

Abstract
Background
Previous research reports that patients with mental health conditions experience benefits, for example, increased empowerment and validation, from reading their patient-accessible electronic health records (PAEHRs). In mental health care (MHC), PAEHRs remain controversial, as health care professionals are concerned that patients may feel worried or offended by the content of the notes. Moreover, existing research has focused on specific mental health diagnoses, excluding the larger PAEHR userbase with experience in MHC.
Objective
The objective of this study is to establish if and how the experiences of patients with and those without MHC differ in using their PAEHRs by (1) comparing patient characteristics and differences in using the national patient portal between the 2 groups and (2) establishing group differences in the prevalence of negative experiences, for example, rates of errors, omissions, and offenses between the 2 groups.
Methods
Our analysis was performed on data from an online patient survey distributed through the Swedish national patient portal as part of our international research project, NORDeHEALTH. The respondents were patient users of the national patient portal 1177, aged 15 years or older, and categorized either as those with MHC experience or with any other health care experience (nonmental health care [non-MHC]). Patient characteristics such as gender, age, education, employment, and health status were gathered. Portal use characteristics included frequency of access, encouragement to read the record, and instances of positive and negative experiences. Negative experiences were further explored through rates of error, omission, and offense. The data were summarized through descriptive statistics. Group differences were analyzed through Pearson chi-square.
Results
Of the total sample (N=12,334), MHC respondents (n=3131) experienced errors (1586/3131, 50.65%, and non-MHC 3311/9203, 35.98%), omissions (1089/3131, 34.78%, and non-MHC 2427/9203, 26.37%) and offenses (1183/3131, 37.78%, and non-MHC 1616/9203, 17.56%) in the electronic health record at a higher rate than non-MHC respondents (n=9203). Respondents reported that the identified error (MHC 795/3131, 50.13%, and non-MHC 1366/9203, 41.26%) and omission (MHC 622/3131, 57.12%, and non-MHC 1329/9203, 54.76%) were “very important,” but most did nothing to correct them (MHC 792/3131, 41.29%, and non-MHC 1838/9203, 42.17%). Most of the respondents identified as women in both groups.
Conclusions
About 1 in 2 MHC patients identified an error in the record, and about 1 in 3 identified an omission, both at a much higher rate than in the non-MHC group. Patients with MHC also felt offended by the content of the notes more commonly (1 in 3 vs 1 in 6). These findings validate some of the worries expressed by health care professionals about providing patients with MHC with PAEHRs and highlight challenges with the documentation quality in the records.
Keywords: electronic health records, EHR, mental health, mental health care, national survey, online records access, open notes, ORA, patient-accessible electronic health record, PAEHR, patients, user experiences
Introduction
Online patient portals are a common means for patients to gain online record access (ORA), often through services referred to as patient-accessible electronic health records (PAEHRs). Through PAEHRs, patients are offered access to, for example, test and laboratory results, a list of prescribed medications, and referrals. Clinical notes, or narrative visit reports, written by the clinician are considered an essential part of any PAEHR and are often referred to as “open notes” when shared with patients [1]. Online patient portals are becoming more widespread internationally. The European Commission has proposed the European Health Data Space, with one of its aims being to give all European Union citizens access to their electronic health record (EHR) [2]. Since April 2021, the US federal law 21st Century Cures Act has mandated all health organizations to offer patients secure online access to their clinical information housed in their EHRs, including notes written by clinicians, tests, lab results, and referrals; however, access excludes psychotherapy notes [3].
In research, patients with mental health conditions have reported that online access to their mental health records increases feelings of greater validation [4], engagement [4-6], potentially augments patient autonomy [4,7], patient empowerment [7-9], and can increase trust in their clinician [4-6]. Other common experiences perceived by patients with mental health conditions when reading their mental health notes include feelings of having control of their care [4,10-12], and increased understanding of their mental health [10,11], and their medication’s potential side effects [10,11,13,14].
However, albeit limited in numbers, some studies report that some patients with mental health conditions could feel worried or offended by the content of the notes [4,5,10-12]. Patients sometimes find the content of the notes judgmental, disrespectful, and inaccurate [4-6,10] and are worried about being misinterpreted by the health care professional (HCP) and finding errors in the notes [15]. The latter is supported by previous research where experts in a Delphi survey agreed that they expected errors to arise in patients’ mental health notes [16]. Another qualitative survey of stakeholders, including mental health professionals, patients, and informaticians, concluded that further refinement of exemption policies, clinician training, and patient guidance are required in writing mental health notes [17]. Furthermore, due to patient access, mental HCPs note that they might change how they document, such as intentionally leaving out essential clinical information [18-25], concerned that patients might be offended, confused, or anxious by what they read [10,18-21,26]. Some HCPs have reported keeping a “shadow record” due to patient access—in other words, keeping notes outside the official EHR system [27]. HCPs in mental health care (MHC) have also expressed fear of threats or violence from patients and adverse effects on the therapeutic alliance [18,28]. However, some HCPs report benefits with patient access to their mental health notes, such as strengthened patient-provider relationships [22,26,29,30], increased feelings of trust [20,26,30], and increased transparency [21,26,30].
MHC in Sweden encompasses physicians, psychologists, nurses, assistant nurses, occupational and physical therapists, social workers, and medical secretaries from inpatient care, outpatient care, and psychotherapy care. In Sweden, it is possible to receive MHC at the primary care level. Patients have access to their mental health information through Journalen, the Swedish national PAEHR, where patients are offered to see their laboratory and test results, diagnoses, referrals, and medications and read their clinical notes from MHC in 17 out of 21 regions [1]. Clinical information is shared with patients in Journalen regardless of the health care profession or health care setting. Since Sweden has a decentralized health care system with 21 autonomous regions, there are geographical differences with respect to the mental health information patients can access in the PAEHR, depending on where the patient seeks care [1].
Sharing access to mental health records is still controversial and raises ethical concerns about balancing openness with the risk of harm [31,32]. Many psychiatric organizations and regions in Sweden have resisted the implementation as HCPs worry that patients will become anxious, confused, or upset by what they read [18,20,23]. Like in other countries where the practice is implemented, research on patients with MHCs’ experiences of accessing and reading their mental health records is limited. Previously published studies exploring the experiences of patients with MHC have been conducted predominantly in the United States [15]. A Swedish national patient survey was conducted in 2016 to investigate patients’ experiences accessing their EHR [8], however, with a limited focus on mental health. In the NORDeHEALTH research project [33], an online patient survey was performed to explore the experiences of patients’ ORA [34], providing a greater opportunity to investigate the experiences of patients with MHC with accessing and reading their PAEHR. Importantly, most or all research on the interaction between the presence of mental health diagnoses and experience with PAEHR has focused on patients with specific diagnoses [15,32]. This excludes the wider user population, who may have experience with MHC but not necessarily a formal diagnosis.
This study aims to understand if and how patients’ experiences of ORA differ depending on whether they have received MHC or not. More specifically, we will (1) explore how participant characteristics and interaction with the national PAEHR differ between patients who have received MHC and those who have not, and (2) compare the rate of errors, omissions, and offenses between patients who have received MHC and those who have not.
Methods
Overview
To study patients’ experiences of ORA, we conducted an online nationwide survey as part of NORDeHEALTH, our international research project studying the implementation of patient portals in Estonia, Finland, Norway, and Sweden [33]. The survey is known as the NORDeHEALTH 2022 Patient Survey, and its methodology is fully described elsewhere [34]. This paper focuses on the Swedish data set.
Survey Structure
The whole Swedish survey consisted of 45 questions (38 closed-ended and 7 free-text) divided into seven thematic sections: (1) sociodemographic information; (2) experience with health care; (3) experience with ORA through the patient portal; (4) reasons for and impact of using the health record; (5) errors, omissions, and offenses; (6) security and privacy; and (7) usefulness of information and functions [34]. This study focuses on the following sections: sociodemographic information; experience with health care; experience with ORA through the patient portal; reasons for using the patient portal (subsection: having access to my health record); errors, omissions, and offenses. There were both single- and multiple-choice questions with various response options: “yes” and “no” answers, and Likert scale ratings. All of the included closed-ended questions were mandatory to answer. Questions were partially developed based on previous studies (Moll et al [8], Kujala et al [35], and Zanaboni et al [36]). Before distribution, the survey was pilot-tested with patients. The pilot study proved to be useful in providing insights into the questions, which involved some changes, such as new words and changes to the sequence of the questions. In Sweden, the survey was administered only in Swedish (Multimedia Appendices 1 and 2).
Data Collection
The survey was distributed through the national patient portal, 1177. The survey link was placed as a notification that appeared to patient users after logging into their national patient portal accounts and entering the PAEHR section of the portal, Journalen. This ensured that only verified users of the portal were surveyed. The data collected through the survey were not linked to the patient accounts, so they remained anonymous. The survey was built using Webropol (Webropol Sverige AB) and was available for 3 weeks from January 23, 2022. Only participants aged 15 years or older were eligible to take part. Participation was voluntary. Data were collected through convenience sampling; there were no preset quotas for gender, age, or other sociodemographic characteristics.
Group Definition
In total, 13,008 patient users answered the online survey. In line with the study’s aims, we focused on a subsample of patients with MHC experience and those with any other health care experience. This was achieved by filtering through the question, “Have you been in contact with a health care professional in the last two years for any of the following?” The answer options were “cancer,” “mental health,” “other health problems,” and “no care or treatment.” It was a multiple-choice question, so participants could select as many as appropriate (Table 1). Participants who indicated no care or treatment (674/13,008, 5.18%) were excluded from the analysis. Those who chose the mental health option were included in the MHC group regardless of whether they also selected the options for cancer and other health problems. Those who did not choose the mental health option and did not select “no care or treatment” were included in the nonmental health care group (non-MHC).
Table 1.
Group definition.
| Survey item | MHCa (n=3131), n (%) | non-MHCb (n=9203), n (%) | |
| Have you been in contact with a health care provider in the last 2 years for any of the followingc? | |||
|
|
Mental health | 3131 (100) | N/Ad |
|
|
Cancer | 174 (5.56) | 1530 (16.63) |
|
|
Other health problems | 2441 (77.96) | 8605 (93.50) |
| On what level of care did you receive MHCc? | |||
|
|
Primary care | 1937 (61.87) | N/A |
|
|
Hospital outpatient | 1809 (57.78) | N/A |
|
|
Hospitalized or inpatient | 443 (14.15) | N/A |
|
|
Emergency care | 386 (12.33) | N/A |
| Duration of MHC | |||
|
|
Less than 3 months | 471 (15.04) | N/A |
|
|
3 months to 1 year | 528 (16.86) | N/A |
|
|
1 to 3 years | 520 (16.61) | N/A |
|
|
Greater than 3 years | 1612 (51.49) | N/A |
| Have you read about your MHC online in Journalen? | |||
|
|
Read all or almost all of my records | 2105 (67.23) | N/A |
|
|
Read some of the records | 697 (22.26) | N/A |
|
|
Did not read the record | 329 (10.51) | N/A |
aMHC: mental health care.
bnon-MHC: nonmental health care.
cDue to the question being multiple-choice, the total will not add up to 100%.
dN/A: not applicable.
Statistical Analysis
Analysis focused on closed-ended questions from the sections on sociodemographic information; experience with health care; experience with ORA through the patient portal; reasons for using the patient portal (having access to my health record); errors, omissions, and offenses (Multimedia Appendix 1). To address aim 1, we calculated descriptive statistics for participant characteristics (gender, age, education, health care education, employment, and health status) and variables describing portal use experience (frequency of use, encouraged or reminded to read the EHR, and positive and negative experience with the PAEHR). Groups were compared on single-choice questions through the Pearson chi-square test, for which statistical significance was set at P<.05. To address aim 2, we calculated summative statistics.
To further analyze group differences in the rates of perceived errors, omissions, and offenses, we used stratified random sampling with proportional allocation [37]. Through it, we created subsamples of the MHC and non-MHC groups that were matched by gender and age. The size of the strata was dictated by the MHC group data (Multimedia Appendix 3). The numbers of participants with “other” as gender response did not match the numbers between the groups for stratification and were thus omitted from both subsamples (n=76; Multimedia Appendix 3). Descriptive statistics and chi-square test were then used to compare the resultant subsamples. The groups were compared on single-choice questions through Pearson chi-square test, for which statistical significance was set at P<.05.
All analyses were carried out in JASP (version 0.16.2; University of Amsterdam) by 2 researchers (AB and AK) independently. Figures were created with Datawrapper (Datawrapper GmbH). Free-text responses will be presented in a future publication to allow for an in-depth qualitative analysis. All data were used, and no outliers were eliminated. A second researcher (AK) validated the data presented in the results.
Ethical Considerations
Ethical approval was granted by the Swedish Ethical Review Authority (EPN 2021/05229) before data collection. Informed consent was acquired at the start of the survey. If participants did not consent to the outlined conditions, they did not proceed with the survey, and no data were recorded. All the collected data were anonymous. Study participants received no compensation.
Results
Overview
Out of 13,008 participants, a total of 12,334 (94.82%) stated that they had received some care or treatment in the last 2 years. Of these, a quarter (3131/12,334, 25.39%) reported seeking MHC in the last 2 years, and the majority (9203/12,334, 74.61%) indicated they required other health care (non-MHC). The geographical distribution of both groups was comparable, but some differences were noted (Figure 1). There were more MHC respondents in the Dalarna and Västra Götaland regions than respondents from the non-MHC group. In both groups, the highest proportion of responses came from the Stockholm and Skåne regions.
Figure 1.
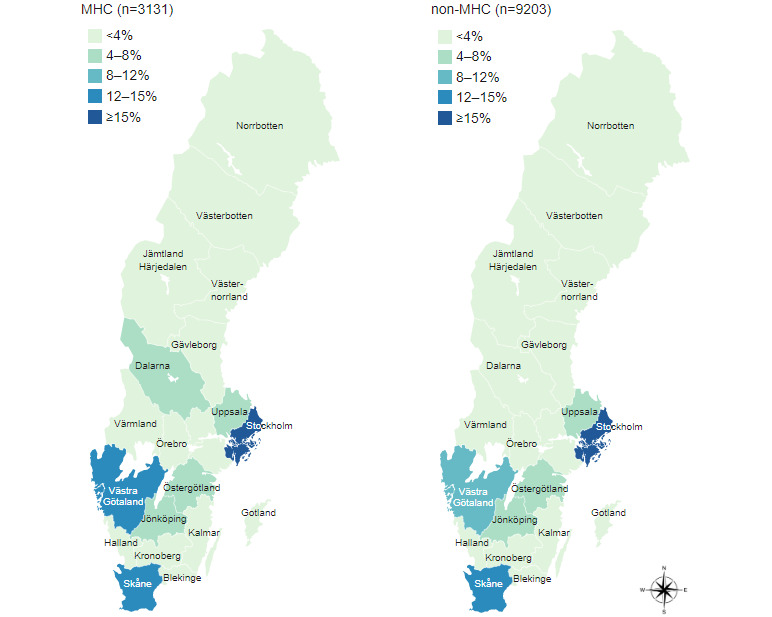
Geographical distribution of which region the respondents’ health care mainly takes place. MHC: mental health care; non-MHC: nonmental health care.
Participant Characteristics
Both MHC and non-MHC respondents most commonly identified themselves as women (MHC 2373/3131, 75.79%, and non-MHC 5936/9203, 64.5%), but the proportion of men was higher in the non-MHC group (MHC 701/3131, 22.39%, and non-MHC 3248/9203, 35.29%; Table 2). Notably, more participants identified as another gender in the MHC group (MHC 57/3131, 1.82%, and non-MHC 19/9203, 0.21%). The largest age group among the MHC respondents was aged between 25 and 34 years (820/3131, 26.19%), while the largest age group among the non-MHC respondents was aged between 65 and 74 years (2403/9203, 26.11%). Among respondents in the MHC group, the most common education level was upper secondary education (920/3131, 29.38%), while in the non-MHC group, the most common education level was second-cycle higher education (2593/9203, 28.18%). In both groups, most of the respondents had no education in health care. The most common employment status in the MHC group was full-time employment (1156/3131, 36.92%), while in the non-MHC group, most of the respondents were retired (3717/9203, 40.39%), closely followed by full-time employment (3555/9203, 38.63%). In both groups, the overall health among the respondents was “fair” (MHC 1149/3131, 36.70%, and non-MHC 3723/9203, 40.45%), but the proportion of participants with poor health, that is, rated as “bad” or “very bad,” was higher among MHC respondents (1225/3131, 39.12%) than the non-MHC respondents (1920/9203, 20.86%).
Table 2.
Sample descriptives.
| Survey item | MHCa (n=3131), n (%) | non-MHCb (n=9203), n (%) | P valuec | |||||
| Gender | <.001 | |||||||
|
|
Woman | 2373 (75.79) | 5936 (64.50) |
|
||||
|
|
Man | 701 (22.39) | 3248 (35.29) |
|
||||
|
|
Other | 57 (1.82) | 19 (0.21) |
|
||||
| Age (years) | <.001 | |||||||
|
|
15-19 | 120 (3.83) | 73 (0.79) |
|
||||
|
|
20-24 | 239 (7.63) | 153 (1.66) |
|
||||
|
|
25-34 | 820 (26.19) | 762 (8.28) |
|
||||
|
|
35-44 | 656 (20.95) | 1053 (11.44) |
|
||||
|
|
45-54 | 638 (20.38) | 1521 (16.53) |
|
||||
|
|
55-64 | 467 (14.92) | 1972 (21.43) |
|
||||
|
|
65-74 | 141 (4.50) | 2403 (26.11) |
|
||||
|
|
75-84 | 48 (1.53) | 1181 (12.83) |
|
||||
|
|
>85 | 2 (0.06) | 85 (0.92) |
|
||||
| Highest attained education | <.001 | |||||||
|
|
No formal education | 19 (0.61) | 49 (0.53) |
|
||||
|
|
Primary school | 311 (9.93) | 730 (7.93) |
|
||||
|
|
Upper secondary education | 920 (29.38) | 2325 (25.26) |
|
||||
|
|
Higher education: vocational | 464 (14.82) | 1431 (15.55) |
|
||||
|
|
Higher education: ≤3 years | 584 (18.65) | 1769 (19.22) |
|
||||
|
|
Higher education: >3 years | 774 (24.72) | 2593 (28.18) |
|
||||
|
|
Higher education: research (licentiate or PhD) | 59 (1.88) | 306 (3.33) |
|
||||
| Have health care education | 1100 (35.13) | 2971 (32.28) | <.001 | |||||
| Employment status | <.001 | |||||||
|
|
Full-time | 1156 (36.92) | 3555 (38.63) |
|
||||
|
|
Part-time | 431 (13.77) | 756 (8.21) |
|
||||
|
|
Student | 380 (12.14) | 288 (3.13) |
|
||||
|
|
Retired | 283 (9.04) | 3717 (40.39) |
|
||||
|
|
Unemployed | 143 (4.57) | 161 (1.75) |
|
||||
|
|
Not able to work | 397 (12.68) | 300 (3.26) |
|
||||
|
|
None of the above | 341 (10.89) | 426 (4.63) |
|
||||
| Health status | <.001 | |||||||
|
|
Very good | 108 (3.45) | 774 (8.41) |
|
||||
|
|
Good | 525 (16.77) | 2606 (28.32) |
|
||||
|
|
Fair | 1149 (36.70) | 3723 (40.45) |
|
||||
|
|
Bad | 961 (30.69) | 1626 (17.67) |
|
||||
|
|
Very bad | 264 (8.43) | 294 (3.19) |
|
||||
|
|
Do not know or do not want to answer | 124 (3.96) | 180 (1.96) |
|
||||
aMHC: mental health care.
bnon-MHC: nonmental health care.
cP value is derived from the chi-square test comparing the MHC and non-MHC subsamples on a given variable.
Interaction With the PAEHR Service
There was a statistically significant association between the respondent group and the frequency of reading the EHR (N=12,334; χ23=176.9; P<.001). Almost half of the MHC group respondents had read their EHR more than 20 times in the last 12 months (1425/3131, 45.48%), compared with a third in the non-MHC group (3027/9203, 32.89%; Table 3). In both groups, most of the respondents indicated that nobody encouraged them to read their EHR (N=12,334; MHC 2028/3131, 64.77%, and non-MHC 6305/9203, 68.51%; χ21=14.9; P<.001). A statistically significant association between the respondent group and negative experiences with the EHR was found (N=12,334; χ21=42.0; P<.001). Almost a third of respondents in the MHC group (999/3131, 31.91%) reported having a very negative experience with the EHR, compared with the non-MHC group (2386/9203, 25.93%).
Table 3.
Interaction with the national patient-accessible electronic health record.
| Survey item | MHCa (n=3131), n (%) | non-MHCb (n=9203), n (%) | P valuec | |||
| How often have you read your EHRd during the last 12 months? | <.001 | |||||
|
|
This is my first time | 56 (1.79) | 195 (2.12) |
|
||
|
|
2 to 9 times | 860 (27.47) | 3467 (37.67) |
|
||
|
|
10 to 20 times | 791 (25.26) | 2514 (27.32) |
|
||
|
|
Greater than 20 times | 1424 (45.48) | 3027 (32.89) |
|
||
| Were you encouraged by someone or reminded to read your EHR? | <.001 | |||||
|
|
Yes | 1103 (35.23) | 2898 (31.49) |
|
||
|
|
No, nobody encouraged me | 2028 (64.77) | 6305 (68.51) |
|
||
| Had a very positive experience with the health record | 1309 (41.81) | 4075 (44.28) | .02 | |||
| Had a very negative experience with the health record | 999 (31.91) | 2386 (25.93) | <.001 | |||
aMHC: mental health care.
bnon-MHC: nonmental health care.
cP value is derived from the chi-square test comparing the MHC and non-MHC subsamples on a given variable.
dEHR: electronic health record.
Among participants who noted they had been encouraged by someone or reminded to read their EHR online, most responses were “family and friends” in the MHC group (MHC 368/1103, 11.75%, and non-MHC 932/2898, 10.13%). In the non-MHC group, most responses were “web pages, for example, PAEHR’s website” (MHC 350/1103, 11.10%, and non-MHC 967/2898, 10.50%; Figure 2).
Figure 2.
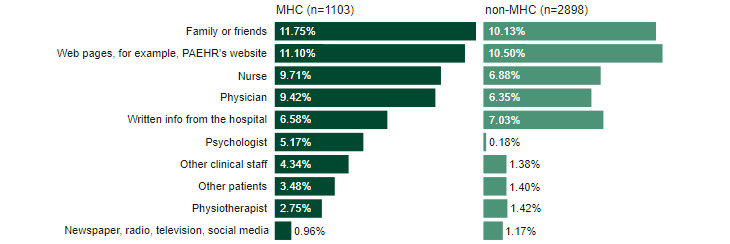
Of those who responded “yes” to the question, “Were you encouraged by someone or reminded to read your EHR?” this figure presents who or what encouraged or reminded them. Due to being a multiple-choice item, the total will not add up to 100%. MHC: mental health care; non-MHC: nonmental health care; PAEHR: patient-accessible electronic health record.
The differences between the groups on how access to EHR improves trust and communication with HCPs were not statistically significant (trust: N=12,334; χ24=6.8; P<.15; and communication: N=12,334; χ24=5.5; P<.24). Respondents in both the MHC group and non-MHC group agreed that trust and communication increased as a result of access to their EHR (Figure 3).
Figure 3.
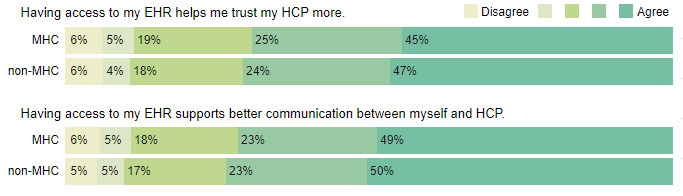
Response distribution to the questions of how access to the electronic health record (EHR) affects trust and communication with health care professionals (HCPs). MHC: mental health care; non-MHC: nonmental health care.
Errors, Omissions, and Offenses
Errors, omissions, and offensive content were perceived to be more common for the MHC group than the non-MHC group (Table 4). Half of the respondents in the MHC group (1586/3131, 50.65%) reported finding an error in their EHR, and about a third (1089/3131, 34.78%) reported an omission. There was a statistically significant association between the respondent group and identified errors and omissions (errors: N=12,334; χ22=303.7; P<.001, and omissions: N=12,334; χ22=192.5; P<.001), indicating that the MHC respondents perceived more errors and omissions than the non-MHC respondents.
Table 4.
Rates of errors, omissions, and offenses.
| Survey item | MHCa (n=3131), n (%) | non-MHCb (n=9203), n (%) | P valuec | ||||||||
| Errors |
|
||||||||||
|
|
Have you found anything that was wrong in your EHRd (not misspellings/typographical)? | <.001 | |||||||||
|
|
|
Yes | 1586 (50.65) | 3311 (35.98) |
|
||||||
|
|
|
No | 904 (28.87) | 4253 (46.21) |
|
||||||
|
|
|
Do not know or do not remember | 641 (20.47) | 1639 (17.81) |
|
||||||
|
|
If yes, how important was the worst mistake for youe? | <.001 | |||||||||
|
|
|
Not at all important | 148 (9.33) | 508 (15.34) |
|
||||||
|
|
|
Somewhat important | 586 (36.95) | 1332 (40.23) |
|
||||||
|
|
|
Very important | 795 (50.13) | 1366 (41.26) |
|
||||||
|
|
|
Not sure | 57 (3.59) | 105 (3.17) |
|
||||||
| Omissions |
|
||||||||||
|
|
Have you found anything you thought was missing from your EHR? | <.001 | |||||||||
|
|
|
Yes | 1089 (34.78) | 2427 (26.37) |
|
||||||
|
|
|
No | 1059 (33.82) | 4418 (48.01) |
|
||||||
|
|
|
Do not know or do not remember | 983 (31.40) | 2358 (25.62) |
|
||||||
|
|
If yes, how serious was the most important missing information for youf? | .47 | |||||||||
|
|
|
Not at all serious | 20 (1.84) | 46 (1.90) |
|
||||||
|
|
|
Somewhat serious | 372 (34.16) | 895 (36.88) |
|
||||||
|
|
|
Very serious | 622 (57.12) | 1329 (54.76) |
|
||||||
|
|
|
Not sure | 75 (6.89) | 157 (6.47) |
|
||||||
|
|
Did you do any of the following when you found a mistake or missing information in your EHRg? | .08 | |||||||||
|
|
|
Informed health care professional at the next visit | 499 (26.02) | 1010 (23.17) |
|
||||||
|
|
|
Contacted care unit by phone | 357 (18.61) | 837 (19.20) |
|
||||||
|
|
|
Did nothing | 792 (41.29) | 1838 (42.17) |
|
||||||
|
|
|
Something else | 270 (14.08) | 674 (15.46) |
|
||||||
| Offense | |||||||||||
|
|
Have you ever felt offended by something you read? |
|
|
<.001 | |||||||
|
|
|
Yes | 1183 (37.78) | 1616 (17.56) |
|
||||||
|
|
|
No | 1948 (62.22) | 7587 (82.44) |
|
||||||
aMHC: mental health care.
bnon-MHC: nonmental health care.
cP value is derived from the chi-square test comparing the MHC and non-MHC subsamples on a given variable.
dEHR: electronic health record.
eDue to the question being responded to by the “yes” of errors, the total of numbers is 1586 (MHC) and 3311 (non-MHC).
fDue to the question being responded to by the “yes” of omissions, the total of numbers is 1089 (MHC) and 2427 (non-MHC).
gDue to the question being responded to by the “yes” of errors or omissions, the total of numbers is 1918 (MHC) and 4359 (non-MHC).
Half of the MHC group (795/1586, 50.13%) rated the most serious error they found as “very important,” and nearly 6 in 10 rated the most serious omission as “very serious” (622/1089, 57.12%). The association between the respondent group and the error rating was significant (N=4897; χ23=51.5; P<.001). Participants in the MHC group rated the errors as more important than those in the non-MHC group. No significant differences were found between the groups regarding the rating of the omissions (N=3516; χ23=2.5; P=.47). In both groups, a large proportion of the respondents reported doing nothing when they found an error or omission (MHC 792/1918, 41.29%, and non-MHC 1838/4359, 42.17%).
The majority of respondents indicated that they had not been offended by something they read. However, the proportion of those who were offended was larger among the MHC respondents: more than a third of the MHC group (1183/3131, 37.78%) reported feeling offended by something they read in their EHR. There was a significant association between the respondent group and offense (N=12,334; χ21=544.7; P<.001).
There were small but statistically significant differences between the groups with respect to the ease with which they noticed mistakes or errors in the EHR (MHC 751/3131, 24%, and non-MHC 2117/9203, 23%; Figure 4; N=12,334; χ24=14.4; P<.001).
Figure 4.

Response distribution to the question of how easy or difficult it is to notice mistakes or errors in the electronic health record (EHR). MHC: mental health care; non-MHC: nonmental health care.
Comparison of Error, Omission, and Offense Rates Between Stratified MHC and Non-MHC Subsamples
To further investigate the rate of errors, omissions, and offenses, we used stratified random sampling with proportional allocation, which resulted in gender- and age-matched MHC and non-MHC subsamples (Table 5). Despite matching the distribution of age and gender, the group differences in rates persisted. Errors were significantly more common in the MHC subsample (errors: N=5830; χ22=131.4; P<.001; as well as omissions: N=5830; χ22=69.2; P<.001; and offenses: N=5830; χ21=177.7; P<.001).
Table 5.
Rates of errors, omissions, and offenses in the stratified subsamples.
| Survey item | MHCa (n=2915), n (%) | Matched non-MHCb (n=2915), n (%) | P valuec | |||||
| Participant characteristics | ||||||||
|
|
Gender | >.99 | ||||||
|
|
|
Woman | 2254 (77.32) | 2254 (77.32) |
|
|||
|
|
|
Man | 661 (22.68) | 661 (22.68) |
|
|||
|
|
Age (years) | >.99 | ||||||
|
|
|
15-19 | 72 (2.47) | 72 (2.47) |
|
|||
|
|
|
20-24 | 147 (5.04) | 147 (5.04) |
|
|||
|
|
|
25-34 | 759 (26.04) | 759 (26.04) |
|
|||
|
|
|
35-44 | 647 (22.20) | 647 (22.20) |
|
|||
|
|
|
45-54 | 634 (21.75) | 634 (21.75) |
|
|||
|
|
|
55-64 | 465 (15.95) | 465 (15.95) |
|
|||
|
|
|
65-74 | 141 (4.84) | 141 (4.84) |
|
|||
|
|
|
75-84 | 48 (1.65) | 48 (1.65) |
|
|||
|
|
|
>85 | 2 (0.07) | 2 (0.07) |
|
|||
| Errors, omissions, and offenses | ||||||||
|
|
Error rate | <.001 | ||||||
|
|
|
Yes | 1471 (50.46) | 1067 (36.60) |
|
|||
|
|
|
No | 858 (29.43) | 1230 (42.20) |
|
|||
|
|
|
Do not know or do not remember | 586 (20.10) | 618 (21.20) |
|
|||
|
|
Omission rate | <.001 | ||||||
|
|
|
Yes | 1017 (34.89) | 829 (28.44) |
|
|||
|
|
|
No | 1000 (34.31) | 1309 (44.91) |
|
|||
|
|
|
Do not know or do not remember | 898 (30.81) | 777 (26.66) |
|
|||
|
|
Offense rate | <.001 | ||||||
|
|
|
Yes | 1084 (37.19) | 621 (21.30) |
|
|||
|
|
|
No | 1831 (62.81) | 2294 (78.70) |
|
|||
aMHC: mental health care.
bnon-MHC: nonmental health care.
cP value is derived from the chi-square test comparing the MHC and non-MHC subsamples on a given variable.
Discussion
Overview
This study presents the first large study of the perceptions of patients with MHC with errors, omissions, and offenses after accessing their online records in Sweden. The study forms part of a larger data set from the NORDeHEALTH 2022 Patient Survey [34]. A central finding was that 1 in 2 patients with MHC have found errors in their health records (50.65%), and about 1 in 3 have identified missing information (34.78%), with about half of the respondents rating both the worst errors and omissions as “very important.” This is a marked increase from the other patients, of whom one-third identified an error (35.98%) or omission (26.37%), a rate that is already higher than one may consider acceptable. Interestingly, almost half of both patients with MHC (41.29%) and non-MHC (42.17%) chose not to do anything to correct the error or omission. When it comes to rates of offensive content in the EHR, about 1 in 3 patients with MHC have felt offended by their notes (41.29%), compared with 1 in 6 patients with non-MHC (17.56%). Noting that the MHC group included more women as well as younger patient users than the non-MHC group, we created stratified subsamples to investigate whether the group differences in error, omission, and offense rates persisted. We found that the non-MHC subsample reported fewer instances of errors, omissions, and offenses, even when the samples were matched by the distribution of age and gender. Notably, when it comes to the positive impact of EHRs on trust in HCPs and communication with HCPs, both patients with MHC and non-MHC had similarly high levels of agreement with both statements. Both patient groups also had more positive experiences than negative ones.
There could be several reasons why respondents in the MHC group reported more errors and considered them more important than in the non-MHC group. One possibility is that individuals in MHC may have more complex health conditions [38] that require more careful monitoring and documentation, making errors more salient. Additionally, mental health conditions may be more subjective and difficult to quantify, leading to more disagreements or discrepancies in how they are recorded in the EHR. Another possibility is that individuals in MHC may be more attuned to their health and more likely to notice and report errors, while individuals in other health care may be more accustomed to their good health and less likely to scrutinize their EHR for errors. While this difference may be interpreted as a reason for not having open mental health notes or keeping shadow records, neither closed notes nor shadow records are a solution. In a Delphi study [16], there was a consensus among experts that open mental health notes would be helpful for patients to find errors in their notes and be able to correct them. Furthermore, the experts agreed upon the adverse effects of closed notes, such as greater patient stigmatization and harm. Other studies have noted the desire of patients with MHC to access and read their mental health notes to ensure the accuracy of the content and that no errors occur [15].
A possible reason for experiencing more errors in the MHC group could be the same as for the more frequently experienced omissions: the complex medical backgrounds, comorbidities, and medications [38], which may render it more challenging for HCPs to document everything accurately. Additionally, patients with mental health issues may be more likely to have communication difficulties [39] and may be subject to different cultural perceptions between patients and therapists [40], which could result in important information not being recorded in their health records. Given that the overwhelming majority of respondents deemed the missing information important, it suggests that patients recognize the importance of accurate and complete health records. The MHC group experienced something in the notes as offensive at a much higher rate than respondents in the non-MHC group. It is not clear what led to higher offense rates in the MHC group. The posed question did not specify whether it was concerning MHC.
It is unclear why most chose to do nothing when they found an error or omission that they deemed very important. One reason may be that patients fear being perceived as complaining or bothersome if they ask the HCP to correct their health record. These findings do not appear to be in line with research reporting on the fear of HCPs regarding increased workload as a consequence of patients asking for the notes to be explained or corrected [15]. Blease et al [41] discuss the phenomenon of epistemic injustice, as it could arise when an individual has a lower level of credibility due to belonging to a stereotypical group. In this case, patients within MHC already have forms of discretion or negative stereotyping, which further impedes their agency in raising queries or asking for corrections to their records. Correcting the health record is burdensome in more practical terms, as no digital solution exists in the Swedish PAEHR.
In previous research, mental HCPs have noted whether sharing notes should be on a case-by-case basis depending on the treatment or diagnosis and whether all details and information should be included. For example, when treating traumatic experiences, HCPs have recommended excluding detailed information from the notes due to privacy and safety reasons for the patient, as well as the severity of the illness and psychiatric diagnosis [15]. The fear among HCPs of misunderstandings, misinterpretations, and patients finding errors and requesting changes has led to them being less candid, less detailed, and changing the tone of their notes [15]. In Norway, HCPs in psychiatric care have been reported to keep a “shadow record” outside the official EHR system due to patient access [27]. A theory of the MHC respondents’ more significant experiences of omissions could be a case of HCPs adjusting the notes, such as intentionally leaving essential details and information out and altering the tone of the notes, concerned with their beliefs about patients’ increased sensitivity. What has been argued for in previous research [42] is the need for more sustained efforts in terms of continuing medical education for HCPs on how to write notes that patients have access to and can read—especially needed within MHC to strengthen HCPs’ knowledge on how to document notes that patients will read to minimize the risks of patients’ negative experiences of open MHC notes.
An observation of the participant characteristics is that the respondents in the MHC group are generally younger than those in the non-MHC group. MHC respondents peak at ages 25 and 54 years, and the same peak can be found at ages 55 and 74 years in the non-MHC group; however, the most common age range is between 25 and 34 years in the MHC group and between 65 and 74 years in the non-MHC group. In both groups, most respondents have stated they have “fair” health; however, respondents in the MHC group have reported either “bad” or “very bad” health status in a higher proportion than in the non-MHC group. This could suggest that mental health issues are more prominent in young people, which is supported by the fact that respondents in the MHC group have reported either “bad” or “very bad” health status in a higher proportion than in the non-MHC group. In the Västra Götaland and Dalarna regions, there were more MHC respondents than non-MHC respondents. This discrepancy may be due to the differences in what health information patients can access in the PAEHR depending on which region they seek care in [1].
Moreover, a higher proportion of the MHC respondents have had a “very negative” experience with the EHR compared with non-MHC respondents. The sensitive nature of mental health issues could explain this. It is possible that reading about mental health problems could trigger negative emotions in patients, leading to a more negative experience with the EHR. Generally, respondents in the MHC group read their EHR more frequently than in the non-MHC group. One possible explanation is that patients with MHC may need to review their medical records more often to keep track of their treatment progress or to better understand their mental health condition. Additionally, patients with MHC may be more engaged in their health care and more motivated to take an active role in their treatment, which could lead to a more frequent review of their EHR. Finally, it is possible that the higher frequency of EHR review in the MHC group could be due to the younger age of the respondents, who may be more comfortable and familiar with digital technology and therefore more likely to access their EHR. With these inherent group differences, it is perhaps unsurprising that there is a divergence when comparing reported error, omission, and offense rates.
Limitations and Future Directions
This study had several limitations. The survey relied on self-report, which limits the accuracy of the findings due to response biases. Further, patients with MHC experience were identified based on whether they had been in contact with a HCP with regard to a mental health condition in the last 2 years. This may have been interpreted in various ways by the respondents. Notably, while the study was advertised inside the patient record, the survey and the record were not connected. It was not possible to verify a respondent’s health care history, unlike in a previous US study where patients’ mental health diagnoses were extracted from the patient record [13]. Nonetheless, our follow-up questions on the mental health care experience allowed us to better categorize the patients, for example, on levels of care and length of treatment.
Another limitation stems from the formulation of the gender question. While patients with MHC selected the answer option “other,” it is not clear what their preferred gender label is. Previous research has found that transgender patients have noted experiences of harm when reading their health records [43]. Here, it is possible that part of the increased rate of errors or offensive content is related to gender. In the future, studies should adopt a more inclusive gender question to ensure that gender-sensitive analyses are possible.
In the NORDeHEALTH project, future analyses will focus on the respondents who responded that the level of MHC has been within emergency care and those who reported to have been hospitalized, as they might have experienced serious mental illness.
Conclusions
In this study, we seek to understand if and how the experiences of patients with and without MHC differ when using PAEHRs. This study reports findings from the largest investigation of the experiences of patients with MHC with accessing online records in Sweden. The analysis revealed that 1 in 2 patients with MHC identified errors in their records, with 1 in 3 identifying omissions or feeling offended by the content of the notes. Moreover, patients in MHC reported these experiences at a much higher rate than other patients. Adding to these concerning findings, most patients reported that they did not act when they found errors or omissions in their records, despite rating them as “very important.”
Additionally, the study raises questions about why respondents in the MHC group detected more missing information than those in the non-MHC group and why they experienced higher offense rates. One reason for more omissions could be that HCPs might adjust the notes to intentionally leave essential details and information out, concerned with their beliefs about patients’ increased sensitivity, highlighting the need for continuous medical education for HCPs on documenting notes that patients will read. Overall, this study highlights identified challenges with the documentation quality in the records. There is a need for better training in how HCPs write notes and the language they use, and for HCPs to recognize that patients can and should act as collaborators with them in improving the records’ accuracy [44].
Acknowledgments
This work was supported by NordForsk through the funding to Nordic eHealth for Patients: Benchmarking and Developing for the Future, NORDeHEALTH (Project #100477), and the Swedish Research Council for Health, Working Life, and Welfare (FORTE) through the funding to Beyond Implementation of eHealth (Project #2020-01229). CB was supported by a Keane Scholar Award. The study funders played no role in the study design, data interpretation, writing of the results, or decision to submit the manuscript for publication.
The authors thank Eli Kristiansen, Paolo Zanaboni, Josefin Hagström, Rose-Mharie Åhlfeldt, Gunnar Klein, Catherine DesRoches, Barbara Haage, Iiris Hörhammer, and Peeter Ross for their contribution in the design and distribution of the survey.
Abbreviations
- EHR
electronic health record
- HCP
health care professional
- MHC
mental health care
- non-MHC
nonmental health care
- ORA
online record access
- PAEHR
patient-accessible electronic health record
Survey overview of the items analysed in this study.
Checklist for Reporting Results of Internet E-Surveys (CHERRIES).
Strata of the stratified random sampling.
Data Availability
The data may be made available upon reasonable request and after consent from the data holder (Maria Hägglund, maria.hagglund@kbh.uu.se).
Footnotes
Authors' Contributions: AB prepared the initial draft of the manuscript, with input from AK and HR. AB and AK were responsible for the statistical analysis. Data was preprocessed by AK and AB and combined into a master data file by AK. AB prepared the tables and initial figures, which were then validated by AK. A draft of the survey was designed by AJF, and MAJ. The questions were then further developed by AB, MH, CB, ÅC, AJF, IH, MAJ, BK, SK, HR, and IS. The survey was translated to Swedish and distributed by MH, AB, and IS. All authors reviewed the manuscript and approved the final draft for submission.
Conflicts of Interest: None declared.
References
- 1.Bärkås A, Scandurra I, Rexhepi H, Blease C, Cajander Å, Hägglund M. Patients' access to their psychiatric notes: current policies and practices in Sweden. Int J Environ Res Public Health. 2021;18(17):9140. doi: 10.3390/ijerph18179140. https://www.mdpi.com/resolver?pii=ijerph18179140 .ijerph18179140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.COM (2022) 197: proposal for a Regulation of the European Parliament and of the Council on the European Health Data Space (2022/0140/COD) Eur-Lex. [2022-11-15]. https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:52022PC0197 .
- 3.O'Neill S, Blease C, Delbanco T. Open notes become law: a challenge for mental health practice. Psychiatr Serv. 2021;72(7):750–751. doi: 10.1176/appi.ps.202000782. https://ps.psychiatryonline.org/doi/10.1176/appi.ps.202000782 . [DOI] [PubMed] [Google Scholar]
- 4.O'Neill S, Chimowitz H, Leveille S, Walker J. Embracing the new age of transparency: mental health patients reading their psychotherapy notes online. J Ment Health. 2019;28(5):527–535. doi: 10.1080/09638237.2019.1644490. [DOI] [PubMed] [Google Scholar]
- 5.Cromer R, Denneson LM, Pisciotta M, Williams H, Woods S, Dobscha SK. Trust in mental health clinicians among patients who access clinical notes online. Psychiatr Serv. 2017;68(5):520–523. doi: 10.1176/appi.ps.201600168. https://europepmc.org/abstract/MED/28142383 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pisciotta M, Denneson LM, Williams HB, Woods S, Tuepker A, Dobscha SK. Providing mental health care in the context of online mental health notes: advice from patients and mental health clinicians. J Ment Health. 2019;28(1):64–70. doi: 10.1080/09638237.2018.1521924. [DOI] [PubMed] [Google Scholar]
- 7.Blease CR, Walker J, Torous J, O'Neill S. Sharing clinical notes in psychotherapy: a new tool to strengthen patient autonomy. Front Psychiatry. 2020;11:527872. doi: 10.3389/fpsyt.2020.527872. https://europepmc.org/abstract/MED/33192647 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Moll J, Rexhepi H, Cajander Å, Grünloh C, Huvila I, Hägglund M, Myreteg G, Scandurra I, Åhlfeldt RM. Patients' experiences of accessing their electronic health records: national patient survey in Sweden. J Med Internet Res. 2018;20(11):e278. doi: 10.2196/jmir.9492. https://www.jmir.org/2018/11/e278/ v20i11e278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wiljer D, Urowitz S, Apatu E, DeLenardo C, Eysenbach G, Harth T, Pai H, Leonard KJ. Patient accessible electronic health records: exploring recommendations for successful implementation strategies. J Med Internet Res. 2008;10(4):e34. doi: 10.2196/jmir.1061. https://www.jmir.org/2008/4/e34/ v10i4e34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Peck P, Torous J, Shanahan M, Fossa A, Greenberg W. Patient access to electronic psychiatric records: a pilot study. Health Policy Technol. 2017;6(3):309–315. doi: 10.1016/j.hlpt.2017.06.003. [DOI] [Google Scholar]
- 11.Klein JW, Peacock S, Tsui JI, O'Neill SF, DesRoches CM, Elmore JG. Perceptions of primary care notes by patients with mental health diagnoses. Ann Fam Med. 2018;16(4):343–345. doi: 10.1370/afm.2287. http://www.annfammed.org/cgi/pmidlookup?view=long&pmid=29987083 .16/4/343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Denneson LM, Chen JI, Pisciotta M, Tuepker A, Dobscha SK. Patients' positive and negative responses to reading mental health clinical notes online. Psychiatr Serv. 2018;69(5):593–596. doi: 10.1176/appi.ps.201700353. https://europepmc.org/abstract/MED/29493408 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Blease C, Dong Z, Torous J, Walker J, Hägglund M, DesRoches CM. Association of patients reading clinical notes with perception of medication adherence among persons with serious mental illness. JAMA Netw Open. 2021;4(3):e212823. doi: 10.1001/jamanetworkopen.2021.2823. https://europepmc.org/abstract/MED/33760088 .2777857 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Etingen B, Hogan TP, Martinez RN, Shimada S, Stroupe K, Nazi K, Connolly SL, Lipschitz J, Weaver FM, Smith B. How do patients with mental health diagnoses use online patient portals? An observational analysis from the Veterans Health Administration. Adm Policy Ment Health. 2019;46(5):596–608. doi: 10.1007/s10488-019-00938-x.10.1007/s10488-019-00938-x [DOI] [PubMed] [Google Scholar]
- 15.Schwarz J, Bärkås A, Blease C, Collins L, Hägglund M, Markham S, Hochwarter S. Sharing clinical notes and electronic health records with people affected by mental health conditions: scoping review. JMIR Ment Health. 2021;8(12):e34170. doi: 10.2196/34170. https://mental.jmir.org/2021/12/e34170/ v8i12e34170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Blease C, Kharko A, Hägglund M, O'Neill S, Wachenheim D, Salmi L, Harcourt K, Locher C, DesRoches CM, Torous J. The benefits and harms of open notes in mental health: a Delphi survey of international experts. PLoS One. 2021;16(10):e0258056. doi: 10.1371/journal.pone.0258056. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0258056 .PONE-D-21-12428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Blease C, Torous J, Kharko A, DesRoches CM, Harcourt K, O'Neill S, Salmi L, Wachenheim D, Hägglund M. Preparing patients and clinicians for open notes in mental health: qualitative inquiry of international experts. JMIR Ment Health. 2021;8(4):e27397. doi: 10.2196/27397. https://mental.jmir.org/2021/4/e27397/ v8i4e27397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Petersson L, Erlingsdóttir G. Open notes in Swedish psychiatric care (part 1): survey among psychiatric care professionals. JMIR Ment Health. 2018;5(1):e11. doi: 10.2196/mental.9140. https://mental.jmir.org/2018/1/e11/ v5i1e11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dobscha SK, Denneson LM, Jacobson LE, Williams HB, Cromer R, Woods S. VA mental health clinician experiences and attitudes toward OpenNotes. Gen Hosp Psychiatry. 2016;38:89–93. doi: 10.1016/j.genhosppsych.2015.08.001.S0163-8343(15)00191-7 [DOI] [PubMed] [Google Scholar]
- 20.Petersson L, Erlingsdóttir G. Open notes in Swedish psychiatric care (part 2): survey among psychiatric care professionals. JMIR Ment Health. 2018;5(2):e10521. doi: 10.2196/10521. https://mental.jmir.org/2018/2/e10521/ v5i2e10521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Strudwick G, Clark C, Sanches M, Strauss J. Predictors of mental health professionals' perceptions of patient portals. AMIA Annu Symp Proc. 2018;2018:989–997. https://europepmc.org/abstract/MED/30815142 . [PMC free article] [PubMed] [Google Scholar]
- 22.Chimowitz H, O'Neill S, Leveille S, Welch K, Walker J. Sharing psychotherapy notes with patients: therapists' attitudes and experiences. Soc Work. 2020;65(2):159–168. doi: 10.1093/sw/swaa010.5814576 [DOI] [PubMed] [Google Scholar]
- 23.Erlingsdóttir G, Petersson L, Jonnergård K. A theoretical twist on the transparency of open notes: qualitative analysis of health care professionals' free-text answers. J Med Internet Res. 2019;21(9):e14347. doi: 10.2196/14347. https://www.jmir.org/2019/9/e14347/ v21i9e14347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fagerlund AJ, Kristiansen E, Johansen MA, Haumann K, Zanaboni P. Elektronisk innsyn i journal for pasienter i psykisk helsevern: Helsepersonells erfaringer. Tidsskrift Norsk Psykologforening. 2021;58(5):380–389. https://psykologtidsskriftet.no/vitenskapelig-artikkel/2021/05/elektronisk-innsyn-i-journal-pasienter-i-psykisk-helsevern . [Google Scholar]
- 25.Johansen MA, Kummervold PE, Sørensen T, Zanaboni P. Health professionals' experience with patients accessing their electronic health records: results from an online survey. Stud Health Technol Inform. 2019;264:504–508. doi: 10.3233/SHTI190273.SHTI190273 [DOI] [PubMed] [Google Scholar]
- 26.Denneson LM, Cromer R, Williams HB, Pisciotta M, Dobscha SK. A qualitative analysis of how online access to mental health notes is changing clinician perceptions of power and the therapeutic relationship. J Med Internet Res. 2017;19(6):e208. doi: 10.2196/jmir.6915. https://www.jmir.org/2017/6/e208/ v19i6e208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kristiansen E, Johansen M, Zanaboni P. Healthcare personnels’ experience with patients’ online access to electronic health records: differences between professions, regions, and somatic and psychiatric healthcare. Proceedings of the 17th Scandinavian Conference on Health Informatics; November 12-13, 2019; Oslo Norway. 2019. pp. 93–98. https://ep.liu.se/ecp/161/016/ecp19161016.pdf . [Google Scholar]
- 28.Åkerstedt US, Cajander Å, Moll J, Ålander T. On threats and violence for staff and patient accessible electronic health records. Cogent Psychol. 2018;5(1):1–11. doi: 10.1080/23311908.2018.1518967. https://www.tandfonline.com/doi/full/10.1080/23311908.2018.1518967 . [DOI] [Google Scholar]
- 29.van Rijt AM, Hulter P, Weggelaar-Jansen AM, Ahaus K, Pluut B. Mental health care professionals' appraisal of patients' use of web-based access to their electronic health record: qualitative study. J Med Internet Res. 2021;23(8):e28045. doi: 10.2196/28045. https://www.jmir.org/2021/8/e28045/ v23i8e28045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Zanaboni P, Kristiansen E, Lintvedt O, Wynn R, Johansen MA, Sørensen T, Fagerlund AJ. Impact on patient-provider relationship and documentation practices when mental health patients access their electronic health records online: a qualitative study among health professionals in an outpatient setting. BMC Psychiatry. 2022;22(1):508. doi: 10.1186/s12888-022-04123-7. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-022-04123-7 .10.1186/s12888-022-04123-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Blease CR, O'Neill S, Walker J, Hägglund M, Torous J. Sharing notes with mental health patients: balancing risks with respect. Lancet Psychiatry. 2020;7(11):924–925. doi: 10.1016/S2215-0366(20)30032-8.S2215-0366(20)30032-8 [DOI] [PubMed] [Google Scholar]
- 32.Blease CR, O'Neill SF, Torous J, DesRoches CM, Hagglund M. Patient access to mental health notes: motivating evidence-informed ethical guidelines. J Nerv Ment Dis. 2021;209(4):265–269. doi: 10.1097/NMD.0000000000001303.00005053-202104000-00009 [DOI] [PubMed] [Google Scholar]
- 33.Hägglund M, Kharko A, Bärkås A, Blease C, Cajander Å, DesRoches C, Fagerlund AJ, Hagström J, Huvila I, Hörhammer I, Kane B, Klein GO, Kristiansen E, Moll J, Muli I, Rexhepi H, Riggare S, Ross P, Scandurra I, Simola S, Soone H, Wang B, Zolbin MG, Åhlfeldt RM, Kujala S, Johansen MA. NORDeHEALTH—learning from the Nordic experiences of patient online record access. JMIR Preprints. doi: 10.2196/preprints.49084. Preprint posted online on May 17, 2023. https://preprints.jmir.org/preprint/49084 . [DOI] [Google Scholar]
- 34.Hägglund M, Kharko A, Hagström J, Bärkås A, Blease C, Cajander Å, DesRoches C, Fagerlund AJ, Haage B, Huvila I, Hörhammer I, Kane B, Klein GO, Kristiansen E, Luks K, Moll J, Muli I, Raphaug EH, Rexhepi H, Riggare S, Ross P, Scandurra I, Simola S, Soone H, Wang B, Zolbin MG, Åhlfeldt RM, Kujala S, Johansen MA. The NORDeHEALTH 2022 patient survey: a cross-sectional survey of national patient portal users in Norway, Sweden, Finland, and Estonia. JMIR Preprints. doi: 10.2196/preprints.47573. Preprint posted online on September 29, 2023. https://preprints.jmir.org/preprint/47573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kujala S, Hörhammer I, Väyrynen A, Holmroos M, Nättiaho-Rönnholm M, Hägglund M, Johansen MA. Patients' experiences of web-based access to electronic health records in Finland: cross-sectional survey. J Med Internet Res. 2022;24(6):e37438. doi: 10.2196/37438. https://www.jmir.org/2022/6/e37438/ v24i6e37438 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zanaboni P, Kummervold PE, Sørensen T, Johansen MA. Patient use and experience with online access to electronic health records in Norway: results from an online survey. J Med Internet Res. 2020;22(2):e16144. doi: 10.2196/16144. https://www.jmir.org/2020/2/e16144/ v22i2e16144 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Iliyasu R, Etikan I. Comparison of quota sampling and stratified random sampling. Biom Biostat Int J. 2021;10(1):24–27. doi: 10.15406/bbij.2021.10.00326. [DOI] [Google Scholar]
- 38.Bahorik AL, Satre DD, Kline-Simon AH, Weisner CM, Campbell CI. Serious mental illness and medical comorbidities: findings from an integrated health care system. J Psychosom Res. 2017;100:35–45. doi: 10.1016/j.jpsychores.2017.07.004. https://europepmc.org/abstract/MED/28789791 .S0022-3999(17)30105-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cohen NJ, Farnia F, Im-Bolter N. Higher order language competence and adolescent mental health. J Child Psychol Psychiatry. 2013;54(7):733–744. doi: 10.1111/jcpp.12060. [DOI] [PubMed] [Google Scholar]
- 40.Fagerlund AJ, Kristiansen E, Simonsen RA. Experiences from using patient accessible electronic health records—a qualitative study within Sámi mental health patients in Norway. Int J Circumpolar Health. 2022;81(1):2025682. doi: 10.1080/22423982.2022.2025682. https://europepmc.org/abstract/MED/35037572 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Blease C, Salmi L, Rexhepi H, Hägglund M, DesRoches CM. Patients, clinicians and open notes: information blocking as a case of epistemic injustice. J Med Ethics. 2021;48(10):785–793. doi: 10.1136/medethics-2021-107275. http://jme.bmj.com/lookup/pmidlookup?view=long&pmid=33990427 .medethics-2021-107275 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Blease C, McMillan B, Salmi L, Davidge G, Delbanco T. Adapting to transparent medical records: international experience with "open notes". BMJ. 2022;379:e069861. doi: 10.1136/bmj-2021-069861. [DOI] [PubMed] [Google Scholar]
- 43.Alpert AB, Mehringer JE, Orta SJ, Redwood E, Hernandez T, Rivers L, Manzano C, Ruddick R, Adams S, Cerulli C, Operario D, Griggs JJ. Experiences of transgender people reviewing their electronic health records, a qualitative study. J Gen Intern Med. 2023;38(4):970–977. doi: 10.1007/s11606-022-07671-6. https://europepmc.org/abstract/MED/35641720 .10.1007/s11606-022-07671-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Blease CR, Bell SK. Patients as diagnostic collaborators: sharing visit notes to promote accuracy and safety. Diagnosis (Berl) 2019;6(3):213–221. doi: 10.1515/dx-2018-0106./j/dx.ahead-of-print/dx-2018-0106/dx-2018-0106.xml [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Survey overview of the items analysed in this study.
Checklist for Reporting Results of Internet E-Surveys (CHERRIES).
Strata of the stratified random sampling.
Data Availability Statement
The data may be made available upon reasonable request and after consent from the data holder (Maria Hägglund, maria.hagglund@kbh.uu.se).