

Editord—Hazardous attitudes contribute to degraded performance in aviation1–4 and surgery.5 Elevated hazardous attitudes scores appear to predispose to poor decision-making and ‘at-risk’ behaviours.4–6 In post-accident analyses, 86% of fatal general aviation accidents involved at least one hazardous attitude.7 A key set of hazardous attitudes was identified by the United States Federal Aviation Administration (FAA): anti-authority, impulsivity, invulnerability, resignation, and macho (describing risk tolerance driven by ego and social concern).1 Their description of hazardous attitudes, pilot behaviours and mindsets, and potential adverse consequences is summarised in Supplementary Table 1. The domains self-confidence and worry were added to scale versions used in healthcare.5,6,8–10
In the USA orthopaedic surgeons, elevated macho scores were associated with higher rates of reoperation or readmission.5 A study of Swedish orthopaedists reported that macho responders were more likely to operate even in cases where studies have shown no or limited benefit.10 Saeed and colleagues6 described low levels of hazardous attitudes in radiation oncologists, but reported an association between macho responses and non-adherence to clinical guidelines. We investigated the prevalence of hazardous attitudes in anaesthesiologists to compare them with patterns seen in other professional populations.2,4–6
After approval by the Vanderbilt University Human Research Protection Program (IRB 20–460), we recruited anaesthesia residents (≥ 6 months of anaesthesia training) and board-certified anaesthesiologists certified after 2000 working hours in the OR ≥20 h per week. All participants completed a pilot hazardous attitudes tool using 28 items adjusted for pertinence to anaesthesia as in other medical studies (Supplementary Appendices A and B)6,8,10 based on the original scale developed and validated by Hunter.3 Our tool omitted one item each in the impulsivity and anti-authority domains as they seemed redundant.
The process used to detect hazardous attitudes followed other medical studies.6,8,10 For each hazardous attitude domain, a response yielding >80% of the possible Likert scale points indicates an hazardous attitude domain ‘of concern’.5,8 There were six missing responses (0.2% of 2856 questions). For five of these, we determined that the individual domains did not change regardless of the missing variable’s value.
Hypothesis tests were evaluated using a testwise type-I error rate of 5%. No familywise hypotheses were specified a priori, and none of the hypotheses warranted familywise type-I error control. This approach is consistent with the study design and aims: to quantify and independently test associations between several hazardous attitudes and anaesthesiologist characteristics.
Using the R Project statistical software package, version 4.1.3,11 continuous variables were summarised by median and interquartile range, and categorical data as frequency and percent. In addition to summaries of concern behaviour within individual domains, we also summed the domains of concern for each participant. Only the macho and self-confidence domains had adequate numbers of ‘concern’ scores to apply logistic regression reliably, allowing control for three covariates (sex, race, and resident/fellow or board-certified anaesthesiologist status). Subgroup analyses of board-certified anaesthesiologist participants included ‘number of active years’ and ‘work at an academic centre’.11
Four of the five domains had reasonable reliability as measured by Cronbach’s alpha: macho 0.88, worry 0.73, anti-authority 0.71, resignation 0.72, and self-confidence 0.50. The impulsivity domain had a low Cronbach’s alpha of −0.02.
There were 42 (41%) residents or fellows and 60 (59%) board-certified anaesthesiologists; 46 (45.1%) were female. The board-certified anaesthesiologists had broad experience (median age 42 yr, 0–23 yr in practice); 43% had completed a clinical fellowship and 50% worked at least part-time at an academic centre. A substantial number (29.4%) of participants manifested at least one hazardous attitude of concern accounting for a total of 42 elevated hazardous attitude scores. Ten participants had hazardous attitudes of concern in more than one domain. As shown in Figure 1, anaesthesiologists had higher hazardous attitude scores in the macho and self-confidence domains, whereas resignation was the lowest (see also Supplementary Fig. 1, and Supplementary Tables 2 and 3).
Figure 1.
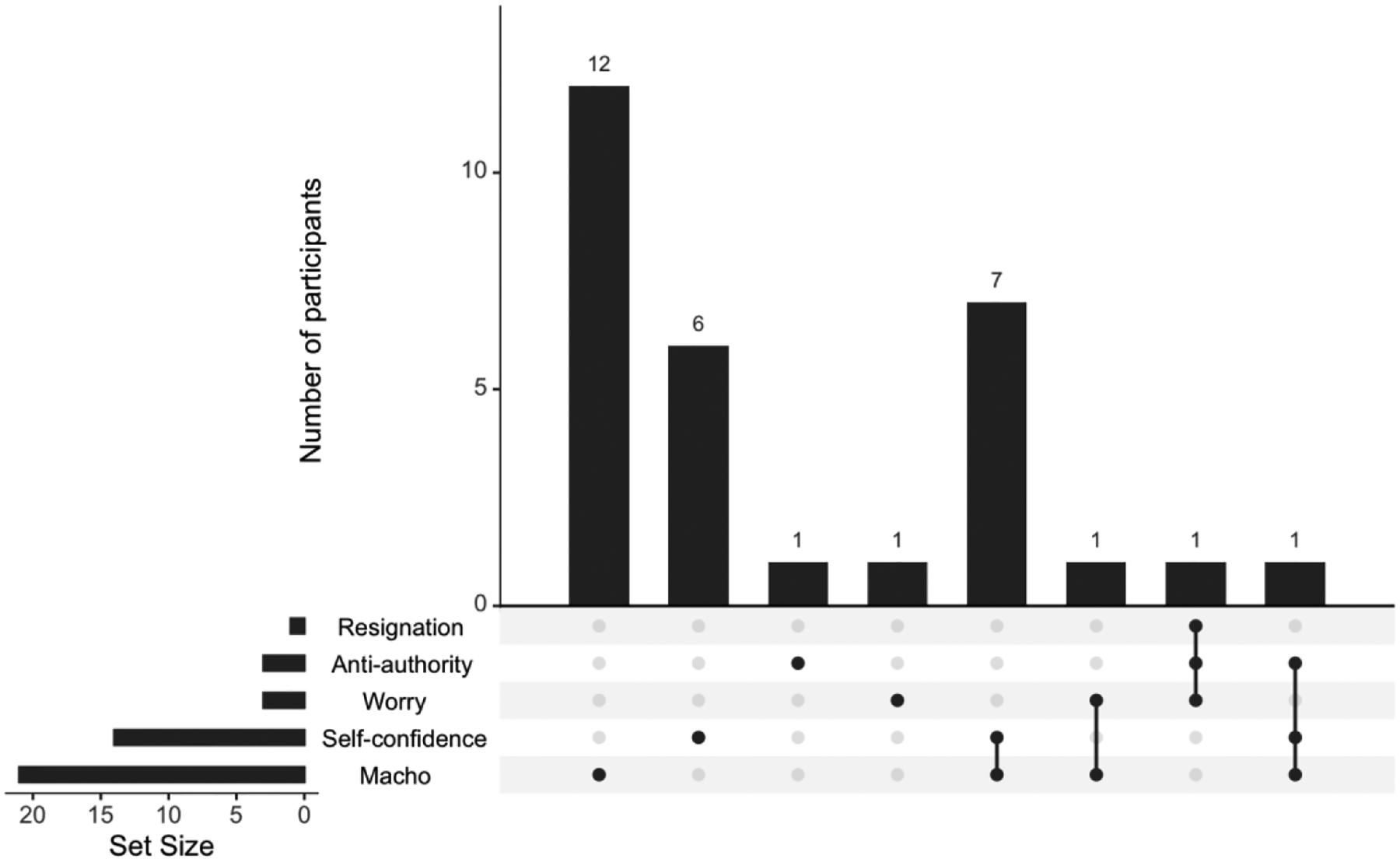
Distribution of Hazardous Attitude Domains of Concern Across Participants.
The linkage bars between HAs show which HA combinations were found in those scoring high for more than one HA (e.g., 1 individual scored high with the combination of Macho, Self-confidence, and Anti-authority)
In looking at the total number of domains of concern, the adjusted odds ratio for male vs female regarding high hazardous attitude scores was 2.7 (95% confidence interval [CI] 1.0–6.9, P=0.045). There was no significant association of elevated hazardous attitude scores with race, level of training, total work hours per week, or experience in challenging clinical situations. For the macho and self-confidence domains, there were a sufficient number of participants with hazardous attitudes of concern to assess their association with demographic variables. In multiple logistic regressions, none of the three covariates (resident vs attending, sex, and race) were statistically significant (Supplementary Table 3).
Our finding of least one hazardous attitude ‘of concern’ at 29.4% is similar to the studies of surgeons by Bruinsma and colleagues8 (38%) and Kadzielski and colleagues5 (30%). The most common elevated scores were in the macho domain where men had higher scores. This is notable, given the impact of the macho hazardous attitude on adverse decision-making and outcomes described in other specialties and industries.3–6,12 The most common hazardous attitudes of concern were macho and self-confidence, paralleling patterns described for pilots.12–14 In subgroup analysis, academic board-certified anaesthesiologists had 11.3 times (95% CI 1.2–101.8) higher odds of exhibiting macho tendencies than non-academic board-certified anaesthesiologists.
Given the sample size of this pilot study, there is a modest level of generalisability of our results. The hazardous attitude study instrument showed content validity (close parallelism with the aviation scale) and face validity, and reasonable internal measures of reliability (Cronbach’s parameters) for most domains. The low internal reliability of the impulsivity domain might have been because of our use of only four items or other contributors.
These findings suggest that hazardous attitudes are observed in many anaesthesiologists. Prior medical hazardous attitudes studies describe potential associations between increased hazardous attitudes and adverse decisions or behaviours.5,6,10 It is plausible that anaesthesiologists with elevated hazardous attitude scores are also at risk. In aviation, identification of hazardous attitudes leads to use of ‘antidote’ phrases and training (Supplementary Table 4) in the context of other safety system considerations.1 Further investigation of the incidence and impact of hazardous attitudes on anaesthetist decision-making and behaviour beyond this pilot work could guide development of remediations to be integrated with other safety improvement strategies in medicine.
Supplementary Material
Acknowledgements
We appreciate the input of David Hunter and members of the Simulation Assessment Research Group (SARG) who contributed significantly to the conduct of the IMPACTS study but did not meet international criteria for authorship of this manuscript.
Funding
Agency for Healthcare Research and Quality (R18 HS026158-05 entitled ‘IMPACTS: Improving Medical Performance during Acute Crises Through Simulation’ to MBW).
Footnotes
Declaration of interest
The authors declare that they have no conflicts of interest pertinent to the content of this work.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.bja.2023.08.012.
References
- 1.US Department of Transportation-Federal Aviation Administration. Pilot’s handbook of aeronautical knowledge, FAA-H-8083-25C. Ch 2: Aeronautical decision-making, p2-1 to 2–32 Oklahoma City, OK, USA: 2023. Available from: https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/faa-h-8083-25c.pdf. [Accessed 16 September 2023] [Google Scholar]
- 2.Nuñez B, López C, Velazquez J, Mora OA, Román K. Hazardous attitudes in US part 121 airline accidents. 20th Int Symp Aviat Psychol 2019: 37e42. Available from: https://corescholar.libraries.wright.edu/isap_2019/7. [Accessed 16 September 2023] [Google Scholar]
- 3.Hunter DR. Measurement of hazardous attitudes among pilots. Int J Aviat Psychol 2005; 15: 23–43 [Google Scholar]
- 4.Hunter DR, Martinussen M, Wiggins M, O’Hare D. Situational and personal characteristics associated with adverse weather encounters by pilots. Accid Anal Prev 2011; 43: 176–86 [DOI] [PubMed] [Google Scholar]
- 5.Kadzielski J, McCormick F, Herndon JH, Rubash H, Ring D. Surgeons’ attitudes are associated with reoperation and readmission rates. Clin Orthop 2015; 473: 1544–51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Saeed NA, Blakaj A, Kelly JR, et al. Hazardous attitudes: physician decision making in radiation oncology. Adv Rad Onc 2022; 7, 101033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wetmore M, Lu CT. The effects of hazardous attitudes on crew resource management skills. Int J Appl Aviat Stud 2006; 6: 165–82 [Google Scholar]
- 8.Bruinsma WE, Becker SJE, Guitton TG, Kadzielski J, Ring D. How prevalent are hazardous attitudes among orthopaedic surgeons? Clin Orthop 2015; 473: 1582–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kadzielski J, McCormick F, Zurakowski D, Herndon JH. Patient safety climate among orthopaedic surgery residents. J Bone Jt Surg 2011; 93: e62. [DOI] [PubMed] [Google Scholar]
- 10.Meunier A, Posadzy K, Tinghög G, Aspenberg P. Risk preferences and attitudes to surgery in decision making: a survey of Swedish orthopedic surgeons. Acta Orthop 2017; 88: 466–71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2022. Available from: https://mirrors.nics.utk.edu/cran/https://www.r-project.org. [Accessed 16 September 2023] [Google Scholar]
- 12.Vail GJ, Ekman LG. Pilot-error accidents: male vs. female. Appl Ergon 1986; 17: 297–303 [DOI] [PubMed] [Google Scholar]
- 13.Furedy M Gender differences and their relation to hazardous attitudes in pilot training. Coll Aviat Rev Int 2019; 37: 73 [Google Scholar]
- 14.Walton RO, Politano PM. Characteristics of general aviation accidents involving male and female pilots. Aviat Psychol Appl Hum Factors 2016; 6 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.