

Abstract
Objectives:
Broadband access is an essential social determinant of health, the importance of which was made apparent during the COVID-19 pandemic. We sought to understand disparities in broadband access within cities and identify potential solutions to increase urban access.
Study design:
This was a descriptive secondary analysis using multi-year cross-sectional survey data.
Methods:
Data were obtained from the City Health Dashboard and American Community Survey. We studied broadband access in 905 large US cities, stratifying neighborhood broadband access by neighborhood median household income and racial/ethnic composition.
Results:
In 2017, 30% of urban households across 905 large US cities did not have access to high-speed broadband internet. After controlling for median household income, broadband access in majority Black and Hispanic neighborhoods was 10–15% lower than in majority White or Asian neighborhoods. Over time, lack of broadband access in urban households decreased from 30% in 2017 to 24% in 2021, but racial and income disparities persisted.
Conclusions:
As an emerging social determinant, broadband access impacts health across the life course, affecting students’ ability to learn and adults’ ability to find and retain jobs. Resolving lack of broadband access remains an urban priority. City policymakers can harness recent infrastructure funding opportunities to reduce broadband access disparities.
Keywords: Social Determinants of Health, Health disparities, Minority health, Urban health
Introduction
Access to fast, reliable internet (“broadband”) is an important resource for obtaining essential services and information, including for health.1 Broadband internet is widely used to access health-related resources, including remote monitoring of medical devices, delivery of healthy food from Web-based food services, and medical information.1 Conversely, lack of broadband hinders access to essential health-related services and social services. For example, broadband access facilitates access to health care, an ability to work from home (thereby reducing exposure to COVID-19), ability to access remote learning, and other essential goods and services.2,3 The ongoing COVID-19 pandemic has exacerbated the consequences of lack of broadband access, raising awareness of its importance, especially for racial/ethnic minority populations and in rural communities.1,4 Despite the growing importance of broadband in daily life, a substantial number of US residents still lack access.2,5
Researchers have characterized city-rural differences in internet access.2,6 Rural communities are more likely than city communities to suffer from lack of any type of internet access. In 2018, 19% of rural households still had no form of internet, compared with 14% of city households. Even fewer households had access to high-speed broadband internet services.7 Requirements for access to high-speed broadband internet services are multifaceted, including whether or not broadband infrastructure and subscription services exist where a given household is located, whether the members of that household can afford to purchase a broadband internet subscription, whether the internet infrastructure meets the minimum speed requirement (25 Megabytes per second [download]/3 Megabytes per second [upload]) to be classified as “high-speed,”8 whether that household can navigate how to connect to internet, and then chooses to adopt high-speed broadband internet services. This is consistent with social inclusion theories9,10 and broadband access as a social determinant of health.1,11 Many studies have attributed these disparities to the lack of investment and deployment of broadband infrastructure in rural areas.2,6 In the 2021 infrastructure bill, $65 billion dollars were allocated to build broadband infrastructure in unserved and underserved areas, a step that should help to ameliorate infrastructure barriers to broadband connection.12 Yet, while most US cities now have the physical infrastructure to support broadband access for all residents,13 substantial disparities in broadband access persist within and across neighborhoods. Broadband gaps in cities are largely influenced by lack of affordability, disparities in digital literacy, and difficulties accessing broadband among populations with lower educational attainment and language barriers.5,14 Previous research has also found evidence of profit-based discrimination in service delivery contributing to racial and geographic disparities in broadband access.9 These factors suggest that infrastructure improvements alone may not be sufficient to eliminate disparities in broadband access for urban households.15
Gaps in broadband access within cities have not been as well characterized as city-rural broadband access disparities. To characterize within-city broadband access disparities across cities, and neighborhoods within them, we examined disparities in broadband access in 905 US cities (consisting of urbanized areas and urban clusters defined by Census16) by contrasting household median-level broadband internet access at the neighborhood level within cities (proxied by Census tract, a small, relatively permanent statistical subdivision of a county, drawn by the Census Bureau) using the data from American Community Survey (ACS), 2017–2021. To understand racial/ethnic and income disparities in broadband access, we stratified by neighborhood racial/ethnic composition and median household income. The goal of this analysis was to provide policymakers and researchers with a clear understanding of within-city disparities in broadband access to identify potential solutions to increase access and utilization.
Methods
We conducted a secondary data analysis using US Census ACS data provided by the City Health Dashboard (the Dashboard). The Dashboard includes all US cities, defined as census incorporated places and minor civil divisions with functioning governments, with a 2020 Decennial Census population of 50,000 or more (n = 861) and 44 additional cities with population between 2800 and 49,578. The complete list of 905 cities can be found on the Dashboard website.17 Broadband Access, as presented on the Dashboard and calculated by ACS, is defined as the percentage of households with self-reported connections to high-speed broadband internet (including cable, fiber optic, and digital subscriber line DSL (digital subscriber line) connections).18,19 Because ACS measured active broadband internet subscription in a household, this definition not only measured the availability of broadband infrastructure but also that the household chose and could afford to purchase broadband subscription.
The metric is reported by ACS as a percentage and presented as reported by ACS on the Dashboard. Households with only cellular data plans are excluded from this metric because cellular plans do not support the range of internet services provided by high-speed broadband.20 We analyzed data from the years 2017–2021 for city and neighborhood broadband access.
We calculated the median percentage of households reporting broadband access at neighborhood level and further disaggregated estimates by median household income and neighborhood racial/ethnic composition. We used one-way analysis of variance to test whether the difference of broadband access across racial/ethnic groups within each income stratum is statistically significant. For median household income disaggregation, we assigned neighborhoods within cities to income quartiles (low, low to medium, medium to high, and high income) using ACS 5-year estimates (ACS variable S1901_C01_012E) relative to the other cities and neighborhoods displayed on the Dashboard. As a robustness check, we reanalyzed the data using different income cut-offs to avoid potential artifactual inferences resulting from cut-off selection (Table A2 & A3). For racial/ethnic composition disaggregation, we categorized neighborhood racial/ethnic composition by whether a racial/ethnic group comprised over half of the total population in the city/neighborhood (ACS table: DP05). Race/ethnicity categories included Asian Americans (AA), non-Hispanic Black (Black), Hispanic/Latino (Hispanic), non-Hispanic White (White), American Indian, Native Hawaiian, and other Pacific Islander (AI or NH&PI, as a single group due to low counts). Neighborhoods without an absolute majority race/ethnicity were categorized as no majority. In the “no majority” group, the average distribution of White, non-Hispanic Black, Hispanic, and AA was 35%, 20%, 28%, and 15%, respectively. As a sensitivity analysis, we also classified neighborhoods based on which racial/ethnic group had the highest population percentage, even if that percentage did not represent a majority of the city/neighborhood’s population. The results of this analysis are displayed in Appendix.
Results
Across Dashboard cities, on average, three-quarters of households (76.5%) were connected to broadband internet in 2021. Income and racial/ethnicity were associated with broadband access (Table 1). The median broadband access by median household income suggested that high-income neighborhoods had the highest broadband access rate (87.2%) and low-income neighborhoods had the lowest broadband access rate (58.8%). The median broadband access by race/ethnicity group suggested that AA majority neighborhoods had the highest broadband access rate (82.3%), followed by White majority neighborhoods (81.2%) and neighborhoods with no majority race/ethnicity (76.1%). Black- and Hispanic-majority neighborhoods had the lowest broadband access rate (59% and 65.4%, respectively). At least 75% of the AA and White majority neighborhoods had higher broadband access rate than the top 25% of Black and Hispanic neighborhoods. The upper quartile of broadband access among the Black- and Hispanic-majority neighborhoods were 69.6% and 74%, respectively. In contrast, the lower quartile of broadband access among the AA and White majority neighborhoods was 73% (Fig. 1 and Table 1).
Table 1.
Broadband access rates by income and majority race/ethnicity, 2017–2021.
| Race/ethnicity | 2017 |
2018 |
2019 |
2020 |
2021 |
# tracts (2020) | % change |
|---|---|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | |||
| Low income: 1st quantile (<45,250 in 2020) | |||||||
| F test (P) | 431.1 (<0.001) | 435.6 (<0.001) | 408.7 (<0.001) | 337.7 (<0.001) | 283.9 (<0.001) | ||
| AI or NH&PI | 36.5 (27.1, 46.7) | 40.0 (30.8, 47.4) | 46.3 (39.5, 51.7) | 48.0 (45.7, 59.2) | 51.2 (49.1, 65.9) | 7 | 40.3 |
| Asian | 56.5 (48.8, 63.2) | 54.3 (49.7, 65.2) | 52.5 (46.2, 60.6) | 55.0 (44.2, 65.9) | 56.3 (49.4, 68.4) | 86 | −0.3 |
| Black | 42.4 (34.4, 50.3) | 43.9 (35.5, 51.8) | 45.9 (37.2, 53.8) | 50.1 (40.9, 58.7) | 53.2 (44.1, 61.9) | 2980 | 25.5 |
| Hispanic | 45.7 (37.4, 54.2) | 47.2 (39.1, 55.3) | 49.2 (41.3, 56.8) | 52.8 (44.4, 60.3) | 56.3 (47.7, 63.9) | 2391 | 23.2 |
| No majority | 52.2 (43.9, 59.1) | 53.6 (45.7, 61.3) | 55.2 (47.4, 62.5) | 59.1 (50.6, 66.3) | 61.8 (53.5, 69.2) | 1887 | 18.4 |
| White | 57.8 (50.2, 65.0) | 59.3 (51.9, 66.2) | 61.0 (53.5, 67.6) | 63.3 (55.7, 70.5) | 65.7 (57.6, 72.4) | 2323 | 13.7 |
| Total | 48.5 (39.0, 57.1) | 49.9 (40.6, 58.8) | 51.7 (42.5, 60.4) | 55.9 (46.3, 64.3) | 58.8 (49.5, 67.1) | 9674 | 21.2 |
|
| |||||||
| Low to medium income: 2nd quantile (45,250–64,395 in 2020) | |||||||
| F test (P) | 326.9 (<0.001) | 297.9 (<0.001) | 257.2 (<0.001) | 226.2 (<0.001) | 189.6 (<0.001) | ||
|
| |||||||
| AI or NH&PI | 59.4 (59.4, 59.4) | 54.2 (54.2, 54.2) | 63.2 (63.1, 65.0) | 57.2 (52.4, 59.8) | 57.6 (54.2, 63.2) | 5 | −3 |
| Asian | 68.1 (61.3, 73.1) | 68.0 (62.8, 72.3) | 69.6 (62.4, 74.0) | 69.5 (62.8, 75.6) | 70.9 (64.7, 77.2) | 167 | 4.1 |
| Black | 60.1 (54.4, 65.9) | 61.8 (55.3, 67.4) | 63.4 (56.8, 69.1) | 66.5 (59.2, 72.4) | 68.4 (61.0, 74.7) | 897 | 13.8 |
| Hispanic | 58.7 (51.1, 65.0) | 59.9 (52.9, 66.5) | 61.7 (54.8, 67.9) | 64.7 (57.3, 71.1) | 67.0 (60, 73.4) | 2177 | 14.1 |
| No majority | 65.7 (59.5, 71.5) | 66.6 (60.6, 72.4) | 68.0 (62.0, 73.7) | 71.1 (64.5, 77.2) | 72.6 (66.3, 78.6) | 2002 | 10.6 |
| White | 68.0 (62.4, 73.3) | 69.2 (63.5, 74.3) | 70.3 (64.7, 75.5) | 72.7 (66.6, 78.3) | 74.4 (68.4, 79.8) | 4423 | 9.4 |
| Total | 64.9 (58.2, 71.0) | 66.0 (59.2, 72.0) | 67.3 (60.6, 73.3) | 70.1 (63.2, 76.5) | 71.9 (65.0, 78.1) | 9671 | 10.8 |
|
| |||||||
| Medium to high income 3rd quantile (64,395–90,803 in 2020) | |||||||
| F test (P) | 118.6 (<0.001) | 121.4 (<0.001) | 119.3 (<0.001) | 148.9 (<0.001) | 138.7 (<0.001) | ||
|
| |||||||
| AI or NH&PI | 65.9 (63.4, 70.0) | 64.9 (62.4, 67.2) | 64.4 (64.0, 66.9) | 67.8 (65.5, 70.2) | 69.0 (67.7, 75.8) | 5 | 4.7 |
| Asian | 74.5 (69.6, 78.9) | 75.2 (70.8, 79.4) | 74.7 (69.0, 78.8) | 75.4 (70.3, 81.2) | 78.0 (71.5, 82.2) | 242 | 4.7 |
| Black | 71.0 (64.7, 76.4) | 71.6 (65.4, 76.6) | 72.5 (65.7, 77.8) | 73.9 (65.7, 79.8) | 75.2 (67.2, 81.7) | 460 | 5.9 |
| Hispanic | 69.7 (63.5, 75.3) | 70.7 (65.1, 76.3) | 72.1 (66.2, 77.1) | 73.5 (67.3, 79.3) | 75.1 (69.3, 80.8) | 1244 | 7.7 |
| No majority | 75.3 (70.2, 80.1) | 76.0 (71.2, 80.9) | 76.7 (72.0, 81.1) | 78.7 (73.4, 83.6) | 79.8 (74.7, 84.8) | 1993 | 6 |
| White | 76.5 (71.5, 81.0) | 77.3 (72.4, 81.8) | 78.0 (73.2, 82.5) | 80.0 (74.8, 84.7) | 81.1 (76.0, 85.7) | 5728 | 6 |
| Total | 75.3 (69.8, 80.2) | 76.2 (70.8, 80.9) | 76.8 (71.6, 81.5) | 78.7 (72.8, 83.7) | 80.0 (74.3, 84.8) | 9672 | 6.2 |
|
| |||||||
| High income: 4th quantile (≥90,803 in 2020) | |||||||
| F test (P) | 60.4 (<0.001) | 77.6 (<0.001) | 94.5 (<0.001) | 75.5 (<0.001) | 72.5 (<0.001) | ||
|
| |||||||
| AI or NH&PI | 77.4 (72.6, 83.3) | 74.9 (70.6, 80.4) | 75.8 (72.8, 79.0) | 72.6 (70.1, 75.7) | 73.2 (69.4, 81.4) | 8 | −5.4 |
| Asian | 85.3 (80.7, 90.0) | 85.7 (81.6, 89.9) | 85.8 (81.1, 89.4) | 86.7 (81.7, 90.7) | 87.3 (82.2, 91.1) | 598 | 2.3 |
| Black | 77.2 (70.4, 82.7) | 76.8 (69.0, 83.3) | 76.8 (68.7, 82.6) | 79.3 (73.8, 85.3) | 81.2 (74.7, 86.0) | 142 | 5.2 |
| Hispanic | 79.7 (73.8, 84.1) | 79.0 (74.5, 84.3) | 79.6 (75.1, 84.9) | 80.8 (74.8, 86.4) | 82.3 (76.8, 87.5) | 284 | 3.3 |
| No majority | 83.3 (78.7, 87.5) | 83.4 (79.1, 87.5) | 83.5 (79.4, 87.8) | 85.2 (80.3, 90.0) | 86.0 (81.3, 90.2) | 1517 | 3.2 |
| White | 84.9 (80.6, 88.6) | 85.4 (81.2, 89.0) | 85.8 (81.9, 89.3) | 86.9 (82.2, 90.6) | 87.6 (83.1, 91.2) | 7123 | 3.2 |
| Total | 84.5 (80.0, 88.4) | 84.9 (80.5, 88.7) | 85.3 (81.1, 89.0) | 86.5 (81.5, 90.4) | 87.2 (82.4, 90.9) | 9672 | 3.2 |
|
| |||||||
| CHDB total | 70.4 (56.9, 80.5) | 71.4 (58.0, 81.2) | 72.4 (59.5, 81.8) | 74.5 (62.4, 83.5) | 76.1 (64.7, 84.5) | 38,689 | 8.1 |
AI, American Indian; CHDB, City Health Dashboard; NH&PI, Native Hawaiian, and other Pacific Islander.
Fig. 1.
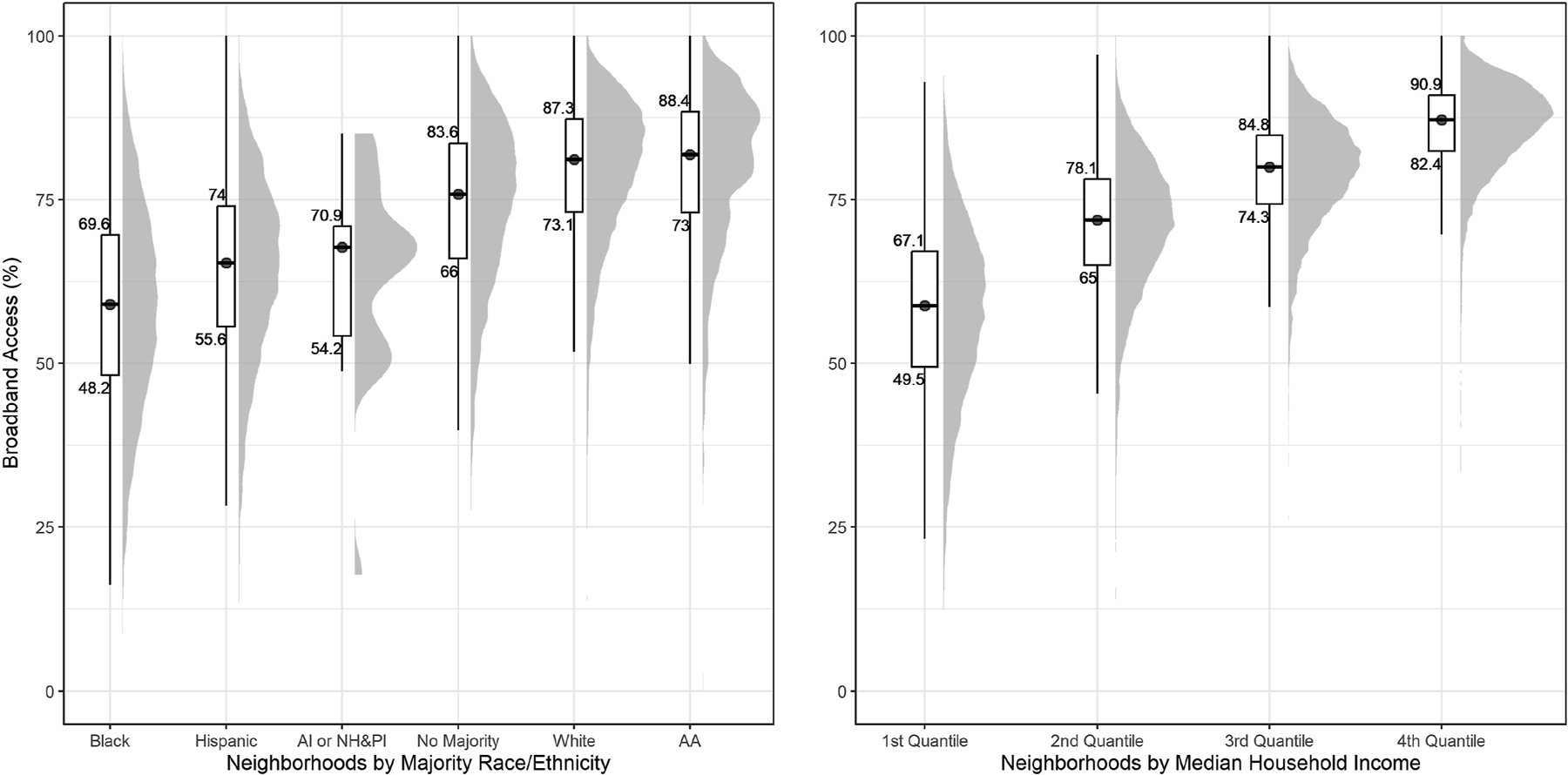
Distribution of broadband access by race/ethnicity and income, 2021.
Neighborhood income quartiles and majority race distributions were highly correlated. According to Table 1, only 3% (142) of the 4479 Black predominant neighborhoods were in high-income neighborhood quartiles, and 67% (2980) were in the lowest income quantile. In contrast to Black neighborhoods, 55% (598/1093) and 36% (7123/19597) predominantly AA and White neighborhoods were considered as high-income neighborhoods, respectively. After stratifying by income, neighborhoods with majority non-White residents consistently have lower broadband access than White majority neighborhoods, including AA majority neighborhoods. Among low-income neighborhoods, the median broadband connection rate for AI and NH&PI majority neighborhoods was 51.2% (interquartile range [IQR]: 49.1, 65.9), for Black majority neighborhoods was 53.2% (IQR: 44.1, 61.9), for Hispanic-majority neighborhoods was 56.3% (IQR: 47.7, 63.9), and for AA majority neighborhoods was 56.3% (IQR: 49.4, 68.4). These numbers were considerably lower than White majority neighborhoods (65.7%; IQR: 57.6, 72.4), and neighborhoods with no majority race/ethnicity (61.8%; IQR: 53.5, 69.2). Roughly similar racial/ethnic disparities were seen in high-income neighborhoods. Overall, 73.2% of households in AI and NH&PI majority neighborhoods, 81.2% in Black majority neighborhoods, and 82.3% in Hispanic-majority neighborhoods had broadband access, whereas 87.3% of households in AA, 87.2% of households in White majority neighborhoods, and 85.2% of the households in neighborhoods with no majority race/ethnicity group were connected to broadband internet. Differences by racial/ethnic groups are statistically significant in all income strata (Fig. 2 and Table 1). Statistical results for AI or NH&PI and AA majority should be interpreted with cautions due to small sample size (Table 1).
Fig. 2.
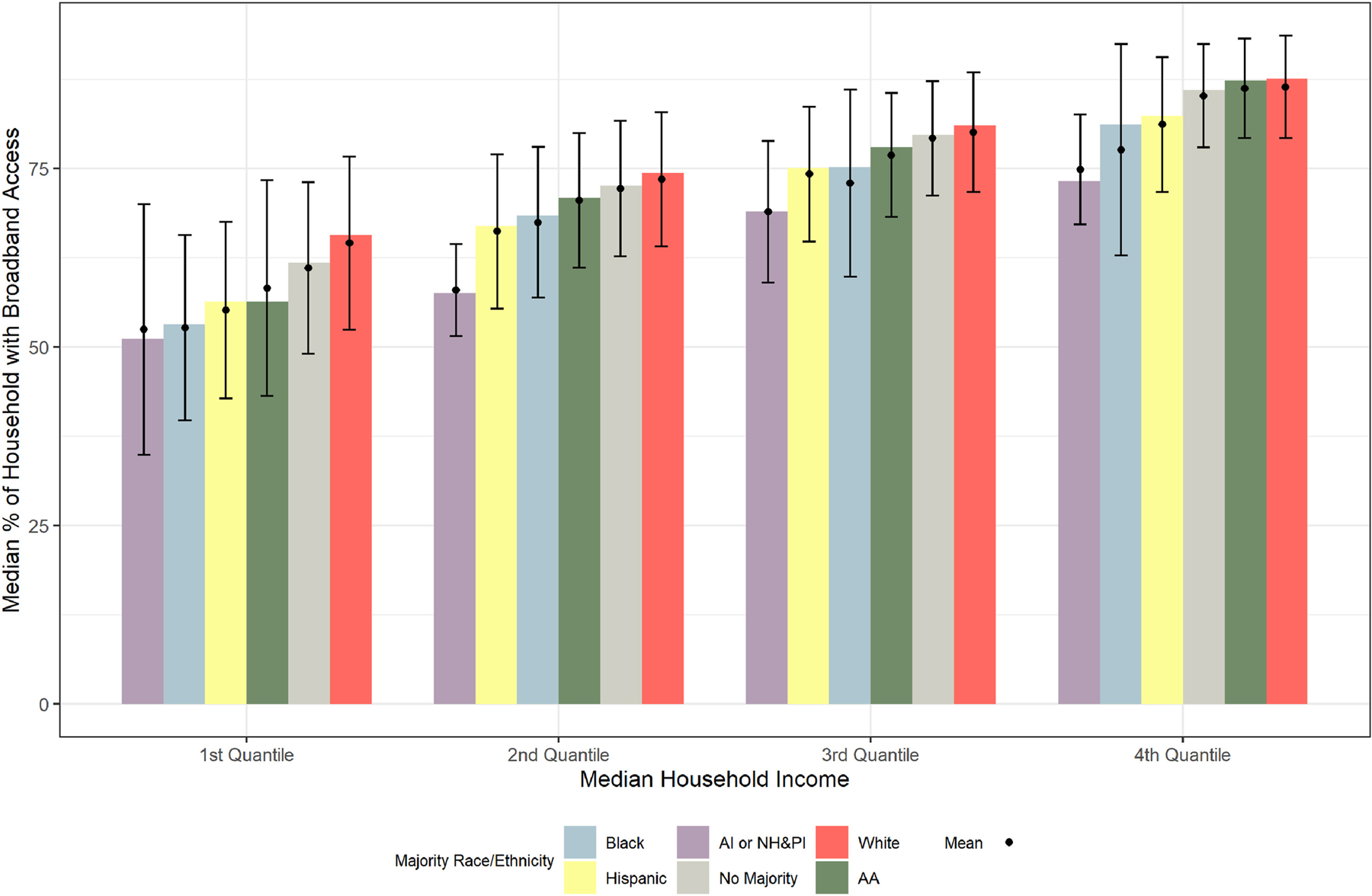
Broadband access rates by Census tracts, median income, and majority race/ethnicity, 2021.
Between 2017 and 2021, access to broadband increased modestly, and disparities in broadband access diminished. Overall, the median broadband connection rate increased from 70.4% to 76.1% across all neighborhoods (Table 1). Broadband access increased by 15.3% in low-income neighborhoods, a faster rate than the 2.4% increase rate in high-income neighborhoods. In each income stratum, increases in broadband access were larger in Black- and Hispanic-majority neighborhoods (2–7%) than in neighborhoods with other race/ethnic compositions. Broadband access in AA majority neighborhoods fluctuated (−2.5% to 1.6%) year by year over the 5-year period (Fig. 3).
Fig. 3.
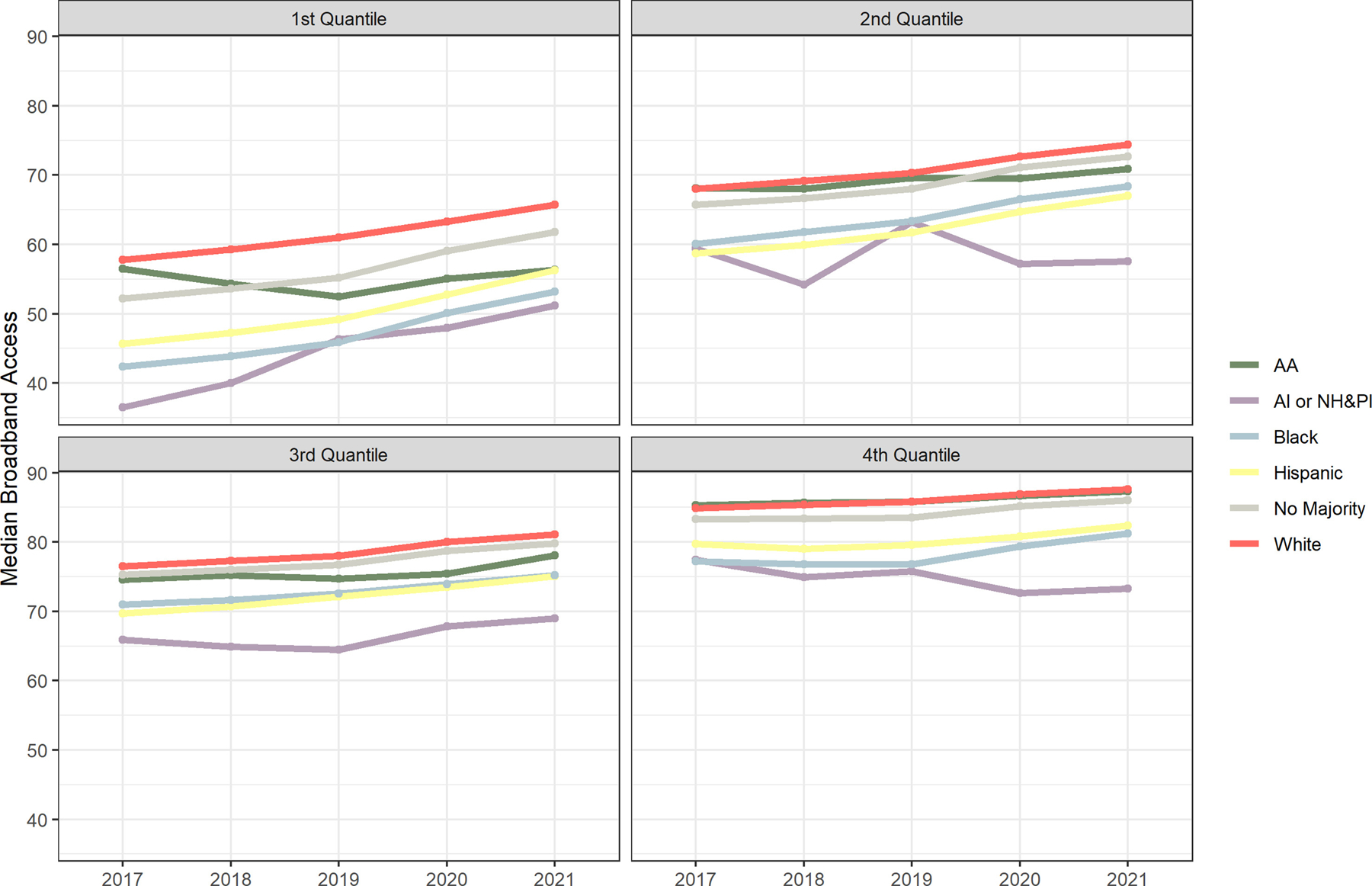
Broadband access by majority race/ethnicity, stratified by income, 2017–2021.
Fig. 4 shows the geographical distribution of broadband access across the 905 Dashboard cities. Generally speaking, cities in the West had higher broadband access than cities in the northeast and south. Cities in the Great Lakes region and along the southern border had the lowest broadband access among the 905 included cities.
Fig. 4.
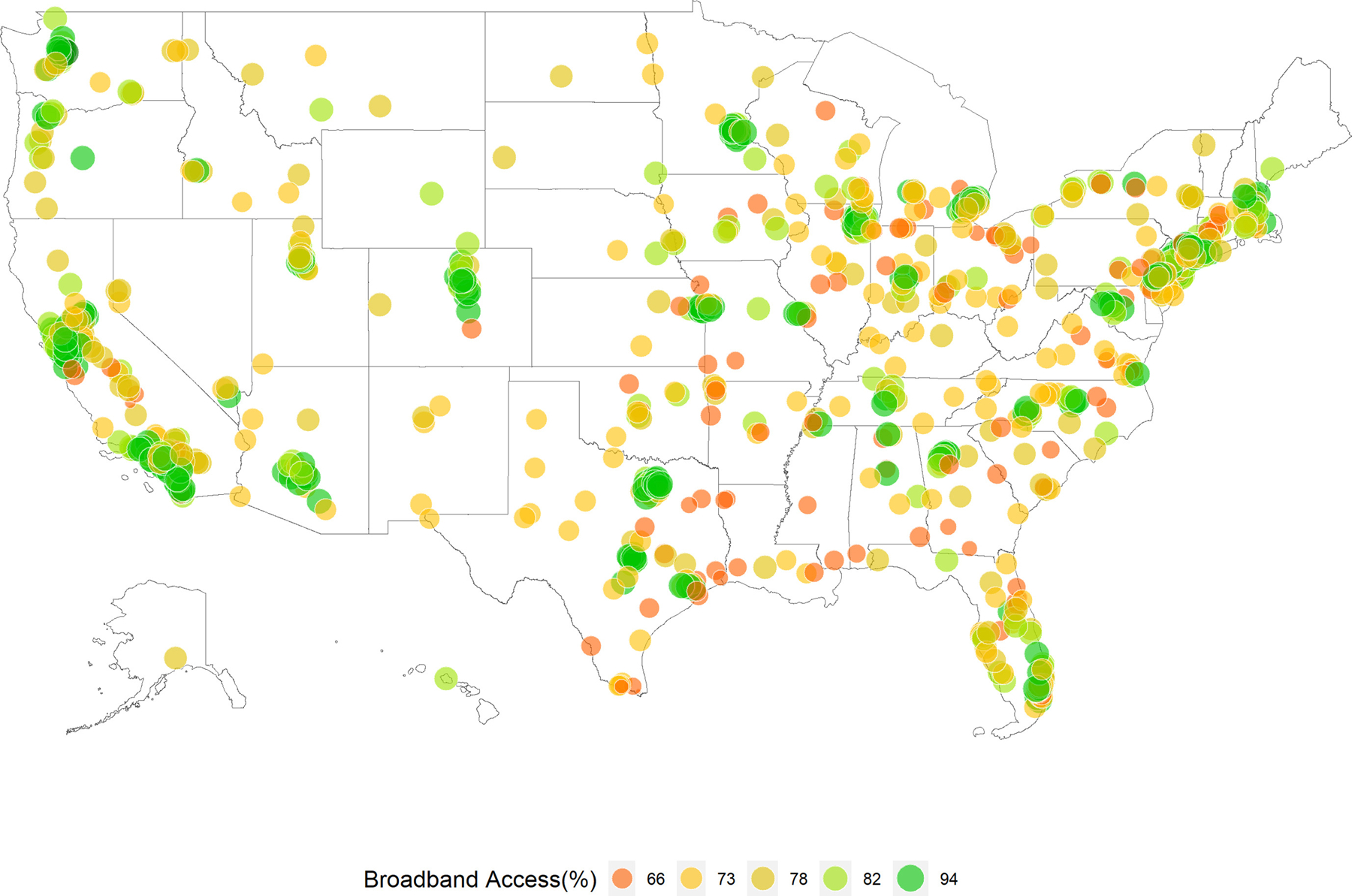
Broadband access rates by city, 2021.
Discussion
Four key findings emerged from our analysis of broadband access in US cities. First, in 2021, about a quarter of households in the 905 largest US cities did not have broadband access at home. Second, households in low-income neighborhoods were less likely to have broadband access compared with households in high-income neighborhoods. Third, predominantly minority neighborhoods had lower broadband access compared to White and no majority neighborhoods, regardless of income level. Our findings confirm patterns previously published by the PEW Research Center and others using smaller surveys or a more limited geographic focus.5,9,21 Fourth, although broadband access increased only modestly between 2017 and 2021, we documented that improvements were larger in low-income and minority-predominant neighborhoods and had the effect of modestly reducing racial/ethnic and income broadband access disparities. To the best of our knowledge, this is the first article to comprehensively examine broadband access of city neighborhoods at national level.
Despite progress made over the 4-year period, our results indicate that substantial broadband access disparities persist in urban settings. Across the 905 cities analyzed, more households from low-income neighborhoods lacked access to high-speed internet than did households from high-income neighborhoods. Previous research generally ascribes lack of broadband access to an absence of broadband infrastructure, unwillingness on the part of broadband providers to invest in such infrastructure, and the cost of broadband service.5,9 However, our data showed that at least 30% of households in low-income neighborhoods had broadband access (see the lower quartile in Fig. 1), suggesting that most of these urban neighborhoods were equipped with broadband infrastructure. Therefore, other factors, such as affordability and digital literacy, may have been the cause of low broadband adoption in these neighborhoods. Reducing the cost of broadband access, potentially through providing direct subsidies for broadband subscriptions and computer devices, could reduce disparities in broadband access.
Because of population hypersegregation by race/ethnicity, the average income of Black neighborhoods only marginally overlaps with White majority neighborhoods across our sample of 905 cities.22 However, our findings suggest that income alone cannot explain comparatively lower broadband connection rates in Black, Hispanic, and AI or NH&PI majority neighborhoods across income strata. For example, if 70% of households in a neighborhood were connected to broadband internet, that neighborhood would be more connected than three-quarters of Black- and Hispanic-majority neighborhoods in American cities, but it would be less connected than three-quarters of AA and White majority neighborhoods. This suggests significant broadband disparities by household race/ethnicity. Even among neighborhoods with high median household income, broadband access in White majority neighborhoods was 12% higher than in Black majority neighborhoods and 7.5% higher than in Hispanic-majority neighborhoods. One explanation is differences in disposable income. Even within the same income quartile, Black and Hispanic households tend to have less family wealth (e.g. savings and home ownership) than White or Asian households, which may make Black and Hispanic households more sensitive to the cost of broadband subscription.23 In addition, in many cities, geographic broadband disparities also likely reflect a broader history of structural racism caused by disinvestment and discriminatory development and zoning practices.24 For example, other studies have demonstrated that neighborhoods redlined more than a half-century ago have lower broadband access today.25
In contrast to Black neighborhoods, AA neighborhoods had the highest median broadband access rate. However, we also noticed that median broadband access in AA neighborhoods was considerably lower than White majority neighborhoods in low-income strata. The high-income AA neighborhoods drove up median broadband access rates for all AA neighborhoods and masking lower access specifically in the low-income stratum. This phenomenon further emphasizes the need for stratification in conducting social health research, especially among racial/ethnic groups that encompass a wide range of ethnic subgroups, such as AA and Hispanic populations.24
In response to the lessons learned from the COVID-19 pandemic, the Federal Communications Commission has launched an Advancing Broadband Connectivity as a Social Determinant of Health Initiative.26 The task force leading the initiative acknowledges that the myriad ways in which internet adoption may influence health are not well characterized, yet correlations between broadband access and improved health outcomes are strong. The use of health-related digital tools to access health care or to seek health-related information is the best-studied route, and socioeconomic disparities in such uptake are well documented. A recent study using data from Health Information National Trends Survey found that utilization of digital health in response to COVID pandemic only increased in high-income groups.27 A similar study also found that older people and people with low education attainment were less likely to use the internet to find healthcare provider or look for health-related information.28 Monitoring the impacts of policy efforts to expand broadband in the post-COVID era and evaluating the subsequent impacts on health and health equity outcomes will be important steps.
There are several limitations of our study. First, ACS data are imperfect. Places with low population density may see large error margins because of sparse data (although most cities in this analysis are densely populated), and there is 2-year lag in data reporting. Methodologically, this may minimize the impact of the data lag.9 Also, the ACS survey instrument does not collect information on the actual speed of respondents’ internet connections, instead asking respondents if they have “high-speed” fixed-line internet and excluded cellular plan from the “high-speed” internet entirely. ACS also does not indicate the physical availability of broadband infrastructure. Therefore, our data cannot identify whether the lack of adoption is due to the absence of infrastructure or the cost of subscription. Second, our broadband access was measured at household level, but our racial/ethnic majority neighborhoods were measured at population level. Household broadband access rate might be higher than population broadband access rate depending on the household size in certain neighborhoods. Certain individual-level attributes, such as age, health status, and education level, cannot be analyzed because a household typically includes multiple people with various level of individual factors. Finally, due to the population distribution and residential segregation, the number of neighborhoods by different race/ethnicity group in each income stratum is unevenly distributed, especially for AI or NH&PI. Estimates from these groups should be interpreted with cautions.
Conclusion
Broadband access is an emerging social determinant of health with impacts across the life course, affecting access to information, education, health care, and other important health determinants.29 The COVID-19 pandemic has substantially increased public understanding of the importance of broadband access. City policymakers should take advantage of recent infrastructure funding targeted at broadband access to eliminate disparities. By providing city-level maps of household broadband access for 905 large US cities, resources such as the City Health Dashboard can be used by city policymakers to target investments and interventions to close the gap in broadband access.
Supplementary Material
Funding
This work is funded by Robert Wood Johnson Foundation Grant number 78440. The authors declare no competing interests. This work uses publicly available data and does not need any ethical approvals or informed consent.
Footnotes
Ethical approval
This work uses publicly available data and does not need any ethical approval or informed consent.
Competing interests
The authors declare no competing interests.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.puhe.2023.02.001.
Data availability
Data are available on https://www.cityhealthdashboard.com/. All experiments were performed in accordance with relevant guidelines and regulations.
References
- 1.Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband internet access is a social determinant of health. Am J Publ Health 2020;110:1123–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Graves JM, Abshire DA, Amiri S, Mackelprang JL. Disparities in technology and broadband internet access across rurality: implications for health and education. Fam Community Health 2021;44:257–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ortega G, Rodriguez JA, Maurer LR, Witt EE, Perez N, Reich A, et al. Telemedicine, COVID-19, and disparities: policy implications. Health Policy Technol 2020;9:368–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Webb Hooper M, Napoles AM, Perez-Stable EJ. COVID-19 and racial/ethnic disparities. JAMA 2020;323:2466–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Perrin A Mobile technology and home broadband 2021. Pew Research Center 2021. [Google Scholar]
- 6.LaRose R, Gregg JL, Strover S, Straubhaar J, Carpenter S. Closing the rural broadband gap: promoting adoption of the Internet in rural America. Telecommun Pol 2007;31:359–73. [Google Scholar]
- 7.Martin M Computer and internet use in the United States 2018. United States Census Bureau; 2021 4/1/2022 Contract No.: ACS-49. [Google Scholar]
- 8.Federal Communications Commission. Broadband progress Report 2016. 2016. [Google Scholar]
- 9.Reddick CG, Enriquez R, Harris RJ, Sharma B. Determinants of broadband access and affordability: an analysis of a community survey on the digital divide. Cities 2020;106:102904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Levitas R Delivering social inclusion The inclusive society? Social exclusion and new labour London: Palgrave Macmillan UK.; 1998. p. 159–77. [Google Scholar]
- 11.Early J, Hernandez A. Digital disenfranchisement and COVID-19: broadband internet access as a social determinant of health. Health Promot Pract 2021;22: 605–10. [DOI] [PubMed] [Google Scholar]
- 12.White House The. Fact sheet: the bipartisan infrastructure deal The White House; 2021. [Google Scholar]
- 13.Trollop A Understanding the urban digital divide: bipartisan policy center 2021. [Google Scholar]
- 14.Prieger JE, Hu W-M. The broadband digital divide and the nexus of race, competition, and quality. Inf Econ Pol 2008;20:150–67. [Google Scholar]
- 15.Massey DS, Rothwell J, Domina T. The changing bases of segregation in the United States. Ann Am Acad Polit Soc Sci 2009;626:74–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.U.S. Census Bureau. Defining “rural” areas understanding and using American community survey data: what rural areas need to know Washington, DC: U.S. Government Printing Office; 2019. p. 2–7. [Google Scholar]
- 17.Dashboard CH. City health dashboard 2021. [cited 2021 4/1/2022]; Available from: https://www.cityhealthdashboard.com/. [Google Scholar]
- 18.Dashboard CH. City health dashboard technical document 2021. [updated 3/29/2022; cited 2021 4/1/2022]; Available from: https://www.cityhealthdashboard.com/technical-documentation. [Google Scholar]
- 19.Verizon. 4G LTE speeds vs. Your home network 2020. Available from: https://www.verizon.com/articles/4g-lte-speeds-vs-your-home-network/#:~:text¼Verizon%204G%20LTE%20wireless%20broadband,to%2012%20Mbps%20are%20common. [Google Scholar]
- 20.Reisdorf BC, Fernandez L, Hampton KN, Shin I, Dutton W. Mobile phones will not eliminate digital and social divides: how variation in internet activities mediates the relationship between type of internet access and local social capital in detroit. Soc Sci Comput Rev 2020:089443932090944. [Google Scholar]
- 21.Perrin AA, Sara. Home broadband adoption, computer ownership vary by race, ethnicity in the U.S. Pew Research Center; 2021. [Google Scholar]
- 22.Massey DS, Tannen J. A research note on Trends in Black hypersegregation. Demography 2015;52:1025–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bhutta NC, Andrew C, Dettling Lisa J, Hsu Joanne W. Disparities in wealth by race and ethnicity in the 2019 survey of consumer finances: board of governors of the federal reserve system (U.S) 2020. Contract No.: FEDS Notes 2020-09-28. [Google Scholar]
- 24.Spoer BR, Juul F, Hsieh PY, Thorpe LE, Gourevitch MN, Yi S. Neighborhood-level asian American populations, social determinants of health, and health outcomes in 500 US cities. Ethn Dis 2021;31:433–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.County Health Rankings & Roadmaps. A digital disadvantage: low broadband rates in urban, segregated pockets compound inequities 2022.. [Accessed 4 January 2022]. [Google Scholar]
- 26.Federal Communications Commission. Studies and data analytics on broadband and health 2022. [Google Scholar]
- 27.Zeng B, Rivadeneira NA, Wen A, Sarkar U, Khoong EC. The impact of the COVID-19 pandemic on internet use and the use of digital health tools: secondary analysis of the 2020 health information national Trends survey. J Med Internet Res 2022;24:e35828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Calixte R, Rivera A, Oridota O, Beauchamp W, Camacho-Rivera M. Social and demographic patterns of health-related internet use among adults in the United States: a secondary data analysis of the health information national Trends survey. Int J Environ Res Publ Health 2020;17:6856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Understanding the broadband access gap. PD&R Edge; [cited 2021]; Available from: https://www.huduser.gov/portal/pdredge/pdr_edge_featd_article_100614.html. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are available on https://www.cityhealthdashboard.com/. All experiments were performed in accordance with relevant guidelines and regulations.