

Abstract
Introduction
Vulvar intraepithelial neoplasia (VIN) is a vulvar skin lesion considered a precursor of vulvar squamous cell carcinoma. No characteristics have been discovered to date that allows us to differentiate between grades of VIN, such as correlating the thickness of involvement of the epithelium (VIN1, VIN2, and VIN3) to the dermoscopic pattern.
Objectives
The aim of this study was to correlate the clinical and dermoscopic features of VIN cases with histopathological findings, with the purpose of identifying dermoscopic characteristics that allow us to differentiate between different grades of VIN.
Methods
A retrospective study of the clinical and dermoscopic characteristics of VINs was recruited. Clinical and dermoscopic characteristics, as well as histopathology data, were gathered from patients at two Dermatology Units in Italy during the period spanning from January 2020 to December 2021.
Results
The study population consisted of 20 patients with a histologically confirmed diagnosis of VIN. The mean age of patients at the time of diagnosis was 55 years. At the dermoscopic level, VIN1 was characterized by a homogeneous erythematous area that completely involved the entire lesion, with a vascular pattern consisting of regular glomerular vessels. VIN3, was characterized by the presence of compact milky white areas that involved almost the entire lesion. VIN2 was characterized by the presence of non-compact white areas that allowed homogeneous erythematous areas to be seen transparently, without other distinguishing aspects.
Conclusions
Although a definitive diagnosis and grading of VIN remains confirmed only histopathologically, our study shows how dermoscopy may aid the differential diagnosis between the different grades of VIN; the presence of a compact milky white area that involves nearly the entire lesion should be interpreted as an alarming feature, while homogeneous erythematous areas or a glomerular vascular pattern are more typical of the first stage of this neoplasia.
Keywords: dysplastic nevus, melanoma, bibliometric analysis, co-citation analysis, CiteSpace
Introduction
Vulvar intraepithelial neoplasia (VIN) is a vulvar skin lesion considered a precursor of vulvar squamous cell carcinoma (SCC). According to the International Society for the Study of Vulvovaginal Disease (ISSVD) [1], a distinction must be made between VIN associated with HPV infection (also known as usual type, uVIN) and the HPV-independent form (differentiated vulvar intraepithelial neoplasia, dVIN), which is related to lichen sclerosus. The ISSVD further divides uVIN classification as either low-grade squamous intraepithelial lesion (L-SIL), which corresponds to VIN1, or high-grade SIL (HSIL or VIN 2/3) [1,2].
The three stages of uVIN are distinguished on the basis of the thickness of involvement of the vulvar epithelium by the dysplastic cells: VIN1 corresponds to involvement of only the lower third of the thickness of the surface layer; VIN2 corresponds to involvement of two-thirds the thickness of the dysplasia and VIN3 corresponds to involvement of the entire surface layer. Regarding the risk of progression into an actual SCC, it must be said that not all VIN types have the same probability of transformation; although isolated dVIN is significantly less common than uVIN, dVIN bears a greater risk for malignant transformation to vulvar SCC and progresses at a faster rate [3,4]. Furthermore, among uVIN, VIN1 (or L-SIL) is not considered a precancerous lesion; rather, it is considered a benign epithelial change caused mainly by the low-risk HPV types 6 and 11.
Despite this well-defined histopathological staging, the clinical morphology has not been clearly delineated, often resulting in delayed diagnosis.
For these reasons, and considering their link with SCC, it would be important to be able not only to recognize these lesions early, but also to type them according to their level of atypia. An early treatment of these injuries would save the patient considerable inconvenience and discomfort given the particular site. At present, there are no validated clinic and dermoscopic criteria available for VIN diagnosis, and little has been written about the dermoscopic patterns that characterize the different types and grades of this condition.
Only a few studies exist on this topic; however, some common dermoscopic features of VIN have been reported, such as a cerebriform pattern, focally distributed glomerular vessels, bluish areas, scales, and blue/brown dots arranged in a linear distribution [5–10]. These dermoscopic findings are mostly described in the uVin type. However, no characteristics have been discovered to date that allows us to differentiate between grades of uVIN, such as correlating the thickness of involvement of the epithelium (VIN1, VIN2, and VIN3) to the dermoscopic pattern.
Since no pathognomonic features have been described to identify VIN, a definitive diagnosis of VIN can only be achieved by biopsy and histological examination. However, we believe that dermoscopy may introduce important diagnostic clues and can complement clinical examination, thereby facilitating differential diagnosis (e.g. vulvar melanoma).
Objectives
Therefore, the objective of this research was to establish a correlation between the clinical and dermoscopic attributes of VIN cases and their corresponding histopathological findings. The ultimate goal was to identify specific dermoscopic characteristics that would enable differentiation among various grades of VIN.
Methods
This retrospective study examined data about patients who received a histopathologic diagnosis of vulvar intraepithelial neoplasia (VIN) between January 2020 and December 2021 at the Skin Cancer Units of the Department of Dermatology at the University of Florence and of the Department of Dermatology at the University of Parma. The Institutional Review Board approved this retrospective study. Patients were ineligible to participate if they were under 18 years old. Additional exclusion criteria included a history of vulvo-vaginal neoplasia, radiation therapy for other tumors, or ongoing or previous immunosuppressive therapy.
The patient database contains information about patient characteristics, in addition to clinical and dermoscopic features of the lesions. Each lesion was photographed clinically and dermoscopically. The equipment used for the dermoscopic examination consisted of a hand-held dermatoscope (HEINE DELTA 20, HEINEOptotechnick, Herrsching, Germany). Both clinical and dermoscopic images of all lesions were captured with a high-resolution compact digital photographic camera (Olympus E-520, a 7.1megapixel digital photo camera with a 3.8 optical zoom lens, a focal length of 28–105 mm in a 35-mm format, and a maximum lens aperture of f/2.8–f/5.8). Dermoscopic images were captured viaDermaphot (HEINEOptotechnick), which connects the dermatoscope to the camera to generate reproducible, high-quality dermoscopic pictures at 10-fold magnification.
Biopsies were taken for all lesions. Initially, an incisional biopsy was performed using a 4mm punch. The biopsy site was selected based on the most clinically and dermoscopically significant areas. Subsequently, the entire lesion was surgically excised. Clinical history, dermoscopic examinations, and histopathological features of the lesions were evaluated. Three investigators (V.D.G., I.S., and F.V.), who are skilled in dermoscopy and experienced in assessing genital lesions at their affiliated institutions, independently analyzed the archived digital dermoscopic images. They had no prior knowledge of the lesion’s clinical history. The investigators completed a printed questionnaire to classify the lesions based on typical dermoscopic pattern analysis. These dermatologists had the same level of training and each had more than 5 years of practical experience in dermoscopy. Dermoscopic pattern and the presence or absence of dermoscopic features in a given lesion was defined by the agreement of at least 2 out of 3 dermatologists. The color of the lesion was also recorded. Histopathological slides were reviewed by a dermatopathologist with expertise in vulvar lesions to confirm the diagnosis and evaluate the dermoscopic-histopathological correlates.
Results
Twenty cases were included in the final analysis. Of the 24 cases of VIN that were observed between January 2020 and December 2021, 4cases were excluded because of lack histological data, absence of clear clinical or dermoscopic images, or both.
The mean age of patients at the time of diagnosis was 55 years (range 41–79), 60% (N= 12) of the patients were in menopause at the time of diagnosis, and 65% (N= 13) had received hormone therapy or contraceptive or hormone replacement following menopause for a period of at least 12 months before VIN diagnosis. Among these 20 patients, 35% (N= 7) were under the age of 50 years (Table 1).
Table 1.
Demographic, clinical and dermoscopic characteristics of the study cases
| N° patients (%) | Age Range | Clinic Characteristics | Dermoscopic Characteristics | |
|---|---|---|---|---|
| Enrolled patients | 20 | 41–79. | N/A | N/A |
| Under 50 years | 7 (35) | N/A | N/A | |
| Menopause | 12 (60) | N/A | N/A | |
| Hormonal Therapy/Contraceptive/ Hormone replacement | 13 (65) | N/A | N/A | |
| Clinical aspect | ||||
| Pigmented VIN | 2 (10) | Pigmented lesion with a color spectrum from light brown to dark brown in the perivaginal keratinized area (not in the mucosa) | Diffuse pigmentation, linear distribution with delimited translucent whitish areas and no pigmented network | |
| Non-Pigmented VIN | 18 (90) | red to white non-pigmented lesions localized in the mucosa | atypical vascular pattern with a variable red to white background | |
| Histopathology | ||||
| uVIN | 15 (75) | N/A | N/A | |
| dVIN | 5 (25) | N/A | N/A | |
| Degree of atypia | ||||
| VIN1 | 10 (50) | Reddish shiny lesions with clear margins | Homogeneous erythematous area (entire lesion), does not disappear under pressure with the dermatoscope. Vascular pattern: regular glomerular vessels. | |
| VIN2 | 3 (15) | whitish erythematous discromic lesion | Non-compact white areas, homogeneous with erythematous areas to be seen transparently. | |
| VIN3 | 7 (35) | Whitishdiscromic lesion | Compact milky white areas (entire lesion) | |
N/A = not applicable; VIN = vulvar intraepithelial neoplasia.
From a clinical point of view, the VIN was pigmented in 10% (2 patients) of cases, and in all of these cases, the pigmentation was not present in the mucosa but in the perivaginal keratinized area. The other lesions (90%) were non-pigmented erythematous and localized in the mucosa.
Regarding the outcomes of histological examinations, 75% (15 patients) were represented by uVIN and only 5 patients by dVIN, while for the grades of atypia, 50% (10 patients) were VIN1, 15% (3patients) were VIN2, and 35% (7 patients) were VIN3. All patients diagnosed with VIN3 were over age 65 years, and in three of these cases, a mucosal melanosis was also present. In five cases (25%), the lesions were multiple, and in one patient all levels of VIN were detected (VIN1, VIN2, VIN3).
At the dermoscopic level, VIN1 was characterized by a homogeneous erythematous area that completely involved the entire lesion, without disappearing following the application of pressure with the dermatoscope. Within this erythematous area, in the absence of other dermoscopic parameters, a vascular pattern consisting of regular glomerular vessels arranged throughout the lesion could be seen (Figure 1). VIN3, on the other hand, was characterized by the presence of compact milky white areas that involved almost the entire lesion, replacing the erythematous areas of VIN1 (Figure 2).
Figure 1.

A 55-year-old patient affected by multiple vulvar intraepithelial neoplasia1. (A) Clinically, reddish papillomatous shiny lesions of the vulva. (B) Dermoscopy showed a homogeneous pink to red background. (C) Dermoscopically, a vascular pattern consisting of regular glomerular vessels arranged throughout the lesion could be seen.
Figure 2.
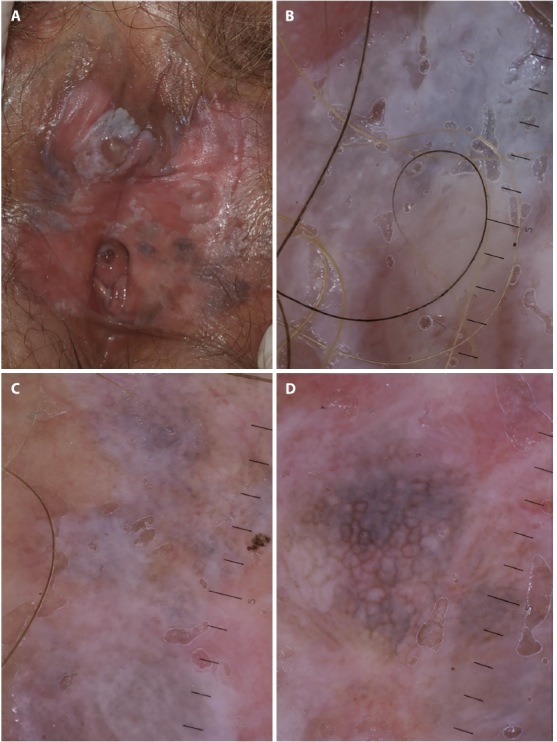
A 72-year-old patient affected by multifocal vulvar intraepithelial neoplasia (VIN). (A)Clinically, numerous erythematous and white areas, some infiltrated with areas of peripheral brown-like pigmentation of the labia minora and vaginal introitus, can be seen. (B)Dermoscopy revealed compact milky-white areas involving areas affected by VIN grade 3. (C)Dermoscopy shows non-compact white areas that allowed homogeneous erythematouszones to be seen transparently, involving area affected by VIN grade 2. (D)Dermoscopically, diffuse pigmentation with a linear arrangement can be seen, with a clearly delimited translucent whitish area involving areas affected by multifocal VIN.
In the three cases of VIN2, dermoscopy was characterized by the presence of non-compact white areas that allowed homogeneous erythematous areas to be seen transparently, without other distinguishing aspects.
Dermoscopically, the pigmented VINs exhibited diffuse pigmentation, with a linear distribution with clearly delimited translucent whitish areas and no pigmented network (Figure 3).
Figure 3.
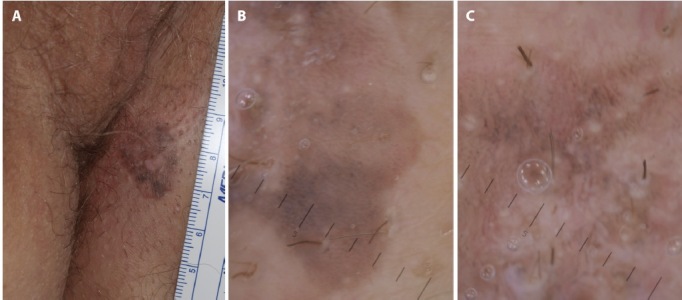
A 70-year-old patient affected by pigmented vulvar intraepithelial neoplasia3. (A) Clinically, flat pigmented perivaginal macule with well demarcated edges, but with inhomogeneous color distribution, can be seen. (B) Dermoscopically, the lesion showed diffuse pigmentation with a linear distribution, with clearly delimited translucent whitish islands and no pigmented network.
In our case series, two patients presented a non-specific pattern due to the absence of well-defined or recognizable dermoscopic features. Furthermore, there were no peculiar dermoscopic parameters that would allow us to make a differential diagnosis between uVIN and dVIN.
Conclusions
Owing to the extreme heterogeneity of lesions, little has been written about the long-term clinical behavior of VINs, and only a few studies to date have analyzed their specific clinical and dermatoscopic features. In this study, we aimed to investigate the dermoscopic characteristics of these conditions, which might be useful not only for VIN characterization and diagnosis, but also to help guide treatment, in order both to assess the efficacy of topical therapy and to ensure conservative excisions in such critical areas.
It is known that it is possible to find multiple sites and different degrees of intrahepitelial neoplasia in the same patient. Several biopsies or a so-called vulvar mapping are commonly performed in patients with multifocal VIN to confirm the clinical diagnosis and to exclude the presence of underlying invasive neoplasia [12]. We believe that the identification of specific dermoscopic features that allow for differentiation between grades of intraepithelial neoplasia could help minimize the number of unneeded genital biopsies and guide topical treatment with imiquimod.
Although a definitive diagnosis and grading of VIN remains confirmed only histopathologically, our study shows how dermoscopy may aid the differential diagnosis between the different grades of VIN; the presence of a compact milky white area that involves nearly the entire lesion should be interpreted as an alarming feature, while homogeneous erythematous areas or a glomerular vascular pattern are more typical of the first stage of this neoplasia. This dermoscopic compact milky white area corresponds histopathologically to an important hyperkeratosis, typical of VIN3 (Fig.4). Therefore, as happens in the dermoscopic evaluation of mucosal melanomas and mucosal melanosis, in the dermoscopic diagnosis of vulvar VIN, a correct evaluation of the colors present in the lesion is important, rather than the presence of isolated dermoscopic parameters. So, the whiter is present, the greater the likelihood that the VIN is at grade 3 (VIN3).
Figure 4.
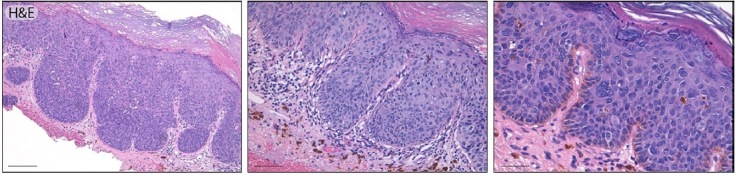
Histological appearance of high grade squamous intraepithelial lesion (vulvar intraepithelial neoplasia III, usual type). The lesion at scanning magnification shows a complete loss of maturation, an increased nuclear density and hyperkeratosis (left image, scale bar 200 micron, original magnification x10). A band of inflammatory cells in the superficial derma can be seen (middle image, scale bar 100-micron, original magnification x20). Higher magnification demonstrates cellular loss of polarity, an increased number of mitoses and nuclear atypia involving all the epithelial layers (right image, scale bar 50 micron, original magnification x40).
In our study, all patients diagnosed with VIN3 were over 65 years of age. Furthermore, all three grades of VIN (VIN1, VIN2, VIN3) were detected in one of our patients, testifying to the slow progression of cytoarchitectural atypia through the vulvar epithelium. In our cohort, we did not observe any distinctive dermoscopic clues that allowed the differentiation between uVIN and dVIN. In a case-series of four female patients [7], Barisani et al. observed differences in vessel morphology between these two entities. Specifically, they reported that uVIN presented with dotted or glomerular vessels, while dVIN presented with many curvy teleangectasias [7]. However, this distinction has not been investigated thoroughly, and these findings may not be relevant given the limited number of cases.
We hardly found typical features of VIN2, which was partially due to the lack of VIN2 cases in our cohort and partially to the fact that VIN2 is considered a type of “gray zone” between VIN1 and VIN3.
According to the few studies published on this topic, 10–15% of VINs are grossly hyperpigmented.7,13 Pigmented VINs accounted for only 10% of the VINs in our study and were present in keratinized perimucosal regions. The clinical picture was characterized by a pigmented lesion with sharp edges but inhomogeneous in pigment distribution. According to some reports, a cerebriform pattern as well as parallel pigmented dots are possible findings in pigmented VIN [6–8]. However, these patterns are also typically found in other skin conditions such as seborrheic keratosis, Bowen disease, and bowenoid papulosis. In our study, dermoscopically, we can see the presence of whitish islands within the lesion, with a brown background pigment. This dermoscopic pattern is difficult to find in other skin lesions and can, therefore, be useful in a preoperative diagnostic process.
In our cohort, the association with vulvar melanosis seems to be strictly linked with VIN grade 3. This finding could either be random or linked to hormonal stimulation. It is well known that estrogens that increase melanin synthesis are involved in the genesis of vulvar melanosis [14,15]. Infact, 65% of our patients underwent hormonal therapy for a period of at least 12 months before VIN diagnosis.
The strength of this study lies in the number of cases; as far as we know, this case series has the largest number of patients reported to date. Nevertheless, further studies are needed to better characterize the dermoscopic features of VIN and to corroborate our findings.
Footnotes
Competing Interests: None.
Authorship: All authors have contributed significantly to this publication.
Funding: None.
References
- 1.Bornstein J, Bogliatto F, Haefner HK, et al. The 2015 International Society for the Study of Vulvovaginal Disease (ISSVD) Terminology of Vulvar Squamous Intraepithelial Lesions. Obstet Gynecol. 2016;127(2):264–268. doi: 10.1097/AOG.0000000000001285. [DOI] [PubMed] [Google Scholar]
- 2.Höhn AK, Brambs CE, Hiller GGR, May D, Schmoeckel E, Horn LC. 2020 WHO Classification of Female Genital Tumors. GeburtshilfeFrauenheilkd. 2021;81(10):1145–1153. doi: 10.1055/a-1545-4279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cohen PA, Anderson L, Eva L, Scurry J. Clinical and molecular classification of vulvar squamous pre-cancers. Int J Gynecol Cancer. 2019;29(4):821–828. doi: 10.1136/ijgc-2018-000135. [DOI] [PubMed] [Google Scholar]
- 4.Thuijs NB, van Beurden M, Bruggink AH, Steenbergen RDM, Berkhof J, Bleeker MCG. Vulvar intraepithelial neoplasia: Incidence and long-term risk of vulvar squamous cell carcinoma. Int J Cancer. 2021;148(1):90–98. doi: 10.1002/ijc.33198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hoang LN, Park KJ, Soslow RA, Murali R. Squamous precursor lesions of the vulva: current classification and diagnostic challenges. Pathology. 2016;48(4):291–302. doi: 10.1016/j.pathol.2016.02.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ronger-Savle S, Julien V, Duru G, Raudrant D, Dalle S, Thomas L. Features of pigmented vulval lesions on dermoscopy. Br J Dermatol. 2011;164(1):54–61. doi: 10.1111/j.1365-2133.2010.10043.x. [DOI] [PubMed] [Google Scholar]
- 7.Barisani A, Dika E, Fanti PA, et al. Dermoscopic findings of vulvar intraepithelial neoplasia: a series of four cases. Br J Dermatol. 2017;176(1):227–230. doi: 10.1111/bjd.14796. [DOI] [PubMed] [Google Scholar]
- 8.Vaccari S, Barisani A, Preti EP, et al. Dermoscopic features of pigmented vulvar intraepithelial neoplasia. Clin Exp Dermatol. 2018;43(1):63–65. doi: 10.1111/ced.13245. [DOI] [PubMed] [Google Scholar]
- 9.Vaccari S, Barisani A, Preti EP, et al. Vulvar intraepithelial neoplasia and vulvar squamous cell carcinoma: differential dermoscopic features in a case series, and a progression model. Clin Exp Dermatol. 2018;43(4):469–471. doi: 10.1111/ced.13380. [DOI] [PubMed] [Google Scholar]
- 10.Maione V, Errichetti E, Dehen L, CavelierBalloy B, Lebbé C. Usual-type vulvar intraepithelial neoplasia: report of a case and its dermoscopic features. Int J Dermatol. 2016;55(12):e621–e623. doi: 10.1111/ijd.13370. [DOI] [PubMed] [Google Scholar]
- 11.Tosti G, Iacobone AD, Preti EP, et al. The Role of Photodynamic Therapy in the Treatment of Vulvar Intraepithelial Neoplasia. Biomedicines. 2018;6(1):13. doi: 10.3390/biomedicines6010013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Thuijs NB, Schonck WAM, Klaver LLJ, et al. Biomarker Expression in Multifocal Vulvar High-Grade Squamous Intraepithelial Lesions. Cancers (Basel) 2021;13(22):5646. doi: 10.3390/cancers13225646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim JM, Lee HJ, Kim SH, et al. Efficacy of 5% imiquimod cream on vulvar intraepithelial neoplasia in Korea: pilot study. Ann Dermatol. 2015;27(1):66–70. doi: 10.5021/ad.2015.27.1.66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.De Giorgi V, Gori A, Salvati L, et al. Clinical and Dermoscopic Features of Vulvar Melanosis Over the Last 20 Years. JAMA Dermatol. 2020;156(11):1185–1191. doi: 10.1001/jamadermatol.2020.2528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cario M. How hormones may modulate human skin pigmentation in melasma: An in vitro perspective. Exp Dermatol. 2019;28(6):709–718. doi: 10.1111/exd.13915. [DOI] [PubMed] [Google Scholar]