

Abstract
Background
Patients have varying levels of chronic conditions and health insurance patterns as they become Medicare age-eligible. Understanding these dynamics will inform policies and reforms that direct capacity and resources for primary care clinics to care for these aging patients. This study 1) determined changes in chronic condition rates following Medicare age eligibility among patients with different insurance patterns and 2) estimated the number of chronically ill patients who remain inadequately insured post-Medicare eligibility among patients receiving care in community health centers.
Method
We used retrospective electronic health record data from 45,527 patients aged 62–68 from 990 community health centers in 25 states in 2014–2019. Insurance patterns (continuously insured, continuously uninsured, uninsured/discontinuously insured who gained insurance after age 65, lost insurance after age 65, discontinuously insured) and diagnosis of chronic conditions were defined at each visit pre- and post-Medicare eligibility. Difference-in-differences Poisson GEE models estimated changes of chronic condition rates by insurance groups pre- to post-Medicare age eligibility.
Results
Post-Medicare eligibility, 72% patients were continuously insured, 14% gained insurance; and 14% were uninsured or discontinuously insured. The prevalence of multimorbidity (≥2 chronic conditions) was 77%. Those who gained insurance had a significantly larger increase in the rate of documented chronic conditions from pre- to post-Medicare (DID: 1.06, 95%CI:1.05–1.07) compared with the continuously insured group.
Conclusions
Post-Medicare age eligibility, a significant proportion of patients were diagnosed with new conditions leading to high burden of disease. One in 4 older adults continue to have inadequate health care coverage in their older age.
Keywords: Chronic Disease, Community Health Centers, Geriatrics, Health Care Disparities, Health Insurance, Health Services Accessibility, Medically Uninsured, Medicare, Multimorbidity, Retrospective Studies, multiple chronic conditions, safety-net
INTRODUCTION
With aging, the incidence of chronic health problems increases and the need for continuous and comprehensive health care access becomes crucial. The prevalence of chronic health conditions increases significantly starting in mid-life.1 In the United States, half of adults aged 55–64 have high cholesterol and/or hypertension. Importantly, the top five leading causes of death among older adults (≥65) are preventable chronic diseases that developed earlier in life.2 Accurate and timely diagnosis are critical to ensure adequate treatment and management of chronic diseases. Yet, many Americans face barriers in accessing continuous care, and live with undetected and unmanaged conditions.
Access to health insurance, a basic need, is inequitably distributed among the United States population and is a contributor to poor chronic disease management. Many studies have shown that lacking insurance, experiencing insurance coverage gaps, or being underinsured is associated with limited access to care, unmet health care needs, difficulty accessing medications, and forgoing care which ultimately lead to poor health outcomes.3–14 There is a bidirectional relationship between having health insurance and chronic disease detection and management. On the one hand, those with health insurance are more likely to have chronic illnesses detected and receive treatments than those without.15–18 For instance, evidence shows that gaining insurance is associated with increased receipt of preventive services and access to primary care visits, which can lead to diagnosis of a previously undetected conditions.15,19–26 On the other hand, those with chronic illnesses may be more motivated to obtain or continue to have health insurance to manage their existing conditions.
Lack of health insurance coverage is particularly concerning among individuals in mid-life, when chronic conditions become more prevalent. Individuals in mid-life without health insurance are more likely to have rapid disease progression and are at increased risk for premature mortality.27,28 Inadequately insured people are also more likely to have lived in poverty and be from underrepresented racial and ethnic minority groups.11,13 A recent study showed that, among economically and socially marginalized patients with multiple chronic conditions, over 48% experience health insurance instability, including 13% without continuous health insurance coverage.29
Understanding how patients with lower socioeconomic resources who have multiple chronic conditions age into Medicare is important to inform Medicare coverage policies. In addition, this knowledge can assist health care systems, especially from safety-net clinics, determine the capacity and resources needed to serve aging patients with complex health needs. Community health centers (CHCs), a large component of the US safety-net system, serve 29 million patients nation-wide and provide health care to medically-underserved populations, regardless of health insurance coverage, documentation status, or ability to pay.30 While CHCs provide excellent quality of care for their patients, patients experience higher rates of social risk and poorer health outcomes compared with patients who seek care outside of the safety-net.30,31 Assessing changes in chronic disease burden among CHC patients aged 65 and older as they transition into Medicare or remain un- or underinsured is important for CHC leaders and providers to inform their geriatric care programs.32 Although Medicare is the government insurance program for older adults, some people aged 65 and older may not have coverage due to eligibility criteria or cost. Typically, people aged 65 and older who are citizens or permanent residents of the United States and are eligible for Social Security benefits or Railroad Retirement Board benefits can receive Medicare coverage.33 Spouses of eligible individuals can also receive Medicare coverage. Medicare part A (hospital insurance) has no premium while Medicare part B (medical insurance) and part D (prescription drug coverage) incur premiums. Those not eligible for Medicare can enroll in other private insurance plans, such as individual marketplace plans. Similar to Medicare Part B and D coverage, these private plans incur premiums, deductibles, and copayments that could be a significant barrier for patients receiving care in CHCs, who often have lower socioeconomic resources. Although there are additional programs that can assist low-income patients with these cost-sharing obligations, they vary by state and require other eligibility criteria which may not ensure continuous coverage.
To our knowledge, no previous study has examined the chronic health burden among older adult patients receiving care in CHCs who transitioned into Medicare coverage or who remain un- or underinsured after the age of 65. Therefore, the purpose of this study was to use longitudinal data to 1) determine changes in rates of chronic conditions and multimorbidity status following Medicare age eligibility among patients with different insurance patterns and 2) estimate the number of chronically ill patients who remain inadequately insured post-Medicare age eligibility.
METHODS
The study protocol was approved by the university’s Institutional Review Board (IRB ID# STUDY00020124).
Data source
Electronic health record (EHR) data were obtained from the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) multi-state clinical research network (CRN) of PCORNnet.34 ADVANCE represents a unique ‘community laboratory’ of clinical data for research with underrepresented populations receiving care in CHCs (http://advancecollaborative.org). The ADVANCE patient population has been found to be representative of the overall CHC population in the US.30,34 OCHIN (not an acronym) created and leads the ADVANCE CRN, one of 11 original CRNs in PCORNet funded by PCORI. The ADVANCE centralized Research Data Warehouse (RDW) merges data from several CHC networks including OCHIN, Health Choice Network, and Fenway. To date, ADVANCE includes >2,000 clinics and >8 million patients across the United States. The ADVANCE RDW is an expansion of the PCORnet Common Data Model (CDM), containing all tables and fields defined for the PCORnet CDM, plus additional ones that support health equity research.35 The RDW contains some elements that define PHI under HIPAA, including encounter dates and date of birth. Analytic data are de-identified before being shared with researchers to ensure that no patients are individually identifiable.
Study cohort
We assessed data from 45,527 older patients in 990 clinics that were active throughout the study period, 2014–2019, operated by 141 health systems in 25 states. Because the aim of this study was to assess the chronic health conditions among patients who reach Medicare age eligibility, patient age was restricted to 62–68 years in the study period (three years pre- and post-Medicare age eligibility, n=291,926). Patients included in the analysis had at least one ambulatory visit prior to and after Medicare age eligibility and had insurance type recorded at each visit (n=60,835). Patients with Medicare before age 65 were excluded (excluding n=15,308) as they are medically different from patients who gain Medicare eligibility post-age 65. This resulted in a final analytic sample of 45,527 patients.
Dependent variable
Twenty-two chronic conditions were chosen from the recommended list by the U.S. Department of Health and Human Services Multiple Chronic Conditions framework for operationalizing multimorbidity36,37: anxiety, arthritis, asthma, autism, cancer, cardiac arrhythmia, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), congestive heart failure, coronary artery disease, dementia, depression, diabetes, hepatitis, human immunodeficiency virus (HIV), hyperlipidemia, hypertension, osteoporosis, post-traumatic stress disorder (PTSD), schizophrenia, substance use disorder, and stroke. Chronic conditions were ascertained from EHR problem lists.38 The number of chronic conditions were calculated for both pre- and post-Medicare age eligibility periods. Chronic condition burden was categorized for descriptive purposes as no multimorbidity: 0–1 conditions, low multimorbidity: 2–4 chronic conditions, and high multimorbidity: ≥5 conditions.
Independent variables
Longitudinal insurance patterns were defined as the change or consistency of insurance in pre- and post-Medicare age eligibility periods and consisted of five mutually-exclusive categories: continuously insured throughout the study period (≥75% insured visits pre- and post-periods), continuously uninsured (≥75% uninsured visits pre- and post-periods), gained insurance after age 65 (uninsured or discontinuously insured pre, ≥75% visits insured post-period), lost insurance after age 65 (≥75% of visits insured pre, ≥75% of visits uninsured post-period), and discontinuously insured throughout the study period (<75% insured or uninsured pre and post-periods). We used the ≥75% cut-off to account for any visits happening during a transition time between insurance application and coverage. Insurance types included Medicare, Medicaid, private insurance, and other public insurance.
Patient-level covariates included sex (female or male), a combined self-reported race and ethnicity variable (Non-Hispanic White, Hispanic, Non-Hispanic Black, Other Race, Unknown), percent of the federal poverty level (always <138% following the Medicaid expansion criteria, some or all visits ≥ 138%, never documented), and rurality of patient’s residence (Urban, Rural, Unknown).
Visit-related indicators were determined using Current Procedural Terminology codes and organized by types of ambulatory care visits: preventive visits, mental health visits, Medicare wellness visits, and other ambulatory visits.
Statistical analysis
We summarized patient characteristics overall, and by longitudinal insurance groups with counts and percentages. We calculated unadjusted visit type rates per 100 visits for pre- and post-Medicare age eligibility periods by longitudinal insurance groups. We used difference-in-differences (DID) Poisson generalized estimating equation (GEE) models with an exchangeable correlation structure to account for clustering of patients within primary care clinics and estimate differences in the change of chronic condition rates by insurance groups from pre- to post-Medicare age eligibility. All models included an indicator for pre- vs. post-Medicare age eligibility, insurance group indicators and their interactions. Additionally, all models accounted for covariates listed above. Type 1 error was set to 0.05. Analyses were performed using R version 4.0.1.
RESULTS
In the pre-Medicare age eligibility period, the prevalence of ≥1 chronic condition in our cohort was 92% (n= 41,710); 77% had ≥2 chronic conditions. The prevalence of ≥2 chronic conditions was highest among those who were continuously insured (79%) compared with continuously uninsured (66%) and discontinuously insured (75%) in the pre-period.
Out of 45,527 patients in our cohort, 72% were continuously insured, 14% gained insurance, 5% were discontinuously insured, 2% lost insurance, and 7% were continuously uninsured. Figure 1 shows insurance pattern changes from the pre- to post-Medicare age eligibility periods. Nearly 50% (D path in Figure 1) and 78% (F path in Figure 1) of those who were uninsured or discontinuously insured respectively in the pre-period, gained insurance post-Medicare age eligibility. Among those insured in the pre-Medicare age eligibility period, 5% lost stable insurance (B, H paths in Figure 1). Post-Medicare age eligibility, 14% of patients were either uninsured or discontinuously insured. Few patient characteristics were associated with longitudinal insurance patterns. Patients with Hispanic ethnicity were more likely to be continuously uninsured or lose insurance post-Medicare age eligibility (Table 1). Patients who were continuously uninsured and those who lost health insurance had fewer visits over the study periods than the other insurance patterns.
Figure 1:
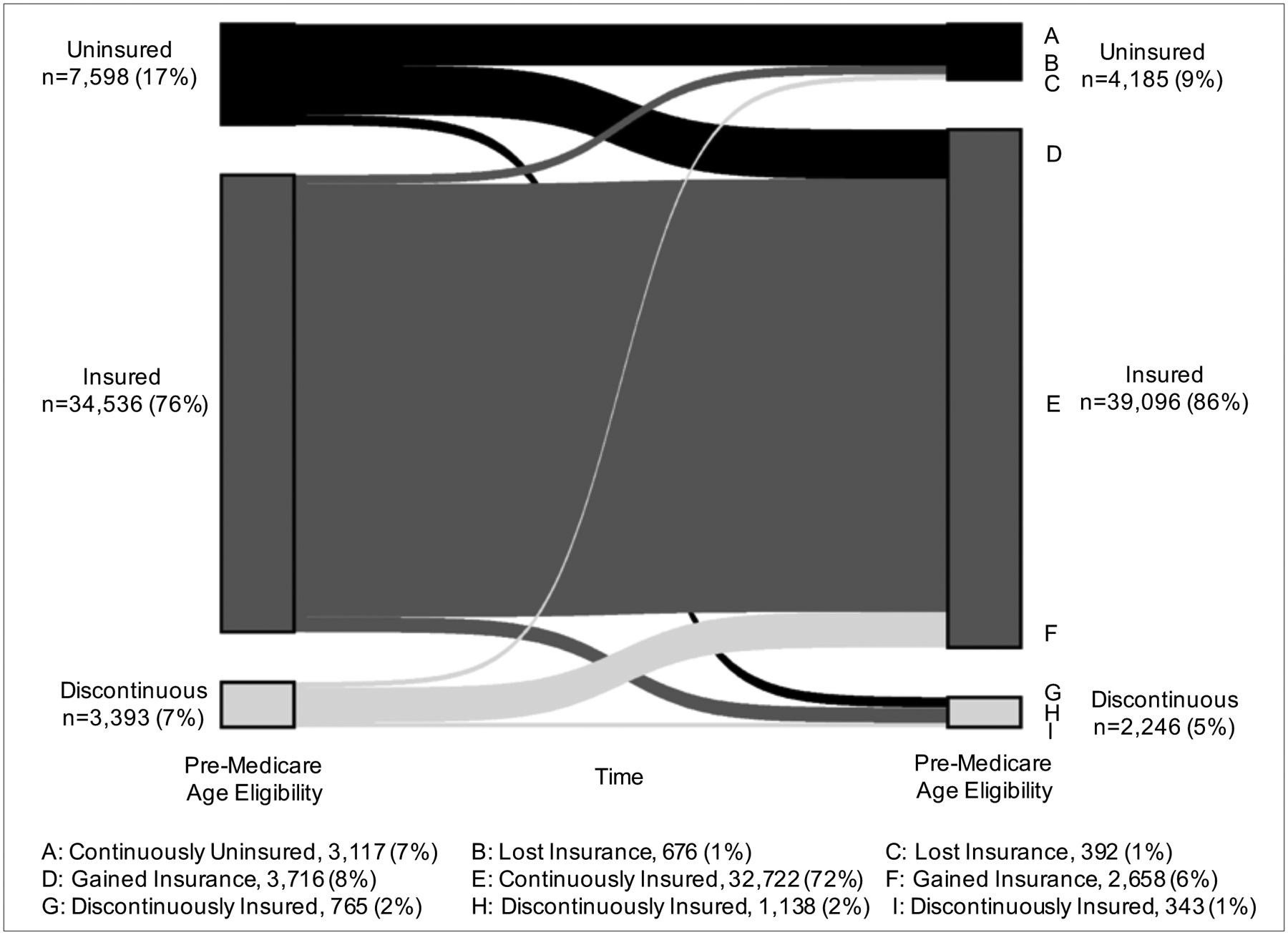
Longitudinal insurance patterns from pre- to post-Medicare age eligibility among 45,527 patients from community health centers
Table 1.
Characteristics of patients by longitudinal insurance patterns, 990 community health centers
| Overall (n= 45527) | Continuously Insured (n=32722) | Continuously Uninsured (n=3117) | Discontinuously Insured (n=2246) | Gained Insurance (n=6374) | Lost Insurance (n=1068) | |
|---|---|---|---|---|---|---|
| Sex, n (%) | ||||||
| Female | 26168 (57.5) | 18758 (57.3) | 1782 (57.2) | 1257 (56.0) | 3786 (59.4) | 585 (54.8) |
| Male | 19359 (42.5) | 13964 (42.7) | 1335 (42.8) | 989 (44.0) | 2588 (40.6) | 483 (45.2) |
| Race and ethnicity, n (%) | ||||||
| Hispanic | 14438 (31.7) | 9658 (29.5) | 1608 (51.6) | 760 (33.8) | 2024 (31.8) | 388 (36.3) |
| Non-Hispanic Black | 7242 (15.9) | 4787 (14.6) | 505 (16.2) | 452 (20.1) | 1314 (20.6) | 184 (17.2) |
| Non-Hispanic White | 18531 (40.7) | 14204 (43.4) | 729 (23.4) | 792 (35.3) | 2463 (38.6) | 343 (32.1) |
| Other | 2809 (6.2) | 2199 (6.7) | 130 (4.2) | 137 (6.1) | 274 (4.3) | 69 (6.5) |
| Unknown | 2507 (5.5) | 1874 (5.7) | 145 (4.7) | 105 (4.7) | 299 (4.7) | 84 (7.9) |
| Federal poverty level, n (%) | ||||||
| Some or all ≥138% | 12851 (28.2) | 9374 (28.6) | 549 (17.6) | 601 (26.8) | 2044 (32.1) | 283 (26.5) |
| Never Documented | 6502 (14.3) | 5620 (17.2) | 274 ( 8.8) | 174 ( 7.7) | 362 (5.7) | 72 (6.7) |
| All <138% | 26174 (57.5) | 17728 (54.2) | 2294 (73.6) | 1471 (65.5) | 3968 (62.3) | 713 (66.8) |
| Geographic location, n (%) | ||||||
| Rural | 4843 (10.6) | 3823 (11.7) | 152 (4.9) | 176 (7.8) | 628 (9.9) | 64 (6.0) |
| Unknown | 2693 (5.9) | 2063 (6.3) | 178 (5.7) | 131 (5.8) | 238 (3.7) | 83 (7.8) |
| Urban | 37991 (83.4) | 26836 (82.0) | 2787 (89.4) | 1939 (86.3) | 5508 (86.4) | 921 (86.2) |
| # visits pre-period, mean (SD) | 3.50 (3.96) | 3.89 (4.36) | 2.36 (2.70) | 4.54 (3.83) | 2.36 (2.37) | 2.14 (2.86) |
| % Preventive visit | 4.4 | 4.6 | 4.1 | 3.7 | 3.4 | 2.4 |
| % Mental health visit | 4.4 | 3.9 | 2.3 | 8.6 | 5.9 | 6.2 |
| % Medicare wellness | 0 | 0 | 0 | 0 | 0 | 0 |
| % Other ambulatory visits | 91.2 | 91.5 | 93.6 | 87.7 | 90.6 | 89.4 |
| # visits post-period, mean (SD) | 9.03 (14.27) | 9.18 (12.86) | 6.52 (23.47) | 10.47 (21.13) | 8.50 (9.11) | 4.93 (10.70) |
| % Preventive visit | 2.7 | 2.5 | 3.4 | 4.2 | 2.5 | 4.4 |
| % Mental health visit | 0.7 | 3.4 | 1.7 | 5.1 | 5.8 | 9.5 |
| % Medicare wellness | 3.7 | 0.8 | 0.5 | 0.0 | 0.5 | 0.1 |
| % Other ambulatory visits | 92.9 | 93.3 | 94.5 | 90.7 | 91.2 | 88.0 |
| ≥2 chronic conditions, n (%) | ||||||
| At Pre-period | 35118 (77.1) | 25944 (79.3) | 2053 (65.9) | 1679 (74.8) | 4716 (74.0) | 726 (68.0) |
| At post-period | 39077 (85.8) | 28543 (87.2) | 2350 (75.4) | 1920 (85.5) | 5474 (85.9) | 790 (74.0) |
Sample included patient aged 62–68 years with at least one visit prior to and after Medicare age eligibility and insurance type recorded for every visit.
Figure 2 illustrates the multimorbidity burden change from pre- to post-period in our cohort. Appendix 1 shows the distribution of patients by number of chronic conditions. The lower numbers of patients with 0–3 chronic conditions in the post-period reflects the number of patients diagnosed with new conditions and thus, moving into higher morbidity levels. More than half of the patients (55%) in our cohort had low levels of multimorbidity (2–4 conditions) and 22% had high multimorbidity burden (≥5 conditions) in the pre-Medicare age eligibility period. Post-Medicare age eligibility, the percentage of patients with a high multimorbidity burden increased from 22 to 33%. Among the 10,409 patients with no multimorbidity in the pre-period, 35% moved to low multimorbidity after reaching Medicare age eligibility.
Figure 2.
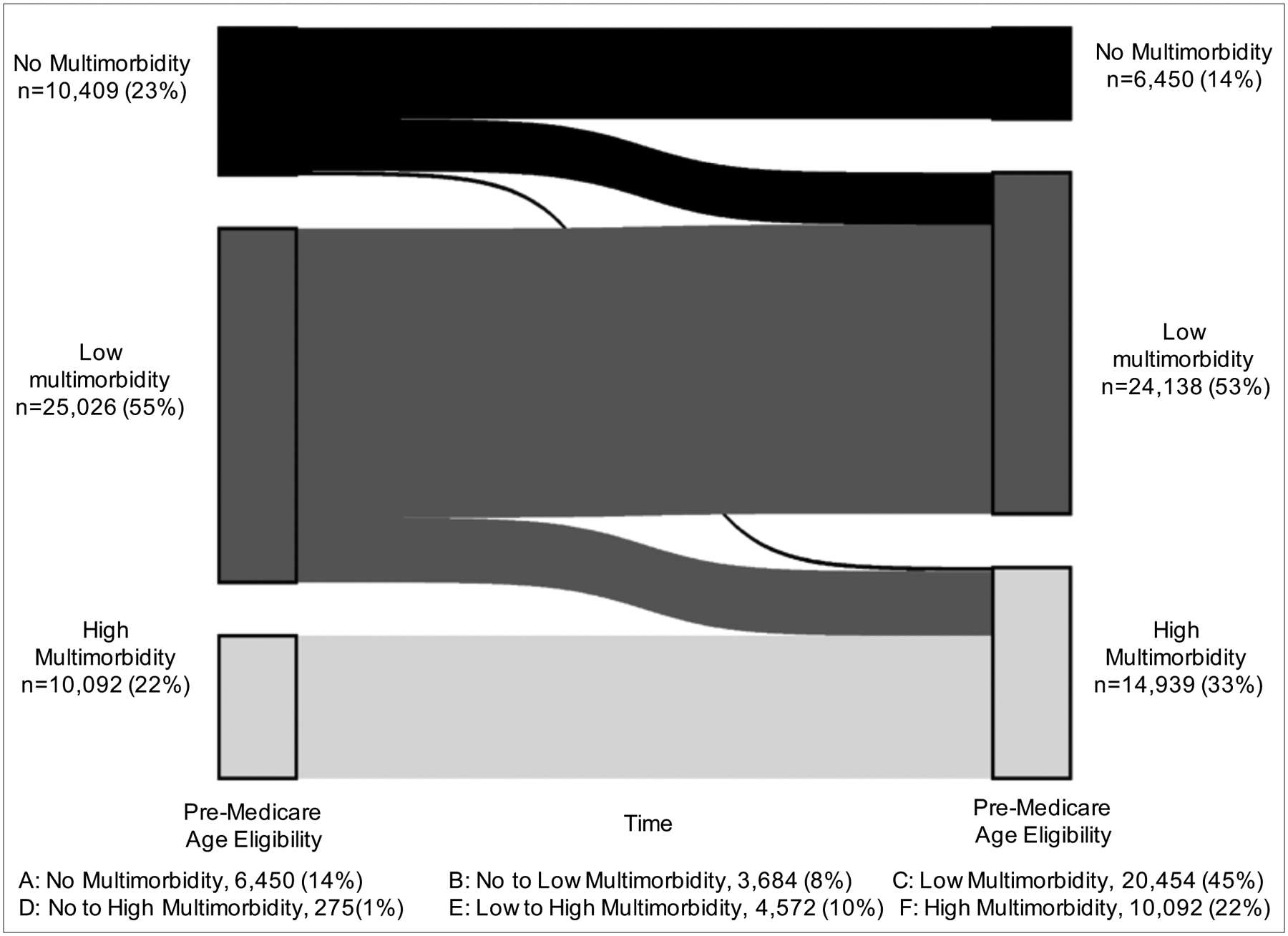
Multimorbidity patterns from pre- to post-Medicare age eligibility among 45,527 patients from community health centers
Note: No multimorbidity: 0–1 conditions, low multimorbidity: 2–4 chronic conditions, and high multimorbidity: ≥5 conditions.
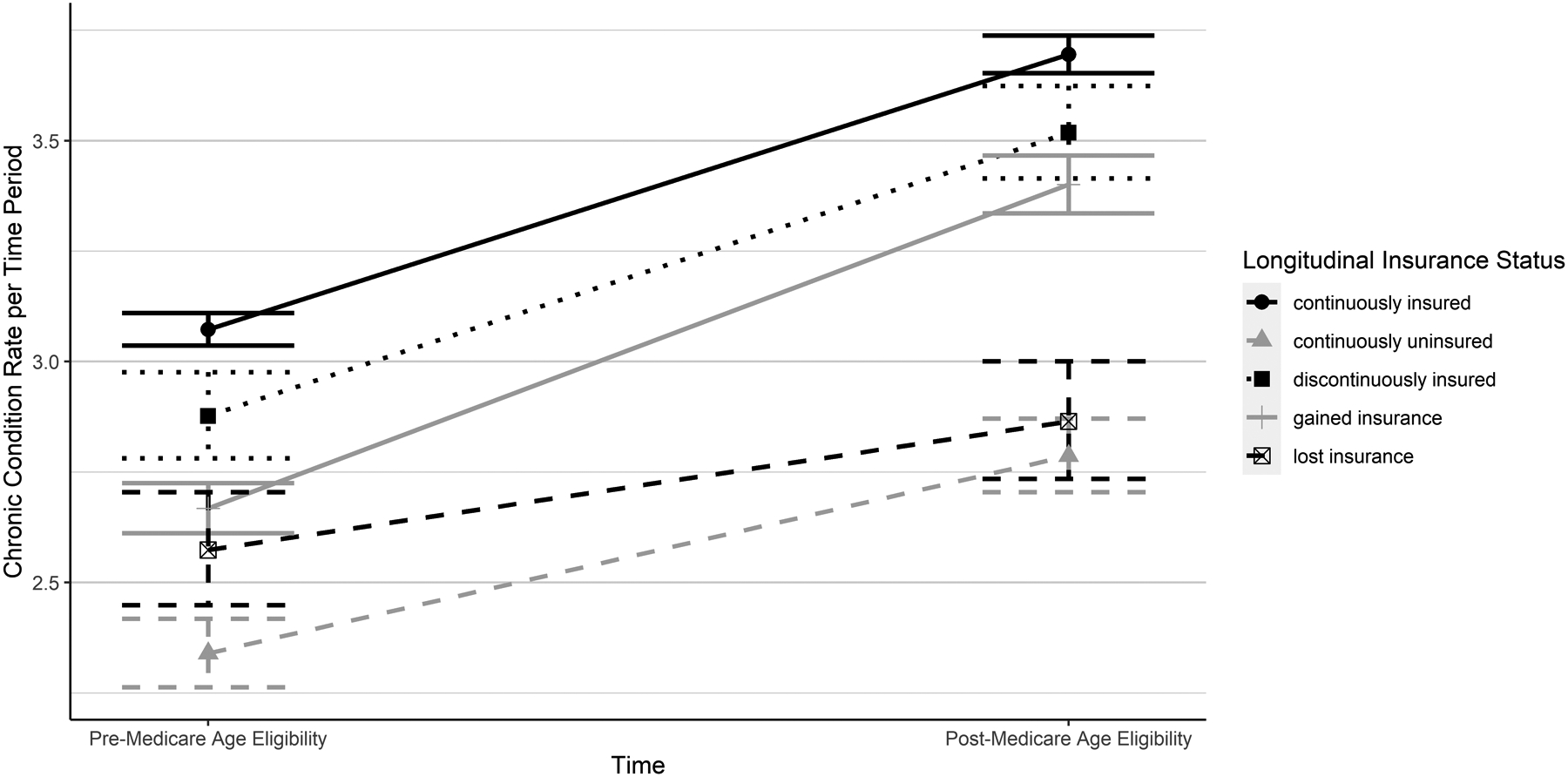
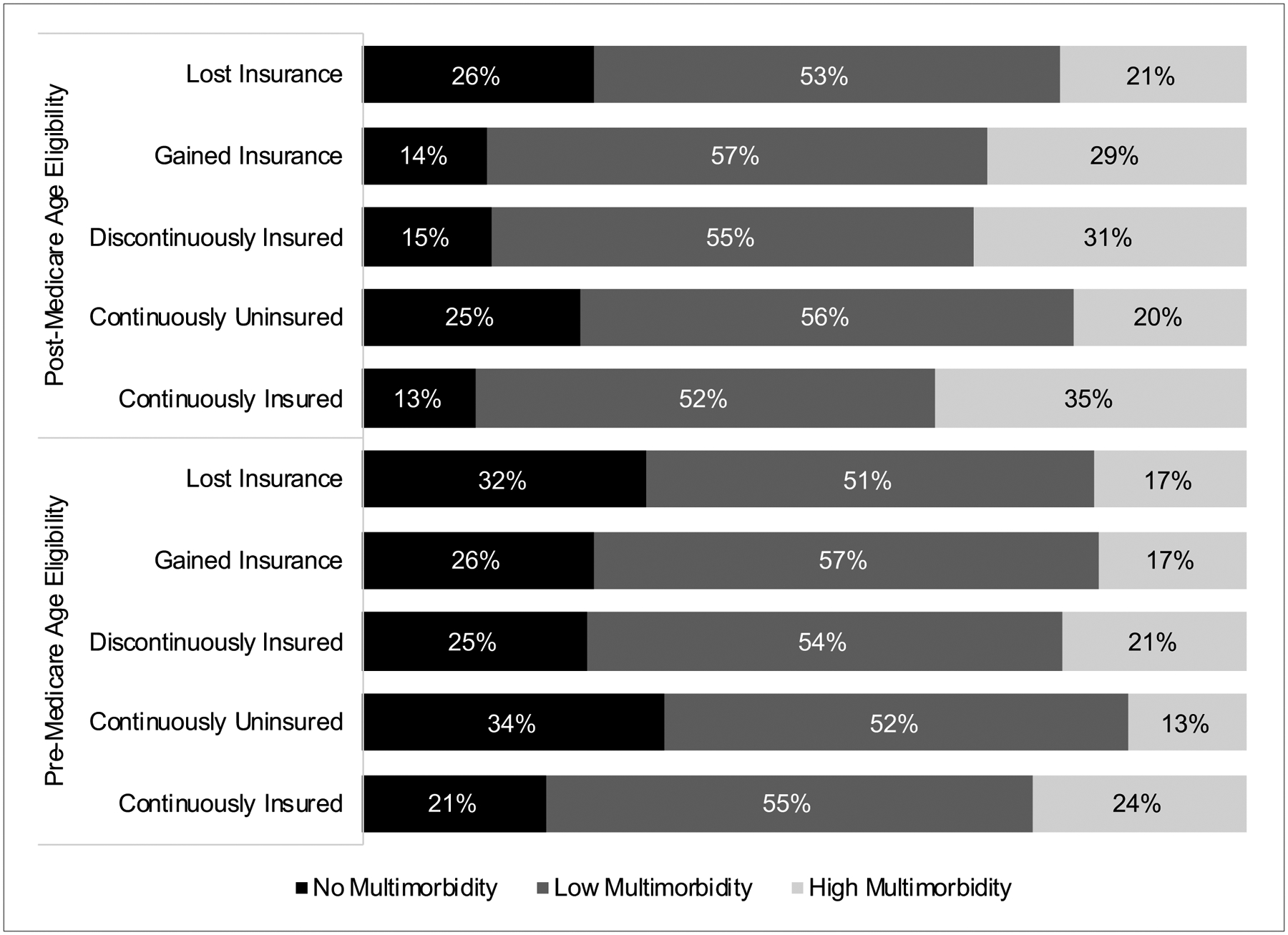
Figure 3 displays multimorbidity burden rates by insurance patterns. Overall, multimorbidity burden increased post-Medicare age eligibility in all insurance groups. The proportion of patients with high multimorbidity burden (≥5 conditions) was highest among patients who were continuously insured (35%). More than half of the patients (52%) who were continuously uninsured had low levels of multimorbidity (2–4 conditions) in the pre-Medicare age eligibility period. Post-Medicare age eligibility, the percentage of patients who gained insurance and had high multimorbidity burden increased from 17 to 29% percent. Results from GEE regression modeling suggest the adjusted rates of chronic conditions increased for all insurance groups (Figure 4) after reaching Medicare age eligibility. Those who gained insurance had the largest increase in the rate of chronic conditions. As seen in Table 2, compared with those who were continuously insured, those who gained insurance had a greater increase in chronic condition rates from pre- to post-period (DID:1.06, 95%CI:1.05–1.07). Those who lost insurance had a smaller increase in chronic condition rates between pre- and post-Medicare age eligibility compared to those continuously insured (DID:0.93, 95%CI:0.91–0.94).
Figure 3.
Multimorbidity patterns from pre- to post-Medicare age eligibility by longitudinal insurance patterns among 45,527 patients from community health centers
Note: No multimorbidity: 0–1 conditions, low multimorbidity: 2–4 chronic conditions, and high multimorbidity: ≥5 conditions.
Figure 4.
Change in rates of chronic conditions per patient from pre-to post-Medicare age eligibility by insurance patterns among 45,527 patients from community health centers
Note: Rates per time period were estimated using a Poisson GEE model with an exchangeable correlation structure clustered on primary clinic adjusted for sex, race and ethnicity, federal poverty level, and geographic location. Error bars represent 95% confidence intervals.
Table 2.
Covariate-adjusted changes in the relative rate of chronic conditions pre- versus post-Medicare age eligibility by longitudinal insurance patterns
| Adjusted Rate Ratio (95% CI) |
|
|---|---|
| Time | |
| Pre-period | Reference |
| Post-period | 1.20 (1.20,1.21) |
| Longitudinal Insurance Pattern | |
| Continuously Insured | Reference |
| Continuously Uninsured | 0.76 (0.73,0.78) |
| Discontinuously Insured | 0.93 (0.90,0.96) |
| Gained Insurance | 0.88 (0.84,0.88) |
| Lost Insurance | 0.82 (0.79,0.87) |
| Time and Longitudinal Insurance Pattern Interaction terms | |
| Post-Period*Continuously Uninsured | 0.99 (0.98,1.01) |
| Post-Period*Discontinuously Insured | 1.02 (1.00,1.03) |
| Post-Period*Gained Insurance | 1.06 (1.05,1.07) |
| Post-Period*Lost Insurance | 0.93 (0.91,0.94) |
Bolded estimates were significant at p<.05. Adjusted rates were computed using Poisson GEE models with an exchangeable correlation structure clustered on primary clinic. Estimates adjusted for sex, race and ethnicity, federal poverty level, and geographic location.
DISCUSSION
The vast majority of older adults receiving care in CHCs have at least one chronic condition and 77% had two or more. After reaching Medicare age eligibility, a sizeable percentage of patients had high multimorbidity burden documented in the EHR, increasing by 48%. Previous studies demonstrate that the most common patterns of multimorbidity in this population include metabolic and cardiovascular diseases (e.g., diabetes, hypertension, and hyperlipidemia);29 conditions requiring daily management and frequent monitoring to reduce the risk of complications. Our results showed increases in the number of overall visits post-Medicare age eligibility for all insurance groups, yet preventive visits declined for most groups. This decline may be attributed to changes in coverage for some preventive services or incomplete reporting. For example, some preventive care services for patients aged 65 and older (CPT 99381–99387) are not covered by Medicare and would incur out-of-pocket expenditures for patients.39 Additionally, only a limited number of immunizations delivered by a physician can be reimbursed by Medicare. Moreover, some preventive services may have been delivered through Medicare Annual Wellness Visits and not recorded with preventive service CPT codes. Future research is needed to understand what types of visits are increasing (e.g., to address more acute problems), which preventive services may be missed, and what strategies could be developed to promote access to preventive care (e.g., outreach, mobile clinics, availability of telehealth).
Our findings also showed that gaining insurance was associated with an increased rate of chronic condition diagnoses. This finding suggests that patients likely lived with the (undetected) conditions prior to Medicare eligibility and were diagnosed after age 65. Undetected conditions can be associated with higher risk for avoidable complications, later stage diagnosis, and poorer health outcomes which can lead to increased care needs, avoidable hospitalizations, and burdensome treatment costs.40 Though this increase in conditions is relatively small, the rate of chronic conditions for this subgroup who gained insurance is similar to that of the highest multimorbidity-burdened group observed in the Health and Retirement Study.41 Previous studies have demonstrated increases in chronic condition diagnoses after patients gain Medicaid insurance, especially among socioeconomically disadvantaged patient populations, stemming from greater access to and contact with the healthcare system.15,26,42 Health care insurance is key to lessening the financial burden associated with receiving care. Regular contact with medical providers facilitates diagnosis of previously undetected conditions, access to medications, enables the provision of chronic disease management and can reduce use of avoidable health care services.
Yet despite reaching Medicare age eligibility, 28% of socioeconomically disadvantaged patients had unstable or no insurance in older age. As noted previously, barriers to insurance coverage in older age include Medicare eligibility and out-of-pocket expenditures. Patients who continued to be uninsured or lost insurance were more likely to be Hispanic. Previous studies have noted challenges Hispanic patients face accessing public insurance programs (e.g., Medicaid, Medicare) which is restricted for some immigrant populations.43,44 Lack of health insurance in older age is particularly concerning as burden of disease, chronic complications, and need for chronic disease management increases with age. The consequences for inadequate management of chronic health issues could result in costly hospital stays and avoidable health care services. Understanding the barriers to insurance access and, importantly, the barriers to continuous insurance coverage in this population are needed to develop strategies, policies, and programs that keep socioeconomically disadvantaged older adults out of hospital emergency departments. This is particularly important for CHCs who care for a large proportion of uninsured patients. CHCs offer many services (behavioral health, dental and vision care, pharmacy services) that could greatly benefit aging CHC patients with increasing need for these services. Supporting the integration of geriatric-focused care into CHCs may be essential to preventing and treating chronic health problems and promoting independent living, especially considering the population of CHC patients aged 65 and older has increased 120% since 2010.30
This study has several limitations. First, this analysis is contingent on access to clinical services and does not assess the CHC patient population who did not have any clinical visits during the study period. As a result, changes in chronic disease burden and insurance status may be underestimated. Second, we relied on problem lists for chronic disease ascertainment in EHR data. While problem list completeness is heterogeneous across clinical practices and health care systems, prior work found problem lists were adequately complete and problem list-ascertained diagnoses were highly concordant with encounter-ascertained diagnoses in our CHC data.45 Specifically, most conditions were reflected in both data sources (59%), 12% were only in encounter diagnosis, and 28% were only recorded on the problem list.45 Our multivariate analysis adjusted for patient panel differences, yet unmeasured confounders could affect our results such as clinic outreach efforts. Finally, we assessed loss to follow-up after Medicare age eligibility, following established methodology46 and found that 59% of patients aged 62–64 years (N=253,835) did not have a follow-up visit within 3 years of turning age 65. The proportion of patients with no multimorbidity burden was higher among those lost to follow-up (32%) than among those with follow-up visits (23%). We cannot determine whether lost to follow-up is attributed to receiving care outside of CHCs, not seeking care within a 3-year period, or death.
Conclusion
The vast majority of older adults receiving care in CHCs have multiple chronic conditions. Following Medicare age eligibility, a significant proportion of patients were diagnosed with new chronic conditions leading to high burden of disease. Over half of the patients with inadequate health care coverage prior to Medicare age eligibility, gained stable insurance via Medicare. However, more than 1 in 4 older adults receiving care in CHCs continue to have inadequate health care coverage as they age. Greater policy efforts targeting access to care and prevention of chronic diseases are needed to support this aging population and the clinics that serve them to promote adequate chronic disease management across the lifespan.
Supplementary Material
Acknowledgement:
This work was conducted with data from the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is a CRN in PCORnet®, the National Patient Centered Clinical Research Network. ADVANCE is led by OCHIN in partnership with Health Choice Network, Fenway Health, and Oregon Health & Science University. ADVANCE’s participation in PCORnet® is funded through the Patient-Centered Outcomes Research Institute (PCORI), contract number RI-OCHIN-01-MC.
Funding:
This study was supported by the National Institute on Aging of the National Institutes of Health award (R01AG061386 to ARQ). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Abbreviation:
- ADVANCE
Accelerating Data Value Across a National Community Health Center Network
- CHCs
community health centers
- CKD
chronic kidney disease
- COPD
chronic obstructive pulmonary disease
- CRN
clinical research network
- DID
difference-in-differences
- EHR
Electronic health record
- GEE
generalized estimating equation
- HIV
human immunodeficiency virus
- PTSD
post-traumatic stress disorder
Footnotes
Conflict of interest statement: None of the authors have conflict of interest.
Data Availability:
Raw data underlying this article were generated from multiple health systems across institutions in the ADVANCE Network; restrictions apply to the availability and re-release of data under organizational agreements.
REFERENCES
- 1.National Center for Health Statistics. Health, United States, 2016: With Chartbook on Long-term Trends in Health. 2017. [PubMed]
- 2.Federal Interagency Forum on Aging-Related Statistics. Older Americans: Key Indicators of Well-Being. Accessed September 11, 2017. https://agingstats.gov/docs/LatestReport/Older-Americans-2016-Key-Indicators-of-WellBeing.pdf
- 3.Ginde AA, Lowe RA, Wiler JL. Health insurance status change and emergency department use among US adults. Arch Intern Med. Apr 23 2012;172(8):642–7. doi: 10.1001/archinternmed.2012.34 [DOI] [PubMed] [Google Scholar]
- 4.Banerjee R, Ziegenfuss JY, Shah ND. Impact of discontinuity in health insurance on resource utilization. BMC Health Serv Res. Jul 6 2010;10:195. doi: 10.1186/1472-6963-10-195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Halterman JS, Montes G, Shone LP, Szilagyi PG. The impact of health insurance gaps on access to care among children with asthma in the United States. Ambul Pediatr. Jan-Feb 2008;8(1):43–9. doi: 10.1016/j.ambp.2007.10.005 [DOI] [PubMed] [Google Scholar]
- 6.Olson LM, Tang SF, Newacheck PW. Children in the United States with discontinuous health insurance coverage. N Engl J Med. Jul 28 2005;353(4):382–91. doi: 10.1056/NEJMsa043878 [DOI] [PubMed] [Google Scholar]
- 7.Bednarek HL, Schone BS. Variation in preventive service use among the insured and uninsured: does length of time without coverage matter? J Health Care Poor Underserved. Aug 2003;14(3):403–19. [DOI] [PubMed] [Google Scholar]
- 8.Broyles RW, Narine L, Brandt EN Jr. The temporarily and chronically uninsured: does their use of primary care differ? J Health Care Poor Underserved. Feb 2002;13(1):95–111. [DOI] [PubMed] [Google Scholar]
- 9.Gold R, DeVoe J, Shah A, Chauvie S. Insurance continuity and receipt of diabetes preventive care in a network of federally qualified health centers. Med Care. Apr 2009;47(4):431–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Collins SR, Rasmussen PW, Beutel S, Doty MM. The problem of underinsurance and how rising deductibles will make it worse. Findings from the Commonwealth Fund Biennial Health Insurance Survey, 2014. Issue Brief (Commonw Fund). May 2015;13:1–20. [PubMed] [Google Scholar]
- 11.Lavarreda SA, Brown ER, Bolduc CD. Underinsurance in the United States: an interaction of costs to consumers, benefit design, and access to care. Annu Rev Public Health. 2011;32:471–82. doi: 10.1146/annurev.publhealth.012809.103655 [DOI] [PubMed] [Google Scholar]
- 12.Voorhees K, Fernald DH, Emsermann C, et al. Underinsurance in primary care: a report from the State Networks of Colorado Ambulatory Practices and Partners (SNOCAP). J Am Board Fam Med. Jul-Aug 2008;21(4):309–16. doi: 10.3122/jabfm.2008.04.080001 [DOI] [PubMed] [Google Scholar]
- 13.Magge H, Cabral HJ, Kazis LE, Sommers BD. Prevalence and predictors of underinsurance among low-income adults. J Gen Intern Med. Sep 2013;28(9):1136–42. doi: 10.1007/s11606-013-2354-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cardinali G, Rhyne RL, Fleg A, et al. Underinsurance before the implementation of the Affordable Care Act: From the Research Involving Outpatient Settings Network (RIOS Net). J Am Board Fam Med. Nov-Dec 2014;27(6):855–7. doi: 10.3122/jabfm.2014.06.140033 [DOI] [PubMed] [Google Scholar]
- 15.Huguet N, Angier H, Hoopes MJ, et al. Prevalence of Pre-existing Conditions Among Community Health Center Patients Before and After the Affordable Care Act. J Am Board Fam Med. Nov-Dec 2019;32(6):883–889. doi: 10.3122/jabfm.2019.06.190087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jerant A, Fiscella K, Tancredi DJ, Franks P. Health insurance is associated with preventive care but not personal health behaviors. J Am Board Fam Med. Nov-Dec 2013;26(6):759–67. doi: 10.3122/jabfm.2013.06.130054 [DOI] [PubMed] [Google Scholar]
- 17.Wharam JF, Lu CY, Zhang F, et al. High-Deductible Insurance and Delay in Care for the Macrovascular Complications of Diabetes. Ann Intern Med. Dec 18 2018;169(12):845–854. doi: 10.7326/M17-3365 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang JX, Huang ES, Drum ML, et al. Insurance status and quality of diabetes care in community health centers. Am J Public Health. Apr 2009;99(4):742–7. doi: 10.2105/AJPH.2007.125534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Marino M, Bailey SR, Gold R, et al. Receipt of Preventive Services After Oregon’s Randomized Medicaid Experiment. Am J Prev Med. Feb 2016;50(2):161–70. doi: 10.1016/j.amepre.2015.07.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.McWilliams JM, Zaslavsky AM, Meara E, Ayanian JZ. Impact of Medicare coverage on basic clinical services for previously uninsured adults. JAMA : the journal of the American Medical Association. Aug 13 2003;290(6):757–64. doi: 10.1001/jama.290.6.757 [DOI] [PubMed] [Google Scholar]
- 21.Busch SH, Duchovny N. Family coverage expansions: Impact on insurance coverage and health care utilization of parents. Journal of Health Economics. 2005;24(5):876–890. doi: 10.1016/j.jhealeco.2005.03.007 [DOI] [PubMed] [Google Scholar]
- 22.Hatch B, Bailey SR, Cowburn S, Marino M, Angier H, DeVoe JE. Community Health Center Utilization Following the 2008 Medicaid Expansion in Oregon: Implications for the Affordable Care Act. Am J Public Health. Apr 2016;106(4):645–50. doi: 10.2105/AJPH.2016.303060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Johnson RW, Crystal S. Uninsured status and out-of-pocket costs at midlife. Health Serv Res. Dec 2000;35(5 Pt 1):911–32. [PMC free article] [PubMed] [Google Scholar]
- 24.Meer J, Rosen HS. Insurance and the utilization of medical services. Soc Sci Med. May 2004;58(9):1623–32. doi: 10.1016/S0277-9536(03)00394-0 [DOI] [PubMed] [Google Scholar]
- 25.McWilliams JM, Meara E, Zaslavsky AM, Ayanian JZ. Use of health services by previously uninsured Medicare beneficiaries. N Engl J Med. Jul 12 2007;357(2):143–53. doi: 10.1056/NEJMsa067712 [DOI] [PubMed] [Google Scholar]
- 26.Angier H, Huguet N, Ezekiel-Herrera D, et al. New hypertension and diabetes diagnoses following the Affordable Care Act Medicaid expansion. Fam Med Community Health. Dec 2020;8(4)doi: 10.1136/fmch-2020-000607 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McWilliams JM, Zaslavsky AM, Meara E, Ayanian JZ. Health insurance coverage and mortality among the near-elderly. Health Aff (Millwood). Jul-Aug 2004;23(4):223–33. doi: 10.1377/hlthaff.23.4.223 [DOI] [PubMed] [Google Scholar]
- 28.Brooks EL, Preis SR, Hwang SJ, et al. Health insurance and cardiovascular disease risk factors. Am J Med. Aug 2010;123(8):741–7. doi: 10.1016/j.amjmed.2010.02.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Quinones AR, Valenzuela SH, Huguet N, et al. Prevalent Multimorbidity Combinations Among Middle-Aged and Older Adults Seen in Community Health Centers. J Gen Intern Med. Jan 28 2022;doi: 10.1007/s11606-021-07198-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.National Association of Community Health Centers. Community Health Center Chartbook 2022. 2022. https://www.nachc.org/research-and-data/research-fact-sheets-and-infographics/2021-community-health-center-chartbook/
- 31.Hicks LS, O’Malley AJ, Lieu TA, et al. The quality of chronic disease care in U.S. community health centers. Health Aff (Millwood). Nov-Dec 2006;25(6):1712–23. doi: 10.1377/hlthaff.25.6.1712 [DOI] [PubMed] [Google Scholar]
- 32.Chin MH. Improving care and outcomes of uninsured persons with chronic disease… now. Ann Intern Med. Aug 5 2008;149(3):206–8. doi: 10.7326/0003-4819-149-3-200808050-00012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Centers for Medicare & Medicaid Services. Original Medicare (Part A and B) Eligibility and Enrollment. Accessed May 24, 2023. https://www.cms.gov/Medicare/Eligibility-and-Enrollment/OrigMedicarePartABEligEnrol
- 34.DeVoe JE, Gold R, Cottrell E, et al. The ADVANCE network: accelerating data value across a national community health center network. J Am Med Inform Assoc. Jul-Aug 2014;21(4):591–5. doi: 10.1136/amiajnl-2014-002744 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.OCHIN. A Short guide to the ADVANCE Clinical Research Network. Accessed May 24, 2023. https://advancecollaborative.org/wp-content/uploads/2022/06/Short-Guide-to-the-ADVANCE-CRN-220511.pdf
- 36.Goodman RA, Posner SF, Huang ES, Parekh AK, Koh HK. Defining and measuring chronic conditions: imperatives for research, policy, program, and practice. Prev Chronic Dis. Apr 25 2013;10:E66. doi: 10.5888/pcd10.120239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.US Department of Health and Human Services. A Strategic Framework Optimum Health and Quality of Life for Individuals with Multiple Chronic Conditions. 2010. https://www.hhs.gov/sites/default/files/ash/initiatives/mcc/mcc_framework.pdf
- 38.Wright A, McCoy AB, Hickman TT, et al. Problem list completeness in electronic health records: A multi-site study and assessment of success factors. Int J Med Inform. Oct 2015;84(10):784–90. doi: 10.1016/j.ijmedinf.2015.06.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.AAFP. Medicare Non-covered Services Accessed May 24, 2023. https://www.aafp.org/family-physician/practice-and-career/getting-paid/coding/non-covered-services.html
- 40.Ramondetta LM, Meyer LA, Schmeler KM, et al. Avoidable tragedies: Disparities in healthcare access among medically underserved women diagnosed with cervical cancer. Gynecol Oncol. Dec 2015;139(3):500–5. doi: 10.1016/j.ygyno.2015.10.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Quinones AR, Botoseneanu A, Markwardt S, et al. Racial/ethnic differences in multimorbidity development and chronic disease accumulation for middle-aged adults. PLoS One. 2019;14(6):e0218462. doi: 10.1371/journal.pone.0218462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rosland AM, Kieffer EC, Tipirneni R, et al. Diagnosis and Care of Chronic Health Conditions Among Medicaid Expansion Enrollees: a Mixed-Methods Observational Study. J Gen Intern Med. Nov 2019;34(11):2549–2558. doi: 10.1007/s11606-019-05323-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Huguet N, Valenzuela S, Marino M, et al. Following Uninsured Patients Through Medicaid Expansion: Ambulatory Care Use and Diagnosed Conditions. Ann Fam Med. Jul 2019;17(4):336–344. doi: 10.1370/afm.2385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sohn H. Racial and Ethnic Disparities in Health Insurance Coverage: Dynamics of Gaining and Losing Coverage over the Life-Course. Popul Res Policy Rev. Apr 2017;36(2):181–201. doi: 10.1007/s11113-016-9416-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Voss RW, Schmidt TD, Weiskopf N, et al. Comparing ascertainment of chronic condition status with problem lists versus encounter diagnoses from electronic health records. J Am Med Inform Assoc. Apr 13 2022;29(5):770–778. doi: 10.1093/jamia/ocac016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Huguet N, Kaufmann J, O’Malley J, et al. Using Electronic Health Records in Longitudinal Studies: Estimating Patient Attrition. Med Care. Jun 2020;58 Suppl 6 Suppl 1:S46–S52. doi: 10.1097/MLR.0000000000001298 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Raw data underlying this article were generated from multiple health systems across institutions in the ADVANCE Network; restrictions apply to the availability and re-release of data under organizational agreements.