

Abstract
Background
Lower third molars (L3M) are the last teeth to erupt in the oral cavity. Uneruption of these teeth still raises questions about its causes, in the literature (1) genetic factors, (2) dental lamina activity and, mainly, (3) insufficient growth and development of the bone bases are included. While the lack of space theory influenced by mandibular morphology and size of L3M was argued to be the main reason for L3M impaction, there is a limitation in the literature in examining such association using more accurate tomographic analysis obtained from CBCT. This work aimed to evaluate the relationship between mandibular morphology and the eruption of L3M.
Methods
In this regard, 85 Cone Beam Computed Tomographies (CBCT), with 147 L3M, were selected from the archives of the Department of Surgery, Stomatology, Pathology and Radiology, Bauru School of Dentistry, obtained using an Accuitomo® Morita device and using the Dolphin Imaging 11.9 software. L3M eruption was related to linear measurements of jaw length (Co-Gn), retromolar space dimension (D2R), mesiodistal width of the L3M crowns, mandibular first molars (L1M) and mandibular canines (LC) and the angle mandibular (Ar-Go-Me). Independent samples t-test, chi-square tests and logistic regression were performed adopting a significance level of 5%.
Results
The average mandible length of 116.446 mm + 6.415 mm, retromolar space of 11.634 mm + 2.385 mm, mesiodistal size of the L3M of 10.054 mm + 0.941 mm, sum of the mesiodistal widths of the L1M and LC of 15.564 mm + 1.218 mm and mandibular angle of 127.23° + 6.109. There was no statistically significant association between these factors and the eruption.
Conclusion
With the results obtained in this study, we conclude that the length and angle of the mandible, teeth size and dimension of the retromolar space are not associated with the L3M eruption.
Keywords: Tomography, Third molar, Mandible, Tooth eruption
Introduction
Third molars are the last teeth to erupt in the oral cavity, with the lower teeth having the highest uneruption rate (17–69%) when compared to other teeth [1].
Inadequate space associated with craniofacial development and mandibular morphology are considered the main causes of uneruption [1-3]. However, other theories such as: eruption in the distal direction or lack of eruptive strength, early physical maturity, delayed mineralization and difficulties related to the peculiarities and morphological variations of L3 are also found in the literature [4-6].
The age at which lower third molars erupt may be influenced by racial variation, nature of the diet, degree of use of the masticatory apparatus and genetic inheritance [7]. According to Cortella, Shofer and Ghafari [8] during puberty, the growth of bone bases and structural transformations are evident. At this stage, the growth of the width of the mandible is completed, leaving only sagittal and vertical development [8].
The mechanisms that determine the uneruption of L3M are still obscure [9]. Most researchers claim that it is the result of a lack of space in the mandible, but they disagree about the primary mechanism: mandibular body width, mandibular angle, timing and mandibular growth in relation to eruption or a combination of these factors [9].
The different morphological characteristics of the L3M, irregular size, root dilacerations and variable position in the mandible, are also associated in the literature with the high rate of uneruption of these teeth [6]. According to Hattab [10] and Vranckx et al. [11] severely angulated third molars have a minimal chance of future eruption and a greater risk of developing a relationship with the mandibular canal, even with adequate retromolar space.
Clinically, the uneruption of the teeth can generate painful symptoms, pericoronitis, trismus, resorptions and periodontal problems in the second molars [12]. To avoid these situations, the evaluation of the dental surgeon is fundamental in indicating the surgical removal of the L3M [12].
Most of the research addressing uneruption of L3M has been carried out using 2D imaging exams, such as panoramic radiography [13, 14]. However, with CBCT it is possible to perform evaluations of the region of interest in the three planes of space, promoting greater accuracy of measurements [15].
In our search in the scientific literature, no studies were found associating various aspects of mandibular morphology and the size of the teeth with the eruption of the L3M in detail, using computed tomography. Therefore, the aim of this work is to analyze the relationship between mandibular morphology and tomographic L3M eruption, using CBCT and Dolphin Imaging software.
Materials & methods
Sample size calculation
Based on the proportion of erupted and unerupted teeth found in the literature and in the pilot study, a sample calculation was carried out according to Peduzzi et al. [16] and Hsieh [17] with the aid of an online sample size calculator (available at: http://estatistica.bauru.usp.br/calculoamostral/ta_diferenca_media_independente.php).
The calculation to define the sample required for the multiple logistic regression analysis was carried out considering the number of independent variables [5] and and the lowest expected proportion (35% erupted). The required sample size was 143.
For the independent samples t-test, the highest standard deviation among the variables analyzed was considered to be 0.89 (Co-Gn), resulting in a necessary N of 51.
Materials
This retrospective study was carried out with CBCT performed between 2015 and 2018 selected from the archives of Radiology Clinic of Bauru School of Dentistry, University of São Paulo, after approval by the Research Ethics Committee, from the same institution. Images were taken with Accuitomo® 170 3D tomograph (J. Morita, United States of America) with FOV (Field of View) of 170 × 120 cm, 80 kVp, 2mAs, acquisition time of 40 seconds and voxel of 80 μm.
The study included patients over 17 years of age, with at least L3M erupted or not and L2M, L1M, LC and lower central incisor (LCI), with intact crowns on the same side of the mandible.
Patients with alterations in the mandible, such as cysts and tumors, fractures, cleft lip and palate, and those whose CT scans had distortions and did not show the complete condyles and chin were excluded.
The studied variables were mandible length, mandibular angle, retromolar space size and teeth size. These measurements were obtained from the sagittal reformats of the Dolphing Imaging software version 11.9.
Methods
To measure the effective length of the mandible (Co-Gn), the distance between the cephalometric points was used, demarcating the condyle (Co) corresponding to the most superior and posterior point of the mandibular condyle until the Gnatium (Gn) being the lowest point and anterior of the mandible according with Mc Namara Jr [18] (Fig. 1).
Fig. 1.

Effective mandible length with Co-Gn points
Then, a sagittal reformat was created in order to pass through the LC, L1M and L3M to measure the size of the teeth corresponding to the mesiodistal width at the level of the prosthetic equator. For each tooth, the most mesial point and the most distal point was marked, on the prosthetic equator being for the canine MC-DC, for the L1M corresponding to the points M1-D1 and for the L3M the points M3-D3 (Fig. 2).
Fig. 2.

Size of teeth A) Measurement of lower first molars (L1M) and canines (LC), B) Measurement of lower third molars (L3M)
It is noteworthy that, in 62 CBCT that had bilateral L3M, the measurements were taken with the points positioned to each side (right and left). For the other 23 CBCT, with unilateral L3M, only the side of interest was measured.
To determine the eruption or not of the L3M, the L3M whose occlusal face was at the same level as the occlusal face of the L2M, that is, in a vertical position, were considered erupted. Other situations were classified as unerupted.
As for the retromolar space size (D2-R), the D2 point corresponding to the most distal point of the cementoenamel junction of the L2M was demarcated and the R point determined by the crossing of the occlusal plane, formed by the straight line that passes through the higher point of the LC and L2M cusps, with the anterior edge of the mandibular ramus. Thus, the retromolar space (D2-R) was measured by the distance from point D2 to point R (Fig. 3).
Fig. 3.

Measurement of retromolar space (D2-R)
For the mandible angle, the following points were marked: Articulare (Ar), Gonio (Go) and Menton (Me), according with Rodriguez-Cardenas et al. [19], Naqvi [20] and Zhang et al. [21]. The software automatically traces the angle according to the Jarabak analysis (Fig. 4).
Fig. 4.

Marking the points of interest in sagittal reformatting: Ar-Go-Me and the gonial angle measurement provided by the software
Statistical analysis
Initially, measurements performed in 30 CBCT, repeated with an interval of 15 days, were used to calculate method error and intra-examiner confidence and sample calculation.
Independent samples t-test, chi-square tests and logistic regression tests were performed,the dependent variable was the eruption of L3M and the independent variables were gender, mandibular length, retromolar space and tooth size. In all tests, a significance level of 5% was developed to analyze differences between variables.
All tests were performed with the SPSS V20 program (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) e Minitab 16 (Minitab 16 Statistical Software 2010. Computer software. State College, PA: Minitab, Inc.).
Results
Sample description
Following the inclusion criteria, 85 CBCT were evaluated, with 147 hemi-mandibles with L3M (Fig. 5), with a mean age of 22.35 years, ranging between 17 and 32 years. More than half of the sample (53.1%) was composed of male patients and 46.9% of female patients.
Fig. 5.
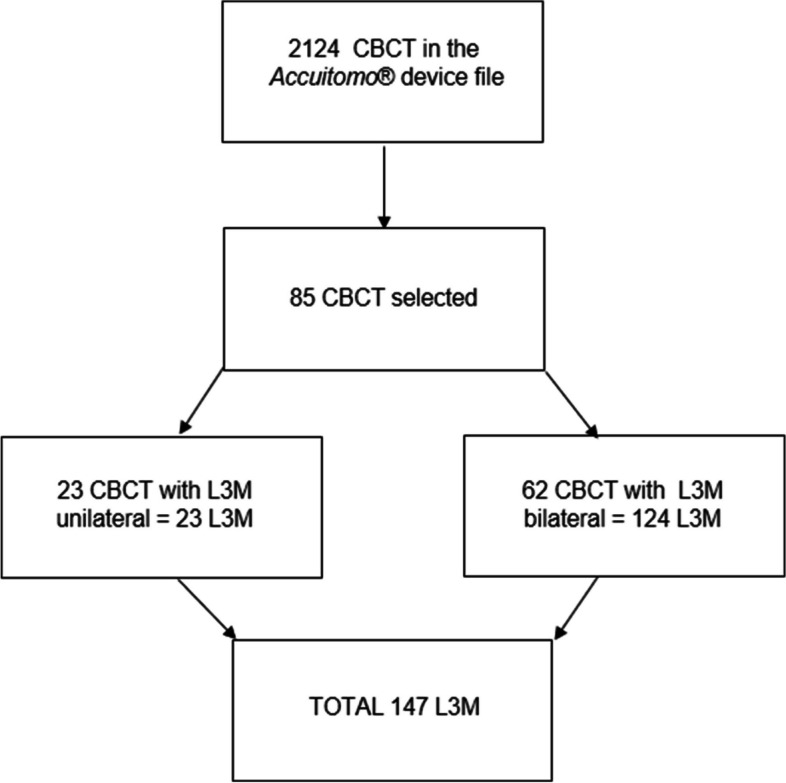
CBCT selection flowchart
Relationship between the variables and the outbreak of L3M
Using the Chi-square test, we sought to identify whether there is a relationship between gender and the eruption rate, however, p = 0.33 indicated that there was no statistically significant difference.
The results of the measurements taken, considering erupted and unerupted teeth, are shown in Table 1. The T-test performed shows the relationship between these measurements and the eruption of the L3M.
Table 1.
Mean and standard deviation of linear measurements and relation to L3M eruption
| Erupted L3M | Unerupted L3M | p value | ||
|---|---|---|---|---|
| Age | N | 55 | 92 | |
| Mean | 23.530 | 21.650 | 0.007* | |
| SD | 0.572 | 0.403 | ||
| Co-Gn (mm) | N | 55 | 92 | |
| Mean | 115.973 | 116.728 | 0.490* | |
| SD | 0.891 | 0.659 | ||
| LC (mm) | N | 55 | 92 | |
| Mean | 6.047 | 6.146 | 0.430* | |
| SD | 0.099 | 0.075 | ||
| L1M (mm) | N | 55 | 92 | |
| Mean | 9.371 | 9.505 | 0.310* | |
| SD | 0.098 | 0.083 | ||
| LC + L1M (mm) | N | 55 | 92 | |
| Mean | 15.418 | 15.651 | 0.263* | |
| SD | 0.153 | 0.131 | ||
| L3M (mm) | N | 55 | 92 | |
| Mean | 10.013 | 10.079 | 0.679* | |
| SD | 0.138 | 0.092 | ||
| D2-R (mm) | N | 55 | 92 | |
| Mean | 1.847 | 1.419 | 0.333* | |
| SD | 0.363 | 0.262 | ||
| Ar-Go-Me | N | 14 | 35 | |
| Mean | 127.800 | 126.900 | 0.628* | |
| SD | 1.932 | 0.919 | ||
*Independent samples t-test
Furthermore, multiple logistic regression analysis was performed having eruption as dependent variable and gender, Co-Gn distances, D2-R, L3M and teeth size as independent variables, but no statistically significant result was obtained in any of the variables (Table 2). The odds ratio was calculated taking uneruption as a reference and the reference used for the variable gender was female.
Table 2.
Multiple logistic regression analysis in relation to the eruption of the L3M
| Independent variables | Wald | p | ORa | CI 95%b |
|---|---|---|---|---|
| Gender (M/F) | 0.254 | 0.614 | 0.82 | 0.37–1.78 |
| Co-Gn | 2.312 | 0.128 | 0.94 | 0.85–1.02 |
| D2-R | 2.007 | 0.157 | 1.12 | 0.95–1.29 |
| L3M width | 0.029 | 0.865 | 0.97 | 0.64–1.44 |
| LC + L1M | 0.524 | 0.469 | 0.89 | 0.64–1.22 |
| Constant | 0.020 | 0.889 | 1.72 |
aOR odds ratio
bCI95 95% confidence interval
For the analysis of the relationship between the angle of the mandible and the eruption of the lower third molars, 51 hemi-mandibles were evaluated. When relating the mandibular angle with the eruption of the L3M, it was possible to observe that the difference is not statistically significant (Table 1).
The result obtained in the logistic regression having eruption as a dependent variable and the mandibular angle as an independent variable, also confirms that the difference is not statistically significant (p = 0.97).
Discussion
The present study was carried out to evaluate the relationship between mandibular morphology and L3M eruption using CBCT and Dolphin Imaging software. The results indicated that the mandibular morphology and the size of the teeth are not associated with the eruption of L3M.
L3M usually erupt between ages 17 and 26, varying considerably between populations and according to gender [7, 22]. In this study, the mean age found was 22 years. The results obtained showed that age is associated with the eruption of L3M, which was expected. Since it influences the process of odontogenesis and consequently the eruption of teeth.
Because they are the last molars to erupt, lack of space is often the justification for these teeth not erupting [22].
Regarding the effective length of the mandible measured in this work by the distance between the point Co and Gn, it was described in the literature by Mc Namara Jr [18]. Used in recent studies such as the one by Santos et al. [8] which standardized the measurements of the dimensions of the maxillomandibular complex in Brazilians, being found for the average of 114.51 mm when combined both genders. These values corroborate those of this study, with an average mandibular length of 116.446 mm. Different from the results of Olayemi [23], who calculated the mandibular length of the Nigerian population with the same reference points, but found higher values. As these are different countries, the ethnicity of the population becomes a determining factor to explain these differences found.
Olayemi [23] also sought to analyze whether the size of other teeth in the arch influences the L3M eruption rate. However, like this study, the size of the teeth did not influence the eruption of the L3M.
To evaluate the relationship between the L3M size and the eruption index, its mesiodistal length was measured separately. However, the mean size obtained for erupted and unerupted L3M was similar.
The lack of space between the second permanent molar and the mandibular ramus was identified as an important factor in the etiology of uneruption of the L3M [24]. In the study by Aliaga-Del Castillo et al. [25], the size of the retromolar space, measured in the most posterior region of the mandible, was presented as a determining factor in the eruption or not of the L3M. In this study, contrary to expectations, the retromolar space did not influence the L3M eruption.
Begtrup et al. [26] sought to relate, through panoramic radiographs, the size and mandibular angle with the rate of eruption of the L3M, according to the authors, the longer the mandible, the greater the chance of eruption of these teeth, however, no relationship was found with the mandibular angle. The results obtained in this study with CBCT indicated that both the mandibular length and the mandibular angle did not affect the eruption of the L3M.
One of the hypotheses would be that the mandibular angle would interfere with the L3M eruption, as the result of Al-Gunaid et al. [27], but in this study the average between the mandibular angle in erupted and unerupted teeth was similar, contradicting this hypothesis.
The study by de Mayama et al. [28] corroborates the findings of this research, in which the average value of the mandibular angle found for patients without skeletal alterations or congenital absence of teeth was 127.8°.
As we can see, the vast majority of studies on the subject were performed with panoramic radiographs and have divergent results in the literature. Panoramic radiography is a two-dimensional image that has distortions inherent to image formation [29, 30]. However, several studies show that the three-dimensional image is more accurate, reliable and ensures surgical planning with greater predictability [29-33].
A limitation of the study is a relatively small sample, this was because all CT scans were performed in a single center. This study showed that mandibular morphology and tooth size are not determinant in the eruption of L3M.However, future studies must be carried out to try to determine other factors that may influence this process.
Conclusion
With the results obtained in this study, we conclude that the length and angle of the mandible, teeth size and dimension of the retromolar space are not associated with the L3M eruption.
Acknowledgements
Not applicable.
Abbreviations
- Ar
Articulare
- CBCT
Cone Beam Computed Tomographies
- CI
Confidence interval
- Co
Condyle
- CT
Computed tomography
- DC
Canine distal
- D1
First molar distal
- D3
Third molar distal
- D2R
Retromolar space dimension
- FOV
Field of View
- Go
Gonion
- Gn
Gnatium
- kVp
Kilovoltage to Peak Power
- L1M
Lower first molars
- L2M
Lower second molar
- L3M
Lower third molar
- LC
Lower canine
- LCI
Lower central incisor
- mAs
Milliampere second
- MC
Canine mesial
- Me
Menton
- mm
Millimeter
- M1
First molar mesial
- M3
Third molar mesial
- N
Number
- OR
Odds ratio
- 2D
Two dimensional
- 3D
Three dimensional
- μm
Micrometer
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JFS and GBB and LLC. The first draft of the manuscript was written by JFS, GBB and OFJ. All authors commented all versions and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
Approved by the Research Ethics Committee of the Dentistry School of Bauru: protocol number 79155917.1.00000.5417.
All stages of the research were carried out after approval of the project by the ethics committee and the personal data and identity of the patients were kept confidential. Because it is an indirect respective study, that is, without direct contact with human beings, consisting only of the analysis of CT scans from the image bank, the ethics committee did not consider necessary the term of free and informed consent for this work.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Muhsin H, Brizuela M. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. Oral surgery, extraction of mandibular third molars. [PubMed] [Google Scholar]
- 2.Barone S, Antonelli A, Averta F, et al. Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study. J Clin Med. 2021;10(18):4057. doi: 10.3390/jcm10184057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Demirel O, Akbulut A. Evaluation of the relationship between gonial angle and impacted mandibular third molar teeth. Anat Sci Int. 2020;95(1):134–142. doi: 10.1007/s12565-019-00507-0. [DOI] [PubMed] [Google Scholar]
- 4.KalaiSelvan S, Ganesh SKN, Natesh P, Moorthy MS, Niazi TM, Babu SS. Prevalence and pattern of impacted mandibular third molar: an institution-based retrospective study. J Pharm Bioallied Sci. 2020;12(Suppl 1):S462–S467. doi: 10.4103/jpbs.JPBS_140_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Adeyemo WL, James O, Oladega AA, et al. Correlation between height and impacted third molars and genetics role in third molar impaction. J Maxillofac Oral Surg. 2021;20(1):149–153. doi: 10.1007/s12663-020-01336-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pithon MM, Baião FCS, LIDA S’A, Silva Coqueiro R, Maia LC. Influence of the presence, congenital absence, or prior removal of third molars on recurrence of mandibular incisor crowding after orthodontic treatment: systematic review and meta-analysis. J World Fed Orthod. 2017. 10.1016/j.ejwf.2017.03.003.
- 7.Hattab FN, Alhaija ES. Radiographic evaluation of mandibular third molar eruption space. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88(3):285–291. doi: 10.1016/s1079-2104(99)70029-6. [DOI] [PubMed] [Google Scholar]
- 8.Cortella S, Shofer FS, Ghafari J. Transverse development of the jaws: norms for the posteroanterior cephalometric analysis [published correction appears in Am J Orthod Dentofacial Orthop 1998 Mar;113(3):299] Am J Orthod Dentofac Orthop. 1997;112(5):519–522. doi: 10.1016/s0889-5406(97)70079-9. [DOI] [PubMed] [Google Scholar]
- 9.Carter K, Worthington S. Predictors of third molar impaction: a systematic review and Meta-analysis. J Dent Res. 2016;95(3):267–276. doi: 10.1177/0022034515615857. [DOI] [PubMed] [Google Scholar]
- 10.Hattab FN. Positional changes and eruption of impacted mandibular third molars in young adults. A radiographic 4-year follow-up study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(6):604–608. doi: 10.1016/s1079-2104(97)90359-0. [DOI] [PubMed] [Google Scholar]
- 11.Vranckx M, Ockerman A, Coucke W, Claerhout E, Grommen B, Miclotte A, Van Vlierberghe M, Politis C, Jacobs R. Radiographic prediction of mandibular third molar eruption and mandibular canal involvement based on angulation. Orthod Craniofac Res. 2019;22(2):118–123. doi: 10.1111/ocr.12297. [DOI] [PubMed] [Google Scholar]
- 12.Marciani RD. Third molar removal: an overview of indications, imaging, evaluation, and assessment of risk. Oral Maxillofac Surg Clin North Am. 2007;19(1):1–13. doi: 10.1016/j.coms.2006.11.007. [DOI] [PubMed] [Google Scholar]
- 13.Jakovljevic A, Lazic E, Soldatovic I, Nedeljkovic N, Andric M. Radiographic assessment of lower third molar eruption in different anteroposterior skeletal patterns and age-related groups. Angle Orthod. 2015;85(4):577–584. doi: 10.2319/062714-463.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ogawa T, Osato S. Growth changes of the mandibular body with eruption of mandibular third molars: analysis of anatomical morphometry and quantitative bone mineral content by using radiography. Ann Anat. 2013;195(2):143–150. doi: 10.1016/j.aanat.2012.07.011. [DOI] [PubMed] [Google Scholar]
- 15.Santos RMG, De Martino JM, Haiter Neto F, Passeri LA. Cone beam computed tomography-based cephalometric norms for Brazilian adults. Int J Oral Maxillofac Surg. 2018. 10.1016/j.ijom.2017.06.030. [DOI] [PubMed]
- 16.Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi: 10.1016/s0895-4356(96)00236-3. [DOI] [PubMed] [Google Scholar]
- 17.Hsieh FY. Sample size tables for logistic regression. Stat Med. 1989;8(7):795–802. doi: 10.1002/sim.4780080704. [DOI] [PubMed] [Google Scholar]
- 18.McNamara JA Jr. A method of cephalometric evaluation. Am J Orthod. 1984. 10.1016/s0002-9416(84)90352-x. [DOI] [PubMed]
- 19.Rodriguez-Cardenas YA, Arriola-Guillen LE, Flores-Mir C. Björk-Jarabak cephalometric analysis on CBCT synthesized cephalograms with different dentofacial sagittal skeletal patterns. Dental Press J Orthod. 2014;19(6):46–53. doi: 10.1590/2176-9451.19.6.046-053.oar. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Naqvi ZA, Shivalinga BM, Ravi S, Munawwar SS. Effect of cleft lip palate repair on craniofacial growth. J Orthod Sci. 2015;4(3):59–64. doi: 10.4103/2278-0203.160236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zhang Y, Sun X, Wang L, Chen K, Wang X, Wu G. Simultaneous orthognathic surgery and mandibular contour Osteoplasty for treating mandibular protrusion with high Gonial angle. J Craniofac Surg. 2020;31(5):1362–1366. doi: 10.1097/SCS.0000000000006360. [DOI] [PubMed] [Google Scholar]
- 22.De Bruyn L, Vranckx M, Jacobs R, Politis C. A retrospective cohort study on reasons to retain third molars. Int J Oral Maxillofac Surg. 2020;49(6):816–821. doi: 10.1016/j.ijom.2019.10.003. [DOI] [PubMed] [Google Scholar]
- 23.Olayemi AB. Assessment and determination of human mandibular and dental arch profiles in subjects with lower third molar impaction in Port Harcourt. Nigeria Ann Maxillofac Surg. 2011. 10.4103/2231-0746.92775. [DOI] [PMC free article] [PubMed]
- 24.Uthman AT. Retromolar space analysis in relation to selected linear and angular measurements for an Iraqi sample. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(4):e76–e82. doi: 10.1016/j.tripleo.2007.05.013. [DOI] [PubMed] [Google Scholar]
- 25.Aliaga-Del Castillo A, Janson G, Arriola-Guillén LE, Laranjeira V, Garib D. Effect of posterior space discrepancy and third molar angulation on anterior overbite. Am J Orthod Dentofac Orthop. 2018. 10.1016/j.ajodo.2017.12.014. [DOI] [PubMed]
- 26.Begtrup A, Grønastøð HÁ, Christensen IJ, Kjær I. Predicting lower third molar eruption on panoramic radiographs after cephalometric comparison of profile and panoramic radiographs. Eur J Orthod. 2013;35(4):460–466. doi: 10.1093/ejo/cjs012. [DOI] [PubMed] [Google Scholar]
- 27.Al-Gunaid TH, Bukhari AK, El Khateeb SM, Yamaki M. Relationship of mandibular ramus dimensions to lower third molar impaction. Eur J Dent. 2019. 10.1055/s-0039-1693922. [DOI] [PMC free article] [PubMed]
- 28.Mayama H, Kuwajima Y, Da Silva JD, Khorashadi S, Lambert RF, Ishida Y, Ishikawa-Nagai S, Miura H, Satoh K. Cephalometric measurements of non-syndromic Oligodontia in early dental age in a Japanese population. Clin Cosmet Investig Dent. 2019. 10.2147/CCIDE.S213111. [DOI] [PMC free article] [PubMed]
- 29.Sant'Ana LF, Giglio FP, Ferreira O, Jr, Sant'ana E, Capelozza AL. Clinical evaluation of the effects of radiographic distortion on the position and classification of mandibular third molars. Dentomaxillofac Radiol. 2005;34(2):96–101. doi: 10.1259/dmfr/29844316. [DOI] [PubMed] [Google Scholar]
- 30.Peker I, Sarikir C, Alkurt MT, et al. Achados de radiografia panorâmica e tomografia computadorizada de feixe cônico no exame pré-operatório de terceiros molares inferiores impactados. BMC Saúde Oral. 2014;14:71. doi: 10.1186/1472-6831-14-71. [DOI] [Google Scholar]
- 31.Aoun Y, Husseini B, Younes R, Ghosn N, Bouserhal J. Assessment of lower third molar space: a comparative radiographic study. Dentomaxillofac Radiol. 2022;51(5):20220049. doi: 10.1259/dmfr.20220049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Baqain ZH, AlHadidi A, AbuKaraky A, Khader Y. Does the use of cone-beam computed tomography before mandibular third molar surgery impact treatment planning? J Oral Maxillofac Surg. 2020. 10.1016/j.joms.2020.03.002. [DOI] [PubMed]
- 33.Freire BB, Nascimento EHL, Vasconcelos KF, Freitas QD, Haiter-Neto F. Radiologic assessment of mandibular third molars: an ex vivocomparative study of panoramic radiography, extraoral bitewing radiography, and cone beam CT. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2018. 10.1016/j.oooo.2018.11.002. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.