

Abstract
Objective:
Alcohol expectancies (AE) during early adolescence predict early alcohol use initiation and problem drinking both cross-sectionally and prospectively well into adulthood. Yet, our understanding of the sociocultural factors associated with AE during this development period remains limited. This study examines associations between AE and sociocultural factors across various domains (i.e., individual, family, peer, school, community, culture) in a demographically diverse sample of 10–14-year-old youth in the ABCD Study®.
Methods:
This cross-sectional study used 2-year follow-up data from the ABCD ® Release 3.0 for N = 5,322 early adolescents [M age =12 years (SD = 0.6); 47% male]. Approximately 60% identified as non-Hispanic/Latinx White, 17% as Hispanic/Latinx, 11% as non-Hispanic/Latinx Black, 2% as non-Hispanic/Latinx Asian, and 11% as mixed/other race-ethnicity. Separate models for positive and negative AE outcomes were conducted using linear-mixed effect models while controlling for demographic covariates.
Results:
Positive AE was most strongly associated with. Negative AE was most strongly associated with the peer-level factor of relational victimization and the individual-level factor of negative life events, followed by other peer, school, and community-level factors.
Conclusion:
The present findings reveal the potential constellation of sociocultural factors that may serve as targets for modifying AE during the middle school years. Study results also underscore the need for future research that integrates cultural factors into our understanding of alcohol-use risk and resilience during early adolescence.
Keywords: alcohol expectancies, sociocultural, familism, adolescence
Introduction
Youth that begin drinking by early adolescence are 4 times more likely to develop alcohol dependence in adulthood (Hingson, Heeren, & Winter, 2006). Adolescence is a time of shifting expectations about the likely positive or negative consequences of alcohol use (Masten, Faden, Zucker, & Spear, 2009). A considerable body of research and theory suggests that expectations for likely outcomes of drinking (i.e., alcohol expectancies) change substantially during early adolescence in ways that may contribute to heavier drinking patterns (Jester et al., 2015). The eco-developmental model posits that multiple social domains (i.e., individual, family, peer, school, community, culture), and the interrelations between them, can influence risk and resilience health behavior trajectories among adolescents (Prado et al., 2010). A greater understanding of how these multi-level factors shape expectations about alcohol use can inform future prevention and intervention programs for adolescents.
Alcohol Expectancies
Alcohol expectancies (AE), defined as one’s beliefs about probable outcomes of alcohol use, are a significant risk factor for underage drinking. Expectancy theory posits that individuals are motivated by their expected probability of receiving a valued reward (Jones et al., 2001). AE emerge in children often before initiation of alcohol use via social learning principles and environmental factors (e.g., family, school, peers, and community) (Smit et al., 2018). Notably, early adolescence is considered a particularly formative period for AE, characterized by increases in positive AE and decreases in negative AE (Colder et al., 2014).
Positive AE are beliefs about the beneficial drinking-related outcomes including perceptions of enhanced sociability, courageousness, and relaxation (Jester et al., 2015). Conversely, negative AE include perceptions of adverse experiences alcohol-related experiences, such as feeling sick or being unable to control one’s actions. Increases in positive AE have been linked to the onset of early-age drinking (Janssen et al., 2018), increased drinking quantity and frequency, and binge drinking in adolescence (Jester et al., 2105; Montes et al., 2019). However, associations between negative AE and drinking outcomes have been less consistent (Smit et al., 2018). Notably, AE can be relatively easy to modify and, as such, may be an essential target for prevention interventions against underage drinking (Campbell & Oei, 2010). Yet, our understanding of the individual, environmental, and cultural factors associated with AE remain limited (Smit et al., 2018).
Sociocultural Influences on Alcohol Expectancies
Individual-level Factors
Individual level factors represent the most proximal level of influence. Within this context, individual exposure to negative life events, or adverse childhood experiences, are strongly associated with alcohol initiation in early- and mid-adolescence (Dube et al., 2006). Previous studies have found adolescents who experienced emotional abuse, emotional neglect, parental separation/divorce, or household substance use were more likely to use alcohol in the past 12 months when compared to those not exposed to these experiences (Afifi et al., 2020). While the association between adverse life experiences and alcohol use is well documented (Hughes et al., 2017), less is known about how these experiences may impact AE during early adolescence.
From a resilience perspective, prosocial behaviors are defined as voluntary behaviors intended to benefit others, such as comforting, sharing, volunteering, donating, and offering physical or emotional assistance to others (Eisenberg, Spinrad, & Knafo-Noam, 2015). A growing body of research has identified prosocial behavior as a protective factor against a myriad of problematic outcomes, including but not limited to substance use (Memmott-Elison et al., 2020). While prosocial behaviors have been posited to have protective effects on AE, the evidence for this association remains limited. Indeed, overall, few studies have examined the impact of individual-level factors on AE, with researchers calling for investigations that elucidate these associations (Smit et al., 2018).
Family-level Factors
There is strong evidence for the influence of family-related factors (e.g., parental alcohol use) on AE (Smit et al., 2018). Other family-level factors, such as parental monitoring, conceptualized as an active tracking and surveillance of adolescent behaviors (Stattin & Kerr, 2000), have been negatively associated with alcohol use, both concurrently and longitudinally in middle school adolescents (Marmorstein, 2019). Evidence suggests possible mechanisms whereby parental monitoring may exert protective effects is through minimizing exposure to negative peer influences that contribute to alcohol use initiation (Hemovich et al., 2011). Conversely, family conflict (e.g., interparental and parent-child conflict) has been linked with increased susceptibility to early alcohol use initiation among youth (Fosco at el., 2018). Existing evidence links parental alcohol use to the development of AE among adolescents, yet less is known about the role that family conflict and parental monitoring play on the formation of AE during early adolescence.
Peer-level Factors
Peer networks are a particularly salient reference group for youth during adolescence and play an important role in shaping how youth navigate their changing social landscape. For instance, involvement with delinquent peers can promote opportunities to engage and socially reinforce drinking behaviors, increase perceptions of youth alcohol use as normative, and shape AE and alcohol initiation (Trucco et al., 2014).
Bullying-related behaviors peak during early adolescence and have been found to impact alcohol use among youth (Filipponi et al., 2020; Maniglo, 2017). Relational aggression is characterized by behavior aimed at harming peers’ relationships through exclusion, manipulation, and rumors (Dallen et al., 2013). Relational victimization occurs when an individual receives this harmful behavior from a peer with the intention of damaging relationships (Card & Hodges, 2008). While evidence has linked bullying to alcohol use, there is limited evidence on how these experiences are influenced by the formation of bullying behavior (Maniglo, 2017). Conversely, positive peer networks such as involvement with prosocial peers (i.e., friends who: earn good grades, are athletes, attend religious services) can have protective effects against alcohol use (Hodder et al., 2016).
School-level Factors
School-level factors may be increasingly important for preventing adolescent future alcohol use due to the amount of time adolescents spend in school settings (Faggiano, Minozzi, Versino & Buscemi, 2014). Existing research indicates that school involvement and connectedness can have protective effects against early-onset drinking (Cummins, Diep, & Brown, 2019), while school disengagement has been linked to alcohol use risk behaviors (Henry et al., 2012). Findings from systematic reviews reveal that multidimensional school-based programs are effective in preventing bullying and illicit substance use as well as promoting sexual health; however, their effectiveness in targeting drinking outcomes is less clear (Cho & Cho, 2021; Hodder et al., 2017; Shackleton et al., 2016). As such, there remains a need to understand school-based risk and protective factors in the context of alcohol use, and in turn, inform effective interventions to deter underage drinking.
Neighborhood-level Factors
Neighborhood-level characteristics, such as residing in an unsafe community, have been associated with adolescents’ alcohol use behaviors (Afifi et al., 2020). Studies have found that adolescents living in unsafe neighborhoods are twice as likely to report alcohol use in the past 12 months compared to those that reside in safe communities (Afifi et al., 2020). Researchers have also posited that neighborhood disadvantage may be associated with adolescent alcohol via diminished family functioning (Byrnes & Miller, 2012) and facilitation of access to deviant peers (Cambron et al., 2018). However, overall, little is known about the influence of neighborhood-related factors on AE.
Cultural-level Factors.
Culture is defined as values, beliefs, and practices shared among a group of people that may be transmitted from one generation to the next (Schwartz, Unger, Zamboanga, & Szapocznik, 2010). Cultural values contribute to adolescent decisions about whether and when to use substances (Shih et al., 2012). Familism, a cultural value that emphasizes the importance of family interdependence and commitment (Sabogal et al., 1987), has been linked with higher negative AE and lower positive expectancies among middle school youth (Shih et al., 2012). Familism as a cultural value applies to numerous cultural groups, yet the bulk of the literature in this area has been founded on research conducted with Hispanic/Latinx populations (Cahill, Updegraff, Causadias, & Korous 2021). Notwithstanding the above-mentioned advances in this area of research, there remains a need to examine the potential role of familism on drinking-related outcomes across diverse racial-ethnic youth.
Acculturation, a shift in cultural practices, values, and identity resulting from contact with another culture, has been linked to adolescent alcohol use, primarily among Hispanic/Latinx youth (Schwartz et al., 2010). Evidence suggests that lower levels of acculturation are associated with decreased rates of underage drinking in this population (Eitle et al., 2009). Indeed, less acculturated Hispanic/Latinx youth have also been found to endorse lower levels of positive AE compared to their more acculturated counterparts (Des Rosiers et al., 2012). Far less is known about the influence of acculturation on substance use across diverse racial-ethnic groups.
The Current Study
The present study will be the first to examine direct associations between multi-level (i.e., individual, family, peer, school, neighborhood, and culture) sociocultural risk/protective factors and AE in a national sample of racial-ethnically diverse early adolescents. Examining how various sociocultural factors influence AE during early adolescence is critical, given that this is a key developmental period for shaping AE and, in turn, subsequent alcohol use behaviors (Colder et al., 2014).
Data from the Adolescent Brain Cognitive Development Study (ABCD Study®), funded by the National Institutes of Health, was used to accomplish two parallel aims and examine the direct effects of sociocultural factors at the individual, family, peer, school, community, and cultural levels on (1) positive and (2) negative AE in early adolescence. We hypothesized the following: (H1) High levels of sociocultural protective factors (i.e., prosocial behaviors and prosocial peers, parental monitoring, school protective factors, neighborhood safety, and familism) will be associated with lower positive and higher negative AE. (H2) High levels of sociocultural risk factors (i.e., adverse life events, family history of alcohol-related problems, family conflict, relational victimization/reputational aggression, delinquent peers, school risk factors, neighborhood disadvantage, and language use with family) will be associated with higher positive AE and lower negative AE among youth during early adolescence.
Unlike most studies that have examined factors across limited domains (i.e., parent, peer), this study contributes to the existing literature by simultaneously examining how multiple sociocultural factors across various eco-developmental levels influence AE among youth. Additionally, the use of a large and diverse national sample of early adolescents was an innovative aspect of the present study. Notably, it is one of few investigations to examine the impact of cultural factors such as familism on AE in a diverse national sample of early adolescents, and to the best of our knowledge, the first to incorporate cultural factors within an eco-developmental framework toward understanding AE in this population.
Methods
The ABCD Study® is a multi-site, longitudinal study that examines the biological and behavioral trajectories of more than 11,000 children across (Compton et al., 2019) national sites beginning at ages 9–10 through adolescence into early adulthood. The ABCD Study® conducted these assessments throughout the year at university and research institution settings with MRI facilities. The cohort was recruited to maximally reflect the demographic and geographic diversity of the U.S. adolescent population. Specifically, the study team used an epidemiologically informed school-based recruitment strategy that was designed to approximate the demographics of the ABCD® sites and the U.S. as a whole (Compton et al., 2019; Volkov et al., 2018). ABCD® research sites either used a central Institutional Review Board at the University of California, San Diego, or used local Institutional Review Boards for the ethical review and approval of the research protocol (Auchter et al., 2018). The baseline ABCD® sample includes 11,875 children aged 9–10 years (52% female, 48% male; 52% non-Hispanic/Latinx White, 15% non-Hispanic/Latinx Black, 20% Hispanic, 12% mixed/other racial-ethnic groups).
The present study used 2-year follow-up data from the ABCD® Release 3.0 for N = 6,567 youth with alcohol-related. Children in the sample were, on average, 12 years old (SD = 0.6 years) and 47% of these children were male, 60% identified as non-Hispanic/Latinx White, 17% as Hispanic/Latinx, 11% as Black, 2% as Asian, and 11% as mixed or other race-ethnicity. Specifically, we utilized measures of behavioral and mental health functioning, substance use, and culture and environment characteristics that are collected annually or biannually (Barch et al., 2018; Zucker et al., 2018; Lisdahl et al., 2018). See the National Institute of Mental Health Data Archive (https://nda.nih.gov/abcd) for additional ABCD Study® information. The description of demographics and measures are shown in Table 1.
Table 1.
Descriptive statistics for all variables in the full sample (N=6567)
| Mean (sd) or n (%) | Range | n Missing (%) | Coefficient Omega | Cronbach’s Alpha | |
|---|---|---|---|---|---|
|
| |||||
| Demographic Measures, mean (sd) | |||||
| Age (years) | 12.0 (0.6) | 10.1 – 13.6 | 0 | -- | -- |
| Sex at Birth, n (%) | 0 | -- | -- | ||
| Female | 3102 (47.2) | -- | -- | -- | -- |
| Male | 3465 (52.8) | -- | -- | -- | -- |
| Family Nativity: Anyone in family born outside U.S. (yes), n (%) | 2105 (32.1) | -- | 0 | -- | -- |
| Race-Ethnicity, n (%) | 45 (0.7) | -- | -- | ||
| Hispanic | 1075 (16.5) | -- | -- | -- | -- |
| Non-Hispanic White | 3841 (58.9) | -- | -- | -- | -- |
| Non-Hispanic Black | 773 (11.8) | -- | -- | -- | -- |
| Non-Hispanic Asian | 141 (2.2) | -- | -- | -- | -- |
| Non-Hispanic Other/Mixed | 692 (10.6) | -- | -- | -- | -- |
| Sibling status, n (%) | 0 | -- | -- | ||
| Singletons | 4221 (64.3) | -- | -- | -- | -- |
| Siblings | 984 (15.0) | -- | -- | -- | -- |
| Twins | 1341 (20.4) | -- | -- | -- | -- |
| Triplets | 21 (0.3) | -- | -- | -- | -- |
| Alcohol Expectancies (AEs), mean (sd) | -- | -- | |||
| Positive AEs | 2.0 (0.8) | 1 – 5 | 61 (0.9) | 0.73 | 0.69 |
| Negative AEs | 4.2 (0.9) | 1 – 5 | 61 (0.9) | 0.69 | 0.68 |
| Sociocultural Level Predictors, mean (sd) | |||||
| Individual level | |||||
| Prosocial behaviors | 1.7 (0.4) | 0 – 2 | 34 (0.5) | 0.66 | 0.66 |
| Number of negative life events | 2.4 (2.3) | 0 – 19 | 0 | -- | -- |
| Family level | |||||
| History of Family Alcohol Misuse (yes), n (%) | 2999 (47.0) | -- | 179 (2.7) | -- | -- |
| Family conflict | 1.9 (1.8) | 0 – 9 | 36 (0.5) | 0.71 | 0.67 |
| Parental monitoring | 4.5 (0.5) | 1 – 5 | 34 (0.5) | 0.65 | 0.59 |
| Peer level | |||||
| Prosocial Peers | 9.4 (2.6) | 2 – 15 | 174 (2.6) | 0.46 | 0.45 |
| Rule breaking/delinquent peers | 3.6 (1.3) | 2 – 15 | 240 (3.7) | 0.59 | 0.57 |
| Relational victimization | 4.8 (2) | 3 – 15 | 27 (0.4) | 0.73 | 0.72 |
| Reputational aggression | 3.2 (0.7) | 3 – 15 | 27 (0.4) | 0.71 | 0.71 |
| School level | |||||
| SRPF School involvement | 12.7 (2.3) | 4 – 16 | 36 (0.5) | 0.77 | 0.72 |
| SRPF School disengagement | 3.9 (1.3) | 2 – 8 | 36 (0.5) | 0.15 | 0.26 |
| SRPF School positive environment | 19.6 (2.8) | 6 – 24 | 36 (0.5) | 0.78 | 0.71 |
| Community level | |||||
| Neighborhood safety | 4.1 (1.0) | 1 – 5 | 34 (0.5) | -- | -- |
| Area deprivation index (ADI) | 37.8 (26.3) | 0 – 100 | 216 (3.3) | -- | -- |
| Cultural level | |||||
| MACV Familism | 3.9 (0.6) | 1 – 5 | 40 (0.6) | 0.94 | 0.93 |
| Lanugage use with family | 3.9 (1.3) | 1 – 5 | 0 | -- | -- |
Language use data available only for participants endorsing speaking another language other than English n = 2350.
Measures
See Supplementary Table 1 for a detailed description of measures within.
Demographic covariates –
Demographic variables included youth age at time of assessment, sex assigned at birth (i.e., female, male), whether youth had a corresponding sibling participating in the study, and family nativity (i.e., family born outside of the U.S., including parents, grandparents, and child). Youth’s race and ethnicity were based on parents’ self-report. Specifically, parents were asked “What race do you consider the child to be? Please check all that apply” and provided a list of 16 possible race categories from which to choose (i.e., American Indian/ Native American, Asian, Black/African American, Chinese, Japanese, White, etc.). For ethnicity, participants were asked if they considered their child to be Hispanic/Latino/Latina. See Barch et al., 2018, 2021 for details.
In the present study, these race and ethnic categories were then collapsed as follows: Hispanic/Latinx, non-Hispanic/Latinx White, non-Hispanic/Latinx Black, non-Hispanic/Latinx Asian, and non-Hispanic Latinx other/mixed race). We collapsed race and ethnicity to contrast Hispanic/Latinx with non-Hispanic/Latinx populations in the ABCD Study® given that most of the literature focusing on the sociocultural determinants of alcohol use has focused on Hispanic/Latinx populations. This allows our findings to be interpreted with the context of the existing literature. However, it should be recognized that race and ethnicity are separate social and political constructs without scientific or biological meaning, that capture both social and structural advantage and disadvantage as well as shared culture and language (Borrell et al., 2021). As such, they remain a useful construct through which to study the impact of sociocultural factors on health and behavior. For all variables comprised of a total score across multiple items, we report the reliability of the measure using the ordinal coefficient omega in Table 1 (Deng & Chan, 2017).
Alcohol Use Expectancies (AE)
Alcohol expectancies were assessed using the Alcohol Expectancy Questionnaire- Adolescent, Brief (AEQ-AB), a 7-item measure with two subscales assessing General Positive Effects, and Potential Negative Effects. See Lisdahl et al., 2018 for details.
Individual-level Measures
Prosocial Behaviors.
Assessed via 3 items from the Prosocial Behavior subscale of the “Strengths and Difficulties Questionnaire.” See Zucker et al., 2018; Gonzalez et al., 2021 for details.
Adverse Life Events.
The PhenX Life Events Scale (Tiet et al., 1998) assessed 25 potential life events. Children are asked to report whether they have ever experienced a given event, and if so, if the event was “mostly good” or “mostly bad” for them. A sum score of the total number of life events that children endorsed as bad (negative) was used with higher scores reflecting greater exposure to negative life events. See Barch et al., 2018, 2021 for details.
Family-level Measures
Family History of Alcohol-Related Problems.
Assessed via the Family History Assessment from the National Consortium on Alcohol and Neurodevelopment in Adolescence (NCANDA) study. Parents were asked if any blood relative of their child has ever had a problem with alcohol including engaging in fights or trouble staying employed. Responses were collapsed into any problematic alcohol use (0 = No, 1 = Yes). See Barch et al., 2018, 2021 for details.
Parental Monitoring.
Measured via the Parental Monitoring Scale with a subset of 5 items assessing parents’ active efforts to track their child’s whereabouts, both in and out of the home (e.g., who they are with; what they are doing). See Zucker et al., 2018; Gonzalez et al., 2021 for details.
Family Conflict.
Assessed with 9 true/false items from the Family Conflict subscale of the Moos Family Environment Scale (FES). See Zucker et al., 2018; Gonzalez et al., 2021 for details.
Peer-level Measures
Relational Victimization/Reputational Aggression.
Measured with two subscales from a modified version of the “Revised Peer Experiences Questionnaire – Bully and Victim” assessing the youth’s own aggression (reputational aggression) and their peers’ aggressions toward them (relational victimization). See Barch et al., 2021 for details.
Prosocial and Rule Breaking/Delinquent Peers.
The Prosocial Peer Involvement and the Rule Breaking/Delinquent Peer Involvement subscales of the Youth Peer Behavior Profile, assessed extent to which youth’s friendship network consists of (a) prosocial peers (e.g., friends who are excellent students, are athletes, etc.), and/or (b) rule breaking/delinquent peers (e.g., friends who skip school, shoplift, etc.); the two sub-scales are not mutually exclusive. See Zucker et al., (2018; Gonzalez et al., 2021 for details.
School-level Measures
School Risk and Protective Factors.
The School Risk and Protective Factors (SRPF) Survey is from the PhenX School Risk and Protective Factors protocol. Three subscale scores are derived: School Environment, School Involvement, and School Disengagement. See Zucker et al., (2018); Gonzalez et al., (2021) for details.
Community-level Measures
Neighborhood Safety.
Assessed via the PhenX Toolkit “Safety from Crime” assessing neighborhood characteristics. For youth, one item thought to be most appropriate for participants’ age range was used to measure neighborhood safety (i.e., “My neighborhood is safe from crime”). See Zucker et al., (2018); Gonzalez et al., (2021) for details.
Neighborhood Disadvantage.
Geocoded data calculated an area deprivation index (ADI), a composite metric of neighborhood disadvantage derived from 17 variables from the U.S. Census Bureau’s American Community Survey (ACS) disadvantage (e.g., unemployment, poverty rates, median family income, low education). ADI for youth participants’ primary residential address at baseline visit is a composite weighted-sum metric of neighborhood disadvantage. Census-tract-level ADI, based on the 2011–2015 five-year ACS estimates, was computed based on coefficient values from Kind et al. (2014) and discretized into national percentiles for the ABCD® data release. See Garavan et al. 2018 for details.
Cultural Measures
Familism.
The Mexican American Cultural Values Scale (MACVS) was used to assess familism. As suggested by the instrument developers, a composite familism score was calculated using mean values for 16 items totaling across three subscales (i.e., family support, family obligation, family referent), with higher scores indicating greater familism. See Zucker et al., 2018; Gonzalez et al., 2021 for details.
Language Use.
Language use with family was used as a proxy for acculturation and was assessed with an adapted version of the PhenX Acculturation protocol. See Zucker et al., 2018; Gonzalez et al., 2021 for details.
It should be noted that data on sociocultural correlates of alcohol use risk among youth has historically been gathered across various levels of data collection, including youth report, parent self-report, and objective measures. Indeed, the level at which specific social effects occur may depend on whether the effect is measured at the level of the effect itself (i.e., neighborhood disadvantage), or at the level of the individual perceiving the effect (i.e., child’s perception of neighborhood safety). In the present study, we examine sociocultural correlates associated with youth’s perception of AE with the exception of family history of alcohol-related problems collected through parent report and neighborhood disadvantage, assessed via U.S. Census data. Previous studies have shown youth’s perceptions of family, peer, school connectedness, and neighborhood safety can be stronger predictors of youth adjustment than those of parent report (Law, Cuskelly, & Carrol, 2013; Witherspoon et al., 2016).
Analysis Plan
Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, North Carolina). The percentage of missing values across the 21 independent variables of interest varied between 0% and 9%. Overall, 1245 of 6567 records (19%) were incomplete due to missing data in one of the variables of interest (see Table 2). Missing at random (MAR) was assumed based on the results from missing mechanism diagnosis with logistic regression and sensitivity (see Supplementary Tables 3 and 4). The missing data was imputed using multilevel multiple imputations with a fully conditional specification (FCS) approach in Blimp 3.0 (Enders, Keller, & Levy, 2018), which imputes variables individually based on their distribution. The clustering effects of the study site and family were taken into account in the multiple imputations. All the variables in the mixed models were included in the multiple imputations. In all, 200 datasets were imputed and used in the present analysis. We applied linear mixed models to each of the 200 imputed datasets for the positive and negative alcohol expectancies, respectively, and then pooled together the 200 estimates for each independent variable to produce a final estimate of the coefficients. Further, the linear correlation coefficients with standard errors were estimated in each imputed dataset separately and combined by applying the Rubin rules (Rubin, 1987) using the PROC MIANALYZE procedure in SAS.
Table 2.
Associations with alcohol expectancies using linear mixed effect models (N=6567), showing standardized beta coefficients (β) and the 95% confidence intervals (CI), and p-values for the model including all independent variables using FCS imputation for missing data.
| Positive Alcohol Expectancies |
Negative Alcohol Expectancies |
|||||||
|---|---|---|---|---|---|---|---|---|
| 95% CI |
95% CI |
|||||||
| Predictors | β | LL | UL | P | β | LL | UL | P |
|
| ||||||||
| Demographics | ||||||||
| Age in years | 6.973 | 5.419 | 8.527 | 0.001 | 3.130 | 1.295 | 4.965 | 0.001 |
| Sex: Male vs. Female | 1.048 | -0.522 | 2.618 | 0.191 | 3.172 | 1.325 | 5.020 | 0.001 |
| Race and ethnicity | ||||||||
| Non-Hispanic Asian vs. Non-Hispanic White | −0.326 | −1.921 | 1.270 | 0.689 | 0.127 | −1.743 | 1.997 | 0.894 |
| Non-Hispanic Black vs. Non-Hispanic White | −2.963 | −4.785 | −1.140 | 0.001 | −3.666 | −5.791 | −1.542 | 0.001 |
| Hispanic vs. Non-Hispanic White | −3.089 | −5.142 | −1.036 | 0.003 | −3.000 | −5.384 | −0.615 | 0.014 |
| Non-Hispanic Other/Mixed vs. Non-Hispanic White | −0.334 | −1.960 | 1.292 | 0.687 | 1.748 | −0.149 | 3.645 | 0.071 |
| Non-Hispanic Asian vs. Non-Hispanic Blacka | 1.006 | −0.735 | 2.748 | 0.257 | 1.776 | −0.262 | 3.813 | 0.088 |
| Hispanic vs. Non-Hispanic Blacka | 0.321 | −2.200 | 2.841 | 0.803 | 1.220 | −1.715 | 4.154 | 0.415 |
| Non-Hispanic Other/Mixed vs. Non-Hispanic Blacka | 2.528 | 0.392 | 4.664 | 0.020 | 5.290 | 2.798 | 7.781 | <0.001 |
| Hispanic vs. Non-Hispanic Other/Mixeda | −2.691 | −5.117 | −0.265 | 0.030 | −5.082 | −7.906 | −2.259 | <0.001 |
| Non-Hispanic Asian vs. Non-Hispanic Other/Mixeda | −0.170 | −1.851 | 1.510 | 0.843 | −0.687 | −2.654 | 1.281 | 0.494 |
| Hispanic vs. Non-Hispanic Asiana | 0.127 | −1.743 | 1.997 | 0.297 | −3.325 | −8.291 | 1.641 | 0.189 |
| Any family member foreign born vs. All U.S. born | 2.539 | 0.726 | 4.352 | 0.006 | −0.322 | −2.435 | 1.791 | 0.765 |
| Have siblings or not | ||||||||
| Siblings vs. Singletons | −2.502 | −4.118 | −0.887 | 0.002 | −0.174 | −2.035 | 1.687 | 0.855 |
| Twins vs. Singletons | −2.812 | −4.888 | −0.736 | 0.008 | −0.626 | −2.980 | 1.727 | 0.602 |
| Triplets vs. Singletons | −1.436 | −3.122 | 0.250 | 0.095 | −1.318 | −3.172 | 0.536 | 0.164 |
| Individual factor | ||||||||
| Prosocial behaviors | −2.128 | −3.883 | −0.374 | 0.017 | 1.994 | −0.079 | 4.068 | 0.059 |
| Number of negative life events | 1.486 | −0.157 | 3.129 | 0.076 | 4.463 | 2.525 | 6.400 | <0.001 |
| Family factor | ||||||||
| Family history of alcohol abuse problems | 0.534 | −1.046 | 2.114 | 0.508 | 2.285 | 0.439 | 4.130 | 0.015 |
| Family conflict | 2.153 | 0.483 | 3.823 | 0.012 | −0.489 | −2.454 | 1.477 | 0.626 |
| Parental monitoring | 0.940 | −0.798 | 2.678 | 0.289 | 0.226 | −1.825 | 2.276 | 0.829 |
| Peer factor | ||||||||
| Prosocial Peers | −0.727 | −2.371 | 0.917 | 0.386 | 0.909 | −1.038 | 2.856 | 0.360 |
| Rule breaking/delinquent peers | 1.430 | −0.271 | 3.130 | 0.099 | −3.218 | −5.235 | −1.201 | 0.002 |
| Relational victimization | 3.084 | 1.471 | 4.697 | <0.001 | 5.696 | 3.788 | 7.603 | <0.001 |
| Reputational aggression | 2.884 | 1.296 | 4.473 | <0.001 | 2.320 | 0.438 | 4.201 | 0.016 |
| School factor | ||||||||
| SRPF School involvement | 0.745 | −1.455 | 2.946 | 0.507 | 2.696 | 0.090 | 5.303 | 0.043 |
| SRPF School disengagement | 2.910 | 1.099 | 4.721 | 0.002 | −3.673 | −5.815 | −1.531 | 0.001 |
| SRPR School environment | −2.361 | −4.377 | −0.345 | 0.022 | −2.312 | −4.694 | 0.071 | 0.057 |
| Community factor | ||||||||
| Neighborhood safety | −0.561 | −2.191 | 1.069 | 0.500 | 3.360 | 1.435 | 5.285 | 0.001 |
| Area deprivation index (ADI) | −2.852 | −4.836 | −0.868 | 0.005 | −3.174 | −5.467 | −0.881 | 0.007 |
| Cultural factor | ||||||||
| Familism | −6.691 | −8.403 | −4.978 | <0.001 | 1.709 | −0.317 | 3.734 | 0.098 |
| Language use b | 2.750 | 0.581 | 4.918 | 0.013 | 0.390 | −2.186 | 2.965 | 0.767 |
Estimates from pairwise comparisons.
Coefficients from sub-sample models with participants who spoke another language other than English, using FCS imputation when including all independent variables (n = 2350).
Note: associations with p < 0.05 are in bold.
For comparison, we also performed the linear mixed modeling on the full data. The models used the dataset with complete data, which included 5821 out of 6567 cases, while 746 cases were excluded due to listwise deletion. To test the effect of language use on alcohol expectancies, we conducted linear mixed modeling on alcohol expectancies with a subset of the imputed data, including the youths who reported speaking another language (n=2350*200). Language use was an independent variable in the models, controlling demographics and all the other sociocultural independent variables.
While using population weights in analyses with the ABCD Study® dataset can be useful for making generalized inferences to the population of the United States, given the inclusion of a cultural dimension in our analyses, we refrained from calculating population-based estimates to interpret the results in context of the specific racial and ethnic composition of the sample analyzed (Dick et al., 2021).
Results
The main full model results for the linear mixed-effect models (using FCS imputation) are summarized in Figure 1, showing associations between all socio-cultural factors with positive and negative AE, and in Table 2, we report the corresponding standardized beta coefficients, 95% confidence intervals, and p-values. Coefficients from the models using the FCS imputation method were similar to results obtained from linear mixed-effect models using the non-missing data subsample n = 5821 (Supplementary Table 5). Bivariate models testing zero-order correlations for each independent variable (i.e., each socio-cultural factor was included as the only independent variable with all covariates) to test associations with positive and negative AE are reported in Supplementary Table 5.
Figure 1.
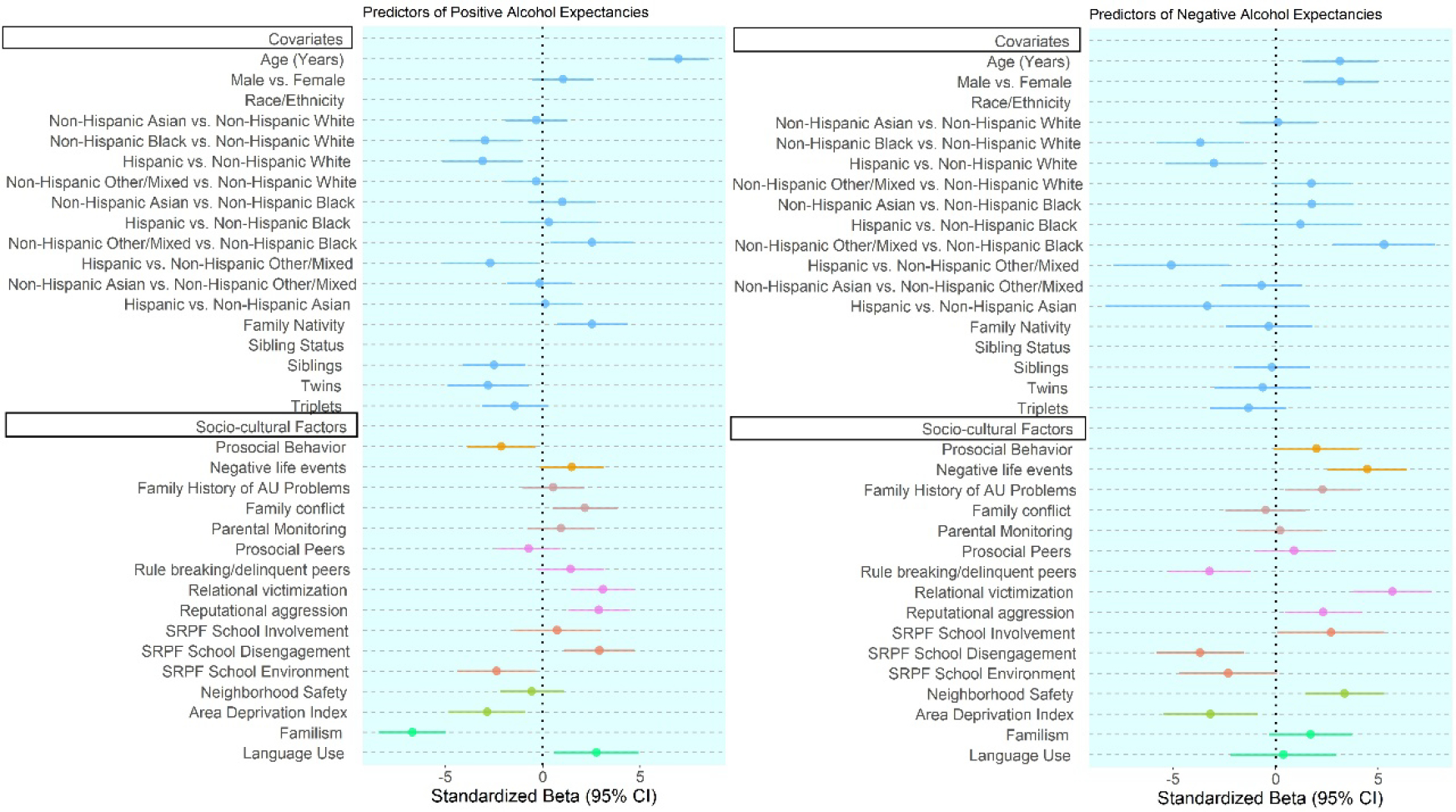
Results of linear mixed-effect models using FCS imputation to test associations between socio-cultural factors and positive and negative AE, showing the effect sizes (i.e., standardized beta coefficient) and 95% confidence intervals for each socio-cultural factor in association with AE. Note: variables with corresponding standard beta 95% CIs that cross zero were interpreted as non-significant effects.
Correlates of Positive and Negative AE
Positive and negative expectancies increased with age (all β > 3.0, p < 0.001). Males at birth reported higher negative AE compared to females, with significant differences for positive AE (β = 3.172, p < 0.001). Higher negative AE and lower positive AE were observed for Non-Hispanic/Latinx Black and Hispanic/Latinx youth compared to non-Hispanic/Latinx White youth, with Non-Hispanic/Latinx Other/Mixed youth showing higher negative AE compared to non-Hispanic/Latinx Black and Hispanic/Latinx youth (all |β| > 2.5, p ≤ 0.03). Higher positive AE were reported among youth with a family member born outside of the U.S., with no differences for negative AE (β = 2.539, p = 0.006). Youth with siblings or twins in the study had lower positive AE compared to singletons (β = −2.502, p = 0.002). There were no other differences in AE between singletons, twins, and triplets (all p ≥ 0.008).
Sociocultural Factors Associated with Positive and Negative AE
Positive AE
At the individual-level, higher prosocial behaviors were associated with fewer positive AE (β = −2.128, p = 0.017), while at the family level, higher family conflict was associated with higher positive AE (β = 2.153, p = 0.012). At the peer level, greater endorsement of relational victimization and reputational aggression were associated with higher positive AE (all |β| > 2.8, p < 0.001). At the school level, greater endorsement of school disengagement and poorer quality school environments were associated with higher positive AE (all |β| > 2.3, p ≤ 0.02). At the community level, greater ADI (more deprivation) was associated with higher positive AE (β = −2.852, p = 0.005). At the cultural level, familism was associated with lower positive AE (β = −6.691, p < 0.001), while greater English use with family was associated with higher positive AE (β = 2.750, p = 0.013). Positive AE was most strongly associated with the cultural-level factor of familism, followed by other peer, school, community, and cultural-level factors, including relational victimization and reputational aggression, school disengagement, ADI, and language use. No other sociocultural factors were significantly associated with positive AE (all p > 0.07). See Figure 1 and Table 2 for summarized results.
Negative AE
At the individual level, higher endorsement of negative life events was associated with higher negative AE (β = 4.463, p < 0.001), while at the family level, having a family history of alcohol abuse problems was associated with more negative AE (β = 2.285, p = 0.015). At the peer level, lower affiliation with rule-breaking/delinquent peers was associated with higher negative AE, while greater endorsement of relational victimization and reputational aggression was also associated with higher negative AE (all |β| > 2.3, p ≤ 0.016). At the school level, while there was a positive correlation between school involvement and negative AE (β = 2.696, p = 0.043), greater school disengagement was more strongly associated with lower negative AE (β = −3.673, p = 0.001). At the community level, higher neighborhood safety was associated with higher negative AE (β = 3.360, p = 0.001), while greater ADI (more deprivation) was also associated with lower negative AE (β = −3.174, p = 0.007). Negative AE was most strongly associated with the peer-level factor, relational victimization and the individual-level factor, negative life events, followed by other peer, school, and community-level factors, such as affiliation with rule breaking/delinquent peers, school disengagement, and neighborhood safety and ADI. No other factors were significantly associated with negative AE, including cultural-level factors of familism and language use with family (all p > 0.09). Figure 1 and Table 2 show the summarized results.
Discussion
The current study builds on previous findings to shed light on sociocultural factors across various levels of influence that may impact AE during early adolescence. Our results revealed distinct multi-level sociocultural factors in association with positive and negative AE. Specifically, the cultural-level factor of familism, followed by other peer, school, community, and cultural level factors, emerged as the strongest correlates of positive AE. The peer-level factor of relational victimization and the individual-level factor (i.e., negative life events), followed by other peer, school, and community-level factors, were associated with negative AE. Robust literature links AE to subsequent early drinking initiation (Smit et al., 2018). Indeed, previous studies using the ABCD Study® sample have found associations between positive AE and alcohol sipping among 9–11-year-old children (Murphy, Dufour, & Gray, 2021). While existing multi-level prevention interventions are shown to be effective in targeting substance use behaviors including smoking and illicit drug use among youth, evidence remains limited regarding their efficacy in reducing underage drinking. We anticipate that knowledge gleaned from the present study can be used to inform multicomponent prevention interventions during early adolescence, a particularly formative developmental period characterized by shifts in AE (Colder et al., 2014). Below, we discuss key findings on the associations between multi-level sociocultural factors and positive/negative AE.
Positive Alcohol Expectancies
The strongest influence on AE (highest β values across all sociocultural factors) emerged at the cultural level. Specifically, greater familism was associated with lower positive AE. This is an important finding given that the protective effects of familism have predominantly been examined among Hispanic/Latinx youth. Few studies have investigated the influence of familism on risk alcohol use among racial and ethnically diverse adolescent samples (Falzarano, Moxley, Pillemer& Czaja, 2021). In a racial-ethnically diverse sample of 193 at-risk youth, Ewing and colleagues (2015) found that high familism was associated with lower levels of alcohol use. Interestingly, the researchers found this effect, even after controlling for race and ethnicity, suggesting that familism was a relevant factor for reducing drinking across racial-ethnic groups. Other studies with diverse samples have also found consistent results (Shih et al., 2012).
An implication of this finding is the potential application of family-based interventions aimed at improving familism across diverse early adolescent populations. Existing interventions aimed at increasing familism have primarily been limited to Hispanic/Latinx study samples due to the cultural origin of the construct. However, our findings (along with others; Shih et al., 2012) suggest that increasing “familism” values (e.g., respect) may be applicable and protective against adverse outcomes for non-Hispanic/Latinx adolescents as well. This may be particularly true during early adolescence when youth are more dependent on family and less autonomous (Zimmer-Gembeck & Collins, 2003).
One aspect of familism, “respeto” or respect, may work to protect adolescents from positive AE through respecting parental rules and boundaries related to alcohol to avoid conflict with parents (Soto et al., 2011). Additionally, higher levels of familism, which may reflect a positive family environment, may protect youth against positive AE through the provision of family support. Youth that feel more supported by their families may have more coping resources to manage life stressors and, thus, may be less likely to rely on alcohol as a coping mechanism (Soto et al., 2002). Overall, our findings suggest the need for a broader consideration of cultural factors in relation to AE. Cultural values such as familism can play an important role in youth’s AE and, thus, may be an important resilience factor to consider in the development of prevention and intervention efforts targeting AE among early adolescents across racial-ethnic groups.
As hypothesized, family conflict was associated with greater positive AE. These findings are consistent with those of previous studies indicating family conflict as a risk factor for child and adolescent substance use (Fosco et al., 2018). Recent studies using the ABCD Study® cohort have found that among youth, those with higher levels of family conflict were more also likely to have a greater curiosity about alcohol and lower perceptions of alcohol use risk (Wade et al., 2021). Interestingly, our findings reveal that family-level factors were not among the strongest correlates of AE. While previous studies have focused heavily on family-level factors (e.g., parental substance use) as predictors of AE in youth, much less is known about individual and environmental factors associated with the AE during adolescence (Shih et al., 2018). Our findings suggest the need to consider the impact of other individual, pee8th-grader, school, community, and cultural factors in the formation of AE during key developmental time periods such as early adolescence.
At the individual level, our results reveal that prosocial behaviors may play an important role in reducing positive expectancies among early adolescents. These findings are consistent with prior research, which found prosocial behaviors to be generally associated with a lower risk of substance use trajectories during adolescence and well into young adulthood (Hodder et al., 2016). Researchers have identified the need for interventions that focus on prosocial behavior skill building among youth, particularly since prosocial behavior are relatively “malleable” and can be properly nurtured through appropriate educational actions (Caprara et al., 2015; Ellis et al., 2016). In an Italian school-based intervention program designed entirely to promote prosocial behaviors in early adolescents, Caprara and colleagues (2016) found significant increases in prosocial behaviors, self-efficacy beliefs, agreeableness, higher grades, and decreased physical aggression. Findings from the present study build on this literature and suggest that interventions targeting prosocial behaviors among at-risk youth (i.e., those with high levels of reputational aggression) could serve to potentially curb positive AE among early adolescents. At the peer level, reputational aggression (i.e., displaying bullying behavior) and reputational victimization (i.e., being bullied) were associated with higher levels of positive AE. Evidence suggests that relational victimization may promote substance use as a means of coping or self-medication to deal with the stress and negative feelings associated with victimization (Mangilo, 2017), whereas perpetrators of reputational aggression may use substance use as a way to enhance social status and gain approval (Spijkerman et al., 2005), particularly when in the company of other deviant peers (Cook et al., 2010). It may be that similar mechanisms exist in the formation of AE. Notably, early adolescence is a key developmental period for the escalation of bullying behaviors (Filipponi et al., 2020). These findings have implications for the timing of substance use prevention programs and their relation to anti-bullying efforts. Specifically, the implementation of anti-bullying campaigns in middle school years may reduce positive AE and, in turn, offset the risk for early alcohol use initiation.
Among the examined school-level factors, school disengagement and poor school environment emerged as risk factors for higher positive AE. Previous studies have documented these factors as predictors of dropout, delinquency, and substance use problems during adolescence and well into early adulthood (Henry et al., 2012). Given that school disengagement escalates during middle school years, our findings suggest an opportunity for intervention during early adolescence to target AE among disengaged youth. Existing evidence suggests that opportunities for administering intervention programs during summer school sessions should be explored. Stoddard and Veliz (2019) found that 8th grade students who attended summer school had higher odds of binge drinking compared to those that never attended summer school (Stoddard & Veliz, 2019). School disengagement also mediated the positive association between summer school attendance and substance use. Taken together, our findings suggest summer school may be a potential outlet to reach early adolescent youth at risk for early onset drinking through modifiable targets such as AE.
At the neighborhood level, results revealed ADI (area deprivation index) was associated with higher positive AE. Previous studies have identified neighborhood disadvantage as a predictor of alcohol use among adolescents (Cambron et al., 2018). Our findings suggest that neighborhood-level factors are also correlated with the development of positive AE during early adolescence. Associations between neighborhood disadvantage and increased alcohol use have been linked via mechanisms such as diminished family functioning (Byrnes & Miller, 2012) and facilitation of access to deviant peers (Cambron et al., 2018). As such, future research is warranted to examine the mediating effects that other multi-level factors (i.e., family conflict, deviant peers) may play in this association between neighborhood deprivation and the formation of AE during early adolescence.
Negative Alcohol Expectancies
Our findings revealed that at the individual level exposure to negative life events was associated with greater negative AE. We posit that youth exposed to greater life adversity may also be more likely to witness negative impacts of drinking among adults in their immediate social environment, and as a result, be more likely to form negative AE. Previous studies also found that negative AE increase as a function of negative experiences with alcohol during adolescence (Pieters et al., 2014). While the present study sheds light on the impact of adverse childhood experiences on AE among early adolescence, there remains a need for future research to examine how negative AE impact alcohol use initiation among youth that have been exposed to adverse childhood experiences. At the family level, youth with a family history of alcohol abuse problems reported greater negative AE. It is posited that this association may be related with increased exposure to the negative consequences of alcohol these youth may have experienced. Nevertheless, there is a strong established association between family history of alcohol misuse and subsequent alcohol use risk (Yap et al., 2017). Future research is needed to examine the multiple pathways whereby the impact of family history on AE may serve as a source of risk or resilience to early alcohol use risk initiation.
At the peer level, our findings revealed that relational victimization and reputational aggression were associated with not only greater positive AE, but with higher negative AE as well. Future research is needed to determine potential pathways whereby AE may link distinct bullying roles (victims/perpetrators) to drinking outcomes during early adolescence. This knowledge can be used to develop and refine anti-bullying interventions, particularly in the middle school years, to target risk factors and leverage resilience factors during early adolescence.
Similarly, our findings suggest that greater involvement with rule-breaking and delinquent peers is directly associated with lower levels of negative AE during early adolescence. Studies have suggested that lack of appropriate parental monitoring and poor parenting practices may set the stage for increased affiliation with deviant peers (Cambron et al, 2018).
At the school level, findings indicated a positive correlation between school involvement and negative AE, while lower levels of negative AE were found among youth with greater school disengagement. These findings underscore the potential utility of targeting school disengagement and AE in multilevel school-based alcohol prevention interventions. Cummins and colleagues (2019) examined the associations between school connectedness, AE, and alcohol use among high school students and found that positive AE moderated the association between alcohol use and misuse, whereby school connectedness had a protective effect only among youth with lower positive expectancies (Cummins, Diep, & Brown, 2019). Notably, findings from systematic reviews have shown promising effects of multi-level school-based interventions on illicit drug use and smoking, with weaker evidence for drinking outcomes across adolescence (Hodder et al., 2017; Shackleton, 2016). It should also be noted that these reviews have focused on general adolescent samples, rather than early adolescence. Our results suggest implications for the potential utility of school-based interventions aimed to build school connectedness and address AE during middle school, when drinking rates remain relatively low. Existing high school-based intervention programs responding to and preventing bullying have included mentoring programs, and the use of peer support and peer leadership strategies to increase opportunities and build skills for students to participate in decision-making within the school. Implementing programs with similar components within middle schools can prove to be effective in reducing the risk of early alcohol use initiation among youth (Patton et al., 2003).
Lastly, at the neighborhood level, negative AE were higher among youth who endorsed living in safer neighborhoods and lower in neighborhoods with greater deprivation. Unsafe neighborhoods may also have higher unemployment rates and increased adolescent risk behavior. Unemployed adults are more likely to initiate or escalate substance use compared to those who are employed. This greater exposure to substance use may weaken adolescents’ beliefs about the potential harm of substance use, as well as provide more opportunities for experimentation, particularly in areas where there is a higher density of liquor stores (Lambert et al., 2004). Indeed, findings from systematic reviews have found levels of community drinking to be associated with increased alcohol use among adolescents (Jackson, Denny, & Amertunga, 2014)
When interpreting these findings, it’s important to consider the lack of clarity in the literature base between negative AE and early alcohol initiation (Smit et al., 2018). While studies have found negative AE are linked to lower alcohol use among youth, others have found the opposite to be true (Montes et al., 2019; Smit et al, 2018). One possible explanation for these varying results may be that adolescents who have never drunk alcohol may not be exposed to its negative consequences and, thus, may be less inclined to think about its adverse effects (Smit et al., 2018). Studies have also found that negative AE increase as a function of negative experiences with alcohol in later adolescence (Pieters et al., 2014). Future research is needed to clearly identify how, when, and under what contexts negative AE can serve as risk or protective factors for early alcohol use initiation.
Demographics and Alcohol Expectancies
Age and race-ethnicity were the key demographic differences associated with AE in the present sample. Specifically, older age was associated with greater positive and negative AE. This is consistent with previous studies, which suggest that AE increase with age as a result of greater exposure to alcohol (Murphy, Dufour, & Gray, 2021). Notably, alcohol use reduction interventions based on AE have demonstrated limited efficacy among adolescents that have already initiated alcohol use (Smit, 2018). As such, shifting the timing of prevention interventions to target early adolescence, when most youth have not begun drinking, may prove to be more effective.
Regarding race-ethnicity, higher negative AE and lower positive AE were found for non-Hispanic/Latinx Black and Hispanic/Latinx youth compared to non-Hispanic/Latinx White youth, with non-Hispanic/Latinx Other/Mixed youth reporting higher negative AE compared to non-Hispanic/Latinx Black and Hispanic/Latinx youth. While some studies have shown differences in AE development based on race-ethnicity (Chung et al., 2008), others have found initial differences between levels of AE then converge similarly in groups over time (Smit et al., 2018). Moreover, while children who identify as non-Hispanic/Latinx Black may report higher positive AE during early childhood compared to non-Hispanic/Latinx Whites, positive AE increase substantially in non-Hispanic/Latinx White children from third to fifth grade, compared only marginally among non-Hispanic/Latinx Black youth (Smit et al., 2018). Banks and colleagues (2017) found no initial racial difference in AE or consumption. However, race moderated the relationship between AE and alcohol use such that greater positive AE predicted alcohol use among non-Hispanic/Latinx White, but not non-Hispanic/Latinx Black youth (Banks & Zapolski, 2017). Future research should examine a broader set of sociocultural risk factors, such as discrimination, minority stress, and structural racism, which are more direct indicators of risk for alcohol use among Black youth (Banks et al., 2017).
Limitations
The primary limitation of this study was an inability to model causal associations between sociocultural factors and AE, which will require follow-up longitudinal studies. Additional instrument-related limitations were evident. Specifically, children were assessed with a brief alcohol expectancy questionnaire (AEQ-AB) rather than the full 90-item AEQ, which may have led to the low internal consistency and prevented the examination of various aspects of AE beyond the global positive and negative subscales (Brown et al., 1987). Internal consistency was found to be less than optimal for other measures as well, which was likely a function of the limited number of items across some scales. As is the case with most large-scale national studies, the need to cover a breadth of constructs within a limited time period often leads to the utilization of adapted versions of scales with a restricted number of items. However, it should be noted that these decisions were made carefully and collaboratively through field experts in the ABCD Study® Workgroups (i.e., ABCD® Mental Health, Culture & Environment Substance Abuse Workgroups) (Barch et al., 2018; Zucker et al., 2018; Lindahl et al., 2018). Another limitation of the current study is that, in contrast to previous investigations, we found family-level factors including family history of problematic alcohol use were not strongly associated with AE. We posit our findings may be related to how this variable was coded, whereby family history of alcohol use problems captured drinking problems related to various biological family members including aunts, uncles, half-siblings, as well as parents. Previous studies have focused solely on parental drinking problems, which may have a more distinct and immediate impact on AE among youth (compared to more distal family members) (Smit et al., 2018). Additionally, only familism and language use were assessed under the cultural domain of the present study. Culture (and in turn acculturation) has been theorized as a multidimensional construct consisting of cultural practices, values, and identity (Schwartz et al., 2010). While these multidimensional cultural constructs were not captured among youth during the two-year follow-up of the ABCD Study®, later waves are scheduled to collect this information, allowing for a more thorough understanding of how culture impacts AE during adolescence. Additionally, most of the measures used in the present study, with the exception of the language use scale, have not been tested for measurement invariance across race-ethnicity or other demographic factors. Notably, the Phenx Acculturation Scale, used to assess language use in this study, has been shown to have measurement invariance across Asian and Hispanic/Latinx adult samples (Kwok, 2022). However, differences between Hispanic/Latinx subgroups have also been documented (Roth, Musci, & Eaton, 2020). In sum, future research is needed to examine if these scales function similarly across diverse demographic groups or if psychometric distinctions exist. Finally, several variables that may be linked to AE, including parental AE and child perceptions of parental alcohol use, were not assessed in ABCD® data and thus could not be explored.
Future Directions
In addition to being important predictors of alcohol use, AE constitute important mediational mechanisms through which the influences of individual and environmental factors may impact underage drinking (Smit et al., 2018). Researchers examining the indirect effects of alcohol use via AE have found that AE function as mediators in the associations between different individual and environmental predictors and alcohol use (Smit et al., 20118). For instance, studies have shown that parental alcohol use is associated with adolescents’ alcohol use through AE (Jester et al., 2015). Individual-level factors such as psychopathology, alcohol-related cognitions, and personality factors have also been linked to alcohol use via AE (Smit et al., 2018). However, less is known about the mediating and moderating influence of sociocultural factors on the development of AE. For instance, school disengagement is associated with other multilevel factors including adverse childhood experiences, delinquent peers, and neighborhood safety (Bae, 2020; Lanza & Taylor, 2010; Ruiz, McMahon, & Jason, 2018). Future longitudinal research is also needed to further examine the pathways in which multilevel sociocultural factors may interact to impact AE among youth. This increased knowledge regarding the sequence in which the precursors of AE, AE, and alcohol use occur could have strong implications for prevention. Given that ABCD® is a longitudinal study with annual assessments, we will be able to follow this cohort and examine how these and other multi-level factors impact AE and subsequent alcohol use initiation over time. The need for developing and testing new theoretical models that incorporate technology, and most notably how social media influences the development of AE among youth are warranted.
There is also a need to further examine the predictors and developmental progression of AE across diverse populations (i.e., culture, ethnicities, religious backgrounds). To date, researchers have had difficulty explaining variation in adolescent drinking among racial-ethnic minoritized youth using traditional individual, family, peer, and environmental risk factors (Malone et al., 2012; Weaver et al., 2011). Thus, future research should continue to examine culturally relevant factors, cultural values, racial discrimination and ethnic identity, which may interact with other psychosocial factors to influence AE and subsequent drinking outcomes among racial-ethnic minority youth (Banks et al., 2017). Lastly, the interconnected nature between positive and negative AE and its impact on AE is complex in nature. As substantiated by the current study findings, associations between AE and known risk and protective factors for substance use are not clear-cut. While youth may endorse both positive as well as negative AE, the optimal combination that predict early alcohol use initiation remains ambiguous and an important area of inquiry in future research.
Conclusion
Prevention science has underscored the importance of using an ecological approach that simultaneously considers effects across the individual, family, peer, school, community, and cultural level when trying to understand the development of alcohol expectancies. Examining these factors during the developmental period of early adolescence is critical as this period is marked by the escalation to positive AE. This framework is particularly helpful in conceptualizing the integrated developmental risk and resilience factors that operate in the lives of youth.
Overall, study findings linked positive and negative AE to various sociocultural factors and found that the strongest associations were related to the cultural value of familism. To this end, we believe the present findings serve as a step toward understanding the potential constellation of sociocultural factors that may serve as targets for modifying AE during the middle school years. These findings also underscore the need for future research that integrates cultural factors into our understanding of alcohol-use risk and resilience among adolescents.
Supplementary Material
Supplementary Table 1. Description and original sources of ABCD Study measures used in the present study.
Supplementary Table 2. Comparison of sample demographics for participants with complete data in the sample analyzed and the sample with missing data.
Supplementary Table 3. Results from simple logistic regression models using positive and negative alcohol expectancies to predict missing status of variable.
Supplementary Table 4. Estimates from sensitivity analysis using minimum and maximum observed value for missingness in the three independent variables.
Supplementary Table 5. Unstandardized beta coefficients (B) and 95% confidence intervals (CI), and p-values.are reported for models using the sample with complete data for n = 5821 for the bivariate models for the zero-order correlations, i.e., models in which each independent variable was entered as the only predictor of alcohol expectancies (AE) while controlling for all covariates, and results are also reported for the full models in which all independent variables were entered simultaneously as predictors of AE while controlling for all covariates.
Acknowledgments
This publication was supported by the ABCD multi-site U grant. A full list of supporters is available at https://abcdstudy.org/federal-partners.html. In addition, M.S. was supported by an NIAAA Pediatric Loan Repayment Award and M.R.G was supported by an NIAAA Diversity Supplement U01AA021692-09S1.
Footnotes
Authors have no conflicts of interest to declare.
References
- Afifi TO, Taillieu T, Salmon S, Davila IG, Stewart-Tufescu A, Fortier J, …& MacMillan HL (2020). Adverse childhood experiences (ACEs), peer victimization, and substance use among adolescents. Child Abuse & Neglect, 106, 104504. 10.1016/j.chiabu.2020.104504 [DOI] [PubMed] [Google Scholar]
- Auchter AM, Hernandez Mejia M, Heyser CJ, Shilling PD, Jernigan TL, Brown SA, Tapert SF, & Dowling GJ (2018). A description of the ABCD organizational structure and communication framework. In Developmental Cognitive Neuroscience, 32, 8–15. 10.1016/j.dcn.2018.04.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bae SM Long-Term Effect of Adverse Childhood Experiences, School Disengagement, and Reasons for Leaving School on Delinquency in Adolescents Who Dropout. (2020). Frontiers in Psychology, Dec 14;11:2096. doi: 10.3389/fpsyg.2020.02096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Banks DE, & Zapolski TCBB (2016). Racial differences in the link between alcohol expectancies and adolescent drinking. Addictive Behaviors, 67, 34–37. 10.1016/j.addbeh.2016.12.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barch DM, Albaugh MD, Avenevoli S, Chang L, Clark DB, Glantz MD, …Sher (2018). Demographic, physical and mental health assessments in the adolescent brain and cognitive development study: Rationale and description. Developmental Cognitive Neuroscience, 32, 55–66. 10.1016/j.dcn.2017.10.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borrell LN, Elhawary JR, Fuentes-Afflick E, Witonsky J, Bhakta N, Wu A, Bibbins-Domingo K, …, & Burchard EG (2021). Race and Genetic Ancestry in Medicine - A Time for Reckoning with Racism. The New England journal of medicine, 384(5), 474–480. 10.1056/NEJMms2029562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown SA, Christiansen BA, & Goldman MS (1987). The alcohol expectancy questionnaire: An instrument for the assessment of adolescent and adult alcohol expectancies. Journal of Studies on Alcohol, 48(5), 483–491. 10.15288/jsa.1987.48.483 [DOI] [PubMed] [Google Scholar]
- Byrnes HF, & Miller BA (2012). The Relationship Between Neighborhood Characteristics and Effective Parenting Behaviors: The Role of Social Support. Journal of Family Issues, 33(12), 1658–1687. 10.1177/0192513X12437693 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cahill KM, Updegraff KA, Causadias JM, & Korous KM (2021). Familism values and adjustment among Hispanic/Latino individuals: A systematic review and meta-analysis. Psychological Bulletin, 147(9), 947–985. 10.1037/bul0000336 [DOI] [Google Scholar]
- Cambron C, Kosterman R, Catalano RF, Guttmannova K, & Hawkins JD (2018). Neighborhood, Family, and Peer Factors Associated with Early Adolescent Smoking and Alcohol Use. Journal of Youth and Adolescence, 47(2), 369–382. 10.1007/s10964-017-0728-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell JM, & Oei TP (2010). A cognitive model for the intergenerational transference of alcohol use behavior. Addictive Behaviors, 35(2), 73–83. 10.1016/j.addbeh.2009.09.013 [DOI] [PubMed] [Google Scholar]
- Caprara GV, Luengo Kanacri BP, Zuffianò A, Gerbino M, & Pastorelli C (2015). Why and How to Promote Adolescents’ Prosocial Behaviors: Direct, Mediated and Moderated Effects of the CEPIDEA School-Based Program. Journal of Youth and Adolescence, 44(12), 2211–2229. https://doi.org/10.1007 [DOI] [PubMed] [Google Scholar]
- Card NA, & Hodges EE (2008). Relational aggression and victimization during adolescence: A meta-analytic review of unique associations with popularity, peer acceptance, rejection, and friendship. School Psychology Quarterly, 23, 451–461. 10.1037/a0012769. [DOI] [PubMed] [Google Scholar]
- Cho MK, & Cho YH (2021). Do alcohol prevention programs influence adolescents’ drinking behaviors? A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 18(16). 10.3390/ijerph18168524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chung T, Hipwell A, Loeber R, White HR, & Stouthamer-Loeber M (2008). Ethnic differences in positive alcohol expectancies during childhood: The Pittsburgh Girls Study. Alcoholism: Clinical and Experimental Research, 32(6), 966–974. 10.1111/j.1530-0277.2008.00651.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colder CR, O’Connor RM, Read JP, Eiden RD, Lengua LJ, Hawk LW, & Wieczorek WF (2014). Growth trajectories of alcohol information processing and associations with escalation of drinking in early adolescence. Psychology of Addictive Behaviors, 28(3), 659–670. 10.1037/a0035271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Compton WM, Dowling GJ, & Garavan H (2019). Ensuring the Best Use of Data: The Adolescent Brain Cognitive Development Study. JAMA Pediatrics, 173(9), 809–810. 10.1001/jamapediatrics.2019.2081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook CR, Williams KR, Guerra NG, Kim TE, and Sadek S (2010). Predictors of bullying and victimization in childhood and adolescence: a meta- analytic investigation. School Psychology Quarterly, 25(25), 65–83. 10.1037/a0020149 [DOI] [Google Scholar]
- Cummins KM, Diep SA, & Brown SA (2019). Alcohol Expectancies Moderate the Association Between School Connectedness and Alcohol Consumption. Journal of School Health, 89(11), 865–873. 10.1111/josh.12829 [DOI] [PubMed] [Google Scholar]
- Dallen ER, Czar KA, Prather E, & Dyess C (2013). Relational Aggression and Victimization in College Students. Journal of College Student Development, 54(2), 140–154. 10.1353/csd.2013.0021 [DOI] [Google Scholar]
- Deng L, & Chan W (2017). Testing the Difference Between Reliability Coefficients Alpha and Omega. Educational and Psychological Measurement, 77(2), 185–203. 10.1177/0013164416658325 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Des Rosiers SE, Schwartz SJ, Zamboanga BL, Ham LS, & Huang S (2013). A cultural and social cognitive model of differences in acculturation orientations, alcohol expectancies, and alcohol-related risk behaviors among Hispanic college students. Journal of Clinical Psychology, 69(4), 319–340. 10.1002/jclp.21859 [DOI] [PubMed] [Google Scholar]
- Dick AS, Lopez DA, Watts AL, Heeringa S, Reuter C, Bartsch H, … & Thompson WK (2021). Meaningful associations in the adolescent brain cognitive development study. Neuroimage, 239, 118262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dube SR, Miller JW, Brown DW, Giles WH, Felitti VJ, Dong M, & Anda RF (2006). Adverse childhood experiences and the association with ever using alcohol and initiating alcohol use during adolescence. Journal of Adolescent Health, 38(4), 444–e1 10.1016/j.jadohealth.2005.06.006 [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Spinrad TL, & Knafo-Noam A (2015). Prosocial Development. In & Lamb VM, Garcia-Coll C, Lerner RM (Ed.), Handbook of Child Psychology (7th ed.). Wiley. 10.1002/9781118963418.childpsy315. [DOI] [Google Scholar]
- Eitle TMN, Wahl AMG, & Aranda E (2009). Immigrant generation, selective acculturation, and alcohol use among Latina/o adolescents. Social Science Research, 38(3), 732–742. 10.1016/j.ssresearch.2009.01.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK, Keller BT, & Levy R (2018). A fully conditional specification approach to multilevel imputation of categorical and continuous variables. Psychological Methods, 23, 298–317. doi: 10.1037/met0000148 [DOI] [PubMed] [Google Scholar]
- Ewing BA, Osilla KC, Pedersen ER, Hunter SB, Miles JNV, & D’Amico EJ (2015). Longitudinal family effects on substance use among an at-risk adolescent sample. Addictive Behaviors, 41, 185–191. 10.1016/j.addbeh.2014.10.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faggiano F, Minozzi S, Versino E, & Buscemi D (2014). Universal school-based prevention for illicit drug use. In Cochrane Database of Systematic Reviews, 12. John Wiley and Sons Ltd. 10.1002/14651858.CD003020.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Falzarano F, Moxley J, Pillemer K, & Czaja SJ (2021). Family Matters: Cross-Cultural Differences in Familism and Caregiving Outcomes. The journals of gerontology. Series B, Psychological sciences and social sciences, gbab160. Advance online publication. 10.1093/geronb/gbab160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Filipponi C, Petrocchi S, & Camerini AL (2020). Bullying and Substance Use in Early Adolescence: Investigating the Longitudinal and Reciprocal Effects Over 3 Years Using the Random Intercept Cross-Lagged Panel Model. Frontiers in Psychology, 11. 10.3389/fpsyg.2020.571943 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fosco GM, & Feinberg ME (2018). Interparental conflict and long-term adolescent substance use trajectories: The role of adolescent threat appraisals. Journal of Family Psychology, 32(2), 175–185. 10.1037/fam0000356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garavan H, Bartsch H, Conway K, Decastro A, Goldstein RZ, Heeringa S, … Jernigan, & Zahs D (2018). Recruiting the ABCD sample: Design considerations and procedures. Developmental Cognitive Neuroscience, 32, 16–22. 10.1016/j.dcn.2018.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez R, Thompson EL, Sanchez M, Morris A, Gonzalez MR, Feldstein Ewing SW, …& Zucker RA (2021). An update on the assessment of culture and environment in the ABCD Study®: Emerging literature and protocol updates over three measurement waves. Developmental Cognitive Neuroscience, 52. 10.1016/j.dcn.2021.101021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hemovich V, Lac A, & Crano WD (2012). Understanding early onset drug and alcohol outcomes among youth. Psychological Health & Medicine, 16(3), 249–267. 10.1080/13548506.2010.532560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry KL, Kelly, Knight E, & Thornberry TP (2012). School Disengagement as a Predictor of Dropout, Delinquency, and Problem Substance Use During Adolescence and Early Adulthood. Journal of Youth and Adolesnce,41(2), 156–166. 10.1007/s10964-011-9665-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hingson RW, Heeren T, & Winter MR (2006). Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Archives of pediatrics & Adolescent Medicine, 160(7), 739–746. 10.1001/archpedi.160.7.739 [DOI] [PubMed] [Google Scholar]
- Hodder RK, Freund M, Wolfenden L, Bowman J, Nepal S, Dray J, & Wiggers J (2017). Systematic review of universal school-based ‘resilience’ interventions targeting adolescent tobacco, alcohol or illicit substance use: A meta-analysis. Preventive Medicine, 100, 248–268. 10.1016/j.ypmed.2017.04.003 [DOI] [PubMed] [Google Scholar]
- Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, Jones L, & Dunne MP (2017). The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. The Lancet Public Health, 2(8), e356–e366. 10.1016/S2468-2667(17)30118-4 [DOI] [PubMed] [Google Scholar]
- Jackson N, Denny S, & Ameratunga S (2014). Social and socio-demographic neighborhood effects on adolescent alcohol use: a systematic review of multi-level studies. Social Science & edicine (1982), 115, 10–20. 10.1016/j.socscimed.2014.06.004 [DOI] [PubMed] [Google Scholar]
- Janssen T, Padovano HT, Merrill JE, & Jackson KM (2018). Developmental relations between alcohol expectancies and social norms in predicting alcohol onset. Developmental Psychology, 54(2), 281–292. 10.1037/dev0000430 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jester JM, Wong MM, Cranford JA, Buu A, Fitzgerald HE, & Zucker RA (2015). Alcohol expectancies in childhood: Change with the onset of drinking and ability to predict adolescent drunkenness and binge drinking. Addiction, 110(1), 71–79. 10.1111/add.12704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones BT, Corbin W, & Fromme K (2001). A review of expectancy theory and alcohol consumption. Addiction 96(1), 57–72). 10.1046/j.1360-0443.2001.961575.x [DOI] [PubMed] [Google Scholar]
- Kwok G (2022). What do we know about acculturation? A measurement invariance examination of acculturation domains between Asian and Latinx populations. Journal of Ethnic & Cultural Diversity in Social Work, 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lambert SF, Brown TL, Phillips CM, & Ialongo NS (2004). The relationship between perceptions of neighborhood characteristics and substance use among urban African American adolescents. American Journal of Community Psychology, 34(3–4), 205–218. 10.1007/s10464-004-7415-3 [DOI] [PubMed] [Google Scholar]
- Lanza HI, & Taylor RD (2010). Parenting in moderation: family routine moderates the relation between school disengagement and delinquent behaviors among African American adolescents. Cultural Diversity & Ethnic Minority Psychology, 16(4), 540–547. 10.1037/a0021369 [DOI] [PubMed] [Google Scholar]
- Law PC, Cuskelly M, & Carroll A (2013). Young people’s perceptions of family, peer, and school connectedness and their impact on adjustment. Journal of Psychologists and Counsellors in Schools, 23(1), 115–140. [Google Scholar]
- Lisdahl KM, Sher KJ, Conway KP, Gonzalez R, Feldstein Ewing SW, Nixon SJ, … & Heitzeg M (2018). Adolescent brain cognitive development (ABCD) study: Overview of substance use assessment methods. Developmental Cognitive Neuroscience, 32, 80–96. 10.1016/j.dcn.2018.02.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malone PS, Northrup TF, Masyn KE, Lamis DA, & Lamont AE (2012). Initiation and persistence of alcohol use in United States Black, Hispanic, and White male and female youth. Addictive Behaviors, 37(3), 299–305. 10.1016/j.addbeh.2011.11.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maniglio R (2017). Bullying and other forms of peer victimization in adolescence and alcohol use. Trauma, Violence & Abuse, 18(4), 457–473. 10.1177/1524838016631127 [DOI] [PubMed] [Google Scholar]
- Marmorstein NR (2019). Investigating associations between caffeinated beverage consumption and later alcohol consumption among early adolescents. Addictive Behaviors, 90, 362–368. 10.1016/j.addbeh.2018.11.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS, Faden VB, Zucker RA, & Spear LP (2009). A developmental perspective on underage alcohol use. Alcohol Research & Health, 32(1), 3. [PMC free article] [PubMed] [Google Scholar]
- Memmott-Elison MK, Holmgren HG, Padilla-Walker LM, & Hawkins AJ (2020). Associations between prosocial behavior, externalizing behaviors, and internalizing symptoms during adolescence: A meta-analysis. Journal of Adolescence, 80, 98–114. 10.1016/j.adolescence.2020.01.012 [DOI] [PubMed] [Google Scholar]
- Montes KS, Witkiewitz K, Pearson MR, & Leventhal AM (2019). Alcohol, tobacco, and marijuana expectancies as predictors of substance use initiation in adolescence: A longitudinal examination. Psychology of Addictive Behaviors, 33(1), 26–34. 10.1037/adb0000422 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy MA, Dufour SC, & Gray JC (2021). The association between child alcohol sipping and alcohol expectancies in the ABCD study. Drug and Alcohol Dependence, 221. 10.1016/j.drugalcdep.2021.108624 [DOI] [PubMed] [Google Scholar]
- Patton G, Bond L, Butler H, & Glover S (2003). Changing schools, changing health? Design and implementation of the Gatehouse Project. Journal of Adolescent Health, 33(4), 231–239. 10.1016/S1054-139X(03)00204-0 [DOI] [PubMed] [Google Scholar]
- Pieters S, Burk WJ, Vorst H. Van Der, Engels RC, & Wiers RW (2014). Impulsive and reflective processes related to alcohol use in young adolescents. Frontiers in Psychiatry, 5(May). 10.3389/fpsyt.2014.00056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prado G, Huang S, Maldonado-Molina M, Bandiera F, Schwartz SJ, de la Vega P, …& Pantin H (2010). An empirical test of Eco-developmental theory in predicting HIV risk behaviors among Hispanic youth. Health Education and Behavior, 37(1), 97–114. 10.1177/1090198109349218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roth KB, Musci RJ, & Eaton WW (2020). Refining acculturation measures for health research: Latina/o heterogeneity in the National Latino and Asian American Study. International journal of methods in psychiatric research, 29(4), 1–12. 10.1002/mpr.1844 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin DB (1987). Multiple Imputation for Nonresponse in Surveys. New York: John Wiley & Sons. [Google Scholar]
- Ruiz LD, McMahon SD, & Jason LA (2018). The role of neighborhood context and school climate in school-level academic achievement. American Journal of Community Psychology, 61(3–4), 296–309. [DOI] [PubMed] [Google Scholar]
- Sabogal F, Marín G, Otero-Sabogal R, Marín BV, & Perez-Stable EJ (1987). Hispanic familism and acculturation: What changes and what doesn’t? Hispanic Journal of Behavioral Sciences, 9(4), 397–412. [Google Scholar]
- Schwartz SJ, Unger JB, Zamboanga BL, & Szapocznik J (2010). Rethinking the concept of acculturation: Implications for theory and research. American Psychologist, 65(4), 237–251. 10.1037/a0019330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shackleton N, Jamal F, Viner RM, Dickson K, Patton G, & Bonell C (2016). School-Based interventions going beyond health education to promote adolescent health: Systematic Review of Reviews. Journal of Adolescent Health, 58(4), 382–396. 10.1016/j.jadohealth.2015.12.017 [DOI] [PubMed] [Google Scholar]
- Shih RA, Miles JNV, Tucker JS, Zhou AJ, & D’Amico EJ (2012). Racial/ethnic differences in the influence of cultural values, alcohol resistance self-efficacy, and alcohol expectancies on risk for alcohol initiation. Psychology of Addictive Behaviors, 26(3), 460–470. 10.1037/a0029254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smit K, Voogt C, Hiemstra M, Kleinjan M, Otten R, & Kuntsche E (2018). Development of alcohol expectancies and early alcohol use in children and adolescents: A systematic review. Clinical Psychology Review, 60, 136–146. 10.1016/j.cpr.2018.02.002 [DOI] [PubMed] [Google Scholar]
- Soto C, Unger JB, Ritt-Olson A, Soto DW, Black DS, Baezconde-Garbanati L (2011). Cultural values associated with substance use among Hispanic adolescents in southern California. Substance Use and Misuse, 46(10),1223–1233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spijkerman R, Van Den Eijnden RJJM, & Engels RCME (2005). Self-comparison processes, prototypes, and smoking onset among early adolescents. Preventive Medicine, 40(6), 785–794. 10.1016/j.ypmed.2004.09.025 [DOI] [PubMed] [Google Scholar]
- Stattin H, & Kerr M (2000). Parental monitoring: A reinterpretation. Child Development, 71(4), 1072–1085. 10.1111/1467-8624.00210 [DOI] [PubMed] [Google Scholar]
- Stoddard SA, & Veliz P (2019). Summer School, School Disengagement, and Substance Use During Adolescence. American Journal of Preventive Medicine, 57(1), e11–e15. 10.1016/j.amepre.2019.01.014 [DOI] [PubMed] [Google Scholar]
- Trucco EM, Colder CR, & Wieczorek WF (2011). Vulnerability to peer influence: A moderated mediation study of early adolescent alcohol use initiation. Addictive Behaviors, 36(7), 729–736. 10.1016/j.addbeh.2011.02.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Volkow ND, Koob GF, Croyle RT, Bianchi DW, Gordon JA, Koroshetz WJ, … Weiss SRB (2018). The conception of the ABCD study: From substance use to a broad NIH collaboration. Developmental Cognitive Neuroscience, 32, 4–7. 10.1016/j.dcn.2017.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Unger J, Ritt-Olson A, Teran L, Huang T, Hoffman BR,, Palmer P (2002). Cultural Values and Substance Use in a Multiethnic Sample of California Adolescents. Addiction Research & Theory.10(3), 257–279. [Google Scholar]
- Wade NE, Palmer CE, Gonzalez MR, Wallace AL, Infante MA, Tapert SF, Jacobus J, & Bagot KS (2021). Risk factors associated with curiosity about alcohol use in the ABCD cohort. Alcohol (Fayetteville, N.Y.), 92, 11–19. 10.1016/j.alcohol.2021.01.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weaver SR, Cheong J, MacKinnon DP, & Pentz MA (2011). Investigating Ethnic Differences in Adolescent Alcohol Use and Peer Norms Using Semi-Continuous Latent Growth Models. Alcohol and Alcoholism, 46(5), 620–626. 10.1093/alcalc/agr034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witherspoon DP, Daniels LL, Mason AE, & Smith EP (2016). Racial-ethnic Identity in Context: Examining Mediation of Neighborhood Factors on Children’s Academic Adjustment. American Journal of Community Psychology, 57(1–2), 87–101. 10.1002/ajcp.12019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yap M, Cheong T, Zaravinos-Tsakos F, Lubman DI, & Jorm AF (2017). Modifiable parenting factors associated with adolescent alcohol misuse: a systematic review and meta-analysis of longitudinal studies. Addiction (Abingdon, England), 112(7), 1142–1162. 10.1111/add.13785 [DOI] [PubMed] [Google Scholar]
- Zimmer-Gembeck MJ, & Collins WA (2003). Autonomy development during adolescence. In Adams GR & Berzonsky M (Eds.), Blackwell handbook of adolescence (pp. 175–204). Oxford, UK: Blackwell Publishers [Google Scholar]
- Zucker RA, Donovan JE, Masten AS, Mattson ME, & Moss HB (2008). Early developmental processes and the continuity of risk for underage drinking and problem drinking. Pediatrics, 121(Suppl. 4). 10.1542/peds.2007-2243B [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table 1. Description and original sources of ABCD Study measures used in the present study.
Supplementary Table 2. Comparison of sample demographics for participants with complete data in the sample analyzed and the sample with missing data.
Supplementary Table 3. Results from simple logistic regression models using positive and negative alcohol expectancies to predict missing status of variable.
Supplementary Table 4. Estimates from sensitivity analysis using minimum and maximum observed value for missingness in the three independent variables.
Supplementary Table 5. Unstandardized beta coefficients (B) and 95% confidence intervals (CI), and p-values.are reported for models using the sample with complete data for n = 5821 for the bivariate models for the zero-order correlations, i.e., models in which each independent variable was entered as the only predictor of alcohol expectancies (AE) while controlling for all covariates, and results are also reported for the full models in which all independent variables were entered simultaneously as predictors of AE while controlling for all covariates.