

Abstract
Background and Aims
Multiple sclerosis (MS) is a crippling, chronic, gender‐related disease that causes burdens to individuals and society. China has a considerable and increasing population of MS. We aim to analyze the gender disparities in the burden of MS in China and predict the trends.
Methods
The study was conducted based on the Global Burden of Disease Study 2019. Data on incidence, prevalence, deaths, and disability‐adjusted life years (DALYs) of MS in China from 1990 to 2019 was descriptively analyzed by year, gender, and age group. The Nordpred package in R (version 4.2.2) was used for age‐period‐cohort analysis to predict the all‐ages numbers and age‐standardized rates of incidence, prevalence, deaths, and DALYs in China from 2020 to 2044.
Results
The number of prevalent cases of MS in 2019 reached 18,143.56 (95% uncertainty intervals [UI]: 13,997.71–22,658.60) in males and 24,427.11 (95% UI: 18,906.02–30,530.21) in females in China. The peak age of prevalence was shifted from 40–44 years in 1990 to 45–49 years in 2019 in females but remained unchanged in males. In contrast to the increased age‐standardized prevalence rate, the age‐standardized death rate (ASDR) and age‐standardized DALYs rate showed downward trends, which were more significant in females. Different from the global, Chinese males showed lower prevalence but higher deaths and DALYs than females for age‐standardized rates and numbers. In the next 25 years, the patient population will remain large and peak around 44,599.78 in 2025–2029. The ASDR, age‐standardized DALYs rate, and DALYs number were expected to decrease. The improvements in deaths and DALYs will be more significant in females.
Conclusion
Males with MS had a lower prevalence but higher deaths and DALYs than females in China. The ASDR and age‐standardized DALYs rate have reduced over the past 30 years and were expected to continue decreasing, especially in females. The burden of MS will remain notable in the next 25 years.
Keywords: disability‐adjusted life years, disease burden, gender, multiple sclerosis, prediction
1. INTRODUCTION
Multiple sclerosis (MS) is a chronic inflammatory disorder of the central nervous system characterized by inflammation, demyelination, axonal loss, and remyelination dysfunction. 1 , 2 Autoimmune inflammatory and neurodegeneration mechanisms are involved in MS. 3 , 4 Alterations in innate and adaptive immune responses and intrinsic central nervous system immune cells contribute to pathogenesis. 3 , 4
MS is crippling and mainly affects young and moderately aged adults, 5 leading to productivity loss and disability. 6 The long duration of MS, difficulty in performing daily activities, and the need for multidisciplinary treatment caused a great burden on individuals, families, and society. 7 The global population of MS was estimated about 2.8 million in 2020, with a prevalence of 35.9 per 100,000 people. 8 In the United States, the total annual economic cost of MS was approximately $28 billion. 6 The morbidity of MS in China is lower than the global, with a prevalence of 3.4 per 100,000 people among males and 6.3 per 100,000 people among females in eight provinces in China mainland, 8 , 9 7.02 per 100,000 in Taiwan and 4.8 per 100,000 in Hong Kong. 9 In China, the annual direct economic cost was 27,655.57 ± 29,204.25 Chinese Yuan per capita, and the annual indirect cost was 11,299.85 ± 3169.54 Chinese Yuan, according to a study involving 50 centers. 7 In addition to the financial burden caused by the long duration of the disease and high‐priced medications, patients with MS may also be troubled by limited healthcare levels. 10 The physical and mental harm caused by MS is remarkable. 11
MS, although classified as a rare disease, is not rare but easily underestimated in its impact. As the most populous country, China has a considerable and growing number of MS patients. 12 , 13 The increase in patient population, average life expectancy, and the demand for life quality increase the demand for medical resources. 11 , 14 , 15 It is essential to evaluate and predict the burden due to MS and take active measures to improve healthcare in related areas. Specifically, detailed descriptions and predictions of epidemiological dynamics are needed to assist policymakers, researchers, and healthcare professionals with better recommendations and decisions. MS is related to acquired environmental factors and genetic susceptibility. It is associated with the HLA‐DRB1*1501 allele, Epstein‐Barr virus infection, smoking, obesity, and low serum vitamin D. 3 , 4 , 16 , 17 Gender is one of the most important risk factors for MS, and gender differences in clinical manifestations and progression have been studied. 3 , 18 , 19 , 20 Generally, although females are more susceptible than males, males have a worse prognosis. 3 , 21 However, to our knowledge, there is a lack of study focus on the burden disparities between genders in the Chinese population. This study aimed to evaluate and predict the burden of MS in China by gender and reflect the disparities, based on data from the Global Burden of Disease Study 2019 (GBD 2019) for better healthcare.
2. MATERIALS AND METHODS
2.1. Data resource
The GBD 2019 is a public data set that estimates the epidemiological burden of 369 diseases and injuries in 204 countries and regions in terms of incidence, prevalence, deaths, disability‐adjusted life years (DALYs), years of life lost (YLLs), and years lived with disability (YLDs). 22 The data can be downloaded from the Global Health Data Exchange (GHDx) (https://vizhub.healthdata.org/gbd-results/). Details on the methodology have been described in previous studies. 22 The incidence is calculated as the number of new cases in a year divided by the mid‐year population, and the prevalence is the total number of cases divided by the total population. 23 The mortality is cause‐specific and is computed by the number of deaths due to a particular reason divided by the mid‐year population. 23 The YLLs correspond to the number of deaths multiplied by the standard life expectancy at the age of death. 10 YLDs are estimated as the product of the prevalence of individual sequelae multiplied by the corresponding disability weight. 10 The disability weight quantifies the severity of sequelae as a number from 0 to 1. 0 represents full health, and 1 represents death. 10 DALYs are the sum of YLLs and YLDs. 24 , 25 All estimates are presented with 95% uncertainty intervals (UIs), defined by the 25th and 975th values of the ordered 1000 values of the posterior distribution. 10 , 22
We extracted the data of the global and China regarding MS from 1990 to 2019 for both genders. “Prevalence,” “incidence,” “death,” and “DALYs (disability‐adjusted life‐years)” were chosen for measures. “China” and “global” were selected for the location, “number” and “rate” for metrics, and “multiple sclerosis” for the cause. In addition, the population estimates from 1990 to 2044 in China were obtained from the GHDx for burden prediction (https://ghdx.healthdata.org/record/ihme-data/gbd-2019-population-estimates-1950-2019; https://ghdx.healthdata.org/record/ihme-data/global-population-forecasts-2017-2100). Ethics approval and informed consent were not applicable due to the public accessibility of the data.
2.2. Statistical analysis
Descriptive analyses were performed by gender, age, and year. The age trends in number and rate of prevalence, deaths, and DALYs were analyzed by 5‐year age groups. The age groups above 80 years were combined. The overall disease burdens are expressed as all‐ages numbers and age‐standardized rates. Moreover, we predicted the burden due to MS from 2020 to 2044 by age‐period‐cohort analysis using the Nordpred package in R, which has been recognized for trend prediction in previous studies. 26 , 27 , 28 We estimated the numbers and age‐standardized rates of incidence, prevalence, deaths, and DALYs by sex per 5‐year period. The change in rates, population size, and age structure were taken into account in this model. The Nordpred age‐period‐cohort analysis is defined as follows:
In this formula, the is the ratio for the age group in the period . corresponds to the age component for group . represents the common linear drift parameter in the observed period and birth cohort. is the nonlinear component for the period . represents the nonlinear component of cohort 28 The power‐5 link function was used to level off growth. The all‐ages numbers were calculated by applying the predicted rates to the national population forecasts. All statistical analyses were performed by open‐access statistical software R (version 4.2.2).
3. RESULTS
3.1. The burden due to MS in China in 2019
For males, the MS‐related age‐standardized incidence rate (ASIR) was 0.16 (95% UI: 0.13–0.19) per 100,000 population, the age‐standardized prevalence rate (ASPR) was 1.96 (95% UI: 1.51–2.46) per 100,000 population, the age‐standardized death rate (ASDR) was 0.10 (95% UI: 0.07–0.15) per 100,000 population, and the age‐standardized DALYs rate of MS was 3.80 (95% UI: 2.83–5.38) per 100,000 population in 2019 (Supporting Information S1: Table 1). For females, the ASIR was 0.18 (95% UI: 0.15–0.22) per 100,000 population, the ASPR reached 2.68 (95% UI: 2.06–3.38) per 100,000 population, the ASDR was 0.08 (95% UI: 0.06–0.11), and the age‐standardized DALYs rate of MS was 3.60 (95% UI: 2.73–4.66) per 100,000 population (Supporting Information S1: Table 1).
Because of the large population base, the number of patients is appalling. The number of prevalent cases in 2019 reached 42,570.67 (95% UI: 33,001.21–53,329.09), with 18,143.56 (95% UI: 13,997.71–22,658.60) males and 24,427.11 (95% UI: 18,906.02–30,530.21) females (Supporting Information S1: Table 1). The numbers of deaths and DALYs were higher in men.
The age patterns of Chinese MS patients were analyzed. The prevalence began its upward trend from the 15–19 age group and peaked at the 45–49 age group, with a following downward trend for both males and females (Figure 1A). The rates were higher among females than males in all age groups (Figure 2A). The death rate in males increased with age and surged once over 75 years (Figure 1B). For females, the death rate gradually increased from the 15–19 age group to the 55–59 age group, after which it decreased from the 60–64 age group to the 75–79 age group and then rose in the 80+ group (Figure 1B). The DALYs rate was the highest in the 55–59 age group for both males and females (Figure 1C). The mortality and DALYs rate were higher among females aged from 15 to 39 but higher among males over the age of 40 (Figure 2C,E). The highest prevalent cases, deaths, and DALYs number occurred in the age group of 50–54 (Figure 2B,D,F).
Figure 1.
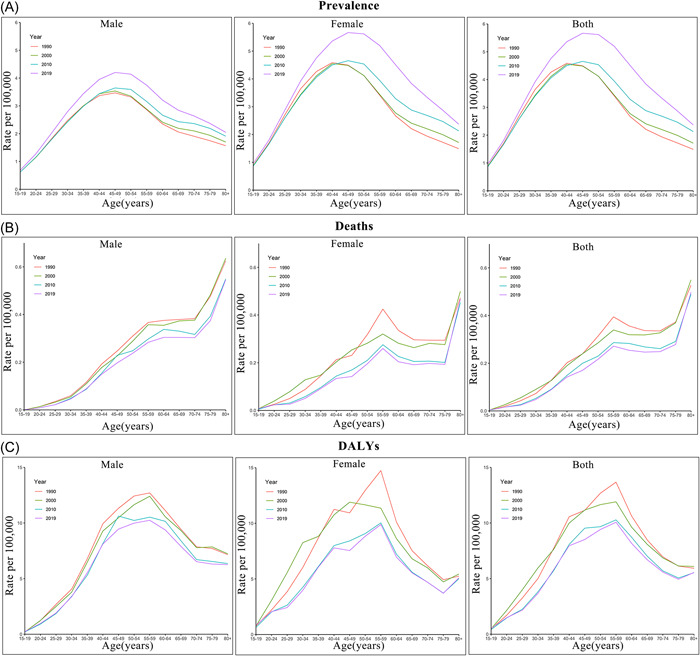
Age trends of (A) prevalence, (B) deaths, and (C) disability‐adjusted life years (DALYs) rates of multiple sclerosis (MS) in China in 1990, 2000, 2010, and 2019.
Figure 2.

Rates and numbers of (A, B) prevalence, (C, D) deaths, and (E, F) disability‐adjusted life years (DALYs) by age group and sex in 1990 and 2019.
3.2. Trends in MS incidence, prevalence, deaths, and DALYs over time
During the studied period, the ASIR was relatively stable for both genders (Figure 3A), whereas the ASPR increased (Figure 3C). The change rate of ASPR was 0.20 (95% UI: 0.18–0.23) and 0.25 (95% UI: 0.21–0.28) in males and females, respectively. The age peak of prevalence in women has shifted from 40‐44 in 1990 to 45–49 in 2019 but remained unchanged in men (Figure 1A). The ASDR and age‐standardized DALYs rate showed downward trends, which were more significant in females (Figure 3E,G). The rate of change of ASDR from 1990 to 2019 was −0.22 (95% UI: −0.52 to 0.31) in males and −0.35 (95% UI: −0.63 to 0.06) in females. The change rate of the age‐standardized DALYs rate was −0.20 (95% UI: −0.48 to 0.29) in males and −0.30 (95% UI: −0.58 to 0.10) in females.
Figure 3.
Time trends of all‐ages numbers and age‐standardized rates of multiple sclerosis (MS) in China by sex from 1990 to 2019, and predicted burden from 1990 to 2044: (A, B) incidence, (C, D) prevalence, (E, F) deaths, and (G, H) disability‐adjusted life years (DALYs).


An assessment of the time trend shows an overall upward trend in the total number of incident cases, prevalent cases, deaths, and DALYs from 1990 to 2109 (Figure 3B,D,F,H), suggesting an increased burden of MS. The age peak of prevalent cases shifted from 35–39 years old to 50–54 years old from 1990 to 2019 for both genders. The age peak of the DALYs numbers also shifted backward.
The female‐to‐male ratios (FMRs) of ASIR, ASDR, and age‐standardized DALYs rate showed downward trends (Figure 4). The ratio of ASIR was 1.27 and 1.13 in 1990 and 2019, respectively. The FMRs of ASDR and age‐standardized DALYs rate showed similar characteristics and trends. They showed a fluctuating upward trend from 1990 to 1999 but a significant downward trend from 2000 to 2019 (Figure 4C,D). The FMR of ASDR was 0.98 in 1990, reached 1.02 in 1999, and dropped to 0.81 in 2019. The FMR of the age‐standardized DALYs rate was 1.09 in 1990, 1.20 in 1999, and 0.95 in 2019. The FMR of ASPR increased from 1.32 in 1990 to 1.37 in 2019. It mostly remained stable from 1990 to 2014 and increased since 2015 (Figure 4B).
Figure 4.

The female‐to‐male ratios of (A) age‐standardized incidence rate (ASIR), (B) age‐standardized prevalence rate (ASPR), (C) age‐standardized death rate (ASDR), and (D) age‐standardized disability‐adjusted life years (DALYs) rate from 1990 to 2019 in global and China.
3.3. The predicted burden of MS in China
In the next 25 years, despite the predicted ASIR being stable, the number of new cases for both genders is expected to increase slowly (Figure 3A,B). The trend lines of the number of new cases for males and females approach and become nearly equal in 2035. The predicted ASPR among females gradually increases, reaching 2.72 per 100,000 population in the time frame of 2025–2029, then decreases to 2.62 per 100,000 population in 2040–2044. Among males, it is expected to reach 2.04 per 100,000 population in 2030–2034 and decline to 2.02 per 100,000 population in 2040–2044 (Figure 3C). The population of MS will continue to increase and peak around 44,599.78 in 2025–2029 (Figure 3D, Table 1). The projection of the ASDR shows a slow and slight downward trend in both sexes. The ASDR is expected to drop to 0.07 per 100,000 population among females and 0.09 per 100,000 population among males in 2040–2044 (Figure 3E). During the projection period, the number of deaths is relatively stable among females but shows an upward trend among males (Figure 3F). The total death number could reach 1860.80 by 2044. The age‐standardized DALYs rate significantly decreases during the 25‐year projection period, especially among females. The rate declined from 3.28 to 2.92 per 100,000 population among females and from 3.64 to 3.44 per 100,000 population among males (Figure 3G). The number of DALYs is expected to continue to decline in China, especially among females (Figure 3H), largely due to a series of therapeutic progress. Although we are pleased to see a downward trend in DALYs, the large total number still reflects a heavy burden caused by MS.
Table 1.
Average annual numbers of incidence, prevalence, deaths, and disability‐adjusted life years (DALYs) of multiple sclerosis (MS) in China from 1990 to 2044.
| Year | Incidence | Prevalence | Deaths | DALYs |
|---|---|---|---|---|
| 1990–1994 | 2068.12 | 22,614.66 | 1282.31 | 55,343.17 |
| 1995–1999 | 2221.35 | 25,256.54 | 1485.82 | 65,086.43 |
| 2000–2004 | 2367.65 | 28,106.64 | 1521.63 | 64,800.10 |
| 2005–2009 | 2505.22 | 31,021.97 | 1530.80 | 63,687.94 |
| 2010–2014 | 2725.23 | 35,512.13 | 1619.60 | 66,162.74 |
| 2015–2019 | 2943.47 | 41,315.86 | 1728.79 | 69,415.69 |
| 2020–2024 | 3051.64 a | 43,541.29a | 1781.58a | 68,360.03a |
| 2025–2029 | 3142.26a | 44,599.78a | 1813.37a | 66,667.91a |
| 2030–2034 | 3226.24a | 44,517.04a | 1831.41a | 64,421.31a |
| 2035–2039 | 3280.66a | 43,409.37a | 1849.80a | 62,141.49a |
| 2040–2044 | 3278.91a | 41,825.30a | 1860.80a | 59,726.62a |
Predicted numbers.
4. DISCUSSION
This study reveals the burden of MS in China from 1990 to 2019 by year, age, and gender, contributing to a better understanding of the epidemiological changes of MS. Compared with the global, China had lower prevalence, mortality, and DALYs rate. We found that males and females have similar age patterns in prevalence and DALYs rate but different patterns in death rate. The age peak of prevalence in women was shifted from 1990 to 2019 for both rates and numbers. The age peak of prevalent cases in men also shifted backwards. The aging trend of MS patients sends an encouraging signal that the population growth of MS has slowed down. Consistent with previous research, ASDR and age‐standardized DALYs rate of MS in China showed downward trends, 13 while the ASPR shows an upward trend. Besides, the improvement in ASDR and age‐standardized DALYs rate was more significant in females. The improvement in medical treatment contributes to earlier and more accurate diagnosis. Economic and medical development, better medical insurance policies, an improved social security system, and enhanced health consciousness played a positive role. Although the burden is projected to remain large over the next 25 years, the age‐standardized rates of death and DALYs are expected to decline. The improvements in deaths and DALYs in females will be more notable.
Although MS is at a low level of prevalence in China, there is a large number of patients due to the huge population base, leading to high disability and economic burden. China places a high premium on the prevention, control, and insurance of rare diseases and has introduced many policies to improve treatment ability and protect patients. The progress in MS management has been proven. However, it is worth noting that there was an overall upward trend in numbers of incidence, prevalence, deaths, and DALYs, and over 40,000 people are expected to suffer from MS in the next 25 years. The huge population of patients deserves ample attention.
MS is closely related to gender. The gender differences in the disease courses, severity, and prognosis of MS have been documented and may be associated with intrinsic CNS differences and genetic, epigenetic, environmental, immunological, and hormonal factors. 18 , 29 According to available research, relapsing‐remitting and secondary progressive MS is more prevalent in women, 29 while men with MS are more likely to develop primary progressive MS. 18 Females have a higher risk of relapse than males, while males have worse outcomes and faster progression. 21 , 30 Males with MS are predisposed to pyramidal, brainstem, and cerebellar relapses, while females present with more frequent visual and sensory relapses. 19 The higher risk of incomplete recovery in pyramidal and cerebellar relapses than visual and sensory relapses may be related to more severe long‐term disability and sex differences in the outcome. 19 , 20 In addition, the male gender is a risk factor associated with the progression from radiologically isolated syndrome to symptomatic MS and from relapsing‐remitting to crippling secondary progressive MS. 31 There is a faster disability progression in males and a shorter time to the landmarks of irreversible disability. 32 , 33 There are also gender differences in medication responses and side effects. In the secondary progressive MS cohort, females benefit more significantly than males on disease progression from interferon beta treatment. 34 Transaminase abnormalities are reported to be more common in males, and infectious episodes are more common in females in adult patients after the first year of fingolimod treatment for relapsing MS. 35
However, to our knowledge, there is a lack of research discussing the gender disparities in the disease burden. Our findings provided epidemiological evidence on the burden difference of MS between males and females. Globally, males had lower morbidity, mortality, and DALYs of MS than females. 14 In this study, although Chinese males had lower ASIR and ASPR than females, they had higher ASDR and age‐standardized DALYs rate. The numbers of deaths and DALYs were also higher in males than females. However, this conclusion should be prudently considered when extrapolated to individuals and a single center due to the possibility of ecological fallacy. The strong effects of gender on the morbidity, activity, progression, and disease burden of MS suggest that sex‐specific treatments are needed for efficacy optimization. However, the current research is insufficient to demonstrate the gender difference in treatment responses and to guide clinical decisions. The sex‐based basic and clinical studies could help with a better understanding of MS and the mechanism of gender difference. Large‐scale studies on gender differences in treatment responses are needed to pave the way for developing sex‐specific personalized treatments. In addition, pregnancy, menstrual cycle, and menopause have important impacts on MS disease activity. The relapse rates of MS decrease during pregnancy but increase in the first 3 months after delivery. 36 Women with MS may experience worsening symptoms before menstruation. 18 Worsening of MS symptoms and greater disability are reported at menopause. 37 The combination of high‐dose estroprogestins and interferon beta has a superior effect compared to single interferon treatment on cognition but showed worsened sexual function. 38 Testosterone treatment has also been demonstrated to have neuroprotective effects and can improve cognitive performance and reverse gray matter atrophy in patients with relapsing‐remitting MS. 39 , 40 Accordingly, sex hormone therapy could be considered a supplementary therapy in subsets of MS patients, while the effect on sexual function should be fully considered. 41
Other measures may be helpful to further improve the management of MS in China. First, strengthening standardized medical education will ensure and improve the level of diagnosis and treatment of MS. Second, regular guidance from tertiary hospitals could help grassroots hospitals improve their treatment level. The disparity in the level of medical care between developed and developing regions may hinder the early diagnosis and systematic treatment of MS in the latter. We should strive to promote medical resource equalization, satisfy the demand for nearby medical services, and reduce the financial and time burden on patients. Third, dual referral between tertiary and grassroots hospitals could ensure comprehensive and proper management throughout the whole process. The case registration system could help to study the overall status of the disease, provide a scientific basis for developing intervention strategies, improve medical services, and adjust medical insurance policies. We also recommend the establishment of multidisciplinary treatment centers, including ophthalmology, neurology, imaging, and rehabilitation departments, to reduce the inconvenience of visiting different departments. Although siponimod, teriflunomide, fingolimod hydrochloride, and fampridine have been covered by national medical insurance in China, the relatively high prices and limited availability of the drugs prevent them from meeting the patients' needs. More studies should be carried out for new medication for MS to address this problem. Increased public spending on healthcare will expand medical insurance coverage and reduce patients' economic burden.
The major limitation of this study is the unavailability of the original surveillance data. Data accuracy, processing, and modeling should be optimized to improve the accuracy of the estimates. The ecological fallacy may occur and affect the conclusion extrapolation to individuals.
5. CONCLUSIONS
In conclusion, Chinese males with MS had a lower prevalence but higher deaths and DALYs than females. The age patterns of MS were similar in prevalence and DALYs rate between genders but different in mortality. The ASDR and age‐standardized DALYs rate have reduced over the past 30 years and were predicted to continue decreasing in the next 25 years, especially in females. The burden of MS in China will remain large in the foreseeable future. The gender differences in the natural history of MS and medication responses are worthy of exploring to guide gender‐specific management and the application of sex hormones. Further improvements are needed in policies, medical level, and scientific research.
AUTHOR CONTRIBUTIONS
Heng Wang: Conceptualization; data curation; formal analysis; methodology; writing—original draft. Xia Zhang: Formal analysis; writing—review and editing. Heyan Li: Formal analysis; methodology. Zixi Sun: Writing—review and editing. Yong Zhong: Project administration; supervision; writing—review and editing.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICS STATEMENT
Ethical approval and informed consent were not required due to the public accessibility of the data.
TRANSPARENCY STATEMENT
The lead author Yong Zhong affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
Supporting information.
Wang H, Zhang X, Li H, Sun Z, Zhong Y. Gender differences in the burden of multiple sclerosis in China from 1990 to 2019 and its 25‐year projection: an analysis of the Global Burden of Diseases Study. Health Sci Rep. 2023;6:e1738. 10.1002/hsr2.1738
DATA AVAILABILITY STATEMENT
All data can be extracted from the GBD 2019 database online (https://ghdx.healthdata.org/gbd-2019). Data are available in a public, open‐access repository. All data are publicly available.
REFERENCES
- 1. Correale J, Gaitán MI, Ysrraelit MC, Fiol MP. Progressive multiple sclerosis: from pathogenic mechanisms to treatment. Brain. 2017;140(3):527‐546. [DOI] [PubMed] [Google Scholar]
- 2. Oh J, Vidal‐Jordana A, Montalban X. Multiple sclerosis: clinical aspects. Curr Opin Neurol. 2018;31(6):752‐759. [DOI] [PubMed] [Google Scholar]
- 3. Bianco A, Antonacci Y, Liguori M. Sex and gender differences in neurodegenerative diseases: challenges for therapeutic opportunities. Int J Mol Sci. 2023;24(7):6354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Yang JH, Rempe T, Whitmire N, Dunn‐Pirio A, Graves JS. Therapeutic advances in multiple sclerosis. Front Neurol. 2022;13:824926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tian DC, Zhang C, Yuan M, et al. Incidence of multiple sclerosis in China: a nationwide hospital‐based study. Lancet Reg Health West Pac. 2020;1:100010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Ma VY, Chan L, Carruthers KJ. Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the United States: stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pain. Arch Phys Med Rehabil. 2014;95(5):986‐995.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Guojun T, Yan X, Weizhi W, et al. A multicenter study to evaluate the disease burden and health economics of inpatients with multiple sclerosis in China. Mult Scler Relat Disord. 2022;60:103732. [DOI] [PubMed] [Google Scholar]
- 8. Walton C, King R, Rechtman L, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult Scler. 2020;26(14):1816‐1821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Lu Y, Gao Q, Ren X, et al. Incidence and prevalence of 121 rare diseases in China: current status and challenges: 2022 revision. Intractable Rare Dis Res. 2022;11(3):96‐104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Feigin VL, Nichols E, Alam T, et al. Global, regional, and national burden of neurological disorders, 1990‐2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459‐480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Sabanagic‐Hajric S, Suljic E, Memic‐Serdarevic A, Mahmutbegovic G. Quality of life in multiple sclerosis patients: influence of gender, age and marital status. Materia Sociomed. 2022;34(1):19‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Wallin MT, Culpepper WJ, Nichols E, et al. Global, regional, and national burden of multiple sclerosis 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(3):269‐285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Li M, Zhou N, Duan S, Zhong H, Jiang R, Yuan N. Burden and trends of multiple sclerosis in China from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open. 2022;12(12):e066335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Qian Z, Li Y, Guan Z, et al. Global, regional, and national burden of multiple sclerosis from 1990 to 2019: findings of global burden of disease study 2019. Front Public Health. 2023;11:1073278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Moghaddam VK, Dickerson AS, Bazrafshan E, et al. Socioeconomic determinants of global distribution of multiple sclerosis: an ecological investigation based on Global Burden of Disease Data. BMC Neurol. 2021;21(1):145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Jacobs BM, Giovannoni G, Cuzick J, Dobson R. Systematic review and meta‐analysis of the association between Epstein–Barr virus, multiple sclerosis and other risk factors. Mult Scler. 2020;26(11):1281‐1297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Horton MK, Shim JE, Wallace A, et al. Rare and low‐frequency coding genetic variants contribute to pediatric‐onset multiple sclerosis. Mult Scler. 2023;29(4‐5):505‐511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Coyle PK. What can we learn from sex differences in MS? J Pers Med. 2021;11(10):1006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Kalincik T, Buzzard K, Jokubaitis V, et al. Risk of relapse phenotype recurrence in multiple sclerosis. Mult Scler. 2014;20(11):1511‐1522. [DOI] [PubMed] [Google Scholar]
- 20. Kalincik T. Multiple sclerosis relapses: epidemiology, outcomes and management. A systematic review. Neuroepidemiology. 2015;44(4):199‐214. [DOI] [PubMed] [Google Scholar]
- 21. Ysrraelit MC, Correale J. Impact of sex hormones on immune function and multiple sclerosis development. Immunology. 2019;156(1):9‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. GBD 2019 Diseases and Injuries Collaborators . Global burden of 369 diseases and injuries in 204 countries and territories, 1990‐2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204‐1222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Institute for Health Metrics and Evaluation . GBD 2019 Data and Tools Overview. 2020.
- 24. Mansouri S, Zayeri F. Global and regional trends of multiple sclerosis disability‐adjusted life years rates: a 25‐year assessment. Neuroepidemiology. 2019;52(1‐2):17‐24. [DOI] [PubMed] [Google Scholar]
- 25. Deuschl G, Beghi E, Fazekas F, et al. The burden of neurological diseases in Europe: an analysis for the Global Burden of Disease Study 2017. Lancet Public Health. 2020;5(10):e551‐e567. [DOI] [PubMed] [Google Scholar]
- 26. Zhang T, Chen H, Yin X, et al. Changing trends of disease burden of gastric cancer in China from 1990 to 2019 and its predictions: findings from Global Burden of Disease Study. Chin J Cancer Res. 2021;33(1):11‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Chen S, Han K, Song Y, et al. Current status, trends, and predictions in the burden of gallbladder and biliary tract cancer in China from 1990 to 2019. Chin Med J (Engl). 2022;135(14):1697‐1706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Luo G, Zhang Y, Etxeberria J, et al. Projections of lung cancer incidence by 2035 in 40 countries worldwide: population‐based study. JMIR Public Health Surveill. 2023;9:e43651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Gold SM, Willing A, Leypoldt F, Paul F, Friese MA. Sex differences in autoimmune disorders of the central nervous system. Semin Immunopathol. 2019;41(2):177‐188. [DOI] [PubMed] [Google Scholar]
- 30. Nytrova P, Dolezal O. Sex bias in multiple sclerosis and neuromyelitis optica spectrum disorders: how it influences clinical course, MRI parameters and prognosis. Front Immunol. 2022;13:933415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Cree BAC, Arnold DL, Chataway J, et al. Secondary progressive multiple sclerosis: new insights. Neurology. 2021;97(8):378‐388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Leray E, Yaouanq J, Le Page E, et al. Evidence for a two‐stage disability progression in multiple sclerosis. Brain. 2010;133(7):1900‐1913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Confavreux C. Early clinical predictors and progression of irreversible disability in multiple sclerosis: an amnesic process. Brain. 2003;126(4):770‐782. [DOI] [PubMed] [Google Scholar]
- 34. Secondary Progressive Efficacy Clinical Trial of Recombinant Interferon‐Beta‐1a in MS Study Group . Randomized controlled trial of interferon‐ beta‐1a in secondary progressive MS: clinical results. Neurology. 2001;56(11):1496‐1504. [DOI] [PubMed] [Google Scholar]
- 35. Manni A, Direnzo V, Iaffaldano A, et al. Gender differences in safety issues during fingolimod therapy: evidence from a real‐life relapsing multiple sclerosis cohort. Brain Behav. 2017;7(10):e00804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Confavreux C, Hutchinson M, Hours MM, Cortinovis‐Tourniaire P, Moreau T. Rate of pregnancy‐related relapse in multiple sclerosis. N Engl J Med. 1998;339(5):285‐291. [DOI] [PubMed] [Google Scholar]
- 37. Bove R, Healy BC, Musallam A, Glanz BI, De Jager PL, Chitnis T. Exploration of changes in disability after menopause in a longitudinal multiple sclerosis cohort. Mult Scler. 2016;22(7):935‐943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. De Giglio L, Marinelli F, Barletta VT, et al. Effect on cognition of estroprogestins combined with interferon beta in multiple sclerosis: analysis of secondary outcomes from a randomised controlled trial. CNS Drugs. 2017;31(2):161‐168. [DOI] [PubMed] [Google Scholar]
- 39. Sicotte NL, Giesser BS, Tandon V, et al. Testosterone treatment in multiple sclerosis: a pilot study. Arch Neurol. 2007;64(5):683‐688. [DOI] [PubMed] [Google Scholar]
- 40. Kurth F, Luders E, Sicotte NL, et al. Neuroprotective effects of testosterone treatment in men with multiple sclerosis. NeuroImage Clin. 2014;4:454‐460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Metzger‐Peter K, Kremer LD, Edan G, et al. The TOTEM RRMS (Testosterone Treatment on neuroprotection and Myelin Repair in Relapsing Remitting Multiple Sclerosis) trial: study protocol for a randomized, double‐blind, placebo‐controlled trial. Trials. 2020;21(1):591. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information.
Data Availability Statement
All data can be extracted from the GBD 2019 database online (https://ghdx.healthdata.org/gbd-2019). Data are available in a public, open‐access repository. All data are publicly available.