

Abstract
Fibrolipoma, a subtype of lipoma, is a painless, well-circumscribed, slow-growing, submucosal benign adipocyte tumour. It is uncommon in the oral cavity and oropharyngeal region. It accounts for 1.6% of all facial lipomas. Fibrolipomas mostly affect the buccal mucosa and buccal vestibule and cause functional and cosmetic disabilities. The diagnosis and differentiation of fibrolipoma with clinically similar lesions such as fibroma and pleomorphic adenoma are very essential for a correct treatment plan and complete follow-up. Here, we present fibrolipoma, a very rare subtype of lipoma involving the buccal mucosa of the left premolar region in a 44-year-old male patient.
Keywords: Adipocyte, benign, lipoma
INTRODUCTION
Lipomas are the most common benign mesenchymal tumours developing in any location where fat is normally present. They develop mostly in the subcutaneous tissues but could also develop in deeper tissues.[1] The aetiology of lipomas is uncertain, and the tumour mainly affects the region of the trunk, shoulders, neck and axilla.[2] Involvement of the oral cavity is rare with only 1%–4% of cases.[3,4,5,6] They usually present as painless, well-circumscribed, slow-growing submucosal masses or superficial lesions, mainly in the buccal mucosa. Histologically, several variants of lipoma have been described, including angiolipoma, fibrolipoma, chondroid lipoma, myolipoma, spindle cell or pleomorphic lipoma, diffuse lipomatous proliferation (lipomatosis) and hibernoma.[3]
Fibrolipoma is classified as an uncommon histological variant of conventional lipoma by the World Health Organization (WHO),[3] in which neoplastic fat cells are embedded along with dense collagen.[2] Most patients are 40 years of age or older.[2] It may occur at various anatomic sites including the buccal mucosa, lips, tongue, palate and floor of the mouth. Although benign in nature, their progressive growth can cause interference with speech and mastication due to the tumour’s dimension.[2,3] Here, we present a case of fibrolipoma in a 44-year-old male patient.
CASE PRESENTATION
A 44-year-old male patient presented with a complaint of swelling in the upper left canine tooth region. The patient was apparently asymptomatic one year back. He noticed a small swelling, which gradually increased in size to reach the present size of 0.5 × 0.5 cm. On inspection, the swelling was present on the buccal side of tooth 24 involving the marginal and attached gingival extending up to the vestibule, sessile in growth, oval in shape and of normal mucosal appearance [Figure 1]. On palpation, the swelling was non-tender, soft in consistency and fluctuant in nature. No bone resorption was evident in the radiograph. A provisional diagnosis of pyogenic granuloma with a differential diagnosis of traumatic fibroma, lipoma and peripheral giant cell granuloma was made.
Figure 1.

Intraoral photograph of the lesion
An excisional biopsy was performed, and the specimen was sent for histopathological examination. The gross specimen measured 8 × 4 × 3 mm and was irregular in shape, brownish back in colour and firm in consistency. Histological sections revealed parakeratinised stratified squamous epithelium with underlying fibrous connective tissue showing bundles of collagen fibres with lobules of adipocytes in deeper areas of the section [Figures 2, 3 and 4]. Histologically, the diagnosis of fibrolipoma was made.
Figure 2.
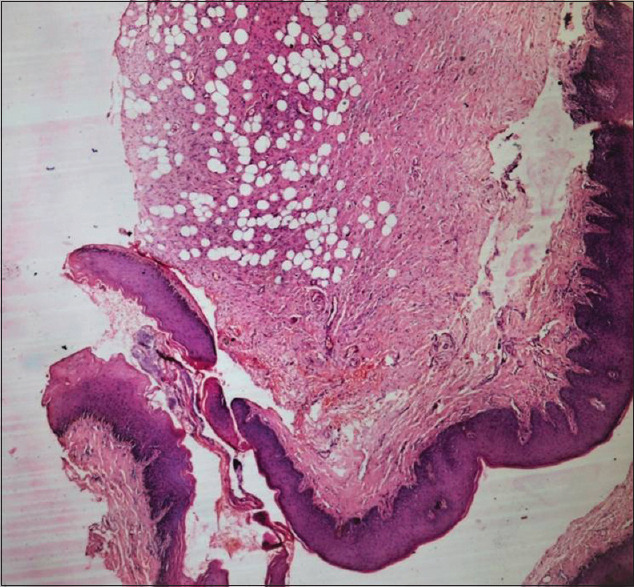
Histopathological image showing a well-circumscribed lesion composed of fibrous connective tissue, showing bundles of collagen fibres with lobules of adipocytes (H and E, ×40)
Figure 3.
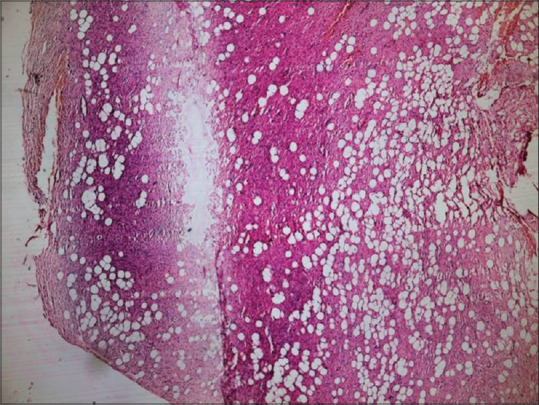
Histopathological image showing adipocytes in a fibrous connective tissue stroma (H and E, ×100)
Figure 4.
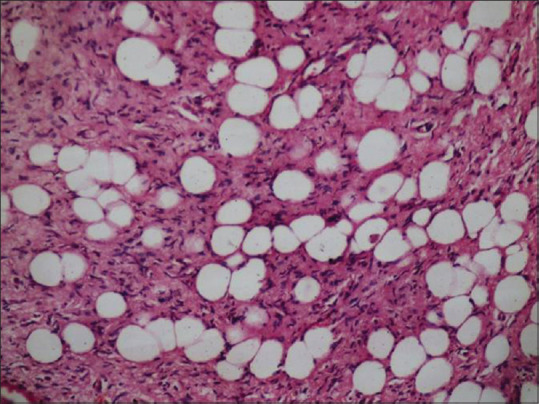
Histopathological image showing adipocytes in a fibrous connective tissue stroma (H and E, ×200)
DISCUSSION
Lipoma is a common benign tumour of adipose tissue, but its presence in the oral and oropharyngeal region is relatively uncommon with a prevalence rate of only 1/5000 adults.[2]
The aetiopathogenesis of lipoma and fibrolipoma is not known. Heredity, fatty degeneration, trauma, hormonal basis, infection, infarction and chronic irritation are some of the suggested causes. In most cases, they represent a developmental anomaly, but they can arise as a result of trauma and rearrangement of chromosome nos. 12q, 13q and 6p.[2] A previous study suggested that fibrolipoma is a congenital lesion caused by an endocrinal imbalance or arises via the degeneration of a fibromatous tumour or arises from the maturation of lipoblastomatosis.[3] It may also arise by preadipocyte differentiation and proliferation mediated by cytokines following soft tissue damage when blunt trauma and hematoma formation occur.[2] Oral fibrolipomas are very rare; only a few cases documented so far. Since the proliferative activity of fibrolipoma is greater than the other variants, the need for accurate diagnosis is important.[3] It has been proposed that disturbance in glucose and lipid metabolism, hormone therapy and trauma can lead to the formation and proliferation of the tumour.[4] In this case, trauma may be the cause of the presence of the lesion on the maxillary buccal gingiva.
Rajendran and Shivapathasundharam have classified intraoral lipomas into three types, depending on their morphology.[3]
Diffuse form affecting deeper tissues.
Superficial form.
Encapsulated form.
Fibrolipoma is a microscopic variant of lipoma characterised by a significant fibrous component intermixed with lobules of fat cells.[1] It is a benign soft tissue tumour, which rarely occurs in oral and maxillofacial regions.[2] The most common sites of occurrence are buccal mucosa and buccal vestibule with a slight female predilection.[1] In the present case, the lesion occurred on the buccal gingiva of the maxillary left first premolar area extending up to the vestibule.
The clinical course of fibrolipoma is usually asymptomatic. Patients classically present with a painless, slow-growing lesion and generally only seek medical attention for aesthetic or functional issues such as chewing, swallowing or phonation dysfunction. Sometimes, the appearance and pseudo-infiltrative nature of fibrolipoma may induce doubt clinically as to whether the lesion is truly benign. In addition, since fibrolipoma and malignant infiltrating lesions such as liposarcoma may not be distinguished clinically with certainty, and also, liposarcoma can occur in long-standing cases of fibrolipoma, and histologic evaluation is essential.[7,8]
Fibrolipoma differs from the classic variant lipoma as the former is composed of lobules of ‘chicken wire’ appearing, benign adipocytes with a component comprised of broad bands of dense collagen.[3] Like the classic lipoma, it is usually well-circumscribed and may be thinly encapsulated.[2] The lesion in the present case showed similar features. Furthermore, fibrolipomas have greater proliferative activity in comparison with other variants of lipomas; thus, accurate histological examination is mandatory,[5] and the differential diagnosis is based on the detection of lack of lobular architecture, areas of prominent fibrosis and, most importantly, on the presence of multivacuolated adipose cells with indented nuclei (lipoblasts), which are typically present in liposarcoma in variable proportion.[2]
The treatment of lipomas including fibrolipoma is usually surgical excision.[9] The lesion in this case was surgically excised without any complications. Postoperative follow-up of 6 months showed no recurrence. The main objective of presenting this case is to create awareness of this rare clinical entity, which may at times mimic a malignant growth.
CONCLUSION
Fibrolipoma is a distinct clinicopathologic entity with increased growth potential. They may be clinically asymptomatic until and unless they attain a larger size. Complete resection is the treatment of choice to avoid recurrence. However, they have a low recurrence potential. An accurate differential diagnosis, postsurgical histological examination and careful follow-up are, however, required. Knowledge and prompt treatment of this tumour are important.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Khubchandani M, Thosar NR, Bahadure RN, Baliga MS, Gaikwad RN. Fibrolipoma of buccal mucosa. Contemp Clin Dent. 2012;3:S112–4. doi: 10.4103/0976-237X.95119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pereira T, Shetty S, Sapdhare S, Tamgadge A. Oral fibrolipoma:A rare histological variant. Indian J Dent Res. 2014;25:672–4. doi: 10.4103/0970-9290.147123. [DOI] [PubMed] [Google Scholar]
- 3.Phulari RG, Soni V, Talegaon TP, Bakutra G. Oral fibrolipoma:A report of two cases and review of literature. Indian J Dent Res. 2018;29:513–6. doi: 10.4103/ijdr.IJDR_730_16. [DOI] [PubMed] [Google Scholar]
- 4.Salih AM, Abdullah AM, Fatah ML, Abdulla BA, Mohammed SH, Kakamad FH. Fibrolipoma of the tongue;A case report with literature review. Ann oMed Surg. 2021;72:1–3. doi: 10.1016/j.amsu.2021.102985. doi:10.1016/j.amsu. 2021.102985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ganakalyan B, Kumar SD. Reviewing the entity:Retropharyngeal fibrolipoma and a rare case report. Iran J Otorhinolaryngol. 2015;27:469–74. [PMC free article] [PubMed] [Google Scholar]
- 6.Devi AN, Sowbhagya MB, Balaji P, Mahesh Kumar TS. An uncommon case of fibrolipoma. Indian J Dent Res. 2017;28:699–701. doi: 10.4103/ijdr.IJDR_718_16. [DOI] [PubMed] [Google Scholar]
- 7.Mungul S, Maharaj S, Masege SD. Lingual Fibrolipoma –A rare clinicopathological entity. S Afr J Surg. 2017;55:36–8. [PubMed] [Google Scholar]
- 8.Reibel JF, Greene WM. Liposarcoma arising in the pharynx nine years after fibrolipoma excision. Otolaryngol Head Neck Surg. 1995;112:599–602. doi: 10.1177/019459989511200417. [DOI] [PubMed] [Google Scholar]
- 9.Shah SN, Jain GS, Patel U, Shah A. Oral fibrolipoma arising from maxillary alveolus:A rare case entity. J Clin Diagn Res. 2022;16:9–11. [Google Scholar]