

Abstract
Introduction
Thyroid specialists influence how hypothyroid patients are treated, including patients managed in primary care. Given that physician characteristics influence patient care, this study aimed to explore thyroid specialist profiles and associations with geo-economic factors.
Methods
Thyroid specialists from 28 countries were invited to respond to a questionnaire, Treatment of Hypothyroidism in Europe by Specialists: an International Survey (THESIS). Geographic regions were defined according to the United Nations Statistics Division. The national economic status was estimated using World Bank data on the gross national income per capita (GNI per capita).
Results
5,695 valid responses were received (response rate 33·0%). The mean age was 49 years, and 65·0% were female. The proportion of female respondents was lowest in Northern (45·6%) and highest in Eastern Europe (77·2%) (p <0·001). Respondent work volume, university affiliation and private practice differed significantly between countries (p<0·001). Age and GNI per capita were correlated inversely with the proportion of female respondents (p<0·01). GNI per capita was inversely related to the proportion of respondents working exclusively in private practice (p<0·011) and the proportion of respondents who treated >100 patients annually (p<0·01).
Discussion
THESIS has demonstrated differences in characteristics of thyroid specialists at national and regional levels, strongly associated with GNI per capita. Hypothyroid patients in middle-income countries are more likely to encounter female thyroid specialists working in private practice, with a high workload, compared to high-income countries. Whether these differences influence the quality of care and patient satisfaction is unknown, but merits further study.
Keywords: hypothyroidism, questionnaire, endocrinologists, healthcare delivery, Europe
1. Introduction
Hypothyroidism is a common condition, with a prevalence of overt and subclinical disease of 0·2 and 5·3%, respectively, and its prevalence is rising (1). Unfortunately, in real life, almost half of the patients do not achieve therapeutic targets (2). A serum TSH outside the normal range while on thyroxine (L-T4) replacement is associated with increased morbidity and mortality (3). Therefore, a significant burden of disease is associated with hypothyroidism, which can be addressed with very cheap interventions (adjustment of L-T4 dose and additional monitoring). However, implementation is vitally dependent on appropriate medical supervision. Failure to achieve a normal serum TSH is a common reason for hypothyroid patients on L-T4 being referred to thyroid specialists (4, 5).
The available information on the characteristics of specialists who treat patients with hypothyroidism in Europe is scanty. A survey of members of the European Society of Endocrinology (ESE) revealed that thyroid disorders comprised 28% of the endocrinologist workload (6). Details regarding the characteristics of specialists treating thyroid diseases were unavailable, and have not emerged since. Furthermore, it is notable that in addition to endocrinologists, clinicians from several other specialities not represented in the ESE survey treat patients with hypothyroidism in Europe. Regional differences in managing some thyroid conditions have been reported (7). However, hypothyroidism has not been studied in this context except for one previous survey, which found that American physicians were more likely to prescribe L-T3 and desiccated thyroid extract (DTE) than their European counterparts (8). The role of thyroid specialists in managing this wave of demands on healthcare systems is likely to be important. Also, primary care physicians tend to follow the lead of specialists (9). Europe comprises countries with differences in healthcare provision, patient demographics, epidemiology of thyroid disease, and gross national income per capita (GNI per capita); therefore, further exploration of these variables can help understand, plan, and improve healthcare delivery (10).
THESIS (“Treatment of Hypothyroidism in Europe by Specialists: An International Survey”) was a survey of European specialists treating patients with hypothyroidism. One of the study aims was to document the demographic and work-related characteristics of specialists who treat hypothyroid patients in European countries. Twenty out of twenty eight countries surveyed have already reported their national data (11–30). Differences in healthcare delivery may impact the patient experience, and therefore comparisons between regions and countries may provide valuable insights. Here, we present the aggregate data from THESIS and explore demographic, work-related and geo-economic characteristics of specialists treating hypothyroidism in Europe.
2. Materials and methods
The THESIS survey was conducted according to the checklist for reporting results of Internet-based e-surveys (CHERRIES) (31). The target population consisted of members of national endocrine and/or thyroid related professional organisations who treated patients with hypothyroidism and comprised primarily endocrinologists, nuclear medicine physicians, and internists. This was a convenience sample (participants were selected through “convenient” data sources for researchers). Project oversight was provided by a Steering Committee (LH, EVN, EP, PP, RA and RN).
2.1. Questionnaire
The THESIS questionnaire was developed in English. It was initially tested in a pilot study of Italian endocrinologists after translation into Italian, following which it underwent revisions to reach its final form (22). The questionnaire included eight questions about the responding physician and twenty-three questions concerning the use of thyroid hormones in different clinical settings (see Appendix). Completion of the survey required less than 15 minutes. National leads had a choice of using the original English version or translations. Translations were performed by a designated bilingual clinician and verified by another bilingual senior clinician. Twelve countries adopted the original English version (Belgium, Denmark, Finland, Greece, Ireland, Israel, Netherlands, Romania, Slovakia, Sweden, Switzerland and the United Kingdom). Fifteen countries translated it into their local language (Austria, Belarus, Bulgaria, Croatia, Czech Republic, France, Germany, Hungary, Italy, Poland, Portugal, Russia, Serbia, Turkey and Ukraine). The Spanish survey was offered to members of the Spanish Society of Endocrinology in both the original English and its Spanish translation. The national leads decided how to distribute the questionnaire to thyroid specialists in their country. Online platforms were used in twenty-six countries, namely Lime Survey in twelve (Croatia, Denmark, Finland, Greece, Hungary, Ireland, Italy, Poland, Romania, Russia, Serbia and Ukraine), SurveyMonkey in nine (Austria, Belgium, Czech Republic, France, Germany, Netherlands, Slovakia, Sweden and Switzerland), Google Forms in four (Israel, Portugal, Spain, Turkey) and Qualtrics by one (United Kingdom), while e-mails were used in Belarus and Bulgaria.
2.2. Selection criteria
European countries fulfilling the following criteria were targeted: a population of at least 4 million, having a national endocrine and/or thyroid professional organisation and a national medical journal. The study aimed for a minimum of 100 respondents from each country. Eligible national endocrine and thyroid professional organisations were approached by the Steering Committee and were invited to participate. Two endocrinologists per country were identified as national leads. All members of the national endocrine and thyroid professional organisations were invited to participate by an e-mail from the President of each organisation, including an electronic link to the questionnaire.
2.3. Survey and data management
Responses on the online platforms were collected anonymously or anonymised when received by e-mail. The THESIS survey started in March 2019 and ended in April 2021. The survey was kept open for a median of 7 weeks (range 3-20) in each country. Respondents agreed to fill out the survey voluntarily, were aware that they could at any point leave the survey and did not receive any incentives. Personally identifiable data were not collected. The national leads and Steering Committee were responsible for data integrity and safekeeping for locally collected and aggregated data, respectively. An institutional board review was not necessary as the survey was anonymous.
2.4. Statistical analyses
Only data from respondents who completed all questions about demographic data were considered valid for statistical analyses. For statistical analyses, R was used (32). Survey data were not weighted. Qualitative variables were reported using frequencies and proportions, and quantitative variables using means and standard deviations. Chi-square and Cramer’s tests were used to test the association between qualitative variables. Statistical analyses were also performed using linear, logistic, and ordinal regression as appropriate (33), using R packages statistics and ordinal. The level of statistical significance was fixed at 5%. The effect size is independent of sample size and p-value and allows disregarding statistically significant but practically irrelevant results (34, 35). Therefore, we report both the p-value and effect size measures and are guided by the effect size measures. Cramer’s V measures effect size, and values were interpreted according to Rea and Parker (34). Cramer’s V values less than 0·1 are interpreted as negligible, between 0·1 and 0·2 as weak, 0·2-0·4 as moderate, 0·4-0·6 as relatively strong, and over 0·6 as a strong association. When necessary, interval variables, such as age, that were aggregated into the groups were converted to means using the R package actuar (36).
Geographic regions were defined according to the United Nations Statistics Division definition (37) (Eastern Europe: Belarus, Bulgaria, Czech Republic, Hungary, Poland, Romania, Russian Federation, Slovakia, Ukraine; Northern Europe: Denmark, Finland, Ireland, Sweden, United Kingdom; Southern Europe: Croatia, Greece, Italy, Portugal, Serbia, Slovenia, Spain; Western Europe: Austria, Belgium, France, Germany, Netherlands, Switzerland; Western Asia: Israel, Turkey). Data on GNI per capita in US dollars were derived from the World Bank (2019, Atlas Method) (38).
3. Results
3.1. Responses
A total of 17,232 invitations led to 6,058 responses, of which 5,695 were valid ( Figure 1 ). The overall valid response rate was 33·0%. The median response rate per country was 40·6% (range 6·8-95·2%, first quartile 25·0%, third quartile 51·4%). Twenty-eight of the 29 invited countries (all in Europe plus Turkey and Israel) agreed to participate, with Norway being the only nation that declined. Response rates significantly differed between countries, ranging from 6·8-95·2% (p <0·01, Figure 2 ).
Figure 1.
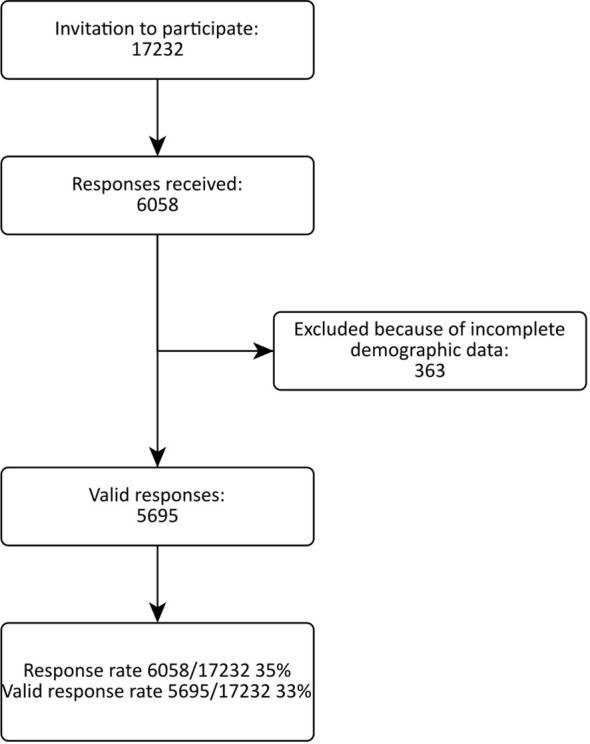
Flow chart of the THESIS survey.
Figure 2.

Responses to the questionnaire by country. The height of the bars represents the total number of invitees. The number of respondents is grey, and the response rate (%) is the number on the top of each bar. Bars are sorted by the response rate, from low to high.
3.2. Baseline characteristics
The baseline characteristics of respondents are shown in Table 1 . The mean age was 49.1 (SD 12.0) years, and 65% were female. Most respondents (98.0%) were working at the patients and 2% were basic scientists, and 93.0% were endocrinologists. Only 9·6% were members of international professional thyroid organisations. A substantial subgroup (38·3%) practised at a university centre, and 16·2% exclusively in private practice. Nearly two-thirds (62·1%) of respondents treated more than 100 hypothyroid patients per year.
Table 1.
Baseline characteristics of respondents.
| Variable | Number (%) |
|---|---|
| Clinical or Research | |
| Clinical | 5,583 (98·0) |
| Research | 112 (2·0) |
| Total | 5,695 |
| Sex | |
| Female | 3,700 (65·0) |
| Male | 1,995 (35·0) |
| Total | 5,695 |
| Age (years) | |
| ≤30 | 282 (5·0) |
| 31-40 | 1,375 (24·1) |
| 41-50 | 1,565 (27·5) |
| 51-60 | 1,479 (26·0) |
| 61-70 | 792 (13·9) |
| 70+ | 202 (3·5) |
| Total | 5,695 |
| Endocrinologist | |
| Yes | 5,299 (93·0) |
| No | 396 (7·0) |
| Total | 5,695 |
| ETA/ATA/LATS/AOTA Member1 | |
| Yes | 544 (9·6) |
| No | 5,151 (90·4) |
| Total | 5,695 |
| Practice at University Centre | |
| Yes | 2,181 (38·3) |
| No | 3,514 (61·7) |
| Total | 5,695 |
| Exclusively in private practice | |
| Yes | 794 (16·2) |
| No | 4,097 (83·8) |
| Total2 | 4,891 |
| Hypothyroid patients per year | |
| Fewer than 10 | 158 (2·8) |
| 10-50 | 787 (13·9) |
| 51-100 | 1,206 (21·2) |
| More than 100 | 3,526 (62·1) |
| Total3 | 5,677 |
1ETA, European Thyroid Association; ATA, American Thyroid Association; LATS, Latin American Thyroid Society; AOTA, Asia and Oceania Thyroid Association. 2Respondents working both in private practice and in the public healthcare sector were excluded from the analysis. 3Some respondents did not answer this question.
3.2.1. Sex
The sex distribution of respondents in our sample was comparable to the sex distribution of the European physicians. Data on the sex distribution of European physicians were obtained from Eurostat, the statistical office of the European Union (39) (largest Cramer’s v 0·027). Sixty-five per cent of THESIS respondents were female, ranging between 36·6-93·9% among different countries. The association between sex distribution and the country was moderate (p < 0·001, Cramer’s v 0·28). The proportion of female respondents differed significantly between regions with a moderate association (p < 0·001, Cramer’s v 0·21) and was lowest in Northern Europe (45·6%) and highest in Eastern Europe (77·2%). Younger age correlated significantly with an increased proportion of female respondents (Cochran-Armitage test for trend, p-value <0·001, two-sided). To explore the impact of differences in retirement age between sexes, we repeated the analysis in respondents younger than 60 years. The proportion of female respondents still ranged widely from 42·7% to 95·6% and did not significantly alter the outcome of the analysis (p < 0·001, Cramer’s v 0·29).
3.2.2. Age
The mean age of respondents was 49.1 (SD 12.0) years (calculated from grouped data). The age distribution significantly differed between countries (country-specific mean age: lowest in Romania 43·4 years, and highest in Finland 55·3 years). However, the association was weak (Cramer’s v 0·18). The association between respondent age and GNI per capita was negligible.
3.2.3. Speciality
On average, 93.0% of the respondents were endocrinologists, ranging between 64·2% in Finland and 100% in Belarus and Ireland ( Supplementary Figure 1 ). The association between the proportion of endocrinologists and country was moderate (p<0·001, Cramer’s v 0·30). There was no association between the proportion of endocrinologists and GNI per capita or age.
3.2.4. Place of work
The study included 2,181 (38·3%) physicians affiliated with university centres and 3,514 (61·7%) not affiliated with university centres ( Supplementary Figure 2 ). The distribution of respondents affiliated with the university centres differed between countries, being lowest in Belarus (5·5%) and Ukraine (11·3%) and highest in Spain (75·7%) and Serbia (71·7%). The association was relatively strong (p<0·001, Cramer’s v 0·42). Neither sex nor GNI per capita was associated with the proportion of respondents affiliated with a university centre.
3.2.4.1. Private practice
To analyse the differences between respondents who worked exclusively in private practice and those who did not, we excluded respondents who worked in both settings. The sample included 794 (16·2%) respondents working exclusively in private practice and 4,097 (83·8%) who did not ( Supplementary Figure 3 ). The distribution of private practitioners differed between countries, and the association was relatively strong (p <0·001, Cramer’s v 0·40). The association between the proportion of private practitioners and sex was negligible (p=0·042, Cramer’s v = 0·03). There was a linear relationship between the proportion of private practitioners and age (Cochran-Armitage test for trend, p <0·001, two-sided). The age distribution differed between private practitioners and other respondents, but the association was weak (Fisher’s exact test, p <0·001, Cramer’s v 0·13). The proportion of private practitioners differed between geographic regions, and the association was moderate (p-value <0·001, Cramer’s v 0·23). Including respondents who worked in private and public practice did not significantly change the results of this analysis.
3.2.5. Number of hypothyroid patients treated per year
A small minority of respondents (n=158, 2·8%) reported that they rarely treated hypothyroid patients, 787 (13·9%) treated 10-50 patients per year, 51-100 patients per year were treated by 1,206 (21·2%), and 62·1% (3,526) treated over 100 patients per year. This distribution differed between countries ( Supplementary Figure 4 ). The lowest proportion of respondents who treated more than 100 patients per year was reported in Sweden, Finland and Denmark (15·5%, 22·0% and 27·2%, respectively) and the highest in Turkey, Greece and the Slovak Republic (92·2%, 86·7%, 83·7%, respectively). The association between country and number of treated patients per year was moderate (p <0·001, Cramer’s v 0·26).
3.3. Multivariate analyses
3.3.1. Response rates, age, sex, survey language and GNI per capita
The mean age of respondents, the proportion of female respondents, survey language (local or English), GNI per capita, number of days the survey was accessible, and number of reminders sent were not associated with response rates (data not shown).
3.3.2. Age, sex, country and geographical region
Logistic regression, where age was nested within the geographic region, showed a significant inverse relationship between age and proportion of female respondents in all regions (p <0·01, AUC 0·69, 95% CI: 0·68-0·71). After restricting age to less than 60 years, logistic regression, where age was nested within the geographic region, showed that the inverse relation between age and proportion of female respondents was lost in Northern Europe and Western Asia (logistic regression p <0·01, AUC 0·65, 95% CI: 0·64-0·67).
3.3.3. Age, sex, private practice, number of hypothyroid patients treated per year, and GNI per capita
A striking relationship was noted between respondent sex and national economic status (expressed as GNI per capita). GNI per capita was inversely associated with the proportion of female respondents (p <0·001 by linear regression, r2 = 0·42, Figure 3 ). Excluding respondents older than 60 years did not significantly alter this finding (p <0·001 by linear regression, r2 = 0·38). Decreasing GNI per capita correlated with an increasing proportion of private practitioners (p <0·011 by linear regression, r2 = 0·23, Figure 4 ). As GNI per capita increased, the proportion of respondents who treated more than 100 patients per year decreased (p <0·01 by linear regression, r2 = 0·36).
Figure 3.

Relation between the proportion of female respondents and gross national income per capita (GNI per capita).
Figure 4.

Relation between gross national income per capita (GNI per capita) and proportion of private practitioners.
4. Discussion
Thyroid specialists play a key role in promoting public health by facilitating early diagnosis and treatment, educating patients on the importance of managing their condition, and collaborating with other healthcare providers to manage and control their patients’ hypothyroidism and other related health conditions. Thyroid specialists are also involved in research and development of guidelines. By addressing these public health aspects, thyroid specialists can improve the overall health and well-being of individuals and communities affected by hypothyroidism.
We surveyed thyroid specialists belonging to national endocrine and thyroid professional organisations of the most populous European countries to document the demographic and work-related characteristics of physicians who treat hypothyroid patients in different European countries and explore associations with geo-economic factors. The overall valid response rate of 33% is comparable to response rates achieved by European physician surveys related to topics focusing on benign thyroid disease since 2008 (median 38%, range 26-52%) (40–43). Comparing physicians’ characteristics (sex distribution by country) from Eurostat (39) with THESIS showed negligible differences (the largest Cramer’s v was 0·027). It has been suggested that the relationship between the survey response rate and non-response bias is small (44). Despite this, we assessed non-response bias using two different approaches (34, 45). One was to assess the influence of measured variables on response rate, and another was to compare the distribution of sample variables with the distribution of the same variables in the reference population. Neither of these approaches showed systematic bias, suggesting that the survey reflects a representative sample.
Moreover, the response rates recorded in THESIS are likely to be underestimated, as national endocrine and thyroid professional organisations include members who are not clinically active and are most likely not to have responded to the questionnaire. The participants are likely to represent European specialists who manage thyroid diseases. The response rate was not statistically dependent on the language used in the questionnaire (national or English language), age, sex of the respondent, allowed time for responding or GNI per capita, but did vary by country, being lowest in the Netherlands, Switzerland, and Austria (6·8-19%) and highest in Germany, Ireland, and Bulgaria (79·1-95·2%). Several reasons could explain the national differences in response rates. In many European countries, patients with hypothyroidism are treated preferably by general practitioners whereas thyroid patients with more complex pathologies are referred to an endocrinologist. Also, endocrine societies include members who do not treat thyroid patients (pathologists, basic scientists etc). Furthermore, thyroid specialists from some national professional organisations are more accustomed to completing surveys (for example the Italian Associazione Medici Endocrinologi) and achieve high response rates compared to others (46). Response rates may also have been negatively influenced by the availability of potential THESIS participants involved with the ongoing COVID-19 pandemic.
An important question is whether the data reported here are relevant to the bulk of care delivered to hypothyroid patients at large. Complementary surveys targeting primary care physicians will be required to address this. However, the participating thyroid specialists (which included national opinion leaders) are likely to exert a major influence on practices in primary care at the national level. Furthermore, it is anticipated that the population of hypothyroid patients managed by thyroid specialists represents those patients who experience difficulties in achieving therapeutic targets or have persistent symptoms and utilise services most. The latter subgroup of hypothyroid patients has been the subject of intense research in the past three decades. Being aware of variations in demographic and geo-economic parameters of health providers is of interest (5).
Most respondents were female (65%), although this varied widely across countries (39-93%), with the largest differences observed between Northern and Eastern Europe, the former showing the lower proportion of female endocrinologists. Restricting the analysis to respondents younger than 60 years (to overcome the potential bias due to the difference in retirement age for men and women) did not significantly change the results. The increase in the proportion of women physicians is a universal finding. Eurostat data show that more females are enrolled in medical schools than men, reaching 60% in 2021 (47). Low salaries may disincentivise male workers and instigate their relocation to other higher-paying employment or countries with a higher GNI per capita. Other possible explanations include increased educational opportunities for women, changing gender norms and attitudes, and supportive policies and initiatives to promote gender equality. However, the influence of the GNI per capita favours the former explanation.
Hypothyroid patients seem to be managed predominantly by young female thyroid specialists in Europe, as demonstrated by the significant inverse linear relationship between the proportion of female respondents and age. This tendency applies across Europe as the relationship was present and robust in all the participating regions and is supported by the Eurostat data. This accords with the global increase in the proportion of women in all medical fields (48). Our finding of a female preponderance, particularly in Eastern European countries, is consistent with a recent trend of rising female sex ratios among Eastern European University staff (49). It has been speculated that low salaries disincentive male workers and instigate their relocation to other higher-paying employments or countries with a higher GNI per capita (49). Our finding of an inverse relation between GNI per capita and the proportion of female respondents is consistent with this hypothesis.
THESIS has shown that the work environment of thyroid specialists differs between countries. Private practice, in particular, varied widely. Of note, GNI per capita was inversely associated with the proportion of private practitioners. This may be explained by the fact that European countries with high GNI per capita have more efficient and easily accessible national healthcare systems than less affluent countries, resulting in a less needed private health sector. Higher salaries for thyroid specialists employed by the public health system in wealthy countries also may reduce the drive to work privately. The linear relationship between age and proportion of respondents engaged in private practice probably reflects a switch by the more experienced (and hence older) physicians from public to private practice in their later careers. Finally, the number of treated patients per year differed between countries and was inversely associated with the GNI per capita. This, too, is likely related to wealthy countries having a well-established and efficient primary care tier that manages most patients with hypothyroidism. The strong association between thyroid specialist characteristics and GNI per capita raises the important question of whether hypothyroid patients are treated differently according to geo-economic factors, and merits further investigation.
Strengths of THESIS include a large number of responses from nearly all European nations with a population of more than 4 million, utilisation of reliable channels for dissemination of the questionnaire in the form of national endocrine and thyroid professional organisations, exploration of a topic that has never been studied in such detail before and the potential repercussions of thyroid specialist characteristics on the patient experience.
There are also limitations: the questionnaire was not validated; the questionnaire had to be translated into several languages; the time for responding was unstandardised and varied substantially between nations; some of the national data were published and available before the end of the study, thus potentially allowing some of the countries access to how others in other countries had responded; the response rates varied considerably between countries; the impact of the COVID-19 pandemic (50, 51). To mitigate bias, strict inclusion criteria were applied, and robust statistical analyses were employed. However, the shortcomings alluded to above may have influenced the results of THESIS.
Thyroid specialists in Europe are predominantly young female endocrinologists, most of whom work in the public sector. Striking inverse associations were shown between the female sex and GNI per capita and private practice and GNI per capita. The most significant contributor to national differences was GNI per capita, but organisational aspects of each healthcare system, historical influences, and socio-political factors might play a role. Demographic and geo-economic variations among specialist healthcare providers for patients with hypothyroidism in Europe are notable and may have a bearing on patient-reported outcomes.
Data availability statement
The datasets presented in this article are not readily available because these are data from members of 28 European Endocrine Societies, currently forming the basis of a multitude of national as well as aggregate data publications. Requests to access the datasets should be directed to milos.zarkovic@med.bg.ac.rs and laszlo.hegedus@rsyd.dk.
Author contributions
LH, EP, EN and PP conceptualized the study. MZ drafted the manuscript and performed the data analyses. MZ, LH EP, EN, RN, RA and PP participated in the interpretation of data, critically reviewed the manuscript, and approved the final draft. CAC, EA, MA, GA, TB, EB, MB, AB, MB, CB, MB, JC, JD, HD, VF, BF, EF, CF, DS, JG, TH, JJ, PK, MK, MK, MK, ML, IL, LL, VL, AM, MM, SM, CM, TM, TM, BB, DN, BP, TP, CP, ER, PR, MR, KR, AS, JF, DU, IV, WV, MV, YY, EY participated in data collection, critically reviewed the manuscript and approved the final draft. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors wish to thank all national endocrine and thyroid professional organizations and their members who responded to the THESIS questionnaire.
Conflict of interest
LH, PP, EP, EN received consultancy fees from IBSA Biochimique SA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer PM declared a shared affiliation with the author TB to the handling editor at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1225202/full#supplementary-material
References
- 1. Razvi S, Korevaar TIM, Taylor P. Trends, determinants, and associations of treated hypothyroidism in the United Kingdom, 2005–2014. Thyroid (2019) 29(2):174–82. doi: 10.1089/thy.2018.0251 [DOI] [PubMed] [Google Scholar]
- 2. Somwaru LL, Arnold AM, Joshi N, Fried LP, Cappola AR. High frequency of and factors associated with thyroid hormone over-replacement and under-replacement in men and women aged 65 and over. J Clin Endocrinol Metab (2009) 94(4):1342–5. doi: 10.1210/jc.2008-1696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Lillevang-Johansen M, Abrahamsen B, Jørgensen HL, Brix TH, Hegedüs L. Over- and under-treatment of hypothyroidism is associated with excess mortality: A register-based cohort study. Thyroid (2018) 28(5):566–74. doi: 10.1089/thy.2017.0517 [DOI] [PubMed] [Google Scholar]
- 4. Carlé A, Laurberg P, Pedersen IB, Knudsen N, Perrild H, Ovesen L, et al. Mainly the younger hypothyroid patients are referred to hospital — Evidence for referral bias. J Clin Epidemiol (2009) 62(4):446–51. doi: 10.1016/j.jclinepi.2008.06.016 [DOI] [PubMed] [Google Scholar]
- 5. Hegedüs L, Bianco AC, Jonklaas J, Pearce SH, Weetman AP, Perros P. Primary hypothyroidism and quality of life. Nat Rev Endocrinol (2022) 18(4):230–42. doi: 10.1038/s41574-021-00625-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. European Society of Endocrinology . Survey “Mapping Endocrinology in Europe” (2018). Available at: https://www.ese-hormones.org/media/2725/meneu-leaflet-a4-final.pdf.
- 7. Decallonne B, Van den Bruel A, Macq G, Elaut N, De Schutter H. The impact of regional variation in clinical practice on thyroid cancer diagnosis: A national population-based study. Eur Thyroid J (2020) 9(1):32–9. doi: 10.1159/000504046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Jonklaas J, Tefera E, Shara N. Prescribing therapy for hypothyroidism: influence of physician characteristics. Thyroid (2019) 29(1):44–52. doi: 10.1089/thy.2018.0369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Burch HB, Burman KD, Cooper DS, Hennessey JV. A 2013 survey of clinical practice patterns in the management of primary hypothyroidism. J Clin Endocrinol Metab (2014) 99(6):2077–85. doi: 10.1210/jc.2014-1046 [DOI] [PubMed] [Google Scholar]
- 10. Taylor PN, Albrecht D, Scholz A, Gutierrez-Buey G, Lazarus JH, Dayan CM, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat Rev Endocrinol (2018) 14(5):301–16. doi: 10.1038/nrendo.2018.18 [DOI] [PubMed] [Google Scholar]
- 11. Ayvaz G, Akarsu E, Attanasio R, Hegedus L, Nagy EV, Papini E, et al. The use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS* questionnaire survey of Turkish physicians. Turkish J Endocrinol Metab (2022) 26(2):85–91. doi: 10.5152/tjem.2022.22024 [DOI] [Google Scholar]
- 12. Bednarczuk T, Attanasio R, Hegedüs L, Nagy EV, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* questionnaire survey of Polish physicians. *THESIS: Treatment of hypothyroidism in Europe by specialists: an international survey. Endokrynol Pol (2021) 72(4):357–65. doi: 10.5603/EP.a2021.0048 [DOI] [PubMed] [Google Scholar]
- 13. Berta E, Lengyel IM, Hegedűs L, Papini E, Perros P, Negro R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of Hungarian physicians. Orv Hetil. (2022) 163(12):463–72. doi: 10.1556/650.2022.32412 [DOI] [PubMed] [Google Scholar]
- 14. Borissova AMI, Boyanov MA, Attanasio R, Hegedus L, Nagy E, Negro R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* Questionnaire survey of Bulgarian physicians (Българско дружество по ендокринология). Endocrinologia (2020) 24(4):229–309. [Google Scholar]
- 15. Buffet C, Belin L, Attanasio R, Negro R, Hegedüs L, Nagy EV, et al. Real-life practice of thyroid hormone use in hypothyroid and euthyroid patients: A detailed view from the THESIS questionnaire survey in France. Ann Endocrinol (Paris). (2022) 83(1):27–34. doi: 10.1016/j.ando.2021.11.002 [DOI] [PubMed] [Google Scholar]
- 16. Burlacu MC, Attanasio R, Hegedüs L, Nagy EV, Papini E, Perros P, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a THESIS* survey of Belgian specialists *THESIS: treatment of hypothyroidism in Europe by specialists: an international survey. Thyroid Res (2022) 15(1):3. doi: 10.1186/s13044-022-00121-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Galofré JC, Attanasio R, Hegedüs L, Nagy E, Negro R, Papini E, et al. Use of thyroid hormone in hypothyroid patients and euthyroid subjects in Spain: A THESIS* questionnaire survey. Endocrinol Diabetes Nutr (Engl Ed). (2022) 69(7):520–9. doi: 10.1016/j.endien.2022.07.001 [DOI] [PubMed] [Google Scholar]
- 18. Jiskra J, Paleček J, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2020 THESIS questionnaire survey of members of the Czech Society of Endocrinology. BMC Endocr Disord (2022) 22(1):117. doi: 10.1186/s12902-022-01027-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Metso S, Hakala T, Attanasio R, Nagy E, Negro R, Papini E, et al. Use of thyroid hormones in the treatment of hypothyroidism: Thesis questionnaire survey for Finnish specialists. Finnish Med J (2021) 48(76):2885–9. [Google Scholar]
- 20. Mustafa M, Ali E, McGowan A, McCabe L, Hegedüs L, Attanasio R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of members of the Irish Endocrine Society. Ir J Med Sci (2022) 192:2179–87. doi: 10.1007/s11845-022-03235-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Nedeljkovic-Beleslin B, Attanasio R, Hegedüs L, Nagy E, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of Serbian physicians. Srp Arh Celok Lek (2022) 150(11–12):667–74. doi: 10.2298/SARH211221110N [DOI] [Google Scholar]
- 22. Negro R, Attanasio R, Nagy EV, Papini E, Perros P, Hegedüs L. Use of thyroid hormones in hypothyroid and euthyroid patients; the 2019 italian survey. Eur Thyroid J (2020) 9(1):25–31. doi: 10.1159/000502057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Niculescu DA, Attanasio R, Hegedüs L, Nagy EV, Negro R, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A thesis* Questionnaire survey of Romanian physicians *Thesis: treatment of hypothyroidism in Europe by specialists: an international survey. Acta Endocrinol (Buchar). (2020) 16(4):462–9. doi: 10.4183/aeb.2020.462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Paschou SA, Alevizaki M, Attanasio R, Hegedüs L, Nagy EV, Papini E, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: a 2020 THESIS questionnaire survey of members of the Hellenic Endocrine Society. Hormones (Athens). (2022) 21(1):103–11. doi: 10.1007/s42000-021-00335-w [DOI] [PubMed] [Google Scholar]
- 25. Planck T, Lantz M, Perros P, Papini E, Attanasio R, Nagy EV, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A 2020 THESIS questionnaire survey of members of the swedish endocrine society. Front Endocrinol (Lausanne). (2021) 12:795111. doi: 10.3389/fendo.2021.795111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Puga F, Simões H, Melo M, Attanasio R, Hegedus L, Nagy EV, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of Portuguese endocrinologists. Rev Portuguesa Endocrinologia Diabetes e Metabolismo (2022) 17(1–2):9–18. doi: 10.26497/AO210050 [DOI] [Google Scholar]
- 27. Riis KR, Frølich JS, Hegedüs L, Negro R, Attanasio R, Nagy EV, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A 2020 THESIS questionnaire survey of members of the Danish Endocrine Society. J Endocrinol Invest. (2021) 44(11):2435–44. doi: 10.1007/s40618-021-01555-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Shepelkevich AP, Dydyshka YV, Yurenya EV, Lоbashova VL, Attanasio R, Hegedüs L, et al. [Features of the use of synthetic analogues of thyroid hormones: а 2020 THESIS* questionnaire survey of members of the Belarusian Public Medical Association of Endocrinology and Metabolism]. Probl Endokrinol (Mosk). (2021) 68(1):18–26. doi: 10.14341/probl12828 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Vardarli I, Brandenburg T, Hegedüs L, Attanasio R, Nagy E, Papini E, et al. A questionnaire survey of german thyroidologists on the use of thyroid hormones in hypothyroid and euthyroid patients: the THESIS (Treatment of hypothyroidism in europe by specialists: an international survey) collaborative. Exp Clin Endocrinol Diabetes. (2022) 130(9):577–86. doi: 10.1055/a-1832-0644 [DOI] [PubMed] [Google Scholar]
- 30. Younes YR, Perros P, Hegedüs L, Papini E, Nagy EV, Attanasio R, et al. Use of thyroid hormones in hypothyroid and euthyroid patients: A THESIS questionnaire survey of UK endocrinologists. Clin Endocrinol (Oxf) (2022) 98(2):238–48. doi: 10.1111/cen.14812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res (2004) 6(3):e34. doi: 10.2196/jmir.6.3.e34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. R Core Team . R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; (2021). Available at: https://www.R-project.org/. [Google Scholar]
- 33. Agresti A. An introduction to categorical data analysis. Third edition. Hoboken, NJ: John Wiley & Sons; (2019). p. 1. [Google Scholar]
- 34. Rea LM, Parker RA. Designing and conducting survey research: a comprehensive guide. Fourth edition. San Francisco, CA: Jossey-Bass, a Wiley brand; (2014). p. 332. [Google Scholar]
- 35. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ (2012) 4(3):279–82. doi: 10.4300/JGME-D-12-00156.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Dutang C, Goulet V, Pigeon M. actuar: an R package for actuarial science. J Stat Software (2008) 25(7):38. doi: doi: 10.18637/jss.v025.i07 [DOI] [Google Scholar]
- 37. United Nations Statistics Division . UNSD — Methodology. Available at: https://unstats.un.org/unsd/methodology/m49/.
- 38. The World Bank . GNI per capita ranking, Atlas method and PPP based | Data Catalog . Available at: https://datacatalog.worldbank.org/search/dataset/0038128.
- 39. Eurostat . Database - Eurostat. Available at: https://ec.europa.eu/eurostat/web/main/data/database.
- 40. Hegedüs L, Frasoldati A, Negro R, Papini E. European thyroid association survey on use of minimally invasive techniques for thyroid nodules. Eur Thyroid J (2020) 9(4):194–204. doi: 10.1159/000506513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Negro R, Attanasio R, Grimaldi F, Marcocci C, Guglielmi R, Papini E. A 2016 italian survey about the clinical use of selenium in thyroid disease. Eur Thyroid J (2016) 5(3):164–70. doi: 10.1159/000447667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Winther KH, Papini E, Attanasio R, Negro R, Hegedüs L. A 2018 european thyroid association survey on the use of selenium supplementation in hashimoto’s thyroiditis. Eur Thyroid J (2020) 9(2):99–105. doi: 10.1159/000504781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Vaidya B, Williams GR, Abraham P, Pearce SHS. Radioiodine treatment for benign thyroid disorders: results of a nationwide survey of UK endocrinologists. Clin Endocrinol (Oxf). (2008) 68(5):814–20. doi: 10.1111/j.1365-2265.2007.03097.x [DOI] [PubMed] [Google Scholar]
- 44. Hendra R, Hill A. Rethinking response rates: new evidence of little relationship between survey response rates and nonresponse bias. Eval Rev (2019) 43(5):307–30. doi: 10.1177/0193841X18807719 [DOI] [PubMed] [Google Scholar]
- 45. Halbesleben JRB, Whitman MV. Evaluating survey quality in health services research: a decision framework for assessing nonresponse bias. Health Serv Res (2013) 48(3):913–30. doi: 10.1111/1475-6773.12002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Negro R, Attanasio R, Grimaldi F, Guglielmi R, Papini E, AME (Associazione Medici Endocrinologi) and AACE (American Association of Clinical Endocrinologists) Italian Chapter . A 2015 Italian survey of clinical practice patterns in the management of graves’ Disease: comparison with european and north american surveys. Eur Thyroid J (2016) 5(2):112–9. doi: 10.1159/000444482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Eurostat . Students enrolled in tertiary education by education level, programme orientation, sex and age. Available at: https://ec.europa.eu/eurostat/databrowser/view/EDUC_UOE_ENRT02/default/table?lang=en&category=educ.educ_part.educ_uoe_enr.educ_uoe_enrt.
- 48. OECD . Health at a Glance 2019: OECD Indicators (2019). Available at: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2019_4dd50c09-en.
- 49. Guglielmi G. Eastern European universities score highly in university gender ranking. In: Nature (2019) d41586-019-0164:2–4. doi: 10.1038/d41586-019-01642-4 [DOI] [Google Scholar]
- 50. Pavlatou MG, Žarković M, Hegedüs L, Priestley J, McMullan C, Perros P. A survey on the psychological impact and access to health care of thyroid patients during the first SARS-COV-2 lockdown. Clin Endocrinol (Oxf). (2022) 96(6):869–77. doi: 10.1111/cen.14649 [DOI] [PubMed] [Google Scholar]
- 51. Žarković M, Perros P, Ćirić J, Beleslin B, Stojanović M, Stojković M, et al. Health care access of thyroid disease patients in Serbia during the COVID-19 pandemic. J Endocrinol Invest. (2022) 45(8):1521–6. doi: 10.1016/j.puhe.2019.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets presented in this article are not readily available because these are data from members of 28 European Endocrine Societies, currently forming the basis of a multitude of national as well as aggregate data publications. Requests to access the datasets should be directed to milos.zarkovic@med.bg.ac.rs and laszlo.hegedus@rsyd.dk.