

Abstract
Purpose
With an increased investment in psychosocial caregiving research, it becomes critical to establish the need for data of key stakeholders and future strategic directions. The purpose of this international Delphi study was to engage caregivers, clinicians, researchers, and managers to identify priority topics for caregiver research in cancer care.
Methods
A three-round, online Delphi survey took place. In round 1, stakeholders generated caregiver research topics by answering an open-ended question. Content analysis of stakeholders’ answers identified topics to be included in the round 2 survey to rate their importance. The round 3 survey included topics with less than 80% agreement for stakeholders to reconsider in light of other participants’ responses.
Results
In round 1, eighty-six topics were generated by 103 clinicians, 63 researchers, 61 caregivers, and 22 managers and grouped into 10 content areas: impact of cancer, support programs, vulnerable caregivers, technology, role in health care, caregiver-centered care, knowledge translation, environmental scan, financial cost of caregiving, and policy. Across rounds 2 and 3, nine topics achieved consensus for all stakeholder panels (e.g., home care interventions), with three of these emphasizing more research needed on the financial impact of informal caregiving (e.g., financial impact of “burnout” for caregivers and society). Of note, vulnerable caregivers and use of technology were content areas prioritized particularly by managers and researchers, but not caregivers.
Conclusion
By establishing a confluence of perspectives around research priorities, this study ensures the interests of key stakeholders are integrated in strategic directions, increasing the likelihood of research capable of influencing practice, education, and policy.
Keywords: Cancer, Caregivers, Family, End-user engagement, Research priorities, Delphi
Internationally, cancer is among the most common illnesses requiring assistance from informal caregivers [17]. With the increased utilization of outpatient treatments, caregivers are, more than ever, taking on complex illness management roles traditionally performed by health care professionals (HCPs) [21]. Patients with cancer receive on average 7–10 hours of informal caregiving per week, with common roles including monitoring of treatment side effects, assisting with activities of daily living, organizing appointments, administering medication, liaising with the medical team, and providing emotional support [17]. Although informal caregivers’ support reduces the demands on the health care system [26], caregivers remain a hidden workforce, operating with little to no formal training [21]. This results in high levels of emotional, physical, social, and/or financial burden for the caregivers [17]. Cancer caregivers have reported higher levels of financial hardship, physical strain, and emotional stress than caregivers of individuals with diabetes or the frail elderly [16].
With the recognition of caregivers’ contribution to patients’ care and the burden that they endure, research to better support caregivers has become a high priority area within cancer care [23] and has increased exponentially over the past two decades. As this field of research expands, it is important to determine key stakeholders’ need for data to focus and shape the future of this field. To date, cancer caregiver research has not been driven by any set of national or international priorities, which in part has resulted in some areas being neglected (e.g., health service research), whereas others are overly studied (e.g., prevalence studies) [20]. Therefore, to ensure that moving forward research is strategic, clear priorities need to be established [20].
The objectives of this study were therefore to (a) identify high-priority research topics for caregivers of cancer patients according to caregivers, managers, clinicians, and researchers and (b) examine the similarities and differences in priorities across these stakeholder groups.
Methods
This study used the Delphi technique: a structured iterative survey process whereby a series (or rounds) of surveys are sent to stakeholders invited on the basis of their experience and/or expertise to make independent ratings on given issues to establish consensus [10, 13, 22]. The Delphi technique was chosen as a large number of participants dispersed over a wide geographical area could respond individually and anonymously. Also, it allows participants the opportunity to revise their opinions in light of others’ responses, without the pressure to maintain previously expressed opinions [10, 13]. In this study, the Delphi technique included parallel consultations with four panels of national and international stakeholders who completed three online surveys. An overview of the study procedures is presented in Fig. 1. The study was approved by the relevant local ethics committees. The first page of the round 1 survey provided additional information about the survey, including participants’ right to withdraw and voluntary participation, and completing the contact detail fields was taken as an indication of written consent.
Fig. 1.
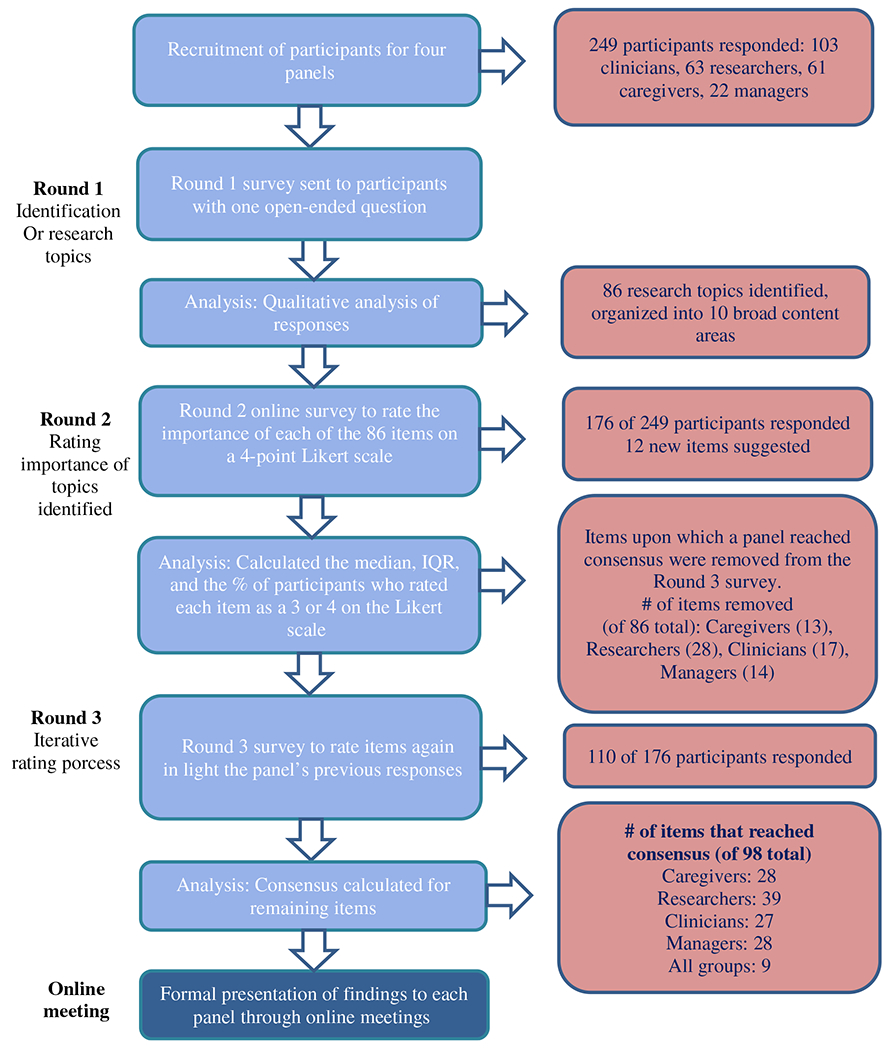
Overview of Delphi procedure and data collection
Sample
Participants included clinicians, managers, researchers, and caregivers. Participants were separated into four panels in recognition that these groups might have different ideas about what should be prioritized, and that these differences might be obfuscated, if they took part in a single panel. Clinicians were members of the multidisciplinary, oncology health professional team, providing direct care to individuals with cancer. Managers were eligible, if they represented oncology clinicians in leadership positions or non-clinicians in relevant managerial positions (e.g., managers of cancer care foundations). Researchers had conducted psychooncology research. The main inclusion criterion for caregivers was caring for or living with a family member with cancer or having previously cared for someone who was since deceased (regardless of cancer type and stage). All stakeholders had to be fluent in English or French.
Sample size
The Delphi group size does not depend on statistical power but rather on group dynamics for arriving at consensus [22]. Based on sample size recommendations for Delphi panels [13, 22], a minimum of 10 to 18 stakeholders per panel were recruited.
Procedures
Stakeholders internationally were identified through several sources. Initially, convenience sampling was undertaken followed by purposive sampling to address gaps in stakeholders’ geographical representation. Recruitment strategies included sending study advertisements through the listserv of relevant professional organizations (e.g., International Psycho-Oncology Society (IPOS), American Psychosocial Society (APOS)). In addition, the study advertisement was sent directly to potential stakeholders identified through electronic searches of directories of government departments, health care centers, non-for-profit organizations, educational institutions, and conference proceedings. Caregivers mainly received the e-mail invitation from one of the collaborating cancer organizations or from their HCP. Participants were also asked to nominate additional stakeholders (snowball sampling) at the end of the first survey. Once stakeholders were identified, an e-mail was sent to introduce the study and provide the link to the round 1 survey.
Data collection
This Delphi study involved completing three online surveys, each round 5–6 months apart [13, 22]. The round 1 survey elicited participants’ demographics, provided a description of the study, and asked stakeholders: “In your opinion, what are priority topics for caregiver research in cancer care over the next decade?” The topic list generated in round 1 formed the basis of the round 2 survey.
In round 2, stakeholders received a structured survey and were asked to rate the importance of conducting more research for each topic identified in round 1 using a 4-point scale (1 = not important to do more research to 4 = very important to do more research). A 4-point scale was chosen, as those between 4 and 7 points have demonstrated the strongest psychometric properties [24], with some evidence of increased reliability for a 4-point as compared to the 6-point scale [4]. Also, as the goal was to identify agreement/disagreement, a scale without a “neutral” mid-point was favored [24]. Space was provided for stakeholders to add topics and/or comments.
The round 3 survey only included the research topics on which panel consensus had not been reached to reduce participation burden [10]; stakeholders had the chance to revise their answers in light of their panels’ responses (encouraging consensus). For each topic listed, the percent of stakeholders’ in that panel indicating it was “very important” to do more research as well as the individual participant’s round 2 response were shown [22]. Further, new priorities that were suggested in round 2 were included. The study concluded with a formal presentation of findings to each panel during online meetings.
Data analysis
Given the open-ended nature of round 1, content analysis of responses was applied using Microsoft Word. During this process, the central meaning of each topic was described using a short statement (i.e., a code). Initially, the first two authors independently analyzed 80 responses to achieve consensus in coding, the remaining responses were then coded by the 2nd author. Codes that shared common features were then grouped into research topics, which were further aggregated in broad research content areas [13]. Responses that did not address the research question were not carried forward.
The analyses in rounds 2 and 3 identified the level of consensus for each research topic as defined by having (a) 80% of stakeholders’ ratings fall within the two highest or two lowest response categories on the 4-point scale and (b) an interquartile range (IQR) of 1 or less [13, 24]. In addition, univariate analysis to identify associations between each topic achieving consensus for at least one panel with the type of panel was performed using the Chi-square test. Then, for each content area multivariate analyses were performed to test the effect of the stakeholder panel on all topics (treated as a vector of correlated binary variables) using logistic regression model [12]. The generalized linear mixed model (GLMM) [6] approach was used to correct for the correlation among the topics. This regression model included a categorical variable to identify each topic and the stakeholder panel. An interaction term, between the panel and the topic, was also included to test if the effect of the panel is different across topics. The interaction term was tested at alpha 0.15. If the interaction was not significant, the effect of the panel was tested at alpha 0.05. All the analyses were conducted with SAS version 9.4.
Results
Participants
Responses to the round 1 survey were returned by 249 stakeholders: 103 clinicians, 63 researchers, 61 caregivers, and 22 managers. The consent rate cannot be calculated, as the number of eligible participants on the different listserves used is not known. Participants’ areas of expertise, demographics, and professional information are presented in Tables 1 and 2.
Table 1.
Demographics of caregivers from round 1 (N = 61, unless specified otherwise)
| Demographics | Number | Percent |
|---|---|---|
| Country of residence | ||
| Canada | 61 | 100 |
| Gender | ||
| Female/male | 48/13 | 78.69/21.31 |
| Ethnicity | ||
| White or Caucasian/Other | 56/5 | 91.80/8.20 |
| Language at home | ||
| English | 45 | 73.77 |
| French | 13 | 21.31 |
| Other | 3 | 4.92 |
| Marital status | ||
| Married/common law | 44 | 72.13 |
| Widowed | 6 | 9.8 |
| Single/never married | 4 | 6.56 |
| Divorced/separated | 4 | 6.56 |
| No response or other | 3 | 4.92 |
| Relationship to patient (n = 59) | ||
| Wife/husband/partner | 42 | 71.19 |
| Parent | 7 | 11.86 |
| Other family member | 6 | 10.17 |
| Other non-family member | 4 | 6.78 |
| Education | ||
| Primary | 0 | 0 |
| Secondary school (high school) | 7 | 11.48 |
| Certificate or diploma | 21 | 34.43 |
| Undergraduate degree | 17 | 27.87 |
| Graduate certificate or diploma | 7 | 11.48 |
| Master’s or doctorate degree | 9 | 14.75 |
| Diagnosis of patient | ||
| Genitourinary (prostate, kidney) | 15 | 24.59 |
| Lung | 8 | 13.11 |
| Breast | 7 | 11.47 |
| Colorectal | 7 | 11.47 |
| Hematological | 6 | 9.84 |
| Gastrointestinal | 4 | 6.56 |
| Head and neck | 4 | 6.56 |
| Skin | 2 | 3.28 |
| Ovarian | 2 | 3.28 |
| No response or other | 6 | 9.84 |
| Stage of cancer | ||
| Advanced stages | 36 | 59.02 |
| Early stages | 15 | 24.59 |
| No response/do not know | 10 | 16.39 |
Table 2.
Demographics of clinicians, researchers, and managers from round 1
| Demographics | Clinicians |
Researchers |
Managers |
|||
|---|---|---|---|---|---|---|
| n = 103 | % | n = 63 | % | n = 22 | % | |
| Country of residence | ||||||
| Canada | 38 | 36.90 | 16 | 25.40 | 10 | 45.45 |
| Australia | 28 | 27.18 | 22 | 34.92 | 7 | 31.82 |
| USA | 27 | 26.21 | 13 | 20.63 | 4 | 18.18 |
| UK | 2 | 1.94 | 7 | 11.11 | 1 | 4.55 |
| Other/unknown | 8 | 7.77 | 5 | 7.94 | 0 | 0 |
| Primary professional field | 0 | |||||
| Social work | 33 | 32.04 | 6 | 9.52 | 2 | 9.09 |
| Nursing | 22 | 21.36 | 15 | 23.81 | 7 | 31.82 |
| Psychology/behavioral sciences | 20 | 19.42 | 22 | 34.92 | 1 | 4.54 |
| Oncology/hematology | 9 | 8.74 | 2 | 3.18 | 3 | 13.64 |
| Psychiatry | 5 | 4.85 | 0 | 0 | 0 | 0 |
| Surgery | 2 | 1.94 | 0 | 0 | 0 | 0 |
| Public Health | 1 | 0.97 | 2 | 3.18 | 0 | 0 |
| Physiotherapy | 1 | 0.97 | 1 | 1.58 | 0 | 0 |
| Gynecology | 1 | 0.97 | 0 | 0 | 0 | 0 |
| Survivorship | 1 | 0.97 | 0 | 0 | 0 | 0 |
| Management | 1 | 0.97 | 0 | 0 | 5 | 22.73 |
| Primary care | 0 | 0 | 2 | 3.17 | 0 | 0 |
| Other | 2 | 1.94 | 11 | 17.46 | 2 | 9.09 |
| Did not answer | 5 | 4.85 | 2 | 3.18 | 2 | 9.09 |
| No. of years’ experience | ||||||
| More than 18 years | 34 | 33.01 | 24 | 38.1 | 9 | 40.91 |
| 12–17 years | 28 | 27.18 | 13 | 20.63 | 5 | 22.72 |
| 6–11 years | 30 | 29.13 | 15 | 23.81 | 3 | 13.64 |
| 0–5 years | 7 | 6.80 | 8 | 12.70 | 2 | 9.09 |
| Did not answer | 4 | 3.88 | 3 | 4.76 | 3 | 13.64 |
| Disease site population | ||||||
| Mixed | 39 | 37.86 | 7 | 11.11 | 7 | 31.82 |
| Breast | 14 | 13.59 | 5 | 7.93 | 1 | 4.55 |
| Hematology | 9 | 8.74 | 1 | 1.59 | 0 | 0 |
| Head and neck | 4 | 3.88 | 2 | 3.17 | 0 | 0 |
| Gastrointestinal | 4 | 3.88 | 0 | 0 | 0 | 0 |
| Genitourinary (prostate, kidney) | 1 | 0.97 | 2 | 3.17 | 1 | 4.55 |
| Lung | 4 | 3.88 | 1 | 1.59 | 0 | 0 |
| Gynecological | 2 | 1.94 | 1 | 1.59 | 0 | 0 |
| Palliative care/hospice | 3 | 2.91 | 1 | 1.59 | 0 | 0 |
| Stem cell transplant | 1 | 0.97 | 0 | 0 | 0 | 0 |
| Well-being | 0 | 0 | 1 | 1.59 | 0 | 0 |
| Advanced cancers | 0 | 0 | 1 | 1.59 | 0 | 0 |
| Not applicable | 11 | 10.68 | 33 | 52.38 | 9 | 40.91 |
| Did not answer | 11 | 10.68 | 8 | 12.7 | 4 | 18.18 |
Priority research topics
Round 1
Participants provided a total of 1180 responses, representing a mean of 4.5 responses per participant. After removing responses that were beyond the scope of this study (n = 59), double responses, and responses from participants who submitted their survey twice (n = 50), the remaining responses were combined into 86 topics within 10 content areas. These were (a) impact of cancer on caregivers (21 items); (b) education, training, and support programs for caregivers (13 items); (c) vulnerable caregivers (12 items); (d) caregivers’ role in health care (11 items); (e) use of technology (8 items); (f) financial cost of caregiving (6 items); (g) caregiver-centered cancer care (5 items); (h) policy and advocacy (5 items); (i) integrating research into cancer care for caregivers (4 items); and (j) environmental scan (1 item).
Round 2
In round 2, the response rate ranged from 64% for managers to 82% for caregivers. Results of round 2 are presented in Table 3. Across items and panels, the proportion of stakeholders giving a rating of 3 or 4 ranged from 13.1% (use CD-ROM to deliver interventions) to 100% (caregivers of low income or with limited education).
Table 3.
Round 2: Delphi panels’ ratings and rankings of research topics that reached consensus
| Research topics | Caregivers (n = 50) |
Researchers (n = 45) |
Clinicians (n = 67) |
Managers (n = 14) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | Rank | IQR | % | Rank | IQR | % | Rank | IQR | % | Rank | IQR | |
| Content area: Impact of cancer on caregivers | ||||||||||||
| Caregivers’ patterns of social burden | 53.19 | 35 | 1 | 81.40 | 13 | 1 | 75.00 | 18 | 0.5 | 64.29 | 8 | 2 |
| Characteristics of caregivers at high-risk of burden or burnout | 77.08 | 12 | 1 | 95.35 | 1 | 1 | 87.30 | 4 | 1* | 85.71 | 3 | 1 |
| Characteristics of “successful” caregivers | 60.42 | 29 | 1 | 88.37 | 6 | 1 | 76.19 | 17 | 1 | 71.43 | 7 | 1 |
| Caregivers’ coping strategies | 81.25 | 8 | 1 | 88.37 | 6 | 1 | 74.60 | 19 | 2 | 78.57 | 5 | 0 |
| Content area: Education, training, and support programs for caregivers | ||||||||||||
| Caregiver peer mentoring or coaching (one-on-one, group, or technology-based) | 63.83 | 25 | 1 | 88.37 | 6 | 1 | 67.19 | 29 | 2 | 64.29 | 8 | 1 |
| Home care | 83.33 | 6 | 1 | 90.70 | 4 | 1 | 88.89 | 3 | 1 | 84.62 | 4 | 1* |
| Training for communicating with patient and other family members | 76.60 | 13 | 1 | 83.33 | 11 | 1 | 90.32 | 2 | 1 | 50.00 | 13 | 1 |
| Practical training (e.g., medication management) | 64.58 | 24 | 1.5 | 76.74 | 17 | 1 | 74.19 | 20 | 1 | 85.71 | 3 | 1 |
| Content area: Vulnerable caregivers | ||||||||||||
| Sandwich generation caregivers | 64.58 | 24 | 1.5 | 88.64 | 5 | 1* | 72.58 | 22 | 2 | 64.29 | 8 | 2 |
| Older caregivers | 73.91 | 15 | 1 | 86.36 | 8 | 1 | 84.13 | 6 | 1 | 57.14 | 10 | 2 |
| Caregivers living in a rural area | 58.33 | 30 | 1 | 88.37 | 6 | 1* | 80.95 | 10 | 1 | 85.71 | 3 | 1 |
| Culturally and linguistically diverse caregivers | 56.25 | 32 | 1 | 88.64 | 5 | 1 | 66.13 | 30 | 2 | 92.86 | 2 | 1 |
| Caregivers of low income or with limited education | 62.50 | 27 | 2 | 76.74 | 17 | 1 | 70.97 | 25 | 1 | 100.00 | 1 | 0 |
| Content area: Use of technology | ||||||||||||
| Web or Internet | 58.33 | 30 | 2 | 83.72 | 10 | 1 | 73.02 | 21 | 2 | 85.71 | 3 | 1 |
| Mobile phone technology (e.g., apps) | 54.17 | 34 | 1 | 81.40 | 13 | 1 | 73.02 | 21 | 2 | 71.43 | 7 | 2** |
| Online chat (e.g., video chat like “Skype”) | 65.96 | 23 | 2 | 81.40 | 13 | 1 | 74.60 | 19 | 2 | 85.71 | 3 | 1 |
| Content area: Caregivers’ role in health care | ||||||||||||
| Caregivers’ perspectives on gaps in health services | 79.17 | 9 | 1 | 81.82 | 12 | 1 | 84.13 | 6 | 1 | 71.43 | 7 | 2** |
| Communication patterns among patients, their caregivers, and the health care team | 81.25 | 8 | 1 | 75.00 | 18 | 1.5 | 74.60 | 19 | 2 | 57.14 | 10 | 2 |
| Caregiver perspectives on how support and information can best be provided to them by health care professionals | 87.50 | 3 | 1 | 90.91 | 3 | 1 | 90.48 | 1 | 1 | 85.71 | 3 | 0 |
| Caregivers’ and patients’ view of the role of the caregiver in cancer care | 87.50 | 3 | 0.5 | 65.91 | 29 | 1 | 74.19 | 20 | 2 | 57.14 | 11 | 1 |
| Impact of caregivers’ involvement in patients’ care on their recovery and/or outcomes | 75.00 | 14 | 1.5 | 70.45 | 22 | 2 | 83.87 | 7 | 1 | 85.71 | 3 | 1 |
| Health care professionals’ perceived “responsibility” towards caregivers | 68.75 | 20 | 2 | 62.79 | 32 | 2 | 80.65 | 11 | 1 | 71.43 | 7 | 1 |
| Caregiver role in planning advanced directives | 81.25 | 8 | 0.5 | 79.55 | 14 | 1 | 71.43 | 24 | 2 | 64.29 | 8 | 2 |
| Factors that contribute to positive caregiver-patient relationships | 82.98 | 7 | 1 | 77.27 | 16 | 1 | 79.03 | 13 | 1 | 78.57 | 5 | 1 |
| Content area: Caregiver-centered cancer care | ||||||||||||
| Screening to identify caregivers at greatest risk of burden | 84.78 | 5 | 1 | 90.70 | 4 | 1* | 82.26 | 9 | 1* | 85.71 | 3 | 0 |
| Caregiver needs assessment integrated in usual care | 56.25 | 32 | 1 | 86.05 | 9 | 1 | 74.19 | 20 | 2 | 64.29 | 8 | 2 |
| Training for health care professionals working with caregivers | 72.92 | 17 | 1 | 86.05 | 9 | 1 | 74.19 | 20 | 2 | 78.57 | 5 | 1 |
| Barriers to caregivers accessing existing services | 73.33 | 16 | 2 | 81.40 | 13 | 1 | 80.65 | 11 | 1 | 78.57 | 5 | 1 |
| Content area: Integrating research into cancer care for caregivers | ||||||||||||
| Develop guidelines that describe the best way to support caregivers in cancer care | 68.75 | 20 | 2 | 90.70 | 4 | 1 | 80.95 | 10 | 1 | 71.43 | 7 | 2 |
| Identify barriers and facilitators to providing the best possible care to caregivers | 76.60 | 13 | 1 | 88.37 | 6 | 1 | 79.37 | 12 | 1 | 71.43 | 7 | 2 |
| Content area: Financial cost of caregiving | ||||||||||||
| Cost benefits of informal caregiving to the health care system | 82.98 | 7 | 1 | 93.02 | 2 | 1* | 76.19 | 17 | 1 | 78.57 | 5 | 1* |
| Financial impact of “burnout” for caregivers and society | 85.11 | 4 | 1 | 86.05 | 9 | 1 | 85.71 | 5 | 1 | 85.71 | 3 | 1 |
| Impacts of financial demands on caregivers | 95.74 | 1 | 1 | 81.40 | 13 | 1 | 88.89 | 3 | 1 | 84.62 | 4 | 1 |
| Direct costs of caregiving for caregivers | 82.98 | 7 | 1 | 83.72 | 10 | 1 | 82.54 | 8 | 1 | 92.86 | 2 | 1 |
| Indirect costs of caregiving | 78.26 | 11 | 1 | 86.05 | 9 | 1 | 82.54 | 8 | 1 | 78.57 | 5 | 1 |
| Cost-effectiveness of different caregiver interventions | 67.39 | 21 | 2 | 88.10 | 7 | 1 | 77.42 | 16 | 1 | 71.43 | 7 | 2 |
| Content area: Policy and advocacy | ||||||||||||
| Impact of health reforms, programs, and policies on caregivers | 93.02 | 2 | 1* | 74.42 | 19 | 2 | 77.78 | 15 | 1 | 78.57 | 5 | 1 |
All research topics included (those that reached consensus in at least one panel) had a median value of 3 or 4 on a 4-point scale (1 = not important to do more research to 4 = very important to more research). Those denoted with a * after the IQR have a median of 4.
Those with ** have a median of 3.5. All other topics received a median rating of 3. % is the percent of participants who rated the topic 3 or 4 on a 4-point Likert scale (1 = not important to do more research to 4 = very important to more research). Rank is how the item was ranked out of the total by the panel according to % agreement. Items that did not reach consensus in any group were removed from this table. % in bold achieved consensus
IQR interquartile range
Caregivers agreed on the importance of 13/86 research topics. The top four topics based on percent consensus included the following: Impacts of financial demands on caregivers (95.74%), Impact of health reforms, programs, and policies on caregivers (93.02%), Caregiver perspectives on how support and information can best be provided to them by health care professionals (87.50%), and Caregivers’ and patients’ view of the role of the caregiver in cancer care (87.50%).
Researchers achieved consensus on the most topics (28/86 topics). The top ranking topic was Characteristics of caregivers at high-risk of burden or burnout (95.35%). Other top ranking topics included Cost benefits of informal caregiving to the health care system (93.02%), Caregiver perspectives on how support and information can best be provided to them by health care professionals (90.91%), and Screening to identify caregivers at greatest risk of burden (90.70%).
For clinicians, 17/86 topics achieved consensus, with Caregiver perspectives on how support and information can best be provided to them by health care professionals (90.48%) also achieving high consensus in this panel. Other high consensus topics were Training for communicating with patient and other family members (90.32%), Impacts of financial demands on caregivers (88.89%), and Home care interventions (88.89%).
Managers agreed that 14/86 topics were important, with 100% of managers agreeing for more research among Caregivers of low income or with limited education. Other top ranking topics, included Direct costs of caregiving for caregivers (92.86%) and Culturally and linguistically diverse (CALD) caregivers (92.86%).
Six items achieved 80% consensus across all four panels: (a) Home care interventions, (b) Caregiver perspectives on how support and information can best be provided to them by health care professionals, (c) Screening to identify caregivers at greatest risk of burden, (d) Financial impact of “burnout” for caregivers and society, (e) Impacts of financial demands on caregivers, and (f) Direct costs of caregiving for caregivers. Of note, half of these items are from the financial cost of caregiving content area.
Comparison of ratings given to research topics within each content area revealed that panels significantly differed on the rating given to topics in the following content areas: impact of cancer on caregivers (p = 0.003), vulnerable caregivers (p < 0.05), and use of technology (p = 0.014). For impact of cancer on caregivers, only four items achieved consensus in at least one panel, with researchers rating these items more highly (87%), particularly in comparison to caregivers (66%). None of the vulnerable caregivers topics achieved 80% consensus among caregivers, but this was a content area prioritized by researchers (e.g., older caregivers or sandwich generation caregivers who are providing care to older family members while also raising children) and to a certain extent managers (e.g., caregivers living in a rural area). Regarding the use of technology in supporting caregivers, managers (84%), and researchers (86%) identified the following as priorities: Web or Internet, mobile phone technology, and online chat. However, caregivers did not prioritize any of these topics (61%, p = 0.014). There were no statistically significant differences across panels for the other content areas. Environmental scan and policy and advocacy research were overall given low priority across panels.
Round 3
In round 3, 12 new topics were proposed based on recurrent themes in participants’ comments in round 2 (Tables 4 and 5). High importance consensus rating ranged from 15.15% (Caregivers who live in a different city than the patient) to 100% (Barriers in providing care, Caregivers of patients in palliative care). As detailed in Table 4, participants’ reevaluation of the importance of remaining topics led to additional consensus. For caregivers, 15 items were added, with top ranking topics including Resources and support for caregivers about death and dying (92.86%) and Caregivers’ patterns of emotional burden (90.63%).
Table 4.
Round 3: Delphi panels’ ratings and rankings of research topics that reached consensus
| Research topics | Caregivers (n = 32) |
Researchers (n = 34) |
Clinicians (n = 33) |
Managers (n = 11) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | Rank | IQR | % | Rank | IQR | % | Rank | IQR | % | Rank | IQR | |
| Content area: Impact of cancer on caregivers | ||||||||||||
| Caregivers’ patterns of emotional burden | 90.63 | 2 | 1 | 75.76 | 13 | 1 | 72.73 | 8 | 1 | |||
| Characteristics of caregivers at high-risk of burden or burnout | 81.25 | 7 | 1** | |||||||||
| Compare the level of burden experienced by cancer caregivers with that of caregivers of patient with other illnesses | 18.75 | 43 | 1§ | 31.25 | 23 | 1§ | 30.30 | 35 | 1§ | 36.36 | 20 | 1§ |
| Characteristics of “successful” caregivers | 62.50 | 23 | 1 | 87.88 | 2 | 1 | 54.55 | 14 | 1 | |||
| Caregivers’ coping strategies | 81.82 | 8 | 1 | 72.73 | 8 | 2 | ||||||
| Variations in burden according to caregiver’s age | 68.75 | 17 | 1.25 | 45.45 | 22 | 1§ | 39.39 | 33 | 1§ | 18.18 | 22 | 1§ |
| Barriers in providing care (e.g., transportation, insurance delays) | 71.88 | 13 | 2 | 63.64 | 18 | 1 | 66.67 | 19 | 1 | 100.00 | 1 | 1 |
| Caregiver guilt | 80.65 | 8 | 1 | 66.67 | 17 | 1 | 75.76 | 13 | 1 | 63.64 | 11 | 1 |
| Caregivers’ patterns of needs, including psychosocial, physical, and spiritual needs | 83.87 | 4 | 1 | 71.88 | 16 | 1 | 63.64 | 21 | 2 | 63.64 | 11 | 2 |
| New topic: Impact on caregivers who are already dealing with their own serious illness or chronic health concerns | 78.57 | 9 | 0.5 | 78.79 | 9 | 1 | 83.33 | 7 | 1 | 55.56 | 13 | 1 |
| Content area: Education, training, and support programs for caregivers | ||||||||||||
| Education sessions about patient’s illness | 83.33 | 5 | 1 | 62.50 | 19 | 1 | 69.69 | 18 | 0.5 | 72.73 | 8 | 1 |
| Training for communicating with patient and other family members | 80.65 | 8 | 1 | 54.55 | 14 | 1 | ||||||
| Training on finding and locating resources | 64.52 | 20 | 2 | 53.13 | 21 | 1 | 72.72 | 15 | 1 | 81.82 | 4 | 0 |
| Practical training | 64.52 | 20 | 2 | 78.13 | 10 | 1 | 81.81 | 9 | 1* | |||
| Stress management training | 64.52 | 20 | 1 | 75.00 | 14 | 1.5 | 78.78 | 11 | 90.91 | 2 | 1* | |
| Health promotion programs for caregivers | 51.72 | 32 | 1 | 84.38 | 6 | 1** | 81.81 | 9 | 1 | 36.36 | 20 | 1§ |
| New topic: Resources and support for caregivers about death and dying, including end of life care at home | 92.86 | 1 | 1 | 94.12 | 3 | 1 | 85.71 | 4 | 1** | 80.00 | 6 | 1 |
| Content area: Vulnerable caregivers | ||||||||||||
| Caregivers who live in a different city/country than the patient | 38.71 | 43 | 1§ | 42.42 | 22 | 1§ | 15.15 | 38 | 0§ | 36.36 | 20 | 1§ |
| Sandwich generation caregivers | 61.29 | 24 | 1 | 87.88 | 2 | 1 | 63.64 | 11 | 2 | |||
| Caregivers living in a rural area | 58.06 | 26 | 1 | |||||||||
| Caregivers of low income or with limited education | 77.42 | 10 | 1 | 81.82 | 8 | 1* | 69.70 | 17 | 1 | |||
| Caregivers of patients in palliative care | 66.67 | 19 | 1 | 100.00 | 1 | 0* | 66.67 | 19 | 1 | 100.00 | 1 | 0* |
| Content area: Use of technology | ||||||||||||
| Web or Internet (e.g., interactive website) | 58.06 | 26 | 2 | 84.85 | 5 | 1 | ||||||
| Mobile phone technology (e.g., apps) | 45.16 | 37 | 1§ | 78.79 | 10 | 1 | 81.82 | 4 | 1* | |||
| Online chat (e.g., video chat like “Skype” or instant messaging) | 61.29 | 24 | 1 | 81.82 | 8 | 1 | ||||||
| Content area: Caregivers’ role in health care | ||||||||||||
| Communication patterns among patients, their caregivers, and the health care team over time | 75.76 | 8 | 0 | 84.85 | 5 | 1 | 81.82 | 4 | 1* | |||
| Caregivers’ involvement in patients’ treatment decision-making | 83.87 | 4 | 1 | 81.82 | 8 | 1 | 54.55 | 14 | 1 | |||
| Impact of caregivers’ involvement in patients’ care on their recovery and/or outcomes | 87.10 | 3 | 1 | 66.67 | 17 | 1 | ||||||
| Caregivers’ perceived level of preparedness for undertaking their roles and responsibilities | 74.19 | 12 | 2 | 81.82 | 8 | 1 | 66.67 | 19 | 1 | 81.82 | 5 | 1* |
| Caregiver role in planning advanced directives and living wills | 84.85 | 1 | 78.79 | 10 | 1 | 72.73 | 8 | 2 | ||||
| Factors that contribute to positive caregiver-patient relationships | * | 84.85 | 1 | 81.82 | 8 | 1 | 81.82 | 4 | 0 | |||
| Content area: Caregiver-centered cancer care | ||||||||||||
| Caregiver needs assessment integrated in usual care | 54.84 | 29 | 2 | 90.63 | 6 | 1 | 69.70 | 17 | 2 | 63.64 | 11 | 2 |
| Training for health care professionals working with caregivers | 87.10 | 3 | 1 | 84.85 | 5 | 1 | 90.91 | 2 | 1 | |||
| Barriers to caregivers accessing existing support and services | 72.73 | 8 | 2 | |||||||||
| New topic: Extent to which current services are aligned with caregivers’ needs | 81.48 | 6 | 1 | 83.87 | 7 | 1 | 83.33 | 7 | 1** | 77.78 | 7 | 0 |
| Content area: Integrating research into cancer care for caregivers | ||||||||||||
| Develop guidelines that describe the best way to support caregivers in cancer care | 80.65 | 8 | 1* | 72.72 | 9 | 2* | ||||||
| Identify barriers and facilitators to providing the best possible care to caregivers | 87.10 | 3 | 1 | 84.84 | 6 | 1 | 63.63 | 12 | 2 | |||
| Inform the public about the challenges and issues faced by caregivers | 41.94 | 40 | 1§ | 56.25 | 20 | 1 | 81.81 | 9 | 1* | 54.54 | 15 | 2 |
| New topic: Developing and evaluating sustainable interventions that can be translated into practice | 62.96 | 22 | 2 | 96.88 | 2 | 1* | 93.33 | 1 | 1* | 90.00 | 3 | 1 |
| New topic: Implementation of the caregiver interventions we already know are effective | 75.00 | 11 | 1* | 90.91 | 4 | 1* | 86.66 | 3 | 1 | 80.00 | 6 | 1 |
| New topic: Identify best ways for delivering resources to caregivers to overcome barriers of high burden and low time | 78.57 | 9 | 1 | 77.42 | 11 | 1 | 86.66 | 3 | 1 | 50.00 | 16 | 2§ |
| Content area: Environmental scan | ||||||||||||
| Conduct environmental scans to identify the resources and services that are currently available for cancer caregivers | 56.67 | 29 | 2 | 74.19 | 15 | 0.5 | 75.76 | 13 | 1 | 80.00 | 6 | 1 |
| Content area: Financial cost of caregiving | ||||||||||||
| Indirect costs of caregiving (e.g., work time and productivity lost) | 81.25 | 7 | 1 | 63.64 | 11 | 2 | ||||||
| Cost-effectiveness of different caregiver interventions | 64.52 | 20 | 2 | 72.73 | 8 | 2 | ||||||
| Content area: Policy and advocacy | ||||||||||||
| Impact of health reforms, programs, and policies on caregivers (e.g., work leave, reimbursement programs) on caregivers | 75.76 | 13 | 0 | 72.73 | 14 | 1.5 | 81.82 | 5 | 0 | |||
Topics that reached consensus in round 2 were not included in the round 3 questionnaires, these cells were left blank. Research topics denoted with a * after the IQR have a median of 4 on a 4-point Likert scale (1 = not important to do more research to 4 = very important to more research).
Those with ** have a median of 3.5, and those with § have a median of 2. All other topics received a median rating of 3. % is the percent of participants who rated the topic 3 or 4 on a 4-point scale (1 = not important to do more research to 4 = very important to more research). Rank is how the item was ranked out of the total by the panel according to % agreement. Items that did not reach consensus in any group were removed from this table. % in bold achieved consensus.
IQR interquartile range
Table 5.
Topics that reached consensus across all four panels
| Topics |
|---|
| 1. Home care interventions |
| 2. Caregiver perspectives on how support and information can best be provided to them by health care professionals |
| 3. Screening to identify caregivers at greatest risk of burden |
| 4. Financial impact of “burnout” for caregivers and society |
| 5. Impacts of financial demands on caregivers |
| 6. Direct costs of caregiving for caregivers |
| 7. Characteristics of caregivers at high-risk of burden or burnout |
| 8. Training for health care professionals working with caregivers |
| 9. Resources and support for caregivers about death and dying |
Researchers added 11 topics, with 100% of them agreeing on Caregivers of patients in palliative care. Other topics achieving high consensus included Developing and evaluating sustainable interventions that can be translated into practice (96.88%), and Resources and support for caregivers about death and dying (94.12%).
Clinicians added 20 items to their list, including Developing and evaluating sustainable interventions that can be translated into practice (93.33%). The following items also achieved high consensus: Cost-effectiveness of different caregiver interventions (87.88%), Characteristics of ‘successful’ caregivers (87.88%), and Sandwich generation caregivers (87.88%).
Managers achieved consensus on 14 more items; 100% of them agreed on Caregivers of patients in palliative care and Barriers in providing care.
Three additional items achieved consensus across all panels in round 3 (total 9 items, see Table 5). These were (a) Characteristics of caregivers at high-risk of burden or burnout, (b) Training for health care professionals working with caregivers, and (c) Resources and support for caregivers about death and dying.
GLMM analyses of topics that achieved consensus in at least one panel revealed that stakeholders continued to significantly differ on the ratings they gave to topics in the following two content areas: vulnerable caregivers (p < 0.05) and use of technology (p = 0.006). Response patterns again showed that caregivers did not prioritize these topics. Panels also significantly differed for content area integrating research into cancer care for caregivers, whereby clinicians gave an overall higher priority rating to these six topics than caregivers (87 vs. 73%, p = 0.031).
Discussion
Clinicians, managers, researchers, and caregivers in the present study agreed on nine consensus research topics that provide a framework for developing a cancer caregiver research agenda and solid research partnerships that cross borders and disciplines. Specifically, consensus items revealed that the financial impact of caregiving required particularly more research attention along with research on routine screening of important caregiver-reported outcomes and training of clinicians. Despite this consensus, panels significantly differed on the priorities given to topics within the vulnerable caregiver and technology content areas. Each of these key findings is discussed in turn.
In the financial impact of caregiving content area, panels agreed on the following three of the six items: Financial impact of “burnout” for caregivers and society, Impacts of financial demands on caregivers, and Direct costs of caregiving for caregivers. The high-importance given to this content area may represent a universal recognition of the responsibilities caregivers take on and the ensuing costs incurred. This is also reflected in the priority topic Home care interventions (i.e., supportive and health care services provided within the home throughout the illness). A recent review by Girgis and Lambert [7] of the financial cost of caregiving found that informal caregiving represents 18–33% of the total cost of cancer. As part of this review, only one European [9] and an American [28] study detailed the direct and indirect costs of caregiving. No study reviewed addressed the financial consequences of caregiver burnout.
The nine consensus research topics further highlighted the need for Screening to identify caregivers at greatest risk of burden. Consistent with this finding was the prioritization by researchers of the topic Caregiver needs assessment integrated in usual care. Integrating routine screening of patient-reported outcomes (PROs) is a priority in cancer care and has been the focus of numerous studies [18]. The present Delphi study adds that stakeholders are now recognizing the need to extend this research to caregivers. Although one PRO often measured is distress, the topic Routine screening for distress in caregivers did not achieve consensus, supporting the uniqueness of caregiver-reported outcomes (CROs).
Across panels, another priority research topic was Training for HCPs working with caregivers. This topic is consistent with the findings from a Delphi study among European oncology nurses [3], whereby cancer nursing education was by far the most important priority research topic. Although communication training for HCPs who care for patients with cancer has received some attention [8], equivalent studies with caregivers have not been found. A study by Moniz et al. [19] found positive effects of training community health nurses to help family caregivers manage behavioral changes in their relative with dementia, including reduced caregiver depression and improved coping.
Despite agreement on nine topics, more differences than similarities were noted across panels. One significant difference among panels was the priority given to research on vulnerable caregiver sub-groups. In round 1, 12 vulnerable caregiver sub-groups were identified: (a) live in a different city/country than the patient, (b) sandwich generation caregivers, (c) older caregivers, (d) caregivers of patients with multi-morbidities, (e) caregivers living in a rural area, (f) LGBTQ caregivers, (g) CALD caregivers, (h) indigenous caregivers, (i) male caregivers, (j) caregivers of low income or with limited education, (k) caregivers other than patient’s spouse, and (l) caregivers of patients in palliative care. None of these groups were subsequently prioritized by caregivers; however, the other panels prioritized sub-groups such as CALD caregivers and older caregivers. This divergence may reflect caregiver’s focus on their individual experience and they might not be aware of the challenges faced by particular sub-groups of caregivers or may have difficulty conceptualizing how these topics might be suitable for a research agenda. The demographics of the caregivers in this study suggest that the majority were not from a CALD background. However, the prioritization of research on vulnerable caregiver sub-groups mirror results recently published by Kent et al. [15] on research priorities for cancer caregiving identified during a meeting with researchers, clinicians, advocates, and representatives from national funding agencies. However, this study did not report on advocates’ or caregivers’ priorities separately, which might explain the discrepancy with the present study.
Another content area not prioritized by caregivers was the use of technologies to deliver interventions. In round 1, eight types of technologies were identified: (a) Web or Internet, (b) mobile phone technology, (c) telephone services, (d) e-mail services, (e) videos, (f) online chat, (g) CD-ROMs, and (h) social media. Researchers, clinicians, and managers narrowed this list down to Web or Internet, mobile phone technology, and online chat. These stakeholders might have particularly focused on intervention design and their delivery, as they are acutely aware of the need to provide low-cost resources to service large-scale populations of caregivers. There is increased recognition that online interventions are a convenient, cost-effective, and efficacious approach for delivering supportive care [2]. The few Internet-based caregiver interventions developed to date have shown promise in enhancing caregivers’ health and well-being [27]. Delivering interventions to caregivers using the Internet was one recommendation from another stakeholder group meeting [11] to identify gaps to the provision of evidence-informed support for caregivers of seniors with dementia or caregivers in end-of-life care. Although caregivers were included in this meeting, they might not have felt comfortable verbally expressing their opinions, which might explain the discrepancy between that study and the present one. Alternatively, findings might reflect that the caregivers in this study felt that their support needs were adequately met through traditional methods of seeking help.
In line with recent efforts to engage end users in research, topics only prioritized by caregivers should not be discounted. Based on a systematic review of the literature, Shippee et al. [25] proposed a four-component framework of service user engagement in research: patient and service user initiation, reciprocal relationships, co-learning and re-assessment, and feedback. The present Delphi study is consistent with the first component of service user initiation, as caregivers were given a voice in steering the research agenda as well as the second component - building reciprocal relationships, whereby caregivers’ perspectives are valued. Future research needs to build on the foundation established by this Delphi study and continue to involve caregivers to better understand their unique research priorities. One reason for the apparent lack of consensus among the panels might be the panels’ different interpretations of the topics.
Strengths and limitations
A strength of this study was that four panels were surveyed, including a panel of caregivers. Overall, the stakeholders were from varied fields or experience. However, most participants were based in Australia or North America and caution is warranted in extending the recommendations outside of these contexts. Further, female caregivers and those caring for people experiencing genitourinary cancers were over-represented, which may have influenced the findings. Future studies among broader community samples, including more demographically diverse caregivers may provide further insight. To capture a wide range of opinions, this study included many more participants than the recommended 10–18 per panel [13, 22], enhancing the credibility of the findings. In line with the most accepted practice, the thresholds for consensus were determined prior to data collection. Finally, to begin the process of disseminating the results, online meetings were offered to each of the panels. In terms of limitations, results are potentially based on stakeholders’ perception of the research already conducted in that area. Whereas surveys are known for their low responses rates, participant attrition can be further exacerbated by the iterative nature of the Delphi process [14]. In this study, response rates across the researchers, caregivers, and managers panels were about 50% between rounds 1 and 3. However, clinicians had a lower response at 32.04%. Despite the declining response rate, the heterogeneity of the participants in each round was generally preserved [1].
Implications
Identification of research priorities for caregiver research in cancer care is imperative in the development of the evidence-base needed for practice. The present Delphi study identified a list of nine research priorities agreed on by all stakeholders that can guide strategic directions in this field. This study also identified priorities unique to caregivers that should not be discounted, even if these did not achieve consensus with other stakeholder panels, given the recent efforts to engage end users in research. Addressing research priorities identified with designs that continue to engage key stakeholders is suggested, such as experience-based co-design (EBCD) [5]. In terms of knowledge translation, summaries of findings, tailored to specific audiences along with statements detailing explicit policy and practice implications, will be disseminated to relevant national and international professional groups, patient representative groups, and funding organizations. These, for example, include the Canadian Partnership Against Cancer, the Clinical Oncology Society of Australia, American Psychosocial Oncology Society, Cancer Australia, International Psycho-Oncology Society, the Canadian Association of Psychosocial Oncology, which are well positioned to integrate these findings that subsequently can influence policy, research priorities and practice. In addition, national carers organizations as well as others representing patients’/caregivers’ views (e.g., Coalition Priorité Cancer in Quebec) will be provided a summary of the key findings to inform their ongoing advocacy activities.
Funding information
This study was funded by a Canadian Institutes of Health Research (CIHR) planning and dissemination grant. S. Lambert is the holder of a Canada Research Chair Tier 2 in self-management. A. Girgis is supported by a Cancer Institute New South Wales Grant. Y. Kim is supported by an American Cancer Society Research Scholar Grant and a National Institute of Health Grant. C. G. Loiselle is supported, in part, by the McGill University Christine and Herschel Victor/Hope & Cope Chair in Psychosocial Oncology.
Footnotes
Conflict of interest The authors declare that they have no conflict of interest.
References
- 1.Alake-Tuenter E, Biemans HJA, Tobi H, Mulder M (2013) Inquiry-based science teaching competence of primary school teachers: a Delphi study. Teach Teach Educ 35:13–24 [Google Scholar]
- 2.Beatty L, Lambert S (2013) A systematic review of internet-based self-help therapeutic interventions to improve distress and disease-control among adults with chronic health conditions. Clin Psychol Rev 33:609–622 [DOI] [PubMed] [Google Scholar]
- 3.Browne N, Robinson L, Richardson A (2002) A Delphi study on the research priorities of European oncology nurses. Eur J Oncol Nurs 6:133–144 [DOI] [PubMed] [Google Scholar]
- 4.Chang L (1994) A psychometric evaluation of 4-point and 6-point Likert-type scales in relation to reliability and validity. Appl Psychol Meas 18:205–215 [Google Scholar]
- 5.Donetto S, Tsianakas V, Robert G (2014) Using Experience-based Co-design to improve the quality of healthcare: mapping where we are now and establishing future directions. In: Editor (ed)^(eds) Book Using Experience-based Co-design to improve the quality of healthcare: mapping where we are now and establishing future directions. King’s College London, City, London [Google Scholar]
- 6.Garrett M, Fitzmaurice NML, Ware JH (2011) Applied longitudinal analysis, 2nd edn. Wiley,Hoboken, p 740 [Google Scholar]
- 7.Girgis A, Lambert SD (2017) Cost of informal caregiving in cancer care. Cancer Forum 41:16–22 [Google Scholar]
- 8.Gysels M, Richardson A, Higginson IJ (2004) Communication training for health professionals who care for patients with cancer: a systematic review of effectiveness. Support Care Cancer 12:692–700 [DOI] [PubMed] [Google Scholar]
- 9.Hanly P, Céilleachair AÓ, Skally M, O’Leary E, Staines A, Kapur K, Fitzpatrick P, Sharp L (2013) Time costs associated with informal care for colorectal cancer: an investigation of the impact of alternative valuation methods. Appl Health Econ Health Policy 11:193–203 [DOI] [PubMed] [Google Scholar]
- 10.Heiko A (2012) Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc Chang 79:1525–1536 [Google Scholar]
- 11.Holroyd-Leduc JM, McMillan J, Jette N, Brémault-Phillips SC, Duggleby W, Hanson HM, Parmar J (2017) Stakeholder meeting: integrated knowledge translation approach to address the caregiver support gap. Can J Aging 36:108–119 [DOI] [PubMed] [Google Scholar]
- 12.Hosmer D, Lemeshow S, Sturdivant RX (2013) Applied logistic regression, 3rd edn. Wiley,Hoboken, p 528 [Google Scholar]
- 13.Hsu C-C, Sandford BA (2007) The Delphi technique: making sense of consensus. Pract Assess Res Eval 12:1–8 [Google Scholar]
- 14.Keeney S, Hasson F, McKenna H (2006) Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs 53:205–212 [DOI] [PubMed] [Google Scholar]
- 15.Kent EE, Rowland JH, Northouse L, Litzelman K, Chou W-YS, Shelburne N, Timura C, O’Mara A, Huss K (2016) Caring for caregivers and patients: Research and clinical priorities for informal cancer caregiving. CNCR Cancer 122:1987–1995 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kim Y, Schulz R (2008) Family caregivers’ strain: comparative analysis of cancer caregiving with dementia, diabetes, and frail elderly caregiving. J Aging Health 20:483–503 [DOI] [PubMed] [Google Scholar]
- 17.Lambert SD, Girgis A, Levesque J (2016) The impact of cancer and chronic conditions on caregivers and family members. In: Koczwara B (ed) Cancer and chronic conditions: addressing the problem of multimorbidity in Cancer patients and survivors. Springer Science+Business Media, Berlin [Google Scholar]
- 18.Mitchell AJ, Vahabzadeh A, Magruder K (2011) Screening for distress and depression in cancer settings: 10 lessons from 40 years of primary-care research. Psychooncology 20:572–584 [DOI] [PubMed] [Google Scholar]
- 19.Moniz-Cook E, Elston C, Gardiner E, Agar S, Silver M, Win T, Wang M (2008) Can training community mental health nurses to support family carers reduce behavioural problems in dementia? An exploratory pragmatic randomised controlled trial. Int J Geriatr Psychiatry 23:185–191 [DOI] [PubMed] [Google Scholar]
- 20.National Institute for Health and Clinical Excellence (2004) Improving supportive and palliative care for adults with cancer. https://www.nice.org.uk/guidance/CSG4. Accessed 17 July 2018
- 21.Northouse LL, McCorkle R (2010) Spouse caregivers of cancer patients. In: Holland JC, Breitbart WS, Jacobsen PB, Lederberg MS, Loscalzo MJ, McCorkle R (eds) Psycho-oncology. Oxford university press, New York, pp 516–521 [Google Scholar]
- 22.Okoli C, Pawlowski SD (2004) The Delphi method as a research tool: an example, design considerations and applications. Inf Resour Manag J 42:15–29 [Google Scholar]
- 23.Rankin N, Butow P, Price M, Evans A (2011) Views of psycho-oncology health professionals on priority psycho-oncology research questions. Support Care Cancer 19:1133–1141 [DOI] [PubMed] [Google Scholar]
- 24.Rayens MK, Hahn EJ (2000) Building consensus using the policy Delphi method. Policy Polit Nurs Pract 1:308–315 [Google Scholar]
- 25.Shippee ND, Domecq Garces JP, Prutsky Lopez GJ, Wang Z, Elraiyah TA, Nabhan M, Brito JP, Boehmer K, Hasan R, Firwana B, Erwin PJ, Montori VM, Murad MH (2015) Patient and service user engagement in research: a systematic review and synthesized framework. Health Expect 18:1151–1166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sinha M (2013) Spotlight on Canadians: results from the General Social Survey. Portrait of caregivers, 2012. In: Editor (ed)^(eds) Book Spotlight on Canadians: results from the General Social Survey. Portrait of caregivers, 2012, City [Google Scholar]
- 27.Tang W, Chan C, So W, Leung D (2014) Web-based interventions for caregivers of cancer patients: a review of literatures. Asia Pac J Oncol Nurs 1:9–15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Van Houtven CH, Ramsey SD, Hornbrook MC, Atienza AA, van Ryn M (2010) Economic burden for informal caregivers of lung and colorectal cancer patients. Oncologist 15:883–893 [DOI] [PMC free article] [PubMed] [Google Scholar]