

Abstract
Behavioral Inhibition is a temperament identified in the first years of life that enhances the risk for development of anxiety during late childhood and adolescence. Amongst children characterized with this temperament, only around 40 percent go on to develop anxiety disorders, meaning that more than half of these children do not. Over the past 20 years, research has documented within-child and socio-contextual factors that support differing developmental pathways. This review provides a historical perspective on the research documenting the origins of this temperament, its biological correlates, and the factors that enhance or mitigate risk for development of anxiety. We review as well, research findings from two longitudinal cohorts that have identified moderators of behavioral inhibition in understanding pathways to anxiety. Research on these moderators has led us to develop the Detection and Dual Control (DDC) framework to understand differing developmental trajectories among behaviorally inhibited children. In this review, we use this framework to explain why and how specific cognitive and socio-contextual factors influence differential pathways to anxiety versus resilience.
Keywords: Temperament, anxiety, child development, developmental psychopathology, electroencephalography
Introduction
The 2022 strategic plan of the National Institute of Mental Health outlines a series of steps considered critical for understanding the developmental origins of mental illness. The plan focuses on the importance of ‘conducting longitudinal studies that track changes in behavior with changes in brain development, psychosocial development, and other normative maturational processes, to characterize the progression from early markers to subsequent impairment in domains of functioning’ (NIMH, 2022). Throughout this plan, emphasis is placed on assessing and tracking infants, children, and adolescents to isolate functional domains that alone or in combination predict the onset and course of mental illnesses. This developmental approach to understanding the early biological and psychosocial origins of psychopathology aligns with the goals of several large-scale longitudinal studies, including our own. In particular, we focus on describing variation in infant temperament and the direct and indirect links between temperament and later risk for psychopathology. Indeed, our own study of individual differences in infants’ reactions to novelty and the neural, cognitive, and social-contextual moderators of the associations between early temperament and later anxiety provides a prototype for studies of the developmental origins of psychopathology.
The field of infant temperament has a long and rich history of describing individual differences in reactivity and regulation that form the foundation of a child’s emerging personality. One of the earliest examples of this research tradition is the New York Longitudinal Study in which Alexander Thomas and Stella Chess asked parents to describe their young children’s reactions to numerous common contexts (e.g. feeding, bathing, and sleeping; Chess & Thomas, 1977; Thomas, Chess, Birch, Hertzig, & Korn, 1963). They noted systematic variation in children’s reactions across contexts and found that these patterns predicted adjustment over time. One dimension along which children varied was their responses to novel people, places, and experiences. Noting the salience of novelty for eliciting a wide range of reactions in not only humans but also non-human species, Jerome Kagan coined the term behavioral inhibition (BI) to describe young children’s negative reactions to novelty (Garcia Coll, Kagan, & Reznick, 1984; Kagan, Reznick, Clarke, Snidman, & Garcia-Coll, 1984). BI is characterized by heightened vigilance to novelty combined with a lack of approach and active avoidance of unfamiliar objects, people, and environments. Studies characterizing the development of this phenotype across infancy, childhood, and adolescence have consistently found that approximately 40% of children with this temperament go on to develop anxiety – specifically, social anxiety – in adolescence (Clauss & Blackford, 2012). Of course, this suggests that roughly 60% of young children with this temperament do not go on to display heightened anxious symptoms or develop a clinical diagnosis of anxiety in later childhood and adolescence. The heterogeneity of clinical outcomes among children with early BI suggests that there must be critical factors that moderate the link between early BI and later psychopathology.
In this article, we review empirical work from our group and others focused on uncovering the behavioral, neurocognitive, interpersonal, and social-contextual moderators that determine which children with early BI go on to develop later anxiety. We first describe the history of work on BI, the characteristics of this temperament, and its measurement and stability across development. Subsequently, we review findings from our program of research examining the developmental pathways from BI to psychopathology with particular emphasis on anxiety, and the moderators of this pathway. We review our own Detection and Dual Control (DDC) model (Fox et al., 2021), which provides a conceptual framework for understanding how different styles of allocating attention might amplify or reduce the risk for anxiety among BI children. Next, we extend the DDC model to describe the role of socialization experiences in the emergence of BI and the development of anxiety, with an emphasis on how specific parenting styles and behaviors might moderate trajectories from BI to anxiety by affecting how children manage their attention in the service of emotional and behavioral self-regulation. Moving towards applications of this program of research, when discussing the moderating impact of parenting behaviors, we also review findings from family-focused interventions targeting the parenting behaviors of parents of behaviorally inhibited children. Finally, we conclude with a discussion of the remaining questions that will guide future directions for research in this area.
Behavioral inhibition
Concepts related to behavioral inhibition
The temperamental construct of BI, observable as a behavioral phenotype, is reflected in variations in children’s observable reactions to novel contexts, objects, and social situations involving an adult (e.g. stranger approach). In response to novelty, children characterized as high in BI are slow to approach, seek proximity to their caregivers, and express negative affect. There are several constructs in the field of psychological science that overlap with BI, including negative reactivity (Kagan & Snidman, 1991a), dysregulated fear (Buss, 2011; Morales, Pérez-Edgar, & Buss, 2014), fearful temperament (Kiel & Buss, 2011; Morales, Beekman, Blandon, Stifter, & Buss, 2015), anxious solitude (Gazelle & Rubin, 2010), social wariness (Degnan, Henderson, Fox, & Rubin, 2008), social reticence (Degnan et al., 2014; Rubin, Coplan, & Bowker, 2009), shyness (Buss & Plomin, 1984; Rubin & Asendorpf, 1993), approach/withdrawal conflict (Prior, Sanson, Oberklaid, & Northam, 1987; Windle & Lerner, 1986), anxious temperament (Kalin & Shelton, 2003), and neophobia (Cavigelli & McClintock, 2003). Although a comprehensive examination of the taxonomy of these different constructs is beyond the scope of this review, it is important to note relations and key differences amongst these constructs. First, these constructs differ in whether they refer to the observable behavioral phenotype (e.g. BI, social wariness and social reticence), or the presumed underlying motivational state (e.g. fearful temperament, approach/withdrawal conflict, and neophobia). Second, several of these constructs are considered antecedents of BI (e.g. negative reactivity) or later developmental expressions of BI (e.g. anxious solitude, social wariness, social reticence, and shyness). Third, constructs like anxious temperament and neophobia are most often used when examining non-human animal models of social fear. Fourth, several constructs, such as dysregulated fear or fearful temperament, overlap with a characterization of the BI phenotype but are specific to contexts of assessment (e.g. social reticence and social wariness are measured in the context of unfamiliar peers; dysregulated fear is measured by examining children’s reactions in high-threat and low-threat contexts). Finally, fearful temperament is a broader construct, or an umbrella term, that encompasses all these forms of withdrawn temperaments and may be measured with a combination of parent reports and behavioral observations. In this review, we will refer to BI when specifically referring to that construct, and fearful temperament when referring to all other constructs. Moreover, we will employ the term ‘BI phenotype’ when referring to the observable constellation of behaviors that are indicative of the underlying construct of BI, and simply ‘BI’ to refer to the construct.
Behavioral inhibition: A brief history
The term Behavioral Inhibition was first coined by Jerome Kagan and his then graduate student Cynthia Garcia-Coll in their 1984 Child Development paper (Garcia Coll et al., 1984). The authors selected 117 21- to 22-month-old White toddlers from nearby Boston communities who were from a larger group of families (n = 350) recruited based on their extreme scores on parent reports of shyness and approach/withdrawal responses to novelty. The 117 toddlers were comprised of 56 who were rated low in temperamental approach and 61 who were rated high in temperamental approach tendencies. These toddlers were brought to a laboratory where they were observed during a warm-up session, a free play session, an interaction with an unfamiliar adult around a set of toys, the approach of another unfamiliar adult, the presentation of a novel and unpredictable toy robot, and during a brief separation from their mother. Based on detailed coding of the toddlers’ behaviors and emotions, children were characterized as either inhibited (displaying a total of nine or more inhibited behaviors; e.g. apprehension or withdrawal, long latency to talk, clinging to the mother, negative affect), uninhibited (displaying two or fewer inhibited behaviors), or neither (three to eight inhibited behaviors).
Forty-three of these children (22 inhibited and 21 uninhibited) were seen again when they were four years of age (Kagan et al., 1984). At that time, in two laboratory sessions, children were administered a series of tasks to assess their behavioral responses to novelty. Each child was also paired with another same-age child and observed in a play situation. In the first session, each participant was paired with a child with a similar temperament (e.g. inhibited/inhibited) and in the second session, each participant was paired with a child with the opposite temperament (i.e. an inhibited child with an uninhibited child). Measures of latency to talk, proximity to the other child, and latency to approach the other child were coded. The results from this follow-up study suggested modest stability of the inhibited profile over the 2-year period. Interestingly, in this small sample, five children who were classified as inhibited at age 2 became much less inhibited over time whereas only one child previously classified as uninhibited became inhibited, raising questions about factors that might promote discontinuity in behavioral expressions of inhibition. In a subsequent follow-up of these children at age 5 and a half, multiple physiological measures (e.g. EKG for heart rate and saliva for cortisol) were acquired and Kagan et al. determined that inhibited children displayed elevated heart rate and heightened sympathetic arousal when faced with novelty (Reznick et al., 1986).
Throughout this early work on BI, Kagan, Reznick, and Snidman (1987) speculated about the underlying biology that may give rise to individual differences in reactions to novelty. Kagan associated the BI phenotype with a specific pattern of autonomic reactivity during cognitively challenging tasks: BI children showed larger increases in heart rate, greater pupillary dilation, and more skeletal muscular tension to challenge compared to uninhibited children. Based on studies of the neural basis of fear conditioning in rodents, Kagan speculated that subcortical brain structures and circuits associated with the detection of novelty or threat were at play. Specifically, he reasoned that the autonomic and behavioral changes associated with BI were the result of individual differences in the threshold for excitability in neural circuits associated with the amygdala, including projections to the ventromedial striatum (for muscle tension) and the cingulate and central gray (associated with distress vocalization).
The contrast in behavioral reactions to the novelty of inhibited and uninhibited children was proposed to arise from variation in the excitability of neural circuits of the limbic system (Kagan & Snidman, 1991a). The original support for the involvement of these areas came from lesion studies with animal models examining fear extinction – the process of learning that a previously threatening stimulus is no longer dangerous (Milad & Quirk, 2012; Morgan, Romanski, & LeDoux, 1993). Later work in adults investigating fear conditioning confirmed the role of similar brain areas in the inhibition of fear in humans (Phelps, Delgado, Nearing, & LeDoux, 2004; Phelps & LeDoux, 2005). In particular, this model focuses on the amygdala, which has been implicated in the generation of fear (Davis, 1992, 1998). Increased activity of the amygdala (especially the central nucleus) would be expected to result in increased activity across response systems that have extensive connections with the central nucleus (see Marshall & Stevenson-Hinde, 2001).
Based on the idea that the biological and behavioral origins of BI assessed at 14 months can be traced back to early infancy, Kagan and Snidman (1991a) proposed that infant reactivity may be an early behavioral antecedent of BI as it may reflect variations in thresholds of excitability in subcortical regions such as the amygdala. To examine this, Kagan et al. assessed infants’ reactivity patterns at 2, 4, 6, and 9 months of age, with follow-up assessments of BI at 14 months and 24 months, in a sample of White infants of primarily college-educated parents (Kagan & Snidman, 1991a, 1991b). They found that individual differences in 4-month-old infants’ negative responses to novel auditory and visual stimuli reliably predicted BI at both 14 and 24 months. Specifically, infants who responded with high levels of motor reactivity (i.e. back arching, unsynchronized arm, and leg movements) and negative affect were more likely to display BI in the second year of life. This association between infant reactivity and BI has been replicated across three independent datasets (two from our own lab and one from Kagan’s; Fox, Snidman, Haas, Degnan, & Kagan, 2015).
Work from our lab
Starting in 1990, we began our own longitudinal studies of temperament by recruiting two cohorts of infants from the general community, and like Kagan, screening them at age 4 months to assess their reactivity to novel auditory and visual stimuli. Unlike Kagan, we selected three groups of infants (N = 173) to follow: infants high in motor reactivity and negative affect (‘high negative’, using Kagan’s approach), high in motor reactivity and positive affect (‘high positive’), and a sample of infants low in all dimensions of reactivity. The high positive group was selected to examine the specificity of findings to negative reactivity versus any type of extreme reactivity. We characterized BI in the laboratory at the age of 14 months and acquired a resting state EEG. The infants identified as high in negative reactivity were indeed more inhibited in the lab and showed greater right frontal EEG asymmetry at rest (interpreted as an index of avoidance motivation). The sample was predominantly White and from middle-to-high socioeconomic backgrounds.
When these children were four years of age, in collaboration with Kenneth Rubin, we created play quartets (one high behaviorally inhibited child, one high positive child, and two children from the low reactive group). These children were observed in a series of unstructured (free play) and structured (clean-up and special toy) activities and their play behaviors were coded. Critically, children who displayed high levels of BI as toddlers engaged in more reticent behaviors (e.g. staying on the periphery of group activities, carefully watching, but not engaging with the other children). Subsequent follow-ups of this cohort of children found that by adolescence children classified as behaviorally inhibited as compared to non-inhibited were 3.79 times more likely to meet the criteria for the diagnosis of lifetime social anxiety (Chronis-Tuscano et al., 2009).
While our reading of the neuroscience and temperament literatures of the time initially led us to hypothesize this direct pathway from BI to psychopathology, it was clear that this was far from a 1:1 mapping. We quickly became fascinated with understanding the internal (i.e. within-child) and external (i.e. social-contextual) factors that could help distinguish between high BI children who went on to develop anxiety disorders versus those who were equally inhibited early on but did not. There is some evidence that girls display slightly (but significantly) more shyness than boys in childhood (Else-Quest, Hyde, Goldsmith, & Van Hulle, 2006), but that shyness is associated with more negative social–emotional functioning in boys (Doey, Coplan, & Kingsbury, 2014). These studies provide broad support for the argument that within-child characteristics alter the developmental context in which BI influences later functioning. Given our own interests in basic attention processes, we speculated that one of the within-child factors that could moderate the relation between early BI and later social anxiety is a child’s attention-orienting to threat. We reasoned that BI children with heightened attention biases to the threat could be at an increased risk for experiencing social withdrawal as this attention pattern could perpetuate or increase their anxiety during interactions with unfamiliar others (Pérez-Edgar et al., 2010). We tested whether attention bias to threat derived from the Dot Probe task (MacLeod, Mathews, & Tata, 1986) could moderate the pathway from early BI to adolescent social withdrawal. In a paper by Pérez-Edgar et al. (Pérez-Edgar et al., 2010), we showed that children with high BI showed a greater attention bias to threat and that the relation between early BI and later social withdrawal was significantly stronger for those with heightened attention biases.
Another within-child factor that we thought would moderate the relation between BI and social anxiety was children’s attentional vigilance to other signs of threat, specifically their own errors. Briefly, error monitoring refers to the ability to internally detect one’s own errors, and the sensitivity of this neurocognitive process can be indexed by an EEG measure known as error-related negativity (ERN; Pérez-Edgar et al., 2010). Based on evidence suggesting that anxious individuals display enhanced (more sensitive) error monitoring (Hajcak, McDonald, & Simons, 2003), we examined whether children with high BI would also exhibit enhanced error monitoring, as indicated by a larger magnitude ERN, and whether enhanced error monitoring would potentiate risk for later clinically significant anxiety among children high in BI. To examine these questions, we administered a Flanker task with EEG to examine adolescents’ responses to their own errors and found that those with BI in infancy who displayed a heightened ERN amplitude were more likely to have an anxiety diagnosis (McDermott et al., 2009) than adolescents with a history of BI who did not show such exaggerated responses to their own errors. Likewise, a subsequent follow-up assessment of the same cohort of participants in young adulthood (Tang et al., 2020) found that infants with high BI at 14 months of age demonstrated more adult internalizing (i.e. anxiety and depression) problems if they displayed heightened error monitoring in adolescence, suggesting that heightened error monitoring strengthened the association between BI in toddlerhood and internalizing psychopathology all the way into adulthood (Tang et al., 2020).
This initial longitudinal study allowed us to identify two important within-child moderators of early BI – attention bias to threat and error monitoring – that, by late childhood/early adolescence, functioned to increase the risk for anxiety. Given our design, we could not examine whether these processes were present early in life soon after the identification of BI or emerged only later in childhood and adolescence. When gathering data from this first longitudinal cohort, we did not measure the caregiving context so could not examine the impact on trajectories of BI over time, despite the fact we suspected these contexts must play a critical role in shaping children’s abilities to regulate their strong reactions to novelty and unfamiliarity.
However, we have been fortunate to continue to follow this first cohort. This has enabled us to examine the impact of early BI on adult personality, social functioning, and mental health. Tang et al. (2020) assessed 115 of these participants when they were in early adulthood (mean age of 26 years) and found that adults who as young children were high in BI, reported being more introverted, and reported poorer functioning in several social and mental health domains. As well, responses to errors, assessed by the ERN ten years earlier continued to moderate the link between BI and anxiety in adulthood.
With funding from the NIH, we undertook the recruitment and selection of the second cohort of infants so we could gather earlier and more comprehensive assessments of attention and socio-contextual factors to not only replicate but extend our prior findings. In total, 779 infants were recruited from the community and were assessed in the lab for reactivity (both motor and affect: positive/negative) at 4 months of age. Three groups (N = 291) were selected: a group of infants who displayed high negative affect and high motor reactivity, a group with high positive affect and high motor reactivity, and a control group whose affective/motor reactivity was not high. The sociodemo-graphic distribution of this sample was similar to that of the United States population, with about 69% White, 17% Black, 7% Latinx or Hispanic, 3% Asian, and 3% other. These participants completed BI assessments at ages 2 and 3. We had four novel goals in designing this new cohort study. First, we designed the study such that we could observe children’s social reticence with unfamiliar peers early in development and repeatedly across childhood. As such, participants were seen at 2, 3, 4, 5, and 7 years of age, each time paired with a different unfamiliar same age, a same-sex child in a free play session. Second, as early in life as we could, we assessed their attention biases towards novelty and threat. This was accomplished by examining brain responses to novel auditory stimuli at 9 months of age and using a Dot Probe task at 5 years of age. Third, we assessed executive skills (inhibitory control, attention shifting) to isolate within-child factors that might either increase the risk for children with a history of BI, or mitigate risk (i.e. attention shifting). Fourth, we examined how social-contextual factors such as parental personality, parenting behaviors, and peer context played a role in changes in inhibited behaviors and the development of anxiety.
This longitudinal study produced discoveries that ultimately led to our formulation of a novel conceptual framework for understanding risk and resilience among children with a history of BI. First, a paper by White, McDermott, Degnan, Henderson, and Fox (2011) examined the moderating role of preschoolers’ inhibitory control (assessed with behavioral measures like the day-night Stroop) and task switching (assessed with the dimensional change card sort task, DCCS) on the association between BI and anxious behaviors. Children high in BI, who were also high in inhibitory control, were more likely to exhibit anxious behaviors while children who were high in BI and task switching skills were less likely to display anxious behaviors. This finding set the stage for a series of theoretical and empirical reports demonstrating that the specific type of executive/attention skill was critical for understanding optimal self-regulation among children with BI. That is, it was not the case that all executive skills were good for children with a history of BI. Rather, the type of skill mattered. Second, as we found in the earlier cohort, both attention biases to external (e.g. angry faces on a Dot Probe task) and internal (e.g. the commission of errors on a Flanker task) signals of threat amplified the relations between early BI and later social reticence and symptoms of anxiety (e.g. Tang et al., 2020; White et al., 2011). Thus, it appeared critical to identify executive skills that would allow children to more flexibly orient their attention given their predispositions to both quickly detect and strongly fixate on the threat. Finally, our studies showed that social context made a big difference in how behaviorally inhibited children allocated and regulated their attention. We manipulated the peer context (presence of unfamiliar peers or not) and found that the magnitude of the ERN and its link to anxiety was heightened for BI children when they were in the presence of peers (Buzzell et al., 2017), suggesting that novel social contexts prime these threat detection processes in this group.
Based on these findings, we summarized our position regarding a model of dual control (Henderson, Pine, & Fox, 2015) with the idea that the influence of early temperament on the development of social anxiety depends on two types of information processing: automatic (novelty detection, attention biases to threat, and incentive processing) and controlled (attention shifting and inhibitory control). We proposed three hypothetical models (Top-Down Model of Control; Risk Potentiation Model of Control; and Overgeneralized Control Model) linking these processes to variability in developmental outcomes for BI children and argued that early BI is associated with an early bias to quickly and preferentially process information associated with motivationally salient cues. We also argued that, when this bias remains strong and stable across development, the risk for social anxiety is increased. Later in development, children with a history of BI tend to display normative levels of performance on controlled attention tasks, but they demonstrate exaggerated neural responses to achieve this, which may further potentiate the risk for anxiety-related problems.
The detection and dual control moderators of temperament and social anxiety framework
As we gather new data and track our participants further into development, we continue to refine our theoretical model. We summarized our position that continuity or discontinuity in the expression of social fear over the course of development could be partially accounted for by a dual processing model involving the interplay of automatic (novelty detection, attention biases to threat, and incentive processing) and controlled (attention shifting and inhibitory control) processing (Buzzell, Troller-Renfree, Morales, & Fox, 2018; Fox, Henderson, Marshall, Nichols, & Ghera, 2005; Henderson et al., 2015; Henderson & Wilson, 2017). In a recent review (Fox et al., 2021), we refined this model and labeled it the DDC model, which builds on and synthesizes our earlier theoretical work conceptualizing the unique role of cognitive control in BI and the development of social anxiety. Here, we provide a further update and expanded discussion of empirical findings that directly support the DDC model, and for the first time, we synthesize this model with a growing body of research investigating caregiving-BI relations. Through these updates to the DDC model, the current review provides a more comprehensive developmental conceptualization of relations between early BI and later risk for social anxiety.
The DDC framework integrates a growing body of empirical work demonstrating the central role of cognitive control in determining developmental outcomes for children exhibiting the BI phenotype (for prior reviews and theoretical conceptualizations, see Buzzell et al., 2017; Pérez-Edgar et al., 2011). This framework distinguishes between ‘Detection’ processes that register and orient attention to the presence of potentially important information in an individual’s (internal or external) environment and ‘Control’ processes that govern what an individual does with this information (i.e. through changes in sensorimotor control). We further parse control into (a) ‘Planful Control’, which is deployed in a proactive, sustained, and the goal-driven manner in anticipation of a future event; and (b) ‘Automatic Control’, which, after being set up (e.g. through initial task instructions) is only transiently activated in a reactive and just-in-time manner in response to an event requiring control. As reviewed below, we propose that BI is characterized by increases in detection processes across a variety of domains and levels of analysis. However, whether a child with BI goes on to develop social anxiety is heavily influenced by the development and use of planful vs. automatic control; individuals with a history of BI who develop and use planful control are at a reduced risk for manifesting social anxiety, whereas individuals with a history of BI who rely more heavily on automatic control throughout childhood and adolescence are at increased risk for social anxiety. The DDC framework further delineates the reasons underlying such relations, which are best illustrated by their theoretical interactions within social interactions, as originally envisioned by Henderson and Wilson (2017). Specifically, because of increased detection of novel, salient, or threatening events, individuals with BI are more likely than non-BI children to have their attention captured by specific, likely innocuous, events during social interactions (e.g. a peer making a confused look during conversation) (Fox et al., 2021). Importantly, such attention capture occurs at the expense of directing attention towards other relevant social cues and detracts from the goal of maintaining a positive social interaction. For BI children who develop the ability to flexibly redirect attention with the goal of maintaining a positive social interaction (i.e. those high in planful control), the detrimental effects of detection and attentional capture can be overcome. However, BI children who rely heavily on automatic control may instead direct even more attention towards the detected event, impairing their ability to (re) engage in the goal of maintaining a positive social interaction and processing positive social cues. Ultimately, we propose that this inability to flexibly engage goal-directed social attention and behavior is what produces the characteristic social behavior of BI, socially reticent, or socially anxious youth, in which they appear to be ‘spinning their wheels’ during social interactions with peers (Fox et al., 2021). Importantly, we believe this framework could provide a heuristic for understanding why certain socialization experiences, such as the experience of overcontrolling parenting, potentiate risk among children with a history of BI (see Figures 1 and 2). Through the lens of the DDC framework, we now turn to a detailed review of specific findings and how they map onto the categories of detection, planful control, and automatic control.
Figure 1.
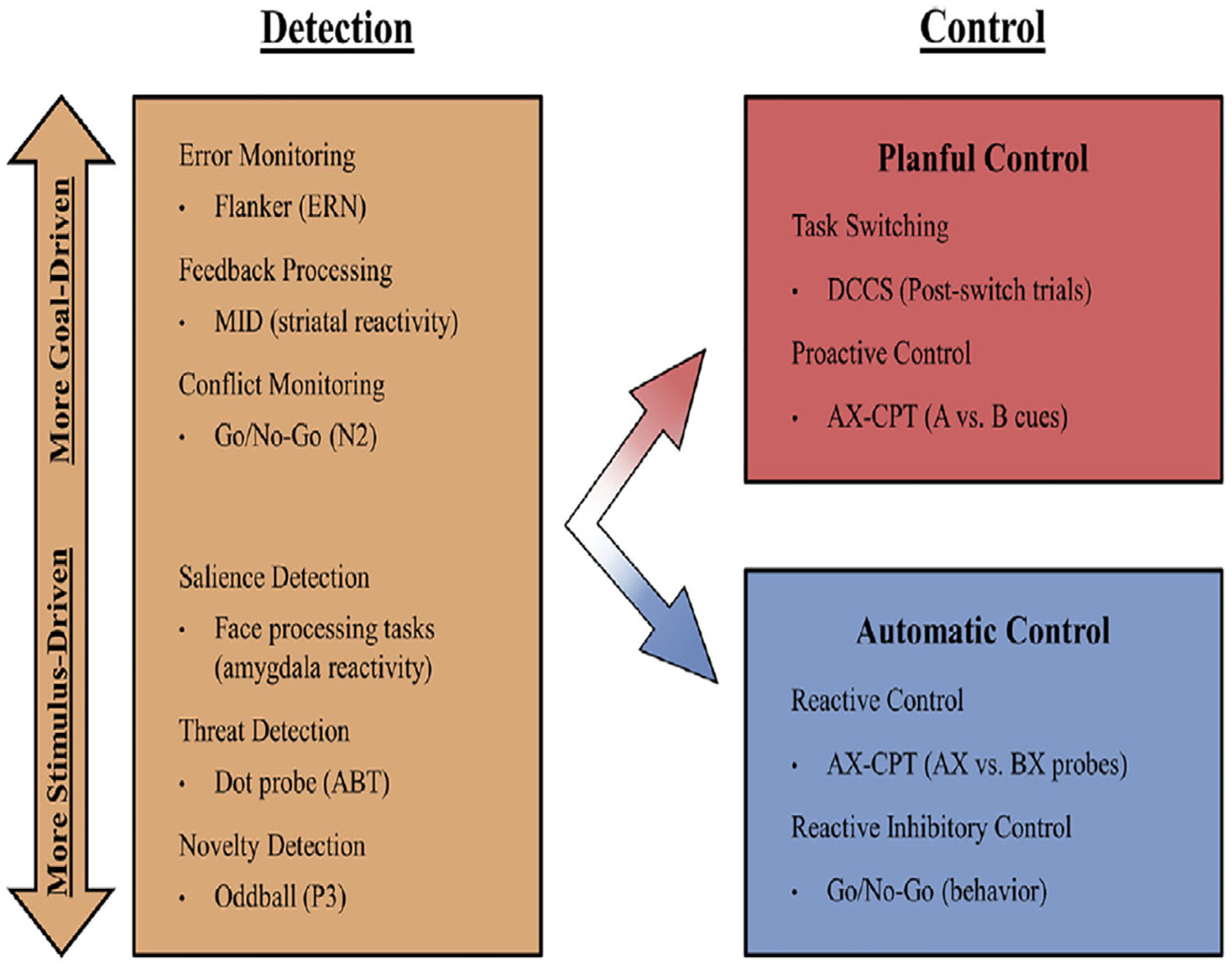
The grouping of attentional and control processes in the current model. Bullets provide an example of a task used in the study of each process, with specific indices from each task presented in parentheses. Note that this list of examples is noncomprehensive. Within the leftmost box, labeled ‘Detection’, processes range continuously from more stimulus-driven at the bottom to more goal-driven. The inclusion of this continuum reflects the heterogeneity of these processes along this dimension, with their unification in a single box reflecting the equivalency in their relationships to behavioral inhibition in the current model. ABT, attention bias to threat; AX-CPT, AX-continuous performance task; DCCS, dimensional change card sort; ERN, error-related negativity; MID, monetary incentive delay
Figure 2.
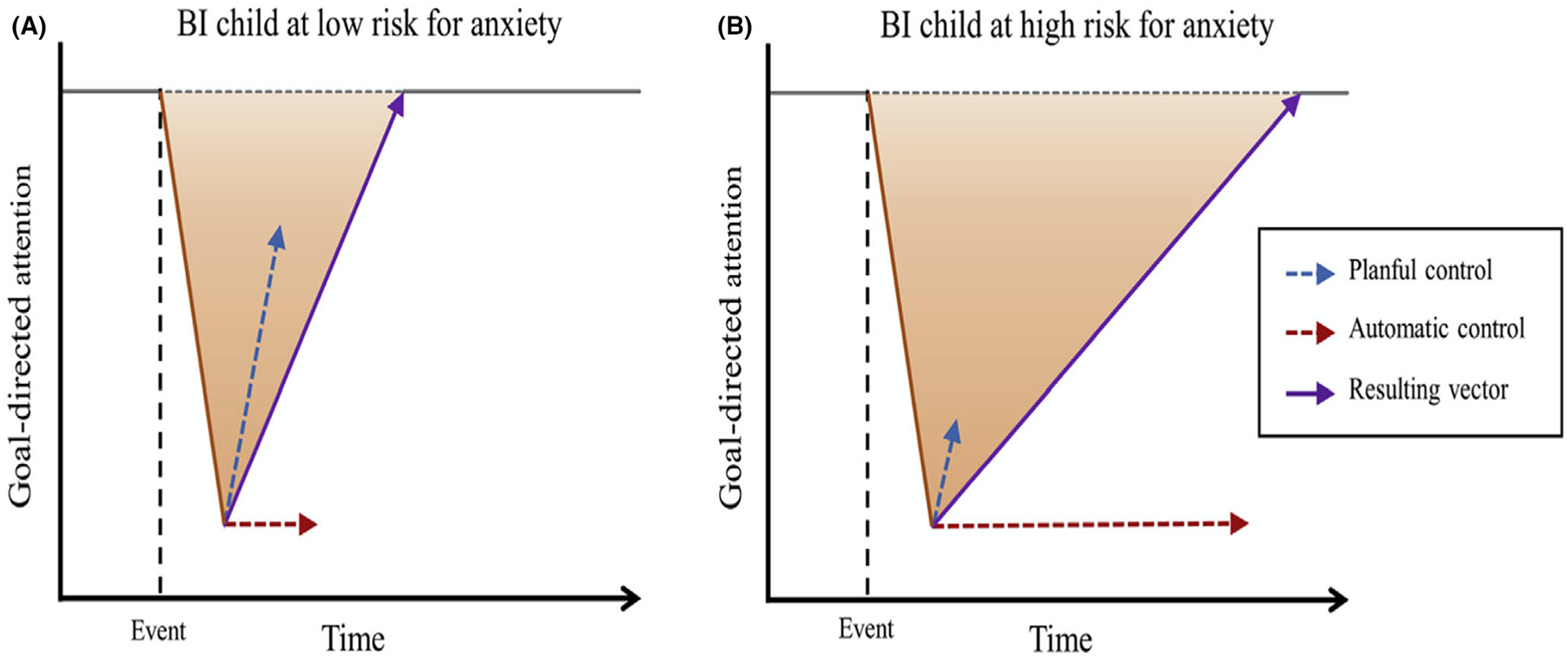
Hypothetical attentional behavior of (A) a child high in behavioral inhibition (BI) at low risk of developing anxiety and (B) a child with high BI at higher risk of developing anxiety. After a salient event occurs, planful control supports the recovery of attention back to goal-relevant information. However, automatic control may instead maintain attention on the salient event and away from goal-relevant information
Behavioral inhibition is associated with increased detection of novelty, threat, and saliency
Within the DDC framework, detection refers to a category of processes that register and orient attention to the presence of potentially important information in an individual’s (internal or external) environment. Detection does not necessarily refer to a specific neural system or network, although it is likely that the amygdala and limbic system play an important role (Fox et al., 2021). Presumably, detection processes exist to provide privileged access to working memory for novel, threatening, or otherwise salient sensorimotor information that require additional processing in a time-sensitive manner to update one’s representation of the environment and/or maintain safety (Ledoux, 1996). While detection often leads to (planful or reactive) control, we conceptualize detection as a theoretically distinct category of processes, which is consistent with longstanding theories of cognitive control (Botvinick, Braver, Barch, Carter, & Cohen, 2001; Miller & Cohen, 2001). Finally, we view detection processes as a single category of processes that exist on a continuum. At one end of the spectrum are lower-level, stimulus-driven processes that tend to emerge earlier in development (e.g. attentional orienting to threatening faces). At the other end of the spectrum are higher-level and more goal-driven processes that tend to only emerge in childhood and continue to develop through adolescence (e.g. the detection of response conflict; Fox et al., 2021; Morales & Fox, 2019).
In line with the traditional characterization of BI as a constellation of behaviors (i.e. the BI phenotype) displayed by some children in response to novel (and/or salient) stimuli (Fox et al., 2005; Fox, Henderson, Rubin, Calkins, & Schmidt, 2001; Kagan et al., 1984) the DDC framework states that trait-level increases in detection processes are central to the underlying temperamental construct of BI. Expanding on the breadth and depth of findings supporting this view, a number of carefully controlled laboratory studies further demonstrate the central role of detection processes in BI. For example, in response to the presentation of novel auditory tones, adolescents with a history of BI in childhood, as well as infants that exhibit greater negative reactivity, display larger neural responses that reflect attentional orienting to the novel stimuli (Marshall, Reeb, & Fox, 2009; Reeb-Sutherland et al., 2009). Children and adolescents with a history of BI exhibit a greater physiological startle response to novel auditory stimuli, as measured by electromyography (Barker et al., 2015; Reeb-Sutherland et al., 2009). When assessing amygdala reactivity to novelty via functional magnetic resonance imaging (fMRI), adults with a history of BI in infancy and childhood exhibit greater neural responses to novelty (Pérez-Edgar et al., 2007; Schwartz et al., 2011; Schwartz, Wright, Shin, Kagan, & Rauch, 2003). In response to threatening faces, adolescents with a history of BI exhibit patterns of behavioral responding consistent with rapid detection of threats (Reeb-Sutherland et al., 2014). In line with heightened responses to saliency, children and adolescents with a history of BI display stronger striatal responses to stimuli signaling either reward (Bar-Haim et al., 2009; Guyer et al., 2006, 2014) or punishment (Helfinstein et al., 2011). In addition, internally salient events, including the detection of stimulus/response conflict (Jarcho et al., 2013; Lamm et al., 2014) and error detection (Buzzell et al., 2017; Lahat et al., 2014; McDermott et al., 2009) are also stronger in children and adolescents with a history of BI.
Collectively, these findings support the notion that increased detection is central to BI. However, it is worth noting that it remains unclear whether such increases in detection reflect a lowered threshold and/or heightened response to the detection of novelty, threat, or saliency (Fox et al., 2021). Relatedly, we emphasize the theoretical importance of the peer context in the assessment of detection processes and BI. Although the role of social/peer context is central to the assessment of BI, later social reticence and social anxiety (Chronis-Tuscano et al., 2009; Degnan et al., 2014; Dyson, Klein, Olino, Dougherty, & Durbin, 2011), limited work has directly examined the role of the peer context on physiological and neural measures of detection in BI (Buzzell et al., 2017).
The DDC framework conceptualizes detection processes as central to BI. While BI is, by definition, a distinct construct from social anxiety, it is nonetheless the best early behavioral predictor of later social anxiety (Chronis-Tuscano et al., 2009; Clauss & Blackford, 2012). Consistent with these ideas, a number of studies find that predicting which children are most likely to develop social anxiety (or anxiety more generally) is enhanced by considering both the behavioral phenotype of BI alongside additional measures of detection processes via cognitive neuroscience and computer-based methods. Compared to their less-anxious peers, children high in both BI and anxiety exhibit greater detection of response conflict, as measured by larger event-related potential (ERP) N2 responses to conflict on Go/No-Go and Flanker tasks (Henderson, 2010; Lamm et al., 2014). Moreover, one of our studies found that BI children’s ERN amplitudes prospectively predicted increased anxiety symptoms 2 years later (Lahat et al., 2014). Finally, a study examining P3 responses to novel auditory tones (which may indicate greater detection of novel stimuli) found that children high in both BI and anxiety have larger P3s than children high in BI but lower in anxiety (Reeb-Sutherland et al., 2009). Similarly, for behavioral measures of attention bias to threat, BI children’s attention bias to threat predicted future anxiety symptoms (Nozadi et al., 2016; White et al., 2017) or continued anxiety risk (Pérez-Edgar et al., 2010, 2011). Overall, ERP and behavioral evidence support the view that children with BI who experience heightened detection of salient stimuli are at greater risk for anxiety difficulties than children with BI who do not. However, in the following section, we turn to the role of planful control vs. automatic control as moderators of risk for anxiety amongst BI children.
Direction of BI-anxiety moderation varies across cognitive control measures
Children’s cognitive control skills have been shown, across multiple measures and at least four independent samples, to moderate anxiety risk among children with a history of high BI (Buzzell et al., 2017; Henderson, 2010; Rydell, Thorell, & Bohlin, 2004; Thai, Taber-Thomas, & Pérez-Edgar, 2016). Importantly, however, the direction of this moderation often varies across cognitive control measures. For example, whereas higher task switching scores (measured, for example, via the DCCS task) are associated with lower anxiety risk among youth with a history of BI, higher accuracy on tasks requiring response inhibition (e.g. Stroop tasks) is instead associated with higher anxiety risk (White et al., 2011). To help make sense of these apparently paradoxical findings, the DDC framework draws from the dual mechanisms of control (DMC) theory, which recognizes the heterogeneity of cognitive control (Braver, 2012).
The DMC theory (Braver, 2012) distinguishes between two temporally distinct modes of control: proactive and reactive. Proactive control is a top-down process involving early selection and maintenance of goal-relevant information. In contrast, reactive control is a more bottom-up, ‘late correction’ process activated on an as-needed basis, usually in response to conflict arising through the course of completing the task (e.g. the conflict between stimulus–response demands, such as that occurring on incongruent trials of Stroop or Flanker tasks). Together, these complementary processes enable individuals to flexibly complete behavioral goals while responding to salient or unexpected events when they occur. However, individuals vary in their preference or bias toward one mode of control or the other in certain kinds of situations, which may have implications for anxiety risk, particularly among individuals with a history of BI.
In line with the DMC theory, our DDC framework predicts differential associations between BI and anxiety as a function of the mode of control the individual relies on the most (i.e. planful or automatic1; Fox et al., 2021). Specifically, children with a history of BI are predicted to experience greater anxiety if they rely predominantly on automatic control compared to planful control.
The AX Continuous Performance Test
A particularly useful paradigm for distinguishing planful from automatic control processes is the AX Continuous Performance Test (AX-CPT; Cohen, Barch, Carter, & Servan-Schreiber, 1999). It presents a series of letter pairs (a cue letter and a probe letter) dissociable into four trial types: AX, AY, BX, and BY. Participants are instructed to make a target response only when they see a specific cue-probe combination (‘A’ followed by ‘X’). The task typically also involves differential probabilities of trials; that is, AX trials appear more frequently than other combinations, making them relatively more expected. Thus, successful performance depends on the ability to detect and maintain memory differences in context (signaled by whether or not the initial cue letter is an ‘A’) while also responding flexibly to relatively unexpected situations (e.g. the infrequent appearance of a non-’X’ probe). In other words, participants must use a combination of proactive and reactive control skills to maintain task accuracy.
Several behavioral and neural indices exist that can help characterize participants’ patterns of responding to AX-CPT trials. D′ context (Cohen et al., 1999) is a behavioral index based on signal detection theory, which contrasts performance on AX trials to that on BX trials. Higher d’ scores indicate greater sensitivity to changes in the context (signaled by the cue letter), indicating greater use of proactive control. Using this and similar behavioral indices, work has found that young children rely predominantly on reactive control because proactive control skills typically develop across the first decade of life and gradually become more efficient during adolescence and young adulthood (Chevalier, James, Wiebe, Nelson, & Espy, 2014; Chevalier, Martis, Curran, & Munakata, 2015; Lucenet & Blaye, 2014; Munakata, Snyder, & Chatham, 2012; Unger, Ackerman, Chatham, Amso, & Badre, 2016). However, the developmental timing of these improvements in proactive control may vary across individuals. At age 13 years, youth with a history of high BI exhibited lower levels of proactive control use (as indicated by lower d’ scores) compared to their low-BI peers (Troller-Renfree, Buzzell, Pine, Henderson, & Fox, 2019). Moreover, Troller-Renfree et al. found that d′ scores moderated the association between early BI and current anxiety at age 13, such that BI was only associated with greater anxiety among children with low or medium levels of proactive control use but not among those with higher levels of proactive control use. In a recent follow-up of these same youth at age 15 years, those with a history of high BI experienced a larger proactive control increase from age 13 to 15 years (Valadez et al., 2022). This 13- to 15-year age window is of particular importance because it captures the typical age of onset for social anxiety disorder (de Lijster et al., 2017). Valadez et al. found that although, on average, youth experienced increased anxiety from age 13 to 15, those with a history of high BI were protected from this anxiety increase if their proactive control skills improved at the mean or greater rates. Those with a history of low BI tended to experience increased anxiety regardless of their proactive control skills. Together, the Troller-Renfree et al. and Valadez et al. studies reveal that (a) BI youth may experience somewhat delayed proactive control development relative to their low-BI peers, and (b) proactive control skills could be especially important for youth with a history of BI as they may help protect these youth from anxiety difficulties.
In contrast to behavioral measures, neural measures permit characterization of activity during the individual cue-locked and probe-locked time windows and thus may provide more specific measures of control processes. Valadez et al. (2021) examined ERPs drawn from EEG data that were simultaneously collected during the 15-year administration of the AX-CPT. Using separate cue- and probe-locked ERPs, they found that BI was associated with anxiety only among youth who tended not to differentiate between cues during the earlier cue period (indicating a less proactive strategy) but instead differentiated between them during the later probe period (indicating a more reactive strategy). In other words, for BI youth, anxiety was elevated only among those with a particular cognitive profile characterized by low use of proactive control and high use of reactive control. Thus, the BI-anxiety relation depended on the interaction between proactive and reactive control processes, rather than being influenced by proactive or reactive control independently. In addition to EEG work, fMRI studies of the AX-CPT and similar tasks have yielded key insights into the brain circuitry involved in proactive control. These studies have noted cue-related (i.e. proactive-control-related) activation in brain areas implicated in goal maintenance, including the dorsolateral and ventro-lateral prefrontal cortex, anterior insula, middle frontal gyrus, and inferior parietal cortex, in addition to ventral visual regions (Delawalla, Csernansky, & Barch, 2008; Lopez-Garcia et al., 2016; Poppe et al., 2016; Ryman et al., 2019). Although fMRI work involving the AX-CPT or similar tasks has yet to be explored in the context of BI, such work will likely help identify brain networks whose functioning may moderate the BI-anxiety relation.
While the DDC model allows us to account for behavioral and neural findings linking salience detection, attention orienting, and reactive versus proactive forms of cognitive control to the expression and varying developmental trajectories of children with a history of BI, we have yet to identify why or how some children develop more biases towards automatic versus planful cognitive control. In the following section, we review the existing evidence relating parent characteristics and intervention-related changes in parenting to BI and anxiety, and in the future directions section, we return to summarize additional parenting findings that we think can be interpreted through the DDC framework.
The role of caregiving in the relation between behavioral inhibition and anxiety
It is clear that caregivers play a critical role in moderating the developmental trajectories of behaviorally inhibited children. In this section, we first review evidence on the associations between maternal mental health and children’s BI. We then present findings regarding the effectiveness of prominent interventions targeting key parenting behaviors that put behaviorally inhibited children at risk for later anxiety. In a later section (under Future directions), we review the scant body of emerging evidence on how caregiving may shape children’s anxiety trajectories by affecting the development of detection and control processes, and in turn impact the development of effective regulation and coping skills among children with a history of BI.
The role of parents’ mental health on the emergence of BI in their children
Current evidence suggests that parental anxiety often predicts the emergence of children’s BI. For example, a study (Rosenbaum et al., 1988) demonstrated that rates of BI were higher in children of parents with anxiety disorders compared to a comparison group of parents without anxiety disorders. Moreover, children with BI were more likely to have multiple anxiety disorders when they were 8–11 years old compared to non-BI children (Biederman et al., 1993). Expanding on this work, Rosenbaum et al. (2000) demonstrated that BI was more frequent in children of parents with mood disorders (i.e. panic disorder and depression) compared to children of parents who had either of these disorders. BI identified in early childhood significantly predicted the onset of social anxiety diagnosis in middle childhood but did not predict other anxiety disorders, suggesting that BI is likely an early precursor of social anxiety disorder in particular (Hirshfeld-Becker et al., 2007). Together, these findings suggest that parental anxiety and mood disorders may be an important predictor of children’s BI and subsequent development of child anxiety, particularly social anxiety. One likely pathway by which parental anxiety may contribute to child BI/anxiety is through heredity, given previous work showing modest-to-high levels of heritability in the traits of BI and social anxiety (Eley et al., 2015; Smith et al., 2012). However, parents with anxiety may also contribute to the development of children’s BI or anxiety by shaping their prenatal (Buss et al., 2012) and/or socialization experiences (Rickman & Davidson, 1994; Zeytinoglu et al., 2022).
Parental behaviors such as modeling of anxious behaviors and verbal communication of threat-relevant information may explain the relation between parental anxiety and child fear and anxiety (Aktar, Majdandžić, de Vente, & Bögels, 2014; Murray et al., 2008, 2014). For example, in a study comparing the infants of mothers with social anxiety to infants of non-anxious mothers, the effect of maternal social anxiety on infants’ avoidance during a stranger approach task was partially mediated by mothers’ anxious modeling (as reflected by their expressed anxiety) during the social referencing task (Murray et al., 2008). Likewise, in a study with 122 infants and their mothers and fathers, parental lifetime anxiety disordersandparentalexpressedanxietyat12months both predicted toddlers’ fear and avoidance responses during a similar social referencing paradigm involving a stranger at 30 months (Aktar et al., 2014); even though, parental anxiety disorders were not concurrently associated with infant fear/avoidance at the baseline assessment at 12 months (Aktar, Majdandžić, de Vente, & Bögels, 2013). These findings together suggest that parentalanxiety disorders may contribute to the early development of infant fear and avoidance, likely as a result of caregivers’ anxious modeling during social referencing situations.
Parents’ verbal communication patterns (i.e. threat attributes and encouragement) have also been shown to mediate the association between parental social anxiety and child outcomes. For example, socially anxious mothers were shown to make more threat attributions during their conversations with children, which in turn predicted children’s anxiety diagnostic status (Murray et al., 2014). Moreover, maternal anxiety also predicted child internalizing problems through mothers’ low levels of encouragements during mother–child conversations (Murray et al., 2014). If BI children had mothers who were highly encouraging, their risk for having negative representations of school (assessed during a novel behavioral ‘doll task’ using anxiety-provoking vignettes) was lower; but if their mothers were not very encouraging, their risk of having negative representations about school was higher (Murray et al., 2014). Together, these findings suggest that mothers’ high threat attributes and low encouragements during verbal communication may explain the relation between maternal anxiety and child anxiety outcomes, and children high in BI may be protected from developing anxious thought patterns if they receive high levels of encouragement from their parents.
The moderating role of parenting in the relation between BI and anxiety
As noted above, approximately 40% of children with a history of BI go on to develop clinically significant anxiety problems, but 60% do not. Caregiving behaviors are considered one of the main moderating factors that either facilitate or prevent the development of anxiety in behaviorally inhibited children (for extensive reviews, see Degnan, Almas, & Fox, 2010; Ryan & Ollendick, 2018). One main category of parenting behaviors theorized to moderate the relation between BI and later anxiety is parental control behaviors such as overcontrol, overprotection, and intrusiveness. Parental control behaviors, that make up authoritarian styles of parenting, are thought to increase behaviorally inhibited children’s risks of developing anxiety because exposure to such caregiving behaviors may reduce children’s sense of self-control, mastery, and independent problem-solving skills (Wood, McLeod, Sigman, Hwang, & Chu, 2003), and prevent them from developing effective self-regulatory skills including emotion regulation and proactive control. As such, behaviorally inhibited children with lower levels of self-regulation as a result of excessive parental control behaviors are more likely to develop anxiety problems.
In support of this perspective, using a longitudinal design, Rubin, Burgess, and Hastings (2002) demonstrated that mothers’ observed intrusive control and derision during mother–child interactions strengthened the association between observed toddlerhood BI and observed social reticence in early childhood. The BI to social reticence association was significant if mothers demonstrated high levels of intrusive control and derisions, but non-significant at low levels of intrusive control and derisions, suggesting that mothers’ intrusive control and derisions played an important role in the maintenance of inhibited and fearful behaviors across early childhood. Similarly, in a prospective longitudinal study, Lewis-Morrarty et al. (2012) found that patterns of consistently high BI across early childhood predicted higher levels of anxiety in adolescence if the parents demonstrated high levels of maternal over-control, but not if they demonstrated low maternal over-control. These findings suggest that overly controlling maternal behaviors may exacerbate the risk of early childhood BI predicting social reticence in early childhood and social anxiety in adolescence. Similarly, in a Dutch sample, Vreeke, Muris, Mayer, Huijding, and Rapee (2013) found that behaviorally inhibited children exhibited higher levels of anxiety symptoms if their parents reported engaging in overprotective parenting. In addition, Rankin Williams et al. (2009) examined whether parenting styles (i.e. authoritative, authoritarian, and permissive) moderated the relation between observed BI and later internalizing problems, and found that only permissive parenting, characterized as high warmth and low levels of restrictive and firm control, moderated the relation between BI and internalizing problems at age 4, such that BI predicted higher levels of internalizing problems among children whose parents were high in permissiveness, but not among those whose parents were low in permissiveness. Together, this body of work suggests parents’ negative control-related behaviors, such as overcontrol, overprotection, as well as permissive parenting indicating the absence of sufficient parental control, may strengthen the relation between BI and later anxiety, likely because they would prevent the children from developing effective and planful regulation strategies that would allow them to flexibly cope with novel or fear-eliciting situations.
In addition to negative forms of parental control, positive parenting behaviors involving gentle encouragement, responsiveness, and acceptance (or opposite of rejection) are theorized to prevent behaviorally inhibited children from developing anxiety problems, as these parenting behaviors promote children’s emotion regulation and independent problem-solving (Degnan et al., 2010; Wood et al., 2003). In a cross-sectional study involving 11- to 15-year-old children, van Brakel, Muris, Bögels, and Thomassen (2006) found that parent–child attachment quality moderated the relation between BI and anxiety symptoms, such that higher levels of self-reported BI predicted higher levels of anxiety problems among children who reported being insecurely attached relative to those who reported secure attachment. Similar to these findings, Hane, Cheah, Rubin, and Fox (2008) showed that preschoolers’ shyness predicted their social withdrawal in childhood only among those whose mothers demonstrated low levels of positivity. Finally, Sentse, Veenstra, Lindenberg, Verhulst, and Ormel (2009) found that high levels of adolescent fearfulness predicted internalizing symptoms 2–3 years later across the sample, but this effect was significantly stronger when child-reported parental rejection was high. These findings together suggest that the relation between BI and later anxiety is stronger if children experience insecure attachment, low positive/responsive parenting, or low acceptance.
The child as an active agent in eliciting certain parenting responses: Potential bidirectional or transactional relations
Although much of the work on BI-caregiver relations examined either the direct influence of parents on children’s fear and anxiety development or the moderating influence of parents on the BI-anxiety association, children are theorized to be active agents in their social world and may themselves elicit certain parenting behaviors from their parents (Pérez-Edgar, LoBue, & Buss, 2021). Thus, it is important to better understand if, when, and to what extent children elicit specific parenting behaviors from their parents (child-to-parent effects), whether these parenting behaviors in turn increase or decrease children’s risk for later anxiety (transactional effects), and/or whether parent–child behaviors mutually affect one another (bidirectional effects).
In order to understand whether a child’s inhibited behaviors elicited specific parenting responses, Belsky, Rha, and Park (2000) observed American and Korean children’s inhibited responses and their mothers’ and fathers’ responses to inhibition across several laboratory episodes. Across both groups, they found that children’s inhibited behaviors elicited three types of parental response: (a) encouraging approach to the stimuli, (b) encouraging withdrawal from the stimuli, and (c) discouraging withdrawal. Interestingly, these three parenting behaviors were positively associated, such that high levels of use of one parenting strategy was associated with high levels of other parental responses. Follow-up analyses showed that there were no subgroups of parents who engaged in certain types of these parenting behaviors more than others; but parents differed with respect to how much they engaged in all three behaviors. Due to the short-term design, the study could not answer whether child-inhibited behaviors had a long-term effect on parenting behaviors, and/or whether child-elicited parenting behaviors predicted children’s later anxiety.
Using a longitudinal design, Rubin, Nelson, Hastings, and Asendorpf (1999) found that high levels of parent-reported child shyness at age 2 predicted lower levels of parental encouragement at age 4, suggesting that parents’ perception of their children’s temperament affected how parents treated them in the years to come. However, there was no support for the opposite relation: low parental encouragement at age 2 did not predict the parental perception of child shyness at age 4. Expanding on these findings, Price and Kiel (2022) found that toddlers’ dysregulated fear in low-threat laboratory tasks at age 2 predicted mothers’ perception of children’s inhibited temperament at age 3, which in turn predicted mothers’ non-supportive responses (i.e. punitive behaviors, minimizing and distress reactions) at age 4. These findings suggest that toddlers who show dysregulated fear elicit non-supportive parental responses by affecting their mothers’ perception of their temperament. Consistent with these findings, Van Zalk and Kerr (2011) demonstrated child-to-parent effects much later in development, in adolescence, such that adolescent shyness predicted increases in parental intrusive overcontrol and rejection and decreases in parental warmth one year later. Together these findings suggest that children’s BI and fearful temperament may elicit certain parenting behaviors (e.g. less encouragement and punitive reactions) during both childhood and adolescence, likely by affecting parents’ perception of children’s temperament.
There is also some evidence suggesting that child-elicited parenting responses contribute to children’s anxiety in the years to come. For example, Buss, Zhou, and Trainer (2021) found that dysregulated fear at age 2 was associated with subsequent maternal over-protection, which in turn was associated with higher levels of child anxiety at age 3. This finding provides some support for a transactional effect, such that children with dysregulated fear elicit overprotective behavior from mothers, and this behavior in turn is associated with increased child anxiety. Interestingly, there is also evidence suggesting that child-elicited parenting behaviors may also have effects on parents’ own mental health. For example, Kiel, Aaron, Risley, and Luebbe (2021) showed that toddlers’ anxiety risk predicted mothers’ use of comforting behaviors in response to toddlers’ solicitations, and toddler-solicited comforting behaviors, in turn, predicted mothers’ later anxiety, suggesting that children may also affect their parents’ mental health by affecting their parenting behaviors.
Finally, based on the idea that parents and children may mutually affect each other, studies have examined bidirectional relations between parent and child temperament and/or anxiety (see Pérez-Edgar et al., 2021, for a review of a special issue on this topic). As discussed by Pérez-Edgar et al., some studies find evidence for bidirectional relations, and some do not. Importantly, there is evidence for both child-to-parent and parent-to-child effects; however, these effects are often not direct but are mediated by other processes, such as parental perception of child behavior (e.g. Price & Kiel, 2022) and/or a specific parenting behavior (e.g. Kiel et al., 2021). These findings and discussions together highlight the importance of understanding when and through which processes mothers and children affect one another.
Parenting interventions for children with behavioral inhibition
Parental behaviors that contribute to the development of social anxiety, such as parental accommodation, have been the targets of parent-focused interventions. Specifically, parental accommodation refers to modifications in parenting behaviors to prevent or reduce their child’s distress when they encounter a fear-invoking situation or stimulus (Kagan, Peterman, Carper, & Kendall, 2016; Thompson-Hollands, Kerns, Pincus, & Comer, 2014). Parental accommodation involves behaviors such as enabling or permitting a child’s anxiety-related avoidance, following rigid rules related to encountering anxiety-provoking stimuli, modifying family routines, and providing excessive reassurance (Lebowitz et al., 2013). Although accommodation can reduce a child’s anxiety in the short term, it contributes to the maintenance of anxiety by promoting future avoidance or ineffective ways of dealing with anxious feelings (Ginsburg, Siqueland, Masia-Warner, & Hedtke, 2004). Likewise, parental oversolicitous behaviors, which are closely related to accommodation, strengthen the relation between BI and maladaptive emotion regulation strategies (i.e. less engaged/active emotion regulation), which in turn led to greater social anxiety (Suarez et al., 2021). In clinical samples, almost all parents of children with anxiety problems have reported frequent use of accommodations to alleviate child distress (Lebowitz et al., 2013; Storch et al., 2015). There is evidence suggesting that parent-focused interventions designed to reduce parental accommodation reduce children’s anxiety symptoms after treatment (Kagan et al., 2016; Lebowitz, Omer, Hermes, & Scahill, 2014), indicating that parental accommodation may be an important target in the prevention and treatment of anxiety problems.
Given that children with a stable pattern of BI are prone to experience anxiety later in life, interventions have also been developed to prevent the development of anxiety in children classified as behaviorally inhibited. One such intervention is Cool Little Kids (CLK) developed by Rapee, Kennedy, Ingram, Edwards, and Sweeney (2010). CLK is a 6-week group treatment for parents that provides psychoeducation about anxiety development, parental strategies for targeting their own anxiety, and strategies for reducing parental overprotection and accommodation. Compared to a no-treatment control group, CLK significantly reduced behaviorally inhibited children’s anxiety symptoms and disorders at a 3-year follow-up (Rapee et al., 2010). Overall, these findings suggest that targeting parents’ own anxiety and parenting behaviors that are known to perpetuate child anxiety (i.e. overprotection) effectively prevented behaviorally inhibited children from developing anxiety. Expanding on this work, the CLK program delivered at a population level to the parents of inhibited children via preschool services had effects on lowering children’s anxiety problems in the first year of school (Bayer et al., 2021) and reducing the risk for internalizing problems in middle childhood for inhibited children with anxious parents (Bayer et al., 2022).
Another well-known intervention designed to prevent the development of anxiety in behaviorally inhibited children is the Turtle Program (Chronis-Tuscano et al., 2022). Turtle is an 8-week-long intervention that includes child and parent treatment sessions. The parent component is based on parent–child interaction therapy for anxiety (Choate, Pincus, Eyberg, & Barlow, 2005). Parent sessions are focused on child-directed interaction (e.g. following the child’s lead, positive reinforcement), bravery-directed interaction (e.g. parent modeling of approach behaviors), and parent-directed intervention (e.g. learning child behavior management strategies). The child component is a modified steady-state free precession (Coplan, Schneider, Matheson, & Graham, 2010) that involves training in enhancing children’s social skills, social problem-solving, emotion regulation, and relaxation. A randomized controlled trial was conducted to test the effectiveness of the Turtle and the CLK programs on both parenting behaviors and child anxiety. Although both interventions yielded significant and comparable improvements in child anxiety outcomes, the Turtle intervention yielded increased observed warmth and decreased parental negative control, compared to CLK (Chronis-Tuscano et al., 2022). Moreover, although parental social anxiety continued to be associated with family accommodation after the CLK program, this relation disappeared as a function of the Turtle program. These findings suggest that certain parenting interventions can effectively reduce parental accommodation and its impact on the development of anxiety problems.
The role of culture in the prevalence and consequences of BI
In this review paper, we focused on BI studies conducted predominantly in North American cultures, mostly in the United States (e.g. Kagan and Fox’s BI cohorts) and Canada (e.g. Rubin’s studies), two societies that place a high emphasis on individuals’ social assertiveness, autonomy, social expression, and being outgoing (Greenfield, Suzuki, & Rothstein-Fisch, 2006; Rubin et al., 2006). Given this cultural emphasis, compared to children with these qualities, children with BI temperament or shy tendencies whose behaviors do not align with or even contradict with these culturally valued qualities, are thought to have a harder time navigating the social world around them and meeting the societal expectations that would bring them success in their family, school, and work lives (Chen & French, 2008). This idea of a misfit between a person and the cultural values held within their developmental context may account for some findings suggesting that shyness is associated with more negative social–emotional functioning for boys than girls in Western societies (Doey et al., 2014). As reviewed in the above sections, BI and shy children often elicit negative reactions from others, as their behaviors may be viewed as problematic by socializers such as parents, teachers, and peers (Chen & French, 2008). This is because these socializers’ perceptions of and attitudes towards these behaviors are largely shaped by the larger cultural context and its values (Chen & French, 2008; Kerr, 2001), and/or because socializers may want to prevent these children from experiencing problems as they may be viewed as incompetent by others. However, given that the meaning of a child’s display of BI and shyness may depend on the cultural context and the values that are emphasized, BI behaviors may not necessarily always associate with mental health problems such as anxiety in other cultural contexts where these behaviors are viewed as aligning with cultural values.
In fact, research from studies conducted in societies that put a greater emphasis on controlling personal desires and self-expression to promote a group-harmony show that BI and shy behaviors are not as negatively evaluated by socializers and do not always associate with negative outcomes such as anxiety, as they may be viewed as promoting social harmony. Much of this evidence comes from research conducted in East Asian countries such as China, South Korea, and Japan (Chen, 2018). For example, in a sample of Chinese children, Chen et al. showed that laboratory-observed BI at age 2 was associated with more peer liking and more positive peer relationships at age 7 (Chen, Chen, Li, & Wang, 2009) and higher levels of social competence and academic outcomes at age 19 (Chen et al., 2021). Consistent with these findings, Chen et al. (1998) also reported that Chinese mothers showed more acceptance to children’s inhibited behaviors than Canadian mothers, and Chinese children demonstrated more positive responses and support, and less rejection to their shy peers’ social initiations compared to their counterparts in Canada (Chen, Rubin, & Li, 1995). Likewise, youth in East Asian countries (China, South Korea, and Japan) were more approving of shy and unassertive behaviors compared to youth in ‘Western’ countries (Australia, Canada, Germany, the Netherlands, and the USA; Heinrichs et al., 2006; Rapee et al., 2011). Together, these findings suggest that inhibited and shy behaviors may be associated with more positive outcomes in East Asian countries as compared to North American contexts, as socializers such as parents, teachers, and peers may react more positively to these behaviors.
Although these findings highlight cross-cultural differences in the socialization and consequences of BI, it is also important to understand that societies and cultural values themselves are subject to change due to factors such as urbanization, globalization, and immigration, which may then impact children’s socialization and outcomes. For example, Chen, Cen, Li, and He (2005) highlight that the rapid sociocultural and economic changes that came along with China’s implementation of the ‘open-door policy’ increased requirements for assertiveness, self-direction, and independence to succeed in China’s new market-oriented economy. These changes are theorized to impact the developmental outcomes of inhibited children given the incompatibility of these behaviors with the new requirements to succeed. In a three-cohort study with data collected in 1990, 1998, and 2002, Chen et al. showed that although shyness was positively associated with positive social and academic outcomes in the 1990 cohort; these relations were weaker in the 1998 cohort; whereas, in the 2002 cohort, shyness was positively associated with social and psychological problems. Specifically, shyness was negatively associated with peer likability, teacher-rated social competence, and positively associated with depression (Chen et al., 2005). These findings suggest that as inhibited and shy behaviors become incompatible with the demands of the new society, children with these qualities may experience socioemotional problems, similar to the ones in North American societies.
In addition to within-society cohort-level differences that parallel the sociocultural changes that follow societal changes, it is also critical to understand whether there are within-society differences in the socialization and consequences of BI and shy behaviors across different communities and sociocultural groups based on the differing cultural values and expectations that may exist in these communities. For example, Chen, Wang, and Wang (2009) showed that BI and shyness were associated with negative outcomes such as social and school problems, and depression in urban Chinese children, but linked with positive outcomes such as teacher-reported competence and academic achievement in rural Chinese children. Likewise, in a different cohort, it was shown that shyness was associated with more adjustment problems in urban children than in migrant rural children (Ding, Chen, Fu, Li, & Liu, 2020). These urban–rural differences are attributed to the different cultural values and socialization practices prominent in urban and rural communities, with rural communities abiding by more traditional Chinese values and thus shy behaviors may be more accepted in these communities.
The majority of the studies reported in previous sections were based upon primarily White, middle-class, and well-educated samples. As such, it is also important to understand whether the socialization and consequences of BI differ across sociocultural groups living in North American countries. There is some evidence suggesting that findings may be generalizable to at least some cultural groups, particularly if their children are evaluated by the dominant cultural norms (Carlo, Cheah, Conejo, & Cho, 2022). For example, similar to White American children, Asian immigrant children’s temperamental shyness was associated with more anxious-withdrawn behaviors, particularly if they received low praise from their mothers, and anxious-withdrawn behavior, in turn, was associated with peer exclusion and passive responses to bullying (Gao et al., 2021), and decreased prosociality and leadership skills (Balkaya, Cheah, Yu, Hart, & Sun, 2018). Similarly, ‘anxious shyness’, reflecting an inability to attend group participation, was associated with peer rejection, whereas ‘regulated shyness’, reflecting more reserved and modest behaviors was not (Xu & Krieg, 2014). Although there are fewer studies on Latin American children, there is some evidence suggesting that Latin American children’s shyness with peers (but not necessarily with adults) was associated with their anxiety symptoms, and, interestingly, high levels of parental collectivistic values determined whether higher levels of shyness with adults predicted shyness with peers (Gudiño & Lau, 2010). Finally, there is also evidence from a sample of Native American adolescents showing that retrospective reports on children’s childhood BI were strongly associated with their social anxiety symptoms (West & Newman, 2007). Together, these findings suggest that BI-anxiety relations seen in White children seem to also exist, at least to some extent, across different ethnic groups in the United States.
Future Directions
As we have shown, there has been extensive work elucidating the nature of BI and factors that moderate its links to anxiety. Yet, key translational questions remain to be answered to help inform clinical assessment and intervention for children with BI. First, is BI simply the earliest manifestation of anxiety problems (i.e. a prodromal state of anxiety) or is it a temperament, found in early childhood, that conveys risk for anxiety but only to some children? There is clear evidence that children with high BI are significantly more likely to develop clinically significant difficulties with anxiety than those with low BI (Sandstrom, Uher, & Pavlova, 2020). However, it remains difficult to distinguish between the multiple possible scenarios that may explain this strong association. Pérez-Edgar and Guyer (2014) described three likely possibilities: (a) BI and anxiety share a core biological mechanism that drives both constructs; (b) BI and anxiety fall on a shared spectrum of socioemotional functioning (with no causal relation between them); and (c) BI plays a causal role in the emergence of anxiety, with BI acting as a diathesis which may be triggered by the presence of another risk factor. Disentangling these possibilities with observational data is difficult. It will require distinguishing BI from other possible causal factors that also relate to anxiety, and also require more large-N prospective longitudinal studies including children with high and low BI, each with high and low levels of anxiety (Pérez-Edgar & Guyer, 2014). More work in this vein is needed to shed light on the multiple etiological pathways toward anxiety, both BI- and non-BI-related.
Second, how early in development can we identify children with BI who have an elevated risk for future anxiety? Prenatal experiences shaped by mothers’ mental health may play a direct role in the emergence of BI by influencing the development of fear-relevant neural circuitry. Evidence from a few studies suggests that this is a probable hypothesis. For example, a longitudinal study with 65 healthy mother–child dyads demonstrated that, in girls, higher levels of maternal cortisol in earlier gestation were associated with a larger right amygdala volume and more affective problems at 7 years of age, and the effect of maternal cortisol on girls’ affective problems was partially mediated by the amygdala volume (Buss et al., 2012). These findings suggest that mothers’ experience of stress, as indexed by their cortisol levels, may have a direct impact on the development of fear-related neural circuitry as well as effective outcomes, especially in girls. Similarly, Qiu et al. (2015) found that prenatal maternal depression was associated with an amygdala functional connectivity pattern (i.e. greater amygdala connectivity with the left temporal cortex and insula and other regions) that is commonly observed in adolescents and adults with depression, suggesting that prenatal maternal depressive symptoms may have an impact of the development of the neural circuitry underlying mood disorders. Complementary to these findings, research from our group has shown that greater post-natal amygdala-cingulate connectivity assessed 3 weeks after birth was associated with greater negative affect towards novel stimuli at 4 months of age (Filippi et al., 2021), suggesting that early fear-relevant neural functioning underlies the development of fear-relevant temperament. Future studies are needed to directly test whether parents’ mental health and stress during pregnancy predict the early emergence of BI during toddlerhood as mediated by infants’ fear-relevant neural functioning.
Third, does BI influence children’s behavior only in social contexts, or do its effects also generalize to non-social contexts? Under the assumption that combining data from different contexts provides a more comprehensive assessment of a child’s temperament, BI is often assessed using standardized batteries that combine measures of avoidance, fear, and vigilance associated with both social and non-social stimuli (Calkins, Fox, & Marshall, 1996; Dyson et al., 2011; Fox et al., 2001; Kagan et al., 1984). However, it may be that BI is not a unitary construct. Efforts to separate BI in social versus non-social contexts reveal weak correlations across the two (Kochanska, 1991; Rubin, Hastings, Stewart, Henderson, & Chen, 1997), with a somewhat more recent study further finding that observationally assessed social and non-social BI have distinct patterns of associations with parent reports of temperament and anxiety symptoms (Dyson et al., 2011). For example, whereas only social BI was significantly associated with a greater likelihood of meeting criteria for social phobia, only non-social BI was significantly associated with a greater likelihood of meeting criteria for specific phobia (Dyson et al., 2011). Buss et al.’s dysregulated fear approach has also focused on the context in which fearful and inhibited responses occur to identify subgroups of fearful children and characterize the heterogeneity in BI (Buss, 2011; Buss et al., 2020). Rather than focus on differences in fear sensitivity between social and non-social contexts, they have focused on identifying toddlers who display high levels of fear in low-threat situations (Buss & McDoniel, 2016). In this context, inappropriate fear responses have been found to predict distinct physiological patterns (Buss, Davis, Ram, & Coccia, 2018; Phelps, Brooker, & Buss, 2016) and increased likelihood of future anxiety, compared to other forms of fearful temperament (e.g. BI; Buss, 2011; Buss et al., 2018). Given the possibility that BI may not be a unitary construct, future work should continue to improve our characterization of BI across situational contexts, and studies investigating moderators of BI-related risk may need to consider whether that moderation may be specific to one aspect of BI versus the other.
Fourth, can the positive effects of parenting strategies and interventions on the developmental trajectories of children with a history of BI be accounted for by changes in children’s cognitive control strategies? That is, can we use our DDC framework to synthesize the largely independent basic and applied literatures on BI and cognitive control and on BI and parenting? Caregivers may contribute to the development of anxiety in behaviorally inhibited children by affecting the development of children’s detection and control processes that mitigate or amplify the risk for anxiety. See Figure 3 for hypothetical relations between parent variables and components of the DDC framework. Understanding the specific parenting behaviors that contribute to the development of children’s detection and control processes described in the DDC framework may clarify the specific mechanisms and offer new avenues for family-focused interventions aimed at preventing behaviorally inhibited children from developing anxiety problems.
Figure 3.
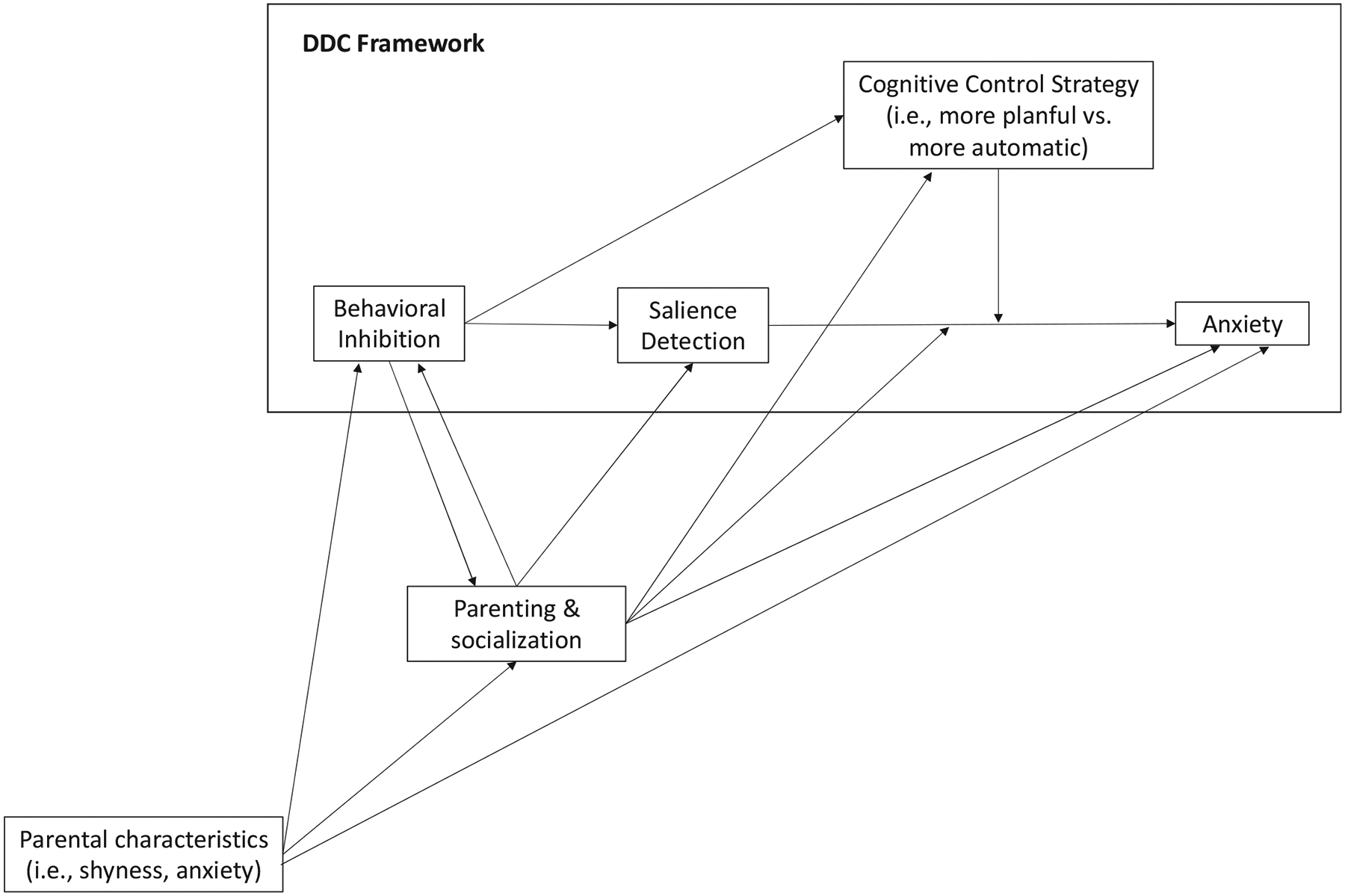
The Detection and Dual Control (DDC) framework and hypothesized links to caregiving
Notably, there is emerging evidence suggesting that heightened parental anxiety may play a role in the development of children’s attention bias to threats. For example, maternal anxiety was concurrently associated with infants’ attention bias to threat (Morales et al., 2017), and maternal anxiety assessed in early childhood predicted children’s faster detection of angry faces among happy faces 3 years later (Aktar, Van Bockstaele, Pérez-Edgar, Wiers, & Bögels, 2019). Likewise, daughters of mothers with a mood or panic disorder have been shown to have greater attention bias to threats compared to daughters of mothers with no psychiatric history (Mogg, Wilson, Hayward, Cunning, & Bradley, 2012; Montagner et al., 2015).
Despite the evidence linking parental anxiety with children’s attention bias to threat, the specific parenting behaviors that may mediate this relation are largely unknown. Although negative parenting behaviors are a good candidate based on the research reviewed above, there may be other under-investigated parenting behaviors that may also explain why parental anxiety predicts children’s attention bias to threats. For example, mothers’ expressed anxiety or modeling of anxious behaviors can explain this relation because such behaviors would direct children’s attention to threats in the environment, enhancing their ability to detect threats more readily. Although there is a need for research in this area, some evidence suggests that both infants and older children learn from their parents’ modeling of anxious behaviors in social referencing paradigms, behaving in more avoidant and anxious ways themselves (e.g. Burstein et al., 2010; de Rosnay et al., 2006; Murray et al., 2008). For example, the effect of maternal anxiety on increases in infants’ avoidance of strangers was mediated by mothers’ expressed anxiety (i.e. or modeling; Murray et al., 2008), suggesting that caregivers’ expression of anxious behaviors in front of their children may play a role in their detection and avoidance of threat in the environment.
In addition to affecting children’s threat detection, certain parenting behaviors may also play a direct role in children’s goal-driven detection processes such as their error monitoring. Specifically, certain negative behaviors such as punitive, harsh, and authoritarian behaviors can contribute to children’s heightened self-monitoring of their own errors (Brooker & Buss, 2014). This is because parents who adopt these negative parenting styles may give punitive or critical reactions to their children’s mistakes, thereby enhancing their error detection responses. In fact, there is evidence showing that punishment (e.g. electric shock and noxious sound) increases the magnitude of individuals’ ERN (Riesel, Weinberg, Endrass, Kathmann, & Hajcak, 2012), especially in anxious individuals (Meyer & Gawlowska, 2017), and this effect persists even when errors are no longer punished. Enhanced error monitoring may allow children to detect their errors and anticipate and prepare for their parents’ punitive reactions that may follow these errors (Banica, Sandre, & Weinberg, 2019).
Consistent with this notion, Brooker and Buss (2014) showed that toddlers’ fearful temperament predicted higher ERN, only if children had exposure to high levels of harsh parenting. This suggests that behaviorally inhibited children may be at a greater risk of experiencing enhanced error monitoring, a neural response associated with anxiety, especially if they are exposed to harsh and punitive parenting behaviors. In a sample with 5- to 7-year-old children and their parents, children’s ERN during parent-observation (but not experimenter-observation) of task performance mediated the relation between parents’ controlling parenting style and children’s anxiety diagnostic status, suggesting that parent-potentiated error monitoring may especially be an important predictor of anxiety (Meyer, Carlton, Chong, & Wisse-mann, 2019). Similarly, in middle childhood and preadolescence, authoritarian parenting continued to relate to children’s elevated ERN, which in turn was associated with their diagnostic status of social anxiety disorder, generalized anxiety, and OCD. This effect was not shown in late adolescence, suggesting that authoritarian parenting may especially shape the development of error monitoring during childhood and early adolescence, which emphasizes the need for earlier interventions for reducing authoritarian and punitive parenting behaviors to prevent the development of anxiety. Consistent with these findings, emerging adult women who reported exposure to higher levels of overprotective/authoritarian parenting behaviors as children showed higher ERN (Banica et al., 2019). Together, these findings suggest that caregivers’ authoritarian, harsh, and punitive behaviors may contribute to the development of children’s anxiety problems by increasing their vigilant error monitoring in the form of heightened ERN, and this effect may be particularly salient for children with BI or fearful temperament.
To our knowledge, there is little research focused on understanding how parents may influence the development of planful and automatic control strategies; however, our DDC framework suggests that understanding parents’ role in the development of these cognitive control strategies may be critical for developing family-focused interventions aimed at equipping inhibited children with the cognitive control strategies that can help prevent the development of anxiety.
Despite limited work in this area, previous work has suggested that responsive and emotionally supportive caregiving behaviors characterized by high responsiveness and autonomy-support, and low levels of intrusiveness and negative/harsh behaviors would facilitate the development of planful forms of cognitive control strategies, especially during early development (e.g. Chen et al., 1995, 1998, 2021). In particular, parents’ engagement in such behaviors during challenging situations that require dyads to plan and problem-solve can allow the child to gradually internalize regulatory skills that can allow them to effectively problem-solve on their own (Bernier, Carlson, Deschênes, & Matte-Gagné, 2012; Gauvain, 2001; Vygotsky, 1978; Zeytinoglu, Calkins, Swingler, & Leerkes, 2017). These parenting behaviors would allow children to learn how to sustain moderate levels of arousal conducive to exerting planful forms of control (Arnsten, 2009; Blair, 2010; Zeytinoglu, Calkins, & Leerkes, 2022) and regulate their attention and emotions to solve problems effectively (Fox & Calkins, 2003). In support of this view, there is longitudinal evidence suggesting that parental emotional support (i.e. high responsiveness, low negativity/intrusiveness) during a semi-structured planning and problem-solving task consistently predicted increases in children’s planful cognitive control (i.e. attention shifting/cognitive flexibility) from one year to the next across early childhood years (Zeytinoglu, Calkins, & Leerkes, 2019). Notably, the vast majority of studies examining the role of parenting in the development of cognitive control focused on the early childhood years (Valcan, Davis, & Pino-Pasternak, 2018), and thus there is a need to understand if and how parenting behaviors later in development contribute to the development of children’s proactive control strategies that would prevent behaviorally inhibited children from developing clinical levels of anxiety.
Finally, in line with the NIMH 2022 strategic plan and its Research Domain Criteria initiative (Insel et al., 2010), the last question concerns the neural circuitry involved in BI-related risk for anxiety. Neural oscillations represent one promising avenue toward elucidating the neural substrates of cognitive control. Time-frequency EEG measures can help characterize oscillatory brain activity among brain regions in ways that are missed by more traditional EEG measures, such as ERPs (Beatty, Buzzell, Roberts, & McDonald, 2020). Oscillations in the theta band (4–8 Hz), in particular, are thought to reflect the organizing activity involved in cognitive control (Cavanagh & Frank, 2014). For example, in adults, increases in theta power over the medial frontal cortex (MFC) are associated with monitoring for conflict or errors (Ullsperger, Fischer, Nigbur, & Endrass, 2014), whereas theta connectivity between MFC and lateral-frontal regions may reflect control recruitment (Cavanagh & Frank, 2014). In adolescents completing a flanker task, MFC connectivity in the theta band preand post-motor response was linked to reactive and proactive control, respectively (Buzzell et al., 2019). When participants believed their performance was being monitored by a peer, participants showed enhancements in theta measures indexing post-response error monitoring and proactive control (Buzzell et al., 2019). These types of time-frequency analytic approaches are more frequently used with young children (Morales et al., 2022; Morales & Bowers, 2022) and may bring us closer to a more mechanistic understanding of the neural processes involved in cognitive control than traditional approaches.
A new approach to studying oscillations involves parameterizing the neural power spectrum into its periodic (putative oscillations) and aperiodic (exponent and offset) components (Donoghue et al., 2020; Ostlund et al., 2022). This contrasts with traditional approaches to characterizing the power spectrum, which generally ignore aperiodic components and often attribute any observed individual differences to specific frequency bands (sometimes mistakenly; Donoghue et al., 2020; Ostlund et al., 2022). In terms of development, children display a flattening of the aperiodic slope with age and a shift from predominantly theta to predominantly alpha oscillations around 7–8 years of age (Cellier, Riddle, Petersen, & Hwang, 2021; McSweeney, Morales, Valadez, Buzzell, & Fox, 2021). A recent comparison of children with and without a history of BI who were assessed in middle childhood revealed that those with BI showed greater alpha band power (Ostlund et al., 2022). By applying spectral parameterization to these data, however, Ostlund et al. (2022) further found that the differences in alpha power were likely due to BI-related differences in the alpha peak frequency. Although more work is needed to understand the functional significance of the rich information revealed by spectral parameterization, it is likely that both time-frequency and spectral parameterization approaches to characterizing oscillatory activity may bring us closer to a more mechanistic understanding of the neural processes involved in BI-related anxiety risk than traditional approaches.
Multimodal neuroimaging techniques may also be needed to probe the neural circuits implicated in BI-related anxiety risk. Planful and automatic control involve overlapping brain regions (Braver, Paxton, Locke, & Barch, 2009) that are engaged together closely in time (van Wouwe, Band, & Ridderinkhof, 2011). Individually, neither electrophysiological nor hemodynamic methods have both the spatial and temporal resolution to separate the two processes in both space and time. When used in combination, however, their individual strengths synergize. fMRI analyses can be used to guide and constrain the localization of EEG signals (Liu, Bai, & Pérez-Edgar, 2019), and new machine learning approaches can be used to identify common features across the two modalities (Cichy & Oliva, 2020). Future work in the characterization of anxiety-relevant neural circuitry will likely benefit from these multimodal approaches (Filippi, Valadez, Fox, & Pine, 2022). Ultimately, this work may lead to the discovery of new and better neural measures that may enhance our ability to make clinical predictions and may highlight novel targets for treatment (Insel et al., 2010).
Key points.
Behavioral inhibition is a temperament that can be identified in infancy.
Young children with the temperament of behavioral inhibition are vigilant of novelty and withdraw from social interaction.
There is an increased risk of development of anxiety disorders in young children with the temperament of behavioral inhibition.
We provide a framework and model for understanding the links between this temperament and the emergence of anxiety.
Acknowledgments
Figures 1 and 2 are reprinted by permission of Elsevier from Understanding the emergence of social anxiety in children with behavioral inhibition, by Fox et al. Biological Psychiatry, 89(7), 681–689, the Copyright year 2020 by the Society of Biological Psychiatry. The authors have declared that they have no competing or potential conflicts of interest.
Footnotes
Conflict of interest statement: No conflicts declared.
Although DMC theory uses the terms ‘proactive’ and ‘reactive’ (Braver, 2012), we instead use the more inclusive terms ‘planful’ and ‘automatic’ when referring to the DDC framework (Fox et al., 2021). This is done to recognize that both proactive control and task switching are negatively associated with anxiety among youth with a history of BI, whereas both reactive control and inhibitory control are positively associated with anxiety among these youth (see Figure 1). In Figure 2 we present hypothetical attentional behavior of (A) children high in behavioral inhibition (BI) and (B) children without BI in response to a novel or salient stimulus in a goal-directed setting.
References
- Aktar E, Majdandžić M, de Vente W, & Bögels SM (2013). The interplay between expressed parental anxiety and infant behavioural inhibition predicts infant avoidance in a social referencing paradigm: Expressed parental anxiety and infant behavioural inhibition. Journal of Child Psychology and Psychiatry, 54, 144–156. [DOI] [PubMed] [Google Scholar]
- Aktar E, Majdandžić M, de Vente W, & Bögels SM (2014). Parental social anxiety disorder prospectively predicts toddlers’ fear/avoidance in a social referencing paradigm. Journal of Child Psychology and Psychiatry, 55, 77–87. [DOI] [PubMed] [Google Scholar]
- Aktar E, Van Bockstaele B, Pérez-Edgar K, Wiers RW, & Bögels SM (2019). Intergenerational transmission of attentional bias and anxiety. Developmental Science, 22, e12772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arnsten AFT (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature Reviews Neuroscience, 10, 410–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balkaya M, Cheah CS, Yu J, Hart CH, & Sun S (2018). Maternal encouragement of modest behavior, temperamental shyness, and anxious withdrawal linkages to Chinese American children’s social adjustment: A moderated mediation analysis. Social Development, 27, 876–890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Banica I, Sandre A, & Weinberg A (2019). Overprotective/authoritarian maternal parenting is associated with an enhanced error-related negativity (ERN) in emerging adult females. International Journal of Psychophysiology, 137, 12–20. [DOI] [PubMed] [Google Scholar]
- Bar-Haim Y, Fox NA, Benson B, Guyer AE, Williams A, Nelson EE, …. & Ernst M (2009). Neural correlates of reward processing in adolescents with a history of inhibited temperament. Psychological Science, 20, 1009–1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barker TV, Reeb-Sutherland B, Degnan KA, Walker OL, Chronis-Tuscano A, Henderson HA, … & Fox NA (2015). Contextual startle responses moderate the relation between behavioral inhibition and anxiety in middle childhood. Psychophysiology, 52, 1544–1549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bayer JK, Brown A, Prendergast LA, Bretherton L, Hiscock H,Mihalopoulos C,. ….&Rapee RM(2022).Follow-up of the cool little kids translational trial into middle childhood. Journal of Child Psychology and Psychiatry, 63, 88–98. [DOI] [PubMed] [Google Scholar]
- Bayer JK, Prendergast LA, Brown A, Bretherton L, Hiscock H, Nelson-Lowe M, … & Rapee RM (2021). Prediction of clinical anxious and depressive problems in mid childhood amongst temperamentally inhibited preschool children: A population study. European Child and Adolescent Psychiatry. [cited 2022 Mar 16]. 10.1007/s00787-021-01857-9 [DOI] [PubMed] [Google Scholar]
- Beatty PJ, Buzzell GA, Roberts DM, & McDonald CG (2020). Contrasting time and frequency domains: ERN and induced theta oscillations differentially predict post-error behavior. Cognitive, Affective, & Behavioral Neuroscience, 20, 636–647. [DOI] [PubMed] [Google Scholar]
- Belsky J, Rha JH, & Park SY (2000). Exploring reciprocal parent and child effects in the case of child inhibition in US and Korean samples. International Journal of Behavioral Development, 24, 338–347. [Google Scholar]
- Bernier A, Carlson SM, Deschênes M, & Matte-Gagné C (2012). Social factors in the development of early executive functioning: A closer look at the caregiving environment. Developmental Science, 15, 12–24. [DOI] [PubMed] [Google Scholar]
- Biederman J, Rosenbaum JF, Bolduc-murphy EA, Faraone SV, Chaloff J, Hirshfeld DR, & Kagan J (1993). A 3-year follow-up of children with and without behavioral inhibition. Journal of the American Academy of Child & Adolescent Psychiatry, 32, 814–821. [DOI] [PubMed] [Google Scholar]
- Blair C (2010). Stress and the development of self-regulation in context. Child Development Perspectives, 4, 181–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Botvinick MM, Braver TS, Barch DM, Carter CS, & Cohen JD (2001). Conflict monitoring and cognitive control. Psychological Review, 108, 624–652. [DOI] [PubMed] [Google Scholar]
- Braver TS (2012). The variable nature of cognitive control: A dual mechanisms framework. Trends in Cognitive Sciences, 16, 106–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braver TS, Paxton JL, Locke HS, & Barch DM (2009). Flexible neural mechanisms of cognitive control within human prefrontal cortex. Proceedings of the National Academy of Sciences of the United States of America, 106, 7351–7356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooker RJ, & Buss KA (2014). Harsh parenting and fearfulness in toddlerhood interact to predict amplitudes of preschool error-related negativity. Developmental Cognitive Neuroscience, 9, 148–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burstein M, & Ginsburg GS (2010). The effect of parental modeling of anxious behaviors and cognitions in school-aged children: An experimental pilot study. Behaviour Research and Therapy, 48, 506–515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss AH, & Plomin R (1984). Temperament: Early developing personality traits (196 p.). London: Psychology Press. [Google Scholar]
- Buss C, Davis EP, Shahbaba B, Pruessner JC, Head K, & Sandman CA (2012). Maternal cortisol over the course of pregnancy and subsequent child amygdala and hippocampus volumes and affective problems. Proceedings of the National Academy of Sciences of the United States of America, 109, E1312–E1319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss KA (2011). Which fearful toddlers should we worry about? Context, fear regulation, and anxiety risk. Developmental Psychology, 47, 804–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss KA, Cho S, Morales S, McDoniel M, Webb AF, Schwartz A, … & Teti DM (2020). Toddler dysregulated fear predicts continued risk for social anxiety symptoms in early adolescence. Development and Psychopathology, 33, 252–263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss KA, Davis EL, Ram N, & Coccia M (2018). Dysregulated fear, social inhibition, and respiratory sinus arrhythmia: A replication and extension. Child Development, 89, e214–e228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss KA, & McDoniel ME (2016). Improving the prediction of risk for anxiety development in temperamentally fearful children. Current Directions in Psychological Science, 25, 14–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss KA, Zhou AM, & Trainer A (2021). Bidirectional effects of toddler temperament and maternal overprotection on maternal and child anxiety symptoms across preschool. Depression and Anxiety, 38, 1201–1210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buzzell GA, Barker TV, Troller-Renfree SV, Bernat EM, Bowers ME, Morales S, & Fox NA (2019). Adolescent cognitive control, theta oscillations, and social observation. NeuroImage, 198, 13–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buzzell GA, Troller-Renfree SV, Barker TV, Bowman LC, Chronis-Tuscano A, Henderson HA, … & Fox NA (2017). A neurobehavioral mechanism linking behaviorally inhibited temperament and later adolescent social anxiety. Journal of the American Academy of Child & Adolescent Psychiatry, 56, 1097–1105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buzzell GA, Troller-Renfree SV, Morales S, & Fox NA (2018). Relations between behavioral inhibition, cognitive control, and anxiety: Novel insights provided by parsing subdomains of cognitive control. In Pérez-Edgar K & Fox NA (Eds.), Behavioral inhibition: Integrating theory, research, and clinical perspectives [Internet] (pp. 213–235). Cham: Springer International Publishing. [Google Scholar]
- Calkins SD, Fox NA, & Marshall TR (1996). Behavioral and physiological antecedents of inhibited and uninhibited behavior. Child Development, 67, 523–540. [PubMed] [Google Scholar]
- Carlo G, Cheah CSL, Conejo LD, & Cho HS (2022). The social development of immigrant children: A focus on Asian and Latino/a children in the United States. In Smith PK & Hart G (Eds.), The Wiley-Blackwell handbook of childhood social development (3rd edn, pp. 161–180). New York, NY: Wiley-Blackwell. [Google Scholar]
- Cavanagh JF, & Frank MJ (2014). Frontal theta as a mechanism for cognitive control. Trends in Cognitive Sciences, 18, 414–421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cavigelli SA, & McClintock MK (2003). Fear of novelty in infant rats predicts adult corticosterone dynamics and an early death. Proceedings of the National Academy of Sciences of the United States of America, 100, 16131–16136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cellier D, Riddle J, Petersen I, & Hwang K (2021). The development of theta and alpha neural oscillations from ages 3 to 24 years. Developmental Cognitive Neuroscience, 50, 100969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen X (2018). Culture, temperament, and social and psychological adjustment. Developmental Review, 50, 42–53. [Google Scholar]
- Chen X, Cen G, Li D, & He Y (2005). Social functioning and adjustment in Chinese children: The imprint of historical time. Child Development, 76, 182–195. [DOI] [PubMed] [Google Scholar]
- Chen X, Chen H, Li D, & Wang L (2009). Early childhood behavioral inhibition and social and school adjustment in Chinese children: A 5-year longitudinal study. Child Development, 80, 1692–1704. [DOI] [PubMed] [Google Scholar]
- Chen X, & French DC (2008). Children’s social competence in cultural context. Annual Review of Psychology, 59, 591–616. [DOI] [PubMed] [Google Scholar]
- Chen X, Fu R, Li D, Chen H, Wang Z, & Wang L (2021). Behavioral inhibition in early childhood and adjustment in late adolescence in China. Child Development, 92, 994–1010. [DOI] [PubMed] [Google Scholar]
- Chen X, Hastings PD, Rubin KH, Chen H, Cen G, & Stewart SL (1998). Child-rearing attitudes and behavioral inhibition in Chinese and Canadian toddlers: A cross-cultural study. Developmental Psychology, 34, 677. [DOI] [PubMed] [Google Scholar]
- Chen X, Rubin KH, & Li B (1995). Social and school adjustment of shy and aggressive children in China. Development and Psychopathology, 7, 337–349. [Google Scholar]
- Chen X, Wang L, & Wang Z (2009). Shyness-sensitivity and social, school, and psychological adjustment in rural migrant and urban children in China. Child Development, 80, 1499–1513. [DOI] [PubMed] [Google Scholar]
- Chess S, & Thomas A (1977). Temperamental individuality from childhood to adolescence. Journal of the American Academy of Child Psychiatry, 16, 218–226. [DOI] [PubMed] [Google Scholar]
- Chevalier N, James TD, Wiebe SA, Nelson JM, & Espy KA (2014). Contribution of reactive and proactive control to children’s working memory performance: Insight from item recall durations in response sequence planning. Developmental Psychology, 50, 1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chevalier N, Martis SB, Curran T, & Munakata Y (2015). Metacognitive processes in executive control development: The case of reactive and proactive control. Journal of Cognitive Neuroscience, 27, 1125–1136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choate ML, Pincus DB, Eyberg SM, & Barlow DH (2005). Parent–child interaction therapy for treatment of separation anxiety disorder in young children: A pilot study. Cognitive and Behavioral Practice, 12, 126–135. [Google Scholar]
- Chronis-Tuscano A, Degnan KA, Pine DS, Pérez-Edgar K, Henderson HA, Diaz Y, et al. (2009). Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. Journal of the American Academy of Child & Adolescent Psychiatry, 48, 928–935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chronis-Tuscano A, Novick DR, Danko CM, Smith KA, Wagner NJ, Wang CH, & Rubin KH (2022). Early intervention for inhibited young children: A randomized controlled trial comparing the Turtle Program and Cool Little Kids. Journal of Child Psychology and Psychiatry, 63, 273–281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cichy RM, & Oliva A (2020). A M/EEG-fMRI Fusion Primer: Resolving human brain responses in space and time. Neuron, 107, 772–781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clauss JA, & Blackford JU (2012). Behavioral inhibition and risk for developing social anxiety disorder: A meta-analytic study. Journal of the American Academy of Child and Adolescent Psychiatry, 51, 1066–1075.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen JD, Barch DM, Carter C, & Servan-Schreiber D (1999). Context-processing deficits in schizophrenia: Converging evidence from three theoretically motivated cognitive tasks. Journal of Abnormal Psychology, 108, 120. [DOI] [PubMed] [Google Scholar]
- Coplan RJ, Schneider BH, Matheson A, & Graham A (2010). ‘Play skills’ for shy children: Development of a social skills facilitated play early intervention program for extremely inhibited preschoolers. Infant and Child Development, 19, 223–237. [Google Scholar]
- Davis M (1992). The role of the amygdala in fear and anxiety. Annual Review of Neuroscience, 15, 353–375. [DOI] [PubMed] [Google Scholar]
- Davis M (1998). Are different parts of the extended amygdala involved in fear versus anxiety? Biological Psychiatry, 44, 1239–1247. [DOI] [PubMed] [Google Scholar]
- de Lijster JM, Dierckx B, Utens EM, Verhulst FC, Zieldorff C, Dieleman GC, & Legerstee JS (2017). The age of onset of anxiety disorders: A meta-analysis. The Canadian Journal of Psychiatry, 62, 237–246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Rosnay M, Cooper PJ, Tsigaras N, & Murray L (2006). Transmission of social anxiety from mother to infant: An experimental study using a social referencing paradigm. Behaviour Research and Therapy, 44, 1165–1175. [DOI] [PubMed] [Google Scholar]
- Degnan KA, Almas AN, & Fox NA (2010). Temperament and the environment in the etiology of childhood anxiety: Temperament, anxiety, and environment. Journal of Child Psychology and Psychiatry, 51, 497–517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Degnan KA, Almas AN, Henderson HA, Hane AA, Walker OL, & Fox NA (2014). Longitudinal trajectories of social reticence with unfamiliar peers across early childhood. Developmental Psychology, 50, 2311–2323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Degnan KA, Henderson HA, Fox NA, & Rubin KH (2008). Predicting social wariness in middle childhood: The moderating roles of child care history, maternal personality and maternal behavior. Social Development, 17, 471–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delawalla Z, Csernansky JG, & Barch DM (2008). Pre-frontal cortex function in nonpsychotic siblings of individuals with schizophrenia. Biological Psychiatry, 63, 490–497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ding X, Chen X, Fu R, Li D, & Liu J (2020). Relations of shyness and unsociability with adjustment in migrant and non-migrant children in urban China. Journal of Abnormal Child Psychology, 48, 289–300. [DOI] [PubMed] [Google Scholar]
- Doey L, Coplan RJ, & Kingsbury M (2014). Bashful boys and coy girls: A review of gender differences in childhood shyness. Sex Roles, 70, 255–266. [Google Scholar]
- Donoghue T, Haller M, Peterson EJ, Varma P, Sebastian P, Gao R, … & Voytek B (2020). Parameterizing neural power spectra into periodic and aperiodic components. Nature Neuroscience, 23, 1655–1665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dyson MW, Klein DN, Olino TM, Dougherty LR, & Durbin CE (2011). Social and non-social behavioral inhibition in preschool-age children: Differential associations with parent-reports of temperament and anxiety. Child Psychiatry & Human Development, 42, 390–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eley TC, McAdams TA, Rijsdijk FV, Lichtenstein P, Narusyte J, Reiss D, … & Neiderhiser JM (2015). The intergenerational transmission of anxiety: A children-of-twins study. American Journal of Psychiatry, 172, 630–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Else-Quest NM, Hyde JS, Goldsmith HH, & Van Hulle CA (2006). Gender differences in temperament: A meta-analysis. Psychological Bulletin, 132, 33–72. [DOI] [PubMed] [Google Scholar]
- Filippi CA, Ravi S, Bracy M, Winkler A, Sylvester CM, Pine DS, & Fox NA (2021). Amygdala functional connectivity and negative reactive temperament at age 4 months. Journal of the American Academy of Child & Adolescent Psychiatry, 60, 1137–1146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Filippi CA, Valadez EA, Fox NA, & Pine DS (2022). Temperamental risk for anxiety: Emerging work on the infant brain and later neurocognitive development. Current Opinion in Behavioral Sciences, 44, 101105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox NA, Buzzell GA, Morales S, Valadez EA, Wilson M, & Henderson HA (2021). Understanding the emergence of social anxiety in children with behavioral inhibition. Biological Psychiatry, 89, 681–689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox NA, & Calkins SD (2003). The development of self-control of emotion: Intrinsic and extrinsic influences. Motivation and Emotion, 27, 7–26. [Google Scholar]
- Fox NA, Henderson HA, Marshall PJ, Nichols KE, & Ghera MM (2005). Behavioral inhibition: Linking biology and behavior within a developmental framework. Annual Review of Psychology, 56, 235–262. [DOI] [PubMed] [Google Scholar]
- Fox NA, Henderson HA, Rubin KH, Calkins SD, & Schmidt LA (2001). Continuity and discontinuity of behavioral inhibition and exuberance: Psychophysiological and behavioral influences across the first four years of life. Child Development, 72, 1–21. [DOI] [PubMed] [Google Scholar]
- Fox NA, Snidman N, Haas SA, Degnan KA, & Kagan J (2015). The relations between reactivity at 4 months and behavioral inhibition in the second year: Replication across three independent samples. Infancy, 20, 98–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gao D, Hart CH, Cheah CS, Balkaya M, Vu KT, & Liu J (2021). Chinese American children’s temperamental shyness and responses to peer victimization as moderated by maternal praise. Journal of Family Psychology, 35, 680–690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garcia Coll C, Kagan J, & Reznick JS (1984). Behavioral inhibition in young children. Child Development, 55, 1005–1019. [Google Scholar]
- Gauvain M (2001). The social context of cognitive development (p. 276). New York, NY: Guilford Press. [Google Scholar]
- Gazelle H, & Rubin KH (2010). Social anxiety in childhood: Bridging developmental and clinical perspectives. New Directions for Child and Adolescent Development, 2010, 1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ginsburg GS, Siqueland L, Masia-Warner C, & Hedtke KA (2004). Anxiety disorders in children: Family matters. Cognitive and Behavioral Practice, 11, 28–43. [Google Scholar]
- Greenfield PM, Suzuki LK, & Rothstein-Fisch C (2006). Cultural pathways through human development. In Renninger KA, Sigel IE, Damon W, & Lerner RM (Eds.), Handbook of child psychology: Child psychology in practice (vol. 4, 6th edn, pp. 655–699). Hoboken, NJ: John Wiley & Sons. [Google Scholar]
- Gudiño OG, & Lau AS (2010). Parental cultural orientation, shyness, and anxiety in hispanic children: An exploratory study. Journal of Applied Developmental Psychology, 31, 202–210. [Google Scholar]
- Guyer AE, Benson B, Choate VR, Bar-Haim Y, Pérez-Edgar K, Jarcho JM, … & Nelson EE (2014). Lasting associations between early-childhood temperament and late-adolescent reward-circuitry response to peer feedback. Development and Psychopathology, 26, 229–243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guyer AE, Nelson EE, Perez-Edgar K, Hardin MG, Roberson-Nay R, Monk CS, … & Ernst M (2006). Striatal functional alteration in adolescents characterized by early childhood behavioral inhibition. Journal of Neuroscience, 26, 6399–6405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hajcak G, McDonald N, & Simons RF (2003). Anxiety and error-related brain activity. Biological Psychology, 64, 77–90. [DOI] [PubMed] [Google Scholar]
- Hane AA, Cheah C, Rubin KH, & Fox NA (2008). The role of maternal behavior in the relation between shyness and social reticence in early childhood and social withdrawal in middle childhood. Social Development, 17, 795–811. [Google Scholar]
- Heinrichs N, Rapee RM, Alden LA, Bögels S, Hofmann SG, Oh KJ, & Sakano Y (2006). Cultural differences in perceived social norms and social anxiety. Behaviour Research and Therapy, 44, 1187–1197. [DOI] [PubMed] [Google Scholar]
- Helfinstein SM, Benson B, Pérez-Edgar K, Bar-Haim Y, Detloff A, Pine DS, & Ernst M (2011). Striatal responses to negative monetary outcomes differ between temperamentally inhibited and non-inhibited adolescents. Neuropsychologia, 49, 479–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henderson HA (2010). Electrophysiological correlates of cognitive control and the regulation of shyness in children. Developmental Neuropsychology, 35, 177–193. [DOI] [PubMed] [Google Scholar]
- Henderson HA, Pine DS, & Fox NA (2015). Behavioral inhibition and developmental risk: A dual-processing perspective. Neuropsychopharmacology, 40, 207–224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henderson HA, & Wilson MJ (2017). Attention processes underlying risk and resilience in behaviorally inhibited children. Current Behavioral Neuroscience Reports, 4, 99–106. [Google Scholar]
- Hirshfeld-Becker DR, Biederman J, Henin A, Faraone SV, Davis S, Harrington K, & Rosenbaum JF (2007). Behavioral inhibition in preschool children at risk is a specific predictor of middle childhood social anxiety: A five-year follow-up. Journal of Developmental & Behavioral Pediatrics, 28, 225–233. [DOI] [PubMed] [Google Scholar]
- Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, & Wang P (2010). Research Domain Criteria (RDoC): Toward a new classification framework for research on mental disorders. American Journal of Psychiatry, 167, 748–751. [DOI] [PubMed] [Google Scholar]
- Jarcho JM, Fox NA, Pine DS, Etkin A, Leibenluft E, Shechner T, & Ernst M (2013). The neural correlates of emotion-based cognitive control in adults with early childhood behavioral inhibition. Biological Psychology, 92, 306–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kagan ER, Peterman JS, Carper MM, & Kendall PC (2016). Accommodation and treatment of anxious youth. Depress Anxiety, 33, 840–847. [DOI] [PubMed] [Google Scholar]
- Kagan J, Reznick JS, Clarke C, Snidman N, & Garcia-Coll C (1984). Behavioral inhibition to the unfamiliar. Child Development, 55, 2212–2225. [Google Scholar]
- Kagan J, Reznick JS, & Snidman N (1987). The physiology and psychology of behavioral inhibition in children. Child Development, 58, 1459. [PubMed] [Google Scholar]
- Kagan J, & Snidman N (1991a). Infant predictors of inhibited and uninhibited profiles. Psychological Science, 2, 40–44. [Google Scholar]
- Kagan J, & Snidman N (1991b). Temperamental factors in human development. American Psychologist, 46, 856. [DOI] [PubMed] [Google Scholar]
- Kalin NH, & Shelton SE (2003). Nonhuman primate models to study anxiety, emotion regulation, and psychopathology. Annals of the New York Academy of Sciences, 1008, 189–200. [DOI] [PubMed] [Google Scholar]
- Kerr M (2001). Culture as a context for temperament: Suggestions from the life courses of shy Swedes and Americans. In Wachs TD & Kohnstamm GA (Eds.), Temperament in context (pp. 139–152). Mahwah, NJ: Erlbaum. [Google Scholar]
- Kiel EJ, Aaron EM, Risley SM, & Luebbe AM (2021). Transactional relations between maternal anxiety and toddler anxiety risk through toddler-solicited comforting behavior. Depression and Anxiety, 38, 1267–1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiel EJ, & Buss KA (2011). Prospective relations among fearful temperament, protective parenting, and social withdrawal: The role of maternal accuracy in a moderated mediation framework. Journal of Abnormal Child Psychology, 39, 953–966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kochanska G (1991). Patterns of inhibition to the unfamiliar in children of normal and affectively ill mothers. Child Development, 62, 250–263. [DOI] [PubMed] [Google Scholar]
- Lahat A, Lamm C, Chronis-Tuscano A, Pine DS, Henderson HA, & Fox NA (2014). Early behavioral inhibition and increased error monitoring predict later social phobia symptoms in childhood. Journal of the American Academy of Child & Adolescent Psychiatry, 53, 447–455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lamm C, Walker OL, Degnan KA, Henderson HA, Pine DS, McDermott JM, & Fox NA (2014). Cognitive control moderates early childhood temperament in predicting social behavior in 7-year-old children: An ERP study. Developmental Science, 17, 667–681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lebowitz ER, Omer H, Hermes H, & Scahill L (2014). Parent training for childhood anxiety disorders: The SPACE program. Cognitive and Behavioral Practice, 21, 456–469. [Google Scholar]
- Lebowitz ER, Woolston J, Bar-Haim Y, Calvocoressi L, Dauser C, Warnick E, … & Leckman JF (2013). Family accommodation in pediatric anxiety disorders. Depression and Anxiety, 30, 47–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ledoux J (1996). The emotional brain: The mysterious underpinnings of emotional life. New York, NY: Simon and Schuster. [Google Scholar]
- Lewis-Morrarty E, Degnan KA, Chronis-Tuscano A, Rubin KH, Cheah CSL, Pine DS, … & Fox NA (2012). Maternal over-control moderates the association between early childhood behavioral inhibition and adolescent social anxiety symptoms. Journal of Abnormal Child Psychology, 40, 1363–1373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu P, Bai X, & Pérez-Edgar KE (2019). Integrating high-density ERP and fMRI measures of face-elicited brain activity in 9–12-year-old children: An ERP source localization study. NeuroImage, 184, 599–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lopez-Garcia P, Lesh TA, Salo T, Barch DM, MacDonald AW, Gold JM, & Carter CS (2016). The neural circuitry supporting goal maintenance during cognitive control: A comparison of expectancy AX-CPT and dot probe expectancy paradigms. Cognitive, Affective & Behavioral Neuroscience, 16, 164–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucenet J, & Blaye A (2014). Age-related changes in the temporal dynamics of executive control: A study in 5-and 6-year-old children. Frontiers in Psychology, 5, 831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacLeod C, Mathews A, & Tata P (1986). Attentional bias in emotional disorders. Journal of Abnormal Psychology, 95, 15–20. [DOI] [PubMed] [Google Scholar]
- Marshall PJ, Reeb BC, & Fox NA (2009). Electrophysiological responses to auditory novelty in temperamentally different 9-month-old infants. Developmental Science, 12, 568–582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall PJ, & Stevenson-Hinde J (2001). Behavioural inhibition: Physiological correlates. In Crozier WR & Alden LE (Eds.), International handbook of social anxiety: Concepts, research and interventions relating to the self and shyness (pp. 53–76). Westport, CT: Wiley. [Google Scholar]
- McDermott JM, Pérez-Edgar K, Henderson HA, Chronis-Tuscano A, Pine DS, & Fox NA (2009). A history of childhood behavioral inhibition and enhanced response monitoring in adolescence are linked to clinical anxiety. Biological Psychiatry, 65, 445–448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McSweeney M, Morales S, Valadez EA, Buzzell GA, & Fox NA (2021). Longitudinal age- and sex-related change in background aperiodic activity during early adolescence. Developmental Cognitive Neuroscience, 52, 101035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer A, Carlton C, Chong LJ, & Wissemann K (2019). The presence of a controlling parent is related to an increase in the error-related negativity in 5–7 year-old children. Journal of Abnormal Child Psychology, 47, 935–945. [DOI] [PubMed] [Google Scholar]
- Meyer A, & Gawlowska M (2017). Evidence for specificity of the impact of punishment on error-related brain activity in high versus low trait anxious individuals. International Journal of Psychophysiology, 120, 157–163. [DOI] [PubMed] [Google Scholar]
- Milad MR, & Quirk GJ (2012). Fear extinction as a model for translational neuroscience: Ten years of progress. Annual Review of Psychology, 63, 129–151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller EK, & Cohen JD (2001). An integrative theory of prefrontal cortex function. Annual Review of Neuroscience, 24, 167–202. [DOI] [PubMed] [Google Scholar]
- Mogg K, Wilson KA, Hayward C, Cunning D, & Bradley BP (2012). Attentional biases for threat in at-risk daughters and mothers with lifetime panic disorder. Journal of Abnormal Psychology, 121, 852–862. [DOI] [PubMed] [Google Scholar]
- Montagner R, Mogg K, Bradley BP, Pine DS, Czykiel MS, Miguel EC, et al. (2015). Attentional bias to threat in children at-risk for emotional disorders: Role of gender and type of maternal emotional disorder. European Child & Adolescent Psychiatry, 25, 735–742. [DOI] [PubMed] [Google Scholar]
- Morales S, Beekman C, Blandon AY, Stifter CA, & Buss KA (2015). Longitudinal associations between temperament and socioemotional outcomes in young children: The moderating role of RSA and gender. Developmental Psychobiology, 57, 105–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morales S, & Bowers ME (2022). Time-frequency analysis methods and their application in developmental EEG data. Developmental Cognitive Neuroscience, 101, 67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morales S, Bowers ME, Leach SC, Buzzell GA, Fifer W, Elliott AJ, et al. (2022). Time–frequency dynamics of error monitoring in childhood: An EEG study. Developmental Psychobiology, 64, e22215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morales S, Brown KM, Taber-Thomas BC, LoBue V, Buss KA, & Pérez-Edgar KE (2017). Maternal anxiety predicts attentional bias towards threat in infancy. Emotion, 17, 874–883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morales S, & Fox NA (2019). A neuroscience perspective on emotional development. In LoBue V, Pérez-Edgar K, & Buss KA (Eds.), Handbook of emotional development (pp. 57–82). Cham, Switzerland: Springer. [Google Scholar]
- Morales S, Pérez-Edgar KE, & Buss KA (2014). Attention biases towards and away from threat mark the relation between early dysregulated fear and the later emergence of social withdrawal. Journal of Abnormal Child Psychology, 43, 1067–1078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan MA, Romanski LM, & LeDoux JE (1993). Extinction of emotional learning: Contribution of medial prefrontal cortex. Neuroscience Letters, 163, 109–113. [DOI] [PubMed] [Google Scholar]
- Munakata Y, Snyder HR, & Chatham CH (2012). Developing cognitive control three key transitions. Current Directions in Psychological Science, 21, 71–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray L, de Rosnay M, Pearson J, Bergeron C, Schofield E, Royal-Lawson M, & Cooper PJ (2008). Intergenerational transmission of social anxiety: The role of social referencing processes in infancy. Child Development, 79, 1049–1064. [DOI] [PubMed] [Google Scholar]
- Murray L, Pella JE, De Pascalis L, Arteche A, Pass L, Percy R, … & Cooper PJ (2014). Socially anxious mothers’ narratives to their children and their relation to child representations and adjustment. Development and Psychopathology, 26(4pt2), 1531–1546. [DOI] [PubMed] [Google Scholar]
- NIMH. (2022). Goal 2: Examine mental illness trajectories across the lifespan [Internet]. Bethesda, MD: National Institute of Mental Health (NIMH). [cited 2022 Mar 16]. Available from: https://www.nimh.nih.gov/about/strategic-planning-reports/goal-2-examine-mental-illness-trajectories-across-the-lifespan [Google Scholar]
- Nozadi S, Troller-Renfree S, White L, Frenkel T, Degnan K, Bar-Haim Y, … & Fox NA (2016). The moderating role of attention biases to threat on the link between behavioral inhibition and anxiety in children. Journal of Experimental Psychopathology, 7, 451–465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ostlund B, Donoghue T, Anaya B, Gunther KE, Karalunas SL, Voytek B, & Pérez-Edgar KE (2022). Spectral parameterization for studying neurodevelopment: How and why. Developmental Cognitive Neuroscience, 54, 101073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Edgar K, Bar-Haim Y, McDermott JM, Chronis-Tuscano A, Pine DS, & Fox NA (2010). Attention biases to threat and behavioral inhibition in early childhood shape adolescent social withdrawal. Emotion, 10, 349–357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Edgar K, LoBue V, & Buss KA (2021). From parents to children and back again: Bidirectional processes in the transmission and development of depression and anxiety. Depression and Anxiety, 38, 1198–1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Edgar K, Reeb-Sutherland BC, McDermott JM, White LK, Henderson HA, Degnan KA, et al. (2011). Attention biases to threat link behavioral inhibition to social withdrawal over time in very young children. Journal of Abnormal Child Psychology, 39, 885–895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Edgar K, Roberson-Nay R, Hardin MG, Poeth K, Guyer AE, Nelson EE, … & Ernst M (2007). Attention alters neural responses to evocative faces in behaviorally inhibited adolescents. NeuroImage, 35, 1538–1546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Edgar KE, & Guyer AE (2014). Behavioral inhibition: Temperament or prodrome? Current Behavioral Neuroscience Reports, 1, 182–190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phelps EA, Delgado MR, Nearing KI, & LeDoux JE (2004). Extinction learning in humans. Neuron, 43, 897–905. [DOI] [PubMed] [Google Scholar]
- Phelps EA, & LeDoux JE (2005). Contributions of the amygdala to emotion processing: From animal models to human behavior. Neuron, 48, 175–187. [DOI] [PubMed] [Google Scholar]
- Phelps RA, Brooker RJ, & Buss KA (2016). Toddlers’ dysregulated fear predicts delta–beta coupling during preschool. Developmental Cognitive Neuroscience, 17, 28–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poppe AB, Barch DM, Carter CS, Gold JM, Ragland JD, Silverstein SM, & MacDonald AW 3rd. (2016). Reduced frontoparietal activity in schizophrenia is linked to a specific deficit in goal maintenance: A multisite functional imaging study. Schizophrenia Bulletin, 42, 1149–1157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price NN, & Kiel EJ (2022). Maternal worry socialization and toddler inhibited temperament: Transactional associations and stability across time. Research on Child and Adolescent Psychopathology, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prior M, Sanson A, Oberklaid F, & Northam E (1987). Measurement of temperament in one to three year old children. International Journal of Behavioral Development, 10, 121–132. [Google Scholar]
- Qiu A, Anh TT, Li Y, Chen H, Rifkin-Graboi A, Broekman BF, … & Meaney MJ (2015). Prenatal maternal depression alters amygdala functional connectivity in 6-month-old infants. Translational Psychiatry, 5, e508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rankin Williams L, Degnan KA, Pérez-Edgar KE, Henderson HA, Rubin KH, Pine DS, … & Fox NA (2009). Impact of behavioral inhibition and parenting style on internalizing and externalizing problems from early childhood through adolescence. Journal of Abnormal Child Psychology, 37, 1063–1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rapee RM, Kennedy SJ, Ingram M, Edwards SL, & Sweeney L (2010). Altering the trajectory of anxiety in at-risk young children. American Journal of Psychiatry, 167, 1518–1525. [DOI] [PubMed] [Google Scholar]
- Rapee RM, Kim J, Wang J, Liu X, Hofmann SG, Chen J, … & Alden LE (2011). Perceived impact of socially anxious behaviors on individuals’ lives in Western and East Asian countries. Behavior Therapy, 42, 485–492. [DOI] [PubMed] [Google Scholar]
- Reeb-Sutherland BC, Rankin Williams L, Degnan KA, Pérez-Edgar K, Chronis-Tuscano A, Leibenluft E, … & Fox NA (2014). Identification of emotional facial expressions among behaviorally inhibited adolescents with lifetime anxiety disorders. Cognition & Emotion, 29, 372–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reeb-Sutherland BC, Vanderwert RE, Degnan KA, Marshall PJ, Pérez-Edgar K, Chronis-Tuscano A, … & Fox NA (2009). Attention to novelty in behaviorally inhibited adolescents moderates risk for anxiety. Journal of Child Psychology and Psychiatry, 50, 1365–1372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reznick JS, Kagan J, Snidman N, Gersten M, Baak K, & Rosenberg A (1986). Inhibited and uninhibited children: A follow-up study. Child Development, 57, 660–680. [Google Scholar]
- Rickman MD, & Davidson RJ (1994). Personality and behavior in parents of temperamentally inhibited and uninhibited children. Developmental Psychology, 30, 9. [Google Scholar]
- Riesel A, Weinberg A, Endrass T, Kathmann N, & Hajcak G (2012). Punishment has a lasting impact on error-related brain activity. Psychophysiology, 49, 239–247. [DOI] [PubMed] [Google Scholar]
- Rosenbaum JF, Biederman J, Gersten M, Hirshfeld DR, Meminger SR, Herman JB, … & Snidman N (1988). Behavioral inhibition in children of parents with panic disorder and agoraphobia: A controlled study. Archives of General Psychiatry, 45, 463–470. [DOI] [PubMed] [Google Scholar]
- Rosenbaum JF, Biederman J, Hirshfeld-Becker DR, Kagan J, Snidman N, Friedman D, … & Faraone SV (2000). A controlled study of behavioral inhibition in children of parents with panic disorder and depression. American Journal of Psychiatry, 157, 2002–2010. [DOI] [PubMed] [Google Scholar]
- Rubin KH, & Asendorpf JB (1993). Social withdrawal, inhibition, and shyness in childhood. Hillsdale, NJ: Erlbau. [Google Scholar]
- Rubin KH, Burgess KB, & Hastings PD (2002). Stability and social–behavioral consequences of toddlers’ inhibited temperament and parenting behaviors. Child Development, 73, 483–495. [DOI] [PubMed] [Google Scholar]
- Rubin KH, Coplan RJ, & Bowker JC (2009). Social withdrawal in childhood. Annual Review of Psychology, 60, 141–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin KH, Hastings PD, Stewart SL, Henderson HA, & Chen X (1997). The consistency and concomitants of inhibition: Some of the children, all of the time. Child Development, 68, 467–483. [PubMed] [Google Scholar]
- Rubin KH, Hemphill SA, Chen X, Hastings P, Sanson A, Coco AL, … & Cui L (2006). A cross-cultural study of behavioral inhibition in toddlers: East–West–North–South. International Journal of Behavioral Development, 30, 219–226. [Google Scholar]
- Rubin KH, Nelson LJ, Hastings P, & Asendorpf J (1999). The transaction between parents’ perceptions of their children’s shyness and their parenting styles. International Journal of Behavioral Development, 23, 937–957. [Google Scholar]
- Ryan SM, & Ollendick TH (2018). The interaction between child behavioral inhibition and parenting behaviors: Effects on internalizing and externalizing symptomology. Clinical Child and Family Psychology Review, 21, 320–339. [DOI] [PubMed] [Google Scholar]
- Rydell AM, Thorell L, & Bohlin G (2004). Two types of inhibitory control: Predictive relations to social functioning. International Journal of Behavioral Development, 28, 193–203. [Google Scholar]
- Ryman SG, El Shaikh AA, Shaff NA, Hanlon FM, Dodd AB, Wertz CJ, … & Mayer AR (2019). Proactive and reactive cognitive control rely on flexible use of the ventro-lateral prefrontal cortex. Human Brain Mapping, 40, 955–966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sandstrom A, Uher R, & Pavlova B (2020). Prospective association between childhood behavioral inhibition and anxiety: A meta-analysis. Journal of Abnormal Child Psychology, 48, 57–66. [DOI] [PubMed] [Google Scholar]
- Schwartz CE, Kunwar PS, Greve DN, Kagan J, Snidman NC, & Bloch RB (2011). A phenotype of early infancy predicts reactivity of the amygdala in male adults. Molecular Psychiatry, 17, 1042–1050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz CE, Wright CI, Shin LM, Kagan J, & Rauch SL (2003). Inhibited and uninhibited infants “grown up”: Adult amygdalar response to novelty. Science, 300, 1952–1953. [DOI] [PubMed] [Google Scholar]
- Sentse M, Veenstra R, Lindenberg S, Verhulst FC, & Ormel J (2009). Buffers and risks in temperament and family for early adolescent psychopathology: Generic, conditional, or domain-specific effects? The trails study. Developmental Psychology, 45, 419–430. [DOI] [PubMed] [Google Scholar]
- Smith AK, Rhee SH, Corley RP, Friedman NP, Hewitt JK, & Robinson JL (2012). The magnitude of genetic and environmental influences on parental and observational measures of behavioral inhibition and shyness in toddlerhood. Behavior Genetics, 42, 764–777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Storch EA, Salloum A, Johnco C, Dane BF, Crawford EA, King MA, … & Lewin AB (2015). Phenomenology and clinical correlates of family accommodation in pediatric anxiety disorders. Journal of Anxiety Disorders, 35, 75–81. [DOI] [PubMed] [Google Scholar]
- Suarez GL, Morales S, Miller NV, Penela EC, Chronis-Tuscano A, Henderson HA, & Fox NA (2021). Examining a developmental pathway from early behavioral inhibition to emotion regulation and social anxiety: The moderating role of parenting. Developmental Psychology, 57, 1261–1273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang A, Crawford H, Morales S, Degnan KA, Pine DS, & Fox NA (2020). Infant behavioral inhibition predicts personality and social outcomes three decades later. Proceedings of the National Academy of Sciences of the United States of America, 117, 9800–9807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thai N, Taber-Thomas BC, & Pérez-Edgar KE (2016). Neural correlates of attention biases, behavioral inhibition, and social anxiety in children: An ERP study. Developmental Cognitive Neuroscience, 19, 200–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas A, Chess S, Birch HG, Hertzig ME, Korn S (1963). Behavioral individuality in early childhood. [Google Scholar]
- Thompson-Hollands J, Kerns CE, Pincus DB, & Comer JS (2014). Parental accommodation of child anxiety and related symptoms: Range, impact, and correlates. Journal of Anxiety Disorders, 28, 765–773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troller-Renfree SV, Buzzell GA, Pine DS, Henderson HA, & Fox NA (2019). Consequences of not planning ahead: Reduced proactive control moderates longitudinal relations between behavioral inhibition and anxiety. Journal of the American Academy of Child & Adolescent Psychiatry, 58, 768–775.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ullsperger M, Fischer AG, Nigbur R, & Endrass T (2014). Neural mechanisms and temporal dynamics of performance monitoring. Trends in Cognitive Sciences, 18, 259–267. [DOI] [PubMed] [Google Scholar]
- Unger K, Ackerman L, Chatham CH, Amso D, & Badre D (2016). Working memory gating mechanisms explain developmental change in rule-guided behavior. Cognition, 155, 8–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valadez EA, Morales S, Buzzell GA, Troller-Renfree SV, Henderson HA, Chronis-Tuscano A, … & Fox NA (2022). Development of proactive control and anxiety among behaviorally inhibited adolescents. Journal of the American Academy of Child and Adolescent Psychiatry [in press]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valadez EA, Troller-Renfree S, Buzzell GA, Henderson HA, Chronis-Tuscano A, Pine DS, & Fox NA (2021). Behavioral inhibition and dual mechanisms of anxiety risk: Disentangling neural correlates of proactive and reactive control. JCPP Advances, 1, e12022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valcan DS, Davis H, & Pino-Pasternak D (2018). Parental behaviours predicting early childhood executive functions: A meta-analysis. Educational Psychology Review, 30, 607–649. [Google Scholar]
- van Brakel AML, Muris P, Bögels SM, & Thomassen C (2006). A multifactorial model for the etiology of anxiety in non-clinical adolescents: Main and interactive effects of behavioral inhibition, attachment and parental rearing. Journal of Child and Family Studies, 15, 568–578. [Google Scholar]
- van Wouwe NC, Band GP, & Ridderinkhof KR (2011). Positive affect modulates flexibility and evaluative control. Journal of Cognitive Neuroscience, 23, 524–539. [DOI] [PubMed] [Google Scholar]
- Van Zalk N, & Kerr M (2011). Shy adolescents’ perceptions of parents’ psychological control and emotional warmth: Examining bidirectional links. Merrill-Palmer Quarterly, 57, 375–401. [Google Scholar]
- Vreeke LJ, Muris P, Mayer B, Huijding J, & Rapee RM (2013). Skittish, shielded, and scared: Relations among behavioral inhibition, overprotective parenting, and anxiety in native and non-native Dutch preschool children. Journal of Anxiety Disorders, 27, 703–710. [DOI] [PubMed] [Google Scholar]
- Vygotsky LS (1978). Mind in society: The development of higher psychological processes (p. 180). Cambridge, MA: Harvard University Press. [Google Scholar]
- West AE, & Newman DL (2007). Childhood behavioral inhibition and the experience of social anxiety in American Indian adolescents. Cultural Diversity and Ethnic Minority Psychology, 13, 197. [DOI] [PubMed] [Google Scholar]
- White LK, Degnan KA, Henderson HA, Pérez-Edgar K, Walker OL, Shechner T, … & Fox NA (2017). Developmental relations among behavioral inhibition, anxiety, and attention biases to threat and positive information. Child Development, 88, 141–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White LK, McDermott JM, Degnan KA, Henderson HA, & Fox NA (2011). Behavioral inhibition and anxiety: The moderating roles of inhibitory control and attention shifting. Journal of Abnormal Child Psychology, 39, 735–747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Windle M, & Lerner RM (1986). Reassessing the dimensions of temperamental individuality across the life span: The Revised Dimensions of Temperament Survey (DOTS-R). Journal of Adolescent Research, 1, 213–229. [Google Scholar]
- Wood JJ, McLeod BD, Sigman M, Hwang WC, & Chu BC (2003). Parenting and childhood anxiety: Theory, empirical findings, and future directions. Journal of Child Psychology and Psychiatry, 44, 134–151. [DOI] [PubMed] [Google Scholar]
- Xu Y, & Krieg A (2014). Shyness in Asian American children and the relation to temperament, parents’ acculturation, and psychosocial functioning. Infant and Child Development, 23, 333–342. [Google Scholar]
- Zeytinoglu S, Calkins SD, & Leerkes EM (2019). Maternal emotional support but not cognitive support during problem-solving predicts increases in cognitive flexibility in early childhood. International Journal of Behavioral Development, 43, 12–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeytinoglu S, Calkins SD, & Leerkes EM (2022). Autonomic profiles and self-regulation outcomes in early childhood. Developmental Science, 25, e13215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeytinoglu S, Calkins SD, Swingler MM, & Leerkes EM (2017). Pathways from maternal effortful control to child self-regulation: The role of maternal emotional support. Journal of Family Psychology, 31, 170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeytinoglu S, Neuman KJ, Degnan KA, Almas AN, Henderson H, Chronis-Tuscano A, & Fox NA (2022). Pathways from maternal shyness to adolescent social anxiety. Journal of Child Psychology and Psychiatry, 63, 342–349. [DOI] [PMC free article] [PubMed] [Google Scholar]