

Abstract
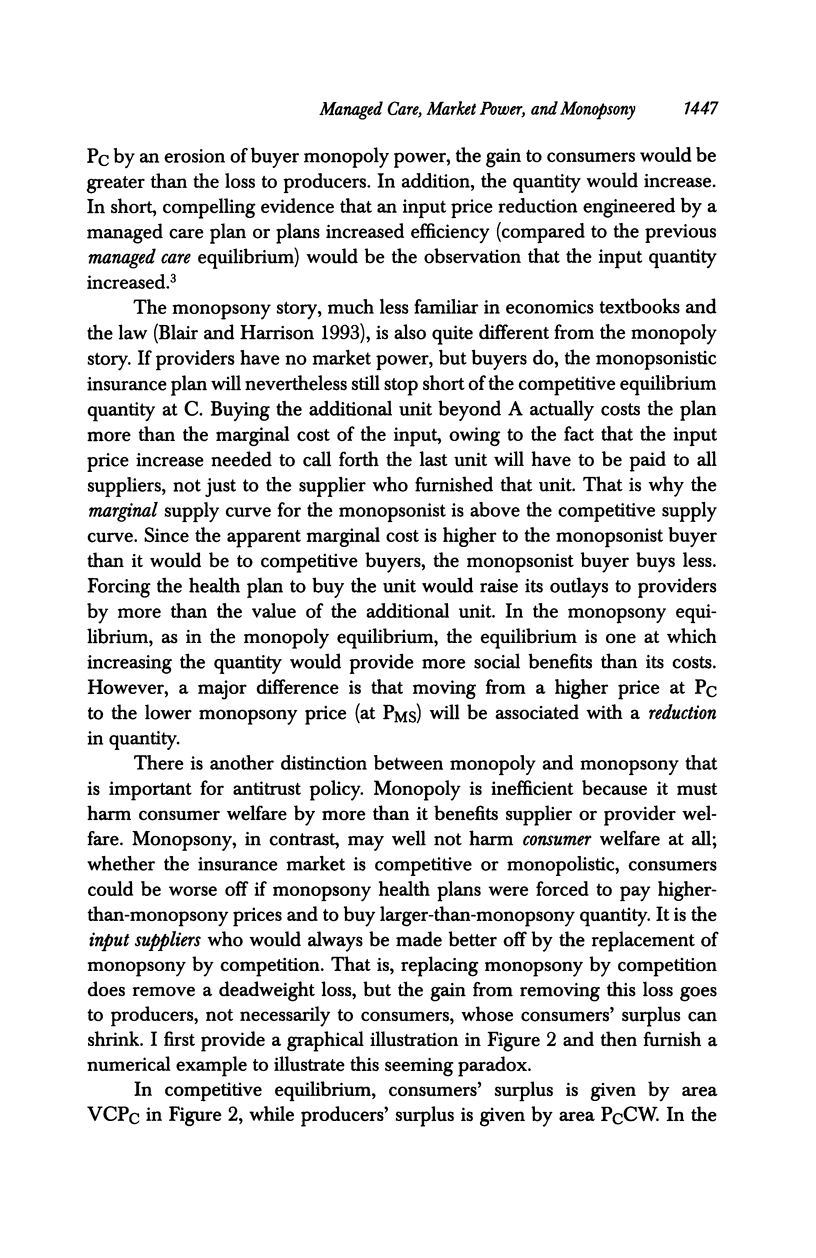
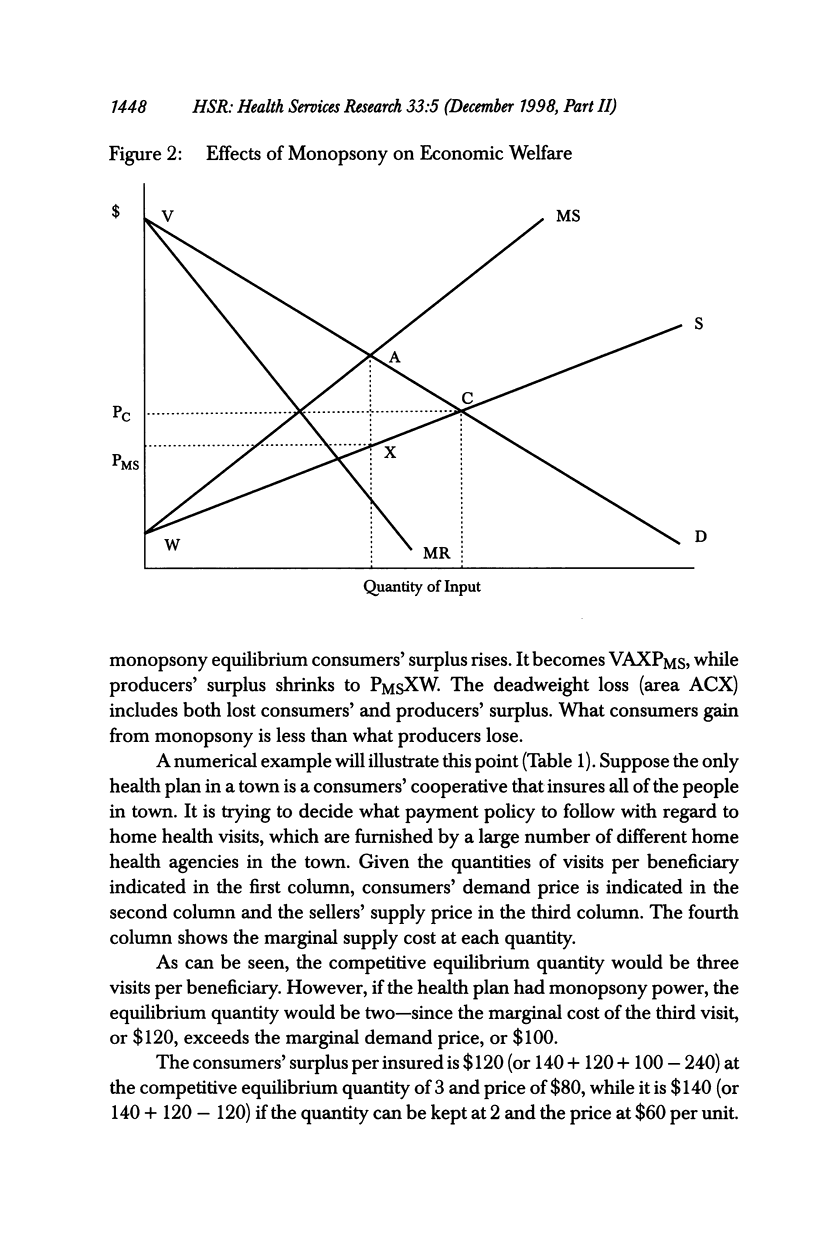
OBJECTIVE: To examine the theoretical possibility of monopsony behavior under managed care insurance. STUDY DESIGN: Use of microeconomic theory to examine how managed care plans with market power would be expected to behave, and effects of that behavior on consumer and supplier welfare. PRINCIPAL FINDINGS: The article shows that, under managed care monopsony, the welfare of consumers may be increased but overall economic welfare will necessarily be reduced. It offers a test for whether the lower prices paid by managed care buyers with larger market share represent welfare-reducing monopsony or a welfare-increasing movement away from provider monopoly. The test says that, if the quantity of inputs (supplied under conditions of increasing long-run marginal cost) declines, monopsony is present. The article also argues that the translation of lower provider prices into lower premiums is consistent with welfare-reducing monopsony by nonprofit health plans. In contrast, for-profit health plans that obtain monopsony may reduce the welfare of consumers as well as that of input suppliers. These theoretical conclusions are shown to be consistent with recent empirical research indicating a negative relationship between buyer market power and cost per enrollee. CONCLUSIONS: Traditional antitrust policy has not been able to deal well with monopsony. The article concludes that health plans that use their market power to reduce medical spending may harm the well-being both of specialized medical workers and of consumers of medical care. Antitrust policy may need to be modified to deal with this situation.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adamache K. W., Sloan F. A. Competition between non-profit and for-profit health insurers. J Health Econ. 1983 Dec;2(3):225–243. [PubMed] [Google Scholar]
- Given R. S. Economies of scale and scope as an explanation of merger and output diversification activities in the health maintenance organization industry. J Health Econ. 1996 Dec;15(6):685–713. doi: 10.1016/s0167-6296(96)00500-0. [DOI] [PubMed] [Google Scholar]
- Melnick G. A., Zwanziger J., Bamezai A., Pattison R. The effects of market structure and bargaining position on hospital prices. J Health Econ. 1992 Oct;11(3):217–233. doi: 10.1016/0167-6296(92)90001-h. [DOI] [PubMed] [Google Scholar]
- Pauly M. V. Market power, monopsony, and health insurance markets. J Health Econ. 1988 Jun;7(2):111–128. doi: 10.1016/0167-6296(88)90011-2. [DOI] [PubMed] [Google Scholar]
- Staten M., Dunkelberg W., Umbeck J. Market share and the illusion of power. Can Blue Cross force hospitals to discount? J Health Econ. 1987 Mar;6(1):43–58. doi: 10.1016/0167-6296(87)90030-0. [DOI] [PubMed] [Google Scholar]
- Wholey D., Feldman R., Christianson J. B., Engberg J. Scale and scope economies among health maintenance organizations. J Health Econ. 1996 Dec;15(6):657–684. doi: 10.1016/s0167-6296(96)00499-7. [DOI] [PubMed] [Google Scholar]
- Wholey D., Feldman R., Christianson J. B. The effect of market structure on HMO premiums. J Health Econ. 1995 May;14(1):81–105. doi: 10.1016/0167-6296(94)00039-7. [DOI] [PubMed] [Google Scholar]