

Abstract
LGBT+ adults demonstrate greater cannabis-related problems (e.g., Cannabis Use Disorder [CUD]) compared to non-LGBT+ counterparts. No study has explored age-related disparities in cannabis problems across the adult lifespan, nor have studies identified specific CUD criteria that contribute to elevated CUD among LGBT+ adults. The purpose of the study was to examine associations between LGBT+ identity and age with endorsement of CUD criteria in a sample of regular cannabis consumers. An online sample of N=4334 (25.1% LGBT+) adults aged 18-64 residing in the U.S. completed an online survey about cannabis use behaviors and CUD diagnostic criteria. Bivariate contrasts revealed significantly greater CUD criteria endorsement among LGBT+ respondents, largely driven by differences at younger ages. However, this effect disappeared in the majority of adjusted logistic regression models. LGBT+ identity was associated with greater probability of use in larger amounts (adjOR=2.10, 95% CI: 1.22-3.60) and use despite physical/mental health problems (adjOR=2.51, 95% CI:1.23-5.03). No age*LGBT+ identity interactions were detected. Plotted trends depict more pronounced disparities in outcomes among LGBT+ adults under 35 years. Several potential risk and protective factors including employment, education, and reasons for use were identified. There were age-related differences in these characteristics among LGBT+ and non-LGBT+ respondents. Initial findings highlight the need for LGBT+ research examining trends in health outcomes and sociodemographic and cannabis characteristics across the lifespan. The study also provides a substantive contribution regarding specific cannabis-related problems that young LGBT+ cannabis consumers may be more likely to endorse than their non-LGBT+ counterparts.
Keywords: LGBT+, sexual and gender minority, cannabis, cannabis use disorder, disparities
1. Introduction
LGBT+ (e.g., lesbian, gay, bisexual, transgender, etc.) adults routinely demonstrate higher rates of cannabis use and more cannabis-related problems compared to cisgender heterosexual counterparts (e.g., Boyd, Veliz & McCabe, 2020; Dyar, 2022; Schuler, Stein & Collins, 2019; Struble et al., 2022). Prevalence of cannabis use disorder (CUD) varies considerably across subgroups (Hasin, Shmulewitz & Sarvet, 2019). For example, CUD estimates are highest among young adults, a subgroup that is more likely to report consuming cannabis regularly (National Institute on Drug Abuse [NIDA], 2022) AND more likely to endorse an LGBT+ identity (Jones, 2022) compared to older peers.
LGBT+ individuals appear more likely to report frequent cannabis consumption and, among cannabis consumers, have greater likelihood and severity of CUD compared to cisgender heterosexual peers (e.g., Boyd et al., 2019; Bränström & Pachankis, 2018; Liautaud, Barrington-Trimis, Liu et al., 2021; Philbin, Mauro, Green & Martins, 2019; Schofield, Cuttler, Conner, Prince, & Addictions Research Team, 2023; Schuler, Rice, Evans-Polce & Collins, 2018). Most research in this area has yet to examine differences in rates of endorsement of specific CUD criteria. Such granular information can guide clinical efforts to assess and treat cannabis-related problems most common among LGBT+ consumers.
The leading framework for fostering a comprehensive understanding of disparities in cannabis outcomes among LGBT+ individuals is the Minority Stress Theory (Meyer, 2003) which posits that LGBT+ individuals face excess chronic stressors that contribute to worsened outcomes including substance use (Dyar, Sarno, Newcomb & Whitton, 2020). Exposure and reactivity to daily stressors decrease with age (Almeida, Rush, Mogle, Piazza, Cerino & Charles, 2023). LGBT+ samples have also demonstrated positive associations between age and resilience (Koziara, Mijas, Galbarczyk et al., 2022) that may offset the impact of minority stressors, but little is known about whether cannabis disparities vary as a function of age. Given that younger age is associated with greater cannabis-related problems in the general population (Substance Abuse and Mental Health Services Administration, 2022), younger LGBT+ consumers may have more risk factors that increase the likelihood of cannabis problems. Other sociodemographic and cannabis characteristics that contribute to disparities in criterion-level CUD problems have not been examined empirically.
The purpose of this study is to explore associations between LGBT+ identity, age, and individual CUD criteria in a sample of regular cannabis consumers aged 18-64. We anticipated that cannabis consumers who identify as LGBT+ would have greater likelihood of cannabis-related problems, and that these disparities would be most pronounced among younger LGBT+ cannabis consumers. Findings will contribute to a better understanding of cannabis problems among LGBT+ individuals across the lifespan, including potential risk and protective factors.
2. Methods
2.1. Sample Population
The sample was recruited as part of a larger study designed to develop accurate measures of cannabis consumption (Budney et al., 2022). Adults aged 18 and older from the United States were recruited from February to April 2022 via Facebook (2022) using keyword-target advertising based on self-reported interests. Advertisements contained a hyperlink to an anonymous survey administered through Qualtrics (2022). Respondents provided informed consent prior to survey access. Study procedures were approved by the Dartmouth College Committee for Protection of Human Subjects. No compensation was provided.
2.2. Survey
Respondents completed a cannabis consumption survey which included sociodemographic and self-reported cannabis use behaviors and problems (American Psychiatric Association; 2022).
2.2.1. LGBT+ Identity.
Respondents selected one option identifying the gender category that best represents them: (a) male/man, (b) female/woman, (c) transgender man, (d) transgender woman, (e) non-binary or gender fluid, (f) prefer to self-describe, and (g) prefer not to say. Respondents identified their sexual orientation by selecting one of the following options: (a) straight/heterosexual; (b) gay, (c) lesbian, (d) bisexual or pansexual, (e) prefer to self-describe, and (f) prefer not to say. Responses to both items were recoded into a single dichotomous variable ‘LGBT+ Identity’. Respondents who reported “prefer not to say” to BOTH items were dropped from analyses. Respondents who reported male/man or female/woman gender identity AND straight/heterosexual sexual identity were coded as ‘non-LGBT+’. Respondents who selected EITHER a sexual or gender minority identity were coded as ‘LGBT+’.
2.2.2. Cannabis Use Disorder Criteria.
Participants completed 16 items assessing the 11 CUD criteria from the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev; [DSM-5-TR]; Grant et al., 2015; Hasin et al., 2015). See supplementary material for item wording and scoring.
2.2.3. Sociodemographic and Cannabis Covariates.
Items surveyed sex, race/ethnicity, education, and employment status. Respondents provided their state of residence which was recoded based on state legalization status as of April 2022. Respondents also reported age of cannabis initiation, past-month frequency, and primary reason for using cannabis.
2.3. Data Analysis
Chi-square and t-tests of independence evaluated differences in sociodemographic and cannabis covariates between non-LGBT+ and LGBT+ groups. Logistic regression models with robust standard errors were used to test the main and interactive effects of LGBT+ identity and age on endorsement of CUD criteria controlling for sociodemographic and cannabis covariates. Adjusted odds ratios (adjORs) and 95% confidence intervals are reported. Descriptive analyses were run in SPSS version 28, while regression models were built and graphed in STATA version 17.
3. Results
3.1. Analytic Sample
Of the 8284 respondents who clicked the link, eligible past-week consumers who completed CUD-related items (n=5001) were included in the present study. Respondents aged 65+ (n=686) were excluded due to low LGBT+ endorsement (8.1%). Among respondents aged 18-64, 74.9% were categorized as non-LGBT+ (n=3248) and 25.1% as LGBT+ (n=1086) resulting in a final analytic sample of N=4334.
3.2. Bivariate Differences
In the overall sample, LGBT+ respondents were younger, more likely to report female-at-birth sex, and less likely to identify as non-Hispanic White than non-LGBT+ respondents. They were also more likely to be students. Regarding cannabis characteristics, LGBT+ participants were more likely to reside in a state with recreational cannabis laws and more likely to report use for recreational reasons only. LGBT+ respondents reported later age of initiation and fewer cannabis using days in the past month than non-LGBT+ respondents.
Bivariate analyses found that LGBT+ respondents were significantly more likely to report 9 of the 11 individual CUD criteria (only endorsement of interpersonal problems and of use in high-risk situations did not differ between groups), indicating substantial disparities in many types of cannabis-related problems. However, these differences were driven by greater criterion endorsement among younger LGBT+ respondents (aged 18-34 years). See Table 1 for complete bivariate results.
Table 1.
Sociodemographic and Cannabis Differences – Bivariate Results
| Overall Sample | 18 – 34 Years | 35 – 49 Years | 50 – 64 Years | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||||||
| Non-LGBT | LGBT | Test Stat | Non-LGBT | LGBT | Test Stat | Non-LGBT | LGBT | Test Stat | Non-LGBT | LGBT | Test Stat | ||
| Sociodemographic and Cannabis Covariates | |||||||||||||
|
| |||||||||||||
| Age (M) | 46.8 | 35.6 | 25.7 | 26.9 | 24.8 | 7.1 | 42.1 | 41.1 | 3.8 | 57.6 | 57.1 | 1.4 | |
|
| |||||||||||||
| Sex (%) | Female | 50.7 | 77.2 | 228.9 | 48.8 | 84.4 | 157.3 | 50.5 | 72.8 | 46.7 | 51.6 | 64.2 | 11.9 |
| Male | 48.3 | 22.8 | 51.2 | 15.6 | 49.5 | 27.2 | 48.4 | 35.8 | |||||
|
| |||||||||||||
| Race (%) | Non-Hispanic White | 86.1 | 83.0 | 6.0 | 81.8 | 82.0 | 0.7 | 83.9 | 82.5 | 0.3 | 89.3 | 86.5 | 2.1 |
| Non-Hispanic Minority | 7.3 | 8.9 | 7.7 | 8.7 | 8.9 | 9.8 | 5.9 | 8.4 | |||||
| Hispanic | 6.6 | 8.1 | 10.5 | 9.4 | 7.2 | 7.7 | 4.8 | 5.1 | |||||
|
| |||||||||||||
| Employment (%) | Employed | 60.7 | 62.3 | 243.0 | 70.9 | 62.4 | 12.2 | 75.4 | 72.2 | 7.8 | 45.3 | 49.1 | 4.8 |
| Unemployed | 35.6 | 21.2 | 9.1 | 8.8 | 23.6 | 24.7 | 54.5 | 50.0 | |||||
| Student | 3.8 | 16.5 | 19.9 | 28.9 | 1.0 | 3.1 | 0.2 | 0.9 | |||||
|
| |||||||||||||
| Education (%) | No College | 46.3 | 43.2 | 3.1 | 53.8 | 52.7 | 0.1 | 42.7 | 36.1 | 4.1 | 46.4 | 26.9 | 29.4 |
| Any College | 53.7 | 56.8 | 46.2 | 47.3 | 57.3 | 63.9 | 53.6 | 73.1 | |||||
|
| |||||||||||||
| Age of Onset (M) | 16.2 | 16.8 | −3.2 | 16.2 | 17.0 | −3.9 | 16.7 | 17.0 | −0.9 | 15.8 | 16.2 | −1.0 | |
|
| |||||||||||||
| Past-30 Days (M) | 27.1 | 25.7 | 5.9 | 26.3 | 24.7 | 3.5 | 27.4 | 27.2 | 0.5 | 27.1 | 26.4 | 1.8 | |
|
| |||||||||||||
| Cannabis Law (%) | No Law | 21.5 | 17.9 | 11.3 | 20.7 | 17.0 | 2.9 | 21.8 | 20.8 | 0.9 | 21.6 | 16.2 | 8.5 |
| Medical Law Only | 33.9 | 32.1 | 33.3 | 33.3 | 34.4 | 32.3 | 33.7 | 28.7 | |||||
| Recreational Law | 44.6 | 50.0 | 46.0 | 49.7 | 43.8 | 46.9 | 44.7 | 55.1 | |||||
|
| |||||||||||||
| Reason (%) | Medical Only | 16.3 | 10.8 | 30.1 | 7.3 | 6.0 | 1.5 | 17.9 | 15.3 | 1.1 | 18.3 | 17.6 | 0.1 |
| Recreational Only | 14.0 | 19.0 | 26.8 | 24.9 | 11.0 | 11.8 | 11.8 | 12.5 | |||||
| Both | 69.7 | 70.3 | 65.9 | 69.1 | 71.1 | 72.9 | 69.9 | 69.9 | |||||
|
| |||||||||||||
| Cannabis Use Disorder Outcomes (% Yes) | |||||||||||||
|
| |||||||||||||
| Using more than intended | 17.8 | 28.0 | 52.6 | 25.0 | 36.8 | 18.2 | 20.4 | 19.4 | 0.1 | 13.1 | 15.7 | 1.1 | |
|
| |||||||||||||
| Failed quit attempts | 13.7 | 25.9 | 86.5 | 31.8 | 37.6 | 4.1 | 12.5 | 13.2 | 0.1 | 8.2 | 11.1 | 2.1 | |
|
| |||||||||||||
| Spending a lot of time using | 51.7 | 58.0 | 13.2 | 62.8 | 64.6 | 0.4 | 54.0 | 57.3 | 1.0 | 45.9 | 41.2 | 1.7 | |
|
| |||||||||||||
| Craving | 54.4 | 63.4 | 26.5 | 64.8 | 71.0 | 4.9 | 54.5 | 55.9 | 0.2 | 50.7 | 52.8 | 0.3 | |
|
| |||||||||||||
| Problems fulfilling obligations | 3.0 | 7.4 | 40.6 | 7.3 | 11.0 | 4.7 | 2.6 | 4.2 | 2.1 | 1.7 | 1.9 | 0.03 | |
|
| |||||||||||||
| Use despite relational problems | 6.1 | 6.7 | 0.5 | 8.4 | 7.7 | 0.2 | 5.1 | 5.2 | 0.01 | 6.1 | 6.0 | 0.01 | |
|
| |||||||||||||
| Giving up important activities | 2.7 | 6.7 | 35.9 | 5.8 | 11.0 | 9.8 | 2.5 | 1.4 | 1.3 | 1.8 | 2.3 | 0.2 | |
|
| |||||||||||||
| Use in high-risk situations | 32.0 | 31.4 | 0.1 | 39.7 | 34.5 | 3.2 | 31.6 | 29.5 | 0.5 | 29.6 | 25.5 | 1.6 | |
|
| |||||||||||||
| Use despite health consequences | 10.9 | 16.2 | 21.6 | 15.5 | 21.0 | 5.7 | 7.9 | 11.1 | 3.0 | 11.6 | 10.2 | 0.4 | |
|
| |||||||||||||
| Tolerance | 24.2 | 34.3 | 42.8 | 36.3 | 43.8 | 6.5 | 25.5 | 26.4 | 0.1 | 18.9 | 19.4 | 0.04 | |
|
| |||||||||||||
| Withdrawal | 13.8 | 24.8 | 71.5 | 26.3 | 33.3 | 6.7 | 13.1 | 19.8 | 8.4 | 9.8 | 8.3 | 0.5 | |
Note.
Overall Sample: Non-LGBT n = 3248, LGBT n = 1086.
18-34 Years: Non-LGBT n = 537, LGBT n = 582.
35-49 Years: Non-LGBT n = 1197, LGBT n = 288.
50-64 Years: Non-LGBT n = 11515, LGBT n = 216.
Bolded test statistic (stat) values denote omnibus group differences at p ≤ .05.
3.3. Adjusted Logistic Regression Models
Age was negatively associated with endorsement of all CUD criteria (adjORs ranged from 0.94–0.99). LGBT+ identity was associated with increased likelihood of endorsement of two criteria including use in larger amounts or over a longer period than intended, adjOR=2.10, 95% CI: 1.22–3.60; and continued use despite physical or mental health problems, adjOR=2.51, 95% CI: 1.23-5.03. Figures 1a-1b demonstrate more pronounced differences in the probability of endorsing Criteria 1 (Figure 1a) and 9 (Figure 1b) among respondents under 35 years of age, although the overall size of the effect of LGBT+ status was small. No significant age*LGBT+ identity interactions emerged after adjusting for sociodemographic and cannabis covariates.
Figure 1: Interaction Plots from Generalized Linear Models.
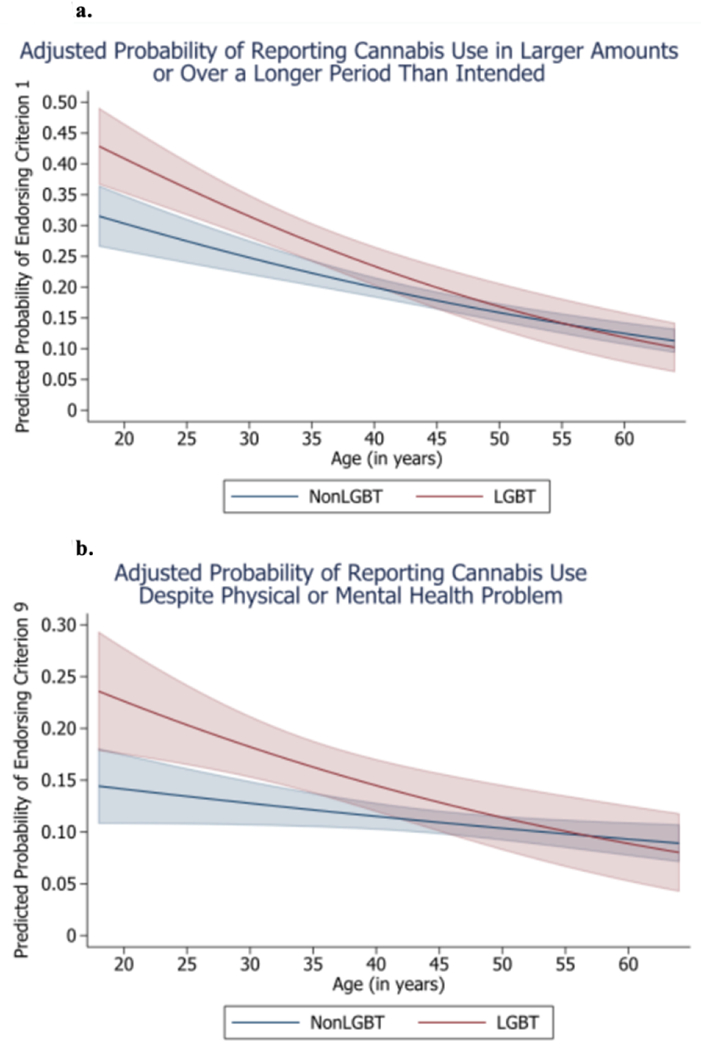
Estimated margins and 95% confidence interval (CI) bands graphed.
a. Adjusted probability of reporting cannabis use in larger amounts or over a longer period of time (Criterion 1). Main effects for LGBT+ identity (adjOR = 2.10, 95% CI: 1.22 – 3.60, p = .007) and age (adjOR = 0.97, 95% CI: 0.96 – 0.98, p < .001). Interaction non-significant (adjOR = 0.99, 95% CI: 0.97 – 1.00, p = .069).
b. Adjusted probability of reporting cannabis use despite it contributing to or worsening physical or mental health problem (Criterion 9). Main effects for LGBT+ identity (adjOR = 2.51, 95% CI: 1.23 – 5.03, p = .009) and age (adjOR = 0.99, 95% CI: 0.9 – 099, p = .019). Interaction non-significant (adjOR = 0.98, 95% CI: 0.97 – 1.00, p = .073).
3.3.1. Sociodemographic and Cannabis Covariates.
The lack of significant LGBT+ effects in adjusted models highlight the substantial impact of covariates as risk and protective factors to CUD problems. Being unemployed (versus employed) was associated with increased odds of endorsing use in larger amounts or over longer periods, failed quit attempts, spending a lot of time using, craving, problems fulfilling obligations, giving up important activities, continued use despite physical or mental health problems, tolerance, and withdrawal (adjORs ranged from 1.21–1.91). In addition, being a student (versus employed) was associated with increased odds of endorsing failed quit attempts, craving, giving up important activities, continued use despite physical or mental health problems, and withdrawal (adjORs ranged from 1.37–2.08). Having a college education was associated with reduced odds of endorsing use in larger amounts or over longer periods, spending a lot of time using, problems fulfilling obligations, and continued use despite physical or mental health problems (adjORs ranged from 0.70–0.87).
In terms of cannabis covariates, cannabis motives (reasons) for use were significantly associated with several cannabis problems. Compared to medical reasons only, use for either recreational reasons alone or combined medical/recreational reasons were associated with increased likelihood of endorsing use in larger amounts or over longer periods, failed quit attempts, spending a lot of time using, craving, giving up important activities, continued use despite physical or mental health problems, and tolerance (Recreational: adjORs ranged from 1.59 – 3.64; Medical/Recreational: adjORs ranged from 1.32–2.71). Use for combined medical and recreational reasons was also associated with increased odds of endorsing withdrawal (adjOR=1.70, 95% CI: 1.27-2.28) compared to medical only reasons for use.
4. Discussion
In an online sample of adult regular cannabis consumers, LGBT+ respondents were more likely than cisgender heterosexual counterparts to endorse using cannabis in larger amounts or over a longer period than intended and continued cannabis use despite physical or mental health problems after controlling for age, sociodemographic and cannabis covariates. Disparities in endorsement of CUD outcomes were most pronounced among young adults, although no interactive effects between LGBT+ status and age emerged.
After adjusting for age and additional sociodemographic and cannabis covariates, fewer differences in CUD criteria endorsement were found between LGBT+ and non-LGBT+ respondents. These covariates may indicate important risk and protective factors that contribute to observed disparities in cannabis problems for LGBT+ (vs. non-LGBT) individuals. These factors can further guide assessing risk of cannabis-related problems and treatment targets among LGBT+ cannabis consumers. Being unemployed and being a student were risk factors associated with endorsing several cannabis problems, while having a college education and reporting cannabis use for medical reasons reduced the odds of endorsing cannabis problems. These factors are reliably associated with cannabis behaviors and problems in the general population (e.g., Mills, Lintzeris, O’Malley, Arnold, & McGregor, 2022; Thompson, Leadbeater, Ames, & Merrin, 2019). While several sociodemographic and cannabis covariates differed among LGBT+ and non-LGBT+ respondents within the overall sample and at distinct age categories, there is a lack of existing data from national or matched studies to determine whether such differences are related to sampling biases or reflect true differences. Moreover, the observed effects of age, LGBT+ status, and sociodemographic and cannabis covariates ranged from small to medium, highlighting the need to explore additional characteristics that may influence probability of CUD-related problems.
Future studies might incorporate measures of minority stress, daily stress, resilience, and reactivity to enhance understanding of the reasons that cannabis-related problems may be elevated in LGBT+ samples, particularly among young adults. Minority stressors can contribute to worsened mental health outcomes, such as depression and anxiety among LGBT+ adults (Baams, Grossman, & Russell, 2015), which may impact the disparity in continued cannabis use despite emotional/physical problems. Further, use in larger amounts or over a longer period may reflect efforts to cope with negative mental health outcomes and/or minority stressors. Recent literature indicates that LGBT+ individuals may be more likely than non-LGBT+ counterparts to be motivated to use cannabis to cope with mental health symptoms (e.g., Schofield et al., 2023). Younger LGBT+ adults may benefit from treatments that seek to explore coping motives for use throughout the day (e.g., continued use to cope with stressors or chronic mental health conditions). Such an intervention might focus on building adaptive coping skills to counter use despite negative physical and/or emotional problems (London-Nadeau et al., 2021; Sherman & McRae-Clark, 2016). Further, interventions that reduce exposure to or impact of minority stressors and improve self-regulation may be particularly beneficial in reducing continued use throughout the day. Data on cannabis coping motives, self-regulation, and both physical and mental health correlates are needed to guide identification of these potential intervention targets.
There are several limitations of this initial study. CUD may be more likely and/or more severe among certain subgroups within the LGBT+ community including bisexual, female-at-birth, and gender diverse individuals (Schofield et al., 2023, Struble et al., 2022). Our study was limited in sample size of diverse LGBT+ identities, particularly at older ages which prevented examination of subgroup trends. Future recruitment strategies will also attempt to engage older LGBT+ respondents aged 65+ to examine extended age and subgroup-specific disparities in cannabis-related problems. Data were obtained from an online sample of regular cannabis consumers, limiting generalizability of the findings. The data are cross-sectional, limiting our understanding of longitudinal trends. The observed disparities across age groups may represent cohort (generational) disparities in cannabis use behaviors and resultant problems or true changes in CUD endorsement throughout the lifespan.
Conclusions
LGBT+ identity was associated with greater endorsement of two CUD criteria, use in larger amounts or over longer periods, and continued use despite physical/emotional problems. While age and LGBT+ identity did not interact, graphs show that disparities are most pronounced among young adults. Several sociodemographic and cannabis covariates may substantially impact endorsement of cannabis problems beyond LGBT+ identity. Employment, college attainment, and use for medical reasons all reduced likelihood of endorsement of CUD. Older LGBT+ adults demonstrated greater rates of these potential protective factors than younger LGBT+ respondents. These trends point to the continued need to understand LGBT+ health outcomes across the lifespan. Future survey iterations will collect data on potential confounds, such as mental and physical health correlates.
Supplementary Material
Highlights.
Sexual and gender minority (LGBT+) disparities in cannabis use and problems exist.
Few studies have examined differences in cannabis problems across the lifespan.
LGBT+ identity associated with CUD and endorsement of CUD Criteria 1 and 9.
No age*identity interactions emerged in adjusted models.
Being employed, college attainment, and medical use protected from problems.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Almeida DM, Rush J, Mogle J, Piazza JR, Cerino E, & Charles ST (2023). Longitudinal change in daily stress across 20 years of adulthood: Results from the national study of daily experiences. Developmental Psychology, 59(3), 515–523. 10.1037/dev0001469 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.American Psychiatric Association. (2022). Substance-related and addictive disorders. In Diagnostic and statistical manual of mental disorders (5th ed., text rev.). [Google Scholar]
- 3.Baams L, Grossman AH, & Russell ST (2015). Minority stress and mechanisms of risk for depression and suicidal ideation among lesbian, gay, and bisexual youth. Developmental psychology, 51(5), 688–696. 10.1037/a0038994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Boyd CJ, Veliz PT, & McCabe SE (2020). Severity of DSM-5 cannabis use disorders in a nationally representative sample of sexual minorities. Substance Abuse, 41(2), 191–195. 10.1080/08897077.2019.1621242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bränström R, & Pachankis JE (2018). Sexual orientation disparities in the co-occurrence of substance use and psychological distress: a national population-based study (2008-2015). Social Psychiatry and Psychiatric Epidemiology, 53(4), 403–412. 10.1007/s00127-018-1491-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Budney AJ, Borodovsky JT, Struble CA, Habib MI, Shmulewitz D, Livne O, Aharonovich E, Walsh C, Cuttler C, & Hasin DS (2022). Estimating THC consumption from smoked and vaped cannabis products in an online survey of adults who use cannabis. Cannabis and Cannabinoid Research, 10.1089/can.2022.0238. Advance online publication. 10.1089/can.2022.0238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dyar C. (2022) A review of disparities in cannabis use and cannabis use disorder affecting sexual and gender minority populations and evidence for contributing factors. Current Addiction Reports, 9, 589–597. 10.1007/s40429-022-00452-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dyar C, Sarno EL, Newcomb ME, & Whitton SW (2020). Longitudinal associations between minority stress, internalizing symptoms, and substance use among sexual and gender minority individuals assigned female at birth. Journal of Consulting and Clinical Psychology, 88(5), 389–401. 10.1037/ccp0000487 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Facebook. (2020). Facebook Ads manager: Ads management for Facebook. https://www.facebook.com/business/tools/ads-manager
- 10.Grant BF, Goldstein RB, Smith SM, Jung J, Zhang H, Chou SP, Pickering RP, Ruan WJ, Huang B, Saha TD, Aivadyan C, Greenstein E, & Hasin DS (2015). The Alcohol Use Disorder and Associated Disabilities Interview Schedule-5 (AUDADIS-5): reliability of substance use and psychiatric disorder modules in a general population sample. Drug and Alcohol Dependence, 148, 27–33. 10.1016/j.drugalcdep.2014.11.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hasin DS, Greenstein E, Aivadyan C, Stohl M, Aharonovich E, Saha T, Goldstein R, Nunes EV, Jung J, Zhang H, & Grant BF (2015). The Alcohol Use Disorder and Associated Disabilities Interview Schedule-5 (AUDADIS-5): Procedural validity of substance use disorders modules through clinical re-appraisal in a general population sample. Drug and Alcohol Dependence, 148, 40–46. 10.1016/j.drugalcdep.2014.12.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hasin DS, Shmulewitz D, & Sarvet AL (2019). Time trends in US cannabis use and cannabis use disorders overall and by sociodemographic subgroups: a narrative review and new findings. The American Journal of Drug and Alcohol Abuse, 45(6), 623–643. 10.1080/00952990.2019.1569668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jones JM (2022, February 17). LGBT identification in U.S. ticks up to 7.1%. GALLOP. Retrieved from https://news.gallup.com/poll/389792/lgbt-identification-ticks-up.aspx on 2023, March 15.
- 14.Koziara K, Mijas ME, Galbarczyk A, Wycisk J, Pliczko MP, Krzych-Miłkowska K, & Grabski B (2022). It gets better with age: Resilience, stigma, and mental health among lesbian, gay, bisexual, transgender and queer persons from Poland. Frontiers in Psychology, 13, 958601. 10.3389/fpsyg.2022.958601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Liautaud MM, Barrington-Trimis JL, Liu F, Stokes A, Krueger EA, McConnell R, & Pang RD (2021). E-cigarette, cigarette, and cannabis use patterns as a function of sexual identity in a sample of Southern California young adults. Addictive Behaviors Reports, 13, 100338. 10.1016/i.abrep.2021.100338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. 10.1037/0033-2909.129.5.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mills L, Lintzeris N, O’Malley M, Arnold JC, & McGregor IS (2022). Prevalence and correlates of cannabis use disorder among Australians using cannabis products to treat a medical condition. Drug and alcohol review, 41(5), 1095–1108. 10.1111/dar.13444 [DOI] [PubMed] [Google Scholar]
- 18.National Institute on Drug Abuse [NIDA]. 2022, August 22. Marijuana and hallucinogen use among young adults reached all time-high in 2021. Retrieved from https://nida.nih.gov/news-events/news-releases/2022/08/marijuana-and-hallucinogen-use-among-young-adults-reached-all-time-high-in-2021 on 2023, March 15.
- 19.Philbin MM, Mauro PM, Greene ER, & Martins SS (2019). State-level marijuana policies and marijuana use and marijuana use disorder among a nationally representative sample of adults in the United States, 2015-2017: Sexual identity and gender matter. Drug and Alcohol Dependence, 204, 107506. 10.1016/i.drugalcdep.2019.06.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Qualtrics. (2022). Qualtrics Survey Software. Provo, UT. [Google Scholar]
- 21.London-Nadeau K, Rioux C, Parent S, Vitaro F, Côté SM, Boivin M, Tremblay RE, Séguin JR, & Castellanos-Ryan N (2021). Longitudinal associations of cannabis, depression, and anxiety in heterosexual and LGB adolescents. Journal of Abnormal Psychology, 130(4), 333–345. 10.1037/abn0000542 [DOI] [PubMed] [Google Scholar]
- 22.Sherman BJ, & McRae-Clark AL (2016). Treatment of cannabis use disorder: Current science and future outlook. Pharmacotherapy, 36(5), 511–535. 10.1002/phar.1747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Schofield K, Cuttler C, Conner BT, Prince MA, & Addictions Research Team (ART) (2023). Pot at the end of the rainbow: Cannabis use among sexual minorities. Cannabis and Cannabinoid Research, 10.1089/can.2022.0240. Advance online publication. 10.1089/can.2022.0240. [DOI] [PubMed] [Google Scholar]
- 24.Schuler MS, Rice CE, Evans-Polce RJ, & Collins RL (2018). Disparities in substance use behaviors and disorders among adult sexual minorities by age, gender, and sexual identity. Drug and Alcohol Dependence, 189, 139–146. 10.1016/j.drugalcdep.2018.05.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schuler MS, Stein BD, & Collins RL (2019). Differences in substance use disparities across age groups in a national cross-sectional survey of lesbian, gay, and bisexual adults. LGBT Health, 6(2), 68–76. 10.1089/lgbt.2018.0125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Substance Abuse and Mental Health Services Administration. (2022). Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report [Google Scholar]
- 27.Struble CA, Borodovsky JT, Habib MI, Hasin DS, Shmulewitz D, Walsh C, Livne O, Aharonovich E, & Budney AJ (2022, July 22-24). Understanding differences in cannabis practices and cannabis-related outcomes among sexual and gender diverse young adults. In Struble CA (Chair), Leveraging digital technology to study cannabis use, benefits, and risks [Symposium]. 6th Annual Meeting for the Research Society on Marijuana (RSMj). Boston, MA, USA. [Google Scholar]
- 28.Thompson K, Leadbeater B, Ames M, & Merrin GJ (2019). Associations Between Marijuana Use Trajectories and Educational and Occupational Success in Young Adulthood. Prevention science : the official journal of the Society for Prevention Research, 20(2), 257–269. 10.1007/s11121-018-0904-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.