

Abstract
Objective To understand the relationship between psychological resilience in social support and anxiety/depression in people living with HIV/AIDS and to verify whether there is a mediating effect. Methods The questionnaire was administered to 161 people living with HIV/AIDS in a hospital. The questionnaire contained a general questionnaire, the Hospital Anxiety and Depression Scale (HADS), the Psychological Resilience Inventory (CD-RICS), and the Social Collaborative Support Scale (PSSS), and Pearson correlation analyses were used to explore the correlation between the factors and anxiety/depression, stratified linear regression analyses were used to validate the mediation model, and the bootstrap method was used to test for mediating effects. Results Anxiety was negatively correlated with psychological resilience and social support (r=-0.232, P < 0.01; r=-0.293, P < 0.01); depression was negatively correlated with psychological resilience and social support (r=-0.382, P < 0.01; r=-0.482, P < 0.01); there was a mediation effect model of social support between psychological resilience and anxiety/depression; psychological resilience played a fully mediating role in social support and anxiety/depression, with an effect contribution of 68.42%/59.34% and a 95% CI(-0.256~-0.036)/(-0.341 to~-0.106). Conclusion Psychological resilience plays a complete mediating effect between social support and anxiety/depression. It is recommended that more channels of social support be provided to patients with HIV/AIDS, thereby enhancing their psychological resilience and reducing anxiety/depression levels.
Keywords: MSM, HIV/AIDS, Social support, Psychological resilience, Anxiety, Depression
Introduction
HIV continues to be a major global public health issue, having claimed 40.4 million lives so far. In 2022, 630 000 people died from HIV-related causes globally. There were approximately 39.0 million people living with HIV at the end of 2022 with 1.3 million people becoming newly infected with HIV in 2022 globally [1]. In order to end the AIDS epidemic, the Joint United Nations Programme on HIV/AIDS (UNAIDS) has put forward the vision of “ending HIV infection by 2030”, and China has also promulgated the “Thirteenth Five-Year Plan of Action for Containing and Preventing AIDS in China” and the “Implementation Plan for Containing the Spread of AIDS (2019–2022)” [2–4].
With the discovery of epidemiological investigations, there is a significant phenomenon of psychological distress in people living with HIV/AIDS(PLWHA ), especially the state of anxiety and depression [5]. Thus, it is essential to study the psychological characteristics of PLWHA. It was found that the prevalence of depression among PLWHA was 22-44% [6, 7]. While the prevalence of anxiety is 19% [8]. These anxiety and depression problems can affect the effectiveness of antiretroviral therapy and adherence, and increase the transmission and spread of HIV [9]. Consequently, reducing the level of anxiety and depression in PLWHA has been the focus of many researchers. In these studies, it has been established that both psychological resilience and social support are strongly correlated with anxiety/depression, respectively [10–12].
In addition, more in-depth studies have shown that increased levels of social support and psychological resilience can reduce levels of anxiety/depression [13, 14]. At the same time, we found that there is a wider range of studies examining the mental health of PLWHA, and few studies have covered the relationship between psychological resilience and social support with anxiety/depression. We also did not find any similar studies that describe psychological resilience, social support and how they affect anxiety/depression in PLWHA. Therefore, we hope that this study will provide a more in-depth understanding of the psychological world of PLWHA and seek to understand the role and connection between psychological resilience and social support. To be able to provide evidence for a more refined study of the psychological world of PLWHA.
Methods
Study design and sample
We are using a cross-sectional research methodology and surveying a specific hospital in Beijing, the capital city of China. In China, information about HIV-infected patients is uploaded to the database of the Chinese CDC, and only specific hospitals are able to receive these HIV-infected patients and administer tests or treatments to them. And it is very appropriate to collect research data in such a specific hospital.
HIV/AIDS patients who attended the HIV outpatient clinic of a hospital in Beijing from January 2023 to August 2023 were selected for the study. Inclusion criteria: (1) Including HIV positive reports; (2) Includes normal cognition, understanding of the study and voluntary participation in cooperating to complete the questionnaire. Exclusion criteria: (1) Including those with significant cognitive impairment or impaired consciousness who could not cooperate in completing the questionnaire; (2) Those who did not want to cooperate in completing the questionnaire for personal reasons.
Data collection
A standardized-trained psychotherapist from the hospital outpatient clinic introduced the purpose of the study, the principle of confidentiality and related requirements to the patients, and instructed the patients to fill in the questionnaire on a one-to-one basis in strict accordance with standardized procedures. The questionnaire containing the General questionnaire, The Hospital Anxiety and Depression Scale, The psychological resilience scale and The Perceived social support scale was used to collect relevant information. The general questionnaire included demographic characteristics, such as age, education, income, number of sexual partners and occupation.
The Hospital Anxiety and Depression Scale (HADS) was used to measure patients’ anxiety and depression levels. The scale contains 7 questions on the anxiety subscale and 7 questions on the depression subscale, for a total of 14 questions, with a score of 1–4 for each question, and a score of more than 8 for each subscale indicates an abnormality, with higher scores indicating a more pronounced abnormality [15]. The Cronbach’s α coefficients of its total scale, anxiety subscale and depression subscale were 0.879, 0.806, 0.806 respectively, with good reliability and validity [16].
The psychological resilience scale (Connor-Davidson resilience scale, CD-RICS) was used to measure the level of psychological resilience of the patients. The scale contains 13 questions on the resilience subscale, 8 questions on the strength subscale, and 4 questions on the optimism subscale, for a total of 25 questions. Each question is scored 0–4, with higher scores indicating better psychological resilience. Its Cronbach’s alpha coefficient was 0.91, with good reliability and validity [17].
The Perceived social support scale (PSSS) was used to measure the level of social support of patients. The scale contains 4 questions on the family subscale, 4 questions on the friends subscale, and 4 questions on the other subscales, for a total of 12 questions. Each topic is scored 1–7, with 12–36 being low support level, 37–60 being medium support level, and 61 or more being high support level. The Cronbach’s alpha coefficients of its total scale, family subscale, friends subscale, and other subscales were 0.840, 0.818, 0.820, and 0.813, respectively, with good reliability and validity [18, 19].
Statistical analysis
Analyses were performed using SPSS 26.0 software. Measurements were expressed as ( ±S), and t-test or one-way line ANOVA was used to test for differences between groups. Pearson correlation analysis was used to explore the correlation between the factors and anxiety and depression. Stratified linear regression analysis was used to validate the mediation model. The bootstrap method was used to test the mediating effect. P < 0.05 was used to indicate a statistically significant difference.
±S), and t-test or one-way line ANOVA was used to test for differences between groups. Pearson correlation analysis was used to explore the correlation between the factors and anxiety and depression. Stratified linear regression analysis was used to validate the mediation model. The bootstrap method was used to test the mediating effect. P < 0.05 was used to indicate a statistically significant difference.
Ethics
This study complied with the World Medical Association’s Declaration of Helsinki’s Ethical Principles and Good Clinical Practice for medical research in humans and all applicable regulations.The clinical research protocol and informed consent form were both approved by the Ethics Committee of the Fifth Medical Centre, General Hospital of the Chinese PLA. The subjects recruited for the clinical trial voluntarily signed the informed consent form. (KY-2023-6-41-1).
Results
Study participant enrollment and characteristics
The questionnaire was distributed to 170 HIV/AIDS patients, and 161 valid questionnaires were collected, with a recovery rate of 94.71%. The average score of the anxiety scale is 13.72 ± 4.10, and the average score of the depression scale is 15.99 ± 2.58 (Table 1).
Table 1.
General Information T( ±S)
±S)
| Variable | Constituent ratio (%) | Anxiety | Depression | ||
|---|---|---|---|---|---|
| Score | t/F | Score | t/F | ||
| Age | 0.229 | 0.279 | |||
| 18~25 | 16(9.94) | 13.35±1.13 | 14.35±0.50 | ||
| 26~30 | 43(26.71) | 14.03±0.62 | 16.95±0.40 | ||
| 31~40 | 53(32.92) | 13.54±0.52 | 16.19±0.33 | ||
| 41~50 | 31(19.25) | 13.42±0.78 | 15.52±0.42 | ||
| >50 | 18(11.18) | 14.40±1.08 | 15.40±0.72 | ||
| Income(RMB) | 1.327 | 0.185 | |||
| <5 000 | 51(31.68) | 14.53±0.56 | 16.04±0.39 | ||
| 5 000~10 000 | 61(37.89) | 13.60±0.54 | 16.09±0.36 | ||
| 10 000~15 000 | 26(16.14) | 13.48±0.81 | 16.02±0.38 | ||
| >15 000 | 23(14.29) | 12.56±0.84 | 15.63±0.43 | ||
| Education | 1.608 | 0.143 | |||
| High school and below | 51(31.68) | 14.48±0.59 | 16.16±0.41 | ||
| Junior college | 38(23.60) | 13.94±0.67 | 15.82±0.43 | ||
| Undergraduate course | 55(34.16) | 13.37±0.55 | 15.93±0.30 | ||
| Graduate student | 17(10.56) | 12.14±0.81 | 16.08±0.63 | ||
| Number of sexual partners | 0.779 | 0.666 | |||
| No fixed | 84(52.17) | 13.41±0.46 | 15.77±0.31 | ||
| 1 | 72(44.72) | 13.98±0.48 | 16.22±0.26 | ||
| 2 or more | 5(3.11) | 15.36±0.89 | 16.44±1.09 | ||
| Occupation | 0.282 | 0.615 | |||
| Student | 3(1.9) | 12.80±4.99 | 20.00±1.38 | ||
| Production | 10(6.2) | 15.84±3.30 | 19.52±3.75 | ||
| Sale | 18(11.2) | 14.53±4.41 | 18.97±1.77 | ||
| Market | 7(4.3) | 13.36±3.55 | 18.97±2.05 | ||
| Customer Service | 10(6.2) | 14.74±5.46 | 18.48±2.90 | ||
| Logistics Work | 7(4.3) | 14.74±5.46 | 18.62±4.92 | ||
| Human Resources | 3(1.9) | 8.80±0.04 | 17.60±6.92 | ||
| Finance | 3(1.9) | 15.46±4.80 | 21.86±3.69 | ||
| Civil Service | 4(2.5) | 11.40±1.36 | 20.60±1.20 | ||
| Technician | 12(7.5) | 12.33±4.17 | 19.46±2.34 | ||
| Administrators | 13(8.1) | 13.35±4.01 | 19.56±2.05 | ||
| Teacher | 9(5.6) | 11.73±3.55 | 18.40±2.03 | ||
| Adviser | 1(0.6) | 11.20±3.56 | 20.00±1.22 | ||
| Professional | 5(3.1) | 16.48±6.36 | 17.12±1.45 | ||
| Others | 56(34.8) | 13.72±4.10 | 18.84±2.23 | ||
Analysis of the correlation between psychological resilience, social support, and anxiety/depression
The correlation analysis results indicate that anxiety is negatively correlated with psychological resilience and social support (r=-0.232, P < 0.01; r=-0.293, P < 0.01). Depression is also negatively correlated with psychological resilience and social support (r=-0.382, P < 0.01; r=-0.482, P < 0.01) (Table 2).
Table 2.
Related analysis(r)
| Variable | Anxiety | Depression |
|---|---|---|
| Psychological resilience | -0.232b | -0.382b |
| Social support | -0.293b | -0.482b |
b:P>0.01
Testing the mediation effect model
Testing the hypothesis of the mediation effect model through layered regression
A model with social support as the independent variable, psychological resilience as the mediator, and anxiety/depression as the dependent variable was developed (Fig. 1).
Fig. 1.
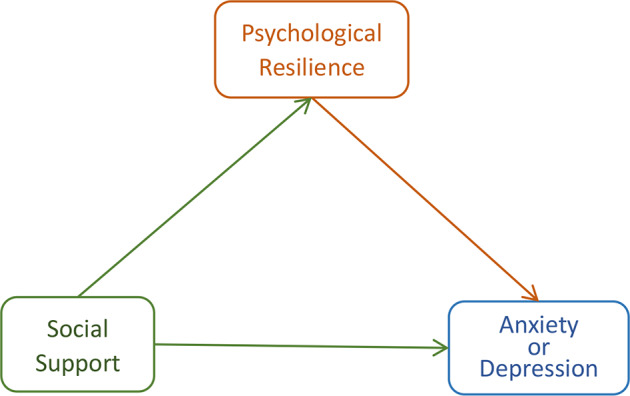
The mediating effect model of psychological resilience between social support and anxiety or depression
Stratified regression analyses were performed when anxiety and depression were the dependent variables, respectively, with control variables (age, income, education, and number of sexual partners) in the first stratum, social support as the independent variable in the second stratum, and mediator variables in the third stratum. The results showed that there was no multicollinearity with VIF>3. In anxiety/depression Eq. 2 (R2 = 0.083, P < 0.05/R2 = 0.156, P < 0.01), social support was a significant impediment to the level of anxiety/depression (95% CI:-0.135 ~ -0.017, P < 0.01/ 95% CI: -0.127 ~ − 0.056, P < 0.01). With the addition of the mediator variable in anxiety/depression Eq. 3 (R2 = 0.120, P < 0.01/R2 = 0.257, P < 0.01), psychological resilience was a significant impediment to higher levels of anxiety/depression (95% CI:-0.138 ~ -0.017, P < 0.05/95% CI: − 0.115 ~ -0.046, p < 0.01). The model hypotheses were valid and psychological resilience played a fully mediating role between social support factors and anxiety/depression ( Table 3).
Table 3.
Stratified regression analyses of anxiety/depression
| Variable | 95%CI | P | R2 | ΔR2 |
|---|---|---|---|---|
| Anxiety model 1 | 0.129 | 0.044 | 0.044 | |
| Age | -0.706 ~ 0.441 | 0.649 | ||
| Income | -1.081 ~ 0.351 | 0.315 | ||
| Education | -1.258 ~ 0.192 | 0.148 | ||
| Number of sexual partners | -0.425 ~ 1.861 | 0.216 | ||
| Anxiety model 2 | 0.019 | 0.083 | 0.039 | |
| Age | -0.641 ~ 0.49 | 0.793 | ||
| Income | -0.998 ~ 0.414 | 0.415 | ||
| Education | -1.135 ~ 0.302 | 0.254 | ||
| Number of sexual partners | -0.455 ~ 1.792 | 0.242 | ||
| social support | -0.135~-0.017 | 0.012 | ||
| Anxiety model 3 | 0.003 | 0.120 | 0.037 | |
| Age | -0.544 ~ 0.577 | 0.954 | ||
| Income | -1.001 ~ 0.386 | 0.382 | ||
| Education | -1.08 ~ 0.334 | 0.299 | ||
| Number of sexual partners | -0.462 ~ 1.747 | 0.253 | ||
| social support | -0.094 ~ 0.047 | 0.505 | ||
| psychological resilience | -0.138~-0.017 | 0.012 | ||
| Depression model 1 | 0.657 | 0.015 | 0.015 | |
| Age | -0.538 ~ 0.194 | 0.355 | ||
| Income | -0.577 ~ 0.337 | 0.605 | ||
| Education | -0.501 ~ 0.425 | 0.872 | ||
| Number of sexual partners | -0.272 ~ 1.187 | 0.217 | ||
| Depression model 2 | 0.000 | 0.156 | 0.141 | |
| Age | -0.444 ~ 0.238 | 0.551 | ||
| Income | -0.458 ~ 0.394 | 0.882 | ||
| Education | -0.331 ~ 0.536 | 0.641 | ||
| Number of sexual partners | -0.28 ~ 1.075 | 0.249 | ||
| social support | -0.127~-0.056 | 0.000 | ||
| Depression model 3 | 0.000 | 0.257 | 0.100 | |
| Age | -0.332 ~ 0.316 | 0.960 | ||
| Income | -0.449 ~ 0.352 | 0.812 | ||
| Education | -0.261 ~ 0.556 | 0.477 | ||
| Number of sexual partners | -0.268 ~ 1.009 | 0.253 | ||
| social support | -0.078 ~ 0.004 | 0.073 | ||
| psychological resilience | -0.115~-0.046 | 0.000 |
Testing for mediating effects via bootstrap
The mediating effects were further tested using the bootstrap method, where the mediating effects model was tested using repeated random sampling 5000 times in the raw data. The results showed that the total effects of anxiety/depression were all significant, none of the direct effects were significant, and none of the confidence intervals for the indirect effects contained 0. Psychological resilience played a fully mediating role in social support factors and anxiety/depression, with an effect contribution of 68.42%/59.34% (Table 4).
Table 4.
Validation of the mediating role of social support between psychological resilience and anxiety/depression
| Variable | Effect | SE | t | P | 95%CI |
|---|---|---|---|---|---|
| Anxiety | |||||
| Total effect | -0.076 | 0.030 | -2.554 | 0.012 | -0.135 ~ -0.017 |
| Direct effect | -0.024 | 0.036 | -0.668 | 0.505 | -0.094 ~ 0.047 |
| Indirect effect | -0.052 | 0.021 | -0.097 ~ -0.014 | ||
| Indirect effects (standardisation) | -0.138 | 0.057 | -0.256 ~ -0.036 | ||
| Depression | |||||
| Total effect | -0.091 | 0.018 | -5.092 | 0.000 | -0.127 ~ -0.056 |
| Direct effect | -0.037 | 0.021 | -1.805 | 0.073 | -0.078 ~ 0.004 |
| Indirect effect | -0.054 | 0.015 | -0.083 ~ -0.024 | ||
| Indirect effects (standardisation) | -0.227 | 0.060 | -0.341 ~ -0.106 | ||
Discussion
Resilience refers to the act of coping, adapting, or thriving from adversity, and reflects a complex and dynamic interplay between individual, environmental, and sociocultural domain [20]. Social support is a social network consisting of three dimensions: family support, friend support, and other support ( such as social relationships with neighbors, leaders, etc.) [21].The level of social support reflects the extent to which an individual is linked to social relationships. The higher the level, the more closely the individual interacts in society [22].
The relationship between psychological resilience, social support, and anxiety/depression is very strong. From the results of this study to observe the relationship between these four factors, an increase in psychological resilience and social support can significantly reduce the level of anxiety/depression, respectively. This result is consistent with the findings of several international studies [23–25]. Among these studies, Leodoro J. Labrague et al.‘s study and Zhi Ye et al.‘s study, although introduced in both social support and psychological resilience can enhance mental health. However, the subjects were healthcare workers and university students, which is different from the target population of this study. While Aneela Hussain et al.‘s study targeted the HIV-infected population and described the importance of social support for mental health. However, none of these studies reported, described the role of psychological resilience in the middle of social support and anxiety/depression.
In the present study, we found that PLWHA who have better scores on psychological resilience and social support mean that they are better able to adapt to being HIV-infected and to survive in society or socialise as HIV-infected people. This adaptation to the environment reduces anxiety or depression due to discrimination or inconvenience of living with HIV infection [26, 27].In looking at PLWHA, Frank H. Galvan concluded that social support is not only an important factor in influencing mental health in addition to the stigma of HIV, but further found a strong relationship between the friend dimension and HIV stigmatization [28].Meanwhile, Cierra N. HOPKINS et al. confirmed the important relationship between psychological resilience and mental health [29]. The results of these two studies are also consistent with some of the results of this study.
In further analysis, we constructed a model of the relationship between psychological resilience, social support, anxiety/depression. The results of the model revealed that social support can directly influence the level of anxiety as well as the level of depression in PLWHA. For a special group of HIV-infected people, the support of family and friends is extraordinarily important [30]. Especially the support of sexual peers. It can even be said that it can influence all aspects of PLWHA, such as how they deal with stigma, whether they take medication as required, and whether they engage in suicidal behaviour [31–33]. Therefore, based on the findings of the study, we suggest that the relevant authorities can pour more resources into family education and sexual peer education for PLWHA.
We found that psychological resilience mediated the effect of social support on anxiety levels or depression levels. Not only can the level of social support directly influence the level of anxiety or depression in PLWHA, but it can also influence the level of anxiety or depression through the strength of psychological resilience. In addition, psychological resilience is an important protective factor for people with low levels of social support and can reduce the occurrence of anxiety and depression [34]. Thus, having good psychological resilience can reduce the occurrence of anxiety or depression at the same level of social support. This provides a strong support in terms of mental health education for PLWHA.
Strengths and limitations
The results of this study, innovatively confirm, the mediating role of psychological resilience. It also proves how social support and psychological resilience influence anxiety/depression levels in PLWHA. It will tell us a way to a further, more refined understanding of the mental world of PLWHA.
Some limitations of this study that may affect our findings include the small sample size; the data collected may be biased. As the sample was only collected within a single hospital in Beijing, the generalisability of the results must be interpreted with caution. In addition, participant-reported data may have limited the results. Even though we took certain measures to maintain data integrity, it is still not possible to avoid participants’ self-reported data being over- or under-reported. Finally, one of the more unfortunate aspects is the low number of factors for demographic characteristics. This could potentially lead to a number of influencing factors being undetected.
Conclusion
This study determined the relationship between psychological resilience, social support, anxiety/depression. Social support reduces levels of anxiety or depression in HIV-infected individuals, as does psychological resilience. In addition, psychological resilience is an important mediator between social support and anxiety or depression. Greater psychological resilience prevents the experience of anxiety or depression due to low levels of social support, and mental health work with PLWHA can be more beneficial if it is undertaken in the context of both social support and psychological resilience. Therefore, based on the results of this study, we recommend increased investment in psychotherapy. Mental health judgement, family and peer education by psychotherapists for PLWHA may be a good option [35–37].
Acknowledgements
The authors would like to thank all participants for their participation in this study.
Author Contributions
Yongbing Sun’s job is to carry out the design of the entire study, promote the implementation of the study, analyze data, and obtain results, and write articles. The work of Bing Song and Juan Cheng is to assist in promoting research implementation. Cheng Zhen and Chao Zhang’s job is to participate in writing and translating articles. The work of Tianjun JIANG supervised the design, implementation, and writing of the entire study.All authors read and approved the final manuscript.
Funding
This study was funded by the [National Key R&D Plan].(2022YFC2305004).
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declarations
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Competing interests
The authors declare no competing interests.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Footnotes
Yongbing Sun and Bing Song are co-first authors.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yongbing Sun and Bing Song are contributed equally to this work.
References
- 1.WHO. Data on the size of the HIV/AIDS epidemic.[EB/OL]. https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/data-on-the-size-of-the-hiv-aids-epidemic?lang=en.
- 2.Jiangping Sun It was written at the end of the three 90% strategic goal of AIDS prevention and control [J] Chin J Prev Med. 2020;54(11):1180–3. doi: 10.3760/cma.j.cn112150-20200915-01204. [DOI] [PubMed] [Google Scholar]
- 3.Jin MHC, Li J, et al. Expand expert consensus on AIDS testing to promote early detection [J] China AIDS STD. 2021;27(11):1202–6. [Google Scholar]
- 4.Hodgins C, Stannah J, Kuchukhidze S, et al. Population sizes, HIV prevalence, and HIV prevention among men who paid for sex in sub-saharan Africa (2000–2020): a meta-analysis of 87 population-based surveys[J] PLoS Med. 2022;19(1):e1003861. doi: 10.1371/journal.pmed.1003861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lazarus JV, Safreed-Harmon K, Barton SE, et al. Beyond viral suppression of HIV - the new quality of life frontier[J] BMC Med. 2016;14(1):94. doi: 10.1186/s12916-016-0640-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yongbing S, Fang H. Huihuang Huang, etc Research progress on AIDS associated depression [J] AIDS and STD in China, 2022,28 (10): 1226–9.
- 7.Rezaei S, Ahmadi S, Rahmati J, et al. Global prevalence of depression in HIV/AIDS: a systematic review and meta-analysis[J] BMJ Support Palliat Care. 2019;9(4):404–12. doi: 10.1136/bmjspcare-2019-001952. [DOI] [PubMed] [Google Scholar]
- 8.Beer L, Tie Y, Padilla M, et al. Generalized anxiety disorder symptoms among persons with diagnosed HIV in the United States[J] AIDS. 2019;33(11):1781–7. doi: 10.1097/QAD.0000000000002286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhao T, Tang C, Yan H, et al. Comparative efficacy and acceptability of non-pharmacological interventions for depression in people living with HIV: a systematic review and network meta-analysis[J] Int J Nurs Stud. 2023;140:104452. doi: 10.1016/j.ijnurstu.2023.104452. [DOI] [PubMed] [Google Scholar]
- 10.Thabet A, Ghandi S, Barker EK et al. Interventions to enhance psychological resilience in forcibly displaced children: a systematic review[J]. BMJ Glob Health, 2023,8(2). [DOI] [PMC free article] [PubMed]
- 11.Sleijpen M, Mooren T, Kleber RJ, et al. Lives on hold: a qualitative study of young refugees’ resilience strategies[J] Childhood. 2017;24(3):348–65. doi: 10.1177/0907568217690031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee MS, Lee JJ, Park S, et al. Is social support associated with postpartum depression, anxiety and perceived stress among Korean women within the first year postpartum?[J] J Psychosom Obstet Gynaecol. 2023;44(1):2231629. doi: 10.1080/0167482X.2023.2231629. [DOI] [PubMed] [Google Scholar]
- 13.Alnazly E, Khraisat OM, Al-Bashaireh AM, et al. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers[J] PLoS ONE. 2021;16(3):e247679. doi: 10.1371/journal.pone.0247679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lyu C, Ma R, Hager R, et al. The relationship between resilience, anxiety, and depression in Chinese collegiate athletes[J] Front Psychol. 2022;13:921419. doi: 10.3389/fpsyg.2022.921419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jiong Zhou Y, Wang Analysis of the relevant factors of six commonly used anxiety and depression scales [J] Chin J Neurol. 2005;38(11):714. [Google Scholar]
- 16.Xin Zhang Z, Wang H, Du, et al. Hope the validity and reliability of the source scale in evaluating medical personnel [J] Chin J Mental Health. 2022;36(4):337–43. [Google Scholar]
- 17.Yang Y. Xiaojun Cao.Multiple mediating effects of sibling relationships and psychological resilience between early childhood psychological abuse and depression in non only child college students [J] Chin J Behav Med Brain Sci. 2022;31(5):455–61. [Google Scholar]
- 18.Zhu FZS, Deng P. Evaluation of the application of the Perception Social Support Scale in the study of social support for hospitalized patients in China [J] Nurs Res. 2018;32(13):2048–52. [Google Scholar]
- 19.Pingyu Tao L, Qiu X, Weng, et al. Investigation of social function and related factors in hospitalized wandering schizophrenia patients [J] J Clin Psychiatry. 2022;32(3):214–6. [Google Scholar]
- 20.Mosheva M, Hertz-Palmor N, Dorman IS, et al. Anxiety, pandemic-related stress and resilience among physicians during the COVID-19 pandemic[J] Depress Anxiety. 2020;37(10):965–71. doi: 10.1002/da.23085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Greenhaus J. Beutell N.Sources of conflict between work and family roles[J] Acad Manag Rev. 1985;10(1):76–88. doi: 10.2307/258214. [DOI] [Google Scholar]
- 22.Liu XLYZ et al. Understanding the impact of social support on stress response during the epidemic: the mediating role of shame and loneliness [J] Chinese Journal of Clinical Psychology, 2022,30 (03): 744–748.
- 23.Cho H, Lee K, Choi E, et al. Association between social support and postpartum depression[J] Sci Rep. 2022;12(1):3128. doi: 10.1038/s41598-022-07248-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bedaso A, Adams J, Peng W, et al. The relationship between social support and mental health problems during pregnancy: a systematic review and meta-analysis[J] Reprod Health. 2021;18(1):162. doi: 10.1186/s12978-021-01209-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Labrague LJ, De Los SJ. COVID-19 anxiety among front-line nurses: predictive role of organisational support, personal resilience and social support[J] J Nurs Manag. 2020;28(7):1653–61. doi: 10.1111/jonm.13121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Labrague LJ. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: a systematic review of quantitative studies[J] J Nurs Manag. 2021;29(7):1893–905. doi: 10.1111/jonm.13336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ye Z, Yang X, Zeng C, et al. Resilience, Social Support, and coping as mediators between COVID-19-related stressful experiences and acute stress disorder among College students in China[J] Appl Psychol Health Well Being. 2020;12(4):1074–94. doi: 10.1111/aphw.12211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Galvan FH, Davis EM, Banks D, et al. HIV stigma and social support among African Americans[J] AIDS Patient Care STDS. 2008;22(5):423–36. doi: 10.1089/apc.2007.0169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hopkins CN, Lee CA, Lambert CC, et al. Psychological resilience is an Independent correlate of health-related quality of life in middle-aged and older adults with HIV in the Deep South[J] J Health Psychol. 2022;27(13):2909–21. doi: 10.1177/13591053211072430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hussain A, Rahim A, Rajput F. The quality of life of HIV positive transgender and homosexual population in Karachi, Pakistan[J] Pak J Med Sci. 2023;39(4):1202–7. doi: 10.12669/pjms.39.4.6445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mokgatle M, Madiba S. Community perceptions of HIV Stigma, discriminatory attitudes, and Disclosure concerns: A Health Facility-based study in selected Health districts of South Africa[J]. Int J Environ Res Public Health, 2023,20(14). [DOI] [PMC free article] [PubMed]
- 32.Babalola OE, Badru OA, Bain LE, et al. Determinants of social support among people living with HIV in Nigeria-a multicenter cross-sectional study[J] Front Public Health. 2023;11:1120192. doi: 10.3389/fpubh.2023.1120192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mohanan P, Kamath A. Family support for reducing morbidity and mortality in people with HIV/AIDS[J] Cochrane Database Syst Rev. 2009;2009(3):D6046. doi: 10.1002/14651858.CD006046.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pineda CN, Naz MP, Ortiz A, et al. Resilience, Social Support, loneliness and quality of life during COVID-19 pandemic: a structural equation Model[J] Nurse Educ Pract. 2022;64:103419. doi: 10.1016/j.nepr.2022.103419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Han S, Zhang Y, Yang X, et al. Exploring core mental health symptoms among persons living with HIV: a network analysis[J] Front Psychiatry. 2023;14:1081867. doi: 10.3389/fpsyt.2023.1081867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Thompson JL, Beltran-Najera I, Johnson B, et al. Evidence for neuropsychological health disparities in Black americans with HIV disease[J] Clin Neuropsychol. 2022;36(2):388–413. doi: 10.1080/13854046.2021.1947387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dhaliwal JS, Chan LG, Goh J, et al. Mental health and implications for antiretroviral adherence in a multiethnic Asian cohort[J] Sex Transm Infect. 2022;98(7):497–502. doi: 10.1136/sextrans-2021-055153. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.