

Abstract
This study aimed to assess the safety of complex inferior vena cava (IVC) filter retrieval techniques through a systematic review of published literature.
Using PubMed, a systematic review was conducted in line with the 2020 Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines to identify articles published through April 2020 that reported on complex IVC filter retrieval techniques in >5 patients. Case reports, review papers, and studies that did not report on primary outcomes or variables of interest were excluded. Risk of bias was assessed using a modified Newcastle–Ottawa Quality Assessment scale. Pooled success and complication rates were calculated for the overall number of complex retrieval attempts as well as for each filter type and each complex retrieval method.
Sixteen fair-quality and three good-quality studies met the inclusion criteria, with 758 patients (428 female) who had undergone 770 advanced retrieval attempts. The mean age of the patients was 46.5 ± 7.1 years (range: 14.1–90), and the mean dwell time was 602.5 ± 388.6 days (range: 5–7336). Regarding filters, 92.6% (702/758) were retrievable and 7.4% (56/758) were permanent. Indications for complex retrieval included the failure of standard retrieval (89.2%; 676/758) and tilting or embedding in the caval wall (53.8%; 408/758); 92.6% (713/770) of the advanced retrieval attempts were successful. The pooled success rate was 92.0% (602/654) for retrievable filters and 96.4% (53/55) for permanent filters (P = 0.422). Only 2.8% (21/758) of patients experienced major complications, and the major complication rate was not significantly associated with filter type (P = 0.183).
Advanced techniques for IVC filter retrieval appear safe for the retrieval of retrievable filters and certain permanent filters, with a low short-term major complication rate. Further studies on complex retrieval techniques used to remove permanent filters should be conducted to clarify their safety with respect to filter type.
Keywords: Advanced filter retrieval, complex filter retrieval, pulmonary embolism, thromboembolism, venous thromboembolism
Main points
• Advanced retrieval techniques demonstrated promising pooled success rates of 92.0% and 96.4% for retrievable and permanent filters, respectively.
• Advanced retrieval techniques demonstrated a low pooled short-term major complication rate of 2.8%, and no patient mortality resulting from procedure-related complications was reported.
• Further studies on complex retrieval techniques used to remove permanent filters should be conducted to clarify their safety with respect to filter type.
Following a 1998 clinical trial that demonstrated the short-term efficacy of inferior vena cava (IVC) filters in preventing pulmonary embolism (PE), the implantation rate of IVC filters increased for years before peaking in 2010.1,2 These filters are not always intended for permanent use, and in 2010, the US Food and Drug Administration recommended the removal of retrievable IVC filters that were no longer required, reinforcing this recommendation in 2014.3 Although Brown et al.4 reported an increase in the 1-year retrieval rates of IVC filters from 14% to 24%, the majority of implanted filters are not retrieved.5 Many factors may contribute to low retrieval rates, including the difficulty of removing filters. Ray et al.6 reported that approximately 15% of filter retrievals were not successful using standard techniques in a population of closely followed patients. Reported causes for standard retrieval failures include tilted, damaged, or thrombosed filters.6,7
Furthermore, not all patients are closely followed up after filter placement, leading to longer dwell times before an attempted retrieval and increased technical complexity during retrieval. In a study of patients with a mean dwell time of 685 days, 60% were referred for complex retrievals, which require the use of techniques and equipment beyond standard snares or dedicated retrieval devices.8 Complex IVC filter retrieval techniques using modified loop snares, forceps, and lasers have been described in the literature. However, further analysis is needed to understand the current usage and safety of these techniques. Herein, we conduct a systematic review of existing literature to assess the safety of complex IVC filter retrievals.
Methods
A systematic review was conducted in line with the 2020 Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines of peer-reviewed literature on complex or advanced retrieval techniques attempted on patients with implanted IVC filters. This study qualifies as “non-human subject research” as per the protocol set by the institutional review board (IRB) at our institution and was thus excluded from a formal IRB review.
Search strategy and study selection
A structured PubMed search was performed for literature published up to and including April 2020. The search performed was as follows: “[(IVC filter retrieval) OR (IVC filter retrieval)] AND [(advanced) OR (advanced technique) OR (complex) OR (complex retrieval) OR (forceps) OR (loop) OR (laser)].” Two authors (NK and KB) used Rayyan QCRI software (Doha, Qatar) to systematically screen article titles and abstracts independently.9 Decisions on studies eligible for a full-text review were made mutually after discussion.
Data extraction
After the preliminary screening of titles and abstracts, the full texts were reviewed for definitive inclusion. The primary outcomes of interest were the number of successful attempts, failed attempts, and major complications. Other variables of interest included demographic data, filter dwell times, filter types, retrieval indications, and retrieval methods. In this review, days are the units used to report dwell time. If studies reported dwell time in months or years, we converted these data to days (365.25 days: 1 year: 12 months). Authors NK and KB independently collected primary outcomes and other variables of interest using Microsoft Excel (Microsoft, Redmond, WA, USA) to determine which study results to include in the data synthesis and to tabulate results. During the full-text screening, bibliography reviews were conducted to find additional relevant publications. Once identified, their full texts were subsequently reviewed. Full texts were also screened for overlapping patient cohorts if study authors were listed in multiple publications. When overlapping cohorts were identified, only the most recent publication was included. The publications in this systematic review provided measures of central tendencies instead of individual patient data; thus, weighted averages were used based on sample size.
Eligibility criteria
This review includes studies reporting the retrieval of IVC filters involving a complex retrieval technique in >5 patients. A complex or advanced technique was defined as any technique other than one involving routine venous access with a snare for the filter hook (apex) or one involving a dedicated retrieval device. Advanced techniques used alone, in combination with other advanced techniques, in combination with standard techniques, or subsequent to failure with standard techniques were all included in this review. Case reports were excluded from this review due to the increased risk of selection bias, and review papers were excluded because of the lack of unique retrieval data. Both retrospective and prospective studies were included. Studies that did not provide specific patient demographics, filter dwell times, filter type, retrieval method, success rate, or major complication rate were excluded. Studies were grouped by filter type and retrieval method.
Definition of outcome measures
Incidence of successful retrievals and incidence of major complications were the primary outcomes of interest. If study authors reported multiple advanced retrieval failures followed by a retrieval success, all attempts were considered. Three studies reported failed advanced retrieval attempts prior to successful advanced retrieval but did not quantify previous advanced attempts or detail which methods were used.10,11,12 As a result, only the final retrieval attempt was considered from these three studies in this review. Study authors also reported complications only for final retrieval attempts; thus, complications following previous failed retrieval attempts were not reported in the complication rate. Successful retrieval was defined as the removal of at least the body of the filter. If another filter part was not removed, such as a tip, hook, barb, or strut, the retrieval attempt was deemed successful but also included as a major complication. Major complications were defined according to the Society of Interventional Radiology (SIR) Clinical Practice guidelines and were assessed using postretrieval IVC imaging in all patients.13 These complications included death, permanent adverse sequelae, prolonged hospitalization, additional therapy, and an unplanned increase in the level of care. Fractured unretrieved parts of IVC filters pose the risk of filter-related morbidity in patients and therefore qualified as potential severe adverse sequelae.14,15 Complications that required only nominal therapy, such as overnight observation, were not deemed major under these guidelines. The number of successful retrievals was summed across all studies. A pooled success rate was calculated using the total number of complex retrieval attempts, including past failed attempts. Similarly, the number of major complications were summed across all studies. However, the major complication rate was computed without the inclusion of past failed attempts because most study authors did not report data on complications following previous attempts. Additional success and complication rates were calculated for permanent and retrievable filters as well as for each complex retrieval method. Patient-level data were not available in the majority of studies, precluding the computation of adjusted effect measures.
Statistical analysis
Descriptive statistics for age and dwell time are presented as mean ± standard deviation. For categorical variables, statistics are presented as percentage (%) and frequency. Success and complication rates for permanent and retrievable filters were compared using two-sided Fisher’s exact tests. Separate rates for permanent and retrievable filters were identified in all but one study, which was included in the overall success and complication rates but excluded from the filter type statistical analysis.16 Success rate was also compared between the three most common retrieval methods (forceps, laser, and loop-snare) using a two-sided Fisher’s exact test. Two studies did not report the retrieval method used in their retrieval failures and were thus not included in the filter technique statistical analysis.10,17 Results were considered significant with P < 0.05. The analysis was performed using SPSS software, version 25 (IBM, Armonk, NY, USA).
Risk-of-bias assessment
Authors NK and KB independently assessed all included studies for risk of bias using a modified Newcastle–Ottawa Quality Assessment scale (NOS) for cohort studies. Modifications included use of a 48-h follow-up time cut-off in line with the SIR Clinical Practice guideline definition of prolonged postprocedural hospitalization of >48 h.13 Further modification included requiring studies to report on consecutive eligible patients to receive a star for the representativeness of their exposed cohort, thus identifying studies with an increased risk of reporting bias. Studies were deemed good quality if they received at least seven of nine possible stars, fair quality with between four and six stars, and low quality with three or fewer stars.
Results
Studies meeting inclusion criteria
In total, 152 unique studies were identified, 147 through PubMed and 5 through a bibliography review (Figure 1). Of these studies, 58 were deemed eligible for a full-text review, including all five studies identified through the bibliography review. After the full-text review, 19 studies were included in this analysis. Seventeen studies were retrospective reviews, and two were prospective. A summary of these studies is provided in Table 1a, 1b. All included studies contained advanced retrieval-specific data on patient age, sex, filter dwell time, success rate, and complication rate. Filter types were provided in all but one study. Six additional studies met the inclusion and exclusion criteria of this review but included overlapping patient cohorts with the 19 included studies.15,18,19,20,21,22 These studies were therefore excluded.
Figure 1.
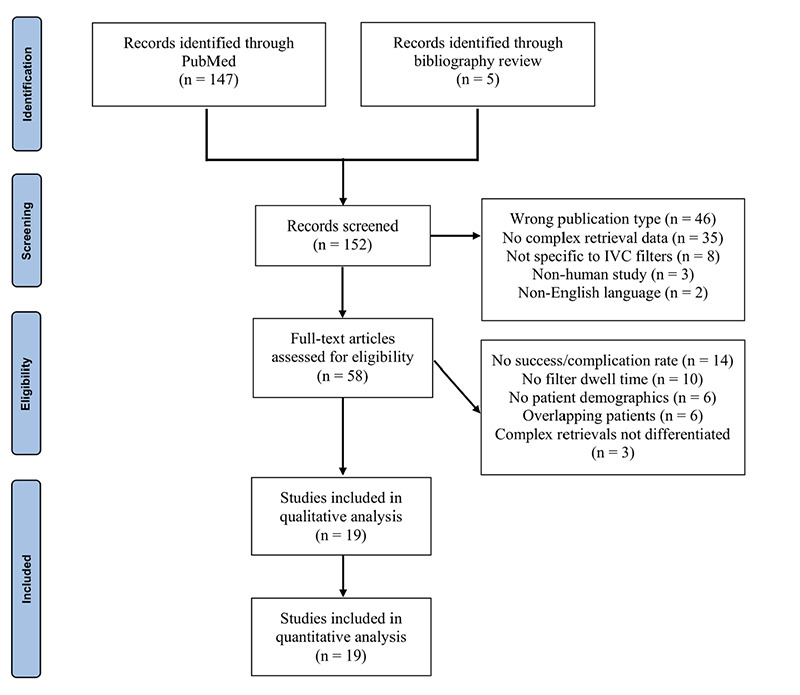
Preferred reporting items for systematic review and meta-analysis flowchart documenting the selection process for articles included in this systematic review. IVC, inferior vena cava.
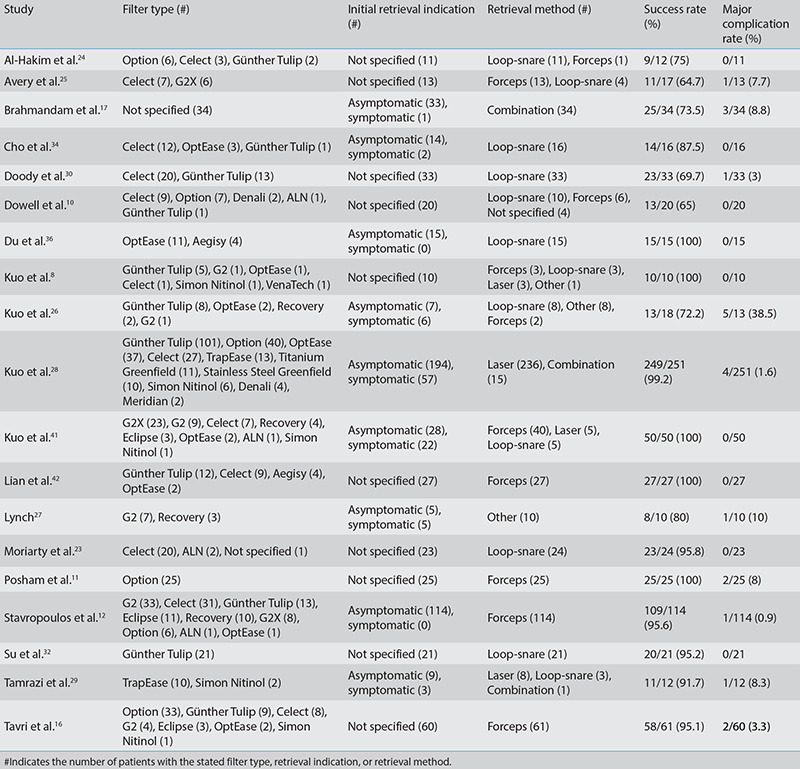
Table 1a. Summary of included studies.
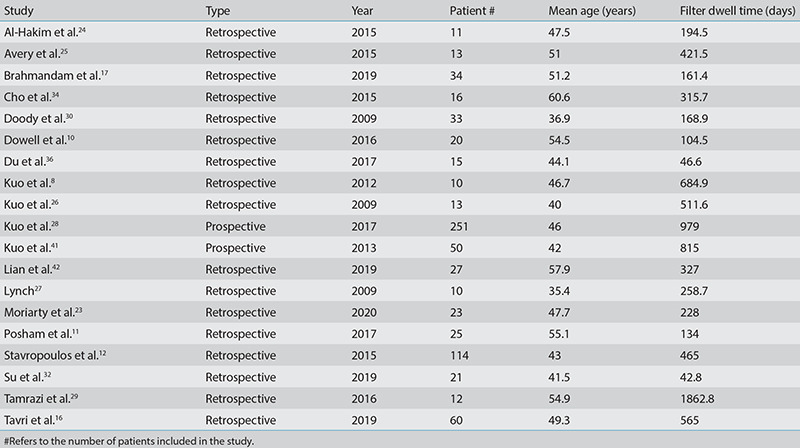
Table 1b. Summary of included studies.
Demographics and filter data
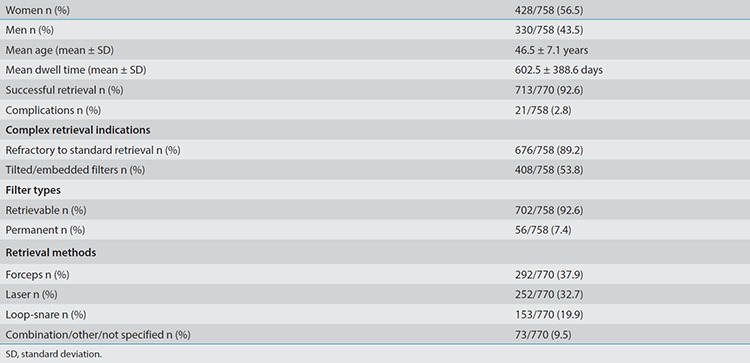
Among the 19 studies in this analysis, data were provided on 758 patients (428 women; mean age: 46.5 ± 7.1 years; range: 14.1–90 years) with implanted IVC filters that required advanced techniques for removal. The mean dwell time of the IVC filters was 602.5 ± 388.6 days (range: 5–7366 days). The majority (92.6%; 702/758) of filters in our analysis were designed as retrievable filters (Table 2). The most common retrievable filters were Günther Tulip (26.5%; 186/702), Celect (21.9%; 154/702), and Option (16.7%; 117/702). The most common permanent filter was TrapEase (41.1%; 23/56). In 35 patients, the exact filter brand was not provided,17,23 although they were identified as retrievable.
Table 2. Retrieval outcomes and characteristics.
Indications for retrieval
Indications for IVC filter retrieval were provided in 67.9% (515/758) of patients. Initial indications for retrieval were categorized as either asymptomatic (81.4%; 419/515) or symptomatic (18.6%; 96/515). Asymptomatic patients underwent retrieval because the IVC filtration was no longer needed. Symptomatic patients experienced filter-related morbidities, such as pain resulting from IVC occlusion or stenosis.
The advanced retrieval methods were commonly indicated after failed attempts using standard retrieval. Of all the filters, 89.2% (676/758) were found to be refractory to standard retrieval methods. Of the remaining 82 filters, an advanced retrieval was the first technique attempted in 40 patients, and standard retrieval attempts were not specified in 42 patients. Radiographic findings were explicitly discussed for 53.8% (408/758) of patients. These 408 patients were all found to have tilted filters or filters embedded in the caval wall. These findings were commonly considered the reason for the failed standard retrieval.
Retrieval success and methods
Of the 758 filters, 770 advanced retrieval attempts were reported. The additional 12 attempts failed previous retrieval attempts with an advanced technique prior to a successful retrieval.16,23,24,25,26 In four cases, a failed loop-snare method led to the use of forceps.25 In another three cases, forceps retrieval failure led to the use of loop-snare-type methods.24,26 In three more cases, snare retrieval with aggressive traction failed, and patient discomfort required a re-attempt under general anesthesia in the two remaining previous advanced retrieval attempts.16,23,26 A total of 92.6% (713/770) of attempts were successful using an advanced technique or combination of advanced techniques. In four patients, filter bodies were successfully removed from the IVC. However, filter fractures resulted in adherent or migrated struts, for which complex retrieval methods were not attempted, or retrieval was not possible.17,25,26,27 These four retrieval attempts were deemed successful but counted as major complications because of the risk of severe adverse sequelae. In one study of 60 patients (59 retrievable filters and one permanent filter) and 61 advanced retrieval attempts, the filter type was not identified for the retrieval failures and complications. This study was included in the overall success and complication rate but excluded from the filter type success or complication statistical analysis.16 The success rate was 92.0% (602/654) for retrievable filters and 96.4% (53/55) for permanent filters (P = 0.422; Table 3).
Table 3. Statistical analysis by filter type and retrieval technique.

Although various advanced retrieval methods were used, three methods were the most common: forceps (37.9%; 292/770), laser (32.7%; 252/770), and modified loop-snare (19.9%; 153/770). Two studies did not report the technique used in their retrieval failures;10,17 these were included in the overall success rate but excluded from individual retrieval method success rate analysis. The success rate of retrieval attempts was 95.5% (273/286) for the forceps method, 98.8% (249/252) for the laser method, and 86.0% (123/143) for the modified loop-snare method. The success rate was significantly different between the three retrieval methods (P < 0.001; Table 3).
Major complications
Major complications occurred in 2.8% (21/758) of patients during or after retrieval attempts, with no patient mortality reported as a result of a procedure-related complication. This included a 2.5% (16/643) complication rate for retrievable filters and 5.5% (3/55) complication rate for permanent filters. Filter type was not provided for two complications. Complication rate was not significantly associated with filter type (P = 0.183; Table 3). No procedure-related mortality was reported.
Eleven patients had major complications localized to the IVC. Six patients experienced IVC thrombosis, which was treated using catheter-directed thrombolysis followed by angioplasty if needed.26,28 One additional patient had a pseudo-aneurysm of the IVC that was treated with balloon tamponade.12 Another patient experienced an extravasation in the IVC wall, and another experienced an IVC dissection that was treated with anticoagulation.16,17 A patient also experienced non-occlusive IVC stenosis, managed through angioplasty, and one patient had a filter strut within the IVC that could not be captured.27,29 Ten major complications were non-localized. Three patients had a significant retroperitoneal hemorrhage, requiring stent graft placement in two of these patients and a 5-day hospitalization in the other patient.16,28 At the femoral vein access sites, one patient experienced a right common femoral vein laceration attributed to the incomplete sheathing of a filter.11 This filter could not be removed, and surgical cutdown and venous closure were required. Another patient also required urgent cutdown and repair of the access-site vein.17 One other patient experienced access-site thrombosis.11 Patients with femoral vein complications did not require prolonged hospitalization. Finally, four patients experienced migratory events after retrieval attempts. Filter struts were found to have migrated in three of these patients to the right heart ventricle, pulmonary artery, or retroperitoneum;17,25,26 attempts to retrieve these struts were unsuccessful or not attempted. In another case, a patient experienced a subsegmental PE that was attributed to filter manipulation, although a filter part was not explicitly identified as the cause.30
Risk of bias
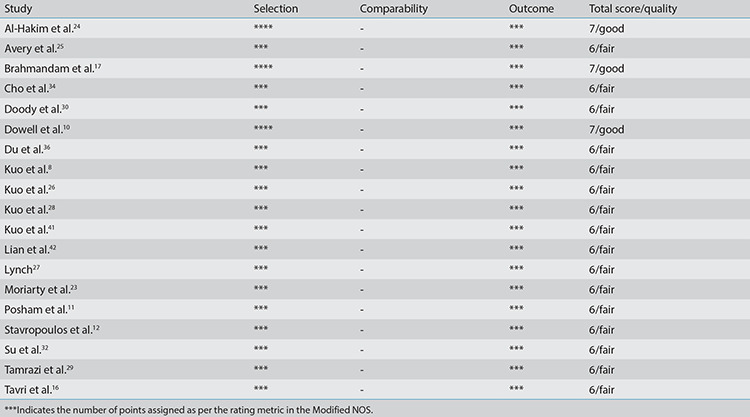
Based on the modified NOS, all included studies were of fair or good quality. All studies received a star for reporting on consecutive patient cohorts. None of the studies statistically controlled for the patient or filter factors and therefore did not receive stars for comparability. The risk-of-bias assessments are summarized in Table 4.
Table 4. Modified Newcastle–Ottawa scale for assessing the quality of non-randomized studies.
Discussion
As yearly retrieval rates of IVC filters remain low and standard retrieval techniques continue to have limitations, further evaluation of complex IVC filter retrievals is warranted.4,5,6 This is particularly true when patients present for the retrieval of filters that have tilted substantially or have been implanted for long periods of time. In our analysis, the average filter dwell time was 602.5 days, and filters were tilted or embedded explicitly in a majority of patients, requiring advanced retrieval techniques. We found that 92.6% (713/770) of advanced retrievals were successful. In comparison, standard retrievals in studies with average dwell times under one year were approximately 85% successful, although this number varied greatly between studies.6,31 Studies reported a higher overall success rate when including standard and advanced retrievals in their retrieval protocols. For example, Su et al.32 reported an increase in retrieval rate from 92.1% to 98.4% after the inclusion of advanced retrieval methods.
Our literature review found three commonly used advanced techniques for complex filter retrieval, categorized as forceps, modified loop-snare, and laser sheath. In the forceps category, forceps are used to dissect embedded filter tips. Although a jugular approach is most commonly used, a femoral approach with filter eversion is also possible.11 The forceps method has also been used to remove localized filter fragments.15 For instance, a Celect filter leg was found embedded in a vertebral body adjacent to the IVC, producing a complaint of back pain. The filter leg was removed from the bone using considerable force applied with forceps. The loop-snare methods in our analysis required adjunct techniques, including a snare-over-guide wire loop (SOGL) method, a hangman method, and a double-loop method.24,29,33 Kuo et al.33 describe a SOGL method in which a wire loop is created through the interstices of the filter body, and an internal jugular vein approach is used. A femoral vein approach can also be employed.34 In another variation, the hangman technique creates a wire loop around the neck of the IVC filter instead of through the interstices of the filter body.23,24 This technique is helpful when the apex of the filter is embedded in the IVC wall. Su et al.32 describe a technique in which the wire loop is created through the filter struts similar to the SOGL method or around the neck of the filter similar to the hangman method. Tamrazi et al.29 describe a method in which two wire loops are formed around the superior and inferior aspects of a TrapEase filter. As a result, internal jugular vein and common femoral vein approaches are both used.29 Blunt dissection with a vascular sheath is then used on both sides of the filter to capture it. In the laser method, photothermal ablation is used to remove the tissue responsible for the embedding of the filter.35 Specifically, this technique can be used to excise adherent struts in cases where the filter tip is not embedded or is unembedded using another technique.28,29 Additionally, combinations of advanced retrieval methods were used substantially in 16 cases, particularly forceps used with laser sheaths to capture intraluminal fragments.28,29
Not all filter retrievals required forceps, laser, or loop-snare methods. Alternative advanced retrievals were attempted in 19 patients. A dual access bi-snare method was attempted in two cases in which snares approaching from the right internal jugular and common femoral veins provided opposite tractions on embedded filters.8,26 Although Du et al.36 also describe a similar bi-snare technique, the SOGL technique was also used. As a result, these cases were categorized as using a modified loop-snare method. Balloon angioplasty was used to free embedded filters in 10 cases,27 and filters were then extracted using a standard recovery cone. Finally, seven cases required aggressive traction using a standard retrieval snare.26 This method was categorized as advanced because of the level of traction. The retrieval methods were unspecified in four patients and were an unspecified combination of methods in 34 patients.10,17 Ultimately, based on our review, several different advanced techniques and combinations thereof may be employed for filter retrieval with promising success rates.
The major complication rate was 2.8% (21/758) in this systematic review. All complications were dealt with during hospitalization, and no mortalities were reported. However, other studies have noted that complications arise considerably more frequently when using advanced techniques than for standard retrievals, and a few patients in this review experienced significant short-term sequelae such as hemorrhage. Ahmed et al.31 reported a major complication rate of 2.1% for advanced retrievals compared with 0% for standard retrievals, and Brahmandam et al.17 reported an overall complication rate in advanced retrievals four times that of standard retrievals. However, the complications noted in our analysis were not always attributed directly to the retrieval methods. Filter tilts and IVC wall embedding inherently pose a risk of complications or retrieval failure regardless of retrieval method. For example, the pseudo-aneurysm reported in our review was located at the site of filter leg penetrations into the IVC wall rather than the site of the forceps dissection of embedding tissue.12
As with all systematic reviews, our review has limitations. The data in this review is limited by the study authors’ reporting, making definitions of successful retrieval and complications difficult to standardize. Individual patient-level data were also not available in the included studies. As a result, we could not compare the retrieval attempt outcomes of different subgroups, such as asymptomatic versus symptomatic retrieval indications. The majority of studies were also retrospective, increasing the possibility of positive reporting bias. Although we excluded small sample case reports through our exclusion criteria, the studies varied greatly in sample size, with smaller studies potentially not representing a full breadth of cases. Finally, the NOS used to assess the risk of bias in this review has limitations because it has not been externally validated, and studies have reported vagueness in its decision rules as well as poor-to-fair inter-rater reliability between reviewers using NOS.37,38 Detailed guidance on how to objectively apply and interpret the scale would have benefited our bias assessment.
Importantly, the majority of the filter retrievals in this review came from institutions that had refined their techniques over a number of years. The success and complication rates are likely subject to the protocol modifications that study authors have implemented in response to early retrieval challenges and increasing technique familiarity. The two largest groups in this review reported outcome improvements after initial retrieval failures and complications. Kuo et al.26 reported implementing an anticoagulation protocol and modifying their retrieval technique to minimize caval wall collapse after four cases of postprocedural caval thrombosis,and Stavropoulos et al.12 noted that three of four retrieval failures occurred in the first 15 attempted cases of a 114-patient study. As a result, studies from these groups reported high success and low complication rates despite most likely encountering difficult cases given their large sample sizes. These results appear unique to high-volume centers specializing in advanced filter retrieval, a sentiment supported by a 2018 survey of vascular specialists that found that the majority of responders were not comfortable using forceps or laser sheath methods.39 Our review reveals that complex retrievals often involve tilted or embedded filters, and when complications do occur, they can be significant and require urgent therapy. To improve retrieval rates and prioritize patient safety, these advanced techniques should be performed in a center with experienced operators and where detailed informed consent is obtained from the patient. Further research on these retrievals should include reporting on protocol modifications and should document the positive changes in quantifiable outcomes that result from iterative protocol refinement. Finally, as demonstrated by Minocha et al.40, implementing a dedicated retrieval clinic may increase retrieval attempts.
Although our review did not identify any significant difference in complication rates between permanent and retrievable filters, it is important to note that only 56 permanent filters were reported in the 19 studies in this review, suggesting that a further evaluation of complex retrieval techniques on permanent filters is needed before conclusions can be drawn. Similarly, 17 filter brands are represented in this review with three comprising the majority of the filters (Günther Tulip, Celect, and Option). Further studies on other filter brands would be helpful in drawing more substantiated conclusions about the retrieval of those filters. Additionally, long-term advanced retrieval-specific follow-up data were not uniformly reported in studies, limiting conclusions to short-term postprocedural complications and warranting further study into long-term complications.
Conclusion
In conclusion, our systematic review suggests that advanced techniques for IVC filter retrieval may be safe for the retrieval of retrievable filters and certain permanent filters with a low short-term major complication rate. These techniques may be successful for IVC filter retrieval when standard techniques fail, particularly when performed by experienced operators who have honed their protocols over a lengthy period of time. Future prospective studies would be beneficial for evaluating individual retrieval techniques and their relation to filter types.
Footnotes
Conflict of interest disclosure
The authors declared no conflicts of interest.
References
- 1.Decousus H, Leizorovicz A, Parent F, et al Prévention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. N Engl J Med. 1998;338(7):409–416. doi: 10.1056/NEJM199802123380701. [DOI] [PubMed] [Google Scholar]
- 2.Reddy S, Lakhter V, Zack CJ, Zhao H, Chatterjee S, Bashir R. Association between contemporary trends in inferior vena cava filter placement and the 2010 US Food and Drug Administration Advisory. JAMA Int Med. 2017;177(9):1373–1374. doi: 10.1001/jamainternmed.2017.2719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Endovascular Today. (2014, May 7). FDA Updates Safety Communication on IVC Filter Retrieval. [Internet]
- 4.Brown JD, Raissi D, Han Q, Adams VR, Talbert JC. Vena cava filter retrieval rates and factors associated with retrieval in a large US cohort. J Am Heart Assoc. 2017;6(9):e006708. doi: 10.1161/JAHA.117.006708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ahmed O, Wadhwa V, Patel K, Patel MV, Turba UC, Arslan B. Rising retrieval rates of inferior vena cava filters in the United States: insights from the 2012 to 2016 Summary Medicare Claims Data. J Am Coll Rad. 2018;15(11):1553–1557. doi: 10.1016/j.jacr.2018.01.037. [DOI] [PubMed] [Google Scholar]
- 6.Ray CE Jr, Mitchell E, Zipser S, Kao EY, Brown CF, Moneta GL. Outcomes with retrievable inferior vena cava filters: a multicenter study. J Vasc Interv Radiol. 2006;17(10):1595–1604. doi: 10.1097/01.RVI.0000239102.02956.65. [DOI] [PubMed] [Google Scholar]
- 7.Rosenthal D, Wellons ED, Levitt AB, Shuler FW, O’Conner RE, Henderson VJ. Role of Prophylactic Temporary Inferior Vena Cava Filters Placed at the ICU bedside under intravascular ultrasound guidance in patients with multiple trauma. J Vasc Surg. 2004;40(5):958–964. doi: 10.1016/j.jvs.2004.07.048. [DOI] [PubMed] [Google Scholar]
- 8.Kuo WT, Cupp JS, Louie JD, et al. Complex Retrieval of Embedded IVC filters: alternative techniques and histologic tissue analysis. Cardiovasc Interv Radiol. 2012;35(3):588–597. doi: 10.1007/s00270-011-0175-1. [DOI] [PubMed] [Google Scholar]
- 9.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan - a Web and Mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi: 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dowell JD, Wagner D, Elliott E, Yildiz VO, Pan X. Factors associated with advanced inferior vena cava filter removals: a single-center retrospective study of 203 patients over 7 years. Cardiovasc Intervent Radiol. 2016;39(2):218–226. doi: 10.1007/s00270-015-1256-3. [DOI] [PubMed] [Google Scholar]
- 11.Posham R, Fischman AM, Nowakowski FS, et al. Transfemoral filter eversion technique following unsuccessful retrieval of option inferior vena cava filters: a single center experience. J Vasc Interv Radiol. 2017;28(6):889–894. doi: 10.1016/j.jvir.2017.02.030. [DOI] [PubMed] [Google Scholar]
- 12.Stavropoulos SW, Ge BH, Mondschein JI, et al. Retrieval of tip-embedded inferior vena cava filters by using the endobronchial forceps technique: experience at a single institution. Radiology. 2015;275(3):900–907. doi: 10.1148/radiol.14141420. [DOI] [PubMed] [Google Scholar]
- 13.Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of Interventional Radiology Clinical Practice guidelines. J Vasc Interv Radiol. 2003;14(9 Pt 2):199–202. doi: 10.1097/01.rvi.0000094584.83406.3e. [DOI] [PubMed] [Google Scholar]
- 14.Tam MD, Spain J, Lieber M, Geisinger M, Sands MJ, Wang W. Fracture and distant migration of the bard recovery filter: a retrospective review of 363 implantations for potentially life-threatening complications. J Vasc Interv Radiol. 2012;23(2):199–205. doi: 10.1016/j.jvir.2011.10.017. [DOI] [PubMed] [Google Scholar]
- 15.Trerotola SO, Stavropoulos SW. Management of fractured inferior vena cava filters: outcomes by fragment location. Radiology. 2017;284(3):887–896. doi: 10.1148/radiol.2017162005. [DOI] [PubMed] [Google Scholar]
- 16.Tavri S, Patel IJ, Kavali P, Irani Z, Ganguli S, Walker TG. Endobronchial forceps-assisted complex retrieval of inferior vena cava filters. J Vasc Surg Venous Lymphat Disord. 2019;7(3):413–419. doi: 10.1016/j.jvsv.2018.08.005. [DOI] [PubMed] [Google Scholar]
- 17.Brahmandam A, Skrip L, Mojibian H, et al. Costs and complications of endovascular inferior vena cava filter retrieval. J Vasc Surg Venous Lymphat Disord. 2019;7(5):653–659. doi: 10.1016/j.jvsv.2019.02.017. [DOI] [PubMed] [Google Scholar]
- 18.Chick JF, Stavropoulos SW, Shin BJ, et al. A 16-F sheath with endobronchial forceps improves reported retrieval success of long-dwelling “closed cell” inferior vena cava filter designs. J Vasc Interv Radiol. 2016;27(7):1027–1033. doi: 10.1016/j.jvir.2016.03.047. [DOI] [PubMed] [Google Scholar]
- 19.Kuo WT, Odegaard JI, Louie JD, et al. Photothermal ablation with the excimer laser sheath technique for embedded inferior vena cava filter removal: initial results from a prospective study. J Vasc Interv Radiol. 2011;22(6):813–823. doi: 10.1016/j.jvir.2011.01.459. [DOI] [PubMed] [Google Scholar]
- 20.Kuo WT, Odegaard JI, Rosenberg JK, Hofmann LV. Excimer laser-assisted removal of embedded inferior vena cava filters: a single-center prospective study. Circ Cardiovasc Interv. 2013;6(5):560–566. doi: 10.1161/CIRCINTERVENTIONS.113.000665. [DOI] [PubMed] [Google Scholar]
- 21.Mintz JD, Stavropoulos SW, Trerotola SO. Is a venacavogram necessary after inferior vena cava filter retrieval? J Vasc Interv Radiol. 2016;27(12):1857–1864. doi: 10.1016/j.jvir.2015.08.016. [DOI] [PubMed] [Google Scholar]
- 22.Stavropoulos SW, Dixon RG, Burke CT, et al. Embedded inferior vena cava filter removal: use of endobronchial forceps. J Vasc Interv Radiol. 2008;19(9):1297–1301. doi: 10.1016/j.jvir.2008.04.012. [DOI] [PubMed] [Google Scholar]
- 23.Moriarty HK, Marshall E, Clements W. A 7-year retrospective review of the technical success of the “low-profile” hangman technique for complicated inferior vena cava (IVC) filter retrievals. Diagn Interv Radiol. 2020;26(2):118–123. doi: 10.5152/dir.2019.19223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Al-Hakim R, McWilliams JP, Derry W, Kee ST. The hangman technique: a modified loop snare technique for the retrieval of inferior vena cava filters with embedded hooks. J Vasc Interv Radiol. 2015;26(1):107–110. doi: 10.1016/j.jvir.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 25.Avery A, Stephens M, Redmond K, Harper J. Initial experience using the rigid forceps technique to remove wall-embedded IVC filters. J Med Imaging Radiat Oncol. 2015;59(3):306–311. doi: 10.1111/1754-9485.12299. [DOI] [PubMed] [Google Scholar]
- 26.Kuo WT, Tong RT, Hwang GL, et al. High-risk retrieval of adherent and chronically implanted IVC filters: techniques for removal and management of thrombotic complications. J Vasc Interv Radiol. 2009;20(12):1548–1556. doi: 10.1016/j.jvir.2009.08.024. [DOI] [PubMed] [Google Scholar]
- 27.Lynch FC. Balloon-assisted removal of tilted inferior vena cava filters with embedded Tips. J Vasc Interv Radiol. 2009;20(9):1210–1214. doi: 10.1016/j.jvir.2009.06.022. [DOI] [PubMed] [Google Scholar]
- 28.Kuo WT, Odegaard JI, Rosenberg JK, Hofmann LV. Laser-assisted removal of embedded vena cava filters: a 5-year first-in-human study. Chest. 2017;151(2):417–424. doi: 10.1016/j.chest.2016.09.029. [DOI] [PubMed] [Google Scholar]
- 29.Tamrazi A, Wadhwa V, Holly B, et al. Percutaneous retrieval of permanent inferior vena cava filters. Cardiovasc Intervent Radiol. 2016;39(4):538–546. doi: 10.1007/s00270-015-1214-0. [DOI] [PubMed] [Google Scholar]
- 30.Doody O, Noë G, Given MF, Foley PT, Lyon SM. Assessment of snared-loop technique when standard retrieval of inferior vena cava filters fails. Cardiovasc Intervent Radiol. 2009;32(1):145–149. doi: 10.1007/s00270-008-9446-x. [DOI] [PubMed] [Google Scholar]
- 31.Ahmed O, Kim YJ, Patel MV, et al. A Single-institutional comparative analysis of advanced versus standard snare removal of inferior vena cava filters. J Vasc Interv Radiol. 2020;31(1):53–60. doi: 10.1016/j.jvir.2019.07.014. [DOI] [PubMed] [Google Scholar]
- 32.Su Q, Ding X, Dong Z, Liu Y, Li G, Jiang J. A modified loop snare technique for difficult retrievals of inferior vena cava filter and migrated coil. Int Heart J. 2019;60(1):93–99. doi: 10.1536/ihj.18-075. [DOI] [PubMed] [Google Scholar]
- 33.Kuo WT, Bostaph AS, Loh CT, Frisoli JK, Kee ST. Retrieval of trapped Günther Tulip inferior vena cava filters: snare-over-guide wire loop technique. J Vasc Interv Radiol. 2006;17(11 Pt 1):1845–1849. doi: 10.1097/01.RVI.0000241946.40524.85. [DOI] [PubMed] [Google Scholar]
- 34.Cho E, Lim KJ, Jo JH, Jung GS, Park BH. Failed inferior vena cava filter retrieval by conventional method: analysis of its causes and retrieval of it by modified double-loop technique. Phlebology. 2015;30(8):549–556. doi: 10.1177/0268355514545353. [DOI] [PubMed] [Google Scholar]
- 35.Kuo WT, Cupp JS. The excimer laser sheath technique for embedded inferior vena cava filter removal. J Vasc Interv Radiol. 2010;21(12):1896–1899. doi: 10.1016/j.jvir.2010.08.013. [DOI] [PubMed] [Google Scholar]
- 36.Du X, Li C, Qian A, et al. Bidirectional pull-back technique for retrieval of strut-embedded cylinder-shaped filters in inferior vena cava. Med Sci Monit. 2017;23:2796–2804. doi: 10.12659/MSM.904550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in metaanalyses. Eur J Epidemiol. 2010;25(9):603–605. doi: 10.1007/s10654-010-9491-z. [DOI] [PubMed] [Google Scholar]
- 38.Hartling L, Milne A, Hamm MP, et al. Testing the Newcastle Ottawa scale showed low reliability between individual reviewers. J Clin Epidemiol. 2013;66(9):982–993. doi: 10.1016/j.jclinepi.2013.03.003. [DOI] [PubMed] [Google Scholar]
- 39.Brahmandam A, Skrip L, Sumpio B, et al. A survey of vascular specialists’ practice patterns of inferior vena cava filter placement and retrieval. Vascular. 2019;27(3):291–298. doi: 10.1177/1708538118815394. [DOI] [PubMed] [Google Scholar]
- 40.Minocha J, Idakoji I, Riaz A, et al. Improving inferior vena cava filter retrieval rates: impact of a dedicated inferior vena cava filter clinic. J Vasc Interv Radiol. 2010;21(12):1847–1851. doi: 10.1016/j.jvir.2010.09.003. [DOI] [PubMed] [Google Scholar]
- 41.Kuo WT, Robertson SW, Odegaard JI, Hofmann LV. Complex retrieval of fractured, embedded, and penetrating inferior vena cava filters: a prospective study with histologic and electron microscopic analysis. J Vasc Interv Radiol. 2013;24(5):622–630. doi: 10.1016/j.jvir.2013.01.008. [DOI] [PubMed] [Google Scholar]
- 42.Lian W, Tian F, Li S, Gu X, Jia Z. Forceps-assisted removal of difficult-to-retrieve filters: preliminary results. Ann Vasc Surg. 2019;61:371–376. doi: 10.1016/j.avsg.2019.05.045. [DOI] [PubMed] [Google Scholar]