

Abstract
Introduction:
The prediction of affective experiences, also known as affective forecasting, is an integral component of individuals’ decision-making processes. Yet, research consistently demonstrates that affective forecasts (AF) and recollections (AR) are generally inaccurate. Recent research has demonstrated distinct patterns of AF/R bias related to psychopathology. The present study examined the relationship between AF/R and features of Borderline Personality Disorder (BPD), anxiety, and depression using Valentine’s Day as the target event.
Methods:
Undergraduate students (N=263; 33% white; 63% female; Mage=19.08) predicted their affective states a week before, and then reported their actual affective states on Valentine’s Day and the two days after, and recalled Valentine’s Day affect two days later.
Results:
Results indicate that higher BPD symptomatology predicted a significant overestimation of negative affect (B=.17, p=.02), even after controlling for anxiety and depression. Additionally, individuals’ levels of depressive, anxious, and BPD symptomatology were significant predictors of AF of positive affect when entered into regression analyses separately, however when entered together, only depressive symptoms remained significant. Specifically, higher depressive symptoms predicted a significant underestimation of positive affect (B=−.21, p=.01).
Discussion:
Results were in line with prior research indicating that unique patterns of AF biases are associated with symptoms of psychopathology. However, results failed to support prior research linking AR biases to symptoms of psychopathology. Implications for future studies of affective biases and psychopathology more generally are discussed.
Keywords: Affective Forecasting, Cognitive Bias, Borderline Personality Disorder, Depression, Anxiety
Introduction
Emotional experiences involve not only experienced affect, but also mental representations (predictions and memories) of affective states, which play an important role in decision-making processes and behaviors. Individuals tend to make decisions based on how they think they will feel as a result—generally attempting to maximize positive affect (PA) and minimize negative affect (NA; Wilson & Gilbert, 2003). Affective forecasting (AF; prediction of future feelings: valence, intensity & duration) and recollection (AR; memory of past feelings) influence individuals’ decisions and behavior across a range of domains (e.g., interpersonal, professional, and recreational) and significance (e.g., major life decisions and minor daily choices; Gilbert et al., 1998; Kurtz, 2018). AF, AR and their accuracy are therefore integral to our understanding of emotions, behaviors, and decision-making processes (Wilson & Gilbert, 2003). In fact, a meta-analysis found that behaviors are often more strongly influenced by forecasted rather than actual affect (DeWall et al., 2016).
While individuals are generally accurate when forecasting/recalling valance (good vs. bad), systematic errors (i.e., biases) become the norm when forecasting/recalling the specifics of emotional reactions—generally overestimating the intensity and duration regardless of valance (Wilson & Gilbert, 2003; Kurtz, 2018). Given AF/R’s centrality in decision making, affective biases could lead to undesirable outcomes (e.g., not ending a ‘toxic relationship’ based on the [over]estimated NA of breaking up; Wenze et al., 2012). Accordingly, researchers have identified specific contributors to affective biases, including focalism (i.e., the tendency to focus on the emotional impact of a specific event without considering the influence of other events), immune neglect (i.e., the tendency to discount one’s ability to cope with NA and habituate to PA), and the peak-and-end rule (i.e., the tendency for the most intense and most recent parts of an experience to have the greatest impact on AF/R; Wilson & Gilbert, 2003; Wilson et al., 2000).
Moving beyond global patterns of bias, researchers have begun exploring the role of between-person factors in AF/R biases. While research on the role of individual differences remains limited, there is preliminary support for the role of emotional intelligence, coping style, mindfulness, and personality traits in AF/R biases (Kurtz, 2018; Wenze et al., 2012). Given the integral role of information-processing biases and emotion dysregulation in psychological disorders, psychopathology symptoms (at both the clinical and subclinical levels) are another between-person factor with promising ties to AF/R biases.
Symptoms of depression (at both clinical and subclinical levels) seem to be linked to a specific pattern of biases in both AF and AR, with higher levels associated with more pessimistically biased AF and AR. Specifically, individuals with more depressive symptoms forecasted and recalled more NA and less PA than they actually experienced—in both nonclinical (Hoerger et al., 2012; Marroquín & Nolen-Hoeksema, 2015; Wenze et al., 2012) and clinical samples (Mathersul & Ruscio, 2019; Zetsche et al., 2019).
Empirical findings regarding biases in the context of anxiety have been more mixed, however. In nonclinical samples, some studies have found higher levels of anxiety to be associated with greater pessimistic bias in the forecasted NA but not PA, nor the AR of either valance (Glenn et al., 2019; Hall et al., 2020; Wenze et al., 2012), while others have failed to find any specific biases related to anxiety (Hoerger et al., 2012; Wenze et al., 2013). Hoerger and colleagues (2012) had individuals’ forecast their affect on Valentine’s Day and found that participants with elevated levels of depression made more pessimistically biased AF compared to those with lower levels of depression, but found no such bias as a function of anxiety levels. In a follow-up study, Martin and Quirk (2015) found that while trait anxiety was, again, not associated with AF bias, social anxiety symptoms did demonstrate a significant positive association with pessimistic AF bias. In the only clinical sample, generalized anxiety disorder severity was associated with more pessimistically biased forecasts and recollection of both NA and PA, but only remained associated with AR biases when controlling for depression severity (Mathersul & Ruscio, 2019). Taken together, these findings may reflect a difference in the dimensional nature of affective biases in anxiety compared to depression, such that subclinical levels of depression demonstrate a similar pattern of bias to that of clinical depression, while subclinical anxiety may not exhibit the same pattern of bias as observed in anxiety disorders.
Borderline Personality Disorder (BPD), considered a disorder of emotion dysregulation (specifically, unstable and intense affect), may also be associated with specific patterns of bias in AF/R. While direct investigations of AF biases in the context of BPD are relatively scant, results from recent ecological momentary assessment (EMA) research has indicated specific AR biases in BPD samples, which in turn may lead to AF biases (Kurtz, 2018). Specifically, individuals with BPD recalled more NA and less PA than experienced (Ebner-Priemer et al., 2007), demonstrated discrepancies between EMA-reported and retrospectively recalled NA (Solhan et al., 2009), and made less accurate AR of the valance of emotions during interpersonal interactions (Brown et al., 2013). Additionally, several cognitive processes associated with BPD may contribute to biases including increased rumination (Selby & Joiner, 2009), disproportionate attention to negative stimuli and access to negative memories, and overall negative beliefs about the world, self, and other people (Baer et al., 2012). Finally, emotion dysregulation mediated the association between trauma symptomatology and more pessimistic affective forecasts regarding both personal and professional negative life events (Rizeq & McCann, 2019).
Despite the indirect evidence of potentially distinct AF/R biases in the context of BPD features, the only study directly investigating it to date found that while increased BPD features were associated with greater forecasted NA, they were also associated with greater experienced/reported NA, which led to greater BPD features being associated with more accurate forecasts (Hughes & Rizvi, 2019). Specifically, participants were asked to forecast how much NA they would feel when they watched a sadness evoking film clip. It is plausible that participants with more BPD features were aware of their emotional reactivity and therefore accurately forecasted that they would experience more NA than those with fewer BPD features. However, the artificial nature of the forecasting paradigm (i.e., occurring in the lab in response to an expected and contrived emotional experience) may limit the generalizability of the findings. Therefore, further research on AF/R biases in the context of BPD, using more naturalistic paradigms, is needed.
Present Study
The present study examined the relationship between AF/R biases and current symptoms of anxiety, depression, and BPD features using Valentine’s Day as the target event, in line with prior work (Hoerger et al., 2012; Martin & Quirk, 2015). In a sample of undergraduate participants, diagnostic features of depression, anxiety, and BPD were examined in relation to patterns of bias in AF/R made regarding emotions on Valentine’s Day. Participants forecasted the extent to which they would feel each of six emotions (3 NA and 3 PA) on Valentine’s Day (2/14), 2/15, and 2/16, then reported their actual affect each day, and recalled their affect from 2/14 on 2/16. We collected forecasts of/ reports from 2/15 and 2/16, as was done in prior AF studies involving Valentine’s Day (Hoerger et al., 2012; Martin & Quirk, 2015), to explore potential differences in AF biases as a function of time from target event (e.g., focalism or immune neglect may interact differently with symptoms of depression than BPD). Given (1) the dimensional nature of depression, anxiety, and BPD, (2) prior work demonstrating AF/R biases linked to symptoms of psychopathology across a range of severities, and (3) the aim of the present study to extend prior research, which was predominantly conducted with non-clinical samples, we felt the use of a student sample, while limiting the clinical implications of the present work, was most appropriate. Further, given the interpersonal difficulties associated with BPD (Linehan, 1993) and the interpersonally sensitive nature of Valentine’s day, a non-clinical sample was preferable for the initial exploration of these constructs as a clinical sample may present with study-interfering safety concerns. We hypothesised that 1) greater symptoms of depression would be associated with more pessimistically biased affective forecasts and recollections (AF/R with more NA and less PA than actually experienced); 2) greater symptoms of anxiety would be associated with more pessimistically biased NA forecasts; and 3) elevated BPD features would be associated with more pessimistically biased AF/R of both positive and negative affect. Additionally, we aimed to assess the unique effects of depression, anxiety, and BPD on AF/R biases when controlling for each other.
Method
Participants
Participants were 263 college students recruited from the online participant pool at a large mid-Atlantic public university and offered extra course credit in exchange for their participation. The sample identified as 62.7% female and 37.3% male. Participants’ ages ranged from 18 to 25 years old (M = 19.08, SD = 1.40; 11 participants declined to report their specific age). Forty-two percent of the sample identified as Asian, 33.1% as White, 3.4% as African American or Black, 6.8% as more than one race, and 2.3% identified as another race. Additionally, 11.8% identified as Hispanic or Latinx. Of the participants, 32.7% were in a committed relationship, 11% were dating but not in a relationship, and 56.3% were single and not dating. On Valentine’s Day, 21.7% of participants had a date, 63.9% did not have a date, and 0.8% declined to report their date status. Based on prior AF research finding date status performed better than relationship status (Horger et al., 2012), date status was use as a covariate for our analyses.
Measures
BPD Features.
The Personality Assessment Inventory, Borderline Personality Subscale (PAI-BOR; Morey, 1991) was used to assess presence and severity of BPD features in participants. On the 24-item self-report subscale, respondents were asked to rate how accurately each statement represents them on a Likert-type scale from 0 (“False/Not at all true”) to 3 (“Very true”). Statements include items such as, “My mood can shift quite suddenly” and, “My relationships have been stormy.” The PAI-BOR demonstrated high internal consistency in the present sample, with a Cronbach’s α of .84.
Depression and Anxiety Symptoms.
The Depression Anxiety and Stress Scale – Short Form (DASS-21; Lovibond & Lovibond, 1995) is a self-report questionnaire, which was used to assess symptoms of depression and anxiety, and experience of stress in participants. The Depression and Anxiety subscales (7 items each) were run as separate variables. Respondents are asked to indicate how often the statements applied to them in the past week, on a Likert-type scale of 0 (“Never”) to 3 (“Almost always”). Items included statements such as, “I felt down-hearted and blue” for depression and, “I felt I was close to panic” for anxiety. The depression subscale had high internal consistency (α = .90), while the anxiety subscale had acceptable internal consistency (α = .78).
Positive and Negative Affect.
Similar to prior AF study designs, forecasted, recalled, and experienced affect was rated using six relevant emotion items: three PA (Happy, Enthusiastic, and Content) and three NA (Sad, Worried, and Embarrassed). Participants rated how strongly they expected to feel or did feel each emotion on a 9-point Likert-type scale from 1 (“Not at all”) to 9 (“Extremely”). The PA and NA items were summed and analysed independently and as separate PA and NA subscales. Reliability was conducted on PA items and NA items for current affect, forecasted affect, and recalled affect for each of the days, with an average Cronbach’s α = .89 (SD = .05, range α = .78 to .95).
Procedure
The study protocol was approved by the institutional review board. After registering for the study online, participants completed a series of online surveys. The first survey, completed during the week before Valentine’s Day, included several measures of psychopathology features, of which the PAI-BOR and DASS were analysed for the purpose of this paper. In the first survey, participants also reported their expected date status for Valentine’s Day, rated how they expected to feel on Valentine’s Day, the day after Valentine’s Day, and two days after Valentine’s Day. Then, on 2/14, 2/15, and 2/16 participants completed brief affect questionnaires for the current day, on 2/14 they reported their actual date status, and on 2/16, they were also asked to recall how they felt on Valentine’s Day.
Data Analytic Strategy
All analyses were conducted using SPSS 25.0 statistical software. First, descriptive statistics of the primary predictor variables (demographics and measures of psychopathology) and outcome variables (affective forecasts, in-vivo reports, and recollections) were examined. We assessed for violations of the assumptions of regressions (e.g., homoscedasticity and outliers), in order to make relevant transformations and removals. We then conducted exploratory factor analyses (EFA) using a direct Oblimin rotation with a delta value of zero (default) used for the rotations and all affect items included to assess if the NA and PA items loaded onto their expected factors. We conducted a total of seven EFAs: one for each AF (of 2/14, 2/15, & 2/16), one for each reported affect (on 2/14, 2/15, & 2/16), and one for AR of 2/14 made on 2/16.
Next, accuracy/bias of AF and AR were assessed using a series of repeated measures ANOVAs to compare affect ratings across time of rating (forecasted vs actual, and actual vs recalled), while controlling for date status (had a date vs did not have a date) and the interaction of time and date status.
In order to assess the potential role of features of psychopathology (i.e., depression, anxiety, and BPD) in AF/R bias, we conducted a series of regression analyses in which each measure of psychopathology was entered as a predictor of forecasted/recalled NA and PA intensity in separate regression equations, while including date status and experienced affect as covariates—a procedure used by previous studies on affective forecasting and recall biases (e.g., Wenze et al., 2012) where the resulting regression coefficients for psychopathology variables reflect their influence of AF/R intensity above and beyond that of their actually experienced affect (i.e., AF/R bias). We then conducted similar regression analyses with all three measures of psychopathology entered as predictors simultaneously, in order to determine each measure’s unique relationship to bias while accounting for shared underlying variance. In order to correct for multiple tests conducted, we conducted the Benjamini-Hochberg Procedure (Benjamini & Hochberg, 1995; setting the false positive rate to 0.05 for 48 separate tests) and determined that a p-value less than 0.02 (instead of 0.05) should be used to indicate significant relationships.
Results
Recruitment and Retention
As participation in the study spanned multiple weeks, not all participants who enrolled in the study completed all parts. A total of 265 participants enrolled in the study. We identified and removed two participants who were significant outliers on all baseline measures due to extreme responding (all minimum ratings for one and all maximum ratings for the other)—leaving a sample of 263 participants; the outlier removals did not alter the overall pattern of results reported below. Two hundred sixty-one participants completed all the baseline questionnaires, 225 (85.55%) made affective forecasts prior to Valentine’s Day, 225 (85.55%) reported their actual affect on Valentine’s Day, 212 (80.61%) reported their actual affect on 2/15, and 184 (69.96%) reported their actual affect and provided affective recollections on 2/16; 179 (68.06%) participants participated in all parts of the study. All available data were used in subsequent analyses, resulting in varied sample sizes across analyses. We assessed whether study dropout was related to any demographic, psychopathology, or AFs through a series of bivariate correlations; no baseline-assessed variables were significantly related to study dropout (all p-values > 0.05).
Descriptive Analyses
Descriptive statistics for affect ratings and measures of psychopathology are displayed in Table 1. Assumptions of regression analyses did not appear to be violated; therefore, no transformations were made. Participants’ scores on the DASS and PAI-BOR fell within the range of prior studies using the measures in young adult samples (Green et al., 2007; Hughes & Rizvi, 2019), however, it is worth noting that average scores were closer to that of clinical populations than that of healthy controls (Henry & Crawford, 2005; Trull et al., 1997). On the DASS-Anxiety subscale, 176 (67.43%) participants scored above the ‘normal’ range, with 109 (41.76%) scoring above the ‘severe’ range. On the depression subscale of the DASS, 138 (52.87%) participants’ scores exceeded the ‘normal’ range and 81 (31.03%) exceeded the ‘severe’ range. On the PAI-BOR, 64 (24.52%) scored above the cut-off for clinically significant BPD features (Morey, 1991).
Table 1.
Descriptive Statistics of all Measures
| Measure | n | Range | Mean (SD) |
||
|---|---|---|---|---|---|
| Total Sample | w/ Date | w/o Date | |||
| PAI-BOR total | 261 | 5–66 | 28.96 (10.84) | 29.71 (9.48) | 28.49 (10.77) |
| DASS-Depression | 261 | 0–42 | 8.45 (8.74) | 8.21 (7.81) | 8.20 (8.84) |
| DASS-Anxiety | 261 | 0–42 | 7.59 (7.11) | 7.79 (7.70) | 7.40 (6.81) |
| AF of 2/14 PA | 225 | 3–27 | 17.30 (7.03) | 22.72 (0.83) | 15.46 (0.49) |
| AF of 2/14 NA | 225 | 3–27 | 8.27 (6.24) | 6.35 (3.82) | 8.92 (6.24) |
| AF of 2/15 PA | 225 | 3–27 | 17.33 (7.04) | 22.06 (0.95) | 15.83 (0.53) |
| AF of 2/15 NA | 225 | 3–27 | 7.31 (6.03) | 5.57 (0.84) | 7.72 (0.47) |
| AF of 2/16 PA | 225 | 3–27 | 17.70 (6.65) | 20.79 (1.01) | 16.70 (0.55) |
| AF of 2/16 NA | 225 | 3–27 | 6.53 (5.26) | 6.05 (4.77) | 7.09 (5.77) |
| 2/14 Reported PA | 225 | 3–27 | 18.64 (6.11) | 21.49 (0.78) | 17.67 (0.46) |
| 2/14 Reported NA | 225 | 3–27 | 7.83 (5.13) | 6.71 (0.64) | 8.50 (0.37) |
| 2/15 Reported PA | 212 | 3–27 | 17.06 (6.14) | 18.22 (0.87) | 16.81 (0.49) |
| 2/15 Reported NA | 212 | 3–27 | 7.84 (5.24) | 8.14 (0.74) | 7.61 (0.42) |
| 2/16 Reported PA | 184 | 3–27 | 18.08 (6.21) | 18.71 (0.96) | 17.93 (0.53) |
| 2/16 Reported NA | 184 | 3–27 | 7.80 (5.31) | 8.31 (5.71) | 7.61 (5.19) |
| AR of 2/14 PA | 184 | 3–27 | 18.17 (6.29) | 21.29 (0.86) | 17.44 (0.47) |
| AR of 2/14 NA | 184 | 3–27 | 7.70 (5.48) | 6.55 (4.76) | 8.01 (5.63) |
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; AF=Affective Forecasting; AR=Affective Recall; NA=Negative Affect; PA=Positive Affect
Factor Analyses
All seven EFAs produced comparable results (i.e., the same items loaded onto the same factors across all EFAs) and are therefore presented summarily. Factor 1 was comprised of the three PA items, with eigenvalues ranging from 3.36 to 3.85 accounting for 58.94 to 64.22% of the total variance and items’ factor loadings ranging from .85 to .97. Factor 2, comprised of the three NA items, had eigenvalues ranging from 1.14 to 1.60 explaining 19.06 to 26.59% of the total variance, and items’ factor loadings ranging from .66 to .96. The factor correlations ranged from −0.56 to −0.38. We then conducted reliability analyses to determine the internal consistency of the NA and PA subscales. Results indicated strong internal consistency, with Cronbach’s alphas ranging from .93 to .95 for PA and .78 to .90 for NA. In sum, factor analyses and reliability of the affect variables indicated that all NA items loaded onto a single factor and all PA items loaded onto a single factor, each of which demonstrated strong internal consistency.
AF & AR Biases as a Function of Time and Date Status
A series of two-way mixed ANOVAs were conducted to examine the main effects of two independent variables (the between-subjects factor of date status [had a date/did not have a date] and the within-subjects factor of time [experienced and forecasted/recalled]), as well as their interaction, on the ratings of PA and NA for Valentine’s Day and the two following days, producing a total of eight ANOVA analyses. A summary of results is presented in the text below and in Table 2, as well as visually in Figure 1.
Table 2.
ANOVA Results
| Date | Effect Type | Effect | F | df | ηp2 | p | |
|---|---|---|---|---|---|---|---|
| Positive Affect | AF of PA on 2/14 | Main Effects | Date Status | 53.82 | 1, 223 | .19 | <.001 |
| Time | 0.80 | 1, 233 | .004 | .37 | |||
| Interaction | Time x Date Status | 9.79 | 1, 233 | .04 | .002 | ||
| Simple Effects | AF: Date vs No Date | 56.71 | 1, 223 | .20 | <.001 | ||
| Experienced: Date vs No Date | 17.86 | 1, 233 | .07 | <.001 | |||
| Date: AF vs Experienced | 1.42 | 1, 56 | .03 | .24 | |||
| No Date: AF vs Experienced | 16.99 | 1, 167 | .09 | <.001 | |||
|
AF of PA on 2/15 |
Main Effects |
Date Status |
19.58 |
1, 205 |
.09 |
<.001 |
|
| Time | 6.05 | 1, 250 | .03 | .015 | |||
| Interaction | Time x Date Status | 17.21 | 1, 250 | .08 | <.001 | ||
| Simple Effects | AF: Date vs No Date | 33.06 | 1, 205 | .14 | <.001 | ||
| Experienced: Date vs No Date | 2.02 | 1, 205 | .01 | .16 | |||
| Date: AF vs Experienced | 16.34 | 1, 48 | .25 | <.001 | |||
| No Date: AF vs Experienced | 2.90 | 1, 157 | .02 | .09 | |||
|
AF of PA on 2/16 |
Main Effects |
Date Status |
6.81 |
1, 180 |
.04 |
.01 |
|
| Time | 0.45 | 1, 180 | .002 | .51 | |||
| Interaction | Time x Date Status | 9.79 | 1, 223 | .04 | .002 | ||
| Simple Effects | AF: Date vs No Date | 12.54 | 1, 180 | .07 | <.001 | ||
| Experienced: Date vs No Date | 19.95 | 1, 180 | .003 | .048 | |||
| Date: AF vs Experienced | 4.33 | 1,41 | .10 | .02 | |||
| No Date: AF vs Experienced | 3.83 | 1, 139 | .03 | .05 | |||
|
AR of PA on 2/14 |
Main Effects |
Date Status |
15.6 |
1, 180 |
.08 |
<.001 |
|
| Time | 0.32 | 1, 180 | .002 | .58 | |||
| Interaction | Time x Date Status | 0.46 | 1, 180 | .003 | .50 | ||
|
Negative Affect |
AF of NA on 2/14 |
Main Effects |
Date Status |
5.87 |
1, 223 |
.03 |
.016 |
| Time | 0.02 | 1, 223 | .001 | .89 | |||
| Interaction | Time x Date Status | 2.97 | 1, 223 | .01 | .09 | ||
|
AF of NA on 2/15 |
Main Effects |
Date Status |
1.21 |
1, 205 |
.01 |
.27 |
|
| Time | 5.40 | 1, 205 | .03 | .02 | |||
| Interaction | Time x Date Status | 6.39 | 1, 205 | .03 | .012 | ||
| Simple Effects | AF: Date vs No Date | 5.01 | 1, 205 | .24 | .02 | ||
| Experienced: Date vs No Date | 0.39 | 1, 205 | .002 | .54 | |||
| Date: AF vs Experienced | 13.74 | 1, 48 | .22 | <.001 | |||
| No Date: AF vs Experienced | 0.04 | 1, 157 | .01 | .85 | |||
|
AF of NA on 2/16 |
Main Effects |
Date Status |
0.05 |
1, 180 |
<.001 |
.83 |
|
| Time | 6.85 | 1, 180 | .04 | .01 | |||
| Interaction | Time x Date Status | 2.72 | 1, 180 | .02 | .10 | ||
|
AR of NA on 2/14 |
Main Effects |
Date Status |
1.89 |
1, 180 |
.01 |
.17 |
|
| Time | 1.42 | 1, 180 | .01 | .23 | |||
| Interaction | Time x Date Status | 0.56 | 1, 180 | .003 | .46 |
Figure 1.
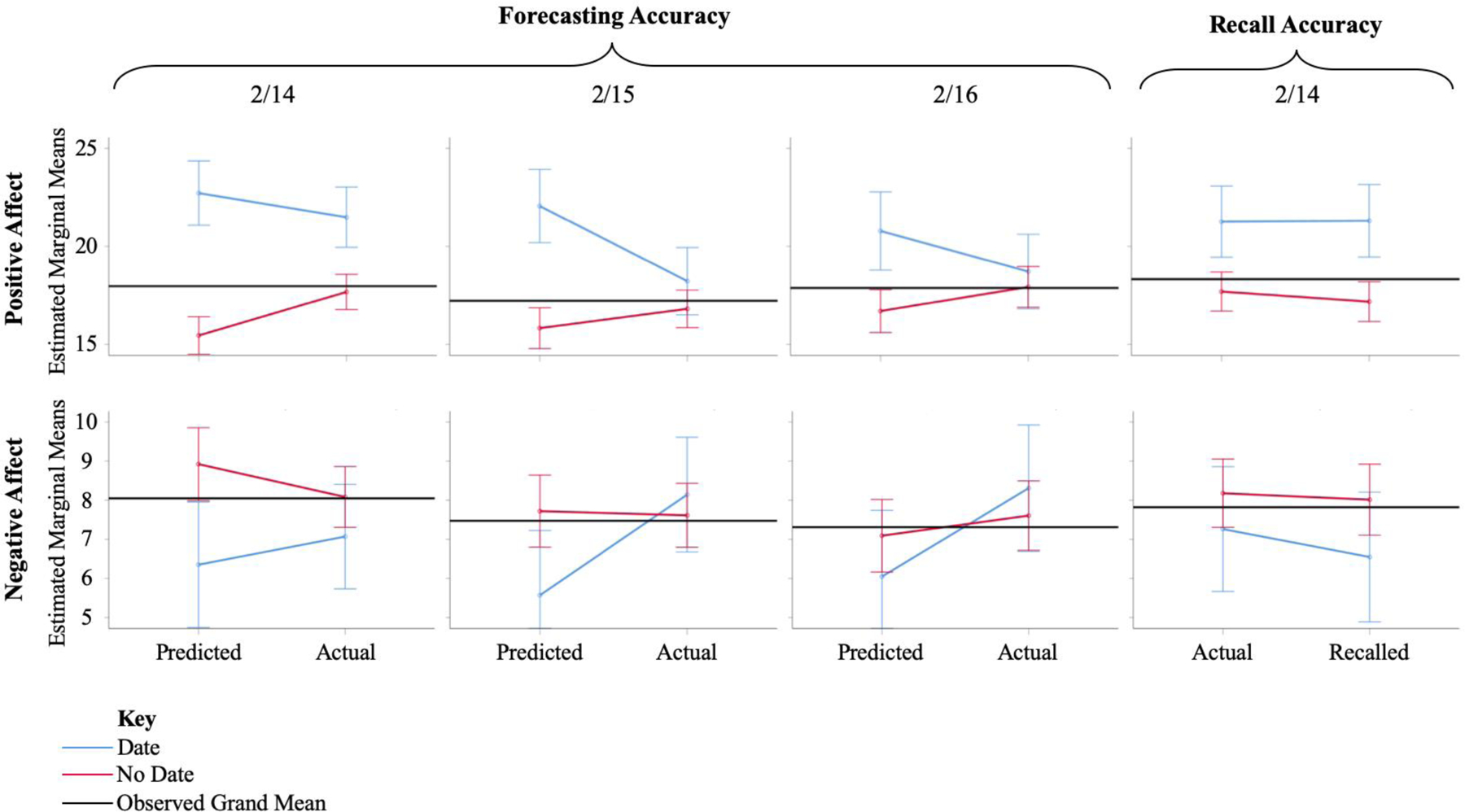
Estimated marginal means of positive and negative affect forecasting and recall accuracy by date status.
Positive Affect
Regarding the forecasted PA for Valentine’s Day, results indicated that there was a significant main effect of date status, but no main effect of time was indicated. Results further indicated that there was a significant time by date status interaction, accounting for 4% of the variance. Specifically, participants without a date forecasted significantly less PA than they experienced, while those with a date forecasted and experienced comparable levels of PA. Further, participants without a date forecasted and experienced significantly less PA than those with one.
Analyses for forecasted PA for 2/15 indicated that there were significant main effects for date status and time, as well as their interaction. Participants with a date forecasted significantly more PA than they experienced while those without a date forecasted and experienced comparable levels of PA. Further, participants without a date forecasted significantly less PA than those with one but experienced comparable levels of PA.
Analyses of forecasted PA for 2/16 produced similar results to that of forecasted PA for Valentine’s Day. There was a significant main effect of date status, no main effect of time, and a significant interaction between time and date status, accounting for 4% of the variance. Specifically, forecasted and experienced PA of participants with a date were not significantly different, nor were the forecasted and experienced PA of participants without a date. Participants without a date forecasted significantly less PA than those with one but experienced comparable levels of PA.
Analyses for recalled PA of Valentine’s Day indicated that there was only a significant main effect of date status, but not for time or their interaction. Participants with a date provided significantly higher ratings of PA than participants without a date, with date status accounting for 8% of the variance.
Negative Affect
Regarding forecasted NA on Valentine’s Day, results indicated that there was a significant main effect of date status, but not for time or their interaction. Participants with a date provided significantly lower ratings of than participants without a date, with date status accounting for 3% of the variance.
Analyses of forecasted NA on 2/15 indicated that there was not a significant main effect of time, nor date status. However, there was a significant time by date status interaction, accounting for 3% of the variance. Specifically, participants with a date forecasted significantly less NA than they experienced, while participants without a date forecasted relatively comparable levels of NA to what they actually experienced. Additionally, those without a date predicted significantly more NA than those with one but experienced comparable levels of NA.
Regarding forecasted NA on 2/16, results indicated that there was a significant main effect of time but not for date status or their interaction. Participants forecasted significantly lower ratings of NA than they actually experienced, with time accounting for 4% of the variance.
Analyses examining recalled NA of Valentine’s Day on 2/16 indicated that there was not significant main of time or date status or interaction effects.
AF & AR and Features of Psychopathology
In order to assess the relationship of features of psychopathology (depression, anxiety, and BPD) on AF/R intensity, we conducted a series of regression analyses in which participants’ forecasted and recalled PA and NA were predicted by psychopathology (first in 3 separate regressions, then simultaneously) while controlling for their actual reported PA/NA, date status, and gender—producing a total of eight sets of regressions, each containing four regressions. The results of the regressions are summarised below and reported in Tables 3–10.
Table 3.
Regression Analyses for 2/14 PA Affect Forecasting
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | 26.57 | 2.76 | 9.64* | .304* | 24.51 | 2.44 | 10.07* | .315* | 23.15 | 2.49 | 9.31* | .282* | 26.45 | 2.73 | 9.72* | .320* |
| Reported Affect | 0.29 | 0.07 | 4.23* | 0.28 | 0.07 | 4.07* | 0.31 | 0.07 | 4.49* | 0.27 | 0.07 | 3.93* | ||||
| Date Status | −6.32 | 0.94 | −6.72* | −6.21 | 0.93 | −6.68* | −6.13 | 0.95 | −6.43* | −6.32 | 0.93 | −6.79* | ||||
| PAI-BOR | −0.12 | 0.04 | −3.36* | −0.08 | 0.04 | −1.81 | ||||||||||
| DASS-Dep | −0.18 | 0.05 | −3.88* | −0.17 | 0.06 | −2.67* | ||||||||||
| DASS-Anx | −0.12 | 0.06 | −2.03 | 0.08 | 0.08 | 1.08 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Table 10.
Regression Analyses for 2/14 NA Affect Recollection
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | 0.54 | 1.48 | 0.36 | .48* | 0.68 | 1.28 | 0.53 | .48* | 0.53 | 1.28 | 0.41 | .48* | 0.61 | 1.50 | 0.40 | .48* |
| Reported Affect | 0.73 | 0.06 | 11.96* | 0.73 | 0.06 | 11.94* | 0.72 | 0.06 | 11.79* | 0.72 | 0.06 | 11.46* | ||||
| Date Status | 0.69 | 0.68 | 1.02 | 0.68 | 0.68 | 1.01 | 0.71 | 0.68 | 1.05 | 0.71 | 0.68 | 1.04 | ||||
| PAI-BOR | 0.01 | 0.03 | 0.26 | 0.00 | 0.03 | −0.09 | ||||||||||
| DASS-Dep | 0.01 | 0.04 | 0.36 | −0.01 | 0.05 | −0.22 | ||||||||||
| DASS-Anx | 0.04 | 0.04 | 0.89 | 0.05 | 0.06 | 0.85 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Positive Affect
Regarding forecasted/recalled PA, models for all days produced a similar pattern of results. Specifically, when entered separately, measures of depression and BPD features were significant predictors along with reported affect and date status1, however, anxiety symptoms only demonstrated a significant relation to AF of PA on 2.16 (but not the 14th and 15th; Tables 3–6). All significant psychopathology variables had negative regression coefficients, indicating that increased levels of psychopathology features contribute to an underprediction of PA intensity after accounting for actual/experienced PA intensity (i.e., more biased predictions of PA intensity) compared to individuals with fewer psychopathology features. When psychopathology measures were entered into the same regression, only symptoms of depression remained significant along with covariates (Tables 3–6). Taken together, this pattern of results indicates that features of depression, BPD, and to a lesser extent anxiety, are each independently associated with greater bias in AF and AR of PA. However, only symptoms of depression significantly influence forecasted/recalled PA intensity beyond the shared underlying variance of the psychopathology variables.
Table 6.
Regression Analyses for 2/14 PA Affect Recollection
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | 12.20 | 2.38 | 5.13* | .54* | 12.72 | 2.14 | 5.95* | .58* | 11.79 | 2.16 | 5.47* | .56* | 12.53 | 2.29 | 5.48* | .58* |
| Reported Affect | 0.69 | 0.06 | 12.50* | 0.66 | 0.05 | 12.50* | 0.68 | 0.05 | 12.75* | 0.66 | 0.05 | 12.44* | ||||
| Date Status | −1.36 | 0.76 | −1.78 | −1.35 | 0.73 | −1.86 | −1.35 | 0.74 | −1.82 | −1.35 | 0.73 | −1.85 | ||||
| Gender | −1.53 | 0.67 | −2.29 | −1.89 | 0.63 | −3.01* | −1.65 | 0.64 | −2.57* | −1.89 | 0.65 | −2.91* | ||||
| PAI-BOR | −0.07 | 0.03 | −2.26* | 0.01 | 0.04 | 0.41 | ||||||||||
| DASS-Dep | −0.17 | 0.04 | −4.68* | −0.14 | 0.05 | −2.84* | ||||||||||
| DASS-Anx | −0.17 | 0.04 | −3.74* | −0.06 | 0.06 | −1.00 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Negative Affect
Results regarding forecast and recall of NA intensity were more varied. Forecasted levels of NA on Valentine’s Day were only predicted by control variables and features of BPD, not depression or anxiety, both when psychopathology variables were entered separately and together (Table 7). Greater levels of BPD features were associated with more intense NA forecasts above and beyond what they actually experienced—BPD features were positively associated with overprediction of NA relative to their actually experienced intensity. NA forecasting biases for 2/15 were significantly predicted by features of both BPD and depression when regressed separately, however neither remained significant when entered simultaneously (Table 8). Forecasted NA for 2/16 was not related to any psychopathology variables, when entered separately or together (Table 9). With regards to recalled intensity of NA, no variables other than actually experienced levels of NA were significant predictors either when regressed separately or together (Table 10). Taken together, results seem to indicate that anxiety, depression, and BPD are significant predictors of NA forecasting bias in the short term (closer to Valentine’s Day), with only BPD features remaining significant when controlling for other psychopathology. Lastly, there does not appear to be a significant relationship between any of our psychopathology variables and NA recall.
Table 7.
Regression Analyses for 2/14 NA Affect Forecasting
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR2 | β | SEβ | t | aR2 | β | SEβ | t | aR2 | β | SEβ | t | aR2 | |
| Intercept | −2.35 | 1.81 | −1.30 | .26* | 0.05 | 1.58 | 0.03 | .24* | 0.03 | 1.60 | 0.02 | .24* | −2.29 | 1.84 | −1.24 | .25* |
| Reported Affect | 0.48 | 0.07 | 6.44* | 0.52 | 0.08 | 6.81* | 0.53 | 0.08 | 6.92* | 0.48 | 0.08 | 6.23* | ||||
| Date Status | 2.21 | 0.83 | 2.66* | 2.05 | 0.84 | 2.44* | 2.07 | 0.84 | 2.45* | 2.20 | 0.83 | 2.64* | ||||
| PAI-BOR | 0.10 | 0.04 | 2.91* | 0.10 | 0.04 | 2.41* | ||||||||||
| DASS-Dep | 0.07 | 0.04 | 1.59 | 0.02 | 0.06 | 0.31 | ||||||||||
| DASS-Anx | 0.07 | 0.05 | 1.25 | −0.01 | 0.07 | −0.20 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Table 8.
Regression Analyses for 2/15 NA Affect Forecasting
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | −2.77 | 2.00 | −1.39 | .15* | −0.44 | 1.74 | −0.25 | .15* | −0.37 | 1.77 | −0.21 | .13* | −2.16 | 2.02 | −1.07 | .16* |
| Reported Affect | 0.32 | 0.08 | 4.25* | 0.30 | 0.08 | 3.91* | 0.33 | 0.08 | 4.28* | 0.30 | 0.08 | 3.84* | ||||
| Date Status | 2.57 | 0.89 | 2.89* | 2.43 | 0.89 | 2.73* | 2.48 | 0.90 | 2.75* | 2.50 | 0.89 | 2.82* | ||||
| PAI-BOR | 0.11 | 0.04 | 2.91* | 0.08 | 0.04 | 1.73 | ||||||||||
| DASS-Dep | 0.14 | 0.05 | 2.94* | 0.11 | 0.06 | 1.75 | ||||||||||
| DASS-Anx | 0.10 | 0.06 | 1.73 | −0.05 | 0.08 | −0.60 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Table 9.
Regression Analyses for 2/16 NA Affect Forecasting
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | −0.03 | 1.84 | −0.02 | .15* | 1.04 | 1.61 | 0.65 | .16* | 1.15 | 1.63 | 0.71 | .15* | 0.48 | 1.87 | 0.25 | .16* |
| Reported Affect | 0.35 | 0.07 | 4.98* | 0.33 | 0.07 | 4.66* | 0.36 | 0.07 | 4.92* | 0.33 | 0.07 | 4.56* | ||||
| Date Status | 1.28 | 0.83 | 1.55 | 1.20 | 0.82 | 1.46 | 1.24 | 0.83 | 1.49 | 1.22 | 0.83 | 1.48 | ||||
| PAI-BOR | 0.05 | 0.03 | 1.57 | 0.03 | 0.04 | 0.67 | ||||||||||
| DASS-Dep | 0.10 | 0.04 | 2.20 | 0.10 | 0.06 | 1.67 | ||||||||||
| DASS-Anx | 0.06 | 0.05 | 1.06 | −0.04 | 0.07 | −0.55 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Discussion
To examine the relationship between psychopathology (i.e., depression, anxiety, and BPD features) and biases in forecasted/recalled affect intensity, the present study recruited individuals to complete surveys regarding how they anticipated feeling on Valentine’s Day and two days following this target event. Participants completed measures of actual emotion for each of these days (i.e., 2/14, 2/15, 2/16) and on 2/16, they were asked to recall how they felt on Valentine’s Day. Results generally supported study hypotheses as related to biases in AF, while fewer significant relationships were found with patterns of AR biases. This built on prior work examining symptoms of anxiety and depression in the context of AF/R biases, and was one of the first to examine affective biases within the context of BPD features. Such research is important considering that affective instability is the most endorsed criterion of BPD and the strongest predictor of suicidal behaviors (Linehan, 1993; Skodol et al., 2002). AF biases may serve as a link between cognitive and emotion dysregulation in BPD; an increased understanding of this overall pattern of bias could help to identify novel points of intervention and treatment targets for clinicians.
In general, participants forecasted that they would experience more NA and less PA on Valentine’s Day than they actually experienced. Through a series of ANOVAs, we explored the accuracy of forecasted/recalled NA/PA intensity relative to experienced NA/PA (effect of time) and the role of date status. In line with previous studies investigating AF biases and Valentine’s Day (Hoerger et al., 2012), we observed that participants with a date demonstrated an optimistic AF bias, predicting more PA and less NA than they actually experienced, while those without a date generally exhibited a pessimistic bias, forecasting less PA and more NA than they actually experienced. Effects were generally stronger on Valentine’s Day and decreased over 2/15 and 2/16, perhaps due to focalism on Valentine’s Day given the salience of the forecasting target. Participants were relatively accurate when recalling PA or NA, perhaps due in part to the discrepancy in AF and AR timeline: AFs were made at least seven days prior while ARs were made after only three days.
We assessed the influence of psychopathology symptoms (depression, anxiety, and BPD) on AF/R intensity through a series of regression analyses, where forecasted or recalled NA or PA was predicted by psychopathology variables (first entered separately, then simultaneously), while controlling for date status and actual NA/PA experienced. The regressions demonstrated that participants predicted and remembered experiencing less PA and more NA than they actually experienced, and these discrepancies increased as symptom severity increased.
In line with prior work investigating psychopathology symptoms’ relation to AF/R biases, we found depressive symptoms to be most robustly related to AF/R biases in the context of PA (Hoerger et al., 2012; Mathersul & Ruscio, 2019; Wenze et al., 2012 & 2013; Zetsche et al., 2019). Extending prior work through the inclusion of BPD features along with symptoms of anxiety and depression, we found that BPD is predictive of PA forecasting bias when entered independently. However, when depression was also included in the model, BPD features became non-significant—indicating that while BPD features are related to AF bias of PA, it does not predict bias above and beyond that of its shared variance with symptoms of depression. The fact that forecasts for the days following Valentine’s Day demonstrated similar patterns of bias seems to support the notion that symptoms of depression are associated with a pessimistic AF/R bias of PA, perhaps due to global anhedonia. The observed depression-related biases could also be contributed to by other cognitive factors associated with depression like worry and rumination.
Turning to NA, contrary to hypotheses and prior research (e.g., Hoerger et al., 2012; Wenze et al., 2012), we did not find depression or anxiety symptoms to be related to NA forecasting bias—even when entered separately. Extending prior work, we did, however, find support for BPD features predicting NA forecasting bias on Valentine’s Day and 2/15, but not 2/16 or when recalling NA, and only on Valentine’s Day when controlling for depressive symptoms. This pattern of results seems to indicate that individuals with greater BPD features exhibit a pessimistic pattern of AF bias that is observed when forecasting affect close to the target event.
Overall, anxiety symptoms were not significant predictors of AF/R intensity bias when controlling for BPD and depression symptoms. This, again, may be due to bias being driven by shared features of anxiety, depression, and BPD. However, the lack of significant findings when entering anxiety separately speaks to other issues at play. For example, this may be due to the non-clinical nature of our sample; previous discrepancies between studies on AF biases and anxiety have been attributed to a less dimensional relationship between anxiety and affective biases, compared to depression, such that subclinical levels of anxiety don’t demonstrate the same pattern of AF or AR biases. The lack of significant results involving anxiety symptoms, while at odds with the findings of Wenze and colleagues (2012), adds to the growing body of literature suggesting that anxiety is less relevant to AF/R at sub-clinical levels than symptoms of depression or BPD (Hoerger et al., 2012; Wenze et al., 2013). Additionally, our use of a general anxiety measure may have contributed as prior work has found more success using disorder specific (e.g., social anxiety and generalized anxiety disorder) measures (Glenn et al., 2019; Mathersul & Ruscio, 2019) and one study found that social anxiety but not trait anxiety predicted AF bias (Martin & Quirk, 2015).
Taken together, results indicate that while symptoms of depression and BPD, and to some extent anxiety, are related to AF/R biases, symptoms of depression are the only ones uniquely predictive of biases in AF/R of PA above and beyond the shared underlying features of the disorders/their symptoms. Further, and most at odds with prior research, symptoms of depression and anxiety were not predictive of bias in the prediction of NA. Instead, BPD features were predictive of AF biases on Valentine’s Day and the 15th, indicating the bias observed is likely more central to Valentine’s Day than AF more broadly, which makes sense given the heightened reactivity to interpersonal events associated with BPD (Skodol et al., 2002). The interpersonal nature of Valentine’s Day, and salience of interpersonal events to BPD, could further help explain the different pattern of results for BPD features compared to anxiety and depression symptoms. The lack of bias related to AR of NA could be due to the limited time between reporting and recall of NA on Valentine’s Day and may explain the lack of significant results.
Limitations and Future Directions
There are several limitations of this study that must be acknowledged and addressed in future research. First, the use of a non-clinical sample likely limits the generalizability of findings to clinical populations as well as potentially contributing to different patterns of/relations to bias, particularly for anxiety symptoms, which seems to function less dimensionally (Martin & Quirk, 2015). Future studies would benefit from sampling clinical populations. Future research could also expand upon the present findings by investigating AF/R biases in the context of other psychopathology (e.g., the role of AF biases, particularly about withdrawal/cravings, in substance use disorders). Second, the difference in time discrepancy between AF and AR (i.e., > 7 days vs < 3 days) limits the interpretability of the AR findings and makes comparison to AF findings problematic. Future research should assess AF and AR with comparable time-delays from the forecasting/recall event. Third, the emotions being assessed were of limited scope (3 PA & 3 NA); future work would benefit from expanding on the specific emotions being assessed and analysed. Fourth, potentially related processes and alternative sources of bias like personality traits (e.g., neuroticism) and cognitive processes (e.g., worry and rumination) were not measured and therefore could not be assessed or controlled for; subsequent studies should do so to explore their potential role in AF/R biases. Fifth, participants AF/R were limited to one target event, Valentine’s Day, which may produce different patterns of bias than other events (e.g., Christmas), especially less interpersonally relevant ones. Future studies should include multiple target events, similar to how Martin and Quirk’s 2010 study involved forecasts of Valentine’s Day and St. Patrick’s Day. Sixth, this study relied upon self-reports and subjective ratings of emotional states, which may be impacted by factors such as response bias. To elicit more naturalistic emotional responses, previous studies have implemented behavioral paradigms such as situations involving exclusion (Williams & Jarvis, 2006), aggression, or invalidation (Herr et al., 2015). Future research may also benefit from using a more frequent EMA method rather than a daily diary to decrease the time between the individual’s affective experience and report, thereby reducing the potential recall bias introduced by time. More frequent affect assessment and prediction would also facilitate analyses regarding how affective experiences and biases vary within-person over time (i.e., are individuals more or less prone to pessimistic forecasts in the morning or evening). Finally, the current sample is relatively imbalanced in terms of date status, which may have hindered analyses that used date status as a predictor. Future research should replicate these findings using larger or stratified samples to ensure adequate subgroups to examine variables of interest.
Table 4.
Regression Analyses for 2/15 PA Affect Forecasting
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | 24.82 | 2.65 | 9.36* | .29* | 23.51 | 2.32 | 10.14* | .30* | 21.75 | 2.29 | 9.49* | .30* | 25.32 | 2.63 | 9.62* | .31* |
| Reported Affect | 0.36 | 0.07 | 5.11* | 0.31 | 0.07 | 4.39* | 0.38 | 0.07 | 5.47* | 0.30 | 0.07 | 4.20* | ||||
| Date Status | −5.79 | 0.96 | −6.05* | −5.70 | 0.94 | −6.04* | −5.66 | 0.96 | −5.87* | −5.78 | 0.95 | −6.12* | ||||
| PAI-BOR | −0.12 | 0.04 | −3.02* | −0.07 | 0.05 | −1.49 | ||||||||||
| DASS-Dep | −0.18 | 0.05 | −3.70* | −0.17 | 0.07 | −2.43* | ||||||||||
| DASS-Anx | −0.13 | 0.06 | −2.22 | 0.05 | 0.08 | 0.62 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Table 5.
Regression Analyses for 2/16 PA Affect Forecasting
| Model 1 (PAI-BOR & Covariates) |
Model 2 (DASS-Dep & Covariates) |
Model 3 (DASS-Anx & Covariates) |
Model 4 (All Variables) |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | β | SEβ | t | aR 2 | |
| Intercept | 21.33 | 2.77 | 7.70* | .22* | 20.97 | 2.39 | 8.79* | .25* | 19.61 | 2.41 | 8.15* | .22* | 21.72 | 2.72 | 8.00* | .25* |
| Reported Affect | 0.35 | 0.07 | 4.80* | 0.29 | 0.07 | 4.00* | 0.34 | 0.07 | 4.76* | 0.29 | 0.07 | 3.95* | ||||
| Date Status | −3.98 | 1.01 | −3.95* | −3.89 | 0.98 | −3.97* | −3.92 | 1.00 | −3.90* | −3.93 | 0.99 | −3.98* | ||||
| PAI-BOR | −0.10 | 0.04 | −2.46* | −0.03 | 0.05 | −0.56 | ||||||||||
| DASS-Dep | −0.20 | 0.05 | −3.95* | −0.18 | 0.07 | −2.57* | ||||||||||
| DASS-Anx | −0.17 | 0.06 | −2.66* | 0.00 | 0.08 | −0.05 | ||||||||||
p<0.02
PAI-BOR=Personality Assessment Inventory-Borderline Personality Disorder Subscale; DASS=Depression Anxiety & Stress Scale; Dep=Depression; Anx=Anxiety
Footnotes
Gender was not significant in any models other than the AR of PA, and therefore we present the regression results without gender for all but the AR of PA models
References
- Baer R, Peters J, Eisenlohr-Moul T, Geiger P, & Sauer S (2012). Emotion-related cognitive processes in borderline personality disorder: a review of the empirical literature. Clinical Psychology Review, 32(5), 359–369. [DOI] [PubMed] [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal statistical society: series B (Methodological), 57(1), 289–300. [Google Scholar]
- Brown W, Tragesser S, Tomko R, Mehl M, & Trull T (2013). Recall of expressed affect during naturalistically observed interpersonal events in those with borderline personality disorder or depressive disorder. Assessment, 21(1), 73–81. [DOI] [PubMed] [Google Scholar]
- DeWall C, Baumeister R, Chester D, & Bushman B (2016). How often does currently felt emotion predict social behavior and judgment? A meta-analytic test of two theories. Emotion Review, 8(2), 136–143. [Google Scholar]
- Ebner-Priemer U, Kuo J, Kleindienst N, Welch S, Reisch T, Reinhard I, Lieb K, Linehan M, & Bohus M (2007). State affective instability in borderline personality disorder assessed by ambulatory monitoring. Psychological medicine, 37(7), 961–970. [DOI] [PubMed] [Google Scholar]
- Gilbert D, Pinel E, Wilson T, Blumberg S, & Wheatley T (1998). Immune neglect: A source of durability bias in affective forecasting. Journal of Personality and Social Psychology, 75(3), 617. [DOI] [PubMed] [Google Scholar]
- Glenn J, Chow P, & Teachman B (2019). How Badly Will I Feel if You Don’t Like Me? Social Anxiety and Predictions of Future Affect. Journal of social and clinical psychology, 38(3), 245–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall KA, Coleman K, & Timpano K (2020). Associations between social anxiety and affective and empathic forecasts: A replication and extension in a Mechanical Turk sample. Behavior therapy, 51(3), 365–374. [DOI] [PubMed] [Google Scholar]
- Henry J, & Crawford J (2005). The short‐form version of the Depression Anxiety Stress Scales (DASS‐21): Construct validity and normative data in a large non‐clinical sample. British Journal of Clinical Psychology, 44(2), 227–239. [DOI] [PubMed] [Google Scholar]
- Herr N, Jones A, Cohn D, & Weber D (2015). The impact of validation and invalidation on aggression in individuals with emotion regulation difficulties. Personality Disorders: Theory, Research, and Treatment, 6(4), 310–314. [DOI] [PubMed] [Google Scholar]
- Hoerger M, Quirk S, Chapman BP, & Duberstein PR (2012). Affective forecasting and self-rated symptoms of depression, anxiety, and hypomania: Evidence for a dysphoric forecasting bias. Cognition & Emotion, 26(6), 1098–1106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes C, & Rizvi S (2019). Biases in affective forecasting and recall as a function of borderline personality disorder features. Journal of Social and Clinical Psychology, 38(3), 200–223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kurtz J (2018). Affective forecasting. Handbook of Wellbeing, eds Diener E, Oishi S, and Tay L (Salt Lake City, UT: DEF Publishers; ). [Google Scholar]
- Linehan M (1993). Cognitive-behavioral Treatment of Borderline Personality Disorder Guilford Press. [Google Scholar]
- Lovibond P & Lovibond S (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behavioral Research and Therapy, 33, 335–342. [DOI] [PubMed] [Google Scholar]
- Marroquín B, & Nolen-Hoeksema S (2015). Event prediction and affective forecasting in depressive cognition: Using emotion as information about the future. Journal of Social and Clinical Psychology, 34(2), 117–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin SM, & Quirk SW (2015). Social anxiety and the accuracy of predicted affect. Cognition and Emotion, 29(1), 51–63. [DOI] [PubMed] [Google Scholar]
- Mathersul D & Ruscio A (2019). Forecasting the future, remembering the past: Misrepresentations of daily emotional experience in generalized anxiety disorder and major depressive disorder. Cognitive Therapy and Research, 1–16.31462838
- Morey L (1991). Personality assessment inventory Odessa, FL: Psychological Assessment Resources. [Google Scholar]
- Rizeq J, & McCann D (2019). Trauma and affective forecasting: The mediating effect of emotion dysregulation on predictions of negative affect. Personality and Individual Differences, 147, 172–176. [Google Scholar]
- Selby E, & Joiner T (2009). Cascades of emotion: The emergence of borderline personality disorder from emotional and behavioral dysregulation. Review of General Psychology, 13(3), 219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skodol AE, Gunderson JG, Pfohl B, Widiger TA, Livesley WJ, & Siever LJ (2002). The borderline diagnosis I: psychopathology, comorbidity, and personaltity structure. Biological psychiatry, 51(12), 936–950. [DOI] [PubMed] [Google Scholar]
- Solhan M, Trull T, Jahng S, & Wood P (2009). Clinical assessment of affective instability: Comparing EMA indices, questionnaire reports, and retrospective recall. Psychological Assessment, 21(3), 425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trull T, Useda J, Conforti K, & Doan B (1997). Borderline personality disorder features in nonclinical young adults: 2. Two-year outcome. Journal of abnormal psychology, 106(2), 307–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenze S, Gunthert K, Ahrens A, & Bos T (2013). Biases in short-term mood prediction in individuals with depression and anxiety symptoms. Individual differences research, 11(3), 91. [PMC free article] [PubMed] [Google Scholar]
- Wenze S, Gunthert K, & German RE (2012). Biases in affective forecasting and recall in individuals with depression and anxiety symptoms. Personality and Social Psychology Bulletin, 38(7), 895–906. [DOI] [PubMed] [Google Scholar]
- Williams K & Jarvis B (2006). Cyberball: A program for use in research on interpersonal ostracism and acceptance. Behavior Research Methods 38(1), 174–180. [DOI] [PubMed] [Google Scholar]
- Wilson T, & Gilbert D (2003). Affective forecasting. Advances in Experimental Social Psychology, 35, 345–411. [Google Scholar]
- Wilson T, Wheatley T, Meyers J, Gilbert D, & Axsom D (2000). Focalism: A source of durability bias in affective forecasting. Journal of Personality and Social Psychology, 78, 821–836. [DOI] [PubMed] [Google Scholar]
- Zetsche U, Bürkner PC, & Renneberg B (2019). Future expectations in clinical depression: Biased or realistic?. Journal of Abnormal Psychology, 128, 678–688. [DOI] [PubMed] [Google Scholar]