

1. BRAIN HEALTH, AGEING AND DEMENTIA THROUGH THE LENSES OF DIVERSITY AND DISPARITY
Brain health, ageing and dementia are influenced by various heterogeneous factors, which do not exhibit universal applicability across diverse contexts. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 Variability in genetics, pathophysiological pathways, clinical presentations, aetiology and exposome is non‐homogeneous across geographical regions. 2 , 9 Additionally, unequal epidemiological patterns related to risk and protective factors, social determinants of health (SDH), socioeconomic disparities and healthcare access play important roles in brain health. 1 , 9 Thus, brain‐phenotype models developed in more homogenous populations from the Global North may misrepresent the characteristics of more diverse populations. 2 , 3 Despite the urgent need to explore regional diversity and provide tailored recommendations, a noticeable research imbalance across regions persists. 3 , 10 Paradoxically, most research has been conducted in high‐income settings within the United States and Europe, often overlooking the diverse and non‐stereotypical populations in the Global South.
The impact of high levels of disparities on brain health and ageing in underserved populations is evident across various aspects, including risk factors, brain dynamics, functionality, cognition, biomarkers, neurodegeneration, allostatic overload and access to novel therapeutic targets. 1 , 6 , 7 , 11 , 12 Social and environmental disparities, such as low education, elevated poverty rates and heightened exposure to adversity, increase the prevalence of chronic conditions associated with brain health and dementia risks. 13 For instance, metabolic disorders such as Type‐2 diabetes mellitus, cardiovascular disease and cerebrovascular disease are more prevalent among underserved populations. 13 , 14 We recently found 1 that health disparities and SDH, such as education, cardiometabolic conditions and social isolation, severely influence the healthy ageing of Latin American populations, impacting cognition and functional ability more than traditional factors like age and gender. This heterogeneity in risk factors was particularly pronounced in lower‐ to middle‐income countries (Colombia and Ecuador). In addition, while educational attainment predicts cognitive performance in older adults from homogeneous populations, 13 , 15 this relationship weakens among heterogeneous groups due to disparities in access to high‐quality education. Altogether, these findings emphasise the significant influence of disparities and region‐specific factors on brain health and ageing. These effects seem to be more accentuated across Global South populations, evidencing the inadequacy of a one‐size‐fits‐all approach.
Similarly, population diversity and disparity have a strong effect on dementia. 8 , 11 , 13 , 16 North Africa/Middle East (8.7%) and Latin America (8.4%) exhibit the current highest dementia prevalence, with Central Europe having the lowest one (4.7%). 17 The larger prevalence in the Global South is associated with health and socioeconomic disparities. 8 , 11 Diversity and disparities are also evident in the projected increases in the number of people living with dementia in 2050, with the most significant percentage changes in North Africa and the Middle East (367%) and the smallest in Western Europe (74%). 17 Additionally, dementia genetic risk factors, such as the apolipoprotein (APOE) 4 allele, the most significant ged8netic risk factor for Alzheimer's disease (AD), seem to differ across populations. This allele is more frequent among individuals with African ancestry but has an attenuated association with AD risk, compared to those of European ancestry. 18 The influence of diversity and disparity is further evident in marked inequalities in care‐seeking and dementia diagnosis among the Global South. For example, in many low‐ and middle‐income countries, the diagnosis of dementia often occurs at a more advanced stage due to low societal awareness, compared to Western countries. 2 The caregiver burden is increased in Latin America, compared to other regions, due to structural adversities in health and social factors. 19 Moreover, most neuropsychological tests used for dementia diagnosis have been developed for educated, predominantly English‐speaking Western populations and may not be suitable for use in other cultures. 2 , 16 Taken together, this evidence highlights that interactions between heterogenous SDH, genetics, biological, exposome and psychosocial factors significantly influence dementia phenotypes, prevalence, risk and diagnosis. To systematically investigate these interactions, it is imperative to include greater diversity from non‐stereotypical populations.
Despite the acknowledged influence of diversity and disparity on brain health, ageing and dementia, 6 , 7 , 11 , 12 more comprehensive assessments of non‐stereotypical populations from the Global South are required (See Figure 1). Future methodological strategies should recognise and embrace the diversity within each country and region to address structural inequities. 1 In future endeavours, it is imperative to prioritise the inclusion of underrepresented older adult groups, improve the documentation of critical participant characteristics and assess the proportional representation of different racial, ethnic and minority groups. 18 Future research needs to integrate sources of population‐level and clinical data and utilise robust methods to address heterogeneity driven by diverse genetic, health, biological, functional, social, behavioral, financial and neighborhood influences on brain health, ageing and dementia in the Global South. 9 , 20
FIGURE 1.
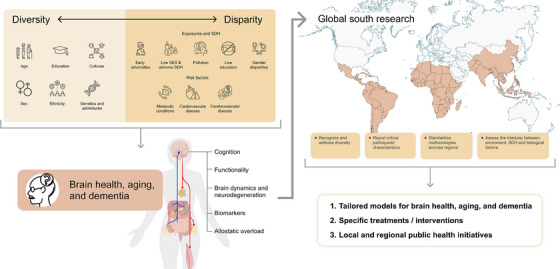
Diversity and disparity impact brain health, ageing and dementia. The left panel illustrates the interconnection between diversity and disparity and their impact on various dimensions of brain health, ageing and dementia (i.e., cognition, functionality, brain dynamics and neurodegeneration, biomarkers and allostatic overload). The upper right diagram highlights critical recommendations for addressing diversity and disparity and further understands their effects on the mentioned multidimensional factors in non‐stereotypical populations from the Global South. In the lower right corner, we outline the main expected outcomes of the proposed Global South research approach. SDH, social determinants of health; SES, socioeconomic status.
Efforts to harmonise and standardise methodologies across regions in the Global South are urgently needed. Initiatives to harmonise clinical research methods have been primarily focused on Caucasian populations, neglecting underrepresented populations. 2 Incorporating genetic and imaging methods alongside locally validated clinical protocols is essential to address diversity effectively. 2 Also, harmonisation frameworks across various disciplines, including epidemiology, clinical research, basic neuroscience and social sciences, are critically needed to provide a comprehensive understanding of the interplay between environmental and biological factors. 4 , 5 Identifying the most effective interventions for dementia in diverse sociocultural contexts of the Global South is crucial. This approach can provide more robust predictive models for brain health and ageing, as well as potential treatments for dementia tailored to the specific needs of diverse populations. These models can serve as valuable guides for local and regional public health initiatives. 1 To develop customised preventive measures, public health and clinical sciences leaders should recognise the complex interplay of disparity‐related factors, including individual health indicators and SDH from a local setting. 4 , 5 This tailored approach represents the foundation for shaping policies that yield synergistic benefits across various aspects of brain health, ageing and dementia (See Figure 1)
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ACKNOWLEDGEMENTS
Agustin Ibanez is supported by grants from ReDLat [National Institutes of Health and the Fogarty International Center (FIC), National Institutes of Aging (R01 AG057234, R01 AG075775, R01 AG21051, CARDS‐NIH), Alzheimer's Association (SG‐20‐725707), Rainwater Charitable Foundation—The Bluefield project to cure FTD, and Global Brain Health Institute)], ANID/FONDECYT Regular (1210195, 1210176 and 1220995); and ANID/FONDAP/15150012. The contents of this publication are solely the authors’ responsibility and do not represent the official views of these institutions.
REFERENCES
- 1. Santamaria‐Garcia H, Sainz‐Ballesteros A, Hernandez H, et al. Factors associated with healthy aging in Latin American populations. Nat Med. 2023;29(9):2248‐2258. doi: 10.1038/s41591-023-02495-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Alladi S, Hachinski V. World dementia: one approach does not fit all. Neurology. 2018;91(6):264‐270. doi: 10.1212/WNL.0000000000005941 [DOI] [PubMed] [Google Scholar]
- 3. Greene AS, Shen X, Noble S, et al. Brain–phenotype models fail for individuals who defy sample stereotypes. Nature. 2022;609(7925):109‐118. doi: 10.1038/s41586-022-05118-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ibáñez A, Legaz A, Ruiz‐Adame M. Addressing the gaps between socioeconomic disparities and biological models of dementia. Brain. 2023;146(9):3561‐3564. doi: 10.1093/brain/awad236 [DOI] [Google Scholar]
- 5. Ibanez A, Zimmer E. Time to synergize mental health with brain health. Nat Ment Health. 2023;1:441‐443. doi: 10.1038/s44220-023-00086-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. de Paula França Resende E, Guerra JJL, Miller BL. Health and socioeconomic inequities as contributors to brain health. JAMA Neurol. Published online March 25, 2019. doi: 10.1001/jamaneurol.2019.0362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Walsh S, Merrick R, Brayne C. The relevance of social and commercial determinants for neurological health. Lancet Neurol. 2022;21(12):1151‐1160. doi: 10.1016/S1474-4422(22)00428-8 [DOI] [PubMed] [Google Scholar]
- 8. Maestre G, Carrillo M, Kalaria R, et al. The Nairobi Declaration—reducing the burden of dementia in low‐ and middle‐income countries (LMICs): Declaration of the 2022 Symposium on Dementia and Brain Aging in LMICs. Alzheimers Dement J Alzheimers Assoc. 2023;19(3):1105‐1108. doi: 10.1002/alz.13025 [DOI] [PubMed] [Google Scholar]
- 9. Aranda MP, Kremer IN, Hinton L, et al. Impact of dementia: health disparities, population trends, care interventions, and economic costs. J Am Geriatr Soc. 2021;69(7):1774‐1783. doi: 10.1111/jgs.17345 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Stephan BCM, Pakpahan E, Siervo M, et al. Prediction of dementia risk in low‐income and middle‐income countries (the 10/66 Study): an independent external validation of existing models. Lancet Glob Health. 2020;8(4):e524‐e535. doi: 10.1016/S2214-109X(20)30062-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet. 2020;396(10248):413‐446. doi: 10.1016/S0140-6736(20)30367-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Murkey JA, Watkins BX, Vieira D, Boden‐Albala B. Disparities in allostatic load, telomere length and chronic stress burden among African American adults: a systematic review. Psychoneuroendocrinology. 2022;140:105730. doi: 10.1016/j.psyneuen.2022.105730 [DOI] [PubMed] [Google Scholar]
- 13. Babulal GM, Quiroz YT, Albensi BC, et al. Perspectives on ethnic and racial disparities in Alzheimer's disease and related dementias: update and areas of immediate need. Alzheimers Dement. 2019;15(2):292‐312. doi: 10.1016/j.jalz.2018.09.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Carnethon MR, Pu J, Howard G, et al. Cardiovascular health in African Americans: a scientific statement from the American Heart Association. Circulation. 2017;136(21):e393‐e423. doi: 10.1161/CIR.0000000000000534 [DOI] [PubMed] [Google Scholar]
- 15. Manly JJ, Schupf N, Tang MX, Stern Y. Cognitive decline and literacy among ethnically diverse elders. J Geriatr Psychiatry Neurol. 2005;18(4):213‐217. doi: 10.1177/0891988705281868 [DOI] [PubMed] [Google Scholar]
- 16. Parra MA, Baez S, Allegri R, et al. Dementia in Latin America: assessing the present and envisioning the future. Neurology. 2018;90(5):222‐231. doi: 10.1212/WNL.0000000000004897 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Prince M, Wimo A, Guerchet M, Ali GC, Wu YT, Prina M, World Alzheimer Report 2015. The global impact of dementia: an analysis of prevalence, incidence, cost and trends. https://www.alzint.org/resource/world-alzheimer-report-2015/ (October 20, 2023)
- 18. Naslavsky MS, Suemoto CK, Brito LA, et al. Global and local ancestry modulate APOE association with Alzheimer's neuropathology and cognitive outcomes in an admixed sample. Mol Psychiatry. 2022;27(11):4800‐4808. doi: 10.1038/s41380-022-01729-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ibáñez A, Pina‐Escudero SD, Possin KL, et al. Dementia caregiving across Latin America and the Caribbean and brain health diplomacy. Lancet Healthy Longev. 2021;2(4):e222‐e231. doi: 10.1016/s2666-7568(21)00031-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kilbourne AM, Switzer G, Hyman K, Crowley‐Matoka M, Fine MJ. Advancing health disparities research within the health care system: a conceptual framework. Am J Public Health. 2006;96(12):2113‐2121. doi: 10.2105/AJPH.2005.077628 [DOI] [PMC free article] [PubMed] [Google Scholar]