

Abstract
The current work tested whether perceivers believe that women, relative to men, are likely to exaggerate versus downplay pain, an effect we refer to as the gender-pain exaggeration bias. The gender-pain exaggeration bias was operationalized as the extent to which perceivers believe women, relative to men, claim more pain than they feel. Across four experiments, we found that women were expected to exaggerate pain more than men and men were expected to downplay pain more than women (Studies 1–4). Further, judgments that women were more emotionally dramatizing than men contributed to this gender-pain exaggeration bias (Studies 2 and 4). We also assessed whether perceiver-level differences in endorsement of gendered emotional dramatization stereotypes (Studies 3–4) moderated this gender-pain exaggeration bias and found that endorsement of gendered emotional dramatization stereotypes moderated this bias. In sum, we document a relative gender-pain exaggeration bias wherein perceivers believe women, relative to men, to be emotionally dramatizing and therefore more likely to exaggerate versus downplay their pain. This bias may lead perceivers to interpret women’s, relative to men’s, pain reports as overstatements, inauthentic, or dramatized. Thus, the current work may have implications for well-documented biases in perceptions of (i.e., underestimating) and responses to (i.e., undertreating) women’s pain.
Keywords: person perception, impression formation, gender, pain, emotion
Pain is a prevalent concern for American women, with more than one in five women currently living with chronic pain (Zelaya et al., 2020). Women also report more post-operative and experimentally induced pain than men (see Fillingim et al., 2009 for review), yet women’s pain is often underestimated (e.g., Pronina & Rule, 2014) and garners less intensive and effective pain treatment than men’s pain (e.g., Chen et al., 2008). Such gender biases in pain perception and treatment have led scholars to theorize that women relative to men are expected to exaggerate pain and their reported pain is therefore minimized or disbelieved (Lloyd et al., 2020; Samulowitz et al., 2018). Specifically, Lloyd and colleagues (2020) argued that women’s pain may be underestimated and undertreated because women reporting pain are viewed as exaggerating, dramatizing, or even lying. They also argued that gendered expectations of pain exaggeration may be informed by gender-emotionality stereotypes that depict women expressing their feelings as dramatic and irrational. In line with this theorizing, qualitative work suggests that women in pain are prone to dismissal and minimization of their pain by physicians (e.g., McManimen et al., 2019). Additionally, Samulowitz and colleagues’ (2018) review of gender and pain outcomes concluded that perceivers often view women’s expressions of pain as indicative of women being emotional and hysterical.
The current work experimentally tests whether lay perceivers exhibit a gender-pain exaggeration bias, wherein women are judged as exaggerating more and downplaying less than men. In line with Boring and colleagues’ (2022) working definitions of pain over-reporting (i.e., exaggeration) and under-reporting (i.e., downplaying), we define pain exaggeration as claiming more pain than one feels, and we define downplaying as the inverse: claiming less pain than one feels. Research has assessed gendered expectations of pain felt (e.g., Summers, Weesner, et al., 2023) but not of pain claimed. The current work assesses expectations of how much pain women and men would feel and claim in painful situations to shed light on gendered pain exaggeration expectations. Of key interest is the relative difference between men and women with respect to exaggeration/downplaying; we theorize perceivers will expect women to exaggerate pain more and downplay pain less than men. We then test if gender-emotionality stereotypes contribute to this gender-pain exaggeration bias and consider perceiver beliefs that may moderate this bias.
An Important Note on Gender and Sex Terminology
The current work employs gender (e.g., woman and man) rather than sex (e.g., female and male) terminology, because we are focused on perceptions of individuals based on gender expression rather than biological differences between individuals. Research on pain often uses gender and sex terminology interchangeably; thus, when discussing previous work, we use language that most resembles language used in that past work. When discussing the current work, we refer to gender expression. The current work focuses on women and men, which does not cover the spectrum of gender but rather reflects existing evidence that women are disadvantaged relative to men when disclosing or seeking care for pain. However, those who are likely most disadvantaged (e.g., gender diverse individuals and those with multiple minoritized identities) are not well represented in health or psychological sciences and are similarly not represented in the current work. We discuss this limitation further in the General Discussion.
Expectations of Others’ Pain Experiences
Expectations about how others experience pain, including sensitivity (i.e., how much pain one will feel) are biased by social group memberships. Research has examined how expectations of others’ pain sensitivity vary by gender (Summers et al., 2021; Summers, Pitts, & Lloyd, 2023; Summers, Weesner, et al., 2023; Wandner et al., 2012), race (Hoffman et al., 2016; Hoffman & Trawalter, 2016; Summers et al., 2021; Summers, Pitts, & Lloyd 2023; Summers, Weesner, et al., 2023; Trawalter et al., 2012; Waytz et al., 2015; Wandner et al., 2012), age (Summers et al., 2022; Summers, Pitts, & Lloyd, 2023; Wandner et al., 2012), and socioeconomic status (Summers et al., 2021; Summers et al., 2022). Women (relative to men), White (relative to Black) individuals, younger (relative to older) individuals, and higher (relative to lower) socioeconomic status individuals are expected to feel more pain. Further, biased pain sensitivity expectations yield biased treatment recommendations. Specifically, Black (relative to White) and low (relative to high) socioeconomic status individuals are expected feel less pain and therefore to require less treatment (Hoffman et al., 2016; Summers et al., 2021; Summers et al., 2022; Summers, Pitts, & Lloyd, 2023), a pattern consistent with disparities wherein Black and low socioeconomic status individuals receive relatively less intensive pain treatment (e.g., Drwecki et al., 2011; Green et al., 2003; Joynt et al., 2013).
Based on findings linking expectations of pain sensitivity and recommended treatment, as well as findings that women are expected to feel more pain, it stands to reason that women would be given more pain care than men. Yet, experimental studies (Hirsh et al., 2013; Hirsh et al., 2015) and national health statistics (Schulman et al., 1999; Chen et al., 2008; Lord et al., 2009) report that women receive less intensive and effective pain care than men. Thus, pain sensitivity expectations cannot explain biases in pain treatment across gender. Instead, we argue that gender biases in pain may be better captured through expectations of pain felt and claimed in tandem. This approach allows researchers to assess whether perceivers expect women relative to men to (a) exaggerate pain (claim > feel) or (b) downplay pain (claim < feel). We theorize the existence of a gender-pain exaggeration bias whereby women are expected to exaggerate pain more and downplay pain less than men.
Though work has yet to disentangle expectations of pain felt and pain claimed, there is ample reason to believe that exaggeration expectations may influence responses to pain. Indeed, physicians often cite concerns about fabricated or exaggerated pain claims when determining an appropriate course of pain treatment (e.g., Aronowitz et al., 2021), and patients, especially women, often report being disbelieved by physicians (e.g., McManimen et al., 2019). Further, Schäfer and colleagues (2016) tested whether perceptions of pain exaggeration from expressions of pain (i.e., judgments of whether expressions of pain map are amplified) are gendered. Here, medical students and clinicians saw videos of female and male patients with shoulder pain and rated the likelihood that each patient was exaggerating, minimizing, and hiding their pain, estimated how much pain each patient was experiencing, and recommended pain treatment. Female patients were judged as experiencing less pain than male patients, consistent with past evidence that women’s pain is underestimated (e.g., Pronina & Rule, 2014; Zhang et al., 2022). Female patients were also recommended less treatment than male patients, and this was unrelated to how much pain patients were judged as experiencing. Of particular interest, female (vs. male) patients’ expressions were judged as more exaggerated and less minimized/hidden. The current work expands this work by testing whether perceivers expect women to exaggerate pain more than men. Previous work found that pain expectations can inform pain treatment biases (e.g., Hoffman et al., 2016). There is also a wealth of evidence that expectations influence downstream judgments (Chalk et al., 2010; de Lange et al., 2018; Kok et al., 2013). Thus, testing whether perceivers’ expectations of the alignment between the amount of pain someone will feel and the amount they will claim are different for women and men is important.
Thus far, we have theorized about a gender-pain exaggeration bias whereby perceivers will expect women to exaggerate pain more and downplay pain less relative to men. Such a bias could manifest in several specific patterns. Perceivers may expect people to exaggerate pain, and to a greater extent for women than men. Conversely, perceivers may expect people to downplay pain, but to a lesser extent for women than men. Finally, perceivers may expect women to exaggerate and men to downplay. Each of these patterns would manifest in target gender (i.e., woman or man) and type of pain expectations (i.e., feel or claim) interactively shaping how much pain a target is attributed. All patterns are consistent with our theorized gender-pain exaggeration bias and may carry implications for biased perceptions of pain expressions and pain care disparities. That is, even if women and men are both expected to downplay, but women to a lesser extent, this may still have negative consequences for women seeking pain care.
Stereotypes Underlie Biases in Pain Expectations and Perceptions
Rich psychological and medical literatures highlight the role that stereotypes can play in shaping pain experiences, expressions, expectations about others’ pain, and perceptions of others’ pain expressions. Of relevance to pain expectations, research on pain sensitivity expectations across race and socioeconomic status found that stereotypes contributed to pain expectation biases. For example, perceivers believed Black and lower socioeconomic status individuals had lived harder lives, and these beliefs contributed to expectations that Black and lower socioeconomic status individuals feel less pain (Hoffman & Trawalter, 2016; Summers et al., 2021; Summers, Pitts, & Lloyd, 2023). The effects of assumed hardship on pain sensitivity expectations are explained as a physical toughening: individuals who are perceived or depicted as having lived hard lives are believed to be physically tougher and relatively inured to pain. Thus, beliefs about an individual’s internal experiences can inform beliefs about their sensitivity to pain. The current work centers distinct yet related beliefs about how external expressions might relate to internal experience (i.e., how someone would depict their internal experience) by leveraging an established literature on gender-emotionality stereotypes.
Gender Stereotypes of Emotionality
In line with Lloyd and colleagues’ (2020) proposition that researchers studying gender biases in pain should test the explanatory value of established gender-emotionality stereotypes, the current work centers gender-emotionality stereotypes. In western cultures, women are stereotyped as more emotional and less in control of their emotions than men (McCormick et al., 2016; Shields, 2013). Gender stereotypes about emotionality often pit expression against internal experience. For example, women are stereotyped as irrational (i.e., their expressions are viewed as illogical for the specific emotion-evoking experience; Brescoll, 2016) and as dramatizing negative emotions (i.e., their expressions are viewed as overstatements; e.g., Hess et al., 2000). Thus, we believe gender-emotionality stereotypes may map onto the contrast between expected amount of pain felt and claimed such that perceivers will expect women to exaggerate pain more than men insofar as they believe women are more emotionally dramatizing than men.
In the current work, we focus on negative feminine stereotypes about dramatizing emotions. Based on the negative feminine personality subscale of Diekman and Eagly’s (2000) Gender-Stereotypic Dimensions scale, we assess the extent to which perceivers believe women and men are whiny, nagging, complaining, and fussy. Hereafter, we refer to these stereotypes as gendered emotional dramatization stereotypes. Providing support for the role of gendered emotional dramatization stereotypes in pain, Samulowitz and colleagues’ (2018) review of experiences, perceptions, and treatment of pain across gender found that women’s claims of pain were perceived as hysterical, emotional, and complaining, whereas men’s claims of pain were perceived as stoic, controlled, and autonomous. The current work directly tests whether expectations that women, relative to men, exaggerate versus downplay pain are informed by differential endorsement and application of emotionality stereotypes to women more than men.
Overview of the Current Work
We present four experiments assessing gendered pain exaggeration expectations. Across studies we assess how much pain perceivers expect women and men to feel and claim in painful situations. Of critical interest is the theorized gender-pain exaggeration bias, whereby perceivers expect women to claim more pain than they feel compared to men. Thus, the effect of critical interest is the interaction between target gender (i.e., man or woman) and type of pain expectation (i.e., feel or claim). Study 1 was an initial test of whether perceivers expect women to exaggerate pain relative to men. Study 2 tested whether application of gendered emotional dramatization stereotypes more to women than men contributed to the gender-pain exaggeration bias. Studies 3–4 tested perceivers’ stereotype endorsement as a moderator of this bias. All studies recruited lay perceivers; limitations and implications of our sample are discussed in the General Discussion. All manipulations, measures, and exclusions are disclosed. Measures not central to the manuscript are not discussed at length, but description and analysis of these measures are in the Supplemental Materials. Sample size was determined before conducting analyses, and all data was collected for a study before conducting analyses. Data and materials are openly accessible (https://osf.io/fwcmj/?view_only=778bacbd7bdb4f6e92d0d36cdcc7d370).
Study 1
Perceivers viewed images of women and men and reported how much pain they expected each individual would feel, then claim, for common injuries. Our primary hypothesis was that target gender (woman/man) and type of expectation (feel/claim) would interact such that women would be expected to exaggerate pain more than men. This interaction could manifest in several specific patterns, all of which may have important implications. Thus, we remained agnostic regarding the specific pattern of simple effects. Based on other work (e.g., Summers, Weesner et al., 2023), we also expected an effect of target gender such that more pain (feel and claim) would be attributed to women than men. Though work has not disentangled expectations of pain feel and claim, Boring and colleagues (2022) found that perceivers expected others to overstate their pain. Thus, we may expect perceivers to evaluate people as claiming more pain than they feel.
Method
Participants
American participants (N=64) were recruited via CloudResearch (Litman et al., 2017). Power analysis via simr (Green & MacLeod, 2016) indicated that our main analytic model could detect a small effect (β1 = 0.10) with adequate power (95% CI [95.68%, 99.69%]). Participants were primarily men (56.3% men, 43.8% women),2 primarily White (71.9% White, 21.9% Black, 6.3% Asian), primarily non-Hispanic (89.1% non-Hispanic, 10.9% Hispanic), and ranged in age from 22 to 67 (M = 38.08, SD = 10.65).3 No participants were excluded.
Procedure
Each participant viewed 10 neutrally expressed images (5 women, 5 men)4 from the Chicago Face Database (Ma et al., 2015). We used the 10 White targets closest to the mean attractiveness for each gender. We divided images into two sets and randomized which set each participant saw (see Supplementals). Participants indicated how much pain they expected each target would feel, then claim, for a sprain/strain, back problems, abdominal problems, a superficial injury/contusion, and a headache/migraine on scales ranging from 1 (“Not painful”) to 4 (“Extremely painful”). These injuries were the top five principal conditions for emergency department visits resulting in discharge for Americans aged 18–44 and were similarly common among women and men (Weiss et al., 2014). Responses to all injuries were averaged to create composite feel and claim scores (higher values indicate more expected pain). Participants then completed a measure of Motivation to Respond Without Sexism (Klonis et al., 2005), which did not consistently moderate effects (see Supplementals). Participants then reported demographics. Scale descriptive statistics and correlations between measures are in Table 1.
Table 1.
Means, standard deviations, reliabilities, and correlations
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|---|
| 1. Expected pain felt by women | 2.71 | 0.39 | (.74) | |||||
| 2. Expected pain claimed by women | 2.76 | 0.41 | .76*** | (.81) | ||||
| 3. Expected pain felt by men | 2.52 | 0.42 | .65*** | .36** | (.79) | |||
| 4. Expected pain claimed by men | 2.26 | 0.56 | .51*** | .32* | .77*** | (.91) | ||
| 5. Internal motivation to respond without sexism | 7.12 | 1.86 | −.02 | −.20 | .03 | .01 | (.92) | |
| 6. External motivation to respond without sexism | 4.51 | 2.16 | .17 | .16 | .27* | .30* | −.19 | (.88) |
Note. M and SD are used to represent mean and standard deviation, respectively. Reliabilities (α) are displayed on the diagonal. For correlations,
indicates p < .05.
indicates p < .01, and
indicates p < .001.
Results
Expectations of Pain Felt and Claimed by Target Gender
To test our hypothesis that target gender and type of pain expectation would interact, we conducted a linear mixed effects regression via lme4 (Bates et al., 2014) regressing amount of expected pain on fixed effects of target gender (woman = −0.5, man = 0.5), type of expectation (feel = −0.5, claim = 0.5), and their interaction with random effects of the intercept and slope of all effects by participant to account for repeated-measures. A likelihood-ratio test indicated that this model fit the data better than a model without fixed effects, χ2(3) = 71.07, p < .001. As expected, the effect of target gender was significant, b = −0.34, β = −0.28, F(1, 63) = 42.16, p < .001, with perceivers attributing women (M = 2.73, SE = 0.05) more pain than men (M = 2.39, SE = 0.06). The effect of type of pain expectation was significant, b = −0.10, β = −0.08, F(1, 63) = 12.25, p = .001, but counter to the predicted direction: perceivers expected targets to claim (M = 2.51, SE = 0.05) less pain than they feel (M = 2.61, SE = 0.05). Of primary interest, the interaction between target gender and type of expectation was significant, b = −0.32, β = −0.13, F(1, 63) = 32.92, p < .001 (Figure 1 – Study 1). Perceivers non-significantly expected women to claim (M = 2.76, SE = 0.06) more than they feel (M = 2.71, SE = 0.06), b = 0.06, β = 0.05, F(1, 63) = 2.76, p = .102, but expected men to claim (M = 2.26, SE = 0.06) significantly less pain than they feel (M = 2.52, SE = 0.06), b = −0.26, β = −0.21, F(1, 63) = 33.38, p < .001.
Figure 1.
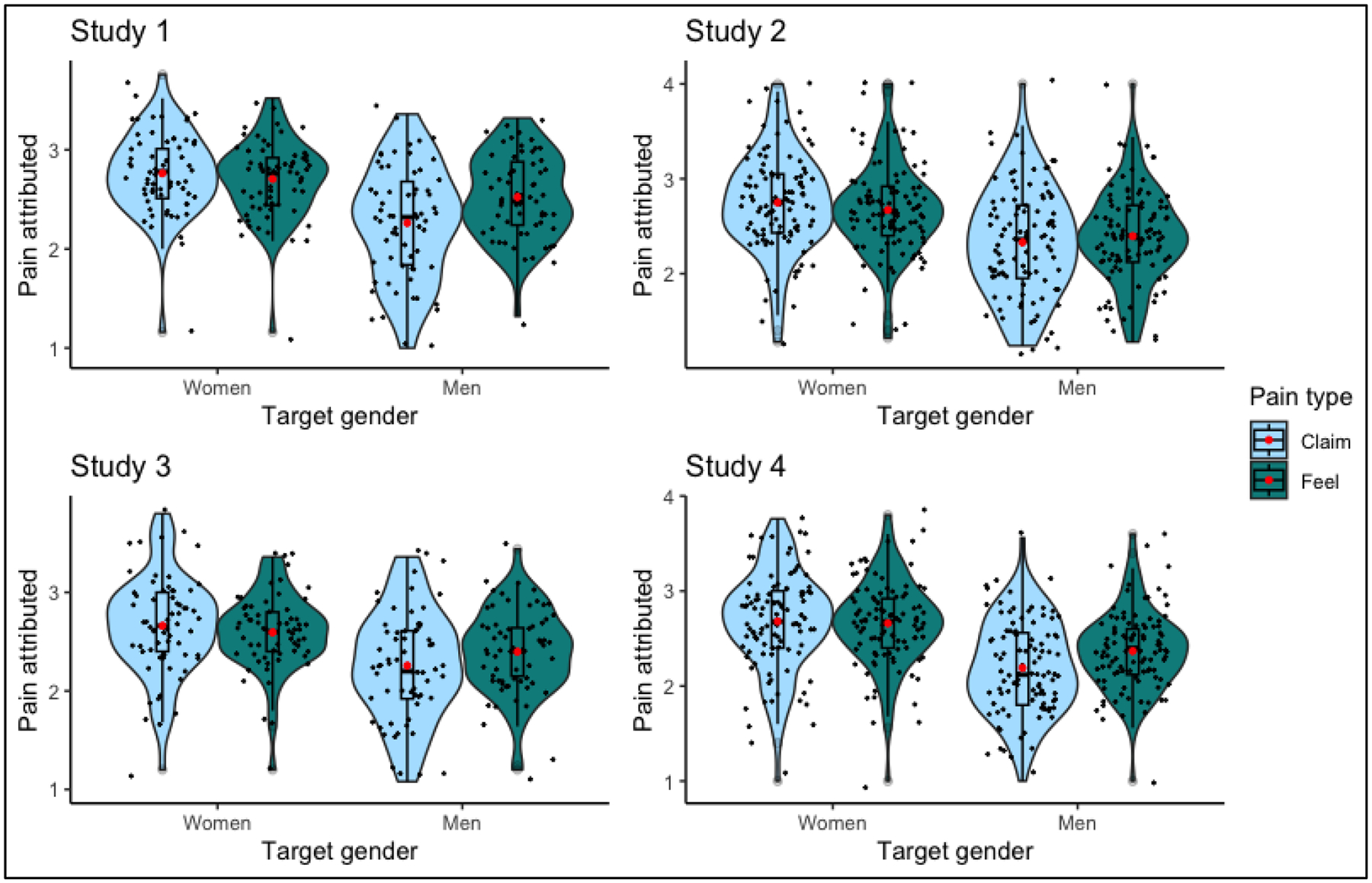
Violin plots depicting expected pain felt and claimed by target gender (higher values = more pain). Red dots are mean, black dots are jittered individual data points.
Discussion
We found initial evidence for the theorized gender-pain exaggeration bias: perceivers expected men to claim less pain than they felt and women to claim more pain than they felt, although only the former simple effect was statistically significant.
Study 2
We tested whether women are expected to exaggerate their pain more than men insofar as they are characterized as more emotionally dramatizing. We expected to replicate Study 1, with an effect of gender (women attributed more pain) and an interactive effect of gender and type of expectation (women expected to exaggerate pain more). Given that the main effect of type of expectation in Study 1 did not align with predictions, we do not offer hypotheses for this effect. We also expected that women would be attributed more emotional dramatization traits than men. Our primary hypothesis was that women would be expected to exaggerate pain more insofar as they are stereotyped as more emotionally dramatizing than men.
Method
Participants
American participants (N=100) were recruited via CloudResearch (Litman et al., 2017). Power analysis via simr (Green & MacLeod, 2016) indicated that our main analytic model could detect a small effect (β = 0.10) with adequate power (95% CI [98.17%, 100.00%]). Participants were primarily men (64.0% men, 36.0% women), primarily White (79.0% White, 10.0% Asian, 7.0% Black, 2.0% American Indian/Alaska Native, 1.0% Native Hawaiian/Pacific Islander, 1.0% self-identified), primarily non-Hispanic (91.0% non-Hispanic, 9.0% Hispanic), and ranged in age from 22 to 70 (M = 38.03, SD = 11.99). No participants were excluded.
Procedure
Participants viewed the images from Study 1 and indicated how much they believed each target is characterized by gendered emotional dramatization stereotypes (i.e., whiny, fussy, nagging, complaining), selected from Diekman and Eagly’s (2000) Gender-Stereotypic Dimensions scale, on a 1 (“Strongly disagree”) to 7 (“Strongly agree”) Likert-type scale. Responses to the traits were averaged for each target; higher values indicate more stereotype application. Then, participants completed the pain expectation procedure from Study 1. Again, responses to all injuries were averaged to create expected feel and claim scores; higher values indicate more expected pain. Participants then completed a Motivation to Respond Without Sexism measure (Klonis et al., 2005), followed by reporting demographics. Scale descriptive statistics and correlations between measures are in Table 2.
Table 2.
Means, standard deviations, reliabilities, and correlations
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Expected pain felt by women | 2.67 | 0.48 | (.83) | |||||||||
| 2. Expected pain claimed by women | 2.75 | 0.52 | .78*** | (.89) | ||||||||
| 3. Expected pain exaggeration by women | 0.08 | 0.33 | −.22* | .44*** | (X) | |||||||
| 4. Expected pain felt by men | 2.40 | 0.48 | .67*** | .44*** | −.28** | (.85) | ||||||
| 5. Expected pain claimed by men | 2.33 | 0.57 | .44** | .39*** | −.02 | .71*** | (.90) | |||||
| 6. Expected pain exaggeration by men | −0.07 | 0.41 | −.18 | .03 | .30** | −.20* | .55*** | (X) | ||||
| 7. Attribution of emotional dramatization traits to women | 3.76 | 1.01 | .04 | .23* | .29** | −.05 | .01 | .07 | (.95) | |||
| 8. Attribution of emotional dramatization traits to men | 3.40 | 0.93 | −.10 | −.14 | −.07 | .01 | .24* | .32** | .30** | (.94) | ||
| 9. Internal motivation to respond without sexism | 7.25 | 1.80 | .07 | .10 | .06 | .05 | .23* | .26** | −.03 | .02 | (.70) | |
| 10. External motivation to respond without sexism | 4.66 | 2.29 | .15 | .18 | .06 | .05 | −.11 | −.21* | .26** | −.11 | −.24* | (.74) |
Note. M and SD are used to represent mean and standard deviation, respectively. Reliabilities (α) are displayed on the diagonal.
indicates p < .05.
indicates p < .01,
indicates p < .001.
Results
Expectations of Pain Felt and Claimed by Target Gender
We conducted a linear mixed effects regression with amount of pain regressed on fixed effects of target gender (woman = −0.5, man = 0.5), type of expectation (feel = −0.5, claim = 0.5), and their interaction with random effects of the intercept and main effect slopes by participant.5 A likelihood-ratio test indicated this model fit the data better than a model with no fixed effects, χ2(3) = 55.58, p < .001. The target gender effect was significant, b = −0.35, β = −0.24, F(1, 99) = 58.74, p < .001, with women (M = 2.71, SE = 0.06) attributed more pain than men (M = 2.36, SE = 0.06). The type of expectation effect was non-significant, b = 0.01, β = 0.00, F(1, 99) = 0.03, p = .863. The target gender by type of expectation interaction was significant, b = −0.14, β = −0.05, F(1, 1699) = 8.98, p = .003 (Figure 1 – Study 2). Perceivers expected women to claim (M = 2.75, SE = 0.07) more than they feel (M = 2.67, SE = 0.07), b = 0.08, β = 0.06, F(1, 899) = 5.05, p = .025, but non-significantly expected men to claim (M = 2.33, SE = 0.07) less than they feel (M = 2.39, SE = 0.07), b = −0.07, β = −0.05, F(1, 99) = −1.63, p = .107.
Attributions of Emotional Dramatization Traits by Target Gender
We assessed whether women were attributed more emotional dramatization traits than men via a linear mixed effects regression with emotional dramatization trait attributions regressed on a fixed effect of target gender and random effects of the intercept and slope of target gender by participant. A likelihood-ratio test indicated this model provided a better fit than a model with no fixed effects, χ2(1) = 9.49, p = .002. The effect of target gender was significant, b = −0.36, β = −0.12, F(1, 99) = 9.86, p = .002, with perceivers attributing women (M = 3.76, SE = 0.10) more emotional dramatization traits than men (M = 3.40, SE = 0.09).
Mediation of Exaggeration Expectations by Attributions of Emotional Dramatization Traits
Of primary interest, we tested whether judgments of women (relative to men) as more emotionally dramatizing contribute to the gender-pain exaggeration bias. Importantly, we do not manipulate the mediator, so the model tested here cannot demonstrate causality (see Fiedler et al., 2018 for discussion of appropriate inferences based on statistical mediation). Rather, this model represents one plausible cognitive pathway to the gender-pain exaggeration bias. To represent pain exaggeration expectations, we computed claim – feel difference scores (higher numbers indicate expecting more exaggeration or less downplaying). Using the R package ‘mediation’ (Tingey et al., 2014), we found a significant indirect effect of attributions of emotional dramatization traits on exaggeration expectations, b = −0.05, 95% CI = [−0.10, −0.01], p = .002 (see Figure 2), such that perceivers believed women, relative to men, were more likely to exaggerate pain insofar as they believed women were more emotionally dramatizing.
Figure 2.
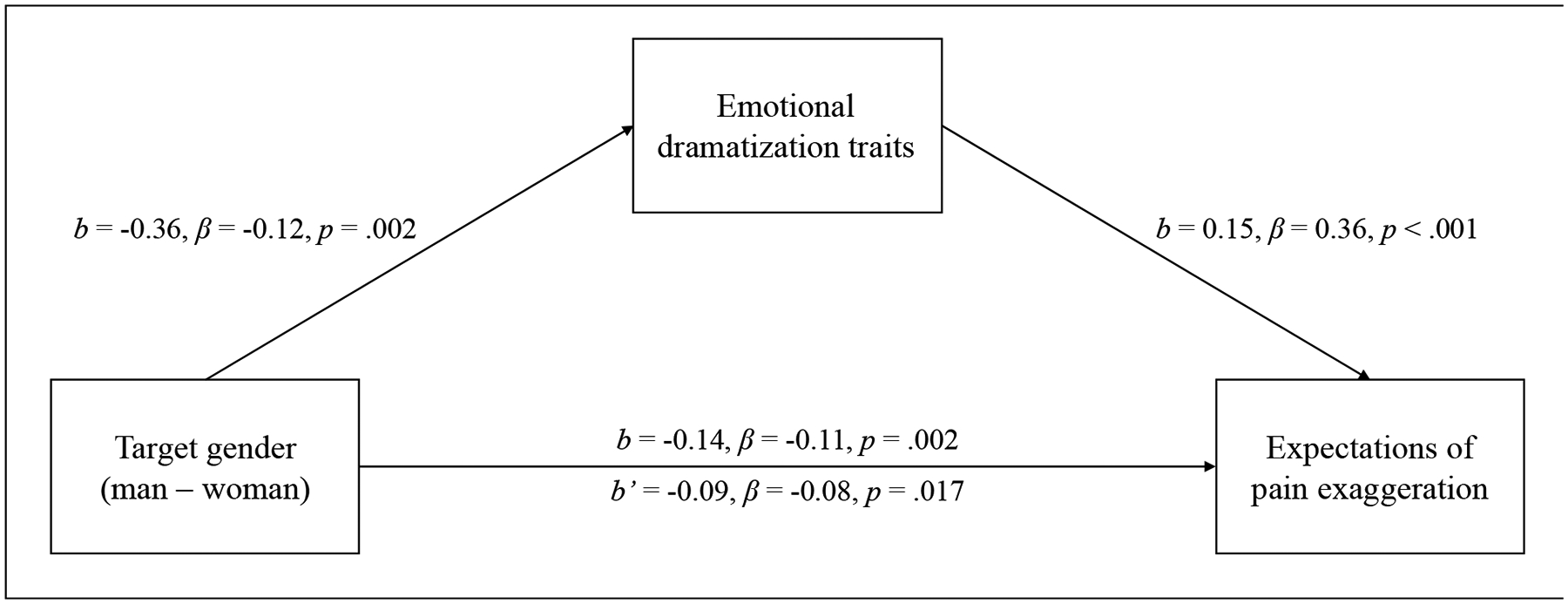
Mediation model depicting the effect of target gender (man – woman) on expected pain exaggeration (higher values = more exaggeration) through attributions of emotional dramatization traits (higher values = more whiny, nagging, fussy, and complaining).
Discussion
We replicated the gender-pain exaggeration bias. We also observed statistical evidence that this bias was informed in part by gendered application of emotional dramatization traits. We caution against causal interpretation (we did not manipulate the mediator), and instead interpret the significant indirect effect as evidence that domain-general emotional dramatization beliefs may contribute to domain-specific expectations that women exaggerate pain more than men.
Study 3
We next test whether perceivers’ gender-related beliefs influence the strength of the gender-pain exaggeration bias. We theorized that perceivers who strongly endorse ambivalent sexism (Glick & Fiske, 1997; Glick & Fiske, 2001) and stereotypes would show an exacerbated gender-pain exaggeration bias. Indeed, endorsing sexism (e.g., Viki & Abrams, 2003) and gender stereotypes (e.g., Hutson-Comeaux & Kelly, 2002) has been linked to negative perceptions of women. In the remaining studies, we test whether perceivers’ gender-related beliefs moderate the gender-pain exaggeration bias. One study, reported in the Supplemental Materials, replicated the gender-pain exaggeration bias but did not find moderation by sexism (Supplemental Study 1). In Study 3, we focus on perceiver stereotype endorsement as a moderator instead. In Study 2, we found that the extent to which emotional dramatization stereotypes were applied more to women informed the extent to which women were believed to be more likely to exaggerate pain. In Study 3, we now test whether perceiver differences in endorsement of these stereotypes for women and men as a group informs the strength of the gender-pain exaggeration bias.
Providing support for the role of group-level gender stereotypes in perceptions of pain expressions, Zhang and colleagues (2021) found that perceivers underestimated female, compared to male, patients’ pain, and this effect was moderated by differential endorsement of gendered pain expressivity stereotypes. That is, perceivers’ relative underestimation of female targets’ pain was strongest among those who most believed that women are more willing to express pain than men. Thus, group-based stereotypes may contribute to gender bias in perception of pain expressions. However, Zhang and colleagues’ stereotype measure was one item about willingness to express pain, which is more similar to our outcome variable (though missing some of the complexity that assessing expectations of pain felt and claimed in tandem affords) than to the stereotype content we assess. We aim to capture general feminine stereotype content: that women are whiny, fussy, nagging, and complaining. These stereotypes are domain-general (i.e., not specific to pain) and socially pervasive (Barrett & Bliss-Moreau, 2009; Bauer, 2015; Brescoll, 2016; Hess et al., 2000; Shields, 2002), which makes understanding consequences of endorsing these stereotypes for pain judgments important.
We expect that group-level endorsement of gendered emotional dramatization stereotypes will moderate the gender-pain exaggeration bias such that this bias will be exacerbated among those high on endorsement of gendered emotional dramatization stereotypes. Hereafter, we refer to such group-based gendered (i.e., more for women than men) endorsement of these stereotypes as gendered stereotype endorsement or GSE. Our primary hypothesis was that GSE would moderate the gender–pain exaggeration bias such that this bias would be strongest among perceivers who endorse emotional dramatization stereotypes more for women than men.
Method
Participants
American participants (N=64) were recruited via CloudResearch (Litman et al., 2017). Power analysis via simr (Green & MacLeod, 2016) indicated that our main analytic model could detect a small (β = 0.10) three-way interaction between target gender, pain type, and GSE with adequate power (95% CI [98.17%, 100.0%]). Participants were primarily men (57.8% men, 40.6% women, 1.6% identified with more than one gender), primarily White (73.4% White, 17.2% Black, 9.4% as Asian), primarily non-Hispanic (89.1% non-Hispanic, 9.4% Hispanic), and ranged in age from 23 to 67 (M = 37.48, SD = 11.46). No participants were excluded.
Procedure
Participants completed the pain expectation procedure from Study 1. Responses to all injuries were averaged to create expected feel and claim scores (higher values indicate more expected pain). Participants then completed a GSE measure. This measure consisted of the traits from Study 2 (i.e., whiny, fussy, nagging, complaining), but participants completed this measure for women on average and once for men on average rather than for each target. The items were presented in a random order and responded to on 1 (“Strongly disagree”) to 7 (“Strongly agree”) Likert-type scales. Responses were averaged separately for women and men (higher values indicate greater belief that women/men on average are emotionally dramatizing). We computed a GSE difference score (women – men) where higher values indicate believing women, relative to men, as a group are more emotionally dramatizing. Finally, participants completed a Motivation to Respond Without Sexism measure (Klonis et al., 2005), then a brief demographic survey. Scale descriptive statistics and correlations between measures are in Table 3.
Table 3.
Means, standard deviations, reliabilities, and correlations
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Expected pain felt by women | 2.59 | 0.38 | (.74) | ||||||||
| 2. Expected pain claimed by women | 2.66 | 0.50 | .83** | (.84) | |||||||
| 3. Expected pain felt by men | 2.40 | 0.42 | .58** | .43** | (.79) | ||||||
| 4. Expected pain claimed by men | 2.26 | 0.54 | .42** | .35** | .74** | (.87) | |||||
| 5. Stereotypes of women as emotionally dramatizing | 4.46 | 1.35 | .15 | .11 | −.08 | −.11 | (.88) | ||||
| 6. Stereotypes of men as emotionally dramatizing | 3.38 | 1.33 | .02 | −.06 | .29* | .39** | .29* | (.86) | |||
| 7. Gendered stereotype endorsement | 1.09 | 1.60 | .11 | .14 | −.31* | −.42** | .61** | −.59** | (X) | ||
| 8. Internal motivation to respond without sexism | 6.66 | 2.02 | −.23 | −.21 | .03 | −.07 | −.45** | −.04 | −.35** | (.91) | |
| 9. External motivation to respond without sexism | 4.53 | 2.23 | .20 | .09 | .16 | .14 | .35** | .35** | .00 | −.12 | (.92) |
Note. M and SD are used to represent mean and standard deviation, respectively. Reliabilities (α) are displayed on the diagonal.
indicates p < .05,
indicates p < .01,
indicates p < .001.
Results
Expectations of Pain Felt and Claimed by Target Gender
We conducted a linear mixed effects regressing by regressing amount of expected pain on fixed effects of target gender (woman = −0.5, man = 0.5), type of expectation (feel = −0.5, claim = 0.5), and their interaction with random effects of the intercept and slope of each fixed effect by participant. A likelihood-ratio test indicated that this model fit the data better than a model with no fixed effects, χ2(3) = 38.87, p < .001. The target gender effect was significant, b = −0.30, β = −0.24, F(1, 63) = 29.09, p < .001, with women (M = 2.63, SE = 0.05) attributed more pain than men (M = 2.33, SE = 0.05). The effect of type of expectation was not significant, b = −0.04, β = −0.03, F(1, 63) = 1.47, p = .230. The target gender by type of expectation interaction was significant, b = −0.21, β = −0.08, F(1, 63) = 14.31, p < .001 (Figure 1 – Study 3). Perceivers non-significantly expected women to claim (M = 2.66, SE = 0.06) more than they feel (M = 2.59, SE = 0.06), b = 0.07, β = 0.06, F(1, 63) = 3.77, p = .057, but expected men to claim (M = 2.26, SE = 0.06) less than they feel (M = 2.40, SE = 0.06), b = −0.14, β = −0.11, F(1, 63) = 9.30, p = .003.
Moderation of Gendered Pain Expectations by GSE
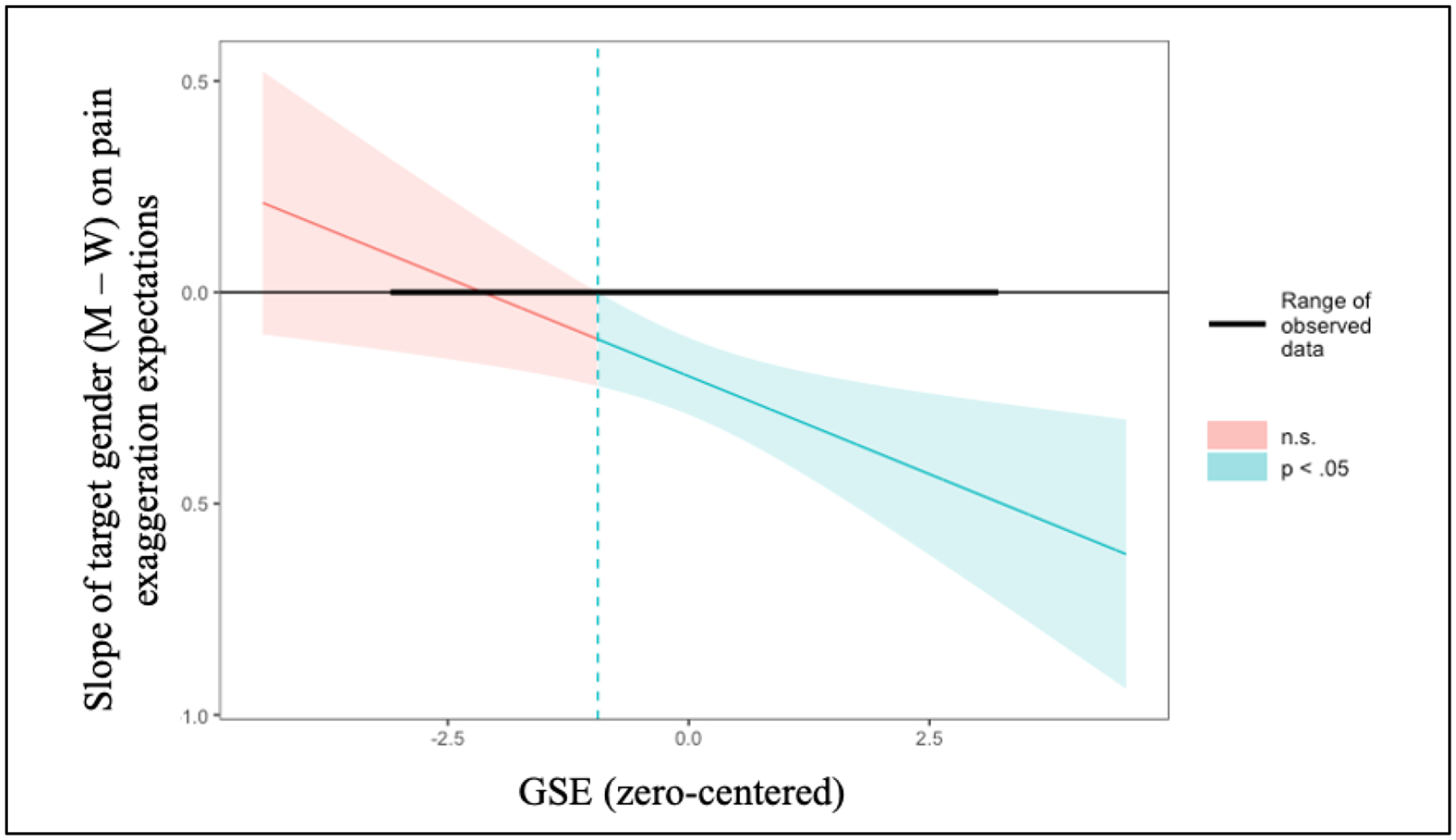
To test whether the effects of target gender and type of pain expectation on amount of pain expected are moderated by GSE, we centered the GSE difference score and added GSE and interactions between GSE and effects reported above to our model. A likelihood-ratio test indicated that this model fit the data better than the model above, χ2(4) = 30.31, p < .001. The main effect of GSE was not significant, b = −0.04, β = 0.09, F(1, 62) = 1.67, p = .201, nor was the interaction between GSE and type of expectation, b = −0.02, β = 0.09, F(1, 62) = 1.34, p = .252. The target gender by GSE interaction was significant, b = −0.15, β = 0.09, F(1, 62) = 24.09, p < .001, as was the predicted target gender by type of expectation by GSE interaction, b = −0.07, β = −0.05, F(1, 62) = 5.27, p = .025. Pattern of effects reported above was unchanged. Given our focus on the gender-pain exaggeration bias, we only probed the significant three-way (target gender by type of expectation by GSE) interaction (see Figure 3). We restructured our data so that expectations of feel and claim for each target and participant were in the same row and computed exaggeration expectation scores (claim – feel; higher numbers indicate expecting more exaggeration/less downplaying). We then ran a Johnson-Neyman test assessing at what levels of GSE the gender-pain exaggeration bias was significant. This test indicated that the effect of gender on pain exaggeration was significant (p < .05) for those with values of GSE > 0.02. GSE > 0 indicates endorsing these stereotypes more for women. That is, perceivers who believed that women tend to be more emotionally dramatizing displayed significant pain-gender exaggeration biases (i.e., a significant effect of gender on the contrast between claim and feel).
Figure 3.
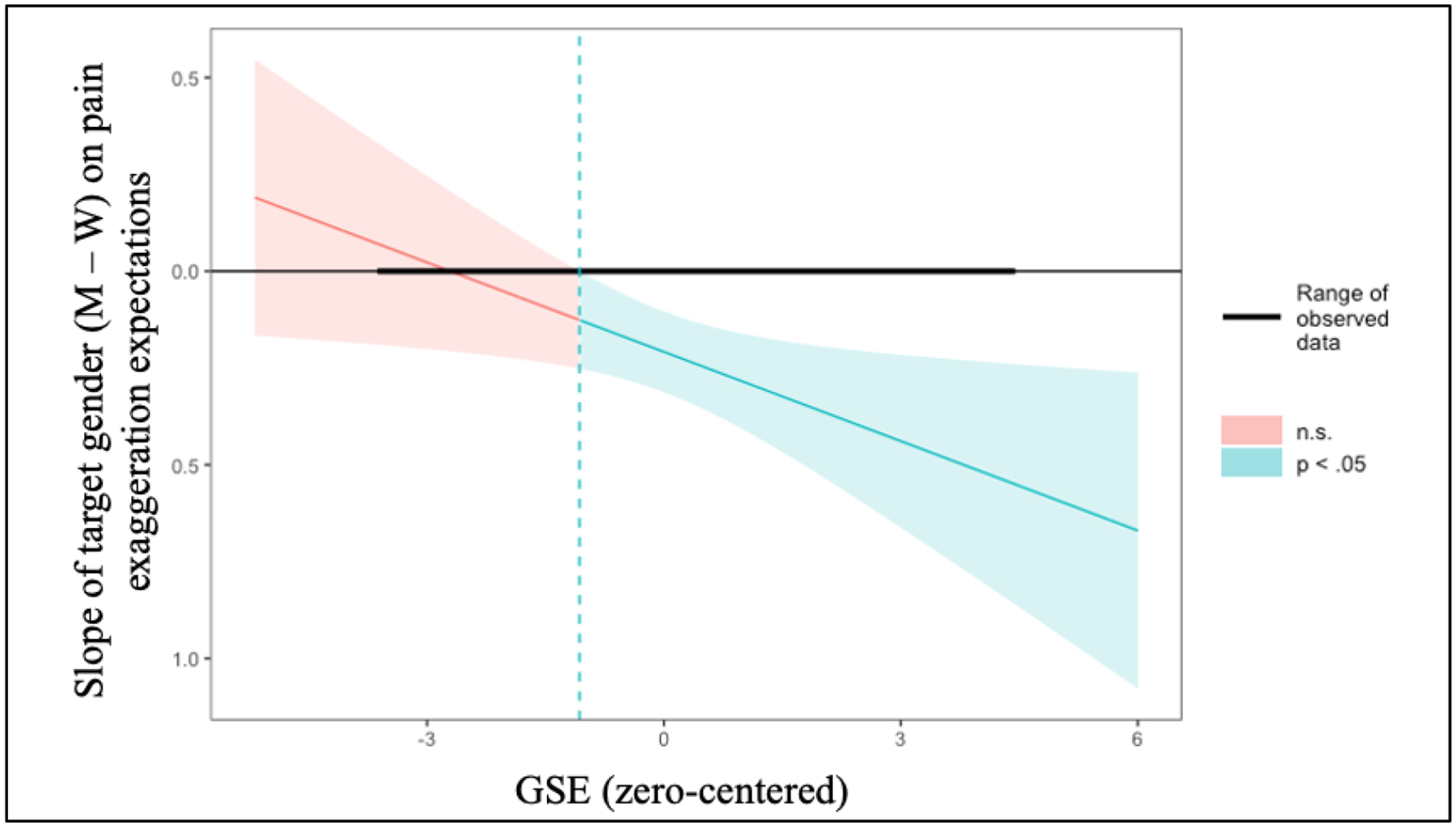
Johnson-Neyman plot of the significance of target gender on exaggeration expectations by GSE; values of GSE to the right of the dotted line are those where the gender-pain exaggeration bias was significant and values to the left are those where the gender-pain exaggeration bias was not significant.
Discussion
We replicated the gender-pain exaggeration bias and found that this bias was exacerbated among those who stereotyped women (vs. men) as a group as more emotionally dramatizing. This complements and extends Study 2 where the extent to which perceivers judged target women (vs. men) as emotionally dramatizing informed how much they expected those women (vs. men) to exaggerate pain. Together, Studies 2 and 3 suggest that both stereotype application and perceiver-level differences in stereotype endorsement can play a role in gendered pain expectations. However, we have not assessed both in the same study; this is the goal of Study 4.
Study 4
We sought to replicate and extend Studies 2 and 3 by assessing general endorsement of emotional dramatization stereotypes (GSE) and application of these traits to targets in the same study. Thus, Study 4 tests a pattern of moderated mediation wherein perceiver GSE moderates the pattern of mediation from Study 2 (the effect of target gender on exaggeration expectations through attributions of emotional dramatization traits). We expected to replicate Study 2 (targets who are women would be judged as relatively more likely to exaggerate pain insofar as they are judged as more emotionally dramatizing) and Study 3 (judgments of women as relatively likely to exaggerate pain will be driven by high GSE perceivers). Of primary interest was whether the pattern of mediation observed in Study 2 similarly emerged regardless of perceivers’ GSE.
Method
Participants
American participants (N=101) were recruited via CloudResearch (Litman et al., 2017). Power analysis via simr (Green & MacLeod, 2016) indicated that our main analytic model was adequately powered to detect a small (β = 0.10) interaction between target gender, pain type, and GSE (95% CI [98.17%, 100.00%]). Participants were primarily men (53.5% men, 40.6% women, 5.0% identified with more than one gender, 1.0% preferred not to identify), primarily White (77.2% White, 8.9% Black, 7.9% Asian, 4.0% bi- or multi-racial, 1.0% American Indian/Alaska Native, 1.0% self-identified), primarily non-Hispanic (85.1% non-Hispanic, 13.9% Hispanic), and ranged in age from 21 to 72 (M = 37.94, SD = 11.83). No participants were excluded.
Procedure
Participants completed the emotional dramatization traits attribution procedure from Study 2. Responses to the four traits were averaged separately for each target and higher values indicate judging a target as more emotionally dramatizing. Participants then completed the pain expectation procedure from Study 1. Responses to all injuries were averaged to create composite expected feel and claim scores separately for each target and higher values indicate higher expectations of pain. Participants then completed the GSE measure from Study 3. Responses to the four traits were averaged separately for women and men. We computed a GSE difference score (women – men) where higher values indicate believing women as a group, relative to men as a group, are more emotionally dramatizing. Finally, participants completed a measure of Motivation to Respond Without Sexism (Klonis et al., 2005) then a brief demographic survey. Scale descriptive information and correlations between measures are presented in Table 4.
Table 4.
Means, standard deviations, reliabilities; and correlations
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Expected pain felt by women | 2.66 | 0.44 | (.83) | ||||||||||||
| 2. Expected pain claimed by women | 2.68 | 0.52 | .80*** | (.89) | |||||||||||
| 3. Expected pain exaggeration by women | 0.02 | 0.31 | −.09 | .52*** | (X) | ||||||||||
| 4. Expected pain felt by men | 2.37 | 0.41 | .59*** | .46*** | −.08 | (.77) | |||||||||
| 5. Expected pain claimed by men | 2.19 | 0.49 | .24* | .27** | .11 | .55*** | (.86) | ||||||||
| 6. Expected pain exaggeration by men | −0.18 | 0.43 | −.29** | −.13 | .20* | −.33*** | .61*** | (X) | |||||||
| 7. Attributions of emotional dramatization traits to women | 3.76 | 1.01 | .22* | .29** | .18 | .15 | .10 | −.03 | (.95) | ||||||
| 8. Attributions of emotional dramatization traits to men | 3.21 | 1.01 | −.22* | −.13 | .09 | .16 | .36*** | .25* | .51*** | (.95) | |||||
| 9. Stereotypes of women as emotionally dramatizing | 4.36 | 1.31 | .25* | .29** | .13 | .12 | .04 | −.06 | .50*** | .21* | (.90) | ||||
| 10. Stereotypes of men as emotionally dramatizing | 3.30 | 1.18 | −.00 | .01 | .02 | .18 | .31** | .18 | .28** | .52*** | .40*** | (.85) | |||
| 11. Gendered stereotype endorsement | 1.06 | 1.36 | .24* | .28** | .11 | −.05 | −.23* | −.21* | .24* | −24* | .61*** | −.47*** | (X) | ||
| 12. Internal motivation to respond without sexism | 7.00 | 2.02 | .02 | −.03 | −.09 | .12 | .18 | .09 | −.21* | .03 | −.28** | .11 | −.36*** | (.91) | |
| 13. External motivation to respond without sexism | 4.12 | 2.29 | .25* | .27** | .08 | .14 | .05 | −.08 | .28** | .12 | .42*** | .16 | .26** | −.10 | 0 |
Note. M and SD are used to represent mean and standard deviation, respectively. Reliabilities (α) me displayed un the diagonal.
indicates p < .05.
indicates p < .01,
indicates p< .001.
Results
Expectations of Pain Felt and Claimed by Target Gender
We conducted a linear mixed effects regression by regressing amount of expected pain on fixed effects of target gender (woman = −0.5, man = 0.5), type of expectation (feel = −0.5, claim = 0.5), and their interaction with random effects of the intercept and all slopes by participant. A likelihood-ratio test indicated this model fit the data better than a model with no fixed effects, χ2(3) = 80.60, p < .001. The target gender effect was significant, b = −0.39, β = −0.29, F(1, 99) = 76.48, p < .001, with women (M = 2.67, SE = 0.04) attributed more pain than men (M = 2.28, SE = 0.04). The type of expectation effect was significant, b = −0.08, β = −0.06, F(1, 99) = 7.48, p = .007, with perceivers expecting people to claim (M = 2.44, SE = 0.04) less than they feel (M = 2.51, SE = 0.04). The target gender by type of expectation interaction was significant, b = −0.20, β = −0.07, F(1, 99) = 17.11, p < .001 (Figure 1 – Study 4). Perceivers non-significantly expected women to claim (M = 2.68, SE = 0.05) more than they feel (M = 2.66, SE = 0.05), b = 0.02, β = 0.02, F(1, 908) = 0.39, p = .531, but expected men to claim (M = 2.19, SE = 0.05) less than they feel (M = 2.37, SE = 0.05), b = −0.18, β = −0.14, F(1, 100) = 17.14, p < .001.
Mediation of Exaggeration Expectations by Attributions of Emotional Dramatization Traits
To replicate Study 2, we computed exaggeration (claim – feel) difference scores (higher numbers indicate expecting more exaggeration and less downplaying) and used the ‘mediation’ package. Again, the model tested here, as well as the moderated mediation, cannot demonstrate causality (see Fiedler et al., 2018). This analysis revealed a significant indirect effect of attributions of emotional dramatization traits on exaggeration expectations, b = −0.07, 95% CI = [−0.10, −0.04] (see Figure 4), such that perceivers believed women, relative to men, would exaggerate pain insofar as they believed women were more emotionally dramatizing.
Figure 4.
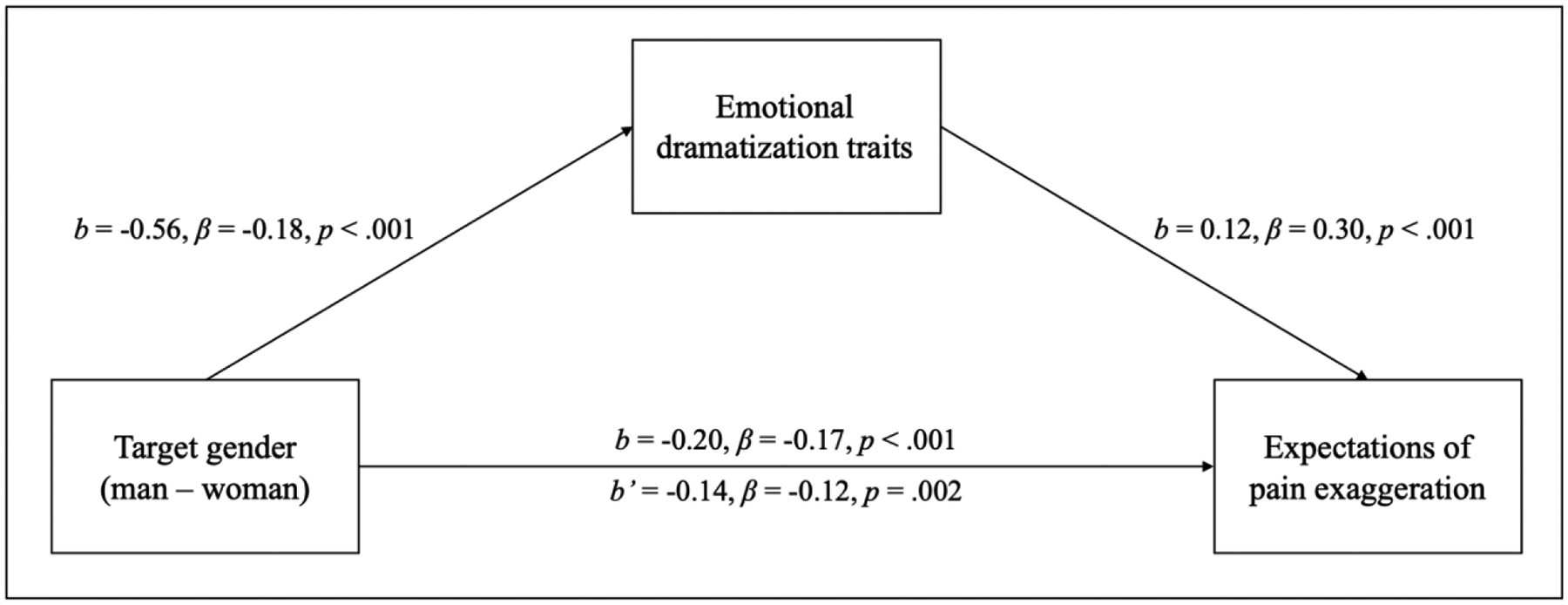
Mediation model depicting the effect of target gender (man – woman) on expected pain exaggeration (higher values = more exaggeration) through attributions of emotional dramatization traits (higher values = more whiny, fussy, nagging, and complaining).
Moderation of Gendered Pain Expectations by GSE
To replicate Study 3, we centered GSE and added GSE and interactions between GSE and our three effects to our model. A likelihood-ratio test indicated that this model provided a better fit than the model without GSE, χ2(4) = 28.41, p < .001. The main effect of GSE was not significant, b = 0.02, β = 0.09, F(1, 98) = 0.70, p = .405, nor was the interaction between GSE and type of expectation, b = −0.02, β = 0.09, F(1, 98) = 0.95, p = .331. There was a significant target gender by GSE interaction, b = −0.15, β = 0.09, F(1, 98) = 91.80, p < .001, and a significant target gender by type of expectation by GSE interaction, b = 0.05, β = −0.08, F(1, 98) = 7.32, p = .008 (see Figure 5). Patterns of effects reported above were unchanged. We again probed the target gender by type of expectation by GSE interaction via slope significance tests. The Johnson-Neyman test indicated that the effect of gender on pain exaggeration was significant (p < .05) for participants with values of GSE > 0.12. Again, this analysis suggests that participants who believed that women in general are more emotionally dramatizing than men in general displayed the pain-gender exaggeration bias to a significant extent.
Figure 5.
Johnson-Neyman plot of the significance of target gender on exaggeration expectations by GSE; values of GSE to the right of the dotted line are those where the gender-pain exaggeration bias was significant and values to the left are those where the gender-pain exaggeration bias was not significant.
Moderated Mediation
Of primary interest, we tested whether the mediation of target gender on exaggeration expectations through emotional dramatization traits is best understood as a moderated mediation wherein this pattern of mediation only emerges among perceivers who strongly endorse GSE. To this end, we dichotomized GSE scores by median splitting and re-ran the mediation separately for low (i.e., below the median) and high (i.e., above the median) GSE perceivers. Because the variables in our base mediation model are assessed as repeated measures, we cannot directly test a continuous moderator of the mediation model. However, the approach employed here is limited in that it dichotomizes a continuous variable, which reduces how much complexity our analyses can capture.6 Nonetheless, this analysis allows us to approximate whether the role of stereotype application in the gender-pain exaggeration bias depends on perceivers’ global endorsement of gender-emotionality stereotypes. We again employed the ‘mediation’ package, now to test whether the mediation above emerges for participants low and high on GSE. For low GSE perceivers, the indirect effect of attributions of emotional dramatization traits on exaggeration expectations was not significant, b = −0.02, 95% CI = [−0.07, 0.01], p = .210 (see Figure 6). Conversely, for high GSE perceivers, the indirect effect of attributions of emotional dramatization traits on exaggeration expectations was significant, b = −0.09, 95% CI = [−0.15, −0.04], p < .001 (see Figure 6), such that perceivers judged women as relatively more likely to exaggerate pain insofar as they were more characterized by emotional dramatization traits.
Figure 6.
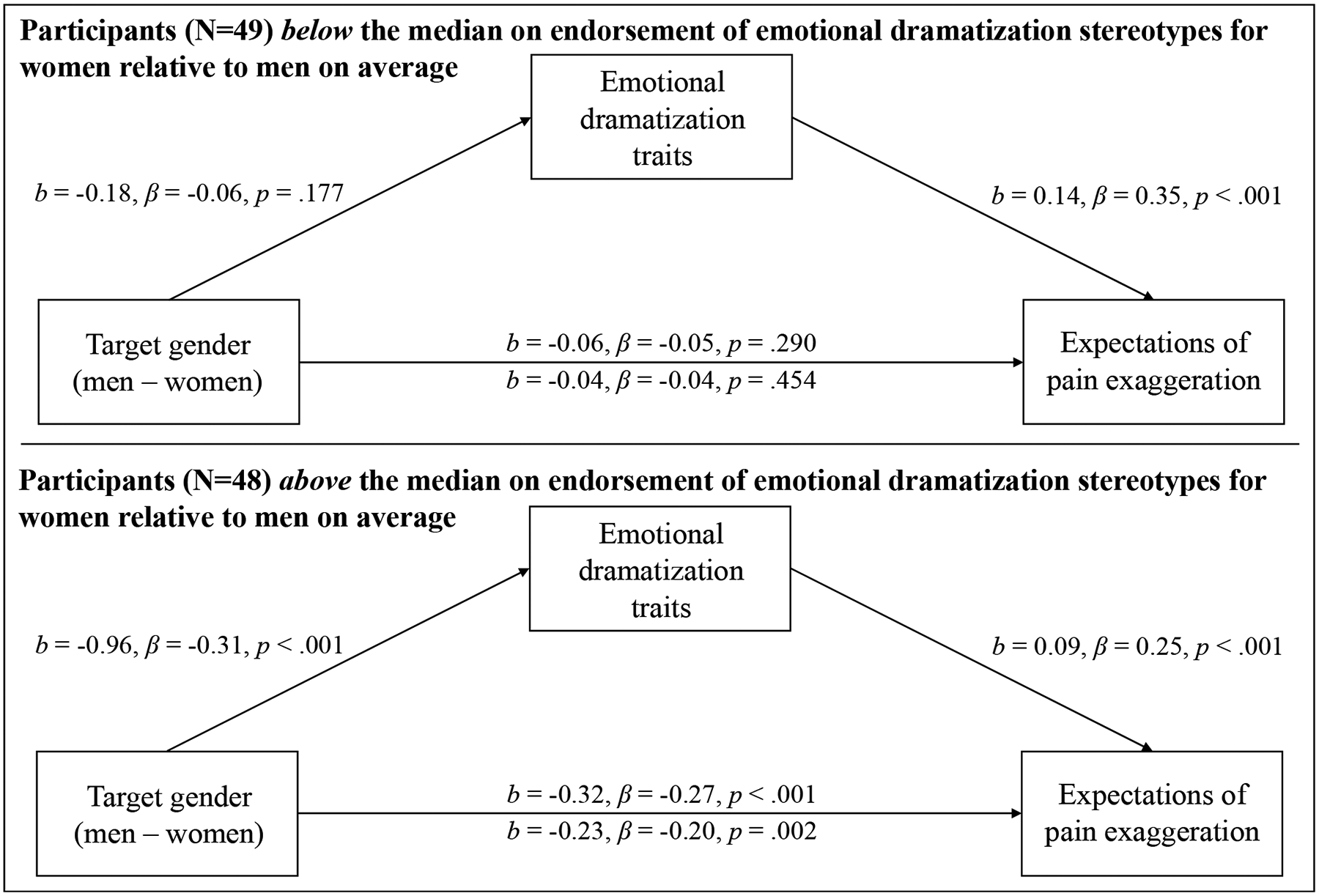
Mediation models depicting the effect of target gender (men – women) on expected pain exaggeration (higher values = more exaggeration) through attributions of emotional dramatization traits (higher values = more whiny, fussy, nagging, and complaining).
Discussion
This study replicated the gender-pain exaggeration bias and replicated findings from Studies 2 (application of emotional dramatization traits mediated gendered expectations of pain exaggeration) and 3 (perceiver GSE moderated the gender-pain exaggeration bias). Finally, we assessed a moderated mediation model finding that application of emotional dramatization traits only mediated the effect of target gender on exaggeration expectations for those high on GSE.
General Discussion
We tested whether perceivers expected women to exaggerate pain relative to men (Studies 1–4), whether this effect was mediated by application of emotional dramatizing traits (Studies 2 and 4), and whether this effect was moderated by perceivers’ endorsement of emotional dramatization stereotypes for women and men as a group (Studies 3–4). We found a consistent gender-pain exaggeration bias whereby women, relative to men, were expected to exaggerate more and downplay pain less. Further, this effect was mediated by judgments that the target women were more emotionally dramatizing than the target men and moderated by perceivers’ overarching gendered emotional dramatization stereotypes.
Given that the simple effects of type of pain expectations for men and women were not consistently significant (i.e., in some studies the simple effect was significant for women but not men, and in other studies the opposite was true), we conducted mini meta-analyses (Goh et al., 2016; McShane & Böckenholt, 2017). We first conducted a single-paper meta-analysis (SPM; McShane & Böckenholt, 2017) on the interactive target gender by type of pain expectations effect across Studies 1–4 and Supplemental Study 1. This SPM point estimate, −0.22, 95% CI [−0.31, −0.12] was significant, Z = 4.41, p < .001; Figure 7 – Panel A. Then, we conducted an SPM on the simple effect of type of pain expectations for women across Studies 1–4 and Supplemental Study 1. This SPM point estimate, −0.06, 95% CI [−0.13, 0.00] was not significant, Z = −1.86, p = .062; Figure 7 – Panel B. Finally, we conducted an SPM on the simple effect of type of pain expectations for men across Studies 1–4 and Supplemental Study 1. This SPM point estimate, 0.15, 95% CI [0.07, 0.43] was significant, Z = 3.82, p = .002; Figure 7 – Panel C. The simple effects mini meta-analyses suggest that this gender-pain exaggeration bias is best characterized as consisting of beliefs about men downplaying pain and beliefs of women as expressing their pain accurately or exaggerating. Thus, the current work may carry implications for both women’s and men’s experiences with pain or seeking pain care.
Figure 7.
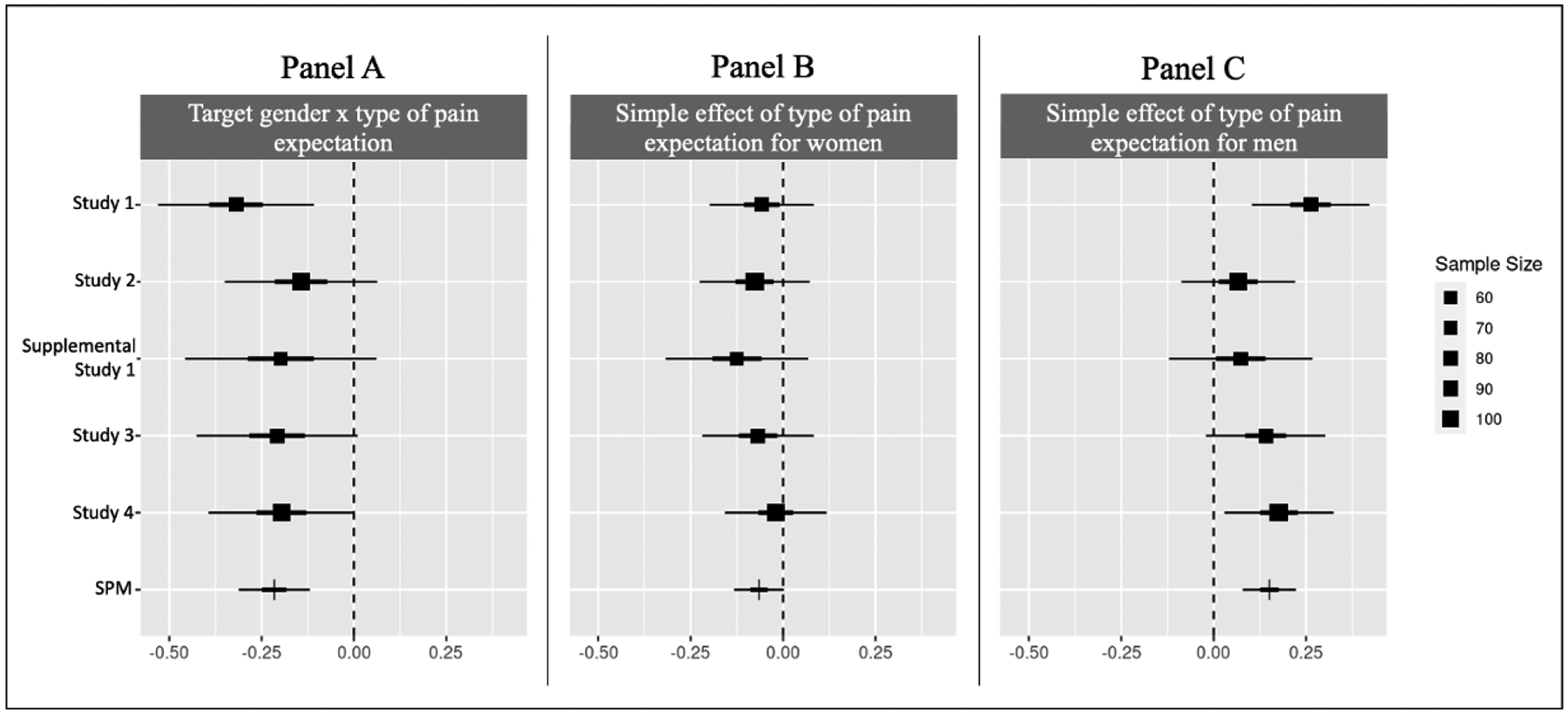
Forest plots of estimates of the target gender by type of pain expectation interaction (Panel A), the simple effect of type of pain expectation for women (Panel B), and the simple effect of type of pain expectation for men (Panel C). The row labeled ‘SPM’ represents the single-paper meta-analytic effect size estimate. Dot size indicates sample size, the thick line indicates the 50% confidence interval, and the thin line indicates the 95% confidence interval.
Implications
The current work offers theoretical and practical insights for pain science and gender equity. We found clear and consistent evidence that perceivers expect women, relative to men, to exaggerate pain more and downplay pain less. This complements and extends work from Schäfer and colleagues (2016) where women’s (relative to men’s) expressions of shoulder pain were judged as more likely to be exaggerated. We found that this bias associating women with exaggerating pain also pervades pain expectations. In our studies, perceivers indicated pain expectations for several images of women and men. All images depicted White individuals who were similarly average in attractiveness, but these images varied freely on other trait dimensions (e.g., trustworthiness). Thus, the current work expanded previous work both theoretically by assessing expectations and practically by considering generalizability across target individuals.
We also tested a potential mediator and moderators of this bias, finding that gendered stereotypes may be particularly influential. Scholars have oft theorized that stereotypes contribute to gender-pain treatment disparities. Here, we found that gendered stereotypes about emotional dramatization – that women are relatively fussy, whiny, nagging, and complaining – influenced gender-pain exaggeration expectations. However, it is yet unknown whether other gender stereotypes might also foster gender bias in pain expectations; we focused on negative feminine stereotypes about emotionality, but it is possible that positive masculine stereotypes about emotional control (e.g., stoic; Diekman and Eagly, 2000) could also contribute to the gender-pain exaggeration bias. Nonetheless, the current work clearly suggests the importance of considering gender stereotypes when studying gender biases in pain, thereby laying groundwork for future work to directly test stereotypes as a mechanism to various gender biases in perceptions of pain expressions and responses to pain.
Further, considering claim and feel in tandem advances literature on pain expectations. First, expectations of pain claimed and felt may contribute to processes, such as pain underestimation, that contribute to inadequate treatment of women’s pain. Past work suggests that laypeople and medical providers alike underestimate others’ pain (e.g., Prkachin et al., 2007), and women’s pain is underestimated more than men’s (e.g., Pronina & Rule, 2016). Pain underestimation is theorized to be a result of where perceivers place their threshold for what amount of expression represents pain (Mende-Siedlecki et al., 2019). Perceivers’ thresholds for labeling an expression as pain may shift based on expectations about how the expression reflects the expresser’s internal experience. For instance, expecting a person to claim more pain than they feel might raise the threshold (i.e., lead one to require more expression to label it as pain), whereas expecting a person to claim less pain than they feel might lower the threshold (i.e., lead one to require less expression to label it as pain). Thus, expecting women to exaggerate and men to downplay may be associated with perceivers setting higher and lower thresholds for women’s and men’s pain respectively. Testing how pain expectations influence judgments of actual pain expressions is a fruitful avenue for future work. Considering pain felt and claimed in tandem may also further research on trust of pain disclosures. Past research on trust for pain has often assessed perceptions of individuals expressing real pain or faking pain. Understanding perceptions of pain expressions is important but is often costly; the current framework offers a less costly alternative. Further, trust in pain is likely more nuanced than judging whether pain is genuine or feigned. A perceiver might believe an expression reflects real pain but is exaggerated, leading them to distrust the expresser. Future research might leverage the framework used here to examine characteristics of targets (e.g., social goals such as gaining attention or hedonic goals such as gaining access to medication) or perceivers (e.g., trait empathy) theorized to affect trust aside from or in addition to gender.
The findings of the current work also have practical implications for gender disparities in pain. Previous work has found that women’s, relative to men’s, pain is undertreated (e.g., Chen et al., 2008), despite perceivers judging women as more sensitive to pain (e.g., Summers, Weesner, et al., 2023). This is interesting given that other work suggests expectations of pain sensitivity are closely related to pain treatment recommendations such that people who are perceived as more sensitive to pain are recommended more intensive pain treatment. That is, gender-pain treatment disparities cannot be explained by the pain sensitivity to pain treatment mechanism theorized to underlie race- and SES-pain treatment disparities. Though not tested in the current work, we believe that the gender-pain exaggeration bias documented herein may inform gender biases in pain estimation and treatment. This is a fruitful avenue for future work aiming to ameliorate gender biases in pain domains.
There are numerous established gender-pain disparities whereby women are disadvantaged relative to men (e.g., women are more prone to pain invalidation and less likely to receive adequate pain care); however, there are also ways in which men are disadvantaged. For example, men tend to report lower levels of health care utilization (e.g., less likely to seek primary care) than women (e.g., Bertakis et al., 2000; Owens, 2008; Pinkhasov et al., 2010). Though not tested in the current work, perhaps the cultural stereotype that men downplay pain contributes to men’s low engagement with health care systems. That is, if men know that they are expected to downplay pain, they may feel like they should not seek care unless pain is extreme. To this point, Boring and colleagues (2022) found that men indicated intentions to report the exact amount of pain they felt – not less. Thus, if men are aware that they are expected to downplay pain but would prefer to express pain accurately, this may lead to seeking pain care being a stressful experience for men.
The gender-pain exaggeration bias we document may have implications for women’s own experiences with pain as well. Though we found that perceivers expected women to exaggerate pain, women in Boring and colleagues’ (2022) examination indicated intentions to downplay pain. It seems plausible that knowledge of societal beliefs about women exaggerating may lead individual women to feel that they should downplay what they are feeling. This would be interesting given that we found that women and men alike expected women would exaggerate pain. The findings of the current work and of Boring and colleagues (2022) in tandem suggest that the gender-pain exaggeration bias documented herein is inaccurate and biased for women and men alike. In this way, the current work implicates several important avenues for understanding how gender expression impacts interpretations of our own and others’ pain.
Limitations
The current work has several limitations worth noting. Though findings of each study are consistent with the theorized gender-pain exaggeration bias, the significance of simple effects was inconsistent. In some studies, perceivers expected men to downplay pain but expectations of women as exaggerating did not achieve statistical significance; in other studies, perceivers expected women to exaggerate pain but expectations of men as downplaying did not achieve statistical significance. One potential explanation for this inconsistency is that we may not have been powered to test simple effects across studies. Another view on this inconsistency is that perhaps a given perceiver holds biased expectations for either men or women but not for both. That is, perhaps some perceivers view women as exaggerating and men as expressing pain accurately, while others view men as downplaying and women as expressing pain accurately. Even if this is the case, viewing men as downplaying and women as expressing pain accurately may have negative consequences for women. Specifically, there are noted disparities and biases in pain that negatively afflict women, and there is reason to believe that beliefs about women may be formed by contrasting women and men. The United States is an androcentric society. Androcentrism, or “the propensity to center society around men and men’s needs, priorities, and values and to relegate women to the periphery” (Bailey et al., 2019), positions men as a gender-neutral standard. This tendency to treat men as a standard may be exacerbated in medical domains where only men were studied in medical research until 30 years ago (Beery, 1995; Merone et al., 2021; Thelwall et al., 2022). Men being the standard of comparison may have consequences for how women are perceived. For example, if men are expected to downplay pain and women are not, men’s pain claims may be viewed as accurate and women’s as overstated.
Further, the current work does not recruit perceivers with expertise in pain (i.e., medical providers). Future work would do well to directly test whether medical providers display a gender-pain exaggeration bias and to assess downstream consequences of this bias in medical environments. There is some evidence that pain-related biases are descriptively weaker among medical providers compared to medical students or lay perceivers who have less pain care experience (e.g., Schäfer et al., 2016; Summers et al., 2021). Thus, health care providers may demonstrate a weaker gender-pain exaggeration bias than lay perceivers. Conversely, medical providers may express similar biases to lay perceivers. Here, some work has found that medical providers and lay perceivers show similar biases in pain expectations (e.g., Summers et al., 2021; Trawalter et al., 2012). Further, medical systems traditionally center men’s experiences and marginalize women’s experiences (Bueter, 2017; Carter, 1994; Merone et al., 2021; Sharma, 2019). There is also qualitative and quantitative evidence that women, relative to men, seeking medical help for pain have worse experiences (Ahlsen et al., 2014; McManimen et al., 2019; Tait et al., 2009; Werner et al., 2004). The gender-pain exaggeration bias documented here may contribute to such examples of women seeking pain care being marginalized and distrusted. However, even if gendered expectations of pain are not as robust among medical providers, the current work suggests that family, friends, coworkers, or employers (especially those who endorse GSE), may judge women as exaggerating their pain. This gender-pain exaggeration bias could have interpersonal (e.g., questioning character), social (e.g., willingness to offer help), or occupational (e.g., amount of paid time off) consequences. Future work would do well to directly explore consequences of viewing women as exaggerating pain more than men.
Further, this work only assessed judgments of White women and men, and thus it is possible that this gender-exaggeration bias may differ in magnitude for or may not generalize to non-White individuals. This limitation is critical because we consistently found that perceivers’ gendered stereotypes about emotional dramatization informed biases in pain expectations; however, some scholars argue that stereotypes of women reflect stereotypes of White women but not women of color (Brescoll, 2016; Collins, 2002; Collins, 2004; Donovan, 2011). For example, Brescoll’s (2016) commentary on gender and emotion noted that “the basic issue of whether Black, Asian American, and Latina women are viewed as more emotional than their male counterparts is largely unknown.” Thus, capturing race-by-gender differences in emotionality stereotypes and pain expectations is needed to understand whether the gender-pain exaggeration bias generalizes to judgments of non-White individuals. The importance of extending the current work in this way is underscored by evidence that women of color often experience substandard pain outcomes (e.g., Bonham 2001; Burgess et al., 2006; Weisse et al., 2003). The current work is also limited in the range of perceiver racial identities represented. Our samples were all majority White American perceivers, consistent with a broader limitation in social psychological science wherein samples are often majority White perceivers (Roberts et al., 2020).
This work is also limited in the scope of target gender identities included and gender bias examined. Specifically, we only consider bias wherein women are disadvantaged relative to men. This focus is not to imply that gender is binary nor that it is unimportant to study expectations of individuals who identify with non-binary gender identities’ pain. Instead, this focus reflects what is presently known about gender disparities in pain – that women’s, relative to men’s, pain is underestimated and undertreated. However, societal understandings of gender and disparities beyond the binary are continually evolving and so too should research on gender-based biases. Indeed, emerging evidence suggests that nonbinary individuals are at a heightened risk to receive inadequate medical care or face discrimination when seeking care (e.g., Liszewski et al., 2018)
Finally, the design of the current work is limited in a few additional ways. In this work, perceivers provided expectations of pain felt before expectations of pain claimed for a given target. Counterbalancing the order in which feel and claim expectations are collected or assessing type of expectation between-subjects would extend the generalizability of this work. Also, in the current work perceivers were instructed that: “Previous research reveals that people report different levels of pain sensitivity. It is possible these differences originate from how much pain people FEEL, but they might also originate from differences in the extent to which people CLAIM pain.” These instructions may have encouraged participants to differentiate between feel and claim more than they otherwise would; however, across studies perceivers differentiated between feel and claim differently for women and men, which was the key effect. Nonetheless, future studies probing expectations of pain felt and claimed would do well to emphasize that a person could claim and feel the same amount of pain, could claim less than they feel, or could claim more than they feel. Though extending the generalizability of the gender-pain exaggeration bias is important, there is reason to believe that this bias would persist across designs and into perceptions of pain expressions. Indeed, Schäfer and colleagues (2016) found that female relative to male patients’ pain expressions were labeled as more exaggerated. Further, there is qualitative evidence that women are vulnerable to having their pain disbelieved (e.g., McManimen et al., 2019) and to being viewed as catastrophizing (e.g., Webster et al., 2023). Thus, there is reason to believe that the bias documented herein may be a culturally persistent bias.
Conclusion
Across four experiments we found evidence for a gender-pain exaggeration bias: women, relative to men, were expected to exaggerate pain more. This bias was statistically mediated by attributions of emotional dramatization traits. Finally, we found that gendered endorsement of emotional dramatization stereotypes for women as a group, compared to men as a group, moderated the strength of this bias. In short, we provide consistent evidence that women are expected to exaggerate pain more and downplay pain less than men. This work may have important implications for how people perceive and respond to others’ pain.
Supplementary Material
Footnotes
Open Practices
The measures, data, and syntax for all studies are available on OSF: https://osf.io/fwcmj/?view_only=778bacbd7bdb4f6e92d0d36cdcc7d370.
We use β to report standardized regression coefficients and b to report unstandardized regression coefficients.
We tested whether perceiver gender moderated the effects of target gender and type of pain expectation in each study, but never found significant moderation; thus, these analyses are available in the Supplementals.
One participant was excluded from age calculations because they reported an impossible age (1989). If they reported the year they were born, the age composition of our sample is largely unchanged (M = 37.97, SD = 10.60).
Target gender with options ‘male’ and female’ is reported in the Chicago Face Database. Given that female and male reflect sex and woman and man reflect gender expression/identity, we use the terms ‘women’ and ‘men.’
The model including an interaction random slope did not converge. In all studies, we tested the maximal model but removed the random interaction slope if that model did not converge.
To address this limitation, we ran Johnson-Neyman tests to test the significance of the slope of target gender on emotional dramatization traits (the a path) and of emotional dramatization traits on expected pain exaggeration (the b path) across GSE. The results of these tests are consistent with the figure below; these tests are in the Supplement.
References
- Ahlsen B, Bondevik H, Mengshoel AM, & Solbrække KN (2014). (Un) doing gender in a rehabilitation context: A narrative analysis of gender and self in stories of chronic muscle pain. Disability and Rehabilitation, 36(5), 359–366. [DOI] [PubMed] [Google Scholar]
- Aronowitz SV, Richmond TS, Compton P, & Jacoby SF (2021). Is It “True” Pain? Pain Treatment Discharge Planning for Seriously Injured Patients. Ethnicity & Disease, 31(1), 139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey AH, LaFrance M, & Dovidio JF (2019). Is man the measure of all things? A social cognitive account of androcentrism. Personality and Social Psychology Review, 23(4), 307–331. [DOI] [PubMed] [Google Scholar]
- Barrett LF, & Bliss-Moreau E (2009). She’s emotional. He’s having a bad day: Attributional explanations for emotion stereotypes. Emotion, 9(5), 649. [DOI] [PubMed] [Google Scholar]
- Bates D, Mächler M, Bolker B, & Walker S (2014). Fitting linear mixed-effects models using lme4. arXiv preprint arXiv:1406.5823 [Google Scholar]
- Bauer NM (2015). Emotional, sensitive, and unfit for office? Gender stereotype activation and support female candidates. Political Psychology, 36(6), 691–708. [Google Scholar]
- Beery TA (1995). Gender bias in the diagnosis and treatment of coronary artery disease. Heart & Lung, 24(6), 427–435. [DOI] [PubMed] [Google Scholar]
- Bertakis KD, Azari R, Helms LJ, Callahan EJ, & Robbins JA (2000). Gender differences in the utilization of health care services. Journal of Family Practice, 49(2), 147–147. [PubMed] [Google Scholar]
- Bonham VL (2001). Race, ethnicity, and pain treatment: Striving to understand the causes and solutions to the disparities in pain treatment. Journal of Law, Medicine & Ethics, 29(1), 52–68. [DOI] [PubMed] [Google Scholar]
- Boring BL, Ng BW, Nanavaty N, & Mathur VA (2022). Over-Rating Pain is overrated: a fundamental self-other Bias in Pain Reporting Behavior. The Journal of Pain, 23(10), 1779–1789. [DOI] [PubMed] [Google Scholar]
- Brescoll VL (2016). Leading with their hearts? How gender stereotypes of emotion lead to biased evaluations of female leaders. The Leadership Quarterly, 27(3), 415–428. [Google Scholar]
- Bueter A (2017). Androcentrism, feminism, and pluralism in medicine. Topoi, 36, 521–530. [Google Scholar]
- Burgess DJ, Van Ryn M, Crowley-Matoka M, & Malat J (2006). Understanding the provider contribution to race/ethnicity disparities in pain treatment: insights from dual process models of stereotyping. Pain Medicine, 7(2), 119–134. [DOI] [PubMed] [Google Scholar]
- Carter H (1994). Confronting patriarchal attitudes in the fight for professional recognition. Journal of Advanced Nursing, 19(2), 367–372. [DOI] [PubMed] [Google Scholar]
- Chalk M, Seitz AR, & Seriès P (2010). Rapidly learned stimulus expectations alter perception of motion. Journal of Vision, 10(8), 2–2. [DOI] [PubMed] [Google Scholar]
- Chen EH, Shofer FS, Dean AJ, Hollander JE, Baxt WG, Robey JL, … & Mills AM (2008). Gender disparity in analgesic treatment of emergency department patients with acute abdominal pain. Academic Emergency Medicine, 15(5), 414–418. [DOI] [PubMed] [Google Scholar]
- Collins PH (2002). Black feminist thought: Knowledge, consciousness, and the politics of empowerment. Routledge. [Google Scholar]
- Collins PH (2004). Black sexual politics: African Americans, gender, and the new racism. Routledge. [DOI] [PubMed] [Google Scholar]
- De Lange FP, Heilbron M, & Kok P (2018). How do expectations shape perception?. Trends in Cognitive Sciences, 22(9), 764–779. [DOI] [PubMed] [Google Scholar]
- Diekman AB, & Eagly AH (2000). Stereotypes as dynamic constructs: Women and men of the past, present, and future. Personality and Social Psychology Bulletin, 26(10), 1171–1188. [Google Scholar]
- Donovan RA (2011). Tough or Tender: (Dis) Similarities in White College Students’ Perceptions of Black and White Women. Psychology of Women Quarterly, 35(3), 458–468. [Google Scholar]
- Drwecki BB, Moore CF, Ward SE, & Prkachin KM (2011). Reducing racial disparities in pain treatment: The role of empathy and perspective-taking. Pain, 152(5), 1001–1006. [DOI] [PubMed] [Google Scholar]
- Fiedler K, Harris C, & Schott M (2018). Unwarranted inferences from statistical mediation tests–An analysis of articles published in 2015. Journal of Experimental Social Psychology, 75, 95–102. [Google Scholar]
- Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, & Riley III JL (2009). Sex, gender, and pain: a review of recent clinical and experimental findings. The Journal of Pain, 10(5), 447–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glick P, & Fiske ST (1997). Hostile and benevolent sexism: Measuring ambivalent sexist attitudes toward women. Psychology of Women Quarterly, 21(1), 119–135. [Google Scholar]
- Glick P, & Fiske ST (2001). Ambivalent sexism. Advances in Experimental Social Psychology, 33, 115–188. [Google Scholar]
- Goh JX, Hall JA, & Rosenthal R (2016). Mini meta‐analysis of your own studies: Some arguments on why and a primer on how. Social and Personality Psychology Compass, 10(10), 535–549. [Google Scholar]
- Green CR, Anderson KO, Baker TA, Campbell LC, Decker S, Fillingim RB, … & Vallerand AH (2003). The unequal burden of pain: confronting racial and ethnic disparities in pain. Pain Medicine, 4(3), 277–294. [DOI] [PubMed] [Google Scholar]
- Green P, & MacLeod CJ (2016). SIMR: An R package for power analysis of generalized linear mixed models by simulation. Methods in Ecology and Evolution, 7(4), 493–498. [Google Scholar]
- Hamberg K (2008). Gender bias in medicine. Women’s Health, 4(3), 237–243. [DOI] [PubMed] [Google Scholar]
- Hess U, Senécal S, Kirouac G, Herrera P, Philippot P, & Kleck RE (2000). Emotional expressivity in men and women: Stereotypes and self-perceptions. Cognition & Emotion, 14(5), 609–642. [Google Scholar]
- Hirsh AT, Hollingshead NA, Bair MJ, Matthias MS, Wu J, & Kroenke K (2013). The influence of patient’s sex, race and depression on clinician pain treatment decisions. European Journal of Pain, 17(10), 1569–1579. [DOI] [PubMed] [Google Scholar]
- Hirsh AT, Hollingshead NA, Ashburn-Nardo L, & Kroenke K (2015). The interaction of patient race, provider bias, and clinical ambiguity on pain management decisions. The Journal of Pain, 16(6), 558–568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoffman KM, & Trawalter S (2016). Assumptions about life hardship and pain perception. Group Processes & Intergroup Relations, 19(4), 493–508. [Google Scholar]
- Hoffman KM, Trawalter S, Axt JR, & Oliver MN (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the National Academy of Sciences, 113(16), 4296–4301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hutson-Comeaux SL, & Kelly JR (2002). Gender stereotypes of emotional reactions: How we judge an emotion as valid. Sex Roles, 47(1), 1–10. [Google Scholar]
- Joynt M, Train MK, Robbins BW, Halterman JS, Caiola E, & Fortuna RJ (2013). The impact of neighborhood socioeconomic status and race on the prescribing of opioids in emergency departments throughout the United States. Journal of General Internal Medicine, 28(12), 1604–1610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klonis SC, Plant EA, & Devine PG (2005). Internal and external motivation to respond without sexism. Personality and Social Psychology Bulletin, 31(9), 1237–1249. [DOI] [PubMed] [Google Scholar]
- Kok P, Brouwer GJ, van Gerven MA, & de Lange FP (2013). Prior expectations bias sensory representations in visual cortex. Journal of Neuroscience, 33(41), 16275–16284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liszewski W, Peebles JK, Yeung H, & Arron S (2018). Persons of nonbinary gender—awareness, visibility, and health disparities. The New England Journal of Medicine, 379(25), 2391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litman L, Robinson J, & Abberbock T (2017). TurkPrime. com: A versatile crowdsourcing data acquisition platform for the behavioral sciences. Behavior Research Methods, 49(2), 433–442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lloyd EP, Paganini GA, & ten Brinke L (2020). Gender stereotypes explain disparities in pain care and inform equitable policies. Policy Insights from the Behavioral and Brain Sciences, 7(2), 198–204. [Google Scholar]
- Lord B, Cui J, & Kelly AM (2009). The impact of patient sex on paramedic pain management in the prehospital setting. The American Journal of Emergency Medicine, 27(5), 525–529. [DOI] [PubMed] [Google Scholar]
- Ma DS, Correll J, & Wittenbrink B (2015). The Chicago face database: A free stimulus set of faces and norming data. Behavior Research Methods, 47(4), 1122–1135. [DOI] [PubMed] [Google Scholar]
- McCormick KT, MacArthur HJ, Shields SA, & Dicicco EC (2016). New perspectives on gender and emotion. In Feminist Perspectives on Building a Better Psychological Science of Gender, 213–230. [Google Scholar]
- McManimen S, McClellan D, Stoothoff J, Gleason K, & Jason LA (2019). Dismissing chronic illness: A qualitative analysis of negative health care experiences. Health Care for Women International, 40(3), 241–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McShane BB, & Böckenholt U (2017). Single-paper meta-analysis: Benefits for study summary, theory testing, and replicability. Journal of Consumer Research, 43(6), 1048–1063. [Google Scholar]
- Mende-Siedlecki P, Qu-Lee J, Backer R, & Van Bavel JJ (2019). Perceptual contributions to racial bias in pain recognition. Journal of Experimental Psychology: General, 148(5), 863. [DOI] [PubMed] [Google Scholar]
- Merone L, Tsey K, Russell D, & Nagle C (2021). Sex and gender gaps in medicine and the androcentric history of medical research. Australian and New Zealand Journal of Public Health, 45(5), 424–426. [DOI] [PubMed] [Google Scholar]
- Owens G (2008). Gender differences in health care expenditures, resource utilization, and quality of care. Journal of Managed Care Pharmacy, 14(3), 2–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinkhasov RM, Wong J, Kashanian J, Lee M, Samadi DB, Pinkhasov MM, & Shabsigh R (2010). Are men shortchanged on health? Perspective on health care utilization and health risk behavior in men and women in the United States. International Journal of Clinical Practice, 64(4), 475–487. [DOI] [PubMed] [Google Scholar]
- Prkachin KM, Solomon PE, & Ross J (2007). Underestimation of pain by health-care providers: towards a model of the process of inferring pain in others. Canadian Journal of Nursing Research Archive, 88–106. [PubMed] [Google Scholar]
- Pronina I, & Rule NO (2014). Inducing bias modulates sensitivity to nonverbal cues of others’ pain. European Journal of Pain, 18(10), 1452–1457. [DOI] [PubMed] [Google Scholar]
- Roberts SO, Bareket-Shavit C, Dollins FA, Goldie PD, & Mortenson E (2020). Racial inequality in psychological research: Trends of the past and recommendations for the future. Perspectives on Psychological Science, 15(6), 1295–1309. [DOI] [PubMed] [Google Scholar]
- Samulowitz A, Gremyr I, Eriksson E, & Hensing G (2018). “Brave men” and “emotional women”: A theory-guided literature review on gender bias in health care and gendered norms towards patients with chronic pain. Pain Research and Management, 1–14. 10.1155/2018/6358624 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schäfer G, Prkachin KM, Kaseweter KA, & de C Williams AC (2016). Health care providers’ judgments in chronic pain: the influence of gender and trustworthiness. Pain, 157(8), 1618–1625. [DOI] [PubMed] [Google Scholar]
- Schulman KA, Berlin JA, Harless W, Kerner JF, Sistrunk S, Gersh BJ, … & Escarce JJ (1999). The effect of race and sex on physicians’ recommendations for cardiac catheterization. New England Journal of Medicine, 340(8), 618–626. [DOI] [PubMed] [Google Scholar]
- Sharma M (2019). Applying feminist theory to medical education. The Lancet, 393(10171), 570–578. [DOI] [PubMed] [Google Scholar]
- Shields SA (2002). Speaking from the heart: Gender and the social meaning of emotion. Cambridge University Press. [Google Scholar]
- Shields SA (2013). Gender and emotion: What we think we know, what we need to know, and why it matters. Psychology of Women Quarterly, 37(4), 423–435. [Google Scholar]
- Summers KM, Deska JC, Almaraz SM, Hugenberg K, & Lloyd EP (2021). Poverty and pain: Low-SES people are believed to be insensitive to pain. Journal of Experimental Social Psychology, 95. [Google Scholar]
- Summers KM, Paganini GA, & Lloyd EP (2023). Poor toddlers feel less pain? Application of class-based pain stereotypes in judgments of children. Social Psychological and Personality Science, 14(2), 130–140. [Google Scholar]
- Summers KM, Weesner RE, Hugenberg K, & Lloyd EP (2023). Group-based pain tolerance stereotypes and their accuracy. Manuscript in Preparation. [Google Scholar]
- Tait RC, Chibnall JT, & Kalauokalani D (2009). Provider judgments of patients in pain: seeking symptom certainty. Pain Medicine, 10(1), 11–34. [DOI] [PubMed] [Google Scholar]
- Thelwall M, Abdullah A, & Fairclough R (2022). Researching women and men 1996–2020: Is androcentrism still dominant?. Quantitative Science Studies, 3(1), 244–264. [Google Scholar]
- Tingley D, Yamamoto T, Hirose K, Keele L, & Imai K (2014). Mediation: R package for causal mediation analysis.
- Trawalter S, Hoffman KM, & Waytz A (2012). Racial bias in perceptions of others’ pain. PloS One, 7(11). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Viki GT, & Abrams D (2003). Infra-humanization: Ambivalent sexism and the attribution of primary and secondary emotions to women. Journal of Experimental Social Psychology, 39(5), 492–499. [Google Scholar]
- Wandner LD, Scipio CD, Hirsh AT, Torres CA, & Robinson ME (2012). The perception of pain in others: how gender, race, and age influence pain expectations. The Journal of Pain, 13(3), 220–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waytz A, Hoffman KM, & Trawalter S (2015). A superhumanization bias in Whites’ perceptions of Blacks. Social Psychological and Personality Science, 6(3), 352–359. [Google Scholar]
- Webster F, Connoy L, Longo R, Ahuja D, Amtmann D, Anderson A, … & Darnall BD (2023). Patient Responses to the Term Pain Catastrophizing: Thematic Analysis of Cross-sectional International Data. The Journal of Pain, 24(2), 356–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss AJ, Wier LM, Stocks C, & Blanchard J (2014). Overview of Emergency Department Visits in the United States, 2011: Statistical Brief #174. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. [Google Scholar]
- Weisse CS, Sorum PC, & Dominguez RE (2003). The influence of gender and race on physicians’ pain management decisions. The Journal of Pain, 4(9), 505–510. [DOI] [PubMed] [Google Scholar]
- Werner A, Isaksen LW, & Malterud K (2004). ‘I am not the kind of woman who complains of everything’: Illness stories on self and shame in women with chronic pain. Social Science & Medicine, 59(5), 1035–1045. [DOI] [PubMed] [Google Scholar]
- Wise EA, Price DD, Myers CD, Heft MW, & Robinson ME (2002). Gender role expectations of pain: relationship to experimental pain perception. Pain, 96(3), 335–342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zelaya CE, Dahlhamer JM, Lucas JW, & Connor EM (2020). Chronic pain and high-impact chronic pain among US adults, 2019. NCHS Data Brief, 390, 1–8. [PubMed] [Google Scholar]
- Zhang L, Losin EAR, Ashar YK, Koban L, & Wager TD (2021). Gender biases in estimation of others’ pain. The Journal of Pain, 22(9), 1048–1059. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.