

Abstract
Question
The aim of this systematic review is twofold: (1) to characterise the purpose and description of available social anxiety apps and (2) to review the evidence on the effectiveness of social anxiety apps.
Study selection and analysis
A search was conducted on three major mobile platforms: Apple iTunes, Google Play and Windows Store. Apps were included if they addressed social anxiety and used an English language interface. A systematic review of the literature from MEDLINE, EMBASE, PsycINFO, Cochrane, Scopus and Web of Science to identify evidence-based evaluations of social anxiety apps was also undertaken.
Findings
Of the 1154 apps identified, 38 apps met the inclusion criteria: iTunes (n=18), Google Play (n=16) and Windows Store (n=4). Over 60% of apps were exclusively focused on social anxiety, while the remainder targeted social anxiety and related conditions. Most developers did not provide information on their organisational affiliations or their content source. Most apps used multimedia while 17 apps used text only. Finally, although the systematic review of the literature identified 94 articles, none of which met inclusion criteria.
Conclusions
Social anxiety apps have the potential to overcome barriers to accessing treatment; however, none of the apps identified have had studies on their effectiveness published. As the evidence base is lacking, it is therefore not currently possible to recommend their use.
Keywords: smartphone application, mobile, apps, social anxiety, phobia
Background
Social anxiety disorder is characterised by chronic fear and avoidance of social engagement, scrutiny by others and social withdrawal to avoid feelings of embarrassment and humiliation.1 It is highly prevalent and associated with major personal, social and economic burden.1–3 Although epidemiological studies on social anxiety have reported varying prevalence, one recent systematic review found that the global prevalence rate (after adjusting for methodological differences) is approximately 7.3%.4
While effective treatments for social anxiety including cognitive–behavioural therapy (CBT) are available, and show large effect sizes5 6 they are underused.7 Several studies have also investigated the barriers to accessing treatment for social anxiety and found a number of contributors including low mental health literacy,8 geographical restrictions, financial cost, lack of awareness of existing and effective treatment options, health system capacity and fear of stigma.9–11 In a 2010 study, 63.9% of respondents reported concerns about financial cost as the main barrier to seeking treatment, followed by uncertainty of where to seek help (63.2%), and long appointment waitlists (52.1%).10
Non-traditional methods of treatment delivery such as mobile applications (apps) can widen the reach of mental health services12–14 and address barriers to treatment. Indeed, by 2012 more than 31% of all health apps available on the Apple iTunes Store were categorised as mental health and healthy eating apps15 and is likely to have increased since then. Several of these apps are designed to address anxiety and their purpose may range from symptom monitoring and psychoeducation through to assessment and management. Ideally, apps should be evidence based, incorporate appropriate therapies such as CBT, provide validated mental health information, have utility for real-time engagement/gamification/reminders, and easily found and accessed.16 However, due to the lack of empirical evidence, the effectiveness of many apps is questionable.17
Apps for a variety of mental health disorders/medical conditions such as depression,18 schizophrenia,19 bipolar affective disorder,20 cancer21 and diabetes22 have been previously reviewed. However, no review of social anxiety apps has been undertaken previously.
Objectives
The objectives of this study were to characterise the purpose and description of available social anxiety apps. This was also complemented by a systematic review of the literature to identify any previous evaluations of social anxiety apps. We asked the following questions:
What social anxiety apps are currently available to mobile (iOS, Android, Windows) users?
What are the characteristics of these apps in terms of information provided about their development (developer affiliations/content source/evidence-based/theory-driven/trials to assess effectiveness/free to use/in-app purchases)?
What are the main purposes of social anxiety apps (education/screening/monitoring/diagnosis/treatment/support/multipurpose)?
Study selection and analysis
Overview
We developed a systematic search strategy with the aim of identifying all relevant social anxiety apps and effectiveness studies. We undertook a systematic review based on methodology used in previous work,12 18 21 to guide both the identification and characterisation of social anxiety apps found on various mobile platforms. We also assessed the empirical evidence of the effectiveness of social anxiety apps in the literature.
Mobile application search
In June 2016, we carried out a search of the three main app platforms: Apple (iTunes), Android (Google Play) and Windows (Windows Store). We searched across all store categories, rather than restricting to a specific category. However, our search was limited to those apps that had any of the keywords below in the title or app description. Two authors (BG, HA) conducted the search independently for all app stores, and data were extracted from app descriptions available. Disagreement on eligibility was resolved by iterative discussion and consensus.
Selection criteria
Identified apps were categorised as either ‘potentially relevant’ or ‘not relevant’ according to the app title and store description. Apps were included if they satisfied five inclusion criteria:1 the keywords ‘social anxiety’, ‘social phobia’, ‘phobia’ or ‘shyness’ in the title or app description2 explicitly specified the purpose was education/symptom monitoring assessment/management/support/therapy or a combination of these3 a focus on social anxiety or that social anxiety was one of the main aspects of app content4 used an English language interface; and5 were not in electronic book format. Apps were excluded if they did not provide sufficient information, had no clear focus on social anxiety, included the keywords in an unrelated context (eg, specific phobias or purely entertainment games) or were duplicates within the same store, but not between stores.
Data extraction and coding
We extracted and coded information from the store description of the identified apps for several variables, based on18 21 and we also collected information on additional variables:
Platform (iTunes, Google Play or Windows Store)
Device (phone only, tablet only, phone and tablet, or universal)
Developer, affiliation (medical institution, non-profit institution or insufficient information)
Release date
Cost (US$)
Target audience (people with social anxiety, laypersons, students, health professionals)
Target age group (4+, 9+, 18+ and all)
Content focus (social anxiety only, or social anxiety plus others)
Content source (expert, external, lived experience or insufficient information)
Main purpose (multipurpose, psychoeducation, assessment, symptom monitoring, symptom management, supportive resources, treatment)
Media type (text, audio, text and audio, text and visual)
Literature search on the effectiveness of social anxiety apps
Overview
We conducted a literature search during June 2016, using six databases, including MEDLINE, EMBASE, PsycINFO, Cochrane, Scopus and Web of Science. We used combinations of the search terms including social phobia or social anxiety or phobia or social anxiety disorders, app store, mobile app, Google Play, Android, iPhone, Windows phone, smartphone, mobile application. This search was also supplemented with a manual search through the identified articles’ bibliography. Two of the authors (BG, HA) independently reviewed the titles and abstracts to identify eligible studies. If deemed potentially relevant, the full text of the article was retrieved.
Selection criteria
Articles were considered potentially relevant if they provided an evaluation of mobile apps for social anxiety, included empirical evidence on the effectiveness of social anxiety apps, and were in English. We excluded articles that evaluated apps for specific phobias and articles that only provided study protocols for future research.
Data extraction and coding
Eligible articles were reviewed by two authors (BG, HA) independently. Only one author (BG) extracted information via a preprepared data extraction tool following PRISMA guidelines.23 Extracted data included year of publication, funding sources, demographic characteristics of participants, condition, characteristics of the app used (eg, purpose, developer and affiliation), study design, results and biases.
Findings
General characteristics
The initial search of the three app stores yielded a total of 1154 apps (see figure 1) potentially relevant to social anxiety (iTunes=212 apps, Google Play=913 apps and Windows Store=29 apps). After screening, 73 apps were relevant to social anxiety but 35 apps were duplicates and hence excluded. Duplicates were excluded within each store but not between stores, because the same apps in different stores may have different content or functionality and so are considered different apps for the purpose of this study and this approach would be consistent with previously published work.24 Overall, 38 apps met the inclusion criteria from the following platforms: iTunes (n=18), Google Play (n=16) and Windows Store (n=4). Figure 2 shows the distribution of social anxiety apps across the mobile platforms.
Figure 1.
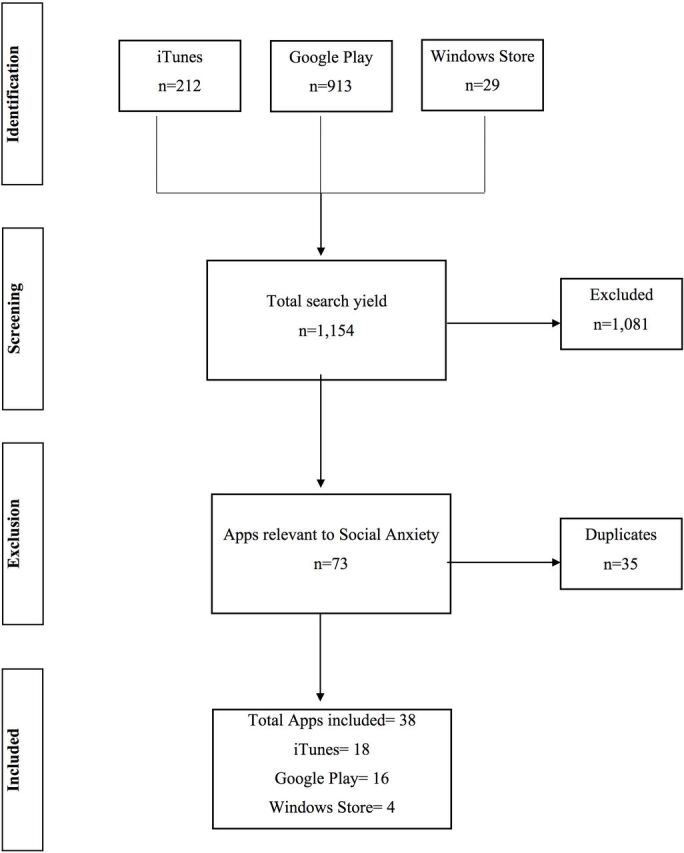
Flow diagram illustrating the exclusion of apps at various stages of the study.
Figure 2.

Distribution of social anxiety apps across the three mobile platforms.
Release dates were available for 34 apps. iTunes apps reported the earliest release date (2009), with the majority being released between 2014 and 2016. Release dates for apps on Google Play ranged between 2011 and 2016, with the majority being released in the last 2 years. However, apps on the Windows Store did not report this information.
Most apps were free to download (n=20). iTunes provided 8 apps for free, and 10 were paid ($1.09–$5.45). Similarly, Google Play had 10 apps free of charge, and 6 were at a cost ranging from $2.18 to $4.64. Windows Store offered two free apps and two paid apps, which were the most expensive of all at $5.45 and $5.79.
Consistent with the literature,21 the majority of developers did not provide information on their organisational affiliations (35/38, 92.1%). Of those that indicated their affiliations, two apps were affiliated with non-profit institutions, and only one paid app was associated with a medical institution (Mayo Clinic).
Purpose of social anxiety apps
As shown in figure 3, more than a third of the apps reported their main purpose as psychoeducation (13/38, 34.2%), symptom management (5/38, 13.16%), treatment (4/38, 10.52%), self-assessment (3/38, 7.89%) and supportive resources (3/38, 7.89%). Multipurpose apps accounted for 26.3% (10/38) of the sample. Furthermore, over 60% of the apps (23/38) were exclusively focused on social anxiety, while the remainder of apps (15/38, 39.5%) focused on social anxiety and other related conditions. Over 65% of the apps did not report their content source, and of those that reported this information in sufficient detail, 23.7% cited as expert and 5.3% as external sources. Most apps used a multimedia format, while 17 apps (44.7%) used text only to deliver content.
Figure 3.

Distribution of social anxiety apps by main purpose.
Over 94.7% (36/38) of apps were targeting the public and only two apps were directed at healthcare professionals. With regard to the target age group, only five apps (13.2%) were unrated, and the remaining were rated as suitable for individuals aged 3+. In addition, about a third of the apps could be downloaded and installed on either smartphones or tablets, 23.7% phone only and the remainder were universal. Table 1 summarises the characteristics of the apps. See online supplementary appendix A for a complete list of included apps.
Table 1.
App characteristics and purpose
| Variable | Main purpose (n) | ||||||
| TT | PE | SA | SM | SR | MP | Total (n) | |
| Overall | 4 | 13 | 3 | 5 | 3 | 10 | 38 |
| Developer affiliation | |||||||
| Medical institution | 1 | 1 | |||||
| Other institutions (non-profit) | 2 | 2 | |||||
| Insufficient info | 4 | 13 | 3 | 5 | 3 | 7 | 35 |
| Content source | |||||||
| Expert | 1 | 8 | 9 | ||||
| External | 1 | 1 | 2 | ||||
| Lived experience | 2 | 2 | |||||
| Insufficient info | 4 | 11 | 3 | 3 | 3 | 1 | 25 |
| Media type | |||||||
| Text only | 1 | 8 | 2 | 2 | 2 | 2 | 17 |
| Audio only | 3 | 1 | 1 | 5 | |||
| Text and audio | 3 | 2 | 5 | ||||
| Text and visual | 2 | 1 | 2 | 1 | 5 | 11 | |
| Platform | |||||||
| Phone only | 1 | 5 | 1 | 2 | 9 | ||
| Phone and tablet | 6 | 2 | 5 | 13 | |||
| Universal | 3 | 2 | 1 | 5 | 2 | 3 | 16 |
| Content focus | |||||||
| Social phobia only | 4 | 7 | 2 | 3 | 1 | 6 | 23 |
| Social phobia plus others | 6 | 1 | 2 | 2 | 4 | 15 | |
MP, multiple purposes; PE, psychoeducation; SA, self-assessment; SM, symptom management; SR, supportive resources; TT, therapeutic treatment.
ebmental-20-65-DC1-inline-supplementary-material-1.docx (109.9KB, docx)
Characterisation of apps by purpose
Therapeutic treatment (four apps)
Therapeutic treatment apps mainly used audio (3/4, 75%) to deliver content, which accounted for the majority of audio apps found in the sample. The content of these apps was primarily in the form of hypnosis. One app provided treatment content via text only, in the form of social challenges. All these apps were exclusively focused on social anxiety, and all reported insufficient information on content source.
Psychoeducation (13 apps)
Psychoeducation apps mostly used text only (8/13, 61.5%), accounting for about half of all text apps in the sample, followed by multimedia format to deliver educational content about social anxiety (5/13, 38.5%). One app provided an audio HypnoSleep tool, which reads out information to the individual. The content included information on definition, symptoms, causes and ways to overcome social anxiety. Most apps did not include sufficient information about content source (11/13, 84.6%), but were available for both smartphones and tablets. Also, while more than half of these psychoeducational apps were social anxiety focused (7/13, 53.8%), accounting for about a third of all apps included in this study, six apps focused on social anxiety plus other conditions (6/13, 46.2%).
Self-assessment (three apps)
None of the self-assessment apps provided enough information on their content source. Despite this, two apps were targeted at health professionals. Two apps used text only media and one app used multimedia format. Two apps were exclusively focused on social anxiety, though did not indicate what type of assessment methods/tools were used, and one app included social anxiety among other conditions such as depression, panic attacks, mania and psychosis. Based on available app description, this app used the Social Phobia Inventory for assessment.25 All three apps were designed for both phones and tablets.
Symptom management (five apps)
Three apps (3/5, 60%) did not provide enough information on their content source, which accounted for 12% of the entire sample. One app reported that the content source was external and one expert. Two apps used multimedia, two used text only and one app used audio only. Three apps were social anxiety specific, while two apps included other conditions. Furthermore, symptom management techniques ranged from asking users to perform social challenges, deep muscle relaxation, breathing exercises and cognitive bias modification (CBM) techniques which provide training in ignoring negative stimuli. Only two apps allowed users to rate their anxiety levels at different time points and track their progress. All five apps were compatible with smartphones and tablets.
Supportive resources (three apps)
None of the supportive resource apps identified the source of their contents. Two apps were text only, while one app used multimedia. Only one app was social anxiety specific. All apps provided online support resources (user chatrooms and social networking).
Multipurpose (10 apps)
This category included the only app that was affiliated with a medical institution (Mayo Clinic). The majority (90%) of these apps reported the source of content, with almost all citing an expert (80%) or external (10%) source. Similarly, the majority also used multimedia (n=7), text only (n=2) and audio only (n=1) format. More than half of these apps (60%) focused solely on social anxiety, while four apps included other conditions. All apps provided multiple functions (a combination of assessment, management and treatment). Eighty per cent specifically focused on CBT. Most apps were compatible with smartphone devices and tablets, with only two apps suitable only for smartphones.
Evaluation of the effectiveness of apps
The literature search yielded 84 articles in total: Medline (12), Embase (34), PsycInfo (15), Cochrane (0), Scopus (12), Web of Science (10) and manual search (1). After independent review of titles and abstracts, 10 articles were retained. Five duplicate articles were excluded. Further analysis eliminated the remaining five articles as they evaluated apps for specific phobia, or did not provide original data, rather they were study protocols and guidelines for future research in this area, or assessed smartphone-delivered interventions but not social anxiety stand-alone apps. However, we found two smartphone-delivered interventions for social anxiety: (1) a mobile-based CBT (mCBT) and a mobile-based interpersonal psychotherapy,26 which the authors found to be effective, but the mCBT demonstrated more lasting positive effects, and (2) a smartphone-based CBM for attention, which was found to be as effective as dot-probe attention bias training.27 Of note, none of the apps included in this study provided any form of evaluation or empirical evidence in their available app descriptions.
Conclusions
This systematic review was the first to characterise the purpose and content description of available social anxiety-focused apps across all main platforms, and to review the evidence base for apps that are currently available. In total, 38 apps were identified as specifically targeting social anxiety. Over 60% of the identified apps were exclusively focused on social anxiety, while the remainder did not solely focus on social anxiety. The purpose of most apps was a combination of some of the following: psychoeducation; symptom management; treatment; self-assessment; or supportive resources. Furthermore, most of the apps neither reported their organisational affiliation nor their content source. More than half of apps used multimedia and approximately half used text only media. Lastly, the systematic review of the literature found a lack of empirical evaluation of social anxiety mobile apps and none of the apps identified in the current study have had evaluation of their effectiveness published.
This study confirms the growing number of mobile apps that are readily accessible.16 18–20 28–30 Included apps were available across the three main mobile platforms, which is unsurprising given the popularity of these platforms. Compared with previous studies31–33 that have restricted their search to one platform, our search strategy enabled a wider evaluation of the major platforms for downloading apps. However, despite a significant increase in the number of health-based apps over recent years, where studies have found apps for a variety of clinical conditions, for example, 295 for cancer;21 243 for depression;18 259 for stress management,34 social anxiety focused apps are still relatively uncommon.
Targeting social anxiety through a mobile platform may help increase access to quality mental healthcare and overcome treatment barriers. This is especially true for conditions such as social anxiety that hinder people from seeking help/accessing services due to several reasons as outlined earlier.9–11 However, apps have their limitations. For example, providing information alone is well recognised to be inaequate when aiming for behaviour change.35 Therefore, apps should also aim to incorporate evidence-based treatment options such as CBT33 36 37 and support self-management skills necessary to translate that knowledge into effective practice.21 The main form of treatment we encountered in the current study was hypnosis whereby the evidence base is less robust and similar research has found that smoking cessation apps often did not adhere to evidence-based practices.29 31 38
Furthermore, absence of evidence on effectiveness and insufficient information of developers’ affiliations are concerning. Previous reviews of health apps have also highlighted these concerns21 31 32 38 39 and discrepancies between information provided in the app and official guidelines.22 31 Additionally, previous work has found that apps targeting healthcare consumers had less valid information than those designed for healthcare professionals (32% vs 96%).32 The findings from our study confirm this whereby of all included apps, only three apps reported their affiliations.
Finally, developers should adhere to evidence-based guidelines and involve users in the development process as has been done in previous work.40 Including users in the development of apps is important41 and has proven successful.42 A study of mental health service users in Ireland43 found that all participants were interested in participating in app design and may help with usability and the overall therapeutic benefit of such apps. With regard to design and development processes, guidelines have also emerged to aid future developers including Bakker's and colleagues recommendations,16 the Purple guideline44 and the Mobile App Rating Scale.45 These guidelines will also help developers in reporting their app features, content and provide relevant attribution to content providers.
Strengths and limitations
The main strength of our approach is that our search covered the three main mobile app platforms and were independently searched by two reviewers. We adopted a search strategy that is already published.18 21 23 However, our study also had limitations. Our search was restricted to app description, rather than physically downloading and testing apps whereby some apps may have contained this missing information within the app itself. As a result, we found that a considerable number of apps failed to disclose their organisational affiliations and content source. Second, it is possible that many of the apps we excluded that were not specific to social anxiety could be valuable for people with the disorder. Social anxiety has high comorbidity with other mental health conditions such as depression and panic disorder.46 47 Apps for these disorders may also be useful. Future research should also test the functionality or usability of the apps we included in this study.
Clinical implications
As with other mental health disorders, social anxiety apps have the potential to overcome barriers to accessing treatment; however, given the small number of apps specifically targeting social anxiety and none with a robust evidence base, finding the appropriate app may prove to be challenging. It is important that researchers consider all platforms when reviewing apps. This study also highlighted the need for standardised reporting and the need for evidence-based evaluations of apps. Future research should focus on evaluating the utility and effectiveness of social anxiety-specific apps.
Footnotes
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Correction notice: This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected these errors and the correct publishers have been inserted into the references.
References
- 1. Bruce LC, Heimberg RG. Social anxiety disorder. New York: John Wiley & Sons, Ltd, 2013. [Google Scholar]
- 2. Stein MB, Stein DJ. Social anxiety disorder. The Lancet 2008;371:1115–25. 10.1016/S0140-6736(08)60488-2 [DOI] [PubMed] [Google Scholar]
- 3. Smit F, Cuijpers P, Oostenbrink J, et al. Costs of nine common mental disorders: implications for curative and preventive psychiatry. J Ment Health Policy Econ 2006;9:193–200. [PubMed] [Google Scholar]
- 4. Baxter AJ, Scott KM, Vos T, et al. Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychol Med 2013;43:897–910. 10.1017/S003329171200147X [DOI] [PubMed] [Google Scholar]
- 5. Ponniah K, Hollon SD. Empirically supported psychological interventions for social phobia in adults: a qualitative review of randomized controlled trials. Psychol Med 2008;38:3–14. 10.1017/S0033291707000918 [DOI] [PubMed] [Google Scholar]
- 6. Mayo-Wilson E, Dias S, Mavranezouli I, et al. Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis. Lancet Psychiatry 2014;1:368–76. 10.1016/S2215-0366(14)70329-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Wang PS, Berglund P, Olfson M, et al. Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey replication. Arch Gen Psychiatry 2005;62:603. 10.1001/archpsyc.62.6.603 [DOI] [PubMed] [Google Scholar]
- 8. Coles ME, Coleman SL. Barriers to treatment seeking for anxiety disorders: initial data on the role of mental health literacy. Depress Anxiety 2010;27:63–71. 10.1002/da.20620 [DOI] [PubMed] [Google Scholar]
- 9. Olfson M, Guardino M, Struening E, et al. Barriers to the treatment of social anxiety. Am J Psychiatry 2000;157:521–7. 10.1176/appi.ajp.157.4.521 [DOI] [PubMed] [Google Scholar]
- 10. Chartier-Otis M, Perreault M, Bélanger C. Determinants of barriers to treatment for anxiety disorders. Psychiatr Q 2010;81:127–38. 10.1007/s11126-010-9123-5 [DOI] [PubMed] [Google Scholar]
- 11. Titov N, Andrews G, Schwencke G, et al. Shyness 1: distance treatment of social phobia over the internet. Aust N Z J Psychiatry 2008;42:585–94. 10.1080/00048670802119762 [DOI] [PubMed] [Google Scholar]
- 12. Mohr DC, Burns MN, Schueller SM, et al. Behavioral intervention technologies: evidence review and recommendations for future research in mental health. Gen Hosp Psychiatry 2013;35:332–8. 10.1016/j.genhosppsych.2013.03.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Donker T, Petrie K, Proudfoot J, et al. Smartphones for smarter delivery of mental health programs: a systematic review. J Med Internet Res 2013;15:e247. 10.2196/jmir.2791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Zhao J, Freeman B, Li M. Can mobile phone apps influence people's health behavior change? an evidence review. J Med Internet Res 2016;18:e287. 10.2196/jmir.5692 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. West JH, Hall PC, Hanson CL, et al. There's an app for that: content analysis of paid health and fitness apps. J Med Internet Res 2012;14:e72. 10.2196/jmir.1977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bakker D, Kazantzis N, Rickwood D, et al. Mental health smartphone apps: review and evidence-based recommendations for future developments. JMIR Ment Health 2016;3:e7. 10.2196/mental.4984 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Steinhubl SR, Muse ED, Topol EJ. Can mobile health technologies transform health care? JAMA 2013;310:2395–6. 10.1001/jama.2013.281078 [DOI] [PubMed] [Google Scholar]
- 18. Shen N, Levitan MJ, Johnson A, et al. Finding a depression app: a review and content analysis of the depression app marketplace. JMIR Mhealth Uhealth 2015;3:e16. 10.2196/mhealth.3713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Firth J, Torous J. Smartphone Apps for Schizophrenia: a Systematic Review. JMIR Mhealth Uhealth 2015;3:e102. 10.2196/mhealth.4930 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Nicholas J, Larsen ME, Proudfoot J, et al. Mobile Apps for bipolar disorder: a systematic review of features and content quality. J Med Internet Res 2015;17:e198. 10.2196/jmir.4581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Bender JL, Yue RY, To MJ, et al. A lot of action, but not in the right direction: systematic review and content analysis of smartphone applications for the prevention, detection, and management of cancer. J Med Internet Res 2013;15:e287. 10.2196/jmir.2661 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Chomutare T, Fernandez-Luque L, Arsand E, et al. Features of mobile diabetes applications: review of the literature and analysis of current applications compared against evidence-based guidelines. J Med Internet Res 2011;13:e65. 10.2196/jmir.1874 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336–41. 10.1016/j.ijsu.2010.02.007 [DOI] [PubMed] [Google Scholar]
- 24. Martínez-Pérez B, de la Torre-Díez I, López-Coronado M, et al. Mobile apps in cardiology: review. JMIR Mhealth Uhealth 2013;1:e15. 10.2196/mhealth.2737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Connor KM, Davidson JR, Churchill LE, et al. Psychometric properties of the Social Phobia Inventory (SPIN). New self-rating scale. Br J Psychiatry 2000;176:379–86. 10.1192/bjp.176.4.379 [DOI] [PubMed] [Google Scholar]
- 26. Dagöö J, Asplund RP, Bsenko HA, et al. Cognitive behavior therapy versus interpersonal psychotherapy for social anxiety disorder delivered via smartphone and computer: a randomized controlled trial. J Anxiety Disord 2014;28:410–7. 10.1016/j.janxdis.2014.02.003 [DOI] [PubMed] [Google Scholar]
- 27. Enock PM, Hofmann SG, McNally RJ. Attention bias modification training via smartphone to reduce social anxiety: a randomized, controlled multi-session experiment. Cognit Ther Res 2014;38:200–16. 10.1007/s10608-014-9606-z [DOI] [Google Scholar]
- 28. Bardus M, van Beurden SB, Smith JR, et al. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial apps for weight management. Int J Behav Nutr Phys Act 2016;13:35. 10.1186/s12966-016-0359-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Powell AC, Torous J, Chan S, et al. Interrater Reliability of mHealth App Rating Measures: Analysis of Top Depression and Smoking Cessation Apps. JMIR Mhealth Uhealth 2016;4:e15. 10.2196/mhealth.5176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Chen J, Lieffers J, Bauman A, et al. The use of smartphone health apps and other mobile health (mHealth) technologies in dietetic practice: a three country study. J Hum Nutr Diet 2017. (Epub ahead of print: 24 Jan 2017). 10.1111/jhn.12446 [DOI] [PubMed] [Google Scholar]
- 31. Abroms LC, Padmanabhan N, Thaweethai L, et al. iPhone apps for smoking cessation: a content analysis. Am J Prev Med 2011;40:279–85. 10.1016/j.amepre.2010.10.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Pandey A, Hasan S, Dubey D, et al. Smartphone apps as a source of cancer information: changing trends in health information-seeking behavior. J Cancer Educ 2013;28:138–42. 10.1007/s13187-012-0446-9 [DOI] [PubMed] [Google Scholar]
- 33. Kertz SJ, Kelly JM, Stevens KT, et al. A review of free iPhone applications designed to target anxiety and worry. J Technol Behav Sci 2017:1–10. [Google Scholar]
- 34. Payne HE, Wilkinson J, West JH, et al. A content analysis of precede-proceed constructs in stress management mobile apps. Mhealth 2016;2:5. 10.3978/j.issn.2306-9740.2016.02.02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Bodenheimer T, Lorig K, Holman H, et al. Patient self-management of chronic disease in primary care. JAMA 2002;288:2469–75. 10.1001/jama.288.19.2469 [DOI] [PubMed] [Google Scholar]
- 36. Sama PR, Eapen ZJ, Weinfurt KP, et al. An evaluation of mobile health application tools. JMIR Mhealth Uhealth 2014;2:e19. 10.2196/mhealth.3088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Harrison AM, Goozee R. Psych-related iPhone apps. J Ment Health 2014;23:48–50. 10.3109/09638237.2013.869575 [DOI] [PubMed] [Google Scholar]
- 38. Choi J, Noh GY, Park DJ. Smoking cessation apps for smartphones: content analysis with the self-determination theory. J Med Internet Res 2014;16:e44. 10.2196/jmir.3061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Wolf JA, Moreau JF, Akilov O, et al. Diagnostic inaccuracy of smartphone applications for melanoma detection. JAMA Dermatol 2013;149:422–6. 10.1001/jamadermatol.2013.2382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Sundram F, Hawken SJ, Stasiak K, et al. Tips and Traps: lessons from codesigning a clinician E-Monitoring Tool for Computerized Cognitive Behavioral therapy. JMIR Ment Health 2017;4:e3. 10.2196/mental.5878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Ben-Zeev D, Kaiser SM, Brenner CJ, et al. Development and usability testing of FOCUS: a smartphone system for self-management of schizophrenia. Psychiatr Rehabil J 2013;36:289–96. 10.1037/prj0000019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Ennis L, Robotham D, Denis M, et al. Collaborative development of an electronic personal health record for people with severe and enduring mental health problems. BMC Psychiatry 2014;14:305. 10.1186/s12888-014-0305-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Goodwin J, Cummins J, Behan L, et al. Development of a mental health smartphone app: perspectives of mental health service users. J Ment Health 2016;25:434–40. 10.3109/09638237.2015.1124392 [DOI] [PubMed] [Google Scholar]
- 44. Schueller SM, Begale M, Penedo FJ, et al. Purple: a modular system for developing and deploying behavioral intervention technologies. J Med Internet Res 2014;16:e181. 10.2196/jmir.3376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Stoyanov SR, Hides L, Kavanagh DJ, et al. Mobile app rating scale: a new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth 2015;3:e27. 10.2196/mhealth.3422 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Kaufman EA, Baucom KJW. Treating comorbid social anxiety and major depression: The challenge of diagnostic overshadowing. Clin Case Stud 2014;13:265–81. 10.1177/1534650113508220 [DOI] [Google Scholar]
- 47. Ohayon MM, Schatzberg AF. Social phobia and depression: prevalence and comorbidity. J Psychosom Res 2010;68:235–43. 10.1016/j.jpsychores.2009.07.018 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
ebmental-20-65-DC1-inline-supplementary-material-1.docx (109.9KB, docx)