

Abstract
Electronic health records (EHRs) constitute vital statistics, current health condition, ongoing therapies, and patient data; hence, their interoperability could be useful for epidemiologic and clinical research. Fast Healthcare Interoperability Resources (FHIR) and blockchain are currently “in-use” and tested for exchange of such data. The annual scientific production of publications for both FHIR and blockchain shows steady growth. The data interoperability and electronic data interchange have been introduced in the field of EHR in 2020, hence inferring that data interoperability is relatively a new domain. The thematic mapping suggested “interoperability” of EHR is well-developed and important for the structure of the research field.
Keywords: Data extraction, electronic health records, healthcare, interoperability
INTRODUCTION
Background
Data are the main component, which is processed to correlate and explore new findings, trends and thereby predict the outcome. In the health-care domain, the two basic sources of data are the patient and drug. Globally, many “Big Data” research projects are working on different approaches for processing patient records, and it is anticipated that the future of healthcare will be based on such projects.[1] Electronic health records (EHRs) are digital forms of patient records and source of valuable data, which are considered as major digital revolution in the healthcare domain and are currently in the phase of “in-process” for deployment as a fully interoperable record.[2,3]
Electronic health record: Datasets for secondary analysis
Initially, EHR was introduced for the purpose of invoicing but now its horizon has extended beyond, to capture vital statistics, health condition, ongoing therapies, and other patient data.[4] National Academies of medicine has also indicated that multiple core functionalities of EHR such as capturing and exchange of health information aid in making optimal clinical/treatment decision, providing patient support, and generating epidemiology report.[5] The types of data that can be mined from EHRs are unique patient identifiers, diagnosis, demographics, therapies, laboratory findings, procedures, adverse events, and vital signs. The standardization of EHR templates and its implementation could be useful for epidemiologic and clinical research. For that to work, the EHRs need to have functional interoperability.[4] An effective functional interoperability needs to follow a standard set of requirements: the ability to exchange information with registry from any provider; and this exchange does not necessitate extensive customization of the EHR or the registry system.
Once the EHR becomes interoperable, more data will be accessible to the healthcare stakeholders for analysis which will be helpful to draw conclusions that can be implemented in clinical practice. This will improve the efficiency of health-care system. The central database which will be available with the help of interoperability would function as a huge information center for providers, researchers, and organizations. Various medical standards are being evaluated to develop an interoperable and consistent medical system.[6]
Fast health interoperability resources (FHIR)
Health Level Seven has introduced FHIR with standard definitions of common healthcare terms as its basic units. Many studies have evaluated the potential of FHIR for the integration of data obtained from hospitals into regional health information systems.[6]
Since FHIR alone does not allow a unified access to EHR data from apps, the Harvard-based Computational Health Informatics Program group developed EHR specifications on open application programming interfaces and produced Substitutable Medical Apps and Reusable Technologies app platform.[7]
Blockchain
Blockchains are information repositories that are distributed, regionalized, and secured using different cryptographic primitives.[8] Blockchain-based EHR is an efficient and cost-effective tool for sharing EHR data.[9,10] This collaboration is a patient-centric approach which provides fast and secure data access to physicians and researchers, hence resulting in a better treatment approach.[10]
Blockchain technology paired with FHIR
In the current scenario, vendors limit the patient access and thus prevent patient engagement and information exchange. Blockchain system paired with FHIR could be a workable solution to address this issue.[8] In 2018, Zhang et al. worked on secure and scalable functionality of blockchain-based integrated system called FHIRChain. The FHIRChain adheres with the Office of the National Coordinator for Health Information Technology constraints for the exchange of clinical data among patients and health-care providers. The FHIRChain consists of unique identifying tags along with design tokens which facilitates the data resource exchange in a verifiable way without uploading the data in a centralized database.[11]
Objectives
The objective of this study is to provide a bibliometric analysis of publications on FHIR and blockchain for EHR processing. Furthermore, a proposal for establishing a central database for EHR to extract different data components has also been presented.
METHODS
Search strategy and data selection
A structured search strategy was adopted to identify publications related to EHR, FHIR, and blockchain. Two search strings were created using keywords: “Electronic Health Records” and “Fast Healthcare Interoperability Resources” (denoted as “string A”); and “Electronic Health Records” and “Block chain” (denoted as “string B”).
String A: “Electronic Health Records” + “Fast Healthcare Interoperability Resources”
String B: “Electronic Health Records” + “Block chain.”
The publication type considered for the literature search was limited to articles, books, editorial, conference, notes, and reviews from the last 10 years (2013 to 2022). The search results from both the search strings were analyzed to understand the publication trends in EHRs in association with FHIR and blockchain. Further, the bibliometric analysis was performed using Bibliometrix software by R-studio to analyze the trends with reference to interoperability of EHR using FHIR and blockchain. Scopus was the database used to conduct this bibliometric analysis. No other databases were used for the same.
Bibliometric analysis
The bibliometric indicators used in this paper include annual scientific publications, country collaboration, leading institutional collaboration, thematic evaluation of keywords, and thematic map of EHRs research.
The annual citations for FHIR and Blockchain during the study period were 302 and 758 respectively [Table 1]. Data were extracted to evaluate the annual scientific output, thematic map, thematic evolution map of the keywords, three field plot and most relevant keywords.
Table 1.
Quantitative analysis of literature search results obtained from scopus
| Description | Results | |
|---|---|---|
|
| ||
| Fast healthcare interoperability resources | Block chain | |
| Time span | 2013–2022 | 2016–2022 |
| Sources (journals, books, etc.) | 116 | 397 |
| Documents | 302 | 758 |
| Average years from publication | 2.82 | 1.82 |
| Average citations per documents | 6.616 | 15.37 |
| Average citations per year per document | 1.317 | 3.72 |
| References | 7655 | 22,703 |
| Document types | ||
| Article | 135 | 305 |
| Book | 1 | 1 |
| Book chapter | 24 | 44 |
| Conference paper | 127 | 315 |
| Conference review | 4 | 27 |
| Editorial | 1 | 2 |
| Note | 3 | 8 |
| Review articles | 7 | 50 |
| Contents of the document | ||
| Keywords plus | 1647 | 2909 |
| Author’s keywords | 722 | 1349 |
| Author related information | ||
| Authors | 1186 | 2235 |
| Author appearances | 1619 | 2866 |
| Authors of single-authored documents | 15 | 32 |
| Authors of multi-authored documents | 1171 | 2203 |
| Authors collaboration | ||
| Single-authored documents | 24 | 61 |
| Documents per author | 0.255 | 0.339 |
| Authors per document | 3.93 | 2.95 |
| Co-authors per documents | 5.36 | 3.78 |
| Collaboration index | 4.21 | 3.16 |
| Annual growth rate (%) | 20.85 | 90.30 |
| Annual total citation (n) | ||
| 2013 | 2 | - |
| 2014 | 1 | - |
| 2015 | 12 | - |
| 2016 | 13 | 2 |
| 2017 | 33 | 18 |
| 2018 | 31 | 57 |
| 2019 | 62 | 125 |
| 2020 | 53 | 214 |
| 2021 | 84 | 247 |
| 2022 | 11 | 95 |
n=Total number of citations in a year
The exploratory qualitative analysis was carried out using the word cloud for text analysis [Figure 1]. In the data visualization of word cloud, larger or distinguished word represents the frequent appearance of that word in analyzed documents.[12] The objective of the word cloud is to present important terms in the form of a visual summarization.
Figure 1.

Exploratory qualitative analysis using word cloud (a) Fast Healthcare Interoperability Resources (FHIR) (b) Block chain
RESULTS
The results of the literature search yielded 302 documents for search string A and 758 documents for search string B. The time span considered for search string A and search string B was from 2013 to 2022 and 2016 to 2022, respectively. For search string B, the time span is three years shorter because there were no studies were published before 2016. The final analysis included articles (search string A = 135; search string B = 305), book (search string A = 1; search string B = 1), book chapters (search string A = 24; search string B = 44), conference papers (search string A = 127; search string B = 315), conference review (search string A = 4; search string B = 27), editorials (search string A = 1; search string B = 2), notes (search string A = 3; search string B = 8), and review articles (search string A = 7; search string B = 50) [Table 1].
Data analysis
Table 1 enlists the total number of records obtained using the two different search strings. The predominant publication type for search string A and search string B were research articles (n = 135, 44.70%) and conference papers (n = 315, 41.55%), respectively. This was followed by conference papers (n = 127; 42.05%) and book chapters (n = 24; 7.9%) for search string A and research articles (n = 305; 40.23%) and book chapters (n = 44; 5.80%) for search string B.
As per the results, the average year from publication (time for publishing) for search string A is 2.82 years and 1.82 years for search string B; the average citation per document for search string A and search string B was 6.616 and 15.37 respectively; and average citation per year per document was 1.37 for search string A and 3.72 for search string B, inferring that blockchain with EHR was more researched area.
Annual scientific production
Table 1 presents the publication trend in EHR and FHIR from 2013 to 2022 and EHR and blockchain from 2016 to 2022. The number of articles published annually in both FHIR and blockchain topics showed steady growth during the period used in the analysis.
The number of publications remained the same number from 2013 to 2014 for EHR and FHIR. The number of publications increased between 2014 and 2015 but showed a very slight increase in number of publications during the next year. A sharp increase in number of publications was observed till 2017 which was followed by slight decrease in the subsequent year (2018). A similar trend of sharp increase followed by a slight decrease in the number of publications was observed from 2018 to 2020. Overall, the publication trend in EHR with FHIR topic could be described as plunged one year followed by slight change in number of publications the next year, and this trend continues.
Overall, a dramatic rise in the number of publications has been observed from 2016 to 2020, for EHR and blockchain, followed by a sharp increase for the next 1 year. As compared to FHIR + EHR, blockchain + EHR became a predominant topic and more research has been done on this during the analyzed period.
Leading contributing countries
The United States of America (USA) holds the top position in terms of producing the most number of documents in both FHIR and blockchain topics. Asia also contributed to the highest number of documents for EHR + blockchain. Other regions contributing to the scientific publications in South America, the United Kingdom (UK), and Australia in EHR + FHIR and South America, UK, Africa, and Australia in the field of EHR + blockchain.
Leading institutional collaboration
The analysis based on institutional collaboration to develop publications in the field of EHR + FHIR and EHR + Blockchain showed that the Harvard Medical School is the leading contributor and worked in collaboration with the Boston’s children group, Vanderbilt University Medical center, and Mayo clinic in the field of EHR + FHIR. On the other hand, only two institutions, Taif University and Monash University worked on EHR + blockchain publications.
Country collaboration network
The collaboration among the top contributing countries in EHRs is presented in Figure 2. The size of the node represents the country’s contribution in publications. According to the data, USA had the highest number of scientific collaborations in the field of EHR + FHIR [Figure 2a]. On the other hand, the publications in EHR + blockchain had collaborations among various countries such as the USA, India, China, UK, and many more [Figure 2b].
Figure 2.
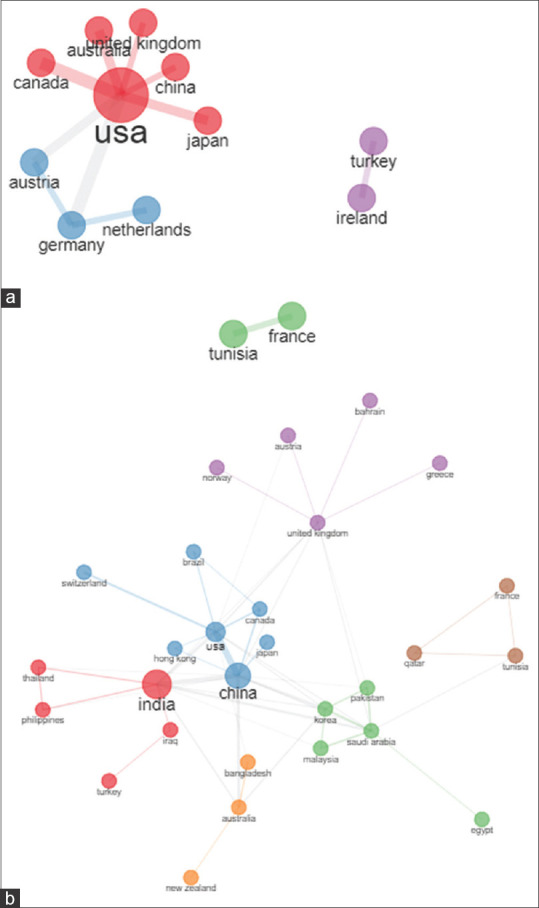
Country Collaboration Network: (a) EHR and Fast Healthcare Interoperability Resources (FHIR) publications and interoperability (b) EHR and Block chain publications and interoperability. EHR = Electronic health record
Thematic evolution map of keywords
The evolution of the thematic areas in EHRs over the last 10 years for search string A remained constant from 2013 to 2022; however, for search string B, the keyword was seen to be constant till 2021. It was observed that the term FHIR was introduced in 2019 unlike blockchain (introduced in 2016). The keyword data interoperability, data mining, and electronic data interchange were introduced in the field of EHR in 2020, hence inferring that data interoperability is relatively a new domain.
Thematic map of electronic health records research
The thematic mapping is based on the frequency of co-occurrence and co-analysis of the keywords. Further, the map is divided into four quadrants, each representing the status of the keyword in research field. The quadrants are defined as follows:
Motor themes
These are presented in upper-right quadrant and are well-developed and important for the structure of the research field.
Niche themes
Placed in upper-left quadrant, denoting that the field is well developed but have a limited or marginal role.
Emerging or declining theme
The lower left quadrant present weakly developed themes with a marginal role in the field.
Transversal theme
The lower right quadrant denotes themes that are not developed but are important for the research field.
The thematic map depicts the overall picture of both the keywords as per their importance and development in scientific research. The thematic map suggests that the interoperability aspect of FHIR is well-developed and significant for the structure of research field [Figure 3a]; whereas blockchain for EHR has a marginal role in research field, although it is well-developed [Figure 3b].
Figure 3.
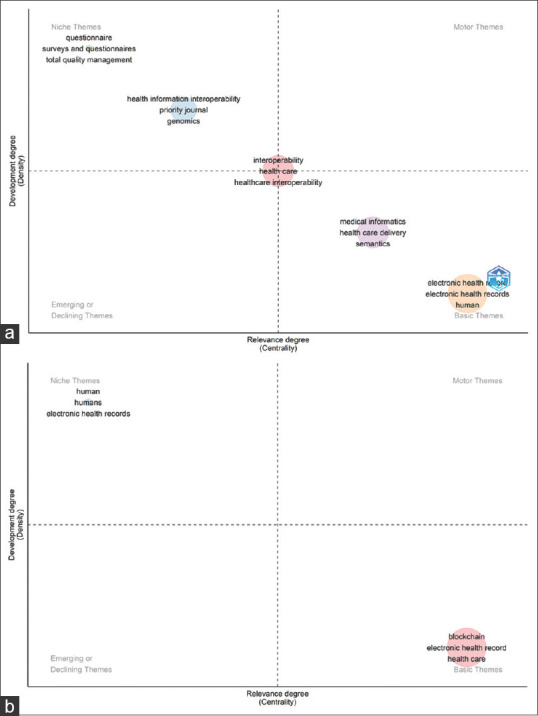
Thematic map: (a) EHRs research with FHIR (2013–2022) (b) EHRs research with Block chain (2016–2022). EHRs = Electronic Health Record
DISCUSSION
Principle findings
The published research related to EHR using different technologies in the last 10 years analyzed using a bibliometric scheme and analysis revealed that the publications and citation trend is increasing in the field of EHR interoperability.
Limitation
The results and inference of this study are limited to only one database (Scopus). Further analysis in other databases should be conducted to draw conclusions.
Future scope
The interoperability is not only the exchange of data but also the use of the data. Research has demonstrated that there is a need of standardized coded data for interpretation. Although the EHR interoperability is a multifaceted and ongoing task, it will be a significant tool in health care in terms of coordinating between multidisciplinary team of clinicians, data extraction, research, and decision-making. The data obtained from different sources could be managed using a secure network where it can further be analyzed, processed, and used by researchers, physicians, and healthcare workers. The data obtained from all the EHRs could be used to extract epidemiology data, adverse drug reactions, and prescribing trends. This can only be possible with a secure, consistent, and effective technical tool which can exchange and identify the data accurately among two networks. By achieving this, the patient can access and share their medical history with a new provider. This approach is not only patient-centric but interoperability of EHR could improve the efficiency of health-care system, cross-organizational communication, and explore the new research aspects.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The editorial review was provided by Dr. Shridevi Venkataramani (Tata Consultancy Services, India). No funding was received toward the development of this article.
REFERENCES
- 1.Agrawal R, Prabakaran S. Big data in digital healthcare:Lessons learnt and recommendations for general practice. Heredity (Edinb) 2020;124:525–34. doi: 10.1038/s41437-020-0303-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jabali AK, Waris A, Khan DI, Ahmed S, Hourani RJ. Electronic health records:Three decades of bibliometric research productivity analysis and some insights. Inform Med Unlocked. 2022;29:100872. [Google Scholar]
- 3.Kruse CS, Stein A, Thomas H, Kaur H. The use of electronic health records to support population health:A systematic review of the literature. J Med Syst. 2018;42:214. doi: 10.1007/s10916-018-1075-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Casey JA, Schwartz BS, Stewart WF, Adler NE. Using electronic health records for population health research:A review of methods and applications. Annu Rev Public Health. 2016;37:61–81. doi: 10.1146/annurev-publhealth-032315-021353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ehrenstein V, Kharrazi H, Lehmann H, Taylor CO. Obtaining data from electronic health records. In: Gliklich RE, Leavy MB, Dreyer NA, editors. Tools and Technologies for Registry Interoperability, Registries for Evaluating Patient Outcomes:A User's Guide. 3rd ed. Addendum. 2. Rockville (MD): Agency for Healthcare Research and Quality (US); 2019. [[Last accessed on 2022 Dec 01]]. Ch. 4. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551878/ [Google Scholar]
- 6.Lazarova E, Mora S, Rubartelli P, Cosolito Vitale A, Pareto L, Maggi N, et al. Integrating an electronic health record system into a regional health information system:An HL7 FHIR architecture. Stud Health Technol Inform. 2021;281:1087–8. doi: 10.3233/SHTI210357. [DOI] [PubMed] [Google Scholar]
- 7.Bloomfield RA, Jr, Polo-Wood F, Mandel JC, Mandl KD. Opening the Duke electronic health record to apps:Implementing SMART on FHIR. Int J Med Inform. 2017;99:1–10. doi: 10.1016/j.ijmedinf.2016.12.005. [DOI] [PubMed] [Google Scholar]
- 8.Hylock RH, Zeng X. A blockchain framework for patient-centered health records and exchange (HealthChain):Evaluation and proof-of-concept study. J Med Internet Res. 2019;21:e13592. doi: 10.2196/13592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mayer AH, da Costa CA, Righi RD. Electronic health records in a Blockchain:A systematic review. Health Informatics J. 2020;26:1273–88. doi: 10.1177/1460458219866350. [DOI] [PubMed] [Google Scholar]
- 10.Dubovitskaya A, Baig F, Xu Z, Shukla R, Zambani PS, Swaminathan A, et al. ACTION-EHR:Patient-Centric blockchain-based electronic health record data management for cancer care. J Med Internet Res. 2020;22:e13598. doi: 10.2196/13598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhang P, White J, Schmidt DC, Lenz G, Rosenbloom ST. FHIRChain:Applying blockchain to securely and scalably share clinical data. Comput Struct Biotechnol J. 2018;16:267–78. doi: 10.1016/j.csbj.2018.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ramlo S. Using word clouds to visually present Q methodology data and findings. J Hum Subjectivity. 2011;9:95–108. [Google Scholar]