2015). Your friends know how long you will live: A 75-year study of peer-rated personality traits. Psychological Science, 26(3), 335–340. doi: 10.1177/0956797614561800 [DOI] [PubMed] [Google Scholar]
- Kandler C, Kornadt AE, Hagemeyer B, & Neyer FJ (2015). Patterns and sources of personality development in old age. Journal of Personality and Social Psychology, 109(1), 175–191. doi: 10.1037/pspp0000028 [DOI] [PubMed] [Google Scholar]
- Kern ML, & Friedman HS (2011). Personality and pathways of influence on physical health. Social and Personality Psychology Compass, 5(1), 76–87. doi: 10.1111/j.1751-9004.2010.00331.x [DOI] [Google Scholar]
- Kline RB (2005). Principles and practice of structural equation modeling (second ed.). The Guilford Press, New York. [Google Scholar]
- Lachman ME, & Bertrand RM (2001). Personality and the self in midlife. (pp. 279–309). Hoboken, NJ, US: John Wiley & Sons, Inc. [Google Scholar]
- Lee LO, James P, Zevon ES, Kim ES, Trudel-Fitzgerald C, Spiro III A, … & Kubzansky LD (2019). Optimism is associated with exceptional longevity in 2 epidemiologic cohorts of men and women. Proceedings of the National Academy of Sciences, 116(37), 18357–18362. doi.org/ 10.1073/pnas.1900712116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucas RE, & Donnellan MB (2011). Personality development across the life span: Longitudinal analyses with a national sample from Germany. Journal of Personality and Social Psychology, 101(4), 847–861. doi: 10.1037/a0024298 [DOI] [PubMed] [Google Scholar]
- Luo J, Zhang B, Cao M, & Roberts BW (2023). The Stressful Personality: A Meta-Analytical Review of the Relation Between Personality and Stress. Personality and Social Psychology Review, 27(2), 128–194. 10.1177/10888683221104002 [DOI] [PubMed] [Google Scholar]
- Luo J, Zhang B, Estabrook R, Graham EK, Driver CC, Schalet BD, … Mroczek DK (2022). Personality and health: Disentangling their between-person and within-person relationship in three longitudinal studies. Journal of Personality and Social Psychology, 122(3), 493–522. doi: 10.1037/pspp0000399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magee CA, Heaven PCL, & Miller LM (2013). Personality change predicts self-reported mental and physical health. Journal of Personality, 81(3), 324–334. doi.org/ 10.1111/j.1467-6494.2012.00802.x [DOI] [PubMed] [Google Scholar]
- Magidson JF, Roberts BW, Collado-Rodriguez A, & Lejuez CW (2014). Theory-driven intervention for changing personality: expectancy value theory, behavioral activation, and conscientiousness. Developmental psychology, 50(5), 1442. doi.org/ 10.1037/a0030583 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEwen BS (2000). Allostasis and allostatic load: Implications for neuropsychopharmacology. Neuropsychopharmacology, 22(2), 108–124. doi.org/ 10.1016/S0893-133X(99)00129-3 [DOI] [PubMed] [Google Scholar]
- McKnight PE, & Kashdan TB (2009). Purpose in Life as a System that Creates and Sustains Health and Well-Being: An Integrative, Testable Theory. Review of General Psychology, 13(3), 242–251. doi.org/ 10.1037/a0017152 [DOI] [Google Scholar]
- Mirowsky J, & Ross CE (2017). Education, social status, and health. Routledge. [Google Scholar]
- Mõttus R, Johnson W, & Deary IJ (2012). Personality traits in old age: Measurement and rank-order stability and some mean-level change. Psychology and Aging, 27(1), 243–249. doi: 10.1037/a0023690 [DOI] [PubMed] [Google Scholar]
- Mõttus R, & Rozgonjuk D (2021). Development is in the details: Age differences in the big five domains, facets, and nuances. Journal of Personality and Social Psychology, 120(4), 1035–1048. doi: 10.1037/pspp0000276 [DOI] [PubMed] [Google Scholar]
- Mroczek DK (2014). Personality plasticity, healthy aging, and interventions. Developmental Psychology, 50(5), 1470–1474. doi: 10.1037/a0036028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mroczek DK, & Spiro A (2007). Personality change influences mortality in older men. Psychological science, 18(5), 371–376. doi.org/ 10.1111/j.1467-9280.2007.01907.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mroczek DK, Weston SJ, Willroth EC (2020). A lifespan perspective on the interconnections between personality, health, and optimal aging. In Hill P, Allemand M (eds), Personality and healthy aging in adulthood. International Perspectives on Aging, vol 26. Springer, Cham. doi.org/ 10.1007/978-3-030-32053-9_12. [DOI] [Google Scholar]
- Mueller S, Wagner J, Smith J, Voelkle MC, & Gerstorf D (2018). The interplay of personality and functional health in old and very old age: Dynamic within-person interrelations across up to 13 years. Journal of Personality and Social Psychology, 115(6), 1127–1147. doi: 10.1037/pspp0000173 [DOI] [PubMed] [Google Scholar]
- Murray AL, & Booth T (2015). Personality and physical health. Current Opinion in Psychology, 5, 50–55. doi.org/ 10.1016/j.copsyc.2015.03.011 [DOI] [Google Scholar]
- Muthén LK, & Muthén BO (1998-2017). Mplus User’s Guide. Muthén & Muthén: Los Angeles, CA. [Google Scholar]
- Roberts BW, & DelVecchio WF (2000). The rank-order consistency of personality traits from childhood to old age: A quantitative review of longitudinal studies. Psychological Bulletin, 126(1), 3–25. doi: 10.1037/0033-2909.126.1.3 [DOI] [PubMed] [Google Scholar]
- Roberts BW, Jackson JJ, Fayard JV, Edmonds G, & Meints J (2009). Conscientiousness In: Leary M & Hoyle R (Eds.), Handbook of Individual Differences in Social Behavior (pp. 369–381). New York, NY, US: Guilford Press. [Google Scholar]
- Roberts BW, Luo J, Briley DA, Chow PI, Su R, & Hill PL (2017). A systematic review of personality trait change through intervention. Psychological Bulletin, 143(2), 117–141. doi.org/ 10.1037/bul0000088 [DOI] [PubMed] [Google Scholar]
- Roberts BW, Walton KE, & Viechtbauer W (2006). Patterns of mean-level change in personality traits across the life course: A meta-analysis of longitudinal studies. Psychological Bulletin, 132(1), 1–25. doi: 10.1037/0033-2909.132.1.1 [DOI] [PubMed] [Google Scholar]
- Ross CE, & Mirowsky J (2011). The interaction of personal and parental education on health. Social Science & Medicine, 72(4), 591–599. doi.org/ 10.1016/j.socscimed.2010.11.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saucier G (1994). Mini-markers: A brief version of goldberg's unipolar big-five markers. Journal of Personality Assessment, 63(3), 506–516. doi: 10.1207/s15327752jpa6303_8 [DOI] [PubMed] [Google Scholar]
- Seeman TE, Singer BH, Rowe JW, Horwitz RI, & McEwen BS (1997). Price of adaptation—allostatic load and its health consequences: MacArthur studies of successful aging. Archives of Internal Medicine, 157(19), 2259–2268. doi: 10.1001/archinte.1997.00440400111013 [DOI] [PubMed] [Google Scholar]
- Shackman AJ, Tromp DPM, Stockbridge MD, Kaplan CM, Tillman RM, & Fox AS (2016). Dispositional negativity: An integrative psychological and neurobiological perspective. Psychological Bulletin, 142(12), 1275–1314. doi: 10.1037/bul0000073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shanahan MJ, Hill PL, Roberts BW, Eccles J, & Friedman HS (2014). Conscientiousness, health, and aging: The life course of personality model. Developmental Psychology, 50(5), 1407–1425. doi: 10.1037/a0031130 [DOI] [PubMed] [Google Scholar]
- Smith TW (2006). Personality as risk and resilience in physical health. Current Directions Psychological Science, 15(5), 227–231. doi: 10.1111/j.1467-8721.2006.00441.x [DOI] [Google Scholar]
- Smith J, & Ryan LH (2016). Psychological vitality in the oldest old. In Schaie KW & Willis SL (Eds.), Handbook of the psychology of aging (8th ed., pp. 303–319). San Diego, CA: Academic Press. 10.1016/B978-0-12-411469-2.00016-9 [DOI] [Google Scholar]
- Stephan Y, Sutin AR, Luchetti M, & Terracciano A (2016). Allostatic load and personality: A 4-year longitudinal study. Psychosomatic medicine, 78(3), 302. doi: 10.1097/PSY.0000000000000281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart RD, Mõttus R, Seeboth A, Soto CJ, & Johnson W (2022). The finer details? the predictability of life outcomes from big five domains, facets, and nuances. Journal of Personality, 90(2), 167–182. doi.org/ 10.1111/jopy.12660 [DOI] [PubMed] [Google Scholar]
- Sutin AR, Zonderman AB, Ferrucci L, & Terracciano A (2013). Personality traits and chronic disease: Implications for adult personality development. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 68(6), 912–920. doi.org/ 10.1093/geronb/gbt036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turiano NA, Pitzer L, Armour C, Karlamangla A, Ryff CD, & Mroczek DK (2012). Personality trait level and change as predictors of health outcomes: Findings from a national study of Americans (MIDUS). Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 67(1), 4–12. doi.org/ 10.1093/geronb/gbr072 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weston SJ, Hill PL, & Jackson JJ (2015). Personality traits predict the onset of disease. Social Psychological and Personality Science, 6(3), 309–317. doi: 10.1177/1948550614553248 [DOI] [Google Scholar]
- Wilkowski BM, & Ferguson EL (2014). Just loving these people: Extraverts implicitly associate people with reward. Journal of Research in Personality, 53, 93–102. doi.org/ 10.1016/j.jrp.2014.08.006 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.