

Abstract
Objective To assess the extent to which observed associations between income inequality and mortality at population level are statistical artifacts. Design Indirect “what if” simulation using observed risks of mortality at individual level as a function of income to construct hypothetical state-level mortality specific for age and sex as if the statistical artifact argument were 100% correct. Method Data from the 1990 census for the 50 US states plus Washington, DC, were used for population distributions by age, sex, state, and income range; data disaggregated by age, sex, and state from the Centers for Disease Control and Prevention were used for mortality; and regressions from the national longitudinal mortality study were used for the individual-level relation between income and risk of mortality. Results Hypothetical mortality, although correlated with inequality (as implied by the logic of the statistical artifact argument), showed a weaker association with the level of income inequality in each state than the observed mortality. Conclusions The observed associations in the United States at the state level between income inequality and mortality cannot be entirely or substantially explained as statistical artifacts of an underlying individual-level relation between income and mortality. There remains an important association between income inequality and mortality at state level above anything that could be accounted for by any statistical artifact. This result reinforces the need to consider a broad range of factors, including the social milieu, as fundamental determinants of health.
INTRODUCTION
Considerable debate surrounds the impact of socioeconomic circumstances on individuals' health. Recent results suggest that there is a link not only between individual socioeconomic circumstances and health but also between the socioeconomic milieu in which individuals live and their health. Research has shown that greater levels of inequality in income among nations, states, or cities in the United States, or other geographically defined populations, are associated with higher mortality. 1, 2, 3, 4
Concerns have been raised by Gravelle, however, that these results may be no more than a statistical artifact.5 Gravelle points out, as others have noted previously, 6, 7 that a “diminishing returns” protective effect of higher individual income on individual risk of death is sufficient to account for differences in mortality between populations if there are differences in the extent of wealth and poverty, hence in the degree of income inequality.
The logic of this argument is correct. At the individual level, higher income (or some closely related but unmeasured factor, such as social status, for which income is a proxy) is causally associated with greater longevity.8 Moreover, while an extra dollar of income is protective, the amount of protective effect tails off as total income rises.8, 9
At the level of a population there is always some mixture of people with low, middle, and high incomes. If one population has a more equal distribution of income than another, this is equivalent to there being fewer individuals with either very high or very low incomes and more with incomes closer to the middle. But if a poorer individual is $1000 better off in a second population the beneficial effect on his or her risk of mortality is larger than the adverse impact on the risk of some richer person being $1000 worse off because of the diminishing protective returns of additional income. Thus, a population with a more equal distribution of income can have a lower mortality, other things being equal, solely as a result of a generic curvilinear individual-level causal relation between income and risk of mortality.
This logical possibility, however, is not a sufficient reason to dismiss the potential importance of inequality in income as an independent determinant of population-level mortality. This remains an empirical question.
We approached this question indirectly by first estimating a generic individual-level relation between income and mortality. We then simulated the extent to which variations in the distribution of income across populations can account for the observed population-level relation between income inequality and mortality. In other words, we asked “what if” our well specified relation between individual-level income and mortality were fully causal: the key step in Gravelle's argument. We therefore applied this relation to all individuals in a population group based on its actual income distribution and then calculated the expected mortality. The extent to which we reproduce the observed population-level association between income inequality and mortality is then an empirical test of the statistical artifact hypothesis.
METHOD
The argument that the association between income inequality and mortality is artifactual depends on bringing together information at two levels. One is the level of individuals, the other is that of populations such as US states.
The first step is to derive a reliable individual-level relation between income and risk of mortality. This generic relation was estimated for the US population by using the national longitudinal mortality study.10 This data set matched files containing household income and other demographic information from the US Census Bureau's current population survey to the National Death Index to provide about 7.6 million person-years of mortality exposure from 10 years of follow up.
The downward sloping curves (close together) in figure 1 show the results: the estimated relation between household income and the relative risk of mortality, plus a 95% confidence interval, after age and sex were controlled for. The relation is highly significant both statistically and substantively and is clearly consistent with a diminishing returns individual-level relation between income and risk of mortality. (Although we assumed logarithmic specification, other analyses determined that this was a reasonable functional form.)
Figure 1.

Relative risk of dying and population distribution in the United States for individuals by household income ($)
The remaining steps in the analysis complement this individual-level relation with consistent population-level data from the 1990 census on income inequality and mortality for each of the 50 states plus Washington, DC. Special Census Bureau tabulations provided counts of the numbers of individuals living in households by state, sex, detailed age groupings, and detailed income ranges. The other “humped” curve in figure 1 shows the resulting distribution of individuals by household income for the whole of the United States. Finally, 3 years of mortality data by state, sex, and age, centered on 1990, were downloaded from the Centers for Disease Control and Prevention Wonder site (http://wonder.cdc.gov/).
Given these data, a series of hypothetical standardized mortality rates specific for states was constructed. For each state, the generic relation between individual-level income and risk of mortality, shown by the income-mortality curve in figure 1, was applied to the actual income distribution within the state. In other words, a set of expected relative risks of mortality was calculated for each detailed age-sex-income-state category. These relative risks were next averaged over income groups, within each age-sex-state group, taking account of the number of individuals in each income interval (within age-sex-state groups). The result is a set of relative risks of dying as if the only reason for differences between states in risks of mortality were differences in income inequality between states (that is, differences in the composition of each state's population by income group).
We then multiplied these relative risks by the corresponding national mortality rates (specific for age-sex) and then standardized the rates by age-sex to the overall population. The result is a set of hypothetical state-specific mortality rates for which the only reason a state's mortality experience should differ from the national pattern is that its population has a different income distribution. These hypothetical mortalities are thus, by construction, exactly those we should observe if Gravelle's artifact hypothesis were 100% correct.
RESULTS
Some of the main results are shown in figure 2 for mortality in infants and working age men (that is, those age 25 to 59). Mortality is on the y axis and income inequality, measured by the proportion of total household income accruing to the bottom half of the population (the “median share”), along the x axis. Each point in these scatter plots represents one of the 50 states plus Washington, DC, with the area of each circle proportional to the state's population.
Figure 2.
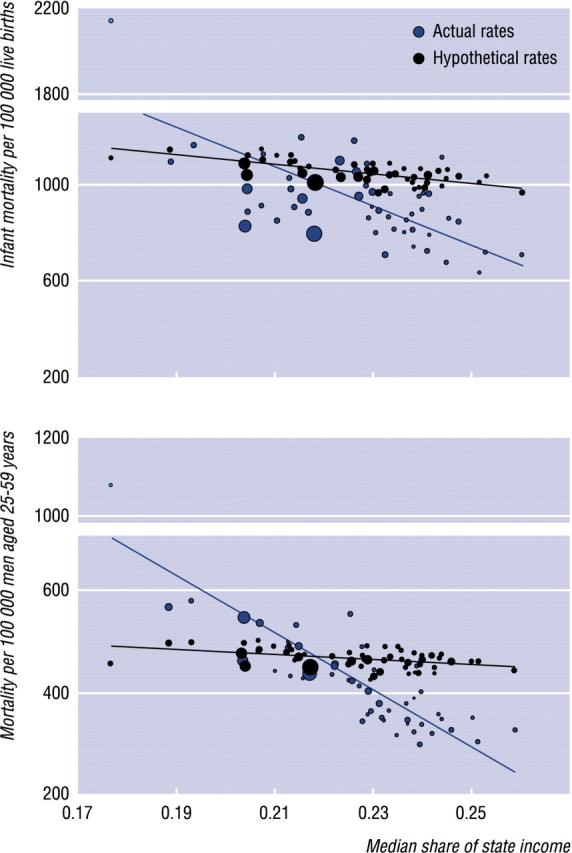
Actual and hypothetical mortality for infants and working age men by income inequality. Lines are ordinary least squares regression fits through the actual and hypothetical data points
DISCUSSION
The pattern of mortality generated from a literal application of Gravelle's artifact hypothesis provides a poor fit with the observed data in the United States. If the observed association between state-level standardized mortality and income inequality were completely artifactual then the two scatters of points (actual and hypothetical) would be on top of one another and the two regression lines would be superimposed. This is clearly not the case. Mortality based on the artifact hypothesis shows some slope in the expected direction: a higher share of income accruing to the bottom half of the population (indicating lower inequality) is associated with lower mortality. But these slopes are considerably less than the slopes of actual mortality in relation to income inequality.
The observed associations in the United States at the state level between income inequality and mortality therefore cannot be entirely, or even substantially, explained as the statistical artifacts of an underlying individual-level relation between income and risk of mortality. There remains an important association between state-level income inequality and mortality, over and above anything that could be accounted for by statistical artifact.
Summary points
Evidence is accumulating that living in a society with greater inequalities in income predisposes its members to higher mortality; however, there is widespread evidence that, for individuals, higher income is protective
This individual-level relation could “explain” the former societal-level relation
The strength of observed levels of association between income inequality and mortality, however, may go beyond what can be explained as a statistical artifact of an individual-level relation between income and mortality
The empirical analysis reported here, based on data from 1990, suggests that the association between income inequality and mortality is considerably stronger than can be accounted for by any statistical artifact
Research underpinning public health policy should therefore take a broad view of the importance of the social milieu as a fundamental determinant of health
Acknowledgments
We acknowledge helpful discussions with Richard Wilkinson, George Davey-Smith, Eric Brunner, Bruce Kennedy, Ichiro Kawachi, Geoff Rowe, and Jean-Marie Berthelot; comments by two anonymous referees; participants in the conference on economic equity in Ann Arbor, June 4-61998; and members of the population health program of the Canadian Institute for Advanced Research for comments on earlier versions of this paper. We also thank Susan Leroux for helpful analytical assistance. We remain responsible for any errors or infelicities.
Funding: MCW received funding from Statistics Canada and the Canadian Population Health Initiative; GK received funding from the University of Michigan Initiative on Inequalities in Health.
Competing interests: None declared
This paper was originally published in the BMJ 1999;319:953-955.
A more detailed version of this paper is on the BMJs website, www.bmj.com
References
- 1.Wilkinson RG. Unhealthy societies: the afflictions of inequality. London: Routledge, 1996.
- 2.Kaplan GA, Pamuk ER, Lynch JW, et al. Inequality in income and mortality in the United States: analysis of mortality and potential pathways. BMJ 1996;312:999-1003 (see correction in BMJ 1996;312:1253). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kennedy BP, Kawachi I, Prothrow-Stith D. Income distribution and mortality: cross-sectional ecological study of the Robin Hood index in the United States. BMJ 1996;312:1004-1007 (see correction in BMJ 1996;312:1194). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lynch JW, Kaplan GA, Pamuk ER, et al. Income inequality and mortality in metropolitan areas of the United States. Am J Public Health 1998;88:1074-1080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gravelle H. How much of the relation between population mortality and unequal distribution of income is a statistical artefact? BMJ 1998;316:382-385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Duleep HO. Mortality and income inequality among economically developed countries. Social Security Bull 1995;58:34-50. [PubMed] [Google Scholar]
- 7.Lynch JW, Kaplan GA. Understanding how inequality in the distribution of income affects health. J Health Psychol 1997;2:297-314. [DOI] [PubMed] [Google Scholar]
- 8.Wolfson M, Rowe G, Gentleman JF, et al. Career earnings and death: a longitudinal analysis of older Canadian men. J Gerontol Soc Sci 1993;48:S167-179. [DOI] [PubMed] [Google Scholar]
- 9.Backlund E, Sorlie PD, Johnson NJ. The shape of the relationship between income and mortality in the United States: evidence from the national longitudinal mortality study. Ann Epidemiol 1996;6:1-9. [DOI] [PubMed] [Google Scholar]
- 10.Rogot E, Sorlie PD, Johnson NJ. Life expectancy by employment status, income, and education in the national longitudinal mortality study. Public Health Rep 1992;107:457-461. [PMC free article] [PubMed] [Google Scholar]