

Key Clinical Message
Congenital mastoid confined cholesteatoma is a very rare entity with only 30 reported cases worldwide. We describe the presentation and treatment of this condition in a 14‐year‐old boy, with maintenance of normal hearing and ear canal function.
Keywords: cholesteatoma, congenital, head and neck, mastoidectomy, otology, pediatrics, rare, reconstruction
Congenital mastoid‐isolated cholesteatoma.
1. CASE
A 14‐year‐old boy presented with a 12‐month history of recurrent low volume malodorous left ear discharge. It was yellow/green in color and persisted despite oral and topical antibiotics.
There was no associated neurotological symptoms.
Examination revealed posterior external canal wall erosion, with cholesteatoma visible in the defect. His tympanic membrane (TM) was normal.
His ear cultured Staphylococcus aureus and anaerobes. Pure tone audiometry (PTA) was normal, with Jerger type A tympanograms.
A high‐resolution temporal bone CT scan confirmed the presence of a large posterior external auditory canal (EAC) defect (Figure 1C) with associated isolated mastoid opacification (Figure 1A) and dehiscence of the vertical segment of the facial canal (Figure 1B). Middle ear cavity was aerated with intact ossicles and outer attic wall.
FIGURE 1.

High‐resolution temporal bone CT scan. (A) Blue arrow—Opacified left mastoid. Middle ear aerated with intact ossicular chain. (B) Green arrow—Posterior external auditory canal erosion. Blue arrow—Facial canal erosion. (C) High resolution temporal bone CT scan – Sagittal plane. Orange arrow—Opacified left mastoid with erosion of posterior EAC.
Treatment was with a left cortical mastoidectomy (See Section 3—Figures 2A–D).
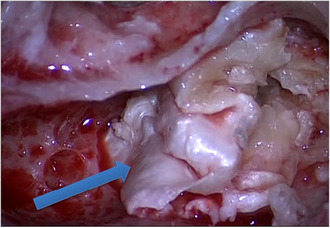
FIGURE 2.
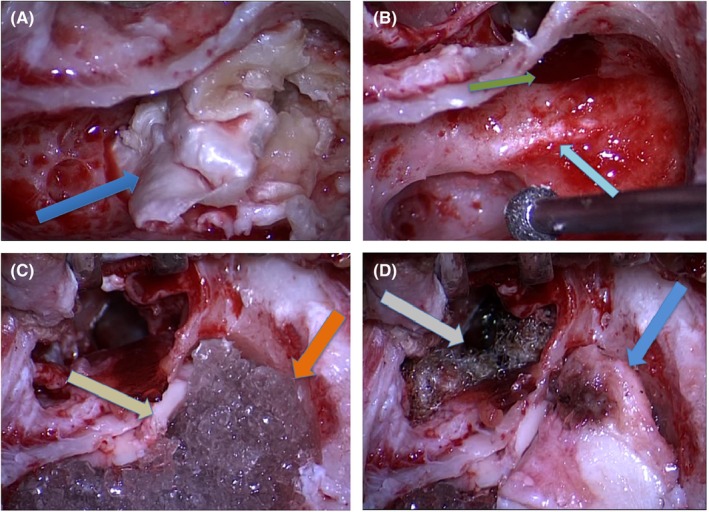
(A) Mastoid cholesteatoma. (B) Blue arrow—Dehiscent facial nerve; Green arrow—Mastoid antrum with posterior EAC bony erosion. (C) Yellow arrow—Conchal cartilage graft; Orange arrow—Bioactive glass. (D) Gray arrow—Fibrillar within the EAC; Blue arrow—Cartilaginous lateral mastoid wall.
At 12 months post‐op, he remains asymptomatic with normal hearing and ear canal appearance. Non‐echo‐planar diffusion‐weighted MRI scan showed no evidence of recurrence.
2. CT IMAGES
Figure 1
3. INTRAOPERATIVE DETAILS
A left cortical mastoidectomy was performed with facial nerve monitoring. Extensive cholesteatoma isolated to the well‐pneumatized mastoid was removed (Figure 2A). Fibrous and bony annulus were intact.
Vertical segment of facial nerve was dehiscent and the mastoid antrum with the posterior EAC bony erosion was clearly visible (Figure 2B).
Conchal cartilage graft was used to reconstruct the large posterior canal wall defect and the mastoid cavity was obliterated with the bioactive glass Bon‐Alive (Figure 2C).
Fibrillar was placed in EAC for graft support, and additional cartilage was used to reconstruct the lateral wall of mastoid cavity (Figure 2D).
4. DISCUSSION
Cholesteatomas are locally destructive, slow‐growing, keratinized squamous epithelial lesions. 1%–5% of cholesteatomas are congenital, usually arising from the petrous apex or middle ear. 1
Congenital cholesteatoma isolated to the mastoid is very rare, with less than 30 published cases. The “Implantation theory” postulates that squamous cells become trapped during the closure of the mastoid fontanelle, eventually forming cholesteatoma. 2
As the middle ear is spared, hearing is usually normal and they can grow significantly before detection, with a mean age of presentation of 51. 3 Presentation can be nonspecific, with vertigo, otorrhea, neck and mastoid pain described. It is often identified incidentally, however, can present with acute mastoiditis in adults. 2 All but one of the published cases have been managed surgically. 3
Careful review of preoperative imaging is vital as exposure of the facial nerve, sigmoid sinus or posterior fossa dura is frequent. As in our case, the external canal wall is commonly eroded.
Our case illustrates a very successful outcome with cortical mastoidectomy, obliteration and reconstruction of the EAC wall with conchal cartilage.
AUTHOR CONTRIBUTIONS
Dominic McKenna: Conceptualization; data curation; project administration; visualization; writing – original draft. Ekambar Reddy: Conceptualization; writing – review and editing.
CONFLICT OF INTEREST STATEMENT
None declared.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
ACKNOWLEDGEMENTS
None.
McKenna D, Reddy E. Congenital mastoid‐isolated cholesteatoma in a 14‐year‐old boy. Clin Case Rep. 2023;11:e8182. doi: 10.1002/ccr3.8182
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no datasets were generated or analyzed.
REFERENCES
- 1. Richards E, Muzaffar J, Cho WS, Monksfield P, Irving R. Congenital mastoid cholesteatoma. J Int Adv Otol. 2022;18(4):308‐314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Tabook S, Abdel Tawab HM, Gopal NK. Congenital cholesteatoma localised to the mastoid cavity presenting as a mastoid abscess. Case Rep Otolaryngol. 2015;2015:305494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Annalisa P, Giannicola I, Valeria R, et al. Isolated congenital mastoid cholesteatoma with no involvement of aditus ad antrum and middle ear. Clin Med Insights Case Rep. 2021;14:11795476211014032. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed.