

Abstract
This report by the European Food Safety Authority and the European Centre for Disease Prevention and Control presents the results of the zoonoses monitoring and surveillance activities carried out in 2022 in 27 Member States (MSs), the United Kingdom (Northern Ireland) and 11 non‐MSs. Key statistics on zoonoses and zoonotic agents in humans, food, animals and feed are provided and interpreted historically. In 2022, the first and second most reported zoonoses in humans were campylobacteriosis and salmonellosis, respectively. The number of cases of campylobacteriosis and salmonellosis remained stable in comparison with 2021. Nineteen MSs and the United Kingdom (Northern Ireland) achieved all the established targets in poultry populations for the reduction of Salmonella prevalence for the relevant serovars. Salmonella samples from carcases of various animal species, and samples for Campylobacter quantification from broiler carcases, were more frequently positive when performed by the competent authorities than when own checks were conducted. Yersiniosis was the third most reported zoonosis in humans, followed by Shiga toxin‐producing Escherichia coli (STEC) and Listeria monocytogenes infections. L. monocytogenes and West Nile virus infections were the most severe zoonotic diseases, with the most hospitalisations and highest case fatality rates. In 2022, reporting showed an increase of more than 600% compared with 2021 in locally acquired cases of human West Nile virus infection, which is a mosquito‐borne disease. In the EU, the number of reported foodborne outbreaks and cases, hospitalisations and deaths was higher in 2022 than in 2021. The number of deaths from outbreaks was the highest ever reported in the EU in the last 10 years, mainly caused by L. monocytogenes and to a lesser degree by Salmonella. Salmonella and in particular S. Enteritidis remained the most frequently reported causative agent for foodborne outbreaks. Norovirus (and other calicivirus) was the agent associated with the highest number of outbreak human cases. This report also provides updates on brucellosis, Coxiella burnetii (Q fever), echinococcosis, rabies, toxoplasmosis, trichinellosis, infection with Mycobacterium tuberculosis complex (focusing on Mycobacterium bovis and Mycobacterium caprae) and tularaemia.
Keywords: Campylobacter, foodborne outbreaks, Listeria, monitoring, parasites, Salmonella, West Nile, zoonoses
Short abstract
This publication is linked to the following EFSA Journal article: https://efsa.onlinelibrary.wiley.com/doi/10.2903/j.efsa.2023.p211202
INTRODUCTION
Legal basis of European Union‐coordinated zoonoses monitoring
The European Union (EU) system for the monitoring and collection of information on zoonoses is based on Zoonoses Directive 2003/99/EC, 1 which obliges EU Member States (MSs) to collect relevant and, when applicable, comparable data on zoonoses, zoonotic agents, antimicrobial resistance and foodborne outbreaks. In addition, MSs shall assess the trends and sources of these agents, as well as outbreaks in their territory, submitting an annual report each year by the end of May to the European Commission (EC) covering the data collected. The EC should subsequently forward these reports to the European Food Safety Authority (EFSA). EFSA is assigned the tasks of examining these data and publishing the EU Annual Summary Reports. In 2004, the EC entrusted EFSA with setting up an electronic reporting system and database for monitoring zoonoses (EFSA Mandate No 2004‐0178, prolonged by M‐2015‐0231 2 ).
Data collection on human diseases from MSs is conducted in accordance with Decision 1082/2013/EU 3 on serious cross‐border threats to health. In October 2013, this Decision replaced Decision 2119/98/EC on setting up a network for the epidemiological surveillance and control of communicable diseases in the EU. The case definitions to be followed when reporting data on infectious diseases to the European Centre for Disease Prevention and Control (ECDC) are described in Decision 2018/945/EU. 4 ECDC has provided data on zoonotic infections in humans and their analysis for the EU Summary Reports since 2005. Since 2008, data on human cases have been received via The European Surveillance System (TESSy), maintained by ECDC.
Reporting requirements
In accordance with List A, Annex I of Zoonoses Directive 2003/99/EC, data on animals, food and feed must be reported for the following eight zoonotic agents: Salmonella, Campylobacter, L. monocytogenes, Shiga toxin‐producing Escherichia coli (STEC), Mycobacterium bovis, Brucella, Trichinella and Echinococcus. In addition, and based on the epidemiological situations in the MSs, data must be reported on the following agents and zoonoses (List B, Annex I of the Zoonoses Directive): (i) viral zoonoses: calicivirus, hepatitis A virus, influenza virus, rabies, viruses transmitted by arthropods; (ii) bacterial zoonoses: borreliosis and agents thereof, botulism and agents thereof, leptospirosis and agents thereof, psittacosis and agents thereof, tuberculosis due to agents other than M. bovis, vibriosis and agents thereof, yersiniosis and agents thereof; (iii) parasitic zoonoses: anisakiasis and agents thereof, cryptosporidiosis and agents thereof, cysticercosis and agents thereof, toxoplasmosis and agents thereof; and (iv) other zoonoses and zoonotic agents such as Francisella and Sarcocystis. Furthermore, MSs provided data on certain other microbiological contaminants in foods: histamine, staphylococcal enterotoxins and Cronobacter sakazakii, for which food safety criteria are set down in the EU legislation.
In accordance with Article 9 of the Directive, MSs shall assess the trends and sources of zoonoses, zoonotic agents and antimicrobial resistance in their territories and each MS shall send to the EC, every year by the end of May, a report on the trends in and sources of, zoonoses, zoonotic agents and antimicrobial resistance. Reports, and any summaries of them, shall be made publicly available.
Terms of Reference
In accordance with Article 9 of Directive 2003/99/EC, EFSA shall examine the national reports and data submitted by the EU MSs regarding their zoonoses monitoring activities as described above, and publish an EU Summary Report on the trends and sources of zoonoses, zoonotic agents and antimicrobial resistance in the EU. Since 2019, the annual EU Summary Reports on zoonoses, zoonotic agents and foodborne outbreaks have been renamed the ‘EU One Health Zoonoses Summary Report’ (EUOHZ), which is co‐authored by EFSA and ECDC. The 2022 MSs data on antimicrobial resistance in zoonotic agents are published in a separate EU Summary Report.
Data sources and report production
Since 2020, support for production of the annual EUOHZ report has been provided by the ZOE (Zoonoses under a One health perspective in the EU) Consortium's Work Package 1. The Consortium is composed of the Istituto Superiore di Sanità (Rome, Italy), the Istituto Zooprofilattico Sperimentale delle Venezie (Padova, Italy), the French Agency for Food, Environmental and Occupational Health & Safety (ANSES) (Maisons‐Alfort, France), the Istituto Zooprofilattico Sperimentale dell'Abruzzo e del Molise (Teramo, Italy) and the Istituto Zooprofilattico Sperimentale della Lombardia e dell'Emilia Romagna (Brescia, Italy), under the coordination of the Istituto Zooprofilattico Sperimentale dell'Abruzzo e del Molise (Teramo, Italy).
We gratefully acknowledge the efforts made by the MSs, the reporting non‐MSs and the EC for the reporting of zoonoses and foodborne outbreak data and in the preparation of this report.
The MSs, other reporting countries, the EC, members of EFSA's Scientific Panels on Biological Hazards (BIOHAZ) and Animal Health and Welfare (AHAW), and the relevant European Union Reference Laboratories (EURLs) were consulted while preparing the EUOHZ 2022 report.
This report focuses on the most relevant information on zoonoses, foodborne outbreaks and food microbiological safety criteria for the EU in 2022. Where substantial differences with regard to the previous years were observed, they have been reported.
On 1 February 2020, the United Kingdom withdrew from the EU and became a third country. 5 Data collection for the 2020 to 2022 period was therefore affected, since the number of EU MSs went from 28 to 27. In descriptive tables, data from the United Kingdom were included in the EU statistics for 2019 and previous years, whereas the 2020 statistical data from the United Kingdom, when available for EFSA data, were assigned to the non‐MS group. As of 2020, human data from the United Kingdom have not been collected by ECDC. With regard to trend analyses for human data, only countries having contributed data for all the years of the considered period were taken into account. For trend analyses of the estimated prevalence at EU level of Salmonella in poultry populations covered by National Control Programmes, any data provided by the reporting MSs were taken into account in the model. The United Kingdom data were only included when available for 2019 and previous years.
Since 2021, the only United Kingdom data reported to EFSA were from Northern Ireland. In accordance with the Agreement on the withdrawal of the United Kingdom from the European Union, and in particular with the Protocol on Ireland/Northern Ireland, the European Union requirements on data sampling are also applicable to and in the United Kingdom with respect to Northern Ireland. Therefore, for the purpose of this report, and pursuant to Article 5(4) and Section 24 of Annex 2 of the Protocol on Ireland/Northern Ireland, which is an integral part of the Agreement on the withdrawal of the United Kingdom of Great Britain and Northern Ireland from the European Union and the European Atomic Energy Community, references to MSs should be read as including Northern Ireland, despite it being part of the United Kingdom. Hence, the European Union requirements on data sampling were also applicable to Northern Ireland (XI 6 ) and data transmitted by the United Kingdom (Northern Ireland) have been assigned to the MSs group.
Human data collection for 2022
In the 2022 EUOHZ report, the analysis of data from human illnesses was prepared by the Food‐ and Waterborne Diseases and Zoonoses (FWD) domain (brucellosis, campylobacteriosis, congenital toxoplasmosis, echinococcosis, listeriosis, salmonellosis, Shiga toxin‐producing E. coli infection, trichinellosis and yersiniosis), the Emerging and Vector‐borne Diseases (EVD) domain (Q fever, rabies, tularaemia and West Nile virus (WNV) infection) and the tuberculosis (TB) domain (infection with Mycobacterium tuberculosis complex, focussing on M. bovis and M. caprae) at ECDC. TESSy is a software platform in which data on 56 diseases and special health issues are collected. Both aggregated and case‐based data are reported to TESSy by the MSs and other European countries. Although aggregated data did not include individual case‐based information, both reporting formats were included, when possible, to calculate the number of cases and country‐specific case notification rates. The human data used in this report were extracted from TESSy as of 25 July 2023 for EVD, as of 24 July 2023 for FWD and as of 29 September 2023 for TB due to M. bovis and M. caprae . The denominators used for calculating notification rates were based on the human population data from Eurostat on 1 January 2023.
The reporting of data to TESSy is underpinned by specific standard definitions applicable to both cases and surveillance systems in place in the MSs and in other European countries, 7 which are also used to summarise the data in this report. When interpreting statistics, data quality issues should be considered, as well as the differences between MS surveillance systems; comparisons between countries should therefore be undertaken with caution.
Data on human cases were received from the 27 MSs and from three non‐MSs (Iceland, Liechtenstein and Norway). Switzerland reported its data on human cases directly to EFSA. In 2021, Liechtenstein resumed the reporting of human data for the first time since 2008; prior to this, they reported this data together with Switzerland.
Information provided in the EUOHZ 2022 report can be integrated into the interactive ECDC Surveillance Atlas of Infectious Diseases even if small discrepancies are present.
Data collection on food, animals, feed and foodborne outbreaks
For the year 2022, the 27 MSs and the United Kingdom (Northern Ireland) submitted data and national zoonoses reports on monitoring results in food, animals, feed and foodborne outbreaks. In addition, data and reports were submitted by four non‐MSs which are also the four European Free Trade Association (EFTA) countries: Iceland, Norway, Switzerland and Liechtenstein. 8 For some food, animal and feed matrices, and for foodborne outbreaks, EFSA received data and reports from the following pre‐accession countries: Albania, Bosnia and Herzegovina, Kosovo, 9 Republic of North Macedonia, Montenegro and Serbia.
Data were submitted electronically to the EFSA zoonoses database, through EFSA's Data Collection Framework (DCF). MSs could also update their data from previous years.
The deadline for data submission was 31 May 2022. Two data validation procedures were carried out, from 1 June to 12 June 2023 and from 28 June to 7 July 2023, respectively. Validated data on food, animals, feed and foodborne outbreaks used in the report were extracted from the EFSA zoonoses database on 21 July 2023.
A detailed description of the terms used in the report is available in EFSA's manuals for reporting on zoonoses (EFSA, Amore, Boelaert, et al., 2023; EFSA, Amore, Beloeil, et al., 2023).
The national zoonoses reports submitted in accordance with Directive 2003/99/EC are published on the EFSA website together with the EU One Health Zoonoses Report. They are available online here.
To provide an overview of all the information reported by the MSs for the production of the EUOHZ 2022 report and to limit its volume, the following interactive communication tools were created: EFSA story maps and dashboards for foodborne outbreaks (FBOs), Campylobacter, Salmonella, Listeria monocytogenes, Shiga toxin‐producing E. coli, Brucella and zoonotic tuberculosis (focussing on M. bovis and M. caprae). The EFSA story maps provide general information on each zoonosis and its epidemiology, including information on characteristics of the zoonotic agent, how people and animals get infected, the occurrence of the pathogen in different sources, the disease it causes and how to prevent infection. In addition, the story maps also illustrate the monitoring activities implemented in the EU and the role of EFSA with respect to these activities. The EFSA story maps include dynamic maps, images, text and multimedia features. The EFSA dashboards on specific zoonoses are graphical user interfaces for searching and querying the large amount of data collected each year by EFSA from the MSs and other reporting countries based on Zoonoses Directive 2003/99/EC. The EFSA dashboards show summary statistics for the monitoring results for the pathogen with regard to major food and animal categories. In the EFSA dashboards, data and related statistics can be displayed interactively through charts, graphs and maps using the online format. Moreover, the main statistics can also be viewed and downloaded in tabular format. Detailed information on the use and features of the dashboards can be found in the user guides that can be downloaded from the online tools. Links to the EFSA story maps and dashboards are available in the relevant sections of each chapter. Some discrepancies between the data and statistics reported in the present report and those shown in the story maps and dashboards may occur. The reason for this is that the data underpinning the report were updated on 21 July 2023, whereas those visualised in the story maps and dashboards were updated on 1 December 2023.
Finalisation of the EUOHZ 2022 report
The draft EUOHZ 2022 report was sent to the MSs for consultation on 9 October 2023 and comments were collected by 24 October 2023. The utmost effort was made to incorporate comments within the available time frame. In general, data amended after the data validation period that ended on 21 July 2023 have not been considered in the summary calculations or other analyses, and footnotes to tables and figures have been added to account for these late data corrections. The report was finalised on 10 November 2023 and published online by EFSA and ECDC on 12 December 2023.
Data analysis and presentation
Data comparability and quality
Humans
For data on human infections, please note that the numbers presented in this report may differ from those found in the national zoonoses reports due to differences in the case definitions used at the EU and national levels or because of differing dates of data submission and extraction. The latter may also result in some divergence in the case numbers and notification rates presented in the different ECDC reports and the reports produced in previous years. Results are not directly comparable among the MSs or between different years. Data collection on human cases of foodborne diseases reported to ECDC through TESSy and to EFSA within the European Union Foodborne Reporting System (EU‐FORS, see chapter on Foodborne Oubreaks, Section 2) is separate and independent. Comparability between the two systems is limited by the different context and purposes of cases reporting and is also limited by the adoption of different case definitions.
Food, animals, feed and foodborne outbreaks
Comparability of data obtained by the EFSA DCF can vary depending on the levels of data quality and harmonisation. The types of data analysis suggested by EFSA for each zoonosis and matrix (food, animals, feed or foodborne outbreaks) strongly depended on this level of harmonisation and can either be a descriptive summary of submitted data, the following‐up of trends (trend watching) or the (quantitative) analyses of trends. Data analyses were carried out in accordance with quality criteria described in Table 1 as adapted from Boelaert et al., 2016. Food, animals, feed and foodborne outbreak data can be classified into three categories depending on the zoonotic agent monitored and the design of the monitoring or surveillance carried out. It follows that the type of data analyses that can be implemented is conditioned by these three distinct categories.
TABLE 1.
Categorisation of the data used in the EU One Health Zoonoses 2022 Summary Report (adapted from Boelaert et al. (2016)).
Rationale of the table of contents
Taking account of the zoonoses listing in Annex I of Directive 2003/99/EC, of the mandatory reporting of foodborne outbreaks and of the above‐mentioned categorisation of food, animal and feed data (Table 1), the following table of contents has been adopted for the 2022 EUOHZ report.
Zoonoses and zoonotic agents included in compulsory annual monitoring (Directive 2003/99/EC List A).
Campylobacter
Salmonella
Listeria
Shiga toxin‐producing Escherichia coli
Infection with Mycobacterium tuberculosis complex, focussing on M. bovis and M. caprae
Brucella
Trichinella
Echinococcus
Foodborne and waterborne outbreaks (in accordance with Directive 2003/99/EC)
Zoonoses and zoonotic agents monitored depending on the epidemiological situation (Directive 2003/99/EC List B).
Yersinia
Toxoplasma gondii
Rabies
Q fever
West Nile virus
Tularaemia
Other zoonoses and zoonotic agents
Microbiological contaminants subject to food safety criteria (Regulation (EC) No 2073/2005).
Chapter sections
The 2022 EUOHZ Report presents a harmonised structure for each chapter:
‘Key facts’,
‘Monitoring and surveillance' in the EU for the specific disease,
‘Results’, summarising the major findings of 2022 as regards trends and sources, starting with a table displaying summary statistics for the last 5 years (2018–2022) for human cases, food matrices and major animal species, and followed by specific sections describing the main results in humans, food and/or animals. References to statistics displayed in the EFSA dashboards are included in some sections of specific chapters, when available.
A ‘Discussion’ section. For foodborne and waterborne outbreaks, the main findings are presented and discussed in a joint ‘Results and discussion’ section and key messages are summarised in the ‘Conclusions’ section.
For each chapter, overview tables present the data reported by each country. However, unless stated otherwise, the tables summarising MS‐specific results and providing EU‐level results for food, animals and feed, exclude data from industry own‐check programmes, hazard analysis and critical control point (HACCP) sampling, as well as data from suspect sampling, selective sampling and outbreak or clinical investigations. Moreover, regional data reported by countries for food, animals and feed without statistics at the national level, were also excluded from these tables.
Data analyses
Statistical trend analyses for humans were carried out to evaluate the significance of temporal variations in the EU over the 2018–2022 period. Further details can be found in the individual chapters. The number of confirmed cases for the EU by month is presented as a trend figure for the 2013–2022 period. All countries that consistently reported cases – or reported zero cases over the whole reporting period – were included. The trend figure also shows a centred 12‐month moving average over the last 5 years, illustrating the overall trend by smoothing seasonal and random variations. Moreover, the same trend analysis was carried out separately for each country (MS and non‐MS countries). Analyses were carried out considering confirmed cases only, except for WNV infection, for which all locally acquired cases (i.e. probable and confirmed cases) were considered. Statistical methods for trend analysis were based on either the regression analysis or nonparametric test (Cox‐Stuart test), where appropriate. The time trend was considered statistically significant with p‐value < 0.01 (p < 0.05 for nonparametric test).
The notification rates were calculated taking into account the coverage of the human population under surveillance (percentage of national coverage). For countries where surveillance did not cover the whole population, the estimated coverage – if provided – was used to calculate the country‐specific rate. Cases and populations of those countries not providing information on national coverage or reporting incomplete data were excluded from the EU notification rate.
ESRI ArcMap 10.8.2 was used to map the data. Choropleth maps with graduated colours over five class scales of values using the natural breaks function proposed by the ArcGIS software, were produced to map the proportion of positive sampling units across the EU and other reporting countries. In the maps included in this report, EU MSs and the United Kingdom (Northern Ireland) were represented with a blue label, whereas all the non‐EU MSs (including the EFTA countries: Iceland, Norway, Switzerland and Liechtenstein; and the pre‐accession countries: Albania, Bosnia and Herzegovina, Kosovo, 10 Republic of North Macedonia, Montenegro and Serbia) were represented with an orange label.
Statistical trend analysis of foodborne outbreaks was performed to evaluate the significance of temporal variations at the single MS level over the 2013–2022 period.
Summary data and the figures for food, animals, feed and foodborne outbreaks used to produce this report, as well as additional information on related projects and internet sources, are published on the EFSA Knowledge Junction on the Zenodo general‐purpose open‐access repository here. All country‐specific data on food, animals, feed and foodborne outbreaks, updated through 30 November 2023, are also available at this URL.
Along with this report, EFSA has also published the following interactive communication tools:
the EFSA story maps on Campylobacter (here), Salmonella (here), L. monocytogenes (here), Shiga toxin‐producing E. coli (here), M. tuberculosis complex, focussing on M. bovis and M. caprae (here), Brucella (here) and foodborne outbreaks (here).
the EFSA dashboards on Campylobacter (here), Salmonella (here), L. monocytogenes (here), Shiga toxin‐producing E. coli (here), zoonotic tuberculosis or tuberculosis due to M. tuberculosis complex (here), Brucella (here) and foodborne outbreaks (here).
Data used in these communication tools were extracted from the EFSA zoonoses database on 1 December 2023.
Summary of human zoonoses data for 2022
The numbers of confirmed human cases of the zoonoses presented in this report are summarised in Table 2. In 2022, campylobacteriosis was confirmed as the most commonly reported zoonosis (as it has been since 2005). It accounted for 61.3% of all the reported and confirmed human cases in 2022. After campylobacteriosis, salmonellosis, yersiniosis, STEC infections and listeriosis were the most frequently reported zoonoses. The severity of the diseases was descriptively analysed based on hospitalisations and the outcomes of reported cases. Based on severity data, listeriosis and West Nile virus infection were the two most severe diseases, with the highest case fatality and hospitalisation rates among reported cases. For these two diseases, almost all cases with available hospitalisation data were hospitalised (96.0% of confirmed cases for listeriosis and 86.9% of locally acquired probable and confirmed cases for West Nile virus infection, respectively). The highest number of deaths was associated with listeriosis (N = 286), followed by West Nile virus infection (N = 92) and salmonellosis (N = 81). Listeriosis and West Nile virus infection were also the zoonoses with the highest fatality rate, 18.1% and 8.3%, respectively.
TABLE 2.
Reported hospitalisations and deaths due to zoonoses in confirmed human cases and among foodborne outbreak cases in the EU, 2022.
| Disease | Surveillance data on human cases (source: ECDC) | Foodborne outbreaks (source: EFSA) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Confirmed human cases | Hospitalisations | Deaths | Outbreaks | Cases | Hospitalisations and proportion of hospitalised cases | Deaths and case fatality | |||||||||||
| Status available | Reporting MSs a | Cases and proportion of hospitalised cases | Outcome available | Reporting MSs a | Deaths and Case fatality | ||||||||||||
| N | N | % | N | N | % | N | % | N | N | % | N | N | N | % | N | % | |
| Campylobacteriosis | 137,107 | 44,876 | 327 | 16 | 10,551 | 23.5 | 84,425 | 61.6 | 17 | 34 | 0.04 | 255 | 1097 | 83 | 7.6 | 0 | 0 |
| Salmonellosis | 65,208 | 29,003 | 44.5 | 17 | 11,287 | 38.9 | 36,856 | 56.5 | 17 | 81 | 0.22 | 1014 | 6632 | 1406 | 21.2 | 8 | 0.12 |
| Yersiniosis | 7919 | 2113 | 26.7 | 17 | 636 | 30.1 | 3765 | 47.5 | 17 | 0 | 0 | 14 | 96 | 4 | 4.2 | 0 | 0 |
| STEC infections | 7117 | 2933 | 41.2 | 17 | 1130 | 38.5 | 4824 | 67.8 | 21 | 28 | 0.58 | 71 | 408 | 63 | 15.4 | 1 | 0.25 |
| Listeriosis | 2738 | 1386 | 50.6 | 19 | 1330 | 96.0 | 1578 | 57.6 | 21 | 286 | 18.1 | 35 | 296 | 242 | 81.8 | 28 | 9.5 |
| West Nile virus infection b | 1111 | 366 | 32.9 | 8 | 318 | 86.9 | 1111 | 100.0 | 11 | 92 | 8.3 | NA | NA | NA | NA | NA | NA |
| Echinococcosis | 722 | 277 | 38.4 | 15 | 128 | 46.2 | 405 | 56.1 | 15 | 1 | 0.25 | 0 | 0 | 0 | – | 0 | – |
| Q fever | 719 | NA | NA | NA | NA | NA | 445 | 61.9 | 14 | 4 | 0.90 | 0 | 0 | 0 | – | 0 | – |
| Tularaemia | 620 | 151 | 24.4 | 10 | 91 | 60.3 | 227 | 36.6 | 11 | 2 | 0.88 | 0 | 0 | 0 | – | 0 | – |
| Brucellosis | 198 | 79 | 39.9 | 10 | 55 | 69.6 | 81 | 40.9 | 10 | 0 | 0 | 0 | 0 | 0 | – | 0 | – |
| Tuberculosis caused by M. bovis, M. caprae | 130 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Trichinellosis c | 41 | 11 | 26.8 | 5 | 7 | 63.6 | 11 | 26.8 | 5 | 0 | 0 | 7 | 68 | 10 | 14.7 | 0 | 0 |
| Rabies | 0 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
Abbreviation: NA, Not applicable, as information is not collected for this disease.
Note: Data on congenital toxoplasmosis are not shown, since 2022 data are not available yet.
Not all countries provided case data for all diseases.
For West Nile virus infection, the total number of locally acquired infection cases was used (includes probable and confirmed cases).
The number of cases also includes two cases reported from Finland, by error.
With regard to FBOs, Salmonella accounted for the highest number of outbreaks and cases, followed by ‘bacterial toxins, unspecified’ and ‘noroviruses and other caliciviruses’ (statistics not displayed in Table 2). The number of foodborne outbreaks increased by 43.9% in 2022 compared with 2021. Moreover, the number of human cases, hospitalisations and reported deaths associated with FBOs also increased by 49.4%, 11.5% and 106.5%, respectively.
Comparison of human zoonoses data for 2021 and 2022
In order to estimate the trends in human infections over the last 2 years, the 2022 data (number of cases and notification rates) were compared with those from 2021 (absolute and relative difference) (Table 3). Relative differences in notification rates have been calculated using exact numbers.
TABLE 3.
Number of confirmed human cases and notification rates (per 100,000 population) in 2022, including the absolute and relative (%) difference with regard to 2021, by zoonosis, EU.
| Zoonosis | Cases (N) | Notification rates (confirmed cases per 100,000 population) | |||
|---|---|---|---|---|---|
| 2022 | 2021 Absolute difference | 2022 | 2021 | ||
| Absolute difference | Relative difference (%) | ||||
| Campylobacteriosis | 137,107 | −210 | 43.1 | < 0.01 | < 0.01 |
| Salmonellosis | 65,208 | 5039 | 15.3 | < 0.01 | < 0.01 |
| Yersiniosis | 7919 | 910 | 2.2 | +0.30 | +16.3 |
| STEC infections | 7117 | 711 | 2.1 | +0.17 | +8.8 |
| Listeriosis | 2738 | 373 | 0.62 | +0.08 | +15.9 |
| West Nile virus infection a | 1111 | 959 | 0.25 | +0.22 | +631.8 |
| Echinococcosis | 722 | 133 | 0.19 | +0.02 | +13.8 |
| Q fever | 719 | 259 | 0.17 | +0.06 | +56.5 |
| Tularaemia | 620 | −261 | 0.14 | −0.06 | −29.5 |
| Brucellosis | 198 | 36 | 0.04 | +0.01 | +29.2 |
| Tuberculosis caused by M. bovis, M. caprae | 130 | 15 | 0.03 | < 0.01 | +13.2 |
| Trichinellosis b | 41 | −38 | 0.01 | −0.01 | −51.9 |
| Rabies | 0 | 0 | 0 | 0 | – |
For West Nile virus infection, the total number of locally acquired infection cases was used (includes probable and confirmed cases).
The number of cases or the number of confirmed cases per 100,000 population also includes two cases reported from Finland, by error.
For the zoonoses causing the highest number of cases (salmonellosis and campylobacteriosis), the notification rates were stable over the last 2 years. For all other zoonoses except trichinellosis (−51.9%) and tularaemia (−29.5%), there was an increase in the notification rates in 2022 compared to 2021. The rate of locally acquired West Nile virus infection increased markedly in 2022 as compared with 2021 (+631.8%) due to an epidemic outbreak mainly involving Italy and Greece. A smaller increase was seen for Q fever (+56.5%), brucellosis (+29.2%), yersiniosis (+16.3%), listeriosis (+15.9%), echinococcosis (+13.8%), tuberculosis caused by M. bovis, M. caprae (+13.2%) and STEC infection (+8.8%) rates.
ZOONOSES AND ZOONOTIC AGENTS INCLUDED IN COMPULSORY ANNUAL MONITORING (DIRECTIVE 2003/99/EC LIST A)
1. CAMPYLOBACTER
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here, and are also retrievable from the EFSA Campylobacter dashboard available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
1.1. Key facts
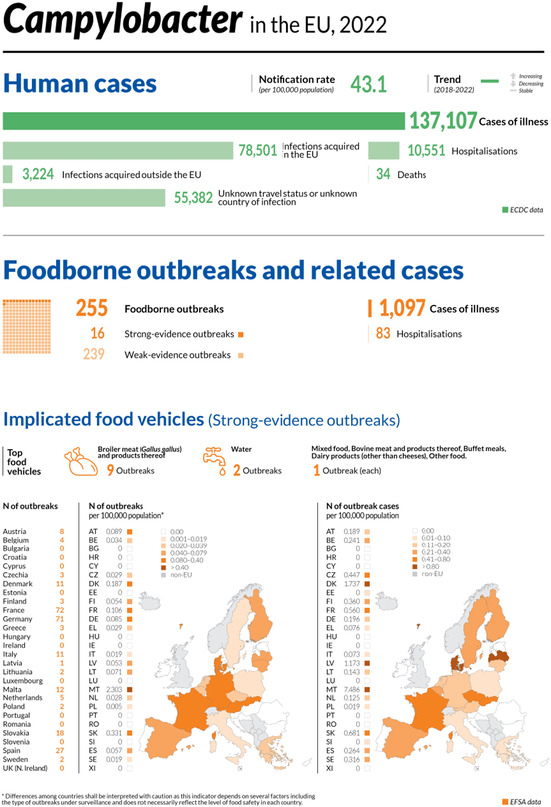
Campylobacteriosis was the most commonly reported foodborne gastrointestinal infection in humans in the European Union .
In 2022, there were 137,107 confirmed cases of human campylobacteriosis, corresponding to an European Union notification rate of 43.1 cases per 100,000 population. The notification rate was stable compared with 2021.
The overall trend for Campylobacter infections showed no significant increase or decrease over the 2018–2022 period.
Twenty‐four Member States and the United Kingdom (Northern Ireland) reported data for 2022 in the context of the Campylobacter process hygiene criterion, set out in Regulation (EC) No 2073/2005. 11 Sixteen Member States and the United Kingdom (Northern Ireland) reported 7905 test results from official controls, with 38.3% Campylobacter‐positive samples and 19.4% exceeding the limit of 1000 CFU/g. Twenty Member States reported 58,372 test results from the monitoring of food business operators, with 39% positive samples and 17.5% exceeding the limit of 1000 CFU/g. Twelve Member States reported results from both samplers, showing that the number of samples exceeding the limit was significantly higher in official samples (22.1%) than in own checks (9%).
In 2022, 0.11% of 2774 ‘ready‐to‐eat’ food sampling units reported by 11 Member States were positive for Campylobacter, with positive samples originating from ‘minced meat from other poultry species intended to be eaten raw’ and from oysters. Of 25,601 ‘non‐ready‐to‐eat’ sampling units reported by 16 Member States, 11.1% were positive, with the highest level of contamination (11.6%) in ‘meat and meat products’. Campylobacter was isolated from all fresh meat categories, with meat from broilers and turkeys showing the highest percentages of contamination, 12% and 11.2%, respectively.
Campylobacter spp. was detected by 14 Member States and the United Kingdom (Northern Ireland) and three non‐Member States in more than 40 different animal categories in 2022. About 40% of units tested in the European Union were from broilers (N = 9035) and the proportion of positives was 18.1%. The proportion of positive sampling units for turkeys, cats and dogs, bovine animals, small ruminants and pigs were 71.9% 12.5%, 6.4%, 2.2% and 1.8%, respectively.
1.2. Surveillance and monitoring of Campylobacter in the EU
1.2.1. Humans
In 2022, all 27 EU MSs reported information on campylobacteriosis in humans. Surveillance of campylobacteriosis is mandatory in 23 EU MSs. In four MSs (Belgium, France, Italy and the Netherlands), notification is based on a voluntary system. The EU case definition was used by 23 MSs. Three MSs used a different case definition for reporting (France, Germany and Italy), and the Netherlands did not specify which case definition it used. All MSs except three (Belgium, Italy and the Netherlands), had a comprehensive surveillance system.
The campylobacteriosis surveillance systems cover the whole population in all MSs except four (France, Italy, the Netherlands and Spain). The estimated coverage of the surveillance system was 20% in France, 64% in the Netherlands and 73% in Spain. These estimated proportions of population coverage were used in the calculation of notification rates for these three MSs. No estimated population coverage was provided for 2018–2020 in Spain, so notification rates were not calculated. No estimate of population coverage in Italy was provided for any year, so no notification rate was calculated for this MS. All countries reported case‐based data except Belgium and Bulgaria, which reported aggregated data.
1.2.2. Food and animals
Campylobacter is monitored along the food chain during the primary production stage (farm animals), during harvest/slaughter, manufacturing and at the distribution stage.
Campylobacter data in the context of Regulation (EC) No 2073/2005
A regulatory limit (microbiological process hygiene criterion (PHC)) of 1000 CFU/g of Campylobacter on the neck skins of chilled broiler carcases was set by Regulation (EC) No 2073/2005 (point 2.1.9 of Chapter 2 of Annex I). This limit applies to a set of 50 pooled samples from 10 consecutive sampling sessions. As of 2022, a maximum number of 15 samples with values exceeding this limit are considered as acceptable. Food business operators (FBOp) failing to comply with this limit are required to carry out corrective actions involving validation and verification of their food safety management procedures based on Hazard Analysis and Critical Control Point (HACCP) principles and Good Manufacturing Practices (GMP). The PHC has been in force since 1 January 2018. On 14 December 2019, Commission Implementing Regulation (EU) 2019/627 12 came into force, harmonising sampling procedures for official controls. This legislation requires the Competent Authority (CA) to verify whether the FBOp is correctly implementing and checking the PHC on broiler carcases by choosing one of two approaches: implementing ad hoc official sampling 13 or collecting all the information from the samples taken by the FBOp. The results obtained in official controls enable improved trend watching and trend analyses (Table 1).
Other monitoring data for food and animals
Campylobacter monitoring data from food and animals submitted to EFSA in compliance with Chapter II ‘Monitoring of zoonoses and zoonotic agents’ of the Zoonoses Directive 2003/99/EC 14 are collected without a harmonised procedure. These data allow descriptive summaries at EU level, but they do not support EU‐level trend analyses and trend watching (Table 1).
In 2022, general data on food and animals reported to EFSA by MSs and non‐MSs were obtained mainly from official sampling, industry sampling HACCP and own checks, as part of national monitoring and surveillance, and/or organised surveys. In addition, for animal data, other reported samples were obtained from clinical investigations by private veterinarians and industry (e.g. artificial insemination centres).
The occurrence of Campylobacter reported in the main food categories for the year 2022 and for the 4‐year period of 2018–2021 was descriptively summarised, making a distinction between ‘ready‐to‐eat’ (RTE) and non‐RTE food. Data sets were extracted using the ‘objective sampling’ strategy, meaning that the reporting MSs collected the sampling units as part of a planned strategy based on the selection of random sampling units that are statistically representative of the population to be analysed.
Other Campylobacter monitoring data, intended solely for monitoring antimicrobial resistance, are obtained from selected animal species and their carcases/meat, using the harmonised sampling scheme set out in the Commission Implementing Decision (EU) 2020/1729. 15 These antimicrobial resistance results are published in a separate EU Summary Report.
The detection and confirmation of Campylobacter in food and animals is generally based on culture, with the use of international standards or equivalent validated methods. Species identification is carried out using biochemical and molecular methods (PCR‐based), as well as matrix‐assisted laser desorption/ionisation–time‐of flight mass spectrometry (MALDI–TOF MS).
EFSA story map on Campylobacter
General information on Campylobacter and its epidemiology, including information on where the pathogen can be found, how people and animals get infected, the occurrence of this pathogen in different sources, the disease it causes and how to prevent infection, is provided in the EFSA story map on Campylobacter (available here). In addition, this story map also illustrates the monitoring activities implemented in the EU and the role of EFSA with respect to these activities.
1.3. Data analyses
A comparison was made of Campylobacter results exceeding 1000 CFU/g from the neck skins of broiler carcases after chilling, as obtained by the CA and FBOp as part of the Campylobacter PHC in compliance with Regulation (EC) No 2073/2005. The significance of any differences was verified by the one‐tailed Fisher's exact probability test in cases where the expected values of any of the cells in a contingency table were below 5; otherwise, the one‐tailed z test was used. The official control sampling results by the CA and the own‐check results by the FBOp were expressed as prevalence ratios with an exact binomial confidence interval of 95%. A p‐value of < 0.10 (Clayton & Hills, 2013) was considered as significant, in order to highlight every possible indication of differences between the data collected by the FBOp and the CA. R software (www.r‐project.org, version 4.2.3) was used to conduct the above analyses.
EFSA dashboard on Campylobacter
Summary statistics for the monitoring results for Campylobacter with regard to major food categories and animal species, Campylobacter‐positive official samples exceeding the PHC limit of 1000 CFU/g for chilled broiler carcases, and the occurrence of Campylobacter in major food categories are displayed, retrievable and downloadable in the EFSA dashboard on Campylobacter (available here).
1.4. Results
1.4.1. Overview of key statistics, EU, 2018–2022
Table 4 summarises EU statistics on human campylobacteriosis, and on the occurrence and prevalence of Campylobacter in food and animals respectively, during the period 2018–2022. In 2022, a similar number of notified human cases were observed as in 2021, so the EU notification rate was unchanged. The food data of interest in this report were classified into two major categories: ‘meat and meat products’ and ‘milk and milk products’, aggregated by year to obtain an annual overview of the volume of data submitted. Since 2019, the number of sampling units reported for ‘meat and meat products’ has increased sharply, probably owing to the Commission Implementing Regulation (EU) 2019/627 establishing compulsory reporting of Campylobacter PHC monitoring data (see above). The animal data collected at the primary production stage were mostly from broilers, cattle and pigs. Results showed comparable and consistent test numbers over the considered period for cattle and pigs, alongside a decreasing trend in the reported sample sizes for broilers. More detailed descriptions of these statistics are provided in the subsections below and in the chapter on foodborne outbreaks.
TABLE 4.
Summary of Campylobacter statistics relating to humans, major food categories and the main animal species, EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 137,107 | 137,317 | 120,543 | 220,639 | 246,570 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 43.1 | 43.1 | 40.2 | 60.6 | 66.0 | ECDC |
| Number of reporting MSs | 27 | 27 | 27 | 28 | 28 | ECDC |
| Infection acquired in the EU | 78,501 | 81,975 | 70,769 | 109,937 | 116,246 | ECDC |
| Infection acquired outside the EU | 3224 | 704 | 1586 | 6514 | 7685 | ECDC |
| Unknown travel status or unknown country of infection | 55,382 | 54,638 | 48,188 | 104,188 | 122,639 | ECDC |
| Number of foodborne outbreak‐related cases | 1097 | 1051 | 1319 | 1770 | 2365 | EFSA |
| Total number of foodborne outbreaks | 255 | 249 | 317 | 542 | 537 | EFSA |
| Food c | ||||||
| Meat and meat products d | ||||||
| Number of sampling units | 107,162 | 87,808 | 66,099 | 57,027 | 26,514 | EFSA |
| Number of reporting MSs | 27 | 25 | 25 | 25 | 26 | EFSA |
| Milk and milk products e | ||||||
| Number of sampling units | 2633 | 2125 | 2145 | 2749 | 3227 | EFSA |
| Number of reporting MSs | 14 | 11 | 11 | 11 | 13 | EFSA |
| Animals f | ||||||
| Cattle (bovine animals) | ||||||
| Number of sampling units | 5698 | 7529 | 4387 | 6850 | 4220 | EFSA |
| Number of reporting MSs | 7 | 11 | 7 | 10 | 8 | EFSA |
| Gallus gallus (chickens) | ||||||
| Number of sampling units | 9389 | 10,162 | 13,628 | 10,472 | 14,093 | EFSA |
| Number of reporting MSs | 13 | 6 | 15 | 8 | 16 | EFSA |
| Pigs | ||||||
| Number of sampling units | 1820 | 4502 | 2110 | 4308 | 2481 | EFSA |
| Number of reporting MSs | 5 | 14 | 4 | 11 | 5 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
For the 2021–2022 period, data on food and animal samples from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020, it became a third country.
The number of sampling units was obtained by totalling all sampling units (single, batch, slaughter batch), sampling stages (processing plant, automatic distribution system for raw milk, border control posts, canteen or workplace catering, catering, cold storage, cutting plant, distribution: wholesale and retail sale, farm, game handling establishment, hospital or medical care facility, household, manufacturing, mobile retailer or market/street vendor, packing centre, primary production, restaurant or cafe or pub or bar or hotel or catering service, retail, school or kindergarten, slaughterhouse, storage, takeaway or fast‐food outlet, unspecified and wholesale), sampling strategies (census, convenience sampling, selective sampling, objective sampling and unspecified) and samplers (official sampling, HACCP and own‐check, industry sampling, official and based on regulation 2019/627).
‘Meat and meat products’ refer to carcases and fresh meat/ready‐to‐eat (RTE), cooked and fermented products.
‘Milk and milk products’ refer to raw and pasteurised milk and all dairy products including cheeses.
The number of sampling units was obtained by totalling all sampling units (single animals, slaughter animal batches, holdings and herds or flocks), sampling stages at primary production (natural habitat, conservation facilities, farm, household, slaughterhouse, unspecified, veterinary activities, veterinary clinics, zoo) except artificial insemination station, sampling strategies (objective sampling, census, convenience sampling, selective sampling and suspect sampling) and samplers (HACCP and own‐check, industry sampling, official sampling and private sampling).
For a further interactive look at Campylobacter monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
1.4.2. Human campylobacteriosis
In 2022, 137,107 confirmed cases of human campylobacteriosis were reported by the 27 EU MSs, corresponding to an EU notification rate of 43.1 cases per 100,000 population (Table 4). This notification rate remained unchanged compared with 2021. Bulgaria, Czechia, Germany, Hungary, Malta, Poland, Portugal and Slovakia reported lower rates in 2022 than in the previous year. The highest country‐specific notification rates in 2022 were observed in Luxembourg (141.3 cases per 100,000), Czechia (137.0), Slovakia (87.9) and Denmark (87.6). The lowest rates in 2022 were observed in Poland, Bulgaria, Romania and Greece (≤ 2.9 per 100,000) (Table 5).
TABLE 5.
Reported confirmed human cases of campylobacteriosis and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National Coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 6294 | 70.1 | 6019 | 67.4 | 5406 | 60.7 | 6572 | 74.2 | 7999 | 90.7 |
| Belgium | Y | A | 5255 | 45.2 | 3273 | 28.3 | 5693 | 49.4 | 7337 | 64.0 | 8086 | 70.9 |
| Bulgaria | Y | A | 107 | 1.6 | 130 | 1.9 | 127 | 1.8 | 229 | 3.3 | 191 | 2.7 |
| Croatia | Y | C | 1467 | 38.0 | 1148 | 28.4 | 1054 | 26.0 | 1722 | 42.2 | 1965 | 47.9 |
| Cyprus | Y | C | 82 | 9.1 | 24 | 2.7 | 18 | 2.0 | 21 | 2.4 | 26 | 3.0 |
| Czechia | Y | C | 14,412 | 137.0 | 16,305 | 152.4 | 17,517 | 163.8 | 22,894 | 215.0 | 22,895 | 215.8 |
| Denmark | Y | C | 5143 | 87.6 | 3740 | 64.0 | 3742 | 64.3 | 5402 | 93.0 | 4559 | 78.9 |
| Estonia | Y | C | 211 | 15.8 | 185 | 13.9 | 265 | 19.9 | 347 | 26.2 | 411 | 31.2 |
| Finland | Y | C | 2462 | 44.4 | 1798 | 32.5 | 2074 | 37.5 | 4382 | 79.4 | 5099 | 92.5 |
| France b | N | C | 9095 | 67.0 | 8875 | 65.6 | 7920 | 58.8 | 7712 | 57.4 | 7491 | 55.9 |
| Germany | Y | C | 43,471 | 52.2 | 47,911 | 57.6 | 46,377 | 55.8 | 61,277 | 73.8 | 67,585 | 81.6 |
| Greece | Y | C | 302 | 2.9 | 260 | 2.4 | 218 | 2.0 | 366 | 3.4 | 357 | 3.3 |
| Hungary | Y | C | 5050 | 52.1 | 5088 | 52.3 | 4461 | 45.7 | 6400 | 65.5 | 7117 | 72.8 |
| Ireland | Y | C | 3617 | 71.5 | 3147 | 62.9 | 2419 | 48.7 | 2776 | 56.6 | 3044 | 63.0 |
| Italy c | N | C | 1539 | – | 1541 | – | 1418 | – | 1633 | – | 1356 | – |
| Latvia | Y | C | 172 | 9.2 | 158 | 8.3 | 104 | 5.5 | 133 | 6.9 | 87 | 4.5 |
| Lithuania | Y | C | 497 | 17.7 | 357 | 12.8 | 684 | 24.5 | 1221 | 43.7 | 919 | 32.7 |
| Luxembourg | Y | C | 912 | 141.3 | 589 | 92.8 | 729 | 116.4 | 271 | 44.1 | 625 | 103.8 |
| Malta | Y | C | 372 | 71.4 | 378 | 73.2 | 206 | 40.0 | 278 | 56.3 | 333 | 70.0 |
| Netherlans d | N | C | 3030 | 26.9 | 2692 | 24.1 | 2549 | 25.2 | 3415 | 34.1 | 3091 | 34.6 |
| Poland | Y | C | 528 | 1.4 | 616 | 1.6 | 414 | 1.1 | 715 | 1.9 | 719 | 1.9 |
| Portugal | Y | C | 868 | 8.4 | 973 | 9.4 | 790 | 7.7 | 887 | 8.6 | 610 | 5.9 |
| Romania | Y | C | 525 | 2.8 | 348 | 1.8 | 300 | 1.6 | 805 | 4.1 | 573 | 2.9 |
| Slovakia | Y | C | 4777 | 87.9 | 6099 | 111.7 | 4921 | 90.2 | 7690 | 141.1 | 8339 | 153.2 |
| Slovenia | Y | C | 938 | 44.5 | 856 | 40.6 | 811 | 38.7 | 1085 | 52.1 | 1305 | 63.1 |
| Spain e | N | C | 20,816 | 60.1 | 20,748 | 60.0 | 6891 | – | 9658 | – | 18,410 | – |
| Sweden | Y | C | 5165 | 49.4 | 4059 | 39.1 | 3435 | 33.3 | 6693 | 65.4 | 8132 | 80.4 |
| EU Total 27 | – | – | 137,107 | 43.1 | 137,317 | 43.1 | 120,543 | 40.2 | 161,921 | 54.0 | 181,324 | 58.3 |
| United Kingdom | – | – | – | – | – | – | – | – | 58,718 | 88.1 | 65,246 | 98.4 |
| EU Total f | – | – | 137,107 | 43.1 | 137,317 | 43.1 | 120,543 | 40.2 | 220,639 | 60.6 | 246,570 | 66.0 |
| Iceland | Y | C | 104 | 27.6 | 58 | 15.7 | 95 | 26.1 | 136 | 38.1 | 145 | 41.6 |
| Norway | Y | C | 2980 | 54.9 | 2049 | 38.0 | 2422 | 45.1 | 4154 | 78.0 | 3668 | 69.3 |
| Liechtenstein | Y | C | 50 | 127.2 | 38 | 97.3 | 6157 | 71.5 | 7165 | 83.5 | 7642 | 89.7 |
| Switzerland g | Y | C | 7546 | 86.4 | 6759 | 78.0 | ||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Sentinel surveillance; notification rates calculated with estimated coverage of 20%.
Sentinel surveillance: no information on estimated coverage. Notification rate cannot be estimated.
Sentinel surveillance; notification rates calculated with estimated coverage of 64% in 2021–2022, 58% in 2019–2020 and 52% in 2018.
Sentinel system; notification rates calculated with an estimated population coverage of 73% in 2021–2022. No information on estimated coverage in 2018–2020, so notification rate cannot be estimated.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
For most (96.1%) of the reported campylobacteriosis cases of known origin, the infection was acquired in the EU (including both domestic and travel‐associated cases within the EU) (Table 4). This figure is slightly down on 2021 (99.1%), but still higher than the average rate (94.2%) of the pre‐pandemic years in 2019–2020. The proportion of domestic cases among the cases of known origin was 80%–100% in all reporting countries, except for three MSs, which reported the highest proportion of travel‐associated cases: Finland (68.7%), Sweden (40.6%) and Denmark (29.6%). Twenty‐one MSs reported imported cases, and the proportion of travel‐related cases was 9.7%, which was higher than in 2021 (3.8%). The number of cases acquired outside the EU increased considerably in 2022 compared with 2021 (Table 4). Of the 7994 travel‐associated cases reported by MSs with a known country of origin, 4036 cases (50.5%) were linked to travel within the EU, with most of the infections being acquired in Spain, Greece, Italy and Croatia (31.1%, 12.5%, 8.6% and 8.1%, respectively). Türkiye, Thailand, Indonesia, Morocco and India were the most frequently reported probable countries of infection outside the EU (23.4%, 11.4%, 6.9%, 4.8% and 3.8%, respectively).
Between 2013 and 2022, the number of confirmed campylobacteriosis cases reported in the EU showed a clear seasonal trend, peaking in the summer months. Annual winter peaks were also observed in January from 2013 to 2022, although peak numbers were lower than those observed during the summer. However, the overall campylobacteriosis trend in 2018–2022 showed no statistically significant increase or decrease (Figure 1). Belgium, Finland, Hungary and Slovakia reported significantly decreasing trends (p < 0.05) during the period 2018–2022. Cyprus, Luxemburg and Portugal reported a significantly increasing trend over the same period.
FIGURE 1.
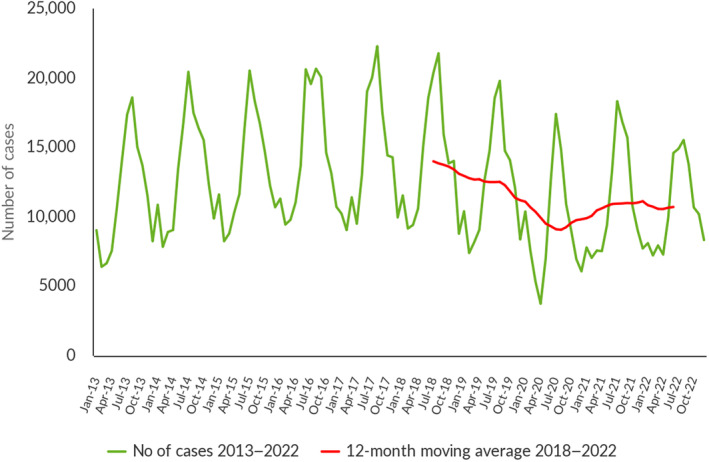
Trends in reported confirmed human cases of campylobacteriosis in the EU, by month, 2018–2022. Source: Austria, Belgium, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Hungary, Ireland, Italy, Latvia, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain and Sweden.
Campylobacteriosis cases were reported in all age groups, with the highest proportion of reported cases in the youngest age group from 0 to 4 years (20,524 cases: 15.6%).
Information on hospitalisation status was provided for 32.7% of all campylobacteriosis cases by 16 MSs, with 10,551 (23.5%) hospitalisations in total. The highest hospitalisation rates were reported in Romania (100%), Cyprus (89.7%), Greece (87.2%) and Poland (82.8%), where all or most of the reported cases were hospitalised. Compared with 2021 (35.3%), reports on hospitalisation status decreased, while the proportion of hospitalised cases (23.2%) remained virtually unchanged. Outcomes were reported for 61.6% of all cases by 17 MSs. Thirty‐four deaths from campylobacteriosis were reported in 2022, resulting in an EU case fatality rate of 0.04%. The average percentage of fatal outcomes observed has remained unchanged over the past 5 years (range 0.03%–0.05%).
Campylobacter species information was provided by 24 MSs for 60.4% of confirmed cases reported in the EU, representing a decrease on 2021 (65.1%). Of these cases, 87.6% were Campylobacter jejuni, 10.7% C. coli, 0.26% C. fetus, 0.17% C. upsaliensis and 0.12% C. lari. Other Campylobacter species accounted for 1.1% of cases, but most of those cases were reported at the national level as ‘C. jejuni/C. coli/C. lari not differentiated’. Belgium, Bulgaria and Denmark provided no information on species.
1.4.3. Campylobacter in food
Campylobacter data in the context of Regulation (EC) No 2073/2005
The requirements of the Official Controls Regulation (EU) 2017/625 (OCR) were introduced for the first time in this report, underpinned by the data reported by MSs in 2022. In contrast with previous legislation, Competent Authorities (CAs) must use methods complying with relevant internationally recognised rules or protocols, including those accepted by the European Committee for Standardisation (CEN). This condition is met by the use of EN ISO methods, which are ISO methods recognised by CEN. Consequently, and in contrast with previous legislation, CAs cannot use the alternative methods mentioned in Commission Regulation (EC) No 2073/2005 to carry out official controls aiming at verifying the correct implementation by FBOs of the provisions set out in this Regulation. The implementation of this change in legislative testing requirements may have impacted the results of official food control samples taken in 2022 as part of Commission Regulation (EC) No 2073/2005, compared with the results of similar samples taken in 2021 and before, when the requirements of the OCR were not yet implemented in the collection of zoonoses data by EFSA. Furthermore, PHC Campylobacter monitoring data may not be directly comparable among Member States due to both the potential authorisation for reduced sampling, as outlined in Commission Regulation (EC) No 2073/2005, and variations due to seasonal sampling practices. For these reasons, the above‐mentioned results should be interpreted with caution.
Campylobacter PHC monitoring data are presented in Table 6 Ad hoc official sampling results were reported by 16 MSs and the United Kingdom (Northern Ireland), while monitoring results from FBOp were reported by 20 MSs, and data from both samplers were provided by 12 MSs. Overall, the reported Campylobacter‐positive samples totalled 11,701 (38.9%) out of 30,101 tested neck skin samples.
TABLE 6.
Comparison of proportions (%) of Campylobacter‐positive single samples and samples exceeding the Campylobacter PHC limit collected from the neck skins of chilled broiler carcases sampled at slaughterhouses in accordance with Regulation (EC) No 2073/2005, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a , b | Interpretation b | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N samples tested | N (%) samples positive | N (%) samples above 1000 CFU/g | CI95 samples above 1000 CFU/g | N samples tested | N (%) samples positive | N (%) samples above 1000 CFU/g | CI95 samples above 1000 CFU/g | |||
| Austria | 290 | 151 (52.1) | 89 (30.7) | [25.4; 36.3] | 1044 | 594 (56.9) | 139 (13.3) | [11.3; 15.5] | < 0.001 | CA > FBOp |
| Belgium | 579 | 344 (59.4) | 95 (16.4) | [13.5; 19.7] | 2622 | NA e | 204 (7.8) | [6.8; 8.9] | < 0.001 | CA > FBOp |
| Bulgaria | 702 | 70 (10.0) | 3 (0.43) | [0.09; 1.2] | – | – | – | – | – | – |
| Croatia | 1035 | 445 (43) | 316 (30.5) | [27.7; 33.4] | – | – | – | – | – | – |
| Cyprus | 205 | 165 (80.5) | 71 (34.6) | [28.1; 41.6] | – | – | – | – | – | – |
| Czechia | – | – | – | – | 3570 | 2098 (58.8) | 1269 (35.5) | [34; 37.1] | – | – |
| Denmark | – | – | – | – | 1090 | 258 (23.7) | 114 (10.5) | [8.7; 12.4] | – | – |
| Estonia | 14 | 2 (14.3) | 1 (7.1) | [0.18; 33.9] | 250 | 0 | 0 | [0; 1.5] c | < 0.001 | CA > FBOp |
| Finland | – | – | – | – | 585 | NA e | 0 | [0; 0.63] c | – | – |
| France | – | – | – | – | 19,376 | NA e | 5249 (27.1) | [26.5; 27.7] | – | – |
| Germany | 10 | NA d | 2 (20.0) | [2.5; 55.6] | 5523 | NA e | 558 (10.1) | [9.3; 10.9] | NS | – |
| Greece | 85 | 85 (100) | 55 (64.7) | [53.6; 74.8] | 2678 | 2145 (80.1) | 112 (4.2) | [3.5; 5.0] | < 0.001 | CA > FBOp |
| Hungary | 634 | 85 (13.4) | 50 (7.9) | [5.9; 10.3] | – | – | – | – | – | – |
| Ireland | 199 | 118 (59.3) | 16 (8.0) | [4.7; 12.7] | 995 | 301 (30.3) | 37 (3.7) | [2.6; 5.1] | 0.0034 | CA > FBOp |
| Italy | 1611 | NA f | 296 (18.4) | [16.5; 20.4] | 6449 | NA f | 726 (11.3) | [10.5; 12.1] | < 0.001 | CA > FBOp |
| Latvia | 100 | 24 (24.0) | 19 (19.0) | [11.8; 28.1] | 531 | 199 (38.4) | 94 (17.7) | [14.5; 21.2] | NS | – |
| Netherlands | 306 | 80 (26.1) | 18 (5.9) | [3.5; 9.1] | 3332 | 167 (5.0) | 167 (5.0) | [4.3; 5.8] | NS | – |
| Poland | 630 | 245 (38.9) | 125 (19.8) | [16.8; 23.2] | 2530 | 889 (35.1) | 323 (12.8) | [11.5; 14.1] | < 0.001 | CA > FBOp |
| Portugal | – | – | – | – | 3705 | 1257 (33.9) | 783 (21.1) | [19.8; 22.5] | – | – |
| Romania | 105 | 0 | 0 | [0; 3.5] c | 1115 | 316 (28.3) | 0 | [0; 0.33] c | NS | |
| Slovakia | – | – | – | – | 417 | 260 (62.4) | 0 | [0; 0.88] c | – | – |
| Slovenia | – | – | – | – | 814 | 620 (76.2) | 316 (38.8) | [35.5; 42.3] | – | – |
| Spain | 850 | 555 (65.3) | 340 (40.0) | [36.7; 43.4] | 700 | 129 (18.4) | 129 (18.4) | [15.6; 21.5] | < 0.001 | CA > FBOp |
| Sweden | – | – | – | – | 1046 | 58 (5.5) | 18 (1.7) | [1.0; 2.7] | – | – |
| United Kingdom (Northern Ireland) | 550 | 41 (7.5) | 41 (7.5) | [5.4; 10] | – | – | – | – | – | – |
| EU Total (27 + XI) | 7905 | 2410 (38.3) d | 1537 (19.4) | [18.6; 20.3] | 58,372 | 9291 (39.0) e | 10,238 (17.5) | [17.2; 17.9] | < 0.001 | CA > FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 4779 | 1260 (48.9) d | 1056 (22.1) | [20.9; 23.3] | 27,769 | 4740 (36.0) e | 2489 (9.0) | [8.6; 9.3] | < 0.001 | CA > FBOp |
Abbreviations: NA, not available; –, Data not reported.
p‐value: NS, not significant.
Relating to the percentage of positive samples above 1000 CFU/g.
One‐sided, 97.5% confidence interval.
Germany did not report Campylobacter‐positive samples below 1000 CFU/g, based on the test results from the Competent Authority.
Belgium, Finland, France and Germany did not report Campylobacter‐positive samples below 1000 CFU/g, based on the test results from food business operators.
Italy informed during the last phase of the production of this report that the number of positive samples not exceeding 1000 CFU/g were reported to EFSA and were for 26.3% for sampling by CA and 55.6% for sampling by FBOp.
Concerning official control samples (N = 7905), 19.4% exceeded the limit of 1000 CFU/g. Considerable variability was observed in percentage test results exceeding the limit. In particular, Romania reported none, while six MSs (Bulgaria, Estonia, Hungary, Ireland, the Netherlands and the United Kingdom [Northern Ireland]) reported 8% or fewer samples exceeding the limit. Conversely, 10 MSs reported a higher percentage of samples above the limit, ranging from 16.4% to 64.7%. The overall percentage of Campylobacter‐positive samples was 38.3%.
Concerning FBOp results for neck skin samples from own‐check sampling activities (N = 58,372), 17.5% exceeded the limit of 1000 CFU/g. Four MSs (Estonia, Finland, Romania, Slovakia) recorded zero samples exceeding the limit, whereas the remaining 16 MSs reported a moderate range in the percentage of samples exceeding the limit, from 1.7% to 38.8%. The overall percentage of Campylobacter‐positive samples was 39%. Three non‐EU MSs (Iceland, Montenegro and Switzerland) reported respectively 1.3% (N = 748), 10% (N = 50) and 11% (N = 890) FBOp samples exceeding the limit.
Twelve MSs reported results from both samplers, in which the overall percentage of samples exceeding the limit was significantly higher for official control samples (22.1%) than for own checks (9%). A higher percentage of samples above the limit was also observed in official samples compared with FBOp samples in eight MSs (Austria, Belgium, Estonia, Greece, Ireland, Italy, Poland, Spain). A substantial difference in the percentage of Campylobacter‐positive samples was also observed, with the figure for official controls (48.9%) being higher than own checks (36%).
Overall, for the Campylobacter PHC monitoring data provided by 24 MSs and the United Kingdom (Northern Ireland), the percentage of samples exceeding the limit was significantly higher in official samples (19.4%) than in FBOp samples (17.5%).
For a further interactive look at Campylobacter monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
Other food monitoring data
In 2022, the occurrence of Campylobacter in sampling units from the main RTE and non‐RTE food categories was 0.11% and 11.1%, respectively. In fresh meat, 12% of sampling units were positive.
In 2022, most of the results from the 2774 RTE food sampling units reported by 11 MSs originated from ‘fruit, vegetables and juices’ (36.9%), followed by ‘milk and milk products’ (25.7%) and ‘meat and meat products’ (11.3%). In total, Campylobacter was detected in three RTE food samples: one from ‘meat and meat products’, more specifically from ‘minced meat from other poultry species intended to be eaten raw’ and two from ‘fish and fishery products’, notably from oysters. During the period 2018–2021, the percentage of Campylobacter‐positive sampling units in RTE food was very low, remaining below 1% for all categories, with the highest percentage detected for ‘raw milk’, 0.90% (N = 1229).
The results reported in 2022 by 16 MSs for non‐RTE food (N = 25,601) showed that ‘meat and meat products’ was the most contaminated food category (11.6%), followed by ‘other food’ (11%) and ‘milk and milk products’ (1.4%). During the period 2018–2021, ‘meat and meat products’ (21.8%) was the most contaminated food category, followed by ‘milk and milk products’ (1.3%).
Fourteen MSs reported results for fresh meat categories. The percentage of Campylobacter‐positive units was similar for meat from broilers (12%) and turkey (11.2%), and higher for ‘other fresh meat’ (15.3%). The percentage for fresh meat from pigs and bovine animals remained relatively low; 2.9% and 1.3%, respectively.
In 2022, a substantial decrease was reported in the percentage of positive units compared with the period 2018–2021, for non‐RTE food (11.1% compared with 19.6%) and fresh meat (12% compared with 21.7%).
For a further interactive look at Campylobacter monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
1.4.4. Campylobacter in animals
Table 7 shows the number of positive Campylobacter spp. sampling units detected during 2022 in the six main animal species, as well as in the ‘other animals’ category containing more than 40 different animal groups. In total, 14 MSs and the United Kingdom (Northern Ireland) and three non‐MSs reported data, primarily relating to broilers (43.9%, N = 12,704), followed by bovine animals (20%, N = 5792) and small ruminants (10.7%, N = 3088). The overall proportion of positive units in the EU was highest in turkeys (71.9%) followed by broilers (18.1%), cats and dogs (12.5%) bovine animals (6.4%), small ruminants (2.2%) and pigs (1.8%). Although fewer sampling units were tested for ‘other animals’, a considerable proportion of positives were detected in samples from ducks collected by Germany (94%, N = 349).
TABLE 7.
Summary of Campylobacter statistics relating to major animal species, reporting EU MSs and non‐MS countries, 2022.
| Animals | EU MSs | Non‐MS countries | ||||||
|---|---|---|---|---|---|---|---|---|
| N reporting countries | N tested a sampling units | Positive sampling units | N reporting countries | N tested a sampling units | Positive sampling units | |||
| N | % | N | % | |||||
| Gallus gallus (broilers) | 13 | 9035 | 1636 | 18.1 | 3 | 3669 | 384 | 10.5 |
| Bovine animals b | 7 | 5698 | 364 | 6.4 | 2 | 94 | 33 | 35.1 |
| Pigs | 5 | 1820 | 32 | 1.8 | 1 | 5 | 1 | 20.0 |
| Small ruminants | 6 | 3082 | 69 | 2.2 | 1 | 6 | 0 | 0 |
| Cats and dogs | 4 | 754 | 94 | 12.5 | 2 | 1542 | 113 | 7.3 |
| Turkeys | 6 | 1201 | 863 | 71.9 | 1 | 30 | 1 | 3.3 |
| Other animals c | 7 | 1737 | 539 | 31.0 | 1 | 295 | 30 | 10.2 |
| Total | 15 | 23,327 | 3597 | 15.4 | 3 | 5641 | 562 | 10.0 |
Abbreviation: MSs, Member States.
Summary statistics were obtained by totalling all sampling units (single samples, batch samples, animals, slaughter animal batches and herds or flocks).
Animals from the sampling stage ‘Artificial insemination stations’ were not included.
Alpacas, Badgers, Bears, Birds, Budgerigars, Buffalos, Camels, Canary, Cantabrian chamois, Crows, Deer, Doves, Ducks, Ferrets, Foxes, Gallus gallus (other than broilers), Gerbils, Giraffes, Guinea pigs, Gulls, Hedgehogs, Kangaroos, Land game mammals, Leporidae, Magpies, Martens, Monkeys, Mouflons, Other animals, Other carnivores, Other ruminants, Parrots, Passeriformes, unspecified, Peafowl, Pigeons, Psittacidae, Raccoons, Rats, Reptiles, Rodents, Solipeds, domestic, Steinbock, Swans, Turtles, Wallabies, Water buffalos, Wild animals, Wild boars, Wild cats (Felis silvestris), Zoo animals, all.
1.5. Discussion
Campylobacteriosis has been the most frequently reported zoonosis in humans across the EU since the beginning of EU‐level surveillance in 2007. Despite comprehensive surveillance and national coverage in most MSs, the number of reported cases is underestimated in the EU (Teunis et al., 2013). The number of campylobacteriosis cases confirmed in 2022 was similar to 2021, and the notification rate remained the same. Interestingly, most EU MSs did not return to the pre‐pandemic notification rates. No specific causes have been reported to explain this generalised phenomenon in the EU. The overall campylobacteriosis trend in 2018–2022 showed no statistically significant increase or decrease.
Most of the reported campylobacteriosis cases were acquired in the reporting country in the EU as in previous years. However, the proportion and number of cases of travel‐associated campylobacteriosis infections increased considerably in 2022 compared to the period 2021–2020, reflecting the gradual easing of international travel restrictions after the COVID‐19 pandemic. The number of cases doubled and quadrupled among travellers inside and outside the EU, respectively. Mediterranean countries were the main destinations of travel‐associated campylobacteriosis cases in 2022, as they were in 2021. Nonetheless, travel‐associated cases still remained at a lower level than in pre‐pandemic years.
Campylobacter has a characteristic seasonality with cases increasing sharply in the summer. Campylobacteriosis cases have been positively associated with temperature and, to a lesser degree, precipitation (Lake et al., 2019). Recent studies have even evidenced a possible association between campylobacteriosis and global climate change (Kuhn et al., 2020).
A smaller but distinct winter peak in the EU has become apparent in the past 10 years, including in 2022. Disease onsets in cases that were notified during the winter peaks occurred predominantly in January. This points to an exposure around the Christmas/New Year period. Reports indicate that meat fondues or table‐top grilling, which are popular during the festive season, could promote the transmission of Campylobacter in some countries, causing the winter peak (Bless et al., 2017; Rosner et al., 2021).
In 2022, more than 10,000 cases of campylobacteriosis resulted in hospitalisation, which is the second highest number of hospitalisations caused by a zoonotic pathogen after salmonellosis. The proportion of hospitalised campylobacteriosis cases was higher than expected in some MSs, where all or most of the confirmed cases were hospitalised. These MSs also reported the lowest notification rates, indicating that surveillance focuses primarily on hospitalised (i.e. severe) cases. This can lead to an overestimation of the proportion of hospitalisations and may also indicate severe underreporting of the actual total number of cases in some countries. As in previous years, C. jejuni and C. coli were the main species notified by MSs in 2022, although there was still a fairly high percentage of campylobacteriosis cases (39.6%), in which the species was not determined. Further, the proportion of isolates characterised at species level was down on the previous year, so further improvements and efforts are needed in species identification and reporting capacity. A One Health approach, using whole genome sequencing (WGS) for typing Campylobacter isolates in humans, food and animals, will contribute to better species characterisation and enhance the monitoring of zoonotic transmission, improving public health surveillance.
In 2022, as part of a food safety control strategy, 24 EU MSs and the United Kingdom (Northern Ireland) submitted Campylobacter PHC monitoring results, with 12 countries reporting both results from official control samples and own‐check samples, five only official results and eight only own‐check results. Official control and FBOp monitoring data showed that about one in five and one in six samples exceeded the limit of 1000 CFU/g, respectively. For the MSs that submitted data from both samplers, one in five samples from the CA and one in 11 from FBOp exceeded the limit, respectively. Moreover, the CA also reported considerably higher percentages of Campylobacter‐positive samples. These discrepancies, observed for the third year, deserve more thorough investigation in order to identify the critical parameters and factors explaining these differences.
A harmonised procedure for reporting the results of official control samples for Campylobacter came into force in late 2019, in accordance with Commission Implementing Regulation (EU) 2019/627. However, implementation is proving to be challenging for a number of MSs. In some cases, the number of positive samples below the limit was not reported. Moreover, a number of unexplained disparities from previous years have been observed in the results. Obtaining a clear and comprehensive overview in Europe is therefore extremely challenging, making it difficult to draw final conclusions.
The PHC aims to decrease Campylobacter counts on broiler carcasses and to minimise human campylobacteriosis cases caused by consuming or handling contaminated chicken/broiler meat. A recent report showed that a 3‐log10 reduction in broiler caecal concentrations would lead to a significant 58% decrease in the campylobacteriosis risk from broiler meat across the EU (EFSA, Koutsoumanis, Allende, Alvarez‐Ordóñez, et al., 2020).
Monitoring of other food in the EU showed overall percentages of Campylobacter‐positive units in RTE and non‐RTE foods of 0.11% and 11.1%, respectively. Although the presence of Campylobacter in RTE foods was very low and has remained stable over the years, these findings are of concern given that contaminated RTE products directly expose consumers to infection. Among RTE foods, ‘minced meat from other poultry species intended to be eaten raw’, and oysters were found to be contaminated with Campylobacter. During the period 2018–2021, most Campylobacter‐positive units in RTE foods concerned meat. The only positive results involving oysters were reported in 2021. Nevertheless, given the common practice of consuming raw shellfish in certain European sub‐regions, the risk of campylobacteriosis from these sources is noteworthy (Teunis et al., 1997). It should also be noted that these data originated from a single EU‐MS, highlighting the need to increase the sampling frequency for food products consumed raw (such as scallops, mussels, oysters) across regions. The generally small size of sampling units could have led to imprecise estimations concerning the prevalence of RTE food sampling units contaminated by Campylobacter.
Monitoring data for non‐RTE food showed positive results for one in nine ‘meat and meat products’, and one in 70 ‘milk and milk products’. A moderate proportion of positive findings, specifically 17.2% (N = 197), were reported in bivalve molluscs (mussels) by a single EU‐MS, paralleling the scenario observed in RTE‐foods. While Campylobacter contamination in fresh meat categories remained moderate in 2022, the number of positive units dropped sharply for the second consecutive year compared with the preceding four‐year period (11.6% vs. 21.8%). Although caution is required when interpreting trend results, due to non‐harmonised monitoring, the data still consistently underline the significant role of these products in spreading campylobacteriosis. This may occur either through direct handling or by cross‐contaminating other foods (Wagenaar et al., 2013).
In 2022, 14 MSs, the United Kingdom (Northern Ireland) and 3 non‐MSs reported data from several animal groups. Campylobacter spp. was detected in all the major animal categories: broilers, turkeys, pigs, bovine animals, small ruminants, cats and dogs. Broilers were tested most frequently and accounted for 43.9% of test results, followed by bovine animals and small ruminants. The highest percentage of positive units, however, was observed for turkeys. Despite an increase in the number of tested units, less than half of MSs reported broiler data in 2022, thereby hampering a fair comparison of data and probably indicating varying positive results as a result of testing taking place in different epidemiological scenarios.
2. SALMONELLA
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here, and are also retrievable from the EFSA Salmonella dashboard available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
2.1. Key facts
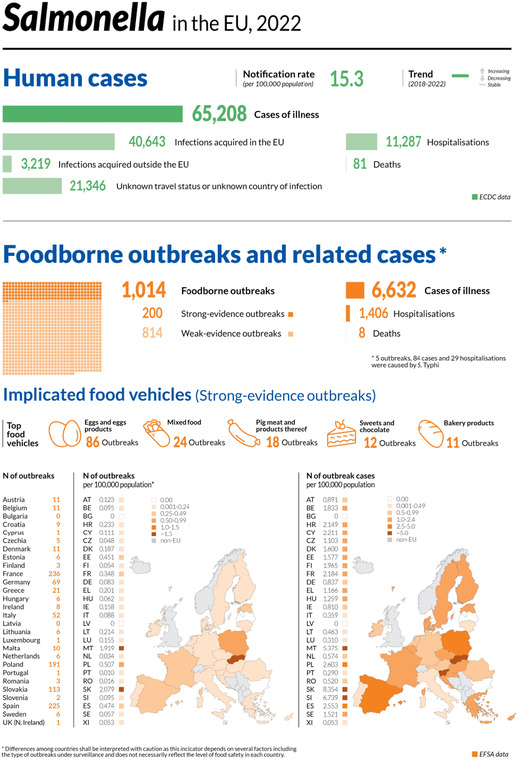
Salmonellosis was the second most commonly reported foodborne gastrointestinal infection in humans in the European Union and was a major cause of foodborne outbreaks in European Union Member States and non‐Member State countries.
In 2022, there were 65,208 confirmed cases of human salmonellosis, corresponding to an European Union notification rate of 15.3 cases per 100,000 population. The notification rate was stable compared with the rate in 2021.
The overall trend for Salmonella infections did not show any significant increase or decrease in the 2018–2022 period.
The proportion of hospitalised cases was 38.9%, which was slightly higher than in 2021, with an European Union case fatality rate of 0.22%, which was similar to 2021.
The top five European Union‐acquired Salmonella serovars involved in human infections were distributed as follows: S. Enteritidis (67.3%), S. Typhimurium (13.1%), monophasic S. Typhimurium (1,4,[5],12:i:‐) (4.3%), S. Infantis (2.3%) and S. Derby (0.89%).
In 2022, 0.16% of 99,341 ‘ready‐to‐eat’ food sampling units reported by 25 Member States were positive for Salmonella, with the highest levels of contamination found in ‘meat and meat products from broilers’ (1.4%; N = 584) and ‘spices and herbs’ (1.1%; N = 1309). Of 521,917 ‘non‐ready‐to‐eat’ sampling units reported by 28 Member States, 2.1% were positive, with the highest levels of contamination found in ‘meat and meat products from broilers’ (5.1%; N = 99,022) and ‘meat and meat products from turkeys’ (3.3%; N = 13,867).
Sampling to verify compliance with process hygiene criteria on carcases at the slaughterhouse in the context of Regulation (EC) No 2073/2005 16 for Member States found the highest proportions of Salmonella‐positive samples among those collected by the competent authorities for turkeys (14%), broilers (11.8%), pigs (2.7%), cattle (0.96%) and sheep (0.75%).
Nineteen Member States and the United Kingdom (Northern Ireland) reporting on Salmonella control programmes met all reduction targets for poultry populations, which is an improvement compared with the previous years. The number of Member States that did not meet the reduction targets was four for breeding Gallus gallus, four for laying hens and one for fattening turkeys, whereas for broilers and breeding turkeys, all Member States reached the reduction targets.
For broilers and fattening turkeys, the EU‐level flock prevalence reported by food business operators was significantly lower than that reported by competent authorities.
There were no significant variations in the estimated European Union flock prevalence for poultry populations over the years, neither for Salmonella spp. nor for target Salmonella serovars. The only exception was for breeding turkeys, for which a significant increase in the estimated Salmonella spp. flock prevalence was noted in 2022 compared with 2016, when it reached the lowest value seen during the entire study period (2010‐2022).
S. Enteritidis was the most commonly reported serovar in laying hens and the second most commonly reported one in broilers. S. Infantis was by far the main serovar isolated from broilers, and ranked among the top four serovars for all the food‐animal sources considered. The most common serovars from pig sources included the monophasic variant of S. Typhimurium and S. Typhimurium. The latter serovar was the most commonly reported one from bovine animals, together with S. Dublin.
2.2. Surveillance and monitoring of Salmonella in the EU
EFSA story map on Salmonella
General information on Salmonella and its epidemiology, including information on where the pathogen can be found, how people and animals get infected, the occurrence of this pathogen in different sources, the disease it causes and how to prevent infection, is provided in the EFSA story map on Salmonella (available here). In addition, this story map also illustrates the monitoring activities implemented in the EU and the role of EFSA with respect to these activities.
2.2.1. Humans
For 2022, all 27 EU MSs reported information on non‐typhoidal salmonellosis infections in humans. The notification of salmonellosis is mandatory in 24 EU MSs, whereas it is voluntary in three MSs (Belgium, France and the Netherlands). The EU case definition was used by 24 MSs, while 3 MSs (France, Germany and Italy) reported using other case definitions. All countries except the Netherlands had a comprehensive surveillance system. The surveillance systems for salmonellosis covered the whole population in all MSs except three: Belgium, the Netherlands and Spain. The estimated coverage of the surveillance system was 85% in Belgium, 64% in the Netherlands and 73% in Spain. These estimated proportions of population coverage were used in the calculation of notification rates for these MSs. No estimated population coverage for 2018–2020 in Spain was provided, so notification rates were not calculated. All countries reported case‐based data except Bulgaria, which reported aggregated data.
2.2.2. Food, animals and feed
Salmonella data in the context of regulation (EC) no 2073/2005
Regulation (EC) No 2073/2005 lays down microbiological criteria, intended as food safety criteria (FSC) and process hygiene criteria (PHC), for Salmonella in specific food categories. Compliance with these criteria must be legally verified by the individual FBOp as part of their own Hazard Analysis and Critical Control Point (HACCP) programme. 17 In addition, the competent authority (CA), through official sampling or oversight of data, should ensure that the FBOp complies with these regulatory requirements. The Salmonella FSC require that the pathogen not be detected in different products during their shelf‐life. Moreover, in fresh poultry meat (from species covered by national control programmes), the FSC require the absence of target serovars (S. Enteritidis and S. Typhimurium including monophasic S. Typhimurium (1,4,[5],12:i:‐) 18 ). The Salmonella PHC are regulated for carcases of pigs, cattle, sheep, goats, horses, broilers and turkeys, as sampled by the FBOp. Moreover, in accordance with Regulation (EU) 2019/627, 19 the CA has to verify whether the FBOp correctly implements and checks these PHC for carcases. Further details on Salmonella surveillance in food can be found in the EFSA story map (here).
Data from national control programmes for Salmonella in poultry populations
According to Regulation (EC) No 2160/2003 20 and its subsequent amendments, MSs have to set up national control programmes (NCPs) for Salmonella aimed at reducing the prevalence of Salmonella serovars that are considered relevant for public health (from this point forward, termed ‘target serovars’). Every year, MSs must report results for their Salmonella NCP and, for broiler flocks and breeding and fattening turkey flocks, results for sampling conducted by the CA and FBOp must also be reported separately. Further details on Salmonella surveillance in animals and NCPs can be found in the EFSA story map (here).
Other monitoring data for food, animals and feed including serovars
Food, animal and feed data other than those described above are not collected in a harmonised way, because there are no specific legal requirements. The reported occurrence of Salmonella in the main food categories was descriptively summarised, with a distinction being made between ‘ready‐to‐eat' (RTE) and non‐RTE food. Data sets were extracted with ‘objective sampling’ being specified as the sampling strategy, which means that sampling units were representative of the population being analysed and were collected in accordance with a planned strategy.
The occurrence of Salmonella in animal populations was descriptively summarised considering all data collected in different sampling contexts and reported as different sampling units (e.g. ‘holding’, ‘herd/flock’, ‘animal’ and ‘slaughter animal batch’), with the exception of data related to poultry populations covered by NCPs, which have been discussed separately.
The reported data on Salmonella serovars were also descriptively summarised. For this purpose, only isolates with the complete antigenic formula and/or serovar name were considered. MSs are required to report the target serovars as part of their NCPs for poultry, whereas for the samples collected in different contexts, serotyping is not mandatory. Also, for the food sector, the FSC is the absence of Salmonella, except for fresh poultry meat, for which the criterion is the absence of target serovars. The compulsory reporting of target serovars in some contexts (NCPs for poultry and FSC for fresh poultry meat) guarantees the consistency of such data over the years and among MSs but could result in the prevalence of these target serovars being overestimated compared with the other serovars.
2.3. Data analyses
2.3.1. Comparison between competent authority and food business operator sampling results
CA and FBOp Salmonella results in the context of NCPs for those poultry populations requiring separate reporting (i.e. broilers and fattening and breeding turkeys) were compared, as were Salmonella PHC monitoring data from carcases. The significance of differences was verified by the one‐tailed Fisher's exact probability test, in cases where the expected values in any of the cells of a contingency table were below five; otherwise, the z‐statistic one‐tailed test was performed. CA control sampling results and the own‐check results of the FBOp were expressed as prevalence and exact binomial confidence interval (95% level). A p‐value < 0.10 (Clayton & Hills, 2013) was considered significant, to include all possible evidence of differences between data collected by the FBOp and CA.
R software (www.r‐project.org, version 4.2.3) was used to conduct the above‐mentioned analyses.
2.3.2. Statistical trend analyses for poultry monitoring data
Statistical trend analyses were carried out with the objective of evaluating the significance of temporal variations in the EU‐level flock prevalence of Salmonella and target Salmonella serovars in poultry since the start of NCP implementation.
The tested flocks can be either positive or negative for target serovars and Salmonella, and so the status of the flocks is a dichotomous outcome variable. Therefore, the binomial probability distribution for the response variable was assumed and the logit link function was computed in the model for the trend analysis. The logit is defined as the logarithm of p/(1 – p), where p/(1 – p) is the odds of being positive for Salmonella.
According to temporal flock prevalence trends in the MSs, B‐spline basic models for the logit of the probability of flocks being positive were fitted for the different poultry populations over the entire period of NCP implementation. Moreover, attention was paid to the period after achievement of the minimum prevalence reported to date, to capture any evidence of a significant increase in Salmonella prevalence. Marginal and conditional generalised linear models for repeated measures were used to perform these trend analyses (EFSA, 2009a, 2011). The marginal models take into account the non‐independence among observations and provide a population‐averaged interpretation (across all MSs). The conditional models take into account the heterogeneity among MSs using random effects (G‐side random effect) and provide a subject‐specific interpretation. Moreover, by adding the R‐side random effect, it is possible to model the correlation among observations of the same MS.
Details about the estimated parameters of the models, odds ratios, prevalence rates and graphical analyses (conditional and marginal) are reported in the supporting information for this report (‘Salmonella poultry outcome trend analyses’ Excel file).
To investigate EU‐level prevalence, considering the relevant heterogeneity among MSs for the flock prevalence of Salmonella and target serovars over time, the results obtained using the conditional generalised model for longitudinal binary data were summarised and discussed in the report, for all poultry populations covered by NCPs. To take into account the different levels (baselines) of probability of MSs having positive flocks, yet with similar patterns over time, a random MS‐specific intercept effect was included in the model. To evaluate the trend over time, the ‘time' variable was included in the model as a fixed effect. The correlation between repeated observations in the same MS in subsequent years was considered using a first autoregressive or exchangeable structure of the correlation matrix for the residuals. To evaluate the significance of the overall effect of fixed factors specified in the model, Type III F‐tests were applied, whereas the receiver operating characteristic (ROC) curve was used to assess the goodness of fit of the model. A p‐value < 0.10 was considered to be significant for both random and fixed effects.
GLIMMIX and SGPLOT procedures in SAS 9.4 software were used to fit the models and to produce the graphical outputs, respectively.
2.3.3. Descriptive analyses of Salmonella serovars
With the aims of evaluating the distribution of Salmonella serovars across the food chain and identifying potential sources of human infections, a Sankey diagram was provided to link the food and food‐producing animal sources to the five most commonly reported Salmonella serovars from human cases acquired within the EU (domestically or during travel within the EU). For animal categories covered by NCPs, only serovar data reported in the context of these programmes were presented. For cattle, meat‐producing animals were considered, whereas for pigs, data from fattening animals were used. In addition to possible reporting biases as regards serovars, reporting for animal or food categories may also have been unbalanced and specific sources (e.g. cattle) may have been underrepresented.
EFSA dashboard on Salmonella
Summary statistics for the monitoring results for Salmonella with regard to major food categories and animal species, Salmonella‐positive official samples in the context of FSC and PHC, the occurrence of Salmonella in major food categories, and the achievement by MSs of Salmonella reduction targets in poultry populations are displayed, retrievable and downloadable in the EFSA dashboard on Salmonella (available here).
2.4. Results
2.4.1. Overview of key statistics, EU, 2018–2022
Humans
In total, the number of reported human salmonellosis cases was higher than in 2021 while the notification rate was constant (Table 8). The number of reported human salmonellosis cases acquired in the EU (i.e. by domestic infection and through travel within the EU) and the number of outbreak‐related cases were lower in 2022 than in 2021, while the total number of foodborne salmonellosis outbreaks was higher in 2022 than in 2021. More detailed descriptions of these statistics are provided in the subsections below and in the chapter on foodborne outbreaks.
TABLE 8.
Summary of Salmonella statistics relating to humans, major food categories and the main animal species, EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 65,208 | 60,169 | 52,690 | 87,907 | 91,858 | ECDC |
| Total number of confirmed cases/100,000 population (notification rate) | 15.3 | 15.3 | 12.1 | 17.5 | 17.6 | ECDC |
| Number of reporting MSs | 27 | 27 | 27 | 28 | 28 | ECDC |
| Infection acquired in the EU | 40,643 | 43,720 | 38,247 | 58,157 | 59,763 | ECDC |
| Infection acquired outside the EU | 3219 | 925 | 973 | 6343 | 6376 | ECDC |
| Unknown travel status or unknown country of infection | 21,346 | 15,524 | 13,470 | 23,407 | 25,719 | ECDC |
| Number of outbreak‐related cases | 6632 | 6755 | 3686 | 10,240 | 11,631 | EFSA |
| T otal number of outbreaks | 1014 | 773 | 694 | 1284 | 1588 | EFSA |
| Food c | ||||||
| Meat and meat products | ||||||
| Number of sampling units | 951,590 | 977,446 | 557,341 | 552,590 | 433,197 | EFSA |
| Number of reporting MSs | 28 | 28 | 26 | 28 | 28 | EFSA |
| Milk and milk products | ||||||
| Number of sampling units | 68,740 | 43,907 | 38,492 | 46,797 | 44,078 | EFSA |
| Number of reporting MSs | 24 | 25 | 24 | 25 | 24 | EFSA |
| Fish and fishery products | ||||||
| Number of sampling units | 22,797 | 14,882 | 16,486 | 13,974 | 17,075 | EFSA |
| Number of reporting MSs | 25 | 25 | 23 | 24 | 22 | EFSA |
| Eggs and egg products | ||||||
| Number of sampling units | 19,105 | 14,696 | 11,579 | 12,093 | 10,611 | EFSA |
| Number of reporting MSs | 22 | 22 | 18 | 21 | 21 | EFSA |
| Fruits and vegetables (and juices) | ||||||
| Number of sampling units | 16,920 | 12,485 | 17,222 | 17,068 | 10,889 | EFSA |
| Number of reporting MSs | 25 | 23 | 23 | 22 | 22 | EFSA |
| Animals d | ||||||
| Gallus gallus (chickens) | ||||||
| Number of sampling units | 742,299 | 812,238 | 620,141 | 752,172 | 720,717 | EFSA |
| Number of reporting MSs | 28 | 28 | 26 | 27 | 27 | EFSA |
| Turkeys | ||||||
| Number of sampling units | 65,637 | 70,869 | 63,473 | 65,950 | 68,009 | EFSA |
| Number of reporting MSs | 26 | 25 | 22 | 23 | 24 | EFSA |
| Ducks and geese | ||||||
| Number of sampling units | 1187 | 3751 | 412 | 8700 | 9846 | EFSA |
| Number of reporting MSs | 6 | 10 | 6 | 9 | 6 | EFSA |
| Pigs | ||||||
| Number of sampling units | 15,283 | 16,689 | 17,234 | 18,619 | 17,868 | EFSA |
| Number of reporting MSs | 15 | 15 | 10 | 14 | 14 | EFSA |
| Cattle (bovine animals) | ||||||
| Number of sampling units | 22,904 | 26,061 | 28,363 | 86,871 | 30,302 | EFSA |
| Number of reporting MSs | 13 | 14 | 11 | 14 | 14 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
For the 2021–2022 period, data on food and animal samples from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
The number of sampling units was obtained by totalling all sampling units (single, batch, slaughter batch), sampling stages (automatic distribution system for raw milk, border control posts, canteen or workplace catering, catering, cold storage, conservation facilities, cutting plant, distribution: wholesale and retail sale, farm, feed mill, game handling establishment, hatchery, hospital or medical care facility, household, hunting, manufacturing, mobile retailer or market/street vendor, packing centre, primary production, processing plant, restaurant or cafe or pub or bar or hotel or catering service, retail, road transport, school or kindergarten, slaughterhouse, storage, takeaway or fast‐food outlet, temporary mass catering (fairs or festivals), unspecified and wholesale), sampling strategies (objective sampling, census, convenience sampling, selective sampling, suspect sampling and unspecified) and samplers (official sampling, HACCP and own check, industry sampling, official, based on Regulation (EU) 2019/627 and private sampling).
The number of sampling units was obtained by totalling all sampling units (single animals, slaughter animal batches, holdings and herds or flocks), sampling stages at primary production (backyard, border control posts, conservation facilities, farm, hatchery, household, hunting, natural habitat, official kennel, processing plant, retail, slaughterhouse, unspecified, veterinary activities, veterinary clinics, wildlife research station and zoo), sampling strategies (census, convenience sampling, objective sampling, selective sampling, suspect sampling and unspecified) and samplers (HACCP and own check, industry sampling, not applicable, official and industry sampling, official sampling and private sampling).
Food categories
A general increase in the number of sampling units reported in 2022 compared with 2021 was seen for all food categories, and this increase was particularly high for ‘milk and milk products’, ‘fish and fishery products’, ‘eggs and egg products’ and ‘fruits and vegetables (and juices)’ and for this last category, there was also an increase in the number of reporting MSs (Table 8).
Animal categories
For all animal categories, a general decrease in the number of reported sampling units was seen between 2021 and 2022. Moreover, for ‘ducks and geese' and ‘cattle (bovine animals)’, the number of reporting MSs also decreased (Table 8).
More detailed descriptions of the above statistics are provided in the subsections below and in the chapter on foodborne outbreaks.
For a further interactive look at Salmonella monitoring results, dashboards have been created (different filters can be applied to query the data) (here).
2.4.2. Human salmonellosis
In total, 65,208 human salmonellosis cases were reported by 27 MSs in 2022, corresponding to an EU notification rate of 15.3 cases per 100,000 population (Table 9), which was stable when compared with the rate of 2021.
TABLE 9.
Reported confirmed human cases of salmonellosis and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 1192 | 13.3 | 993 | 11.1 | 817 | 9.2 | 1866 | 21.1 | 1538 | 17.4 |
| Belgium b | N | C | 2375 | 24.1 | 2084 | 18.0 | 1595 | 13.8 | 2527 | 22.1 | 2958 | 26.0 |
| Bulgaria | Y | A | 310 | 4.5 | 241 | 3.5 | 187 | 2.7 | 594 | 8.5 | 586 | 8.3 |
| Croatia | Y | C | 1047 | 27.1 | 593 | 14.7 | 786 | 19.4 | 1308 | 32.1 | 1323 | 32.2 |
| Cyprus | Y | C | 66 | 7.3 | 41 | 4.6 | 70 | 7.9 | 62 | 7.1 | 44 | 5.1 |
| Czechia | Y | C | 7563 | 71.9 | 9894 | 92.5 | 10,516 | 98.3 | 13,009 | 122.2 | 10,901 | 102.7 |
| Denmark | Y | C | 898 | 15.3 | 692 | 11.8 | 614 | 10.5 | 1119 | 19.3 | 1168 | 20.2 |
| Estonia | Y | C | 134 | 10.1 | 112 | 8.4 | 91 | 6.8 | 150 | 11.3 | 314 | 23.8 |
| Finland | Y | C | 666 | 12.0 | 474 | 8.6 | 516 | 9.3 | 1175 | 21.3 | 1431 | 26.0 |
| France c | Y | C | 11,162 | 16.4 | 9315 | 28.7 | 7071 | 21.9 | 8935 | 27.7 | 8936 | 27.8 |
| Germany | Y | C | 9064 | 10.9 | 8144 | 9.8 | 8664 | 10.4 | 13,494 | 16.3 | 13,293 | 16.1 |
| Greece | Y | C | 640 | 6.1 | 284 | 2.7 | 381 | 3.6 | 643 | 6.0 | 640 | 6.0 |
| Hungary | Y | C | 3249 | 33.5 | 3298 | 33.9 | 2964 | 30.3 | 4452 | 45.6 | 4161 | 42.6 |
| Ireland | Y | C | 340 | 6.7 | 173 | 3.5 | 214 | 4.3 | 347 | 7.1 | 352 | 7.3 |
| Italy d | Y | C | 3302 | 5.6 | 1776 | 3.0 | 2713 | 4.5 | 3256 | 5.4 | 3635 | 6.0 |
| Latvia | Y | C | 90 | 4.8 | 218 | 11.5 | 296 | 15.5 | 438 | 22.8 | 409 | 21.1 |
| Lithuania | Y | C | 234 | 8.3 | 281 | 10.1 | 419 | 15.0 | 736 | 26.3 | 779 | 27.7 |
| Luxembourg | Y | C | 161 | 24.9 | 133 | 21.0 | 93 | 14.9 | 131 | 21.3 | 135 | 22.4 |
| Malta | Y | C | 199 | 38.2 | 249 | 48.2 | 176 | 34.2 | 131 | 26.5 | 116 | 24.4 |
| Netherlands e | N | C | 1027 | 9.1 | 862 | 7.7 | 695 | 6.2 | 1197 | 10.8 | 1061 | 9.6 |
| Poland | Y | C | 6054 | 16.1 | 7708 | 20.4 | 5192 | 13.7 | 8373 | 22.0 | 9064 | 23.9 |
| Portugal | Y | C | 412 | 4.0 | 361 | 3.5 | 262 | 2.5 | 432 | 4.2 | 302 | 2.9 |
| Romania | Y | C | 1010 | 5.3 | 518 | 2.7 | 408 | 2.1 | 1383 | 7.1 | 1410 | 7.2 |
| Slovakia | Y | C | 3669 | 67.5 | 4439 | 81.3 | 3385 | 62.0 | 4992 | 91.6 | 6791 | 124.8 |
| Slovenia | Y | C | 384 | 18.2 | 185 | 8.8 | 214 | 10.2 | 362 | 17.4 | 274 | 13.3 |
| Spain f | N | C | 8832 | 25.5 | 6168 | 17.8 | 3526 | – | 5087 | – | 8730 | – |
| Sweden | Y | C | 1128 | 10.8 | 933 | 9.0 | 825 | 8.0 | 1990 | 19.5 | 2041 | 20.2 |
| EU Total 27 | 65,208 | 15.3 | 60,169 | 15.3 | 52,690 | 12.1 | 78,189 | 18.0 | 82,392 | 18.2 | ||
| United Kingdom | – | – | – | – | – | – | – | – | 9718 | 14.6 | 9466 | 14.3 |
| EU Total g | 65,208 | 15.3 | 60,169 | 15.3 | 52,690 | 12.1 | 87,907 | 17.5 | 91,858 | 17.6 | ||
| Iceland | Y | C | 42 | 11.2 | 53 | 14.4 | 32 | 8.8 | 50 | 14.0 | 63 | 18.1 |
| Norway | Y | C | 712 | 13.1 | 389 | 7.2 | 441 | 8.2 | 1092 | 20.5 | 961 | 18.1 |
| Liechtenstein | Y | C | 5 | 12.7 | 7 | 17.9 | 1254 | 14.5 | 1534 | 17.9 | 1463 | 17.2 |
| Switzerland h | Y | C | 1838 | 21.0 | 1479 | 17.1 | ||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
In 2022, notification rates calculated with an estimated population coverage of 85%.
Sentinel system until 2021; notification rates calculated with an estimated population coverage of 48%. For 2022, voluntary system with population coverage of 100%.
According to data published in EUOHZ 2021 (EFSA and ECDC, 2022), Italy reported 3768 confirmed cases in 2021, corresponding to 6.4 cases per 100,000 population.
Sentinel system; notification rates calculated with an estimated population coverage of 64%.
Sentinel system; notification rates calculated with an estimated population coverage of 73% in 2021–2022. No information on estimated coverage in 2018–2020, so notification rate cannot be estimated.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
As in the previous year, the highest notification rates in 2022 were reported by Czechia (71.9 cases per 100,000 population) and Slovakia (67.5 cases per 100,000 population), while the lowest rates were reported by Bulgaria, Greece, Italy, Latvia, Portugal and Romania (≤ 6.1 cases per 100,000 population).
The proportion of domestic versus travel‐associated cases varied markedly between countries, but most of the confirmed salmonellosis cases were acquired in the EU (62.3%), representing a decrease compared with 2021 (72.8%), whereas 5.0% reported travel outside the EU and 32.7% of infections were of unknown origin (Table 8). A decrease was observed when comparing the cases acquired in the EU with the median for the years 2018–2020 (67.2%). Considering all cases in EU MSs for which information on importation status of the cases was available, the highest proportions of domestic cases (99–100%) were reported by Croatia, Hungary, Latvia, Malta, Poland, Romania, Slovakia and Spain. The highest proportions of travel‐associated cases with known data were reported by three countries: Finland (50.7%), Denmark (39.8%) and Sweden (39.6%).
Of 4135 travel‐associated cases with known information on the probable country of infection, 77.8% involved travel outside the EU. Türkiye, Egypt, Morocco and Thailand were the most frequently reported travel destinations outside the EU (24.8%, 11.2%, 7.0% and 5.3%, respectively). For travel‐associated cases in the EU, the most common countries of infection were Spain and Italy.
A seasonal trend was observed for confirmed salmonellosis cases in the EU in 2013–2022, with more cases reported during summer months (Figure 2). In 2022, a slight increase in notified human cases was registered compared with 2021. Notwithstanding, the overall trend for salmonellosis in 2018–2022 did not show any significant increase or decrease.
FIGURE 2.
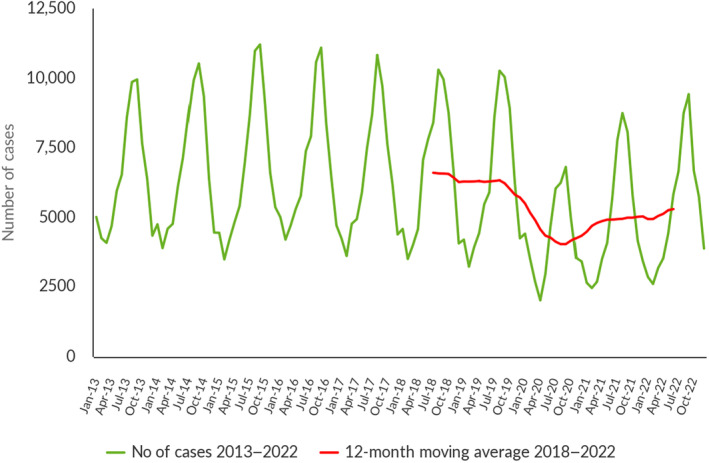
Trend in reported confirmed human cases of non‐typhoidal salmonellosis in the EU by month, 2018–2022. Source: Austria, Belgium, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Luxembourg, Latvia, Malta, the Netherlands, Poland, Portugal, Romania, Spain, Slovakia, Slovenia and Sweden.
Denmark, Germany, Finland, Latvia and Sweden reported a significantly decreasing trend (p < 0.05) in the last 5 years (2018–2022). No MSs reported a significantly increasing trend (p < 0.05).
Seventeen MSs provided information on hospitalisation for 29,003 cases (44.5%) at the EU level. Among these, the proportion of hospitalised cases was 38.9%, which was higher than in 2021. The highest proportions of hospitalised cases were reported in Cyprus, Greece, as in previous years and Romania. All these countries also reported low notification rates (5.3%–7.3%) for salmonellosis, which may suggest that the surveillance systems in these countries primarily capture the most severe cases. Within different specimen types, higher proportions of hospitalised cases were confirmed from cerebrospinal fluid (CSF) (100%, one sample), blood (85.6%) and pus (54.5%) compared to the non‐hospitalised cases. Though, the most common specimen type among the hospitalised patients were faeces samples (87%) among the 16 countries reporting this information.
Seventeen EU MSs provided data on the outcome of salmonellosis, accounting for 56.5% of confirmed cases. Among these, nine countries reported 81 fatal cases, resulting in an EU case fatality rate of 0.22%. The highest percentage of fatal cases (7.2%) was registered for blood infections.
2.4.3. Salmonella in food
Data collected in the context of regulation (ec) no 2073/2005
In the present report underpinned by 2022 data reported by MSs, requirements from the Official Controls Regulation (EU) 2017/625 (OCR) have been introduced for the first time. Unlike in previous legislation, competent authorities (CAs) must use methods complying with relevant internationally recognised rules or protocols including those that the European Committee for Standardization (CEN) has accepted. This condition is met when EN ISO methods, which are ISO methods recognised by CEN, are used. Consequently, and unlike in previous legislation, CAs cannot use alternative methods mentioned in Commission Regulation (EC) No 2073/2005 when they carry out official controls aimed at verifying the correct implementation of the provisions of this Regulation by FBOs. The implementation of this change in legislative testing requirements may have impacted the results of 2022 official food control samples taken in the context of Commission Regulation (EC) No 2073/2005, as compared with the results of similar samples in 2021 and before, when requirements from the OCR were not yet implemented in EFSA's zoonoses data collection. For this reason, the above‐mentioned results should be interpreted with caution.
Food safety criteria
The number of official single samples collected at distribution (N = 30,990 samples, notified by 14 MSs) was higher than that at manufacturing (N = 17,559 samples, notified by 11 MSs), but the proportion of positive samples was slightly higher at the manufacturing stage (3.4%) than at the distribution stage (2.3%) (Table 10).
TABLE 10.
Proportion (%) of Salmonella‐positive samples from official sampling as part of the verification of Salmonella FSC in accordance with Regulation (EC) No 2073/2005, by stage in the food chain, EU, 2022.
| Food matrices | Manufacturing stage (including processing) | Distribution stage (including retail) | ||||
|---|---|---|---|---|---|---|
| N MSs | N tested samples | N (%) positives | N MSs | N tested samples | N (%) positives | |
| Cheeses, butter and cream made from raw milk or milk that has undergone a lower heat treatment than pasteurisation | 9 | 1482 | 1 (0.07) | 6 | 3880 | 2 (0.05) |
| Cooked crustaceans and molluscan shellfish | 3 | 95 | 0 (0) | 8 | 729 | 2 (0.27) |
| Dried follow‐on formulae | – | – | – | 5 | 131 | 1 (0.76) |
| Dried infant formulae and dried dietary foods for special medical purposes intended for infants below 6 months of age | 1 | 60 | 0 (0) | 5 | 1150 | 0 (0) |
| Egg products, excluding products where the manufacturing process or the composition of the product will eliminate the Salmonella risk | 6 | 150 | 6 (4.0) | 5 | 580 | 0 (0) |
| Fresh poultry meat | 8 | 2826 | 198 (7.0) | 10 | 4835 | 337 (7.0) |
| Gelatine and collagen | 1 | 5 | 0 (0) | 7 | 470 | 9 (1.9) |
| Ice cream, excluding products where the manufacturing process or the composition of the product will eliminate the Salmonella risk | 7 | 294 | 1 (0.34) | 7 | 956 | 0 (0) |
| Live bivalve molluscs and live echinoderms, tunicates and gastropods | 3 | 518 | 10 (1.9) | 5 | 1767 | 27 (1.5) |
| Meat products intended to be eaten raw, excluding products where the manufacturing process or the composition of the product will eliminate the Salmonella risk | 7 | 832 | 5 (0.60) | 6 | 1098 | 8 (0.73) |
| Meat products made from poultry meat intended to be eaten cooked | 3 | 3218 | 286 (8.9) | 6 | 367 | 13 (3.5) |
| Mechanically separated meat (MSM) | 6 | 109 | 0 (0) | 4 | 85 | 0 (0) |
| Milk powder and whey powder | 7 | 613 | 0 (0) | 6 | 433 | 0 (0) |
| Minced meat and meat preparations intended to be eaten raw | 1 | 75 | 0 (0) | 6 | 340 | 5 (1.5) |
| Minced meat and meat preparations made from other species than poultry intended to be eaten cooked | 8 | 3733 | 41 (1.1) | 12 | 7468 | 206 (2.8) |
| Minced meat and meat preparations made from poultry meat intended to be eaten cooked | 8 | 3442 | 55 (1.6) | 12 | 2334 | 116 (5.0) |
| Pre‐cut fruit and vegetables (ready‐to‐eat) | 3 | 39 | 0 (0) | 7 | 2460 | 0 (0) |
| Ready‐to‐eat foods containing raw egg, excluding products where the manufacturing process or the composition of the product will eliminate the Salmonella risk | 1 | 15 | 0 (0) | 1 | 490 | 0 (0) |
| Sprouted seeds (ready‐to‐eat) | 2 | 28 | 0 (0) | 5 | 240 | 1 (0.42) |
| Unpasteurised fruit and vegetable juices (ready‐to‐eat) | 2 | 25 | 0 (0) | 5 | 1177 | 0 (0) |
| EU Total a | 11 | 17,559 | 603 (3.4) | 14 | 30,990 | 727 (2.3) |
Abbreviation: MSs, Member States.
Data on food and animal samples from the United Kingdom (Northern Ireland) were taken into account in 2022. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
‘Meat products made from poultry meat intended to be eaten cooked’ was by far the matrix with the highest Salmonella prevalence (8.9% at manufacturing stage), as it had been in 2021 (10.0% at manufacturing stage). Next came ‘fresh poultry meat’, which was the food category with the second highest Salmonella prevalence (7.0% at both stages), and for this matrix, an increase in the prevalence was seen compared with 2021, when the prevalence of positive samples had been 3.1% and 6.5% at manufacturing and distribution level, respectively.
For a further interactive look at Salmonella monitoring results, dashboards have been created (different filters can be applied to query the data) (here).
Process hygiene criteria
Considering data on Salmonella from carcases of different species, irrespective of the sampler, the prevalence values found for neck skin samples from broilers and turkeys were much higher than those reported for carcase surfaces of ruminants (cattle, sheep and goats) and horses.
Pig carcases
Considering all PHC monitoring data from pig carcases collected at the slaughterhouse after dressing but before chilling sent by a total of 24 MSs and the United Kingdom (Northern Ireland), the overall proportion of Salmonella‐positive samples based on official controls (CA) was 2.1% and was significantly higher than that based on own checks (FBOp) (1.1%) (Table 11). The same finding was true considering overall data from the 11 MSs that reported data collected by both the CA (2.7%) and the FBOp (0.83%) and was specifically confirmed for nine MSs (Belgium, Estonia, Greece, Ireland, Italy, Malta, the Netherlands, Poland and Spain).
TABLE 11.
Comparisons of proportions (%) of Salmonella‐positive single samples from pig carcases after dressing, but before chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 4416 | 0 | [0; 0.08] b | – | – |
| Belgium | 826 | 44 (5.3) | [3.9; 7.1] | 2031 | 33 (1.6) | [1.1; 2.3] | < 0.001 | CA > FBOp |
| Bulgaria | 2190 | 0 | [0; 0.17] b | 375 | 0 | [0; 0.98] b | NS | |
| Croatia | 1677 | 11 (0.66) | [0.33; 1.2] | – | – | – | – | – |
| Cyprus | 5 | 0 | [−] | – | – | – | – | – |
| Czechia | 4641 | 35 (0.75) | [0.53; 1.0] | – | – | – | – | – |
| Denmark | – | – | – | 10,677 | 90 (0.84) | [0.68; 1.0] | – | – |
| Estonia | 359 | 22 (6.1) | [3.9; 9.1] | 1734 | 4 (0.23) | [0.06; 0.59] | < 0.001 | CA > FBOp |
| France | – | – | – | 12,301 | 496 (4.0) | [3.7; 4.4] | – | – |
| Germany | – | – | – | 18,147 | 101 (0.56) | [0.45; 0.68] | – | – |
| Greece | 135 | 9 (6.7) | [3.1; 12.3] | 617 | 0 | [0; 0.60] b | < 0.001 | CA > FBOp |
| Hungary | 2653 | 28 (1.1) | [0.70; 1.5] | – | – | – | – | – |
| Ireland | 234 | 10 (4.3) | [2.1; 7.7] | 2230 | 36 (1.6) | [1.1; 2.2] | 0.0093 | CA > FBOp |
| Italy | 5103 | 247 (4.8) | [4.3; 5.5] | 9851 | 92 (0.93) | [0.75; 1.1] | < 0.001 | CA > FBOp |
| Latvia | – | – | – | 534 | 2 (0.38) | [0.04; 1.3] | – | – |
| Luxembourg | – | – | – | 375 | 4 (1.1) | [0.29; 2.7] | – | – |
| Malta | 60 | 16 (26.7) | [16.1; 39.7] | 175 | 12 (6.9) | [3.6; 11.7] | < 0.001 | CA > FBOp |
| Netherlands | 286 | 24 (8.4) | [5.5; 12.2] | 7130 | 156 (2.2) | [1.9; 2.6] | < 0.001 | CA > FBOp |
| Poland | 8696 | 69 (0.79) | [0.62; 1.0] | 25,569 | 11 (0.04) | [0.02; 0.08] | < 0.001 | CA > FBOp |
| Portugal | – | – | – | 9328 | 96 (1.0) | [0.83; 1.3] | – | – |
| Romania | 2227 | 3 (0.14) | [0.03; 0.39] | 3654 | 1 (0.03) | [0; 0.15] | NS | |
| Slovakia | – | – | – | 2629 | 0 | [0; 0.14] b | – | – |
| Slovenia | – | – | – | 980 | 0 | [0; 0.38] b | – | – |
| Spain | 1200 | 127 (10.6) | [8.9; 12.5] | 3350 | 128 (3.8) | [3.2; 4.5] | < 0.001 | CA > FBOp |
| United Kingdom (Northern Ireland) | – | – | – | 610 | 10 (1.6) | [0.79; 3.0] | – | – |
| EU Total (27 + XI) | 30,292 | 645 (2.1) | [2.0; 2.3] | 116,713 | 1272 (1.1) | [1.0; 1.2] | < 0.001 | CA > FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 21,316 | 571 (2.7) | [2.5; 2.9] | 56,716 |
473 (0.83) |
[0.76; 0.91] | < 0.001 | CA > FBOp |
Abbreviations: –, Data not reported; [–], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Finland, Sweden and Norway, which are countries with special guarantees in relation to Salmonella on pig carcases (according to Regulation (EC) No 853/2004 21 ), reported the following monitoring results: 1 positive out of 2329 own‐check samples taken by the FBOp (0.04%) in Finland, 0 positive out of 2968 official samples in Norway and 0 positive out of 6740 official samples in Sweden. Moreover, Switzerland reported 0 positive out of 1190 samples collected by the FBOp.
Broiler carcases
The overall proportion of Salmonella‐positive PHC neck skin samples collected at the slaughterhouse from broiler carcases after chilling based on official controls was 11.7%, which was significantly higher than that based on own checks (2.6%) (Table 12). Similarly, for the eight MSs that reported data collected by both samplers, the overall proportion of Salmonella–positive samples detected by the CA (11.8%) was significantly higher than that reported by the FBOp (4.6%), and this finding was specifically confirmed for five MSs (Belgium, Greece, Italy, Poland and Romania).
TABLE 12.
Comparisons of proportions (%) of Salmonella‐positive single samples from broiler carcases (neck skin samples) after chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 1023 | 190 (18.6) | [16.2; 21.1] | – | – |
| Belgium | 579 | 59 (10.2) | [7.8; 12.9] | 2792 | 106 (3.8) | [3.1; 4.6] | < 0.001 | CA > FBOp |
| Bulgaria | 13 | 0 | [0; 24.7] b | – | – | – | – | – |
| Croatia | 1035 | 117 (11.3) | [9.4; 13.4] | – | – | – | – | – |
| Cyprus | 205 | 35 (17.1) | [12.2; 22.9] | – | – | – | – | – |
| Czechia | 950 | 70 (7.4) | [5.8; 9.2] | – | – | – | – | – |
| Denmark | – | – | – | 230 | 2 (0.87) | [0.1; 3.1] | – | – |
| Estonia | – | – | – | 10,540 | 0 | [0; 0.04] b | – | – |
| France | – | – | – | 15,806 | 263 (1.7) | [1.5; 1.9] | – | – |
| Germany | – | – | – | 10,131 | 139 (1.4) | [1.2; 1.6] | – | – |
| Greece | 90 | 32 (35.6) | [25.7; 46.3] | 2245 | 4 (0.18) | [0.05; 0.46] | < 0.001 | CA > FBOp |
| Hungary | 697 | 96 (13.8) | [11.3; 16.6] | – | – | – | – | – |
| Ireland | – | – | – | 1165 | 15 (1.3) | [0.72; 2.1] | – | – |
| Italy | 1352 | 421 (31.1) | [28.7; 33.7] | 5696 | 504 (8.8) | [8.1; 9.6] | < 0.001 | CA > FBOp |
| Latvia | 100 | 0 | [0; 3.6] b | 599 | 11 (1.8) | [0.92; 3.3] | NS | |
| Malta | 15 | 13 (86.7) | [59.5; 98.3] | – | – | – | – | – |
| Netherlands | 314 | 23 (7.3) | [4.7; 10.8] | 3563 | 226 (6.3) | [5.6; 7.2] | NS | |
| Poland | 8008 | 748 (9.3) | [8.7; 10.0] | 2947 | 72 (2.4) | [1.9; 3.1] | < 0.001 | CA > FBOp |
| Portugal | – | – | – | 2713 | 0 | [0; 0.14] b | – | – |
| Romania | 563 | 48 (8.5) | [6.4; 11.1] | 3190 | 0 | [0; 0.12] b | < 0.001 | CA > FBOp |
| Slovakia | – | – | – | 292 | 2 (0.69) | [0.08; 2.5] | – | – |
| Slovenia | – | – | – | 851 | 26 (3.1) | [2.0; 4.4] | – | – |
| Spain | 800 | 59 (7.4) | [5.7; 9.4] | 1900 | 140 (7.4) | [6.2; 8.6] | NS | |
| United Kingdom (Northern Ireland) | – | – | – | 255 | 0 | [0; 1.4] b | – | – |
| EU Total (27 + XI) | 14,721 | 1721 (11.7) | [11.2; 12.2] | 65,938 | 1700 (2.6) | [2.5; 2.7] | < 0.001 | CA > FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 11,806 | 1390 (11.8) | [11.2; 12.4] | 22,932 | 1063 (4.6) | [4.4; 4.9] | < 0.001 | CA > FBOp |
Abbreviation: –, Data not reported.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Finland and Sweden, which are countries with special guarantees in relation to Salmonella on broiler carcases (according to Regulation (EC) No 853/2004), reported the following monitoring results: Finland (N = 1300 collected by the FBOp) and Sweden (N = 2150 collected by the CA) did not report any positive samples. Moreover, Switzerland reported 3 positive out of 761 samples (0.39%) and Montenegro 0 positive out of 50 samples tested by the FBOp.
Turkey carcases
The overall percentage of Salmonella‐positive PHC neck skin samples collected at the slaughterhouse from turkey carcases after chilling based on official controls was 8.3% and was significantly higher than the percentage based on own‐check samples collected by the FBOp (1.8%) (Table 13). The same finding was true considering the overall proportion of positive samples for the five MSs that reported data from both samplers, and this finding was specifically confirmed for three MSs (Italy, Poland and Spain).
TABLE 13.
Comparisons of proportions (%) of Salmonella‐positive single samples from turkey carcases (neck skin samples) after chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 136 | 0 | [0; 2.7] b | – | – |
| Belgium | 49 | 0 | [0; 7.3] b | 140 | 0 | [0; 2.6] b | NS | |
| Croatia | 5 | 0 | [−] | – | – | – | – | – |
| Czechia | 465 | 3 (0.64) | [0.13; 1.9] | – | – | – | – | – |
| France | – | – | – | 3152 | 17 (0.54) | [0.31; 0.86] | – | – |
| Germany | – | – | – | 2311 | 25 (1.1) | [0.70; 1.6] | – | – |
| Greece | – | – | – | 55 | 0 | [0; 6.5] b | – | – |
| Hungary | 695 | 33 (4.7) | [3.3; 6.6] | – | – | – | – | – |
| Ireland | – | – | – | 670 | 0 | [0; 0.55] b | – | – |
| Italy | 267 | 92 (34.5) | [28.8; 40.5] | 1250 | 131 (10.5) | [8.8; 12.3] | < 0.001 | CA > FBOp |
| Latvia | – | – | – | 11 | 0 | [0; 28.5] b | – | – |
| Poland | 655 | 43 (6.6) | [4.8; 8.7] | 335 | 1 (0.30) | [0.01; 1.7] | < 0.001 | CA > FBOp |
| Portugal | – | – | – | 919 | 2 (0.22) | [0.03; 0.78] | – | – |
| Romania | 18 | 0 | [0; 18.5] b | 280 | 0 | [0; 1.3] b | NS | |
| Slovakia | – | – | – | 60 | 0 | [0; 6.0] b | – | – |
| Slovenia | – | – | – | 403 | 6 (1.5) | [0.55; 3.2] | – | – |
| Spain | 100 | 17 (17.0) | [10.2; 25.8] | 250 | 0 | [0; 1.5] b | < 0.001 | CA > FBOp |
| United Kingdom (Northern Ireland) | – | – | – | 5 | 0 | [−] | – | – |
| EU Total (27 + XI) | 2254 | 188 (8.3) | [7.2; 9.6] | 9977 | 182 (1.8) | [1.6; 2.1] | < 0.001 | CA > FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 1089 | 152 (14.0) | [12.0; 16.2] | 2255 | 132 (5.9) | [4.9; 6.9] | < 0.001 | CA > FBOp |
Abbreviation: –, Data not reported; [−], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Finland, Sweden and Norway are countries with special guarantees in relation to Salmonella on turkey carcases (according to Regulation (EC) No 853/2004). Finland (N = 266 collected by the FBOp) and Sweden (N = 76 collected by the CA) did not report any positive samples, whereas Norway did not report any data for turkey carcases. Moreover, Switzerland reported 0 positive out of 120 tested turkey samples collected by the FBOp.
Bovine carcases
The overall percentage of Salmonella‐positive PHC samples from bovine carcases collected at the slaughterhouse after dressing but before chilling based on official controls was 0.69% and was significantly higher than that based on own checks conducted by the FBOp (0.26%) (Table 14). The same finding was true considering the overall proportion of positive samples for the nine MSs that reported data from both samplers (0.96% collected by the CA and 0.44% collected by the FBOp) and this finding was specifically confirmed for Estonia, Italy and the Netherlands.
TABLE 14.
Comparisons of proportions (%) of Salmonella‐positive single samples from bovine carcases after dressing but before chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 2879 | 1 (0.04) | [0; 0.19] | – | – |
| Belgium | 1116 | 5 (0.45) | [0.15; 1.0] | 3331 | 10 (0.30) | [0.14; 0.55] | NS | |
| Bulgaria | 512 | 0 | [0; 0.72] b | 60 | 0 | [0; 6.0] b | NS | |
| Croatia | 1599 | 4 (0.25) | [0.07; 0.64] | – | – | – | – | – |
| Czechia | 4034 | 13 (0.32) | [0.17; 0.55] | – | – | – | – | – |
| Denmark | – | – | – | 4272 | 5 (0.12) | [0.04; 0.27] | – | – |
| Estonia | 211 | 3 (1.4) | [0.29; 4.1] | 1275 | 0 | [0; 0.29] b | 0.0028 | CA > FBOp |
| France | – | – | – | 19,017 | 34 (0.18) | [0.12; 0.25] | – | – |
| Germany | – | – | – | 3489 | 10 (0.29) | [0.14; 0.53] | – | – |
| Greece | 114 | 0 | [0; 3.2] b | 344 | 0 | ] b | NS | |
| Hungary | 302 | 2 (0.66) | [0.08; 2.4] | – | – | – | – | – |
| Ireland | – | – | – | 6875 | 1 (0.01) | [0; 0.08] | – | – |
| Italy | 2825 | 50 (1.8) | [1.3; 2.3] | 10,784 | 60 (0.56) | [0.42; 0.72] | < 0.001 | CA > FBOp |
| Latvia | – | – | – | 1760 | 0 | [0; 0.21] b | – | – |
| Luxembourg | – | – | – | 285 | 0 | [0; 1.3] b | – | – |
| Malta | – | – | – | 175 | 9 (5.1) | [2.4; 9.5] | – | – |
| Netherlands | 276 | 6 (2.2) | [0.8; 4.7] | 3100 | 27 (0.87) | [0.58; 1.3] | 0.0479 | CA > FBOp |
| Poland | 524 | 1 (0.19) | [0; 1.1] | 1666 | 0 | [0; 0.22] b | NS | |
| Portugal | – | – | – | 3677 | 16 (0.44) | [0.25; 0.71] | – | – |
| Romania | 1802 | 0 | [0; 0.20] b | 2960 | 0 | [0; 0.12] b | NS | |
| Slovakia | – | – | – | 2079 | 0 | [0; 0.18] b | – | – |
| Slovenia | – | – | – | 1746 | 0 | [0; 0.21] b | – | – |
| Spain | 750 | 13 (1.7) | [0.93; 2.9] | 750 | 11 (1.5) | [0.73; 2.6] | NS | |
| United Kingdom (Northern Ireland) | – | – | – | 1603 | 1 (0.06) | [0; 0.35] | – | – |
| EU Total (27 + XI) | 14,065 | 97 (0.69) | [0.56; 0.84] | 72,127 | 185 (0.26) | [0.22; 0.30] | < 0.001 | CA > FBOp |
|
EU Total (27 + XI) providing CA and FBOp data |
8130 | 78 (0.96) | [0.76; 1.2] | 24,270 | 108 (0.44) | [0.36; 0.54] | < 0.001 | CA > FBOp |
Abbreviation: –, Data not reported.
One‐sided, 97.5% confidence interval.
p‐value: NS, not significant.
Finland, Sweden and Norway are countries with special guarantees in relation to Salmonella on bovine carcases (according to Regulation (EC) No 853/2004). Finland (N = 2291 collected by the FBOp) and Sweden (N = 3996 collected by the CA) did not report any positive samples, whereas Norway reported 1 positive out of 3081 tested samples collected by the CA (0.03%). Moreover, Switzerland reported 1 positive sample out of 1125 (0.09%) and Montenegro 0 positive out of 166 tested samples collected by the FBOp.
Sheep carcases
The overall percentage of Salmonella‐positive PHC samples from sheep carcases collected at the slaughterhouse after dressing but before chilling based on official controls was 0.63% and was higher, but not significantly, than that based on own checks (0.53%) (Table 15). Considering the seven MSs providing both CA and FBOp data, the overall percentage of positive samples based on official controls (0.75%) was significantly higher than that based on own checks (0.13%), and this finding was specifically confirmed for Italy and the Netherlands.
TABLE 15.
Comparisons of proportions (%) of Salmonella‐positive single samples from sheep carcases after dressing but before chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 250 | 0 | [0; 1.5] b | – | – |
| Belgium | 349 | 2 (0.57) | [0.07; 2.1] | 1007 | 2 (0.20) | [0.02; 0.72] | NS | – |
| Bulgaria | 419 | 0 | [0; 0.88] b | 45 | 0 | [0; 7.9] b | NS | – |
| Croatia | 1264 | 6 (0.48) | [0.17; 1.0] | – | – | – | – | – |
| Cyprus | 5 | 1 (20.0) | [−] | – | – | – | – | – |
| Czechia | 426 | 3 (0.70) | [0.14; 2.0] | – | – | – | – | – |
| Estonia | – | – | – | 171 | 0 | [0; 2.1] b | – | – |
| Finland | – | – | – | 57 | 0 | [0; 6.3] b | – | – |
| France | – | – | – | 6709 | 66 (0.98) | [0.76; 1.2] | – | – |
| Germany | – | – | – | 525 | 0 | [0; 0.70] b | – | – |
| Greece | 126 | 0 | [0; 2.9] b | 457 | 0 | [0; 0.80] b | NS | |
| Hungary | 212 | 0 | [0; 1.7] b | – | – | – | – | – |
| Ireland | – | – | – | 1748 | 1 (0.06) | [0; 0.32] | – | – |
| Italy | 402 | 4 (1.0) | [0.27; 2.5] | 1958 | 4 (0.20) | [0.06; 0.52] | 0.0328 | CA > FBOp |
| Latvia | – | – | – | 161 | 0 | [0; 2.3] b | – | – |
| Malta | – | – | – | 144 | 6 (4.2) | [1.5; 8.8] | – | – |
| Netherlands | 136 | 9 (6.6) | [3.1; 12.2] | 315 | 0 | [0; 1.2] b | < 0.001 | CA > FBOp |
| Poland | 31 | 0 | [0; 11.2] b | 20 | 0 | [0; 16.8] b | NS | – |
| Portugal | – | – | – | 2444 | 16 (0.66) | [0.38; 1.1] | – | – |
| Romania | 526 | 0 | [0; 0.70] b | 803 | 0 | [0; 0.46] b | NS | – |
| Slovakia | – | – | – | 334 | 0 | [0; 1.1] b | – | – |
| Slovenia | – | – | – | 152 | 0 | [0; 2.4] b | – | – |
| Spain | 100 | 0 | [0; 3.6] b | – | – | – | – | – |
| United Kingdom (Northern Ireland) | – | – | – | 520 | 0 | [0; 0.71] b | – | – |
| EU Total (27 + XI) | 3996 | 25 (0.63) | [0.41; 0.92] | 17,820 | 95 (0.53) | [0.43; 0.65] | NS | |
| EU Total (27 + XI) providing CA and FBOp data | 1989 | 15 (0.75) | [0.42; 1.2] | 4605 | 6 (0.13) | [0.05; 0.28] | < 0.001 | CA > FBOp |
Abbreviation: –, Data not reported; [−], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Moreover, Switzerland reported 0 positive out of 250 tested samples collected by the FBOp.
Goat carcases
The overall percentage of Salmonella‐positive PHC samples from goat carcases collected at the slaughterhouse after dressing but before chilling based on own checks was 1.7% and was significantly higher than that based on official controls (0.28%) (Table 16).
TABLE 16.
Comparisons of proportions (%) of Salmonella‐positive single samples from goat carcases after dressing but before chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 12 | 0 | [0; 26.5] b | – | – |
| Belgium | 105 | 0 | [0; 3.5] b | 51 | 0 | [0; 7.0] b | NS | |
| Croatia | 195 | 0 | [0; 1.9] b | – | – | – | – | – |
| Czechia | 66 | 0 | [0; 5.4] b | – | – | – | – | – |
| France | – | – | – | 229 | 12 (5.2) | [2.7; 9.0] | – | – |
| Germany | – | – | – | 5 | 0 | [−] | – | – |
| Greece | 43 | 0 | [0; 8.2] b | 23 | 0 | [0; 14.8] b | NS | |
| Italy | 87 | 0 | [0; 4.2] b | 167 | 0 | [0; 2.2] b | NS | |
| Latvia | – | – | – | 21 | 0 | [0; 16.1] b | – | – |
| Malta | – | – | – | 31 | 2 (6.5) | [0.79; 21.4] | – | – |
| Netherlands | 102 | 2 (2.0) | [0.24; 6.9] | 5 | 0 | [−] | – | – |
| Poland | 10 | 0 | [0; 30.9] b | – | – | – | – | – |
| Portugal | – | – | – | 834 | 9 (1.1) | [0.5; 2.0] | – | – |
| Slovakia | – | – | – | 2 | 0 | [−] | – | – |
| Slovenia | – | – | – | 10 | 0 | [0; 30.9] b | – | – |
| Spain | 100 | 0 | [0; 3.6] b | – | – | – | – | – |
| EU Total (27 + XI) | 708 | 2 (0.28) | [0.03; 1.0] | 1390 | 23 (1.7) | [1.1; 2.5] | 0.0031 | CA < FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 337 | 2 (0.59) | [0.07; 2.1] | 246 | 0 | [0; 1.5] b | NS | |
Abbreviation: –, Data not reported.
p–value: NS, not significant.
One–sided, 97.5% confidence interval.
Horse carcases
The overall percentage of Salmonella‐positive PHC samples from horse carcases collected at the slaughterhouse after dressing but before chilling based on official controls was 0.52% and was not significantly higher than that based on FBOp own checks (0.25%) (Table 17).
TABLE 17.
Comparisons of proportions (%) of Salmonella‐positive single samples from horse carcases before chilling, by sampler and reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N Tested samples | N (%) positive samples | CI95 | N Tested samples | N (%) positive samples | CI95 | |||
| Austria | – | – | – | 1 | 0 | [−] | – | – |
| Belgium | 35 | 0 | [0; 10.0] b | 53 | 0 | [0; 6.7] b | NS | |
| Croatia | 21 | 0 | [0; 16.1] b | – | – | – | – | – |
| Czechia | 5 | 0 | [−] | – | – | – | – | – |
| France | – | – | – | 54 | 0 | [0; 6.6] b | – | – |
| Germany | – | – | – | 9 | 0 | [−] | – | – |
| Ireland | – | – | – | 63 | 0 | [0; 5.7] b | – | – |
| Italy | 171 | 2 (1.2) | [0.14; 4.2] | 352 | 1 (0.28) | [0.01; 1.6] | NS | |
| Latvia | – | – | – | 2 | 0 | [−] | – | – |
| Netherlands | – | – | – | 23 | 0 | [0; 14.8] b | – | – |
| Poland | 45 | 0 | [0; 7.9] b | – | – | – | – | – |
| Portugal | – | – | – | 30 | 0 | [0; 11.6] b | – | – |
| Romania | 111 | 0 | [0; 3.3] b | 138 | 0 | [0; 2.6] b | NS | |
| Slovenia | – | – | – | 34 | 0 | [0; 10.3] b | – | – |
| Spain | – | – | – | 50 | 1 (2.0) | [0.05; 10.6] | – | – |
| EU Total (27 + XI) | 388 | 2 (0.52) | [0.06; 1.9] | 809 | 2 (0.25) | [0.03; 0.89] | NS | |
| EU Total (27 + XI) providing CA and FBOp data | 317 | 2 (0.63) | [0.08; 2.3] | 543 | 1 (0.18) | [0; 1.0] | NS | |
Abbreviations: –, Data not reported; [−], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
For a further interactive look at Salmonella monitoring results, dashboards have been created (different filters can be applied to query the data) (here).
Occurrence in food
Monitoring data reported for food samples, which do not fit with the criteria described in the previous paragraphs, were described by merging investigations from all sampling stages (primary production, manufacturing, distribution and others), all samplers except ‘HACCP and own checks’ and ‘private sampling’, and all sampling units (single, batch and slaughter animal batch). Only sampling units collected through ‘objective sampling’ were considered in this context. For an interactive look at summary statistics for the Salmonella monitoring results with regard to major food categories sorted as RTE and non‐RTE food, dashboards have been created (here).
RTE food and non‐RTE food
For 2022, 99,341 RTE and 521,917 non‐RTE food sampling units were reported from 25 and 28 MSs with very low (0.16%) and low (2.1%) proportions of positive sampling units, respectively.
Within the category of RTE food, the vast majority of the sampled matrices had very low proportions of Salmonella‐positive sampling units, with the exception of ‘meat and meat products from broilers’ and ‘spices and herbs’, for which the prevalence of positive sampling units was low (1.4%; N = 584 and 1.1%; N = 1309, respectively).
Within the category of non‐RTE food, the highest percentages of positive sampling units were reported for ‘meat and meat products from broilers’ (5.1%; N = 99,022), ‘meat and meat products from turkeys’ (3.3%; N = 13,867), ‘other meat and meat products’ (2.0%; N = 115,068), ‘mixed meat and meat products’ (1.6%; N = 10,439) and ‘meat and meat products from pigs’ (1.3%; N = 159,738). Some Salmonella isolates were also reported for ‘eggs and egg products’ (0.65%; N = 7988), ‘fish and fishery products’ (0.61%; N = 14,094) and ‘meat and meat products from bovine animals’ (0.43%; N = 92,993).
Comparing the results for the year 2022 and the 4‐year period of 2018–2021, a slight decrease in the overall percentage of Salmonella‐positive RTE food sampling units was noted during the last year (0.16%) compared with the previous ones (0.28%); on the other hand, for non‐RTE food, the overall percentage remained stable over the years (2.2%). No major differences in contamination were noted over the years for specific food matrices.
Fresh meat
For fresh meat, in 2022, 1.9% of sampling units (N = 425,097) were positive for Salmonella. Within this category, the highest percentages of positive units were reported for ‘fresh meat from broilers’ (N = 88,702, 4.6%) and ‘fresh meat from turkeys’ (N = 12,764, 3.3%); these rates were both lower than the proportions of positive samples reported in the previous years.
2.4.4. Salmonella in animals
For a further interactive look at Salmonella monitoring results, dashboards have been created (different filters can be applied to query the data) (here).
Poultry monitoring data in accordance with the national control programmes for Salmonella
Achievement of Salmonella reduction targets
Breeding flocks of Gallus gallus
In total, 25 MSs, the United Kingdom (Northern Ireland), and 3 non‐MSs reported Salmonella NCP data for breeding flocks of G. gallus. Luxembourg and Malta do not have such flocks. In the EU in 2022, considering merged data from the CA and FBOp, Salmonella was found in 290 (2.1%, ranging from 0% to 10.2%) of the 13,526 flocks tested, compared with 2.5% and 2.0% for 2021 and 2020, respectively. In 2022, the prevalence of flocks that were positive for any of the five target serovars was 0.84% (ranging from 0% to 2.9%) and it increased compared with 2021 and 2019 (0.58% and 0.52%, respectively). All reporting countries, except Croatia, Czechia, Greece and Poland, met the flock prevalence target of 1% maximum (Figure 3). The most frequently reported target serovar was S. Enteritidis (EU flock prevalence of 0.58%, 79 positive flocks), with 53 flocks (67.1%) reported by Poland. The total number of S. Enteritidis‐positive breeding flocks (79) increased compared with 2021 (54 positive flocks) and 2020 (29 positive flocks). S. Typhimurium (including the monophasic variant) and S. Infantis were the second most commonly reported target serovars, with 16 positive flocks each. For S. Infantis, the number of positive breeding flocks was 6 in 2021 and 11 in 2020. With regard to the other target serovars, two flocks tested positive for S. Virchow (0.01%) and no flocks tested positive for S. Hadar (Table 18).
FIGURE 3.
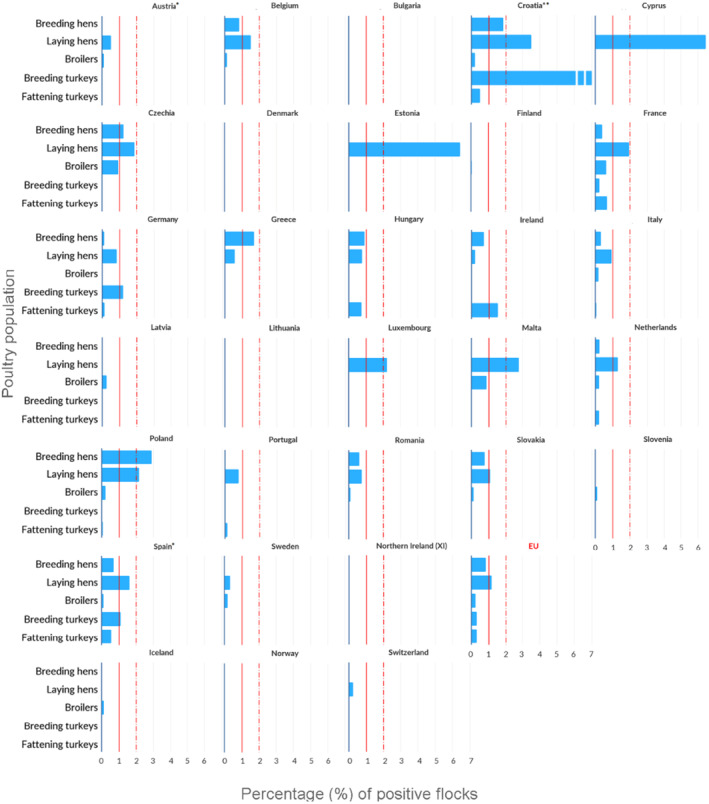
Prevalence of poultry flocks (breeding flocks of Gallus gallus, laying hens, broilers, breeding turkeys and fattening turkeys) positive for target Salmonella serovars, EU MSs and non‐MS countries, 2022. Note: Vertical bars indicate the target to be reached, which was set at 1% for all poultry populations with the exception of laying hens, for which it was 2%. For laying hens, according to Reg. (EU) No 517/2011, Poland and Luxembourg reached the reduction target (Article 1 (a): reduction of prevalence of 10% compared to previous year for Poland; Article 1 (b): one adult flock can remain positive for MSs with less than 50 flocks, for Luxembourg). For breeding turkeys, according to Reg. (EU) No 1190/2012, Croatia and Spain reached the reduction target (Article 1: one adult flock can remain positive for MSs with less than 100 flocks). *Austria amended the data for laying hens and for broilers in the last phase of the preparation of the present report. The prevalence of positive flocks for target Salmonella serovars was 0.50% instead of 0.53% (laying hens) and 0.11% instead of 0.13% (broilers). Spain amended the data for breeding Gallus gallus in the last phase of the preparation of the present report. The prevalence of positive flocks for target serovars was 0.36% instead of 0.71%. **Croatia reported having tested one breeding turkey flock, which was found positive for target Salmonella serovars (100%).
TABLE 18.
Salmonella in breeding flocks of Gallus gallus during the production period (all types of breeding flocks, flock‐based data) in countries running control programmes in accordance with Regulation (EC) No 2160/2003, 2022.
| Country |
N tested Flocks |
N (%) positive for Salmonella spp. | N (%) positive for target serovars | N (%) positive flocks for | ||||
|---|---|---|---|---|---|---|---|---|
| S. Enteritidis | S. Typhimurium a | S. Hadar | S. Infantis | S. Virchow | ||||
| Austria | 180 | 1 (0.56) | 0 | 0 | 0 | 0 | 0 | 0 |
| Belgium | 594 | 9 (1.5) | 5 (0.84) | 2 (0.34) | 2 (0.34) | 0 | 1 (0.17) | 0 |
| Bulgaria | 185 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Croatia | 108 | 2 (1.9) | 2 (1.9) | 0 | 1 (0.93) | 0 | 1 (0.93) | 0 |
| Cyprus | 31 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | 639 | 10 (1.6) | 8 (1.3) | 8 (1.3) | 0 | 0 | 0 | 0 |
| Denmark | 228 | 3 (1.3) | 0 | 0 | 0 | 0 | 0 | 0 |
| Estonia | 8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland | 157 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | 1452 | 18 (1.2) | 6 (0.41) | 2 (0.14) | 2 (0.14) | 0 | 2 (0.14) | 0 |
| Germany | 796 | 6 (0.75) | 1 (0.13) | 0 | 1 (0.13) | 0 | 0 | 0 |
| Greece | 235 | 24 (10.2) | 4 (1.7) | 0 | 0 | 0 | 3 (1.3) | 1 (0.43) |
| Hungary | 543 | 5 (0.92) | 5 (0.92) | 3 (0.55) | 1 (0.18) | 0 | 1 (0.18) | 0 |
| Ireland | 139 | 1 (0.72) | 1 (0.72) | 1 (0.72) | 0 | 0 | 0 | 0 |
| Italy | 1197 | 43 (3.6) | 4 (0.33) | 2 (0.17) | 1 (0.08) | 0 | 1 (0.08) | 0 |
| Latvia | 37 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Lithuania | 55 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | 1608 | 5 (0.31) | 4 (0.25) | 3 (0.19) | 1 (0.06) | 0 | 0 | 0 |
| Poland | 1964 | 64 (3.3) | 57 (2.9) | 53 (2.7) | 2 (0.10) | 0 | 2 (0.10) | 0 |
| Portugal | 509 | 1 (0.20) | 0 | 0 | 0 | 0 | 0 | 0 |
| Romania | 489 | 6 (1.2) | 3 (0.61) | 2 (0.41) | 0 | 0 | 1 (0.20) | 0 |
| Slovakia | 129 | 1 (0.78) | 1 (0.78) | 0 | 0 | 0 | 1 (0.78) | 0 |
| Slovenia | 128 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Spain | 1681 | 91 (5.4) | 12 (0.71) b | 3 (0.18) | 5 (0.30) | 0 | 3 (0.18) | 1 (0.06) |
| Sweden | 155 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| United Kingdom (Northern Ireland) | 279 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EU Total (27 + XI) | 13,526 | 290 (2.1) | 113 (0.84) b | 79 (0.58) | 16 (0.12) | 0 | 16 (0.12) | 2 (0.01) |
| Iceland | 60 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway | 223 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Switzerland | 139 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Salmonella Typhimurium, including monophasic Salmonella Typhimurium with the antigenic formula 1,4,[5],12:i:‐.
Spain amended the data in the last phase of the preparation of the present report. The number of positive flocks for target serovars was 6 instead of 12 with a prevalence of (0.36%). One flock was positive for S. Enteritidis instead of three; three flock was positive for S. Typhimurium, instead of five; one flock was positive for S. Infantis instead of three.
Flocks of laying hens
All MSs, the United Kingdom (Northern Ireland), and three non‐MSs reported Salmonella NCP data for laying hen flocks. Considering merged data from the CA and FBOp, Salmonella was found in 1306 flocks (3.4%, ranging from 0% to 21.5%), compared with 1323 (3.3%) in 2021. The EU prevalence of laying hen flocks that were positive for either of the two target serovars was 1.2% (ranging from 0% to 6.5%), which was comparable with 2021, when 1.3% of tested flocks were positive for target serovars.
Four MSs (Croatia, Cyprus, Estonia and Malta) did not meet the reduction target of 2% or less (Figure 3). The most frequently reported target serovar was S. Enteritidis (EU flock prevalence of 0.89%), with 80.6% of 340 S. Enteritidis‐positive flocks reported by six MSs. France alone accounted for 28.8% (98 positive flocks) of the S. Enteritidis‐positive flocks notified; this situation was similar to that in the previous years (28.0% in 2021 and 29.2% in 2020). For S. Typhimurium (including the monophasic variant), 114 positive flocks were reported (EU flock prevalence of 0.30%) and the majority (57.0%) were reported by France (35 positive flocks) and Germany (30 positive flocks) Table 19).
TABLE 19.
Salmonella in laying hen flocks of Gallus gallus during the production period (flock‐based data) in countries running control programmes in accordance with Regulation (EC) No 2160/2003, 2022.
| Country | N tested flocks | N (%) positive for Salmonella spp. | N (%) positive for target serovars | N (%) positive flocks for | |
|---|---|---|---|---|---|
| S. Enteritidis | S. Typhimurium a | ||||
| Austria | 3386 | 44 (1.3) | 18 (0.53) b | 9 (0.27) | 9 (0.27) |
| Belgium | 659 | 30 (4.6) | 10 (1.5) | 10 (1.5) | 0 |
| Bulgaria | 245 | 4 (1.6) | 0 | 0 | 0 |
| Croatia | 285 | 36 (12.6) | 10 (3.5) | 8 (2.8) | 2 (0.70) |
| Cyprus | 124 | 17 (13.7) | 8 (6.5) | 8 (6.5) | 0 |
| Czechia | 475 | 11 (2.3) | 9 (1.9) | 5 (1.1) | 4 (0.84) |
| Denmark | 418 | 1 (0.24) | 0 | 0 | 0 |
| Estonia | 31 | 2 (6.5) | 2 (6.5) | 0 | 2 (6.5) |
| Finland | 576 | 0 | 0 | 0 | 0 |
| France | 6739 | 309 (4.6) | 133 (2.0) | 98 (1.5) | 35 (0.52) |
| Germany | 7009 | 94 (1.3) | 59 (0.84) | 29 (0.41) | 30 (0.43) |
| Greece | 845 | 40 (4.7) | 5 (0.59) | 4 (0.47) | 1 (0.12) |
| Hungary | 905 | 7 (0.77) | 7 (0.77) | 5 (0.55) | 2 (0.22) |
| Ireland | 465 | 1 (0.22) | 1 (0.22) | 0 | 1 (0.22) |
| Italy | 4312 | 284 (6.6) | 41 (0.95) | 36 (0.84) | 5 (0.12) |
| Latvia | 58 | 0 | 0 | 0 | 0 |
| Lithuania | 47 | 0 | 0 | 0 | 0 |
| Luxembourg | 45 | 1 (2.2) | 1 (2.2) c | 1 (2.2) | 0 |
| Malta | 107 | 23 (21.5) | 3 (2.8) | 2 (1.9) | 1 (0.94) |
| Netherlands | 2688 | 46 (1.7) | 35 (1.3) | 34 (1.3) | 1 (0.04) |
| Poland | 2078 | 84 (4.0) | 45 (2.2) c | 42 (2.0) | 3 (0.14) |
| Portugal | 500 | 19 (3.8) | 4 (0.80) | 4 (0.80) | 0 |
| Romania | 792 | 22 (2.8) | 6 (0.76) | 4 (0.50) | 2 (0.25) |
| Slovakia | 274 | 3 (1.1) | 3 (1.1) | 3 (1.1) | 0 |
| Slovenia | 274 | 9 (3.3) | 0 | 0 | 0 |
| Spain | 3140 | 211 (6.7) | 51 (1.6) | 35 (1.1) | 16 (0.51) |
| Sweden | 872 | 4 (0.46) | 3 (0.34) | 3 (0.34) | 0 |
| United Kingdom (Northern Ireland) | 788 | 4 (0.51) | 0 | 0 | 0 |
| EU Total (27 + XI) | 38,137 | 1306 (3.4) | 454 (1.2) b | 340 (0.89) | 114 (0.30) |
| Iceland | 41 | 0 | 0 | 0 | 0 |
| Norway | 887 | 0 | 0 | 0 | 0 |
| Switzerland | 804 | 2 (0.25) | 2 (0.25) | 1 (0.12) | 1 (0.12) |
Salmonella Typhimurium, including monophasic Salmonella Typhimurium with the antigenic formula 1,4,[5],12:i:‐.
Austria amended the data in the last phase of the preparation of the present report. The number of positive flocks for target serovars was 17 instead of 18 with a prevalence of (0.50%). One flock was positive for both S. Typhimurium and monophasic S. Typhimurium.
For laying hens, according to Reg. (EU) No 517/2011, Poland and Luxembourg reached the reduction target (Article 1 (a): reduction of prevalence of 10% compared to previous year for Poland; Article 1 (b): one adult flock can remain positive for MSs with less than 50 flocks, for Luxemburg).
Broiler flocks
All MSs, the United Kingdom (Northern Ireland), and three non‐MSs reported Salmonella NCP data for broiler flocks. Considering merged data from the CA and FBOp, Salmonella was found in 3.5% (10,747 flocks; ranging from 0% to 21.3%) of the tested flocks, compared with 3.8% in 2021 and 3.9% in 2020. The EU prevalence of broiler flocks positive for either of the two target Salmonella serovars was 0.25%, corresponding to 763 flocks (ranging from 0% to 0.96%), which was similar to the prevalence in previous years (0.28% in 2021 and 0.25% in 2020). All MSs met the target of 1% or less of broiler flocks positive for S. Enteritidis and/or S. Typhimurium, including its monophasic variant (Figure 3), unlike the previous year, when three countries did not meet the target. Regarding the EU prevalence of the two target serovars, in 2022, S. Enteritidis accounted for 59.6% of flocks positive for target serovars, whereas S. Typhimurium (including its monophasic variant) accounted for 40.4%. France and Poland accounted for 64.6% of all the EU flocks positive for S. Enteritidis, and France alone accounted for 63.0% of all the EU broiler flocks positive for S. Typhimurium (Table 20).
TABLE 20.
Salmonella in broiler flocks of Gallus gallus before slaughter (flock‐based data) in countries running control programmes in accordance with Regulation (EC) No 2160/2003, 2022.
| Country | N tested flocks | N (%) positive for salmonella spp. | N (%) positive for target serovars | N (%) positive flocks for | |
|---|---|---|---|---|---|
| S. Enteritidis | S. Typhimurium a | ||||
| Austria | 6155 | 169 (2.7) | 8 (0.13) b | 2 (0.03) | 6 (0.10) |
| Belgium | 11,076 | 233 (2.1) | 17 (0.15) | 3 (0.03) | 14 (0.13) |
| Bulgaria | 557 | 0 | 0 | 0 | 0 |
| Croatia | 2844 | 86 (3.0) | 6 (0.21) | 6 (0.21) | 0 |
| Cyprus | 1014 | 14 (1.4) | 0 | 0 | 0 |
| Czechia | 4797 | 78 (1.6) | 46 (0.96) | 45 (0.94) | 1 (0.02) |
| Denmark | 3680 | 6 (0.16) | 1 (0.03) | 0 | 1 (0.03) |
| Estonia | 705 | 0 | 0 | 0 | 0 |
| Finland | 4017 | 2 (0.05) | 2 (0.05) | 0 | 2 (0.05) |
| France | 59,129 | 1440 (2.4) | 377 (0.64) | 183 (0.31) | 194 (0.33) |
| Germany | 26,282 | 228 (0.87) | 9 (0.03) | 5 (0.02) | 4 (0.01) |
| Greece | 8504 | 13 (0.15) | 3 (0.04) | 2 (0.02) | 1 (0.01) |
| Hungary | 7119 | 2 (0.03) | 2 (0.03) | 1 (0.01) | 1 (0.01) |
| Ireland | 3295 | 13 (0.40) | 1 (0.03) | 1 (0.03) | 0 |
| Italy | 27,049 | 5766 (21.3) | 55 (0.20) | 45 (0.17) | 10 (0.04) |
| Latvia | 749 | 11 (1.5) | 2 (0.27) | 1 (0.13) | 1 (0.13) |
| Lithuania | 137 | 0 | 0 | 0 | 0 |
| Luxembourg | 9 | 1 (11.1) | 0 | 0 | 0 |
| Malta | 453 | 21 (4.6) | 4 (0.88) | 0 | 4 (0.88) |
| Netherlands | 15,547 | 497 (3.2) | 35 (0.22) | 25 (0.16) | 10 (0.06) |
| Poland | 48,868 | 223 (0.46) | 112 (0.23) | 111 (0.23) | 1 (< 0.01) |
| Portugal | 10,315 | 20 (0.19) | 4 (0.04) | 0 | 4 (0.04) |
| Romania | 14,078 | 293 (2.1) | 14 (0.10) | 10 (0.07) | 4 (0.03) |
| Slovakia | 2775 | 33 (1.2) | 4 (0.14) | 4 (0.14) | 0 |
| Slovenia | 2508 | 353 (14.1) | 3 (0.12) | 0 | 3 (0.12) |
| Spain | 38,352 | 1229 (3.2) | 50 (0.13) | 11 (0.03) | 39 (0.10) |
| Sweden | 4047 | 9 (0.22) | 8 (0.20) | 0 | 8 (0.20) |
| United Kingdom (Northern Ireland) | 6404 | 7 (0.11) | 0 | 0 | 0 |
| EU Total (27 + XI) | 310,465 | 10,747 (3.5) | 763 (0.25) b | 455 (0.15) | 308 (0.10) |
| Iceland | 685 | 12 (1.8) | 1 (0.15) | 0 | 1 (0.15) |
| Norway | 4679 | 0 | 0 | 0 | 0 |
| Switzerland | 633 | 0 | 0 | 0 | 0 |
Salmonella Typhimurium, including monophasic Salmonella Typhimurium with the antigenic formula 1,4,[5],12:i:‐.
Austria amended the data in the last phase of the preparation of the present report. The number of positive flocks for target serovars was seven instead of eight with a prevalence of (0.11%). One flock was positive for both S. Typhimurium and monophasic S. Typhimurium.
Regulation (EU) No 200/2012 22 requires that MSs separately report the results obtained by the FBOp and the CA for broiler flocks. Most MSs (22) and the United Kingdom (Northern Ireland) reported both the overall merged results collected as part of the NCP and separate results from the CA and FBOp investigations, for their broiler flocks. Two MSs, Bulgaria and Hungary, reported only data collected by the CA. Three MSs (Croatia, Lithuania and the Netherlands) did not comply (Figure 3), as in the previous year. Considering all the data sent by the MSs providing data from both the CA and the FBOp, the EU flock prevalence of target Salmonella serovars based on CA sampling was 2.9% (N = 5713), which was significantly higher than that based on FBOp sampling (0.20%, N = 280,780). The flock prevalence of target Salmonella serovars in broilers obtained by the CA was also significantly higher for Czechia, France, Germany, Greece, Ireland, Italy, Poland, Romania and Spain. For the remaining reporting MSs, the differences between the results obtained by the two samplers were not significant, or the sample sizes for one or both samplers were too small to be analysed (Table 21).
TABLE 21.
Comparisons of the prevalence of target Salmonella serovar‐positive broiler flocks, by sampler and by reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N tested flocks | N (%) flocks positive for target serovars | CI95 | N tested flocks | N (%) flocks positive for target serovars | CI95 | |||
| Austria | 123 | 1 (0.81) | [0.02; 4.4] | 6041 | 7 (0.12) | [0.05; 0.24] | NS | |
| Belgium | 86 | 0 | [0; 4.2] b | 11,064 | 17 (0.15) | [0.09; 0.25] | NS | |
| Bulgaria | 20 | 0 | [0; 16.8] b | – | – | – | – | – |
| Cyprus | 9 | 0 | [−] | 1014 | 0 | [0; 0.36] b | – | – |
| Czechia | 38 | 2 (5.3) | [0.64; 17.7] | 4762 | 44 (0.92) | [0.67; 1.2] | 0.0508 | CA > FBOp |
| Denmark | 275 | 0 | [0; 1.3] b | 3680 | 1 (0.03) | [0; 0.15] | NS | |
| Estonia | 203 | 0 | [0; 1.8] b | 437 | 0 | [0; 0.84] b | NS | |
| Finland | 506 | 0 | [0; 0.73] b | 3511 | 2 (0.06) | [0.01; 0.21] | NS | |
| France | 417 | 13 (3.1) | [1.7; 5.3] | 58,712 | 364 (0.62) | [0.56; 0.69] | < 0.001 | CA > FBOp |
| Germany | 265 | 3 (1.1) | [0.23; 3.3] | 26,280 | 6 (0.02) | [0.01; 0.05] | < 0.001 | CA > FBOp |
| Greece | 87 | 3 (3.4) | [0.72; 9.7] | 8503 | 0 | [0; 0.04] b | < 0.001 | CA > FBOp |
| Hungary | 7119 | 0 | [0; 0.05] b | – | – | – | – | – |
| Ireland | 99 | 1 (1.0) | [0.03; 5.5] | 3295 | 1 (0.03) | [0; 0.17] | 0.0575 | CA > FBOp |
| Italy | 872 | 44 (5.0) | [3.7; 6.7] | 26,961 | 11 (0.04) | [0.02; 0.07] | < 0.001 | CA > FBOp |
| Latvia | 6 | 1 (16.7) | [−] | 744 | 1 (0.13) | [0; 0.75] | – | – |
| Luxembourg | 3 | 0 | [−] | 9 | 0 | [−] | – | – |
| Malta | 6 | 2 (33.3) | [−] | 447 | 2 (0.45) | [0.05; 1.6] | – | – |
| Poland | 1516 | 89 (5.9) | [4.7; 7.2] | 47,352 | 23 (0.05) | [0.03; 0.07] | < 0.001 | CA > FBOp |
| Portugal | 110 | 0 | [0; 3.3] b | 10,315 | 4 (0.04) | [0.01; 0.10] | NS | |
| Romania | 358 | 2 (0.56) | [0.07; 2.0] | 13,720 | 12 (0.09) | [0.04; 0.15] | 0.048 | CA > FBOp |
| Slovakia | 34 | 0 | [0; 10.3] b | 2741 | 2 (0.07) | [0.01; 0.26] | NS | |
| Slovenia | 33 | 0 | [0; 10.6] b | 2475 | 3 (0.12) | [0.03; 0.35] | NS | |
| Spain | 458 | 7 (1.5) | [0.62; 3.1] | 38,312 | 44 (0.12) | [0.08; 0.15] | < 0.001 | CA > FBOp |
| Sweden | 163 | 0 | [0; 2.2] b | 4047 | 8 (0.20) | [0.09; 0.39] | NS | |
| United Kingdom (Northern Ireland) | 46 | 0 | [0; 7.7] b | 6358 | 0 | [0; 0.06] b | NS | |
| EU Total (27 + XI) | 12,852 | 168 (1.3) | [1.1; 1.5] | 280,780 | 552 (0.20) | [0.18; 0.21] | < 0.001 | CA > FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 5713 | 168 (2.9) | [2.5; 3.4] | 280,780 | 552 (0.20) | [0.18; 0.21] | < 0.001 | CA > FBOp |
Abbreviation: –, Data not reported; [−], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Breeding flocks of turkeys
For breeding turkeys, 13 MSs and 2 non‐MSs reported Salmonella NCP data. Considering merged data from the CA and FBOp, Salmonella was found in 54 of the 1266 flocks tested (4.3%), compared with 3.9% in 2021 and 5.1% in 2020. In 2022, the prevalence of flocks positive for either of the two target Salmonella serovars was 0.32% (four positive flocks), compared with 0.49% and 0.48% in 2021 and 2020, respectively. All MSs met the reduction target of 1% or less of breeding flocks of turkeys positive for S. Enteritidis and/or S. Typhimurium (including its monophasic variant) (Figure 3, Table 22).
TABLE 22.
Salmonella in breeding flocks of turkeys during the production period (flock‐based data) in countries running control programmes in accordance with Regulation (EC) No 2160/2003, 2022.
| Country | N tested flocks | N (%) positive for Salmonella spp. | N (%) positive for target serovars | N (%) positive flocks for | |
|---|---|---|---|---|---|
| S. Enteritidis | S. Typhimurium a | ||||
| Bulgaria | 2 | 0 | 0 | 0 | 0 |
| Croatia | 1 | 1 (100.0) | 1 (100.0) b | 1 (100.0) | 0 |
| Finland | 7 | 0 | 0 | 0 | 0 |
| France | 422 | 15 (3.6) | 1 (0.24) | 0 | 1 (0.24) |
| Germany | 82 | 2 (2.4) | 1 (1.2) | 0 | 1 (1.2) |
| Greece | 10 | 0 | 0 | 0 | 0 |
| Hungary | 129 | 0 | 0 | 0 | 0 |
| Ireland | 4 | 0 | 0 | 0 | 0 |
| Italy | 283 | 32 (11.3) | 0 | 0 | 0 |
| Poland | 191 | 0 | 0 | 0 | 0 |
| Slovakia | 42 | 0 | 0 | 0 | 0 |
| Spain | 89 | 4 (4.5) | 1 (1.1) b | 0 | 1 (1.1) |
| Sweden | 4 | 0 | 0 | 0 | 0 |
| EU Total (27 + XI) | 1266 | 54 (4.3) | 4 (0.32) | 1 (0.08) | 3 (0.24) |
| Iceland | 3 | 0 | 0 | 0 | 0 |
| Norway | 15 | 0 | 0 | 0 | 0 |
Salmonella Typhimurium, including monophasic Salmonella Typhimurium with the antigenic formula 1,4,[5],12:i:‐.
For breeding turkeys, according to Reg. (EU) No 1190/2012, Croatia and Spain reached the reduction target (Article 1: one adult flock can remain positive for MSs with less than 100 flocks).
In accordance with Regulation (EC) No 1190/2012, 23 Salmonella NCP monitoring data for breeding turkey flocks must be reported separately for sampling performed by the CA and the FBOp, in addition to the overall merged data. Nine MSs complied with this requirement, whereas four MSs did not report separate results from the CA and FBOp (Bulgaria, Croatia, Hungary and Poland). Considering all the data sent by those MSs that provided data from both samplers (CA and FBOp), the EU prevalence of target Salmonella serovar‐positive flocks based on CA sampling was 0.28% (N = 354), which was similar to that based on FBOp sampling (0.34%, N = 875) (Table 23).
TABLE 23.
Comparisons of the prevalence of target Salmonella serovar‐positive flocks of breeding turkeys, by sampler and by reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N tested flocks | N (%) flocks positive for target serovars | CI95 | N tested flocks | N (%) flocks positive for target serovars | CI95 | |||
| Finland | 7 | 0 | [−] | 7 | 0 | [−] | – | – |
| France | 42 | 0 | [0; 8.4] b | 349 | 1 (0.29) | [0.01; 1.6] | NS | |
| Germany | 67 | 1 (1.5) | [0.04; 8.0] | 82 | 1 (1.2) | [0.03; 6.6] | NS | |
| Greece | 3 | 0 | [−] | 10 | 0 | [0; 30.9] b | – | – |
| Ireland | 4 | 0 | [−] | 4 | 0 | [−] | – | – |
| Italy | 132 | 0 | [0; 2.8] b | 283 | 0 | [0; 1.3] b | NS | |
| Slovakia | 42 | 0 | [0; 8.4] b | 47 | 0 | [0; 7.5] b | NS | |
| Spain | 53 | 0 | [0; 6.7] b | 89 | 1 (1.1) | [0.03; 6.1] | NS | |
| Sweden | 4 | 0 | [−] | 4 | 0 | [−] | – | – |
| EU Total (27 + XI) | 354 | 1 (0.28) | [0.01; 1.6] | 875 | 3 (0.34) | [0.07; 1.0] | NS | |
| EU Total (27 + XI) providing CA and FBOp data | 354 | 1 (0.28) | [0.01; 1.6] | 875 | 3 (0.34) | [0.07; 1.0] | NS | |
Abbreviations: –, Data not reported; [−], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Flocks of fattening turkeys
For fattening turkey flocks, 23 MSs, the United Kingdom (Northern Ireland), and 3 non‐MSs provided data. In the EU in 2022, considering merged data from the CA and FBOp, Salmonella was found in 2825 (9.2%, ranging from 0% to 42.5%) fattening turkey flocks, compared with 9.1% and 8.8% in 2021 and 2020, respectively. The EU prevalence of flocks positive for either of the two target Salmonella serovars was 0.32% (ranging from 0% to 1.5%), compared with 0.31% in 2021 and 0.38% in 2020. Ireland did not meet the reduction target of 1% (Figure 3). The EU flock prevalence was higher for S. Typhimurium (and its monophasic variant) (0.23%, 70 flocks) than for S. Enteritidis (0.09%, 27 flocks), which was very similar to the previous year. Three MSs (France, Spain and Hungary) accounted for 82.9% of all the EU fattening turkey flocks positive for S. Typhimurium (and its monophasic variant), and France alone accounted for 51.9% of all the EU fattening turkey flocks positive for S. Enteritidis (Table 24).
TABLE 24.
Salmonella in fattening flocks of turkeys before slaughter during the production period (flock‐based data) in countries running control programmes in accordance with Regulation (EC) No 2160/2003, 2022.
| Country | N tested flocks | N (%) positive for Salmonella spp. | N (%) positive for target serovars | N (%) positive flocks for | |
|---|---|---|---|---|---|
| S. Enteritidis | S. Typhimurium a | ||||
| Austria | 511 | 4 (0.78) | 0 | 0 | 0 |
| Belgium | 209 | 1 (0.48) | 0 | 0 | 0 |
| Bulgaria | 2 | 0 | 0 | 0 | 0 |
| Croatia | 393 | 15 (3.8) | 2 (0.51) | 1 (0.25) | 1 (0.25) |
| Cyprus | 6 | 1 (16.7) | 0 | 0 | 0 |
| Czechia | 269 | 2 (0.74) | 0 | 0 | 0 |
| Denmark | 132 | 3 (2.3) | 0 | 0 | 0 |
| Finland | 318 | 0 | 0 | 0 | 0 |
| France | 5355 | 189 (3.5) | 37 (0.69) | 14 (0.26) | 23 (0.43) |
| Germany | 4320 | 13 (0.30) | 6 (0.14) | 4 (0.09) | 2 (0.05) |
| Greece | 57 | 0 | 0 | 0 | 0 |
| Hungary | 1732 | 13 (0.75) | 13 (0.75) | 0 | 13 (0.75) |
| Ireland | 455 | 18 (4.0) | 7 (1.5) | 4 (0.88) | 3 (0.66) |
| Italy | 4292 | 1823 (42.5) | 3 (0.07) | 1 (0.02) | 2 (0.05) |
| Lithuania | 9 | 0 | 0 | 0 | 0 |
| Netherlands | 443 | 11 (2.5) | 1 (0.23) | 1 (0.23) | 0 |
| Poland | 6125 | 8 (0.13) | 4 (0.06) | 2 (0.03) | 2 (0.03) |
| Portugal | 1358 | 35 (2.6) | 2 (0.15) | 0 | 2 (0.15) |
| Romania | 282 | 7 (2.5) | 0 | 0 | 0 |
| Slovakia | 118 | 1 (0.85) | 0 | 0 | 0 |
| Slovenia | 107 | 7 (6.5) | 0 | 0 | 0 |
| Spain | 3939 | 674 (17.1) | 22 (0.56) | 0 | 22 (0.56) |
| Sweden | 166 | 0 | 0 | 0 | 0 |
| United Kingdom (Northern Ireland) | 37 | 0 | 0 | 0 | 0 |
| EU Total (27 + XI) | 30,635 | 2825 (9.2) | 97 (0.32) | 27 (0.09) | 70 (0.23) |
| Iceland | 29 | 0 | 0 | 0 | 0 |
| Norway | 292 | 0 | 0 | 0 | 0 |
| Switzerland | 37 | 0 | 0 | 0 | 0 |
Salmonella Typhimurium, including monophasic Salmonella Typhimurium with the antigenic formula 1,4,[5],12:i:‐.
Salmonella NCP monitoring data for fattening turkey flocks must be reported separately for sampling performed by the CA and FBOp, in addition to the overall merged results, as defined in Regulation (EU) No 1190/2012. Eighteen MSs and the United Kingdom (Northern Ireland) complied with the requirement, whereas three MSs (Bulgaria, Croatia and the Netherlands) did not report separate results from the CA and FBOp, and Hungary only reported results from the CA. Considering all the data sent by those MSs that provided data from both samplers (CA and FBOp), the EU prevalence of target Salmonella serovar‐positive flocks based on CA sampling was 2.0% (N = 982), which was significantly higher than that based on FBOp sampling (0.22%, N = 27,673). The same finding was also observed for data provided by France, Germany, Ireland, Italy, Poland and Spain (Table 25).
TABLE 25.
Comparisons of the prevalence of target Salmonella serovar‐positive flocks of fattening turkeys, by sampler and by reporting MS, EU, 2022.
| Country | Competent authority (CA) | Food business operator (FBOp) | p‐value a | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|
| N tested flocks | N (%) flocks positive for target serovars | CI95 | N tested flocks | N (%) flocks positive for target serovars | CI95 | |||
| Austria | 23 | 0 | [0; 14.8] b | 503 | 0 | [0; 0.73] b | NS | |
| Belgium | 4 | 0 | [−] | 209 | 0 | [0; 1.8] b | – | – |
| Cyprus | 2 | 0 | [−] | 5 | 0 | [−] | – | – |
| Czechia | 16 | 0 | [0; 20.6] b | 269 | 0 | [0; 1.4] b | NS | |
| Denmark | 112 | 0 | [0; 3.2] b | 132 | 0 | [0; 2.8] b | NS | |
| Finland | 61 | 0 | [0; 5.9] b | 257 | 0 | [0; 1.4] b | NS | |
| France | 60 | 2 (3.3) | [0.41; 11.5] | 5295 | 35 (0.66) | [0.46; 0.92] | 0.064 | CA > FBOp |
| Germany | 177 | 6 (3.4) | [1.3; 7.2] | 4320 | 0 | [0; 0.09] b | < 0.001 | CA > FBOp |
| Greece | 7 | 0 | [−] | 54 | 0 | [0; 6.6] b | – | – |
| Hungary | 1732 | 0 | [0; 0.21] b | – | – | – | – | – |
| Ireland | 22 | 4 (18.2) | [5.2; 40.3] | 455 | 3 (0.66) | [0.14; 1.9] | < 0.001 | CA > FBOp |
| Italy | 135 | 3 (2.2) | [0.46; 6.4] | 4279 | 0 | [0; 0.09] b | < 0.001 | CA > FBOp |
| Poland | 179 | 3 (1.7) | [0.35; 4.8] | 5946 | 1 (0.02) | [0; 0.09] | < 0.001 | CA > FBOp |
| Portugal | 19 | 0 | [0; 17.6] b | 1358 | 2 (0.15) | [0.02; 0.53] | NS | |
| Romania | 30 | 0 | [0; 11.6] b | 252 | 0 | [0; 1.5] b | NS | |
| Slovakia | 9 | 0 | [−] | 109 | 0 | [0; 3.3] b | – | – |
| Slovenia | 7 | 0 | [−] | 100 | 0 | [0; 3.6] b | – | – |
| Spain | 86 | 2 (2.3) | [0.28; 8.1] | 3931 | 20 (0.51) | [0.31; 0.78] | 0.0794 | CA > FBOp |
| Sweden | 29 | 0 | [0; 11.9] b | 166 | 0 | [0; 2.2] b | NS | |
| United Kingdom (Northern Ireland) | 4 | 0 | [−] | 33 | 0 | [0; 10.6] b | – | – |
| EU Total (27 + XI) | 2714 | 20 (0.74) | [0.45; 1.1; 1.1] | 27,673 | 61 (0.22) | [0.17; 0.28] | < 0.001 | CA > FBOp |
| EU Total (27 + XI) providing CA and FBOp data | 982 | 20 (2.0) | [1.2; 3.1] | 27,673 | 61 (0.22) | [0.17; 0.28] | < 0.001 | CA > FBOp |
Abbreviations: –, Data not reported; [−], The confidence interval is not provided because of the small sample size.
p‐value: NS, not significant.
One‐sided, 97.5% confidence interval.
Salmonella prevalence trends in poultry flocks
Trends in the estimated EU prevalence of poultry flocks positive for Salmonella spp. and target Salmonella serovars, for different poultry populations, since the implementation of the EU‐wide 2007–2022 NCP, are displayed in Figure 4. From 2020, data provided by the United Kingdom were not considered, whereas from 2021, data provided by the United Kingdom (Northern Ireland) were taken into account.
FIGURE 4.
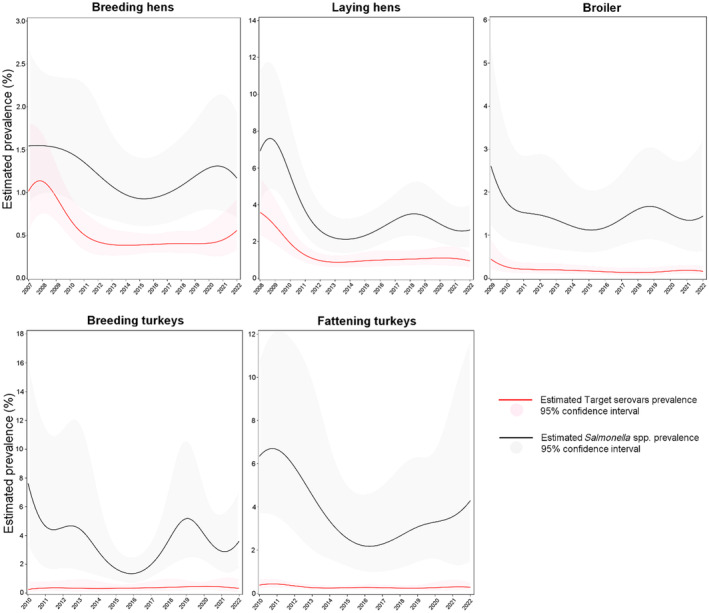
Trend in the estimated prevalence of poultry flocks positive for Salmonella spp. and target Salmonella serovars, at EU level for different poultry populations, 2007–2022.
In the supporting information for this report (‘Salmonella poultry outcome trend analyses’, here), the EU percentages of positive flocks for Salmonella, target and non‐target Salmonella serovars, and S. Enteritidis over time are shown and compared for each poultry population covered by the NCP. Moreover, figures show the modelling of prevalence trends for Salmonella spp. and target Salmonella serovars in poultry flocks. Detailed outputs of trend analyses (at subject level and population level) are reported.
The apparent discrepancy between the proportion of positive flocks (both for target Salmonella serovars and for Salmonella spp., as described in the previous paragraphs) and the estimated prevalence shown below is due to the fact that the first value is the ratio of all positive to all tested flocks, whereas the estimated prevalence is obtained by modelling the ratio of positive to all tested flocks in each reporting country, taking into account inter‐country variability and the correlation between years.
Breeding flocks of Gallus gallus: 2007–2022
Since the beginning of the NCPs, there has been an overall decreasing trend for the prevalence of breeding G. gallus flocks positive for target serovars (Figure 4). The prevalence estimated by modelling decreased from 1% CI95[0.57; 1.8] in 2007 to 0.38% CI95[0.27; 0.54] in 2014, when the estimated prevalence reached its lowest value. Over the next few years, the estimated prevalence slightly increased, reaching 0.56% CI95[0.33; 0.92] in 2022, but this increase was not significant.
The estimated EU prevalence of Salmonella‐positive breeding flocks was 1.5% CI95[0.89; 2.7] in 2007 and then decreased, reaching the minimum value of 0.93% CI95[0.61; 1.4] in 2015. During the following years, it increased slightly to reach 1.3% CI95[0.79; 2.1] in 2021 and decreased to 1.2% CI95[0.71; 1.9] in 2022. This prevalence was not significantly different from that of the previous 2 years or compared with the lowest prevalence estimated in 2015.
Flocks of laying hens: 2008–2022
Since the beginning of the NCPs, there has been an overall decreasing trend for the prevalence of flocks positive for target serovars (Figure 4). The prevalence estimated by modelling was 3.6% CI95[2.4; 5.4] in 2008 and decreased to reach the lowest value of 0.88% CI95[0.63; 1.2] in 2013, with a steep downturn. From 2014 onwards, it increased slightly and stabilised at 0.95% CI95[0.64; 1.4] in 2022. This prevalence was not significantly different from that of the previous 2 years or compared with the lowest prevalence estimated in 2013.
The estimated EU prevalence of Salmonella spp. in laying hen flocks was 6.9% CI95[4.2; 11.1] in 2008 and decreased to 2.1% CI95[1.4; 3.2] in 2014, with a steep downturn. In the following years, it increased and reached 3.5% CI95[2.3; 5.2] in 2018 and then decreased to 2.6% CI95[1.7; 4.0] in 2022. In 2022, the estimated Salmonella prevalence in laying hen flocks was not significantly different from that in the previous 2 years or compared with the lowest and the highest prevalence estimated in 2014 and 2018 after NCP introduction, respectively.
Broiler flocks: 2009–2022
From the beginning of the NCPs, the flock prevalence of target serovars estimated by the model steeply decreased in the first time interval (until 2011) and then further decreased (Figure 4). The estimated prevalence was 0.44% CI95[0.22; 0.88] in 2009 and decreased to 0.16% CI95[0.09; 0.27] in 2022. This prevalence was not significantly different from that in the previous 2 years.
The EU prevalence of Salmonella spp.‐positive broiler flocks estimated by modelling decreased from 2.6% CI95[1.3; 5.3] in 2009 to 1.1% CI95[0.61; 2.0] in 2015 and then increased to 1.4% CI95[0.65; 3.2] in 2022. Nevertheless, the estimated EU prevalence of Salmonella‐positive broiler flocks in 2022 was not significantly different to that of the previous 2 years or that of 2015, when the estimated prevalence reached its lowest value.
Breeding turkey flocks: 2010–2022
From the beginning of the NCPs, the prevalence of target Salmonella serovar‐positive breeding turkey flocks remained rather stable, between 0.26% CI95[0.09; 0.77] and 0.46% CI95[0.28; 0.77], with some slight fluctuations. In 2022, the estimated prevalence was 0.33% CI95[0.12; 0.92] (Figure 4). This trend may have been affected by the low number of MSs with breeding turkey flocks positive for target Salmonella serovars.
With regard to EU‐level Salmonella spp.‐positive breeding turkey flocks, after an initial fluctuation in the EU prevalence from 7.6% CI95[3.5; 15.9] in 2010 to 1.4% CI95[0.75; 2.5] in 2016, when this estimated prevalence reached the lowest value seen in the entire study period, the estimated prevalence increased over time to reach 3.6% CI95[1.8; 7.0] in 2022. This estimated prevalence in 2022 was not significantly different from that of the previous 2 years, but it was significantly higher than the estimated prevalence in 2016 (p‐value = 0.04).
Fattening turkey flocks: 2010–2022
The estimated flock prevalence of target serovars was 0.38% CI95[0.23; 0.61] in 2010; it decreased to 0.24% CI95[0.17; 0.34] in 2014 and then increased to 0.28% CI95[0.17; 0.46] in 2022, after some small temporal fluctuations (Figure 4 Nevertheless, there were no significant differences in the estimated prevalence of the target Salmonella serovars in EU fattening turkey flocks in the last 2 years or compared with the lowest prevalence estimated in 2014.
For this poultry population, after an initial fluctuation in the EU prevalence of Salmonella spp.‐positive flocks from 6.3% CI95[3.7; 10.6] in 2010 to 2.2% CI95[1.0; 4.5] in 2016, when the estimated prevalence reached its lowest value, the prevalence increased to 4.3% CI95[1.5; 11.6] in 2022. Nevertheless, the prevalence in 2022 was not significantly different from that in the previous 2 years or from the lowest estimated prevalence in 2016.
Salmonella data for other animals
Considering all the collected data on the presence of Salmonella in different categories of animal species in the EU, with the exception of data collected in the framework of NCPs for poultry, 61,756 sampling units collected from animals of various species were reported by 18 MSs. The overall prevalence of Salmonella spp.‐positive sampling units was 4.3% (N = 2672). The highest number of sampling units was from cattle (bovine animals) (N = 22,836 notified by 12 MSs), and 3.5% were reported as being positive for Salmonella, as in the previous year. The highest prevalence of positive samples was notified for cats (50.4% for five MSs) and wild boar (10.8% for three MSs). For pigs, based on data reported by 14 MSs, the prevalence of positive sampling units was 0.60% (92 positive samples, N = 15,271). For solipeds, 2.2% of sampling units was positive for Salmonella (11 positive samples) and were notified by seven MSs. These data must be interpreted with caution since the reported prevalence may have been affected by the sampling context and scope. For a further interactive look at Salmonella monitoring results, dashboards have been created (different filters can be applied to query the data) (here).
2.4.5. Salmonella in feed
In 2022, the overall EU‐level occurrence of Salmonella‐positive sampling units in any ‘animal and vegetable‐derived feed’ was 0.53% (N = 77,304). In compound feed (finished feed for animals), the prevalence of Salmonella‐positive units was 0.80% for samples from cattle feed (N = 2859), 0.46% for samples from poultry feed (N = 15,155) and 0.40% for samples from pig feed (N = 3539), with the latter mainly being reported by Poland. There were no noticeable isolates in 2022. The prevalence of Salmonella‐positive sampling units for pet food was 1.71% (N = 2051).
2.4.6. Salmonella serovars in humans, food and animals
Humans
For humans, information on Salmonella serovars was available for 72.3% of the total number of confirmed cases (47,122 cases out of 65,208) for 25 MSs (Bulgaria and Spain did not report serovar data. For Spain, serovar information was not available when the Salmonella serovar data were analysed for this report, but these are shown in the Surveillance Atlas). Data included all cases reported with serovar information regardless of travel status. The proportion of cases of Salmonella with serovar data available decreased compared with 2021 (80.3%) due to delayed reporting from Spain. As in previous years, the three most commonly reported Salmonella serovars in 2022 were S. Enteritidis (54.6%), S. Typhimurium (12.1%) and monophasic S. Typhimurium (1,4,[5],12:i:‐) (10.4%), representing 77.1% of the 47,122 confirmed human cases. S. Enteritidis decreased by 8.2%, when considering the absolute number of cases of this serovar, but it decreased by only 3.4% compared with 2021 with respect to the total number of isolates. Monophasic S. Typhimurium (1,4,[5],12:i:‐) increased by 2.2% compared with 2021, when considering the absolute number of cases of this serovar in these years, but the proportion remained stable compared with 2021 with respect to the total number of isolates in the relative years.
The proportion of these three serovars, mainly driven by S. Enteritidis, increased during the previous 2 years, with a slight decrease in 2022: it rose from 79.6% in 2020 to 80.1% in 2021 and then dropped to 77.1% in 2022. The fourth serovar, S. Infantis, was at the same level as in 2020 and 2019; the fifth serovar, S. Newport, increased in proportion, replacing S. Derby and rising 43.4% compared with 2021 but only 0.36% with respect to the total number of isolates (Table 26).
TABLE 26.
Distribution of reported confirmed cases of human salmonellosis in the EU, 2020–2022, for the 20 most frequent Salmonella serovars in 2022.
| Serovar | 2022 | 2021 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases | MSs | % | Cases | MSs | % | Cases | MSs | % | |
| Enteritidis | 25,737 | 25 | 54.6 | 28,045 | 25 | 58.0 | 24,008 | 25 | 56.1 |
| Typhimurium | 5694 | 25 | 12.1 | 5841 | 25 | 12.1 | 5337 | 25 | 12.5 |
| Monophasic Typhimurium 1,4,[5],12:i:‐ | 4906 | 14 | 10.4 | 4802 | 15 | 9.9 | 4697 | 16 | 11.0 |
| Infantis | 1093 | 25 | 2.3 | 1071 | 25 | 2.2 | 1064 | 23 | 2.5 |
| Newport | 522 | 20 | 1.1 | 364 | 21 | 0.75 | 336 | 21 | 0.79 |
| Derby | 513 | 20 | 1.1 | 489 | 18 | 1.0 | 525 | 20 | 1.2 |
| Napoli | 448 | 14 | 0.95 | 352 | 12 | 0.73 | 412 | 12 | 0.96 |
| Agona | 343 | 19 | 0.73 | 142 | 17 | 0.29 | 157 | 18 | 0.37 |
| Chester | 338 | 17 | 0.72 | 333 | 13 | 0.69 | 129 | 13 | 0.30 |
| Coeln | 333 | 19 | 0.71 | 481 | 16 | 1.00 | 324 | 19 | 0.76 |
| Kentucky | 314 | 17 | 0.67 | 143 | 15 | 0.30 | 154 | 16 | 0.36 |
| Virchow | 276 | 17 | 0.59 | 229 | 17 | 0.47 | 121 | 16 | 0.28 |
| Stanley | 238 | 17 | 0.51 | 205 | 17 | 0.42 | 208 | 21 | 0.49 |
| Bovismorbificans | 226 | 17 | 0.48 | 233 | 15 | 0.48 | 337 | 15 | 0.79 |
| Braenderup | 218 | 15 | 0.46 | 381 | 15 | 0.79 | 93 | 12 | 0.22 |
| Mbandaka | 205 | 14 | 0.44 | 98 | 13 | 0.20 | 68 | 13 | 0.16 |
| Brandenburg | 177 | 16 | 0.38 | 229 | 16 | 0.47 | 309 | 16 | 0.72 |
| Hadar | 173 | 17 | 0.37 | 106 | 14 | 0.22 | 120 | 14 | 0.28 |
| Panama | 167 | 11 | 0.35 | 94 | 10 | 0.19 | 159 | 12 | 0.37 |
| Montevideo | 163 | 15 | 0.35 | 225 | 12 | 0.47 | 102 | 14 | 0.24 |
| Other | 5038 | – | 10.7 | 4456 | – | 9.2 | 4115 | – | 9.62 |
| Total a , b | 47,122 | 25 | 100 | 48,319 | 25 | 100 | 42,775 | 25 | 100 |
Abbreviations: MSs, Member States; –, Data not reported.
Source(s): 2022–25 MSs: Austria, Belgium, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia and Sweden. 2021–25 MSs: Austria, Belgium, Croatia, Cyprus, Czechia, Denmark, Estonia, Germany, Greece, Finland, France, Hungary, Ireland, Italy, Latvia, Lithuania, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain and Sweden. 2020–25 MSs: Austria, Belgium, Croatia, Cyprus, Czechia, Denmark, Estonia, Germany, Greece, Finland, France, Hungary, Ireland, Italy, Latvia, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Sweden and Spain.
Only isolates with the complete antigenic formula and/or serovar name have been considered.
Serovars acquired in the EU
To estimate the impact of Salmonella infections acquired at the EU level, serovar data were analysed for domestic and travel‐associated cases in which the probable country of infection was an EU MS. Information on Salmonella serovars with travel data (importation and/or probable country of infection) was available from 24 MSs, representing 60.1% of cases with known serovar data in 2022. Compared with previous years, one country less (the Netherlands) reported domestic cases in 2022. Most cases (91.7%) with a known serovar and with travel data were infected within the EU. For the travel‐associated cases, the most frequently reported travel destinations in the EU were Spain (25.0%), Italy (10.7%), Croatia (8.8%) and Greece (7.2%). For the reported cases of human salmonellosis acquired in the EU, S. Enteritidis dominated and 67.3% of these reported cases were infected with this serovar. S. Enteritidis, S. Typhimurium and monophasic S. Typhimurium (1,4,[5],12:i:‐) together represented 84.7% of the confirmed human cases acquired in the EU in 2022 (Table 27). S. Enteritidis cases were predominantly (74.1%) infected within the EU. The proportions of cases of S. Enteritidis, S. Typhimurium and its monophasic variant (1,4,[5],12:i:‐) were at the same level as in 2020–2021, when considering the number of these serovars versus the total number of reported serovars. Also, S. Infantis and S. Derby remained approximately at the same level as in 2021, while S. Agona and S. Mbandaka slid up to eighth and eleventh positions, respectively.
TABLE 27.
Distribution of reported cases of human salmonellosis acquired in the EU, 2020–2022, for the six most frequently reported serovars in 2022.
| Serovar | 2022 | 2021 | 2020 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases | MSs | % | Cases | MSs | % | Cases | MSs | % | |
| Enteritidis | 19,079 | 24 | 67.3 | 23,928 | 24 | 69.6 | 21,203 | 23 | 68.7 |
| Typhimurium | 3712 | 23 | 13.1 | 4076 | 24 | 11.9 | 3702 | 22 | 12.0 |
| Monophasic Typhimurium 1,4,[5],12:i:‐ | 1217 | 14 | 4.3 | 1519 | 15 | 4.4 | 1530 | 16 | 5.0 |
| Infantis | 649 | 22 | 2.3 | 667 | 24 | 1.9 | 716 | 21 | 2.3 |
| Derby | 252 | 17 | 0.89 | 249 | 17 | 0.72 | 260 | 17 | 0.84 |
| Coeln | 199 | 16 | 0.70 | 331 | 15 | 0.96 | 201 | 17 | 0.65 |
| Other | 3230 | – | 11.4 | 3607 | – | 10.5 | 3234 | – | 10.5 |
| Total a | 28,338 | 24 | 100.0 | 34,377 | 24 | 100.0 | 30,846 | 23 | 100.0 |
Abbreviations: MSs, Member States; –, Data not reported.
Only isolates with the complete antigenic formula and/or serovar name have been considered.
A seasonal trend was observed for confirmed S. Enteritidis infections acquired in the EU in 2018–2022, with more cases reported during summer months. A decrease in cases was observed in 2020, due to the COVID‐19 pandemic, and in 2022, due to a general decrease in this serovar. Notwithstanding, the overall trend for S. Enteritidis in 2018–2022 did not show any significant increase or decrease Figure 5). Ireland showed a significantly decreasing (p < 0.05) trend in S. Enteritidis infections within the EU over the last 5 years (2018–2022). A significant increasing trend (p < 0.05) was observed in France, Malta and Slovenia.
FIGURE 5.
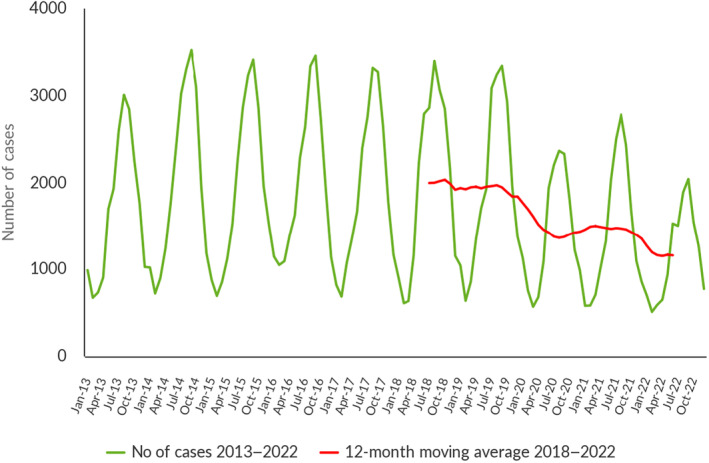
Trend in reported confirmed human cases of S. Enteritidis infections acquired in the EU, by month, 2018–2022. Source: Austria, Belgium, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Malta, Portugal, Slovakia, Slovenia and Sweden.
Food and animals
Descriptive analyses were undertaken using serotyped isolates (isolates with the complete antigenic formula and/or serovar name) from food and animals. In this context, only isolates related to the most common food‐producing animal species and food matrices thereof were considered and were aggregated into the following categories for further analysis: ‘broiler flocks – broiler meat’, ‘laying hen flocks – eggs’, ‘fattening turkey flocks – turkey meat’, ‘fattening pigs – pig meat’ and ‘cattle – bovine meat’. Overall, a selection of 17,848 serotyped Salmonella isolates meeting the aforementioned inclusion criteria were obtained (Table 28).
TABLE 28.
Distribution of Salmonella isolates (number and percentage of positive sampling units) with and without serotype identification among the different selected sources (food and animals), EU, 2022.
| Source | Salmonella‐positive sampling units without serotyped isolates | Salmonella‐positive sampling units with serotyped isolates | ||
|---|---|---|---|---|
| N | % | N | % | |
| Broilers | 1762 | 13.1 | 9028 | 50.6 |
| Broiler meat | 2395 | 17.8 | 4046 | 22.7 |
| Cattle | 8 | 0.06 | 117 | 0.66 |
| Cattle meat | 290 | 2.2 | 230 | 1.3 |
| Pigs | 10 | 0.07 | 14 | 0.08 |
| Pig meat | 7548 | 56.2 | 999 | 5.6 |
| Turkeys | 666 | 5.0 | 2174 | 12.2 |
| Turkey meat | 413 | 3.1 | 204 | 1.1 |
| Layers | 320 | 2.4 | 990 | 5.5 |
| Eggs and egg products | 27 | 0.20 | 46 | 0.26 |
| Total | 13,439 | 100 | 17,848 | 100 |
The large majority of the serotyped isolates were from ‘broilers’ (both animals [50.6%] and food [22.7%]); the percentage of serotyped isolates from broiler meat increased by 38.8% in comparison to 2021. ‘Turkey’ sources (animals and food) accounted for 13.3% of the serotyped isolates, while ‘laying hen’ and ‘pig’ sources represented 5.8% and 5.7% of the serotyped isolates, respectively. Serotyped isolates from ‘cattle' sources made up about 2.0% of the total.
Isolates belonging to the five most frequently reported Salmonella serovars involved in cases of human salmonellosis acquired in the EU in 2022 were considered for further analysis; these serovars were S. Enteritidis, S. Typhimurium, monophasic S. Typhimurium (1,4,[5],12:i:‐), S. Infantis and S. Derby. From the above‐mentioned food‐animal sources, a total of 17,848 serotyped isolates were reported, of which S. Infantis accounted for 38.3%, S. Enteritidis 7.9%, S. Typhimurium 4.0%, monophasic S. Typhimurium (1,4,[5],12:i:‐) 2.4% and S. Derby 2.1%.
A Sankey diagram (Figure 6) illustrates how these top five EU‐level Salmonella serovars involved in human salmonellosis cases acquired in the EU were linked with the major animal species.
FIGURE 6.
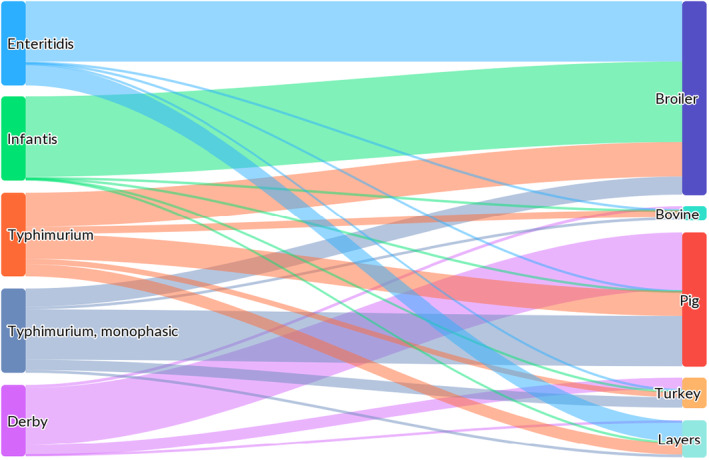
Sankey diagram of the distribution of the top five EU‐level Salmonella serovars involved in human salmonellosis cases acquired in the EU, reported from specified food–animal categories, by food–animal source, EU, 2022. Note: The left side of the diagram shows the five most commonly reported Salmonella serovars involved in human salmonellosis cases acquired in the EU: S. Enteritidis (light blue), S. Infantis (green), S. Typhimurium (orange), monophasic S. Typhimurium (1,4,[5],12:i:‐) (indigo) and S. Derby (violet). Animal and food data from the same source were merged: ‘broiler’ includes isolates from broiler flocks and broiler meat, ‘bovine' includes isolates from bovine animals for meat production and from bovine meat, ‘pig’ includes isolates from fattening pigs and pig meat, ‘turkey’ includes isolates from fattening turkey flocks and turkey meat, and ‘layers’ includes isolates from laying hen flocks and eggs. The right side shows the five sources considered (broilers (blue), bovine animals (light green), pigs (red), turkeys (light orange) and layers (light mint green)). The width of the coloured bands linking the sources and serovars is proportional to the percentage of isolates of each serovar from each source.
S. Enteritidis was primarily related to ‘broiler’ sources (71.7% of the S. Enteritidis isolates were from broiler flocks and meat) and also to ‘layers and eggs’ (24.9%). S. Typhimurium isolates were distributed among the different sources, although they were mainly related to ‘broiler’ and ‘pig’ sources (41.0% and 29.6% of the isolates were from these sources respectively), followed by ‘laying hen’, ‘bovine' and ‘turkey’ sources (14.4%, 8.6% and 6.4%). Monophasic S. Typhimurium (1,4,[5],12:i:‐) was related mainly to ‘pig’ (59.7%) and secondly to ‘broiler’ (21.5%) sources. S. Infantis was strictly related to ‘broiler’ sources (95.6%). S. Derby was primarily related to ‘pig’ (68.2%) and secondly to ‘broiler’ (14.4%) and ‘turkey’ (13.3%) sources. To interpret these data, it is important to be aware that the distribution of the serotyped isolates among the different sources is very unbalanced in terms of the number of isolates per source, and the large majority of the serotyped isolates for the subsets considered were from poultry populations covered by NCPs, especially broilers.
Table 29 shows the top 20 serovars notified, considering all serotyped isolates (including those from both food and animals) from the following species: laying hens, broilers, turkeys, pigs and bovine animals. For laying hens, 44.3% of the isolates (N = 1022) belonged to two target serovars (S. Enteritidis [34.1%] and S. Typhimurium [10.2%]). The other most common serovars from this source were S. Kentucky (12.1%) and S. Infantis (9.6%). For broilers (N = 13,061), three serovars (S. Infantis, S. Enteritidis and S. Mbandaka) represented 65.2% of the serotyped isolates, with S. Infantis comprising 50.1% of all strains, and this serovar was notified from poultry sources by 22 MSs. S. Thompson and S. Livingstone were two other serovars isolated from this source (4.2% and 3.1%). Also, for turkey sources (N = 2416), two serovars (S. Agona [46.3%] and S. Anatum [23.4%]) were by far the most common ones, with S. Agona reporting being increased by 97.0% versus the previous year, and with S. Anatum being notified only by three MSs. S. Infantis was the third main serovar notified from turkey sources (4.5%) and overall, S. Typhimurium, its monophasic variant and S. Enteritidis accounted for 5.5% of the isolates from this species. For pigs, the monophasic variant of S. Typhimurium (25.7%), S. Derby (23.9%) and S. Typhimurium (21.9%) represented 71.5% of the serotyped strains (N = 1068) from this source, with S. Infantis (4.9%) and S. Rissen (4.8%) being two other common serovars. Considering serotyped isolates from bovine sources (N = 790), two serovars were by far the most common ones: S. Typhimurium and S. Dublin represented 35.8% and 34.3% of the serotyped isolates from this source, respectively. S. Infantis appears among the top four serovars for all three sources of poultry populations considered, as well as for pig and bovine sources.
TABLE 29.
Distribution of the top 20 Salmonella serovars by food–animal source (laying hens, broilers, turkeys, pigs and bovine animals), EU, 2022.
| Poultry population | |||||||||||
| Serovar | N (%) positive sampling units | N MSs | Serovar | N (%) positive sampling units | N MSs | Serovar | N (%) positive sampling units | N MSs | |||
| Laying hens | |||||||||||
| Enteritidis | 349 (34.1) | 19 | Broilers | Infantis | 6540 (50.1) | 22 | Turkeys | Agona | 1118 (46.3) | 8 | |
| Kentucky | 124 (12.1) | 6 | Enteritidis | 1009 (7.7) | 19 | Anatum | 565 (23.4) | 3 | |||
| Typhimurium | 104 (10.2) | 14 | Mbandaka | 964 (7.4) | 13 | Infantis | 108 (4.5) | 8 | |||
| Infantis | 98 (9.6) | 13 | Thompson | 547 (4.2) | 6 | Newport | 82 (3.4) | 4 | |||
| Corvallis | 29 (2.8) | 6 | Livingstone | 403 (3.1) | 7 | Senftenberg | 64 (2.6) | 5 | |||
| Mbandaka | 25 (2.5) | 8 | Typhimurium | 296 (2.3) | 19 | Typhimurium, monophasic | 55 (2.3) | 8 | |||
| Agona | 20 (2.0) | 4 | Java | 293 (2.2) | 3 | Derby | 51 (2.1) | 7 | |||
| Braenderup | 18 (1.8) | 5 | Senftenberg | 274 (2.1) | 10 | Typhimurium | 48 (2.0) | 9 | |||
| Kottbus | 18 (1.8) | 7 | Montevideo | 261 (2.0) | 6 | Enteritidis | 28 (1.2) | 7 | |||
| Livingstone | 16 (1.6) | 8 | Kedougou | 230 (1.8) | 5 | Coeln | 27 (1.1) | 7 | |||
| Hadar | 14 (1.4) | 3 | Agona | 224 (1.7) | 14 | Bredeney | 24 (0.99) | 2 | |||
| Typhimurium, monophasic | 14 (1.4) | 6 | Newport | 151 (1.2) | 14 | Saintpaul | 24 (0.99) | 1 | |||
| Ohio | 13 (1.3) | 3 | Bredeney | 148 (1.1) | 4 | Hadar | 21 (0.87) | 5 | |||
| Mikawasima | 12 (1.2) | 2 | Virchow | 139 (1.1) | 9 | Heidelberg | 17 (0.70) | 2 | |||
| Napoli | 12 (1.2) | 2 | Give | 128 (0.98) | 3 | Napoli | 17 (0.70) | 2 | |||
| Senftenberg | 11 (1.1) | 4 | Napoli | 90 (0.69) | 2 | Kentucky | 15 (0.62) | 3 | |||
| Anatum | 10 (0.98) | 3 | Anatum | 88 (0.67) | 8 | Kedougou | 14 (0.58) | 2 | |||
| Coeln | 10 (0.98) | 8 | Typhimurium, monophasic | 85 (0.65) | 8 | Haifa | 13 (0.54) | 1 | |||
| Newport | 10 (0.98) | 6 | Tennessee | 67 (0.51) | 5 | Lagos | 13 (0.54) | 1 | |||
| Toulon | 8 (0.78) | 1 | Liverpool | 61 (0.47) | 3 | Montevideo | 11 (0.46) | 2 | |||
| Other serovars | 107 (10.5) | 25 | Other serovars | 1063 (8.1) | 27 | Other serovars | 101 (4.2) | 19 | |||
| Total | 1022 | Total | 13,061 | Total | 2416 | ||||||
| Pigs and cattle (bovine animals) | |||||||||||
| Serovar | N (%) positive samples | N MSs | Serovar | N (%) positive sampling units | N MSs | ||||||
| Pigs | |||||||||||
| Typhimurium, monophasic | 274 (25.7) | 18 | Bovine animals | Typhimurium | 283 (35.8) | 17 | |||||
| Derby | 255 (23.9) | 18 | Dublin | 271 (34.3) | 9 | ||||||
| Typhimurium | 234 (21.9) | 20 | Infantis | 46 (5.8) | 8 | ||||||
| Infantis | 52 (4.9) | 14 | Enteritidis | 26 (3.3) | 10 | ||||||
| Rissen | 51 (4.8) | 11 | Typhimurium, monophasic | 25 (3.2) | 6 | ||||||
| Brandenburg | 25 (2.3) | 4 | Derby | 14 (1.8) | 6 | ||||||
| Give | 16 (1.5) | 8 | Havana | 11 (1.4) | 4 | ||||||
| Choleraesuis | 14 (1.3) | 3 | Muenster | 11 (1.4) | 3 | ||||||
| Enteritidis | 12 (1.1) | 8 | Rissen | 11 (1.4) | 2 | ||||||
| Litchfield | 11 (1.0) | 2 | Mbandaka | 8 (1.0) | 5 | ||||||
| London | 10 (0.94) | 2 | Manhattan | 6 (0.76) | 2 | ||||||
| Livingstone | 9 (0.84) | 3 | Montevideo | 6 (0.76) | 4 | ||||||
| Senftenberg | 8 (0.75) | 3 | Chester | 5 (0.63) | 1 | ||||||
| Bredeney | 7 (0.66) | 3 | Coeln | 5 (0.63) | 2 | ||||||
| Coeln | 6 (0.56) | 2 | Altona | 4 (0.51) | 2 | ||||||
| Panama | 6 (0.56) | 3 | Napoli | 4 (0.51) | 1 | ||||||
| Goldcoast | 5 (0.47) | 3 | Newport | 4 (0.51) | 2 | ||||||
| Kapemba | 5 (0.47) | 3 | Nottingham | 4 (0.51) | 1 | ||||||
| Bovismorbificans | 4 (0.37) | 3 | Agona | 3 (0.38) | 1 | ||||||
| I 6,7:‐:1,5, Kimuenza | 4 (0.37) | 1, 2 | Bovismorbifican, Drogana, Give, Senftenberg | 3 (0.38) | 2, 1, 1, 1 | ||||||
| Other serovars | 56 (5.2) | 24 | Other serovars | 31 (3.9) | 23 | ||||||
| Total | 1068 | Total | 790 | ||||||||
Abbreviation: MSs, Member States.
2.5. Discussion
Salmonellosis remained the second most common foodborne zoonosis in humans in the EU in 2022 after campylobacteriosis. In 2022, a slight increase in notified human cases was registered compared with 2021: this may have been due to the slow resumption of daily activities (social events, doctor's visits, travel) after COVID‐19 restrictions. The number of human salmonellosis cases acquired in the EU was higher in 2022 than in 2020 but lower than in 2021 and in previous years. The number of human salmonellosis cases acquired outside the EU was higher in 2022 than in 2021–2020 and may have been a consequence of the restored possibility of travel outside the EU. Travel‐associated cases still remained at a lower level than before the pandemic. The number of outbreak‐related cases was stable compared with 2021 while the number of foodborne salmonellosis outbreaks was higher in 2022 than in 2021. Notwithstanding, the overall EU trend for salmonellosis in 2018–2022 did not show any significant increase or decrease. Conversely, over the period 2018–2022, Denmark, Germany, Finland, Latvia and Sweden reported a decreasing trend.
In addition, notification rates for salmonellosis in humans varied between MSs, reflecting potential variations, for example, in the quality, coverage and disease‐severity focus of the surveillance systems, in sampling and testing practices, in disease prevalence in the food‐producing animal population and in food and animal trade between MSs.
The hospitalisation rate varied from 22.1% to 100% between countries. Countries reporting the lowest notification rates for salmonellosis had the highest proportions of hospitalisation, suggesting that the surveillance systems in these countries are focused on the most severe cases and underlining the variability of national surveillance systems. It is important to note that a higher hospitalisation rate was reported for patients with specimens from blood (85.6%), suggesting that people with systemic infection are more likely to be hospitalised.
In 2022, a decrease in the proportion of reported data for Salmonella serovars was observed compared with 2021. In 2022, the proportion of monophasic S. Typhimurium (1,4,[5],12:i‐) slightly increased and the proportion of S. Enteritidis decreased compared with previous years. Concerning the slightly decreased proportion of S. Enteritidis cases both in general and acquired in the EU, it was partly but not entirely due to a delay in serovar data reporting for one MS (Spain) and to the discontinued reporting of domestic cases by another MS (the Netherlands) compared with previous years. Since 2022, the Netherlands only reported the travel‐associated cases, whereas other cases were reported with unknown importation status or an unknown probable country of infection.
Regarding the cases acquired in the EU, the ranking of the five most common serovars was stable. Overall, the three most commonly reported human serovars, S. Enteritidis, S. Typhimurium and its monophasic variant (1,4,[5],12:i:‐), continued to account for over 70% of human cases acquired in the EU, as has been observed since 2014, reaching 84.7% in 2022. S. Infantis has consistently been the fourth most frequently reported serovar involved in domestically acquired and travel‐associated human infections among cases within and outside the EU. After S. Infantis, S. Derby was the fifth most frequently reported serovar among the EU‐acquired cases in 2022, while S. Agona and S. Mbandaka slid up to eighth and eleventh positions, respectively. This was probably due to a multi‐country outbreak of S. Mbandaka ST413 in seven EU MSs, possibly linked to consumption of chicken meat (ECDC and EFSA, 2022c).
Concerning Salmonella NCPs, although no significant trends for target serovar prevalence were identified over the most recent years, in 2022, the number of MSs that reached the reduction targets for all the poultry categories increased compared with the previous years (16 and 19 MSs in 2021 and 2022, respectively). Moreover, in 2022 for broilers and breeding turkeys, all MSs reached the reduction targets, whereas in 2021 for all poultry categories, at least one MS did not reach the target. These positive signals suggest that the control and management practices in place (including biosecurity, vaccination, cleaning and disinfection, probiotics and prebiotics, and feed and water acidification with organic acids) seem to be working properly to control the prevalence of the serovars that have been identified as ‘target’ serovars at EU level in the context of NCPs. Still, the prevalence of poultry flocks positive for Salmonella spp., irrespective of target/non‐target serovars, was high for some MSs (especially for broilers and fattening turkeys).
Although S. Enteritidis and S. Typhimurium (including its monophasic variant) have historically been the serovars responsible for the great majority of human cases (almost 85% in 2022), the high prevalence of some non‐target Salmonella serovars in animal but also food sources may be critical, especially in the case of emerging serovars/clones, which can enter specific niches, colonise them and become persistent.
Since 2014, S. Infantis has by far been the no. 1 serovar isolated in broiler production in many MSs (Montoro‐Dasi et al., 2023); such phenomena could also occur with other serovars, which are progressively increasing in other poultry populations. For instance, over the last couple of years, S. Anatum and S. Agona were reported in turkeys and ranked in the top positions for the serovars identified, even though their notification from human cases is rather uncommon. The same is also true for S. Kentucky, which is frequently found in poultry flocks (it is the second most common serovar from laying hens [12.1%]); fortunately, it is rarely associated with human infections (Samper‐Cativiela et al., 2022). These serovars can possess, as demonstrated especially for S. Infantis, various genetic strategies (e.g. presence of antimicrobial resistance genes, resistance to heavy metals, mobile virulence genes, ability to form biofilm) that could enhance their epidemiological fitness and provide additional traits of virulence and persistence throughout the food chain (Alba et al., 2023). The surveillance of newly emerging Salmonella serovars is important especially in the event that these bacteria have developed mechanisms to survive even under harsh environmental conditions (Chousalkar & Willson, 2022). Moreover, surveillance must be planned, taking into account the specific epidemiological situation of the area where it should be implemented (EFSA BIOHAZ Panel et al., 2019). Still, a cost–benefit approach focusing on the local epidemiological scenario is essential to estimate to what extent control measures in the different contexts would be feasible and affordable. To further complicate this situation, several studies have demonstrated that control strategies based on ‘serovars’ without consideration of the actual pathogenic potential of the single strain, as is promoted by the current EU legislation, might overlook highly pathogenic Salmonella strains, which do not necessarily belong to the target serovars. Such strains could spread as emerging clones, becoming potential causes of new outbreaks (Petrin et al., 2023). Unfortunately, so far, the identification of virulence patterns to unambiguously predict Salmonella pathogenicity in different hosts still remains very challenging.
As far as target serovars are concerned, S. Enteritidis was the most frequent target serovar found in laying hens and broilers, whereas for turkeys, pigs and bovine animals, S. Typhimurium and the monophasic variant were the most frequent ones. The relevance of S. Enteritidis was confirmed by the fact that in 2022, the combination of Salmonella‐eggs/egg products caused the highest number of foodborne outbreaks, and in this context, S. Enteritidis was largely the predominant serovar. The content of intact eggs can become contaminated through two different routes: horizontal transmission, where Salmonella can penetrate the eggshell, and vertical transmission, where Salmonella infects the reproductive organs and the content of the eggs is directly infected. For S. Enteritidis, this second route of contamination seems to be the most relevant.
Notably, considering food data, both those collected in the context of current legislation (PHC and FSC in accordance with Regulation (EC) 2073/2005) and other food prevalence data, poultry meat/carcases and derived products were consistently identified as the matrices with the highest prevalence of Salmonella contamination. These observations are consistent with the fact that three out of the seven rapid outbreak assessments (ROAs) published by ECDC and EFSA in 2022 and 2023 pointed to food products containing poultry meat as the likely sources of infection of multi‐country outbreaks due to S. Virchow, S. Mbandaka and S. Enteritidis, respectively (ECDC and EFSA, 2022c, 2023a, 2023c). Moreover, data collected in this context confirmed that, especially for poultry (broiler and turkey) carcases, the proportion of positive samples, identified by sampling conducted by the CA, was significantly higher than that notified for samples taken by the FBOp. This discrepancy was also observed for national control programmes for poultry, where separate reporting on controls carried out by the CA and FBOp is mandatory. Investigations to define the reasons for discrepancies between the results of sampling conducted by the CA and FBOp should be encouraged as an essential prerequisite to ensure the trustworthiness of the data collected in both contexts.
Pre‐harvest interventions, which take place at the farm level and during the transport of flocks, aim to reduce as much as possible the introduction, persistence and transmission of Salmonella on farms (Pessoa et al., 2021). Meat safety depends to a great extent on the bacterial load of the incoming animals to the slaughterhouse and on the procedures aimed at reducing cross‐contamination during slaughter and meat processing (Salines et al., 2023). Indeed, for this specific purpose, risk categorisation of farms and slaughterhouses according to their hygiene process performance along with harmonised epidemiological indicators in a combined risk categorisation system (Langkabel et al., 2023) have been identified as essential components of the risk‐based meat safety assurance system, according to EFSA's opinion published a decade ago (EFSA BIOHAZ Panel, EFSA CONTAM Panel and EFSA AHAW Panel, 2012).
3. LISTERIA MONOCYTOGENES
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here, and are also retrievable from the EFSA Listeria monocytogenes dashboard available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
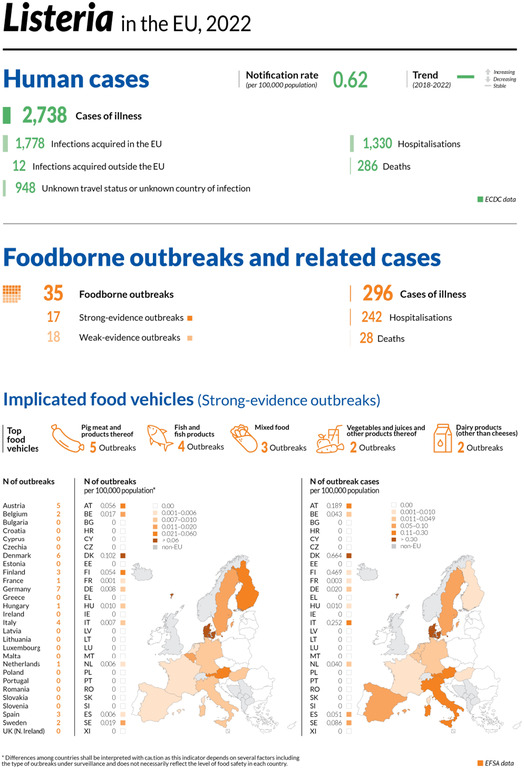
3.1. Key facts
In 2022, 27 Member States reported 2738 confirmed invasive human cases of L. monocytogenes. These cases resulted in 1330 hospitalisations and 286 deaths in the European Union. Listeriosis was the fifth most commonly reported zoonosis in humans in the European Union and one of the most serious foodborne diseases under European Union surveillance.
The European Union notification rate was 0.62 cases per 100,000 population, which was an increase of 15.9% compared with 2021 (0.53 cases per 100,000 population) and the highest rate and number of cases reported since 2007.
The overall trend for listeriosis did not show any significant increase or decrease, in the 2018–2022 period.
The overall European Union case fatality rate was high (18.1%), higher than 2021 and 2020 (13.7% and 13.0%, respectively).
26 Member States reported a total of 312,849 sampling units from different ‘ready‐to‐eat’ food categories, from the distribution or manufacturing stages.
At distribution, the proportions of positive results for single sample enumeration tests for L. monocytogenes carried out by the competent authorities as part of verification of L. monocytogenes Food Safety Criteria listed in Regulation (EC) No 2073/2005 24 remained rare (< 0.1%) to very low (0.1%–1.0%) in 9 out of 10 focussed ‘RTE’ food categories. The highest proportion at distribution was observed for ‘fish’ (2.3%).
In the same context, at manufacturing, the proportions of single samples positive for L. monocytogenes based on the detection test were higher compared with those at the distribution level, for all categories of ‘ready‐to‐eat’ food except for ‘milk’, for which no Listeria was detected regardless of the stage. The highest proportions at manufacturing were observed for ‘fish’ (2.6%), ‘fishery products’ (2.5%) and ‘products of meat origin other than fermented sausages’ (2.5%).
The occurrence of L. monocytogenes gives an indication of the reasonably foreseeable contamination rate in these ‘ready‐to‐eat’ food categories. Results varied according to the ‘ready‐to‐eat’ food category, the sampling stage, the number of tested sampling units and the number of reporting countries. In the framework of objective sampling, all samplers and sampling units included, overall occurrences remained generally rare (< 0.1%) to low (1%–10%) in these categories. The overall highest values (from 2% to 7%) were observed for ‘fish and fishery products’, ‘meat products from bovines or pigs’, ‘fruits and vegetables’ and ‘cheeses from sheep milk’.
At primary production, the percentage of positive units was very low in pigs (0.35%) and low in cattle (1.2%), which was the most sampled animal species in the European Union. The low number of Member States reporting data reflects the absence of minimum legal requirements for harmonised sampling and reporting at primary production.
3.2. Surveillance and monitoring of Listeria monocytogenes in the EU
EFSA story map on Listeria monocytogenes
General information on L. monocytogenes and its epidemiology, including information on where the pathogen can be found, how people and animals get infected, the occurrence of this pathogen in different sources, the disease it causes and how to prevent infection, is provided in the EFSA story map on L. monocytogenes (available here). In addition, this story map also illustrates the monitoring activities implemented in the EU and the role of EFSA with respect to these activities.’
3.2.1. Humans
Surveillance of listeriosis in humans in the EU focuses on invasive forms of L. monocytogenes infection, mostly manifesting as septicaemia, influenza‐like symptoms, meningitis or spontaneous abortion.
Surveillance of listeriosis is mandatory in all MSs, except in one country (Belgium). The EU case definition was used by 24 countries. Two countries (Germany and Italy) reported using other case definitions, and one country (France) did not specify which case definition was used.
All countries had comprehensive surveillance systems. The surveillance systems for listeriosis cover the whole population in all MSs, except in two (Belgium and Spain). The estimated coverage of the surveillance system was 80% in Belgium and 97% in Spain for 2021–2022. These estimated proportions of population coverage were used in the calculation of notification rates for these two countries. No estimated population coverage was provided for Spain prior to 2021, so notification rates were not calculated. In 2020, Spain did not receive data from all regions that normally report, so the case numbers may therefore not be complete. Bulgaria reported aggregated data, while the other 26 countries reported case‐based data.
3.2.2. Food, animals and feed
Monitoring of L. monocytogenes is carried out along the food chain, at primary production, manufacturing and distribution.
The public health risk associated with ‘ready‐to‐eat' (RTE) foods depends mainly on the effectiveness of control measures implemented by food business operators (FBOps), including:
-
–
Good Agricultural Practices (GAPs) at primary production
-
–
Good Manufacturing Practices (GMP) and Hazard Analysis and Critical Control Point (HACCP) programmes at manufacturing and distribution
-
–
Microbiological criteria for RTE foods as defined by Regulation (EC) No 2073/2005
Official sampling is scheduled by national CAs to verify whether FBOps correctly implement the legal framework of their own‐check programmes. Official control samples are thus part of the verification of L. monocytogenes food safety criteria (FSC). Data provided to EFSA within this context enable a descriptive summary of contamination levels, especially of RTE foods, at the EU level.
The rationale for surveillance and monitoring of L. monocytogenes in animals, feed, and food at the different stages along the food chain and the number of sampling units provided to EFSA are shown in Figure 7.
FIGURE 7.
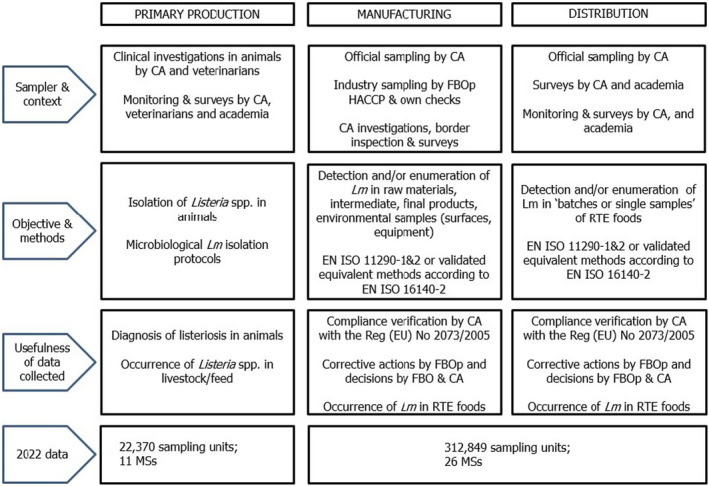
Overview of Listeria monocytogenes testing along the food chain according to the sampling stage, the sampler and the objective of the sampling, EU.
At the manufacturing and distribution stages, in 2022, 26 MSs reported 312,849 sampling units tested for L. monocytogenes involving different RTE food categories. Compared with 2021, the number of reporting MSs and the number of tested sampling units at these stages were higher (24 reporting MSs and 244,357 sampling units tested in 2021).
At primary production, data are far more comparable with previous years, with 11 MSs reporting 22,370 sampling units in 2022, compared with 23,564 sampling units in 2021 (12 MSs) and 22,567 units in 2020 (13 MSs). Most of the reported data in animals and feed are generated by non‐harmonised monitoring schemes across MSs, and for which mandatory reporting requirements do not exist. Data on the occurrence of L. monocytogenes in feed are only collected as part of clinical investigations in farm animals. Hence, monitoring data on L. monocytogenes in animal feed are rarely available.
3.3. Data analyses
3.3.1. Data on RTE food in the context of Regulation (EC) No 2073/2005 on microbiological criteria
These data are based on single samples collected by CAs as part of verification of L. monocytogenes FSC listed in Regulation (EC) No 2073/2005, which are to be complied with by FBOps. These FSC are specified by RTE food category, and by sampling stage, and are underpinned by the results of either detection or enumeration analytical methods (Table 30). These data were extracted from the database using the criteria ‘official sampling’ for the sampler, ‘single units’ for the sampling unit and ‘objective sampling’ for the sampling strategy Table 33).
TABLE 30.
Listeria monocytogenes FSC as described in Regulation (EC) No 2073/2005 for the different RTE categories across the food chain, 2022.
| Sampling stage | RTE foods intended for infants and RTE foods for special medical purposes | Other RTE foods | |
|---|---|---|---|
| Able to support growth of Lm | Unable to support growth of Lm | ||
| Manufacturing a | NA | Based on detection method: Lm not detected in 25 g of sample (n = 5, c = 0) c | NA |
| Distribution b | Based on detection method: Lm not detected in 25 g of sample (n = 10, c = 0) | Based on enumeration method: limit of 100 CFU/g (n = 5, c = 0) d | Based on enumeration method: limit of 100 CFU/g (n = 5, c = 0) |
Abbreviations: Lm, Listeria monocytogenes; NA, not applicable; RTE, ready‐to‐eat.
Before the food has left the immediate control of the food business operator that has produced it.
Products placed on the market during their shelf‐life.
n = number of units comprising the sample (number of sample units per food batch that are required for testing); c = the maximum allowable number of sample units yielding unsatisfactory test results. In a two‐class attributes sampling plan defined by n = 10, c = 0 and a microbiological limit of ‘not detected in 25 g’, in order for the food batch to be considered acceptable, L. monocytogenes must not be detected in qualitative (detection) analyses of 25 g food test portions obtained from each one of 10 sample units taken from the batch. If even one of the sample units from the batch is found to contain L. monocytogenes (detected in 25 g), then the entire batch is deemed unacceptable. This criterion applies to products before they have left the immediate control of the producing food business operator, when the operator is not able to demonstrate, to the satisfaction of the CA, that the product will not exceed the limit of 100 CFU/g throughout the shelf‐life.
This criterion applies if the manufacturer is able to demonstrate, to the satisfaction of the CA, that the product will not exceed the limit of 100 CFU/g throughout the shelf‐life. The operator may fix intermediate limits during the process that should be low enough to guarantee that the limit of 100 CFU/g is not exceeded at the end of the shelf‐life.
TABLE 33.
Proportions (%) of positive single samples at the manufacturing and distribution stage from official sampling by CAs in the context of verification of implementation by FBOps of the Listeria monocytogenes FSC according to Regulation (EC) No 2073/2005, EU, 2022.
| RTE food category a | Manufacturing b | Distribution c | ||
|---|---|---|---|---|
| Analytical method d | ||||
| Detection (EN ISO 11290‐1) | Detection (EN ISO 11290‐1) | Enumeration (EN ISO 11290‐2) | ||
| % positive samples (N samples tested, N reporting MS) d | % positive samples (N samples tested, N reporting MS) d | % positive samples (N samples tested, N reporting MS) d | % of samples exceeding 100 CFU/g e | |
| Foods intended for infants and for medical purposes: data reported from BE, CY, GR, HR, HU, IT, RO, SK, SI, ES | 0 (N = 1244; 10 MS) | |||
| Fish: data reported from AT, BE, BG, CY, CZ, DK, ES, FR, GR, HR, HU, IT, LV, PL, SI, SK | 2.6 (N = 971; 9 MS) | 2.3 (N = 1022; 14 MS) | 0 | |
| Fishery products: data reported from AT, BE, BG, DK, EE, ES, FR, HR, IT, LV, RO, SI, SK | 2.5 (N = 842; 8 MS) | 0.67 (N = 1935; 11 MS) | 0.05 | |
| Cheeses, soft and semi‐soft: data reported from AT, BE, BG, CZ, ES, GR, HR, HU, IT, LV, PL, RO, SK | 0.33 (N = 6407; 11 MS) | 0.08 (N = 2537; 11 MS) | 0.08 | |
| Cheeses, hard: data reported from BG, CZ, ES, IT, SK | 0.56 (N = 359; 5 MS) | 0 | ||
| Cheeses, unspecified: data reported from AT, BE, ES, HU, IT, PL, SI | 1.5 (N = 1981; 6 MS) | 0.30 (N = 337; 5 MS) | 0.30 | |
| Other dairy products (excluding cheeses) – entire category: data reported from AT, BE, BG, CZ, ES, GR, HR, HU, IT, PL, RO, SI, SK | 0.14 (N = 6544; 11 MS) | 0 (N = 1857; 10 MS) | 0 | |
| Milk: data reported from AT, BG, CY, CZ, E+S, GR, HR, IT, PL, RO, SK | 0 (N = 566; 9 MS) | 0 (N = 167; 6 MS) | 0 | |
| Products of meat origin, fermented sausages: data reported from BE, BG, CY, DK, EE, HR, HU, SK | 0.28 (N = 359; 8 MS) | 0 | ||
| Products of meat origin, other than fermented sausages: data reported from AT, BE, BG, CZ, DK, EE, ES, GR, HR, HU, IT, LV, PL, RO, SI, SK | 2.5 (N = 18,061; 13 MS) | 0.41 (N = 4628; 15 MS) | 0.13 | |
| Other products: data reported from AT, BE, BG, CY, CZ, DK, ES, GR, HR, HU, IT, LV, MT, RO, SK | 0.79 (N = 2403; 8 MS) | 0.31 (N = 6803; 15 MS) | 0.12 | |
Note: Grey boxes are not applicable in relation to the analytical method for the specific food category and sampling stage in the context of Regulation (EC) No 2073/2005.
Abbreviations: CFU, colony forming units; MSs, Member States; N, number of single samples tested; RTE, ready‐to‐eat.
In the absence of relevant physicochemical data (pH, aw), EFSA assumes that foods listed under ‘fish and fishery products’, ‘soft and semi‐soft cheeses’, ‘unspecified cheeses’, ‘milk’, ‘products of meat origin other than fermented sausages’, ‘other dairy products’ and ‘other products’ belong to the category of foods that are able to support the growth of L. monocytogenes. EFSA assumes that ‘fermented sausages’ and ‘hard cheeses’ belong to the category of foods that are unable to support the growth of L. monocytogenes, because foods classified under these two categories of RTE products undergo ripening/fermentation and are expected to have low pH and moderate aw values. For ‘other dairy products’, EFSA presents the results in a conservative way, by considering all foods included in this category as capable of supporting the growth of L. monocytogenes.
Includes sampling units that were collected from ‘cutting plants’ and ‘processing plants’.
Includes sampling units that were obtained from ‘catering’, ‘hospital or medical care facility’, ‘retail’, ‘wholesale', ‘not available', ‘unspecified’, ‘restaurant or cafe or pub or bar or hotel or catering service', ‘automatic distribution system for raw milk’, ‘border inspection’ and ‘packing centre'.
Proportion (%) of positive samples (detection of L. monocytogenes in 25 g of sample for qualitative analyses, or number of L. monocytogenes > or ≤ 100 CFU/g for enumeration analyses); in parentheses the number of tested samples and the number of reporting MSs.
Proportion (%) of samples exceeding 100 CFU/g for enumeration analyses.
Data reported by MSs were classified into the different categories of RTE food/sampling stages based on the assumptions described in the EU Summary zoonoses and foodborne outbreaks report of 2016 (EFSA and ECDC, 2017). Briefly, these assumptions are: all sampling units that were collected from ‘cutting plants’ and ‘processing plants’ were considered units collected at the manufacturing stage, while sampling units that were obtained from ‘catering’, ‘hospital or medical care facility’, ‘retail’, ‘wholesale', ‘restaurant or cafe or pub or bar or hotel or catering service', ‘border inspection activities’, ‘packing centre' and ‘automatic distribution system for raw milk’ were considered units collected at distribution. When the stage was ‘not available' or ‘unspecified’, data were also considered part of the distribution stage. Other assumptions concerning the RTE categories are presented in the footnotes of Table 33.
3.3.2. Other monitoring data for Listeria monocytogenes in RTE food
The overall occurrence of L. monocytogenes in different RTE food categories, regardless of the stage, was assessed from detection results reported by MSs. All levels of sampling unit (single and batches), sampling stages, sampler and sampling contexts (surveillance, monitoring and surveillance – based on Regulation (EC) No 2073/2005) were considered. Only data obtained from the sampling strategies ‘objective sampling’ and ‘census sampling’ were used, excluding data reported from ‘convenient sampling’, ‘suspect sampling’, ‘selective sampling’ and ‘other’ contexts.
Since data were mostly reported by a limited number of MSs and are of a heterogeneous nature, results may not be representative of the EU level or directly comparable across years.
3.3.3. Monitoring data for Listeria monocytogenes in animals and feed
For animals and feed, all sampling strategies were included, even data reported for ‘suspect sampling’ and ‘selective sampling’.
EFSA dashboard on Listeria monocytogenes
Summary statistics for the monitoring results for L. monocytogenes with regard to major RTE food categories, L. monocytogenes‐positive official samples in the context of FSC in accordance with Regulation (EC) No 2073/2005 and official samples exceeding the FSC limit of 100 for specified food matrices and other monitoring statistics are displayed, retrievable and downloadable in the EFSA dashboard on L. monocytogene (available here).
3.4. Results
3.4.1. Overview of key statistics, EU, 2018–2022
Table 31 summarises EU‐level statistics on human listeriosis and on sampling units from RTE food tested for L. monocytogenes during the period 2018–2022. Food data of interest reported were classified into the major categories and aggregated by year to obtain an annual overview of the volume of data submitted. More detailed descriptions of these statistics are provided in the below subsections and in the chapter on foodborne outbreaks.
TABLE 31.
Summary of Listeria monocytogenes statistics relating to invasive human infections and major RTE food categories, EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 2738 | 2365 | 1887 | 2621 | 2544 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0.62 | 0.53 | 0.43 | 0.46 | 0.47 | ECDC |
| Number of reporting MSs | 27 | 27 | 27 | 28 | 28 | ECDC |
| Infection acquired in the EU | 1778 | 1546 | 1286 | 1816 | 1640 | ECDC |
| Infection acquired outside the EU | 12 | 5 | 5 | 14 | 8 | ECDC |
| Unknown travel status or unknown country of infection | 948 | 814 | 596 | 791 | 896 | ECDC |
| Number of outbreak‐related cases | 296 | 104 | 120 | 349 | 159 | EFSA |
| Total number of outbreaks | 35 | 23 | 16 | 21 | 14 | EFSA |
| Sampled major RTE food categories c | ||||||
| Meat and meat products | ||||||
| Number of sampling units | 135,148 | 107,198 | 40,291 | 64,971 | 58,060 | EFSA |
| Number of reporting MSs | 24 | 23 | 22 | 22 | 22 | EFSA |
| Fish and fishery products | ||||||
| Number of sampling units | 25,009 | 29,783 | 11,212 | 13,366 | 14,031 | EFSA |
| Number of reporting MSs | 24 | 24 | 23 | 22 | 22 | EFSA |
| Milk and milk products | ||||||
| Number of sampling units | 97,157 | 66,633 | 49,132 | 61,866 | 59,313 | EFSA |
| Number of reporting MSs | 24 | 23 | 23 | 23 | 23 | EFSA |
| Products intended for infants or special medical purposes | ||||||
| Number of sampling units | 2672 | 2764 | 2394 | 2346 | 2433 | EFSA |
| Number of reporting MSs | 19 | 19 | 19 | 19 | 18 | EFSA |
| Other products | ||||||
| Number of sampling units | 120,530 | 94,841 | 81,575 | 80,167 | 28,204 | EFSA |
| Number of reporting MSs | 25 | 23 | 24 | 24 | 23 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States; RTE, ready‐to‐eat.
Data on animal samples from the United Kingdom (Northern Ireland) were taken into account for 2021. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Number of sampling units tested by detection or enumeration method.
For a further interactive look at L. monocytogenes monitoring results, also at the level of the MSs, dashboards have been created (different filters can be applied to query the data) (here).
3.4.2. Human listeriosis
In 2022, 27 MSs reported 2738 confirmed cases of invasive listeriosis in humans (Tables 31 and 32). The EU notification rate was 0.62 cases per 100,000 population, 15.9% higher than in 2021 (0.53 per 100,000 population). The highest notification rates were observed for Denmark, Finland, Sweden, Spain, Slovenia and Belgium, with 1.5, 1.3, 1.2, 0.95, 0.95 and 0.94 cases per 100,000 population, respectively. The lowest notification rates were reported by Bulgaria, Croatia, Cyprus, Greece, Malta and Romania (≤ 0.20 per 100,000). Some countries had double the number of cases: Czechia 48 in 2022 versus 24 in 2021 and Slovakia 25 in 2022 versus 13 in 2021. In Italy, cases increased by 115 and in Spain by 82; other countries also reported increased case numbers (Austria, Belgium, Bulgaria, Denmark, Estonia, France, Hungary, Ireland, Lithuania, the Netherlands, Poland, Portugal, Romania, Slovenia and Sweden) (Table 32) Likewise, the reported number of foodborne outbreaks of listeriosis has increased (35 in 2022 vs. 23 in 2021), specifically in Austria (5), Belgium (2), Hungary (1), Italy (4), the Netherlands (1), Spain (3) and Sweden (2). (See FBO chapter for more info).
TABLE 32.
Reported confirmed human cases of invasive listeriosis and notification rates per 100,000 population in EU MS and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 47 | 0.52 | 38 | 0.43 | 41 | 0.46 | 38 | 0.43 | 27 | 0.31 |
| Belgium b | N | C | 87 | 0.94 | 68 | 0.74 | 54 | 0.59 | 66 | 0.72 | 74 | 0.81 |
| Bulgaria | Y | A | 5 | 0.07 | 3 | 0.04 | 4 | 0.06 | 13 | 0.19 | 9 | 0.13 |
| Croatia | Y | C | 5 | 0.13 | 8 | 0.20 | 5 | 0.12 | 6 | 0.15 | 4 | 0.10 |
| Cyprus | Y | C | 1 | 0.11 | 1 | 0.11 | 2 | 0.23 | 1 | 0.11 | 1 | 0.12 |
| Czechia | Y | C | 48 | 0.46 | 24 | 0.22 | 16 | 0.15 | 27 | 0.25 | 31 | 0.29 |
| Denmark | Y | C | 86 | 1.5 | 62 | 1.1 | 43 | 0.74 | 61 | 1.1 | 49 | 0.85 |
| Estonia | Y | C | 11 | 0.83 | 5 | 0.38 | 3 | 0.23 | 21 | 1.6 | 27 | 2.05 |
| Finland | Y | C | 70 | 1.3 | 70 | 1.3 | 94 | 1.7 | 50 | 0.91 | 80 | 1.45 |
| France | Y | C | 451 | 0.66 | 435 | 0.64 | 334 | 0.50 | 373 | 0.56 | 338 | 0.50 |
| Germany | Y | C | 548 | 0.66 | 562 | 0.68 | 546 | 0.66 | 571 | 0.69 | 678 | 0.82 |
| Greece | Y | C | 7 | 0.07 | 21 | 0.20 | 20 | 0.19 | 10 | 0.09 | 19 | 0.18 |
| Hungary | Y | C | 64 | 0.66 | 35 | 0.36 | 32 | 0.33 | 39 | 0.40 | 24 | 0.25 |
| Ireland | Y | C | 17 | 0.34 | 14 | 0.28 | 6 | 0.12 | 17 | 0.35 | 21 | 0.43 |
| Italy | Y | C | 345 | 0.58 | 230 | 0.39 | 155 | 0.26 | 202 | 0.34 | 178 | 0.29 |
| Latvia | Y | C | 8 | 0.43 | 10 | 0.53 | 8 | 0.42 | 6 | 0.31 | 15 | 0.78 |
| Lithuania | Y | C | 13 | 0.46 | 7 | 0.25 | 7 | 0.25 | 6 | 0.21 | 20 | 0.71 |
| Luxembourg | Y | C | 4 | 0.62 | 4 | 0.63 | 4 | 0.64 | 3 | 0.49 | 5 | 0.83 |
| Malta | Y | C | 1 | 0.19 | 0 | 0 | 5 | 0.97 | 5 | 1.0 | 1 | 0.21 |
| Netherlands | Y | C | 94 | 0.53 | 86 | 0.49 | 90 | 0.52 | 103 | 0.60 | 69 | 0.40 |
| Poland | Y | C | 142 | 0.38 | 120 | 0.32 | 57 | 0.15 | 121 | 0.32 | 128 | 0.34 |
| Portugal | Y | C | 63 | 0.61 | 57 | 0.55 | 47 | 0.46 | 56 | 0.54 | 64 | 0.62 |
| Romania | Y | C | 14 | 0.07 | 11 | 0.06 | 2 | 0.01 | 17 | 0.09 | 28 | 0.14 |
| Slovakia | Y | C | 25 | 0.46 | 13 | 0.24 | 7 | 0.13 | 18 | 0.33 | 17 | 0.31 |
| Slovenia | Y | C | 20 | 0.95 | 19 | 0.90 | 26 | 1.2 | 20 | 0.96 | 10 | 0.48 |
| Spain c | N | C | 437 | 0.95 | 355 | 0.77 | 191 | – | 504 | – | 370 | – |
| Sweden | Y | C | 125 | 1.2 | 107 | 1.0 | 88 | 0.85 | 113 | 1.1 | 89 | 0.88 |
| EU Total 27 | – | – | 2738 | 0.62 | 2365 | 0.53 | 1887 | 0.43 | 2467 | 0.49 | 2376 | 0.50 |
| United Kingdom | – | – | – | – | – | – | – | – | 154 | 0.23 | 168 | 0.25 |
| EU Total d | – | – | 2738 | 0.62 | 2365 | 0.53 | 1887 | 0.43 | 2621 | 0.46 | 2544 | 0.47 |
| Iceland | Y | C | 2 | 0.53 | 5 | 1.4 | 4 | 1.1 | 4 | 1.1 | 2 | 0.57 |
| Norway | Y | C | 30 | 0.55 | 20 | 0.37 | 37 | 0.69 | 27 | 0.51 | 24 | 0.45 |
| Liechtenstein | Y | C | 0 | 0 | 0 | 0 | 58 | 0.67 | 36 | 0.42 | 51 | 0.60 |
| Switzerland e | Y | C | 78 | 0.89 | 33 | 0.38 | ||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Sentinel system; notification rates calculated with an estimated population coverage of 80%.
Sentinel system; notification rates calculated with an estimated population coverage of 97% in 2021–2022. No information on estimated coverage in 2018–2020, so notification rate not estimated.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
Most (99.3%) listeriosis cases (N = 1778) with known origin of infection were reported to have been acquired in the EU in 2022 (Table 31). Twelve travel‐associated listeriosis cases were reported from outside the EU in 2022 (Algeria, Bosnia and Herzegovina, Ecuador, Eritrea, Iraq, Thailand, Türkiye, the United Kingdom, United States, Uzbekistan and South Africa) versus five cases outside the EU in 2021. No data on travel status or country of infection were reported for 948 cases (34.6%).
The distribution by month appears to be relatively stable. Over the last 5 years (2018–2022), there has been slightly greater reporting of cases in the second half of the year, peaking in July (Figure 8. Although an increase in cases and rates was observed in 2022, the overall EU trend for listeriosis cases in the period 2018–2022 did not show any significant increase or decrease. A significantly (p < 0.05) increasing trend was reported for Austria, Denmark, France and Hungary, whereas a significantly decreasing trend was reported by Estonia over the period 2018–2022.
FIGURE 8.
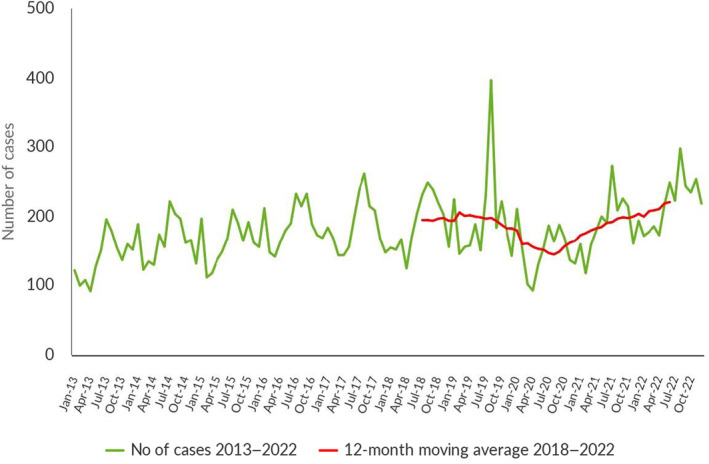
Trends in reported confirmed human cases of listeriosis in the EU by month, 2018–2022. Source: Austria, Belgium, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain and Sweden.
Information on hospitalisation was provided by 19 MSs for 50.6% of all confirmed cases in 2022. Among the cases with information on hospitalisation status, 96.0% were hospitalised, totalling 1330 hospitalised cases. Information on outcome was provided by 21 MSs and was reported for 1578 confirmed cases (57.6%). Nineteen MSs reported a total of 286 deaths from listeriosis in 2022. This represented a 53.8% increase compared with 2021 (186 deaths) (EFSA and ECDC, 2022). The overall EU case fatality rate among cases with known outcome was 18.1%. France reported the highest number of fatal cases (73), followed by Spain (67), Germany (33) and Poland (22). All reporting countries except Cyprus and Malta reported deaths.
L. monocytogenes infections were most commonly reported in the age group over 64. In 2022, 70.9% of listeriosis cases were reported in this age group. Within fatal cases of listeriosis, 59.8% were in the age group 65–84 years, while 24.3% were in the age group > 84 years.
3.4.3. Listeria monocytogenes in RTE food
Data collected in the context of Regulation (EC) No 2073/2005
In total, 19 MSs reported data in the context of the FSC according to the specifications mentioned above (Section 3.3.1) for 11 RTE food categories (Table 33).
Overall L. monocytogenes occurrences reported from official sampling were low, both at distribution and manufacturing (from 0% to 2.6%). Food categories for which data were reported both at manufacturing and distribution showed lower occurrences at distribution. The highest occurrences (from 2.3% to 2.6%) were found at distribution for ‘fish’, and at manufacturing for ‘fish’, ‘fish and fishery products’ and ‘products of meat origin, other than fermented sausages’.
For all food categories, the proportion of samples exceeding the limit of the food safety criteria at distribution (100 CFU/g) was rare to very low (0% to 0.30%).
For a further interactive look at L. monocytogenes monitoring results, dashboards have been created (different filters can be applied to query the data) (here).
The below text summarises results for the major food categories according to the criteria described in Section 3.3.2.
Other monitoring data for Listeria monocytogenes in RTE food
Fish and fishery products, RTE
In 2022, 21 MSs and 2 non‐MSs (Iceland and Serbia) reported detection data for fish or fishery products. In the EU, as in previous years, the occurrence of L. monocytogenes remained one of the highest in all RTE food categories, with an overall mean of 7.1% (N = 9727), varying from 0% and 20.0% according to the MS. The number of tested samples from fish remained particularly high for Poland. Poland contributed 50.6% of tested units (4921 and 5812 tested samples reported in 2022 and 2021, respectively). Excluding Poland, three MSs (Italy, the Netherlands and Spain) contributed 62% of the remaining reported data for these categories.
Meat and meat products, RTE
In 2022, 20 MSs and 4 non‐MSs (Iceland, Montenegro, Republic of North Macedonia and Serbia) reported detection data for meat and meat products.
In the EU, the overall occurrence of L. monocytogenes, all matrices included, was 2.1% (N = 60,952 tested units for detection), varying from 0% to 13.8% according to the MS. 69.1% of reported data were provided by Poland. Excluding Poland, five MSs contributed 76% of remaining reported data (Bulgaria, Czechia, Italy, Romania and Spain). In all, 59.8% of tested units were assigned to the four main animal species (pigs, bovine animals, broilers and turkeys). The remaining 40.2% of tested sampling units were reported from other or unspecified animals. RTE meat and meat products from pigs were the most frequently tested (52.7%). RTE meat and meat products from bovine animals, broilers and turkeys represented 4.4%, 1.8% and 0.21% of all tested units, respectively.
Pork products
Eighteen MSs and three non‐MSs (Iceland, Republic of North Macedonia and Serbia) reported data for RTE pig meat products. In the EU, the overall occurrence of L. monocytogenes showed a continuous decrease by half from 2019 to 2022: 1.9% in 2022 (N = 32,090), 2.6% in 2021 (N = 24,736), 3.0% in 2020 (N = 6585) and 4.2% in 2019 (N = 14,035). As in previous years, four MSs provided 89.5% of data on pork meat products (Czechia, Poland, Romania and Spain) with 63.3% of data provided by Poland (N = 20,306).
Poultry meat products (broilers and turkeys)
Twelve MSs and one non‐MS (Montenegro) reported data for RTE poultry meat products. In the EU, the overall occurrence of L. monocytogenes in RTE poultry meat products was 0.64% (N = 1248). This low occurrence is comparable with previous years: 1.3% (N = 895) in 2021 and 0.65% (N = 464) in 2020. No positive samples were detected in RTE meats from turkeys in 2022 (N = 129). In 2022, five MSs provided 90.5% of data on poultry meat products (Bulgaria, Czechia, Hungary, Poland and Romania).
Bovine meat products
Seventeen MSs and one non‐MSs (Serbia) reported data for RTE bovine meat products. In the EU, the overall occurrence of L. monocytogenes reported in RTE bovine meat products was 4.9% (N = 2712). Five MSs provided 89.6% of data on bovine meat products (Czechia, Italy, Luxembourg, the Netherlands and Poland). For comparison, occurrences were 3.9% in 2021 (N = 2217), 7.4% in 2020 (N = 856) and 4.2% in 2019 (N = 1248).
Milk and milk products, RTE
In 2022, 21 MSs and 4 non‐MSs (Albania, Montenegro, Republic of North Macedonia and Serbia) reported data for RTE milk and milk products, all categories included. 44% of tested units for detection were provided by Poland. 84% of the remaining data were provided by seven MSs (Bulgaria, Czechia, Hungary, Italy, the Netherlands, Romania and Spain).
In the EU, the overall occurrence of L. monocytogenes in RTE milk products, all matrices included, was 0.37% (N = 52,045 tested units for detection). This overall occurrence was 0.18% for cheeses from pasteurised milk (N = 9559), 1.3% (N = 2221) for cheeses from raw milk or low heat‐treated milk and 0.87% for milk (N = 2422). As in previous years, cheeses made from raw or low heat‐treated sheep milk presented the highest occurrence of this food category (soft and semi‐soft cheese: 2.0%, N = 147; hard cheese: 2.4%, N = 209). Eight MSs (Bulgaria, Czechia, Hungary, Italy, the Netherlands, Poland, Romania and Spain) provided 91.2% of data. Additionally, 42.6% of data were assigned to milk or specified cheeses of bovine, goat or sheep origin. The remaining data were reported from other dairy products and cheeses made from mixed milk or unspecified animals. Among assigned tested samples, 62.6% of cheese samples and 85.0% of milk samples were of bovine origin.
Fruits, vegetables and juices, RTE
Sixteen MSs reported data for RTE fruits, vegetables and juices. The overall occurrence was 2.6% (N = 1435). A total of 83.3% of data were reported by six MSs (Bulgaria, Hungary, Italy, Romania, Slovenia and Spain).
3.4.4. Listeria spp. in animals
In 2022, 10 MSs, Northern Ireland and 2 non‐MSs (Republic of North Macedonia and Switzerland) reported 22,459 data points in several animal categories (food‐producing, wild‐, zoo‐ and pet animals, including birds) from different species.
In the EU, reported data (Table 34) were mainly results from ‘animals’ (86.0%, N = 19,248) compared with other sampling unit levels (‘herd/flock’ and ‘holding’). Considering all sampling unit levels, cattle were the major animal species concerned by Listeria testing (59.1% of total units tested), followed by small ruminants (30.7%) and pigs (7.6%). The percentages of positive units for Listeria spp. in these animals were 1.2%, 5.8% and 0.35%, respectively. The sample size, as well as the sampling strategy and the proportion of positive units varied considerably among the reporting countries and animal species. In all, 88.6% of EU data were reported by three MSs: the Netherlands (49.9%), Ireland (23.7%) and Italy (15.0%).
TABLE 34.
Summary of Listeria species statistics relating to major animal species, MSs, 2022.
| Animal species | N reporting MSs | N tested units | % positive units | N positive units for L. monocytogenes | N positive units for L. Ivanovii | N positive units for L. innocua | N positive units for other listeria species |
|---|---|---|---|---|---|---|---|
| Cattle | 11 | 13,227 | 1.2 | 115 | 0 | 6 | 34 |
| Sheep and goats | 11 | 6857 | 5.8 | 300 | 83 | 1 | 77 |
| Pigs | 4 | 1696 | 0.35 | 5 | 0 | 1 | 0 |
| Others | 7 | 590 | 5.4 | 20 | 1 | 0 | 11 |
| Total EU | 11 | 22,370 | 2.9 | 440 | 84 | 8 | 122 |
Among the positive units for Listeria (N = 654), 67.3% were reported as L. monocytogenes. Only limited positive findings were reported as L. ivanovii (12.8%) and L. innocua (1.2%). As in previous years, many positive findings for Listeria (18.7%) were reported as other or unspecified species.
3.5. Discussion
In 2022, the number of confirmed cases of human listeriosis was 2738, corresponding to an EU notification rate of 0.62 per 100,000 population and resulting in an increase of 15.9% in the notification rate compared with the rate in 2021. This was the highest rate and number of cases reported in the EU since the beginning of EU‐level surveillance in 2007. Listeriosis was the fifth most commonly reported zoonosis in humans in the EU in 2022, and one of the most serious foodborne diseases under EU surveillance due to the high rate of hospitalisations, and elevated morbidity and mortality, particularly among elderly people.
In 2022, there was a progressive increase of cases of listeriosis (+15.8% vs. 2021), which could be partially explained by the increase of outbreak cases specifically in Austria, Belgium, Denmark, Finland, Germany, Hungary, Italy and Spain. However, the general EU trend for listeriosis in 2018–2022 showed no significant increase or decrease, except for some MSs (Austria, Denmark, France and Hungary) with a significant increase, and for Estonia with a statistically relevant decrease.
The listeriosis notification rate increased in the last year (0.62 in 2022 vs. 0.53 in 2021). Listeriosis continues to be one of the foodborne infections with the highest number of hospitalisations and fatal cases in the EU. L. monocytogenes infections were most commonly reported in the age group over 64. Within fatal cases of listeriosis, 59.8% of cases were in the age group 65–84 years, while 24.3% were in the age group > 84 years. Clinical symptoms are most severe in susceptible populations (elderly people over 65, pregnant women, newborns and immunocompromised people) and include fever, meningitis and septicaemia and require hospitalisation and medical treatment and subsequent notification to the national health system (Radoshevich & Cossart, 2018; Quereda et al., 2021). With the ageing of the European population (21% of the European population is over 65) (Eurostat, 2022) and the increase in chronic age‐related diseases (EFSA BIOHAZ Panel, Koutsoumanis, Alvarez‐Ordóñez, Bolton, et al., 2020), more people are entering the high‐risk categories for severe forms of Listeria infections. Outbreaks, mainly relating to the consumption of RTE foods (cold smoked salmon, meat and meat products, dairy products and frozen vegetables) are not necessarily linked to social and community events, but to consumption of these RTE foods in households (ECDC and EFSA, 2018a, 2018b, 2019). Particularly, it is important to continue raising awareness of listeriosis and its risks associated with certain consumption habits and types of food in risk groups (ECDC and EFSA, 2018a, 2018b; EFSA BIOHAZ Panel et al., 2018; ECDC and EFSA, 2019; Fernández‐Martínez et al., 2022; Halbedel et al., 2023).
The molecular characterisation of clinical isolates of Listeria is based on WGS, combined with core genome multi‐locus sequence typing (cgMLST) for strain typing. Almost all MSs have moved from pulsed‐field gel electrophoresis (PFGE) (Fernández‐Martínez et al., 2022; Halbedel et al., 2023) to WGS (ECDC, 2019), ensuring greater accuracy in typing L. monocytogenes. Prior to the use of WGS, a system of rapid and accurate identification of clusters was lacking in sensitivity and, at the European level, many outbreaks were not detected early (Van Walle et al., 2018).
In the food sector, we observed an overall increase of the number of tested units in RTE products (+26.3% in 2022 compared with 2021). The sampling effort at manufacturing and distribution remained focused on RTE products of animal origin. The occurrence of L. monocytogenes as assessed from detection results reported by MSs (covering objective sampling of single samples and batches) varied according to the food category and sample stage. Occurrences remained generally rare to low in RTE foods. The highest values were observed for fish and fishery products (7.1%), meat products from bovines (4.9%), fruits and vegetables (2.6%), and hard cheeses from raw or low heat‐treated sheep milk (2.4%). Interestingly, there has been a decrease in the prevalence of L. monocytogenes in RTE pig meat between 2019 and 2022, from 4.2% to 1.9%.
As in previous years, the highest proportions of positive official control samples, as part of verification of L. monocytogenes FSC, were observed at manufacturing compared with distribution. The results from official sampling showed that the proportion (%) of samples at distribution exceeding the limit of 100 CFU/g was rare to very low (< 1.0%) in 9 out of 10 focussed RTE food categories. The highest proportion at distribution was observed for ‘fish’ (2.3%).
In primary production, cattle were the most frequently sampled animal species and presented a low proportion of positive units (1.2%).
Interpreting national data and trends for the occurrence of L. monocytogenes in food or animals over time must be carried out with caution. Currently, surveillance data come from systems that are not fully harmonised and that vary in nature and effectiveness depending on the MS. Moreover, data may be reported by a limited number of MSs depending on each food/animal category.
Combining human, animal and food epidemiological data with molecular and genotyping data provides an efficient methodology to better understand the ecology of this pathogen at different stages of the food chain and will improve the investigation of listeriosis outbreaks affecting one or more MSs (ECDC, EFSA and ANSES, 2021). L. monocytogenes surveillance in the EU currently uses tools based on genotyping to characterise food and animal contamination and listeriosis outbreaks. ECDC and EFSA are working jointly to quickly identify outbreaks. In 2022, the EFSA One Health WGS System that interoperates with the ECDC Molecular Typing system was opened to MSs for the exchange of cgMLST profiles and minimum metadata (EFSA, Costa, et al., 2022). The aim is to collect typing information to detect clusters of foodborne disease and to generate hypotheses on the possible food vehicles involved, supporting risk managers. At the international level, the joint FAO/WHO expert meetings on microbial risk assessment (JEMRA) recommended expanding risk assessments on L. monocytogenes in RTE food incorporating a primary‐production‐to‐consumption perspective, and reviewing groupings of susceptible populations (FAO and WHO, 2022). Models for the risk assessment of L. monocytogenes for lettuce, cantaloupe, frozen vegetables and RTE fish were developed, and recommendations have been made to conduct a possible revision of the Guidelines on the Application of General Principles of Food Hygiene to the Control of Listeria monocytogenes in Foods (CXG 61–2007). FAO and WHO also established a roster of experts in 2022 to obtain more representative data on L. monocytogenes in foods and to develop a new, full farm‐to‐table risk assessment.
4. SHIGA TOXIN‐PRODUCING ESCHERICHIA COLI (STEC)
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here, and are also retrievable from the EFSA Shiga toxin‐producing Escherichia coli dashboard available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
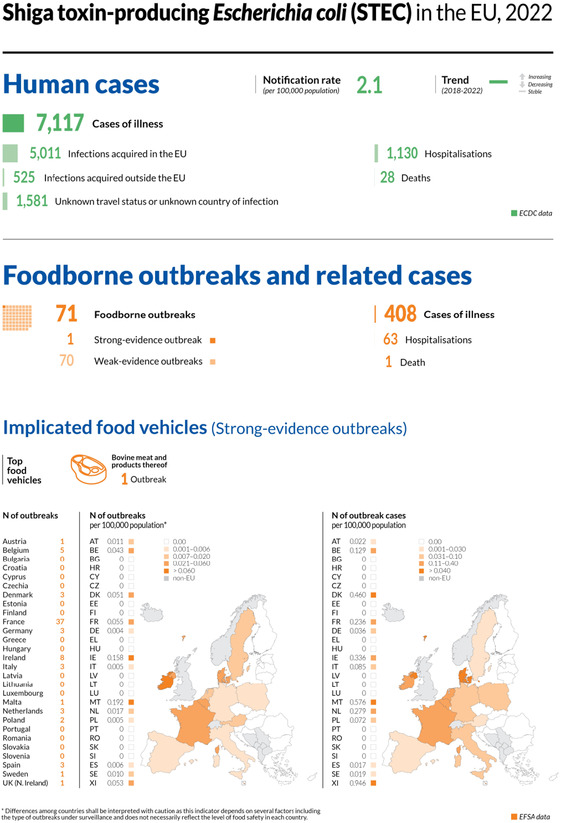
4.1. Key facts
STEC infections were the fourth most reported gastrointestinal foodborne illnesses in humans in the European Union.
In 2022, there were 7117 confirmed cases of human STEC infections, corresponding to an European Union notification rate of 2.1 cases per 100,000 population. This was an increase of 8.8% compared with 2021 (1.9 cases per 100,000 population).
The overall trend for STEC infections did not show any significant increase or decrease in the 2018–2022 period.
Nine Member States tested 472 official control samples of ‘sprouted seeds’ in the context of Regulation (EC) No 2073/2005 25 taken at retail and processing plants, with no positive results.
In 2022, 1.1% of 8556 ‘ready‐to‐eat’ food sampling units reported by 15 Member States were positive for STEC, with positive sampling units originating from ‘milk and milk products’ (1.7% positives), ‘meat and meat products’ (1.0%) and ‘fruits, vegetables and juices’ (0.14%). Of the 10,259 ‘non‐ready‐to‐eat’ sampling units reported by 18 Member States, 2.5% were positive, with the highest level of contamination (3.3%) in ‘meat and meat products’. Overall, STEC were isolated from 347 sampling units, with ‘fresh meat from sheep’ and ‘other fresh meat’ showing the highest percentages of STEC‐positive sampling units of 6.1% and 7.6%, respectively.
In 2022, STEC were detected by four Member States in five different animal categories. Most of the units tested in the European Union (N = 1916) were from ‘goats and sheep’ (N = 1300) and the proportion of positives was 1.3%. The proportions of positive sampling units from ‘cattle', ‘pigs’, ‘other ruminants’ and ‘other animals’ were 41.5%, 0%, 6.7% and 0.81%, respectively.
4.2. Surveillance and monitoring of STEC infections in the EU
4.2.1. Humans
For 2022, 26 MSs reported information on STEC infections in humans.
STEC surveillance is mandatory in 24 MSs and voluntary in two MSs (Belgium, France) and based on another system in Italy.
The EU case definition was used by 24 countries. Three countries reported using a different case definition (France, Germany and the Netherlands).
All MSs except Italy indicated that the surveillance system is comprehensive. The surveillance systems for STEC infections cover the whole population in all EU MSs except for three MSs (France, Italy and Spain). The notification rates were not calculated in two of these countries for the following two reasons: (a) in France, STEC surveillance in humans is based on paediatric haemolytic‐uraemic syndrome (HUS) cases; (b) in Italy, STEC surveillance is sentinel and primarily based on the HUS cases reported through the national registry for HUS. For Spain, population coverage of STEC cases was estimated at 97% for 2022. No estimate of population coverage in Spain was provided prior 2021, so notification rates were not calculated.
Twenty‐five MSs reported case‐based data, whereas Bulgaria reported aggregated data.
4.2.2. Food and animals
STEC data in the context of Regulation (EC) No 2073/2005, STEC food safety criterion for sprouts and seeds at the distribution level
The food safety criterion (Regulation (EC) No 2073/2005) specifies that sprouts placed on the market during their shelf‐life shall not contain detectable STEC O157, O26, O111, O103, O145 or O104:H4 in 25 g of product. The ISO TS 13136:2012 method with the adaptation developed by the EURL for E. coli for detecting O104:H4 is indicated as the reference testing methodology. FBOps are also allowed to use alternative methods validated according to the requirements of ISO 16140.
Nevertheless, the sampling objectives and the sampling frequency vary or are interpreted differently among MSs, resulting in non‐harmonised data.
Other STEC monitoring data from food and animals
All the other food and animal testing data originate from the reporting obligations of MSs under Directive 2003/99/EC 26 (i.e. the Zoonoses Directive). Due to the absence of explicitly indicated sampling strategies in this directive, the data generated by MSs are based on investigations with non‐harmonised sampling programmes. Therefore, STEC monitoring data according to Directive 2003/99/EC are not comparable between MSs and preclude assessing temporal and spatial trends at the EU level.
In certain food categories, different sampling designs and inaccuracies due to limited numbers of samples also preclude an accurate estimation of prevalence.
Nevertheless, descriptive summaries of sample statistics at the EU level can be compiled and used to indicate the circulation of certain STEC types in food and animals, provided that the above‐mentioned relevant limitations of the data set are taken into consideration.
Recently, following risk assessment exercises, it has been recommended that the presence of the main virulence genes be reported (FAO and WHO, 2018; NACMCF, 2019; EFSA BIOHAZ Panel, Koutsoumanis, Allende, Alvarez‐Ordonez, et al., 2020). Moreover, considerations relating to the virulence of the different STEC types underlined the importance of determining the virulence gene combinations (virulotypes) of the isolated STEC strains, with an emphasis on stx gene subtyping (EFSA BIOHAZ Panel, Koutsoumanis, Allende, Alvarez‐Ordonez, et al., 2020).
EFSA story map on STEC
The EFSA story map on STEC (available here) is a new interactive communication tool developed by EFSA and geared to the general public. This story map provides general information on the pathogen and its epidemiology, including information on where the pathogen can be found, how people and animals get infected, the occurrence of this pathogen in different sources, the disease it causes and how to prevent infection. In addition, this story map also illustrates the monitoring activities implemented in the EU and the role of EFSA with respect to these activities. Users can easily display and explore the content of the different sections in the story map, browsing the dynamic maps, images, text and multimedia features.
4.3. Data analyses
4.3.1. Occurrence in food and animals
The monitoring data on sprouts as part of Regulation (EC) No 2073/2005 were aggregated and summarised for trend watching according to the following ‘filters’: Sampling context: ‘surveillance, based on Regulation No 2073/2005’; Sampling unit type: ‘single'; Sampling stage: ‘distribution’; Sampling strategy: ‘objective sampling’ and Sampler: ‘official sampling’.
For the description of the occurrence of STEC‐positive sampling units in the different food categories, the subset of the monitoring data with ‘objective sampling’ specified as sampling strategy was used (N = 18,815), meaning that the reporting MSs collected the sampling units according to a planned strategy based on the selection of random samples statistically representative of the population to be analysed.
4.3.2. Serogroups and virulence features in food and animals
In 2022, the methods targeting any STEC were based on stx gene PCR and included the ISO TS 13136:2012 method (ISO, 2012), other PCR‐based methods and commercial kits using the same principle. The methods designed to detect only E. coli O157 were the ISO 16654:2001 method (ISO, 2001), the NMKL 164:2005 method (NMKL, 2005), the DIN 10167:2004–03 (DIN, 2004) method, and the AFNOR BIO 12/25 05/09, ELFA method for E. coli O157. The method indicated as the OIE method for E. coli O157 is an adaptation of the ISO 16654:2001 method used for animal samples (WOAH, 2023).
For the descriptive analyses of STEC findings in food and animals, primarily those on virulence gene types and on their frequency distribution, the full data set, regardless of the sampling strategy but with the exclusion of the samples assayed with methods detecting E. coli O157 only, was used (N = 22,401 for food and N = 1279 for animals).
EFSA dashboard on STEC
The EFSA dashboard on STEC (available here) is a graphical user interface for searching and querying the large amount of data collected each year by EFSA from EU MSs and other reporting countries based on Zoonoses Directive 2003/99/EC. The STEC dashboard shows summary statistics for the monitoring results for the pathogen with regard to major food categories, and the occurrence of STEC in major food categories and animal species. STEC data and related statistics can be displayed interactively using charts, graphs and maps in the online EFSA dashboard. In this tool, the main statistics can also be viewed and downloaded in tabular format. Detailed information on the use and features of the STEC dashboard can be found in the user guide that can be downloaded from the online tool. Links to the dashboard are available in the relevant sections of this chapter.
4.4. Results
4.4.1. Overview of key statistics, EU, 2018–2022
Table 35 summarises EU‐level statistics on human STEC infections and on sampling units from food and animals tested for STEC during 2018–2022. Food and animal data were classified into major categories and aggregated by year to obtain an annual overview of the volume of data submitted. Noteworthily, the number of foodborne outbreaks caused by STEC in 2022 increased by 129.0% with respect to the same figure reported in 2021. More detailed descriptions of these statistics are provided in the below subsections and in the chapter on foodborne outbreaks.
TABLE 35.
Summary of STEC statistics relating to humans, major food categories and the main animal species, EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 7117 | 6406 | 4489 | 7801 | 8167 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 2.1 | 1.9 | 1.5 | 2.1 | 2.3 | ECDC |
| Number of reporting MSs | 26 | 27 | 27 | 28 | 28 | ECDC |
| Infection acquired in the EU | 5011 | 4365 | 3370 | 4836 | 5783 | ECDC |
| Infection acquired outside the EU | 525 | 117 | 148 | 751 | 693 | ECDC |
| Unknown travel status or unknown country of infection | 1581 | 1924 | 971 | 2214 | 1691 | ECDC |
| Number of foodborne outbreak‐related cases | 408 | 275 | 208 | 273 | 390 | EFSA |
| Total number of foodborne outbreaks | 71 | 31 | 34 | 42 | 50 | EFSA |
| Food c | ||||||
| Meat and meat products | ||||||
| Number of sampling units | 9932 | 12,160 | 10,866 | 14,110 | 9250 | EFSA |
| Number of reporting MSs | 21 | 19 | 17 | 20 | 17 | EFSA |
| Milk and milk products | ||||||
| Number of sampling units | 5957 | 4094 | 4665 | 5479 | 5339 | EFSA |
| Number of reporting MSs | 14 | 11 | 10 | 13 | 14 | EFSA |
| Fruits and vegetables (and juices) | ||||||
| Number of sampling units | 2975 | 4044 | 3398 | 2696 | 3371 | EFSA |
| Number of reporting MSs | 15 | 16 | 15 | 13 | 13 | EFSA |
| Animals d | ||||||
| Cattle (bovine animals) | ||||||
| Number of sampling units | 282 | 3316 | 868 | 1615 | 1112 | EFSA |
| Number of reporting MSs | 3 | 5 | 3 | 7 | 5 | EFSA |
| Small ruminants (sheep, goats) and deer | ||||||
| Number of sampling units | 1456 | 151 | 227 | 320 | 188 | EFSA |
| Number of reporting MSs | 3 | 2 | 2 | 6 | 4 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States; STEC, Shiga toxin‐producing Escherichia coli.
For the 2021–2022 period, data on animal samples from the United Kingdom (Northern Ireland) were considered. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were considered for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Number of sampling units was obtained by totalling all sampling units (single, batch), sampling stages (Automatic distribution system for raw milk, Border Control Posts, Canteen or workplace catering, Catering, Cutting plant, Distribution: wholesale and retail sale, Farm, Game handling establishment, Hospital or medical care facility, Household, Hunting, Manufacturing, Mobile retailer or market/street vendor, Packing centre, Primary production, Processing plant, Restaurant or Cafe or Pub or Bar or Hotel or Catering service, Retail, Road transport, School or kindergarten, Slaughterhouse, Storage, Takeaway or fast‐food outlet, Unspecified and Wholesale), sampling strategies (convenience sampling, objective sampling, selective sampling and suspect sampling) and samplers (official sampling, industry sampling and HACCP and own check).
Number of sampling units was obtained by totalling all sampling units (animals, holdings and herds or flocks), sampling stages at primary production (farm, natural habitat, slaughterhouse, veterinary activities and zoo), sampling strategies (convenience sampling, objective sampling and suspect sampling) and samplers (industry sampling, official sampling and private sampling).
For a further interactive look at STEC monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
4.4.2. STEC infections in humans
In 2022, 7117 confirmed cases of STEC infections were reported in the EU (Table 36). Twenty‐three MSs reported at least one confirmed STEC case and three MSs reported zero cases (Bulgaria, Cyprus and Lithuania). In 2022, the EU notification rate was 2.1 per 100,000 population. For 2022, there was an increase of 8.8% in the annual notification rate reported compared with year 2021 (1.9 cases per 100,000 population).
TABLE 36.
Reported confirmed human cases of STEC and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National Coverage a ) | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 469 | 5.2 | 383 | 4.3 | 288 | 3.2 | 284 | 3.2 | 305 | 3.5 |
| Belgium | Y | C | 181 | 1.6 | 124 | 1.1 | 84 | 0.73 | 131 | 1.1 | 112 | 0.98 |
| Bulgaria | Y | A | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Croatia | Y | C | 16 | 0.41 | 12 | 0.30 | 8 | 0.20 | 22 | 0.54 | 10 | 0.24 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | Y | C | 58 | 0.55 | 36 | 0.34 | 32 | 0.30 | 33 | 0.31 | 26 | 0.25 |
| Denmark | Y | C | 413 | 7.0 | 928 | 15.9 | 445 | 7.6 | 623 | 10.7 | 493 | 8.5 |
| Estonia | Y | C | 11 | 0.83 | 7 | 0.53 | 10 | 0.75 | 6 | 0.45 | 7 | 0.53 |
| Finland | Y | C | 291 | 5.2 | 288 | 5.2 | 175 | 3.2 | 311 | 5.6 | 210 | 3.8 |
| France b | N | C | 473 | – | 298 | – | 262 | – | 335 | – | 259 | – |
| Germany | Y | C | 1873 | 2.3 | 1635 | 2.0 | 1409 | 1.7 | 1907 | 2.3 | 2226 | 2.7 |
| Greece | Y | C | 14 | 0.13 | 10 | 0.09 | 3 | 0.03 | 5 | 0.05 | 1 | 0.01 |
| Hungary | Y | C | 26 | 0.27 | 24 | 0.25 | 8 | 0.08 | 23 | 0.24 | 14 | 0.14 |
| Ireland | Y | C | 892 | 17.6 | 878 | 17.5 | 734 | 14.8 | 798 | 16.3 | 966 | 20.0 |
| Italy b | N | C | 118 | – | 65 | – | 45 | – | 62 | – | 73 | – |
| Latvia | Y | C | – | – | 13 | 0.69 | 2 | 0.10 | 48 | 2.5 | 3 | 0.16 |
| Lithuania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | Y | C | 9 | 1.4 | 10 | 1.6 | 0 | 0 | 4 | 0.65 | 3 | 0.50 |
| Malta | Y | C | 78 | 15.0 | 68 | 13.2 | 43 | 8.4 | 53 | 10.7 | 41 | 8.6 |
| Netherlands | Y | C | 585 | 3.3 | 484 | 2.8 | 323 | 1.9 | 459 | 2.7 | 488 | 2.8 |
| Poland | Y | C | 34 | 0.09 | 7 | 0.02 | 3 | 0.01 | 14 | 0.04 | 6 | 0.02 |
| Portugal | Y | C | 6 | 0.06 | 2 | 0.02 | 5 | 0.05 | 1 | 0.01 | 2 | 0.02 |
| Romania | Y | C | 28 | 0.15 | 6 | 0.03 | 14 | 0.07 | 36 | 0.19 | 20 | 0.10 |
| Slovakia | Y | C | 4 | 0.07 | 5 | 0.09 | 1 | 0.02 | 3 | 0.06 | 12 | 0.22 |
| Slovenia | Y | C | 58 | 2.8 | 48 | 2.3 | 30 | 1.4 | 31 | 1.5 | 32 | 1.6 |
| Spain c | N | C | 623 | 1.3 | 422 | 0.89 | 74 | – | 269 | – | 126 | – |
| Sweden | Y | C | 857 | 8.2 | 653 | 6.3 | 491 | 4.8 | 756 | 7.4 | 892 | 8.8 |
| EU Total 27 | 7117 | 2.1 | 6406 | 1.9 | 4489 | 1.5 | 6214 | 2.0 | 6327 | 2.2 | ||
| United Kingdom d | – | – | – | – | – | – | 1587 | 2.4 | 1840 | 2.8 | ||
| EU Total | 7117 | 2.1 | 6406 | 1.9 | 4489 | 1.5 | 7801 | 2.1 | 8167 | 2.3 | ||
| Iceland | Y | C | 4 | 1.1 | 7 | 1.9 | 4 | 1.1 | 27 | 7.6 | 3 | 0,86 |
| Norway | Y | C | 518 | 9.6 | 437 | 8.1 | 331 | 6.2 | 511 | 9.6 | 494 | 9.3 |
| Liechtenstein | Y | C | 4 | 10.2 | 7 | 18.0 | 710 | 8.2 | 962 | 11.2 | 879 | 10.3 |
| Switzerland e | Y | C | 1191 | 13.6 | 927 | 10.7 | ||||||
Abbreviations: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Sentinel surveillance; mainly haemolytic‐uraemic syndrome (HUS) cases are notified. Notification rate not calculated.
Sentinel system; notification rates calculated with an estimated population coverage of 97% in 2021–2022. No information on estimated coverage in 2018–2020, so notification rate cannot be estimated.
Cases reported by the United Kingdom for the period 2018–2019 were also considered for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided the data directly to EFSA. The human data for Switzerland include data from Liechtenstein for years 2018–2020.
The highest country‐specific notification rates among the EU MSs were observed in Ireland, Malta, Sweden and Denmark (17.6, 15.0, 8.2 and 7.0 cases per 100,000 population, respectively). Three countries (Portugal, Slovakia and Poland) reported ≤ 0.09 cases per 100,000 population.
Most STEC cases reported were infected in the EU (90.4% domestic cases or travel‐associated in the EU, 9.5% acquired outside the EU, excluding those with unknown travel status or no information on the country of infection, representing 21.9% of the total cases reported) (Table 35). Overall, for year 2022, 95.7% of the 5011 reported STEC cases in humans who acquired the infection in the EU (Table 35) were domestic (acquired within the home country), and 4.3% of the cases were acquired through travel in another EU country. The proportion of human STEC cases infected within the EU remained stable during 2018–2022.
In 2022, the number of cases infected through travel outside the EU showed an increase compared with the pandemic years 2020–2021. However, it is still lower than that reported in 2018–2019. The proportion of cases infected through travel outside the EU in 2022 was 7.4%, whereas it was 10.6% in 2019 in 8.4% in 2018 (Table 35).
Sweden, Germany, the Netherlands and Finland reported the highest number of travel‐associated cases (245, 176, 124 and 87, respectively), altogether representing 82.8% of all imported cases (EU and non‐EU).
Spain, Greece, Italy and Croatia were the most frequently reported as the probable country of infection within the EU (20.6%, 11.4%, 10.5% and 8.8%, respectively). Regarding non‐EU countries, Türkiye was the most frequently reported as the probable country of infection, followed by Egypt and Morocco (30.3%, 18.6% and 4.5%, respectively).
The seasonal trend in confirmed STEC cases was maintained in 2018–2022, with more cases reported during the summer months (Figure 9). The observed STEC infection seasonality is in line with that reported in the literature (Sapountzis et al., 2020). The overall trend for STEC in 2018–2022 did not show any significant increase or decrease. At the MS level, a significant increasing trend (p < 0.05) was observed over the same time span in Austria, France, Spain and Malta. No countries reported decreasing trends from 2018 to 2022.
FIGURE 9.
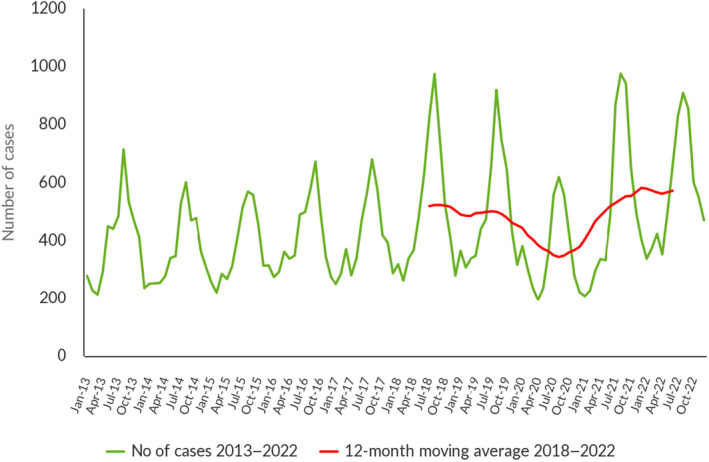
Trends in reported confirmed human cases of STEC infection in the EU by month, 2013–2022. Source: Austria, Belgium, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain and Sweden.
The reported cases were distributed across all age classes with a marked peak in those corresponding to paediatric ages (0–19 years, 44.1% of all cases with the information on the patient's age), particularly in children aged 0–9 years, representing 34.8% of all cases with information on the patient's age.
Out of the 2933 cases with known hospitalisation status, 38.5% were hospitalised. Seventeen MSs provided information on hospitalisation for 41.2% of all confirmed STEC cases in the EU in 2022. The highest proportions of hospitalised cases were reported by Greece, Portugal and Slovakia (100% each, out of the cases with known hospitalisation status). However, these MSs only reported a few cases of infection (14,6 and 2, respectively). Other MSs also reporting high proportions of hospitalised cases were Italy (83.1%), Poland (82.4%) and Romania (75.0%). Noteworthily, the high proportion of hospitalised cases observed in Italy is due to the sentinel surveillance system, which is mainly based on HUS notification. France, with similar system based on HUS notifications, did not report hospitalisation data. The overall proportion of hospitalised cases was similar to that observed in 2021.
A total of 562 HUS cases were reported in 2022, affecting mainly children aged 0–4 years; 20 of these cases were fatal, representing 71.4% of the total fatalities (28 cases) reported. As observed in 2021, the most common serogroups among HUS cases in 2022 were O26 (51.3% of all HUS cases with serogroup reported), O157 (14.5%), O80 (6.1%) and O145 (5.8%).
Nine MSs reported one to six fatal cases each and 12 MSs reported no fatal cases. This resulted in an EU case fatality rate of 0.6% among the 4911 confirmed cases with known outcome (69.0% of all reported confirmed cases). Deaths were mostly reported in the 65+ age group (42.9%) with and without HUS and followed by the 0–4 years age group (25.0%). In the youngest age group, all deaths were linked to HUS.
4.4.3. STEC in food
For year 2022, 23 MSs provided results from analyses of 21,692 food units (batches or single samples) regardless of the sampling strategy adopted and assayed with methods detecting any STEC.
The most recent and comprehensive source attribution analysis available for STEC underlined that ‘bovine meat and products thereof’, ‘milk and milk products’ and ‘vegetables, fruits and products thereof’ were the vehicles most frequently implicated in STEC infections in the EU during the 2012–2017 period (inclusive) (EFSA BIOHAZ Panel, Koutsoumanis, Allende, Alvarez‐Ordonez, et al., 2020), confirming the results of previous reports (FAO and WHO, 2018). These categories were indeed the most tested in the EU in 2022 and represented 87.2% of the total number of food samping units tested (N = 21,692). For a further interactive look at STEC monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
Data collected in the context of Regulation (EC) No 2073/2005
In the present report underpinned by 2022 data reported by MSs, requirements from Regulation (EU) 2017/625 27 (known as the Official Controls Regulation, OCR) were introduced for the first time. As opposed to previous legislation, Competent Authorities (CAs) must use methods complying with relevant internationally recognised rules or protocols including those that the CEN has accepted. This condition is met when EN ISO methods, which are ISO methods recognised by CEN, are used. Consequently, and in contrast to previous legislation, CAs cannot use the alternative methods mentioned in Commission Regulation (EC) No 2073/2005 when they carry out official controls aiming at verifying the correct implementation by FBOps of provisions of this Regulation. The implementation of this change in legislative testing requirements may have affected the 2022 results of official food control samples taken in the context of Commission Regulation (EC) No 2073/2005, compared with the 2021 and earlier results on similar samples, when requirements from the OCR were not yet implemented in EFSA's zoonoses data collection. For this reason, the above‐mentioned results should be interpreted with caution.
Regarding 2022 data for STEC on sprouted seeds in the context of Regulation (EC) No 2073/2005, 395 samples taken at the distribution level and 77 at processing plants were tested by nine MSs with no positive results. As noted in previous years, sprouted seeds are still not widely tested at the EU level, despite the microbiological criterion for this food commodity being laid down in Regulation (EC) No 2073/2005 since 2013. For a further interactive look at STEC data, look at the dashboards (here).
Other STEC monitoring data from food
Overall, 1.8% of the 18,815 food sampling units tested by 20 MSs and collected using an objective sampling strategy were positive for STEC. For years 2021, 2020, 2019 and 2018, the figures for the reported STEC‐positive food units were higher: 3.6%, 2.4%, 2.8% and 2.8%, respectively (EFSA and ECDC, 2022).
RTE food
As regards ‘ready‐to‐eat' (RTE) food, the testing of 8556 sampling units was reported. The food category with the highest number of sampling units tested was ‘milk and milk products’ with 4177 sampling units assayed, particularly cheeses (45.5%), followed by ‘fruits, vegetables and juices’ (17.3%) and ‘meat and meat products’ (13.4%). In total, 93 RTE food sampling units were found to be positive for STEC: 1.7% in ‘milk and milk products’ (particularly cheese), 1.0% in ‘meat and meat products’ (particularly those of bovine origin) and 0.14% in ‘fruits, vegetables and juices’.
RTE and non‐RTE food
To provide overall statistics, the following descriptive analyses are based on merged data from RTE food and non‐RTE food.
Meat and meat products
Bovine meat
In 2022, 5043 units of fresh and unprocessed bovine meat were tested by 16 MSs. At the distribution level, 1961 units were sampled by 14 MSs with 1.4% of positives. Sampling units taken at the manufacturing level (N = 3082) were the most contaminated (4.0%, 12 MSs). Most specimens sampled at the manufacturing level (78.6%) were taken at the slaughterhouse and 4.3% tested positive for STEC.
Sheep and goat meat
Small ruminants are an important reservoir of STEC (Persad & LeJeune, 2014). In 2022, five MSs reported the results of an investigation on 505 sampling units of fresh sheep meat with 6.1% of these being STEC‐positive, whereas two MSs reported on fresh goat meat with one STEC‐positive sampling unit out of the five tested.
The sampling stage that yielded the highest proportion of positive fresh sheep meat sampling units was the distribution level, with 9.2% of samples producing a STEC isolate. Conversely, the sampling units taken at the slaughterhouse showed a lower STEC contamination rate (4.8%).
Meat from other ruminants
In 2022, only two MSs provided information on the presence of STEC in 85 fresh deer meat samples with 16 positive sampling units (18.8%). The sampling units taken at the distribution and manufacturing levels displayed similar STEC contamination rates with 19.2% and 16.7%, respectively.
Meat from other animal species
Six MSs tested fresh pig meat in 2022 and reported data on 444 samples, with nine of these being positive for STEC (2.0%).
Fresh meat from animal species other than bovine, ovine, goat, pig and deer species, was tested in 2022 by four MSs that reported on analyses carried out on 146 sampling units. These included samples taken from poultry, ducks, wild and farmed game, horses, rabbits, wild boars, quail and meat from unspecified animal species. Two samples were reported as STEC‐positive (1.4%).
Meat products and meat preparations
Meat products and meat preparations other than fresh meat were sampled in 2022 by 13 MSs that tested 3494 sampling units, resulting in 41 isolated STEC strains (1.2%).
Milk and milk products
Overall, STEC were found in 69 (1.7%) out of 4177 sampling units of RTE milk and milk products reported by 10 MSs and in 19 (1.5%) out of 1306 sampling units of non‐RTE milk and milk products reported by 8 MSs.
In 2022, eight MSs reported on the testing of 1258 sampling units of raw cows' milk with 18 positive units (1.4%). Five MS reported monitoring results on 29 sampling units of raw goats' milk, and three MS reported only 10 samples of raw sheep milk. Neither category included positive samples.
The presence of STEC in RTE milk products other than milk and cheeses was reported by three MSs, which tested 173 sampling units of butter, cream, ice cream, yoghurt, whey and fermented dairy products. One positive sample was detected (0.6%).
For the cheese samples, 3893 samples were tested for the presence of STEC, with 67 (1.7%) positive units from 10 MSs in 2022.
Vegetables juices and fruits
STEC were found in two (0.09%) out of 2305 samples of juices, fruits and vegetables.
In total, 1184 sampling units of RTE spice and herbs, salads and sprouted seeds were tested, and two STEC‐positive units were reported (0.17%).
Other foodstuffs
This category contains miscellaneous food commodities not comprised in the previously mentioned categories, and included ‘cereals and meals’, ‘bakery products’, ‘fish and fishery products’, ‘infant formula’ and ‘other’. For the whole category, 1303 samples were analysed by eight MSs with nine (0.69%) positive samples reported from the ‘cereals and meals’ (7) and ‘bakery products’ (2) food categories.
For a further interactive look at STEC data, look at the dashboards (here), (different filters can be applied to query the data).
4.4.4. STEC in animals
For year 2022, results from 1916 sampling units (single heads or herds or flocks) from animals were reported by four MSs. The number of animals tested was about half (51.1%) of that assayed in 2021.
The most tested animal category in 2022 was goats and sheep, with 1300 sampling units tested (67.8% of all animal samping units tested) by three MSs and 1.3% positives. The highest prevalence of STEC was recorded in cattle with 41.5% of the total 282 sampling units being positive.
For a further interactive look at STEC data, look at the dashboards (here), (different filters can be applied to query the data).
4.4.5. Focus on STEC strain features: virulence genes and serogroups
Humans
In 2022, the information on the serogroups of STEC was reported for 47.4% of the human cases (N = 3374 cases of 7117 total confirmed STEC cases). The most frequently reported serogroups in the EU were O157 (22.3%) and O26 (20.0%). These two serogroups together represented 42.3% of the total number of confirmed human cases with known serogroups in 2022. The proportion of non‐typable STEC isolates decreased to 9.9% of the isolates with information on the serogroup reported, with respect to 2021 (26.1%).
Data on virulotypes (based on Shiga toxin genes stx1, stx2) were reported for 56.3% (N = 4009) and together with the intimin‐coding gene eae for 41.4% (N = 2944) of confirmed STEC infections in 2022. stx gene subtyping was provided for 27.1% (N = 1930) of the confirmed STEC infections. The most frequently reported virulence gene combination in strains isolated from severe STEC cases (HUS, bloody diarrhoea and hospitalised cases) was stx2+/eae+, accounting for 47.8% of these strains (Table 37). The proportion of the second most common virulotype stx1+/stx2+/eae + accounted for 16.6% of these cases (Table 37). The most common stx gene subtypes in strains from severe human infections were stx2a (43.9% of 665 isolates with reported stx gene subtyping data), stx1a (23.2%), stx2c (10.7%) and stx2b (7.4%) (here).
TABLE 37.
Virulotypes (stx type and presence of eae) identified in food, animal and human STEC isolates causing severe infection (haemolytic‐uraemic syndrome (HUS), hospitalisation and bloody diarrhoea) in 2022.
| Virulence gene profile | N of animal isolates in 2022 a | N of food isolates in 2022 a | N of human isolates in 2022 (%) | Relative frequency of the virulotype in b | ||
|---|---|---|---|---|---|---|
| HUS | Hospitalisation | Bloody diarrhoea | ||||
| stx2; eae+ | 14 | 37 | 410 (47.8) | 17.7 | 42.0 | 40.2 |
| stx1; stx2; eae+ | 9 | 32 | 142 (16.6) | 5.9 | 35.7 | 64.8 |
| stx2; eae‐ | 5 | 154 | 110 (12.8) | 2.7 | 24.3 | 14.8 |
| stx1; eae+ | 24 | 61 | 84 (9.8) | 1.2 | 27.4 | 27.3 |
| stx1; eae‐ | 4 | 50 | 59 (6.9) | 0.3 | 20.3 | 14.1 |
| stx1; stx2, eae‐ | 3 | 62 | 52 (6.1) | 1.4 | 15.3 | 19.4 |
| Total | 59 | 396 | 857 (100) | – | – | – |
Abbreviations: STEC, Shiga toxin‐producing Escherichia coli; HUS, haemolytic‐uraemic syndrome. The stx genes were characterised at the type level (stx1 and stx2).
Due to the low number of isolates virulotyped for food and animals, only the number of isolates is shown.
Relative frequencies (%) of the different combinations of stx gene types with or without the eae gene in STEC isolated from severe disease (TESSy data, 2012–2017) (EFSA BIOHAZ Panel, Koutsoumanis, Allende, Alvarez‐Ordonez, et al., 2020).
Food
The information on the serogroups of STEC strains from food was reported for 47.6% of the isolates (211 strains out of the total 443 strains). The six serogroups most reported in strains from human infections, namely O157, O26, O103, O146, O145 and O91, representing 60.9% of the human strains with the information on the serogroup (3374 strains in total), were also among the nine most frequent serogroups in food isolates.
Information on stx1 and/or stx2 and eae genes was provided for 396 (89.4%) of the 443 isolated STEC strains (Table 37). Only 104 STEC isolates were subtyped for the stx gene. As observed for human strains from severe disease, the most frequent stx gene subtype identified in STEC food isolates was stx2a, which was detected in 23.8% of the STEC strains with the information on the toxin gene subtypes. The EFSA dashboards on STEC (here) summarises the information on serogroups and virulotypes of strains isolated in 2022.
Animals
This section includes the analysis of the data relating to the 1279 animal sampling units tested with methods detecting any STEC, of which 10.3% (N = 132) were positive for the presence of STEC.
For the analysis of the distribution of STEC serogroups and virulotypes, all the 132 STEC strains isolated from animal samples were considered. Of these, 112 strains (84.8%) were provided with information on the serogroups. The isolates with a known serogroup belonged to 24 different O‐groups, with O171, O26 and O55 ranking first with 11 strains each. The dataset included also strains of O157 and O103 serogroups with seven and five isolates each.
For the analysis of the virulence genes, 59 STEC animal isolates (44.7%) were provided with their virulotype based on the identification of the stx1, stx2 and eae genes (Table 37). None of the 132 isolates from animal samples were provided with information on stx gene subtyping.
4.5. Discussion
In 2022, 26 MSs provided information on STEC infections in humans. The number of confirmed cases of STEC infections increased in 2022, with an 8.8% rise in the annual notification rate compared with 2021, now reaching the pre‐pandemic level. However, the overall trend of STEC infections during the 2018–2022 five‐year period did not show any significant increase or decrease.
In line with the lifting of the travel restrictions in place during COVID‐19, STEC infections acquired outside the EU sharply increased in 2022 compared with years 2020 and 2021, approaching the pre‐pandemic values. This increase was somewhat expected because the volume of international travel increased after the lifting of travel restrictions.
In 2022, almost half of the confirmed human cases reported by EU MSs had information on the serogroup with the most frequently reported being O157, followed by O26, O103 and O146. STEC strains belonging to these serogroups were also isolated from food samples in 2022. In contrast, considering the STEC strains isolated from HUS, the most common serogroup was O26 (over half of the cases), followed by O157, O80 and O145. The proportion of non‐typeable STEC isolates decreased to 9.9% with respect to 2021 (26.1%), but these non‐typeable isolates still accounted for the third most reported STEC serogroup in 2022. This high number of isolates for which the serogroup was not determined is possibly due to either the application of pheno/genotyping methods targeting only a reduced panel of serogroups or the laboratory skipping the serotyping procedure altogether. Similarly, less than half of the STEC isolates were reported with information on the presence of virulence genes (stx1 or stx2 and the eae genes), and about one third of the samples were provided with information on stx subtypes. HUS cases were reported in all age classes, with the highest proportion of patients in the youngest age group, 0–4 years. As in the previous year, most cases of death were reported in the 65+ age group, followed by the 0–4 years age groups, both being the age groups more prone to developing the more severe forms of the infection such as HUS.
In 2022, 23 MSs reported monitoring results of STEC in 21,692 food samples. The food categories most tested were ‘bovine meat and products thereof’, ‘milk and milk products’ and ‘vegetables, fruits and products thereof’, representing 87% of all food samples assayed. This selection of matrices takes into account those most frequently involved in STEC outbreaks as shown by the source attribution exercise (EFSA BIOHAZ Panel, Koutsoumanis, Allende, Alvarez‐Ordonez, et al., 2020).
In 2022, 1.8% of the total samples tested were positive for STEC, representing a remarkable decrease considering the proportion of positive samples recorded in the previous 4 years 2018–2021 (3.6%, 2.4%, 2.8% and 2.8%). The reason behind this decrease is not clear, because it does not appear to be caused by the contribution of a specific matrix or category of commodities, but rather by a generalised reduction of the positivity rates.
Overall, STEC were isolated in 1.1% of the tested RTE products; within this food group ‘milk and milk products’, particularly cheese, was the most contaminated matrix, 1.7%. Testing of RTE food commodities for STEC is important because these foods are consumed without any treatment to reduce or eliminate the possible presence of the pathogen, posing a direct risk to the consumer.
Meat from small ruminants was confirmed to be the most contaminated meat category: deer meat and sheep meat displayed the highest rates of contamination, 18.8% and 6.1%, respectively. Bovine meat samples taken at the manufacturing level were more contaminated (4.0%) than those collected at the distribution level (1.4%). The opposite situation was observed for sheep meat, in which the highest contamination level was observed at the distribution level.
As in the previous years, testing sprouted seeds was still not widely applied at the EU level, with only 472 official control samples taken in the context of Regulation (EC) No 2073/2005 and tested by nine MSs, with no positive results.
In 2022, the number of animal samples continued to decrease. The total number of these specimens was about half (N = 1916, 51.1%) of those tested in 2021 (N = 3746). As expected, the highest prevalence of positive STEC samples was detected in cattle (41.5%), followed by goats and sheep, which were the most reported animal categories.
In 2022, 47.6% of food isolates were provided with information on the O‐group. Interestingly, the six most reported serogroups in strains from human infections, namely O157, O26, O103, O146, O145 and O91, were among the nine most frequent serogroups in food isolates, in accordance with their zoonotic and foodborne origin.
Virulotyping of STEC isolates, namely the determination of the presence of the stx and eae virulence genes and especially of the stx gene subtypes, is the most informative strain feature for attempting to associate certain strains with the most severe forms of human infections. In 2022, approximately 90% of the food isolates were typed for stx and eae genes, but data on virulotypes was available for only 41.4% of human and 44.7% of the animal isolates. The stx gene subtype most frequently associated with the severe forms of human infections, stx2a (EFSA BIOHAZ Panel, Koutsoumanis, Allende, Alvarez‐Ordonez, et al., 2020 ), was also the one most frequently identified in food isolates. However, stx gene subtyping was provided for only 27.1% and 23.8% of the human and food isolates, respectively. The increase observed in virulotyping of food isolates seems to parallel a wider adoption of next‐generation sequencing in the food sector. Clearly, this typing technique enables a comprehensive characterisation of the isolates and should be encouraged in all sectors to promote a One Health approach to the assessment of the cases of disease in humans, the causative agent and the vehicles of infection. Detailed characterisation of the isolates has proven to be crucial in managing STEC outbreaks, particularly for the identification of the sources.
5. INFECTION WITH MYCOBACTERIUM TUBERCULOSIS COMPLEX (FOCUSING ON MYCOBACTERIUM BOVIS AND MYCOBACTERIUM CAPRAE)
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here, and are also retrievable from the EFSA Mycobacterium bovis/M. caprae dashboard available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
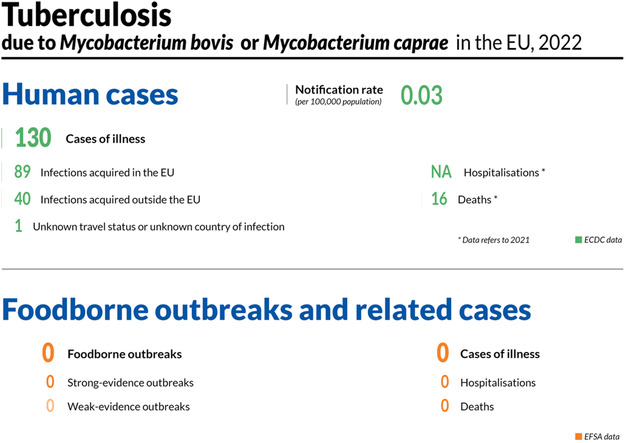
5.1. Key facts
In 2022, there were 130 confirmed cases of human tuberculosis due to M. bovis or M. caprae, corresponding to an European Union notification rate of 0.03 cases per 100,000 population. This resulted in a notification increase of 13.2% compared with 2021.
Cases of human tuberculosis due to M. bovis or M. caprae in the European Union progressively increased in both 2022 and 2021 following the drop observed in 2020, the first COVID‐19 pandemic year. In 2022, the number of human cases among the 27 Member States exceeded the number of cases reported in 2019.
In 2022, the M. bovis and M. caprae case notification rate was 0.03 cases per 100,000 among European Union Member States with disease‐free status and 0.04 per 100,000 in European Union Member States with non‐disease‐free status for the bovine population.
The majority of M. bovis and M. caprae cases in humans (68.5%) were of European Union origin (native cases and/or cases originating from other Member States).
In bovines, in 2022, the overall prevalence of tuberculosis (0.61%) due to M. bovis or M. caprae increased slightly compared with the previous year (0.54%), and the number of infected cattle herds in the European Union increased from 9384 to 9845 herds.
Similar to previous years, the distribution of positive herds was heterogeneous and spatially clustered, with a national herd‐level prevalence ranging from < 0.01% (Belgium, Poland) to 12.2% (the United Kingdom [Northern Ireland]).
Seventeen Member States had disease‐free status during 2022. Ten Member States and the United Kingdom (Northern Ireland) have an approved eradication programme, of which three Member States had disease‐free status zones.
Overall, 149 cattle herds (0.015%) proved infected with the M. tuberculosis complex in disease‐free status zones, confirming that infection occurs rarely in these zones.
In the zones under an eradication programme within 10 Member States and the United Kingdom (Northern Ireland), 8696 cattle herds (1.5% of total herds) were positive for the M. tuberculosis complex in 2022. The United Kingdom (Northern Ireland) (12.2%), Ireland (4.6%) and Spain (2.5% in zones under an eradication programme) were the only countries that reported a prevalence higher than 1%. No positive herds were reported by Malta or Cyprus.
In the last 10 years (2013–2022), the annual number of positive cattle herds in under eradication programme zones has decreased by 46.3%. This decrease is mainly attributable to the withdrawal of the United Kingdom from the European Union in 2020.
5.2. Surveillance and monitoring of tuberculosis due to Mycobacterium bovis or Mycobacterium caprae in the EU
5.2.1. Humans
The notification of tuberculosis in humans is mandatory in all EU MS and covers the whole population. Countries can update their data retroactively; reported numbers are therefore subject to change in the future or may vary from numbers reported in previous reports. The M. bovis and M. caprae EU notification rate is calculated using the combined population of the EU MSs that reported data in 2022. The proportion of tuberculosis cases caused by M. bovis or M. caprae was calculated using the preliminary estimate of the total number of confirmed tuberculosis cases in 2022 among reporting EU MSs' species‐specific data. In 2022, no human data on M. bovis or M. caprae cases were available for France because this MS did not report species‐specific data within the M. tuberculosis complex (MTBC) for human tuberculosis cases. France has not reported species‐specific data in any previous years. In addition, Latvia did not report any MTBC data for 2018–2020.
Because tuberculosis is a chronic disease with a long incubation period, it is not possible to assess travel‐associated cases in the same way as for diseases with acute onset. Instead, a distinction is made between individuals with the disease originating from an EU MS (cases of EU origin) and those originating from outside the EU (case originating outside of the EU). In the analysis, origin is mainly based on the reported birthplace, except for cases from Austria, Belgium, Greece, Hungary and Poland, whose origin is based on reported nationality. The treatment outcome for tuberculosis due to M. bovis or M. caprae is assessed 1 year (12 months) after case notification, because the shortest duration for treatment completion is 6 months, according to the international treatment guidelines for tuberculosis.
5.2.2. Animals
Bovine tuberculosis surveillance data
Article 2 of Regulation (EU) 2016/429 of the European Parliament and of the Council (the new ‘Animal Health Law’ – AHL) states that its scope applies to transmissible diseases, including zoonoses, without prejudice to the rules laid down in Directive 2003/99/EC (i.e. the Zoonoses Directive). Therefore, the annual zoonoses data reporting requirements for MSs in accordance with Directive 2003/99/EC, implemented by EFSA using specific tools, manuals and guidance, are not affected by the entry into force of Commission Implementing Regulation (CIR) (EU) 2020/2002. 28 The EU MSs need to report to the EU ADIS 29 on outbreaks of infection with MTBC in bovine (cattle, buffalo and bison), caprine and ovine animal populations, in other even‐toed ungulates (Artiodactyla) and in terrestrial mammals. Regular summaries are posted online. CIR (EU) 2020/2002 details compulsory notification and annual reporting requirements from MSs to ADIS.
In accordance with the Zoonoses Directive, MSs must report annual surveillance data for bovine tuberculosis. These data originate from the compulsory national eradication and surveillance programmes that the MSs implement in accordance with EU legislation (AHL). The reports submitted by the MSs are harmonised and can be used for the assessment of the epidemiological situation and analysis of trends in MSs and MS zones.
Article 36 of Regulation (EU) 2016/429 provides for the approval by the European Commission of the disease‐free status of Member States or zones thereof from infection with MTBC. Because the risk of infection with MTBC in disease‐free zones is different from that of zones with an approved eradication programme (under an eradication programme – UEP), these zones have been considered separately in this report.
All cases of tuberculosis in cattle caused by the infectious MTBC members (M. bovis, M. caprae or M. tuberculosis) were taken into account to summarise the EU situation on bovine tuberculosis. Whenever possible, reporting MSs distinguish descriptively between these MTBC species.
Mycobacterium surveillance data from food and from animals other than bovine animals
Mycobacterium spp. monitoring data from food and from animals other than bovine animals are submitted to EFSA in accordance with Directive 2003/99/EC. Data collected allow for descriptive summaries to be compiled at the EU level, but do not allow trend watching or trend analyses (Table 1).
In accordance with CIR (EU) 2020/2002, notification to ADIS and surveillance rules apply to other Artiodactyla (such as camelids, cervids, ovine and caprine animals) as species susceptible to infection with MTBC.
EFSA story map on the Mycobacterium tuberculosis complex (focusing on M. bovis and M. caprae)
The EFSA story map on the M. tuberculosis complex (focusing on M. bovis and M. caprae) (available here) is a new interactive communication tool developed by EFSA and geared to the general public. This story map provides general information on the pathogen and its epidemiology, including information on where the pathogen can be found, how people and animals get infected, the occurrence of this pathogen in different sources, the disease it causes and how to prevent infection. In addition, this story map also illustrates the monitoring activities implemented in the EU and the role of EFSA with respect to these activities. Users can easily display and explore the content of the different sections in the story map, browsing the dynamic maps, images, text and multimedia features.
EFSA dashboard on the Mycobacterium tuberculosis complex (focusing on M. bovis and M. caprae)
The EFSA dashboard on the M. tuberculosis complex (focusing on M. bovis and M. caprae) (available here) is a graphical user interface for searching and querying the large amount of data collected each year by EFSA from EU MSs and other reporting countries based on Zoonoses Directive 2003/99/EC. M. tuberculosis complex (focusing on M. bovis and M. caprae) data and related statistics can be displayed interactively using charts, graphs and maps in the online EFSA dashboard. In this tool, the main statistics can also be viewed and downloaded in tabular format. Detailed information on the use and features of the M. tuberculosis complex (focusing on M. bovis and M. caprae) dashboard can be found in the user guide that can be downloaded from the online tool. Links to the dashboard are available in the relevant sections of this chapter. Some discrepancies between the data and statistics reported in the present report and those shown in the dashboard may occur. The reason is that not all MSs provided distinct statistics for all their disease‐free status zones and zones under eradication programme.
5.3. Results
5.3.1. Overview of key statistics, EU, 2018–2022
Table 38 summarises the EU‐level statistics on human tuberculosis due to M. bovis or M. caprae and on bovine tuberculosis during 2018–2022. More detailed descriptions of these statistics are provided in the subsections below.
TABLE 38.
Summary of tuberculosis due to Mycobacterium bovis and Mycobacterium caprae statistics relating to humans and bovine animals (stratified by disease status of MSs/zones), EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Number of confirmed M. bovis cases | 125 | 106 | 95 | 141 | 168 | ECDC |
| Number of confirmed M. caprae cases | 5 | 9 | 4 | 11 | 13 | ECDC |
| Total number of confirmed cases | 130 | 115 | 99 | 152 | 181 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0.03 | 0.03 | 0.03 | 0.03 | 0.04 | ECDC |
| Number of EU MSs that reported data on M. bovis or M. caprae cases | 26 | 26 | 25 | 26 | 26 | ECDC |
| M. bovis or M. caprae cases in individuals of EU origin | 89 | 66 | 60 | 107 | 105 | ECDC |
| M. bovis or M. caprae cases in individuals originating from outside EU | 40 | 46 | 35 | 40 | 68 | ECDC |
| M. bovis or M. caprae cases in individuals of unknown origin | 1 | 3 | 4 | 5 | 8 | ECDC |
| Total number of foodborne outbreaks | 0 | 0 | 0 | 0 | 0 | EFSA |
| Number of outbreak‐related cases | 0 | 0 | 0 | 0 | 0 | EFSA |
| Animals | ||||||
| Bovine animals | ||||||
| Number of infected herds in disease‐free status zones c | 149 | 139 | 139 | 143 | 172 | EFSA |
| Number of reporting disease‐free status MSs c | 17 | 17 | 17 | 17 | 17 | EFSA |
| Number of infected herds in zones under an eradication programme | 9696 | 9255 | 7233 | 16,277 | 18,801 | EFSA |
| Number of reporting MSs with zones under an eradication programme d | 10 | 10 | 9 e | 11 | 11 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
Data from the United Kingdom (Northern Ireland) were taken into account for 2021–2022. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling also apply to the United Kingdom (Northern Ireland).
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
The Member States or zones thereof with disease‐free status regarding infection with the Mycobacterium tuberculosis complex (M. bovis, M. caprae, M. tuberculosis) (MTBC).
The Member States or zones thereof with an approved eradication programme for infection with MTBC. In addition United Kingdom (Northern Ireland) has an approved eradication programme for infection with MTBC.
No data from Bulgaria.
5.3.2. Tuberculosis due to Mycobacterium bovis or Mycobacterium caprae in humans
In 2022, 130 confirmed human cases of tuberculosis due to M. bovis or M. caprae were reported from 10 MSs (Austria, Belgium, Germany, Greece, Ireland, Italy, the Netherlands, Romania, Spain and Sweden) (Table 39). Tuberculosis cases due to M. bovis (125 cases) were reported in all these countries, and only one MS (Spain) also notified cases caused by M. caprae (five cases). Overall, tuberculosis cases due to M. bovis or M. caprae accounted for a small proportion (0.4%) of the total tuberculosis cases reported in the EU by 26 MSs with species‐specific data on MTBC available in 2022 (see Section 5.2.1). Sixteen MSs did not report any cases. Cases of human tuberculosis due to M. bovis or M. caprae in the EU increased in 2022 and 2021 following the drop observed in 2020, the first COVID‐19 pandemic year. In 2022, the number of human tuberculosis cases due to M. bovis or M. caprae among the 27 MSs exceeded the number of cases reported in 2019.
TABLE 39.
Reported confirmed human cases of tuberculosis due to Mycobacterium bovis or Mycobacterium caprae and notification rates per 100,000 population in EU MS and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Status | National coverage a | Data format a | Confirmed cases and rates | Confirmed cases and rates | Confirmed cases and rates | Confirmed cases and rates | Confirmed cases and rates | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | ||||
| Austria | DFS | Y | C | 5 | 0.06 | 4 | 0.04 | 0 | 0 | 3 | 0.03 | 2 | 0.02 |
| Belgium | DFS | Y | C | 9 | 0.08 | 10 | 0.09 | 6 | 0.05 | 0 | 0 | 5 | 0.04 |
| Bulgaria | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Croatia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Czechia | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 |
| Denmark | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Estonia | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland | DFS | Y | C | 0 | 0 | 0 | 0 | 1 | 0.02 | 0 | 0 | 0 | 0 |
| France b | DFS | – | – | – | – | – | – | – | – | – | – | – | – |
| Germany | DFS | Y | C | 39 | 0.05 | 43 | 0.05 | 37 | 0.04 | 51 | 0.06 | 64 | 0.08 |
| Greece | Y | C | 1 | 0.01 | 0 | 0 | 2 | 0.02 | 1 | 0.01 | 0 | 0 | |
| Hungary | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ireland | Y | C | 4 | 0.08 | 2 | 0.04 | 4 | 0.08 | 7 | 0.14 | 7 | 0.14 | |
| Italy | Y | C | 15 | 0.03 | 12 | 0.02 | 6 | 0.01 | 11 | 0.02 | 17 | 0.03 | |
| Latvia c | DFS | Y | C | 0 | 0 | 0 | 0 | – | – | – | – | – | – |
| Lithuania | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Netherlands | DFS | Y | C | 5 | 0.03 | 5 | 0.03 | 6 | 0.03 | 5 | 0.03 | 11 | 0.06 |
| Poland | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Portugal | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Romania | Y | C | 1 | 0.01 | 0 | 0 | 1 | 0.01 | 1 | 0.01 | 0 | 0 | |
| Slovakia | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Slovenia | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Spain | Y | C | 45 | 0.09 | 35 | 0.07 | 30 | 0.06 | 35 | 0.07 | 46 | 0.10 | |
| Sweden | DFS | Y | C | 6 | 0.06 | 4 | 0.04 | 6 | 0.06 | 3 | 0.03 | 4 | 0.04 |
| EU Total 27 | – | – | 130 | 0.03 | 115 | 0.03 | 99 | 0.03 | 117 | 0.03 | 157 | 0.04 | |
| United Kingdom d | – | – | – | – | – | – | – | – | – | 35 | 0.05 | 24 | 0.04 |
| EU Total | – | – | 130 | 0.03 | 115 | 0.03 | 99 | 0.03 | 152 | 0.03 | 181 | 0.04 | |
| Iceland e , f | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Norway | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.02 | 0 | 0 |
| Liechtenstein | DFS | Y | C | 0 | 0 | 0 | 0 | 3 | 0.03 | 4 | 0.05 | 3 | 0.04 |
| Switzerland g | DFS | Y | C | 1 | 0.01 | 3 | 0.03 | ||||||
Abbreviation: –, Data not reported; DFS, Disease‐free status, i.e. free of infection with M. bovis, M. caprae or M. tuberculosis in the bovine animal population.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Not reporting species of the M. tuberculosis complex.
Latvia did not report any MTBC data during 2018–2020.
Cases reported by the United Kingdom for the 2018–2019 period were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020 it became a third country.
In Iceland, which has no special agreement concerning animal health (status) with the EU, the last outbreak of bovine tuberculosis was in 1959.
Iceland reported MTBC data for 2021 with a delay.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
 All zones of the MS have disease‐free status.
All zones of the MS have disease‐free status.
 Not all zones of the MS have disease‐free status.
Not all zones of the MS have disease‐free status.
 No zones of the MS have disease‐free status.
No zones of the MS have disease‐free status.
The EU notification rate in 2022 was 0.034 cases per 100,000 population, which was an increase of 13.2% compared with 2021, when the notification rate was 0.030 per 100,000 population.
In 2022, the highest notification rate was reported by Spain (0.09 per 100,000), followed by Belgium and Ireland (0.08 per 100,000).
Among the 17 MSs with disease‐free status in 2022, 16 MSs reported on MTBC species. M. bovis and M. caprae human cases were reported in five MSs. The notification rate in these 16 MSs reporting on MTBC species was 0.03 cases per 100,000 population. The notification rate for M. bovis and M. caprae human cases reported in the 10 non‐DFS MSs in 2022 was 0.04 cases per 100,000 population.
The majority of the M. bovis and M. caprae human cases reported in 2022 (89/130; 68.5%) were of EU origin (native cases and/or cases originating from other MSs). The other cases originated from outside the EU (N = 40; 30.8%) or had unknown origin (N = 1; 0.8%) (Table 38). Notification rates of M. bovis and M. caprae human cases of EU origin were lower in disease‐free status MSs (N = 34; 38.2%) than in non‐disease‐free status MSs (N = 55; 61.8%).
Information on treatment outcome after 12 months was reported for 89.6% (103/115) of the human M. and M. caprae cases notified in 2021. The treatment was reported to be successful for 61 cases (59.2%). Four cases (3.9%) were still being treated at 12 months. Deaths were reported in 16 cases (15.5%). Twenty‐two cases (21.4%) were reported as lost to follow‐up.
Regarding drug resistance, out of 93 antibiograms, resistance to rifampicin (two cases), to ethambutol (one case), to isoniazid (four cases) and to streptomycin (one case) were reported. One multidrug‐resistant (MDR) case (resistant to isoniazid and rifampicin) was reported in Germany; no extensively drug‐resistant (XDR) cases were reported. Resistance to pyrazinamide is natural in M. bovis.
Figure 10 shows, for year 2022, the number of confirmed tuberculosis cases due to M. bovis or M. caprae in individuals of EU origin overlaid with the national aggregated herd prevalence of bovine tuberculosis.
FIGURE 10.
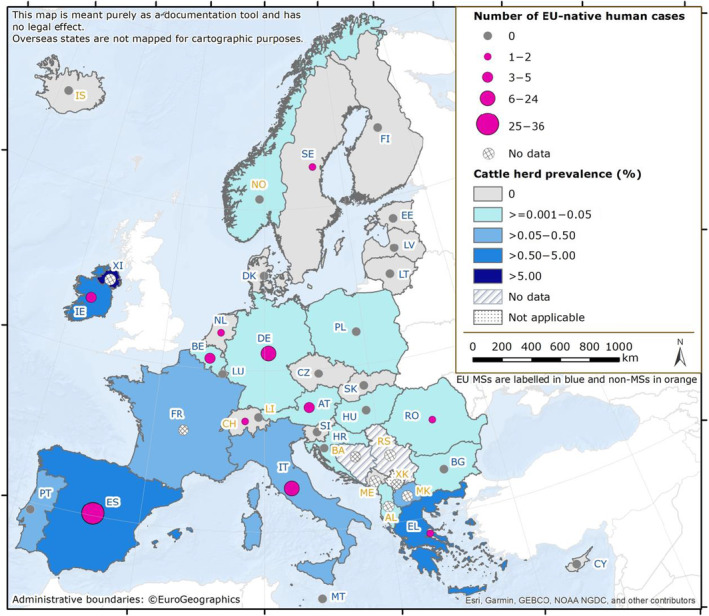
Map of the number of confirmed tuberculosis cases due to Mycobacterium bovis or Mycobacterium caprae in individuals of EU origin, and national herd prevalence of tuberculosis in the bovine population in EU MS and non‐MS countries, 2022. Note: The United Kingdom (Northern Ireland) informed during the last phase of the production of this draft report that the numbers of positive herds for bovine tuberculosis were 2785 in 2022 and 2303 in 2021.
5.3.3. Mycobacterium in food
No Mycobacterium species monitoring data from food were submitted for the year 2022.
5.3.4. Tuberculosis in bovine animals
Bovine tuberculosis surveillance data
Seventeen MSs had DFS regarding MTBC during 2022 (Table 38). Of the remaining 10 MSs and the United Kingdom (Northern Ireland), 3 MSs had disease‐free status zones or provinces:
-
–
Italy: 12 regions and 16 provinces;
-
–
Portugal: Two regions (Algarve and Azores, except the island of São Miguel);
-
–
Spain: Four autonomous communities (Canary Islands, Galicia, País Vasco and Principado de Asturias).
Seven MSs had no zones with DFS regarding MTBC. The United Kingdom (Northern Ireland) had no disease‐free status zones either.
Norway, Switzerland and Liechtenstein had DFS, in accordance with the EU legislation. In Iceland, which has no special agreement with the EU on animal health status, the last outbreak of bovine tuberculosis was reported in 1959. A map of MS disease status, provided by EFSA, is available at link here.
During 2022, in the EU, the overall proportion of cattle herds infected with MTBC was very low (0.61%), which is slightly higher than that reported in 2021 (0.54%). Compared with the previous year, the number of bovine herds infected with MTBC in the EU increased from 9384 to 9845 herds. Thirteen MSs (11 having disease‐free status and 2 UEP countries) reported no cases of bovine tuberculosis. The remaining MSs reported bovine tuberculosis with a wide range of prevalence at the national level. MTBC infection in cattle herds primarily affected the UEP zones: the overall occurrence of bovine tuberculosis in UEP zones (1.5%) was 100 times higher than in disease‐free zones (0.015%).
Most MSs reported MTBC infections without specifying the species involved. Infection with M. bovis was specifically detected in Bulgaria, France, Germany, Ireland, Italy, Poland, Romania and the United Kingdom (Northern Ireland), whereas infection with M. caprae was specifically reported by Austria, Germany and Romania. Infection of cattle herds with M. tuberculosis was not reported.
MSs and MSs' zones with disease‐free status regarding Mycobacterium tuberculosis complex infection
The majority of the whole EU cattle herd population (60.4%) is located in the disease‐free status zones of the 20 MSs having such zones. However, the number of cattle herds has been steadily decreasing (−26.8% in 2022 compared with 2013), affecting the calculation of the prevalence of herds infected with MTBC. From 2013 to 2022, there was a marked decrease in the annual number of infected cattle herds (−24.4%), whereas prevalence has remained stable (Figure 11).
FIGURE 11.
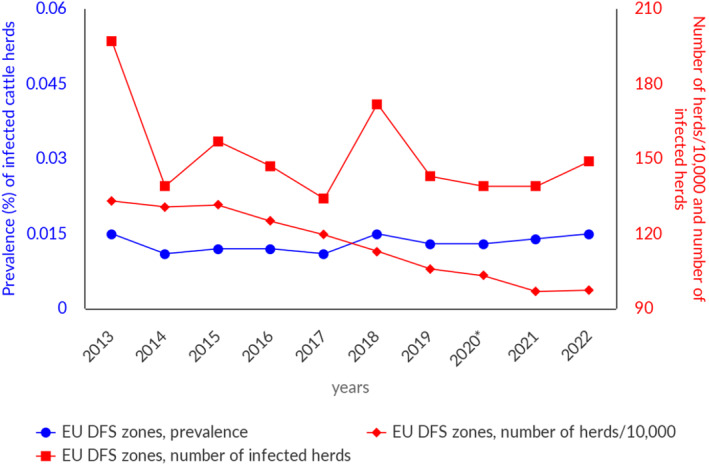
Prevalence of cattle herds infected with the Mycobacterium tuberculosis complex in disease‐free status (DFS) zones, EU, 2013–2022. aIn contrast to years 2013–2019, the year 2020 does not include the United Kingdom data. Since 1 February 2020, the United Kingdom has withdrawn from the EU and has become a third country.
Eight MSs with disease‐free status zones reported a total of 149 MTBC‐infected bovine herds, confirming that the detection of bovine tuberculosis in disease‐free status zones is sporadic. When comparing data from 2022 and 2021, the number of MTBC‐infected cattle herds increased by 10 units, with an almost unchanged prevalence (0.014% vs. 0.015%), although the total number of cattle herds has increased by 0.60%.
MSs and MSs' zones with an approved eradication programme for infection with Mycobacterium tuberculosis complex
The zones with an approved eradication programme (i.e. UEP zones), belonging to 10 MSs and the United Kingdom (Northern Ireland), account for 39.6% of the whole EU cattle herd population, which has been steadily decreasing over time (−53.0% in 2022 compared with 2013; Figure 12). Over the last 10 years, the prevalence of bovine tuberculosis in UEP zones has shown different trends. During 2013–2019, the data involved EU‐28 MSs. The significant decrease in 2020 is due to the withdrawal of the United Kingdom from the EU and to the absence of data from Bulgaria in that year. Starting from 2021, the increase in the number of cattle herds can be mainly attributed to the data provided by Bulgaria after its 2020 hiatus and by the United Kingdom (Northern Ireland), in accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland. In the last 10 years (2013–2022), the overall annual number of positive cattle herds reported in UEP zones decreased by 46.3%, whereas prevalence increased by 14.2%.
FIGURE 12.
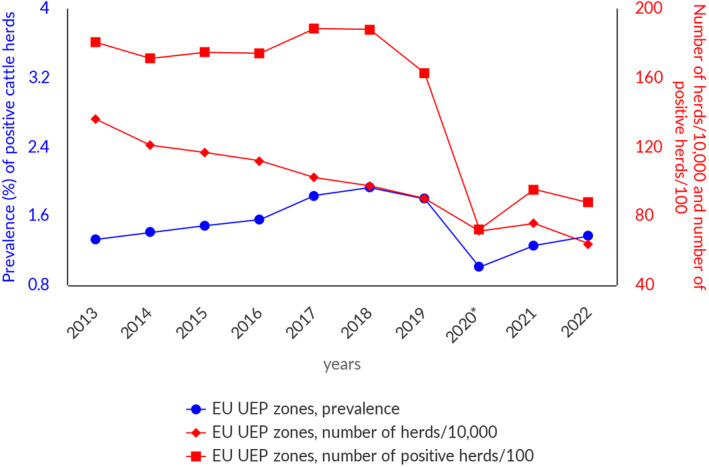
Prevalence of cattle herds positive for bovine tuberculosis in zones under an eradication programme (UEP), EU, 2013–2022. *In contrast to years 2012–2019, year 2020 does not include the United Kingdom data. Since 1 February 2020, the United Kingdom has withdrawn from the EU and has become a third country. No data were reported from Bulgaria.
In 2022, 8 MSs and the United Kingdom (Northern Ireland) reported a total of 9696 herds positive for bovine tuberculosis. Compared with 2021 (9255), the number of positive herds increased by 4.8%.
In 2022, prevalence varied widely among MSs with an approved eradication programme: Ireland (4.6%) and Spain (2.5% in UEP zones) were the only MSs that reported prevalence higher than 1%; no positive herds were reported by Malta or Cyprus. The United Kingdom (Northern Ireland), which has no disease‐free status zones, reported prevalence of 12.2%*. In UEP zones, the overall prevalence increased slightly (1.3% in 2021 compared with 1.5% in 2022), mainly due to a higher number of infected herds in the United Kingdom (Northern Ireland).
For a further interactive look at M. tuberculosis complex (focusing on M. bovis and M. caprae) monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
Non‐Member States and pre‐accession countries
Bovine tuberculosis was not detected in 2022 in Iceland, Liechtenstein or Switzerland, whereas Norway reported two infected cattle herds and a prevalence of 0.02%. Among the pre‐accession countries, Montenegro, as in 2020–2021, reported no infected herds; Republic of North Macedonia reported a prevalence of 0.10% MTBC‐infected herds (13/13,652), whereas, for the first time, Albania reported a prevalence of 0.01% MTBC‐infected herds (10/117,795). Kosovo 30 reported a prevalence of 3.1% intradermal tuberculin skin test‐positive bovines (78/2500).
5.3.5. Mycobacterium surveillance data from animals other than bovine animals
In 2022, three MSs (Finland, Slovenia, Sweden), the United Kingdom (Northern Ireland) and one non‐MS (Norway) reported surveillance data on infection in farmed deer. In particular, Sweden reported data from a control programme in farmed deer. Two cases of MTBC infection were reported in deer herds by the United Kingdom (Northern Ireland).
MSs also reported cases of MTBC infection in other mammal species. In particular, M. bovis was detected in farmed alpacas (Ireland, the United Kingdom (Northern Ireland)), pigs (France, Ireland, the United Kingdom [Northern Ireland]), cats (France), wild deer (Spain, Ireland), wild boars (Spain, France, Italy), foxes (Spain) and badgers (Spain, France, Ireland, the United Kingdom (Northern Ireland)). Small ruminants (sheep and goats) infected were reported in Spain.
For a further interactive look at Mycobacterium monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
5.4. Discussion
In 2022, the reporting of human tuberculosis due to M. bovis and M. caprae resulted in a total of 130 cases, an increase compared with years 2021 and 2020. This corresponded in a notification increase of 13.2% in 2022 (0.034) compared with 2021 (0.030) per 100,000 population. Several factors should be considered when analysing the differences in the notification rates in the last 5 years, such as taking into account the withdrawal of the United Kingdom from the EU and the context of the COVID‐19 pandemic. A relatively stable epidemiological situation was observed in most countries with few exceptions during this period. The COVID‐19 pandemic clearly had an impact on the entire healthcare system, but mainly in 2021 and 2020. Nevertheless, Austria, Italy and Spain reported an increase in their notification rates in 2021–2022, and Belgium observed an increase during 2020–2022.
Tuberculosis cases of zoonotic origin (due to M. bovis or M. caprae) and notification rates are highly likely to have been underestimated. Bias is introduced by those EU MSs that do not regularly perform routine tests to distinguish M. bovis and M. caprae from M. tuberculosis, resulting in under‐notification at the EU level, because all cases in those MSs are reported as M. tuberculosis, and undermining the possibility of tracing the origin of infections (Fujiwara & Olea‐Popelka, 2016). Furthermore, a lower notification rate was observed in EU MSs with DFS compared with non‐DFS MSs, supporting the effectiveness of the surveillance programmes. Regarding the treatment outcome reported in 2021, decreased successful treatment rates (59.2%) and increased deaths (15.5%) may be related to poor compliance during the COVID‐19 pandemic, but also to the increased number of drug‐resistant cases observed (discussed below), although data on potential correspondence between deaths and drug‐resistant cases are not available. The increased percentage of deaths, due to infection by M. bovis or M. caprae, also appears to suggest that the total burden of cases may be underestimated. Furthermore, there was a significant change in the ratio of cases of EU origin versus cases in non‐EU persons compared with 2021. Although it is difficult to interpret these data, it is possible that, during the COVID‐19 pandemic, low‐income and marginal populations suffered from reduced access to the healthcare system, resulting in a smaller number of diagnosed cases. These populations are generally composed of non‐EU persons. In addition, the high proportion of lost‐to‐follow‐up cases, despite a slight improvement compared with 2020, must be taken into account and the limited number of M. bovis and M. caprae cases in such a large population is more subject to stochastic annual variations.
There is no doubt that the most concerning observation in 2022 human data is the increase in drug resistance. In 2021, only one mono‐resistant (isoniazid resistance) case was reported, whereas in 2022 four isoniazid‐resistant, one ethambutol‐resistant, two rifampicin‐resistant and one streptomycin‐resistant cases were reported. It must be noted that the total number of resistant cases may actually be lower, because Germany reported one MDR case, which was resistant at least to isoniazid and rifampicin, but may also account for resistance to ethambutol and streptomycin, both observed in Germany. These data are consistent with what has been observed around the world in tuberculosis caused by M. tuberculosis WHO, 2022) globally, there was an increase in MDR and rifampicin‐resistant tuberculosis in 2021, after years of decreased incidence. Drug resistance generally arises from poor compliance with therapy protocols, a direct effect of the COVID‐19 pandemic. Natural resistance to pyrazinamide (Scorpio & Zhang, 1996) complicates the therapeutical approach to M. bovis drug‐resistant infections.
In conclusion, 2022 human data show changes directly dependent on the events that took place in recent years, stressing the importance of surveillance, in particular regarding the control of drug resistance and the implementation of DFS programmes.
The regulatory framework for bovine tuberculosis changed substantially in the EU during 2021. Tuberculosis caused by MTBC infection is currently considered a disease to be controlled in all MSs with the goal of eradicating the disease in bovine animals throughout the EU, while being kept under surveillance in other mammals. All MSs are to have a surveillance, or a control and eradication, programme approved by the European Commission. This should lead, in the coming years, to progressive improvement in the already satisfactory epidemiological situation. In 2022, the overall EU proportion of cattle herds infected with MTBC was 0.61%, slightly higher than in 2021. Bovine tuberculosis was reported by 14 MSs and by the United Kingdom (Northern Ireland). Its distribution was highly heterogeneous and spatially clustered in the EU, with a national herd prevalence ranging from 0% to 12.2%.
Seventeen MSs had DFS and three MSs with an approved eradication programme also had disease‐free status zones. The number of disease‐free zones increased during 2022. Thirteen of these MSs reported no cases of bovine tuberculosis in cattle. In the disease‐free zones, the detection of bovine tuberculosis remained a rare event, as in the previous 10 years.
Eight UEP MSs and the United Kingdom (Northern Ireland) detected bovine tuberculosis during 2022, with a positive herd prevalence of 1.5%. When comparing 2022 with 2021 data, the overall annual number of positive cattle herds, and the total number of cattle herds decreased in these zones. This reduction has led to a slight increase in the prevalence of positive cattle herds, attributable to the proportionally greater decrease in the total number of herds.
In the last 10 years (2013–2022), the overall annual number of positive cattle herds reported in UEP zones decreased by 46.3%, whereas prevalence increased by 14.2%. These different trends can be attributed for the most part to the withdrawal of the United Kingdom from the EU, to the decreased number of herds (−53.0%), to the gradual progression of DFS in zones within MSs with an approved eradication programme (i.e. UEP) and to unfavourable environmental conditions hindering the eradication process in several UEP zones (de la Cruz et al., 2019; Byrne et al., 2022).
In 2022, M. bovis was reported to be isolated from a wide range of domestic and wild mammal species (other than bovine animals), which is a reflection of the broad host range that this pathogen has. M. caprae, acknowledged to cause bovine tuberculosis, was reported only in cattle.
There is a major obstacle to eradication of bovine tuberculosis in areas where infection is endemic in wildlife. Successfully tackling bovine tuberculosis also involves addressing the wildlife reservoir of the disease. In 2018, Ireland introduced a vaccination policy in the Eurasian badger (Meles meles), a species known to be a maintenance host of M. bovis. Among other control measures, Ireland is also reducing the badger population (Gormley et al., 2017). On the other hand, in the United Kingdom (Northern Ireland), no active badger intervention or vaccination took place in 2022. Stagnating or increasing trends in the prevalence of bovine tuberculosis demonstrate that eradication of this disease is a challenge, owing to the complex interactions between the pathogen, hosts and local environments (EFSA AHAW Panel, 2014). MS‐specific evaluations of status, trends and the relevance of bovine tuberculosis as a source of disease for humans can be found in the 2022 Annual National Zoonoses Country Reports available online here.
6. BRUCELLA
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here and are also retrievable from the EFSA Brucella dashboard available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
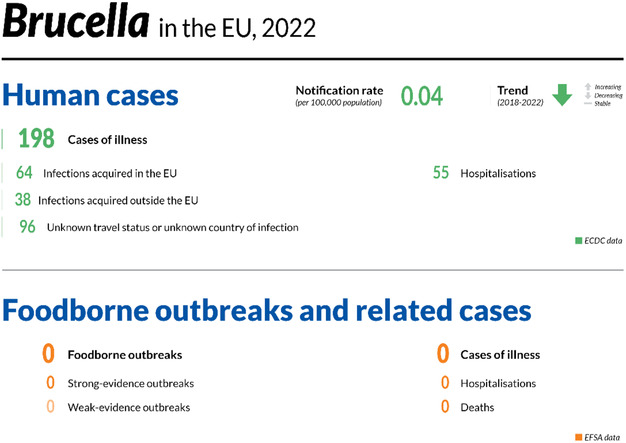
6.1. Key facts
In 2022, there were 198 confirmed cases of human brucellosis, corresponding to an European Union notification rate of 0.04 cases per 100,000 population. This was an increase of 29.2% compared with 2021 (0.03 cases per 100,000 population).
The overall trend for Brucella infections showed a significantly decreasing trend in 2018–2022.
Four Member States (Germany, Greece, Italy and Portugal) had significantly decreasing 5‐year trends from 2018 to 2022.
Brucella melitensis was reported as the aetiological agent in 84 (94.4%) out of 89 human cases of brucellosis with information reported on the Brucella species.
In total, 22 Member States and the United Kingdom (Northern Ireland) were disease‐free for brucellosis in cattle, while five Member States (Bulgaria, Greece, Hungary, Italy and Portugal) were non‐disease‐free (under an eradication programme). Overall, in the disease‐free status zones of the European Union, there were 13 positive herds in 2022, demonstrating a rare occurrence (prevalence < 0.001%). In the zones under an eradication programme, bovine brucellosis remained very low, with 411 positive herds (0.39%). The number of positive herds ranged between 603 (in 2020) and 411 (in 2022) during 2018–2022.
In total, 20 Member States and the United Kingdom (Northern Ireland) were disease‐free for brucellosis in sheep and goats, while seven Member States (Bulgaria, Croatia, overseas French regions, Greece, Italy, Malta and Portugal) were non‐disease‐free. Overall, in the disease‐free status zones of the European Union, there were only two infected herds in 2022, demonstrating a rare occurrence (< 0.01%). In zones under an eradication programme, brucellosis in sheep and goats remained very low, with 234 flocks reported to be infected (0.15%), which represents a decrease from 620 in 2018.
Brucellosis is still an animal health concern with public health relevance in southern European countries that are not disease‐free for brucellosis.
6.2. Surveillance and monitoring of Brucella in the EU
6.2.1. Humans
For 2022, 26 MSs reported information on brucellosis in humans. Surveillance is mandatory in 25 MSs. Belgium has another (unspecified) system. Denmark has no surveillance system in place for brucellosis, and the disease is not notifiable or reported at the EU level. The EU case definition was used by 23 countries, three countries (France, Germany and Italy) reported using another case definition. All countries had a comprehensive surveillance system, with full national coverage in all MSs reporting brucellosis data. All countries reported case‐based data with the exception of Bulgaria, which reported aggregated data.
6.2.2. Food and animals
Surveillance data for bovine brucellosis, and ovine and caprine brucellosis
Article 2 of Regulation (EU) 2016/429 31 of the European Parliament and of the Council (the new ‘Animal Health Law’ – AHL) states that its scope applies to transmissible diseases, including zoonoses, without prejudice to the rules laid down in Directive 2003/99/EC. 32 Therefore, the annual zoonoses data reporting requirements for MSs in accordance with Directive 2003/99/EC, implemented by the European Food Safety Authority (EFSA) using specific tools, manuals and guidance, are not affected by the entry into force of CIR (EU) 2020/2002. 33 The EU MSs need to report to the EU ADIS 34 on outbreaks of infection with B. abortus, B. melitensis and B. suis in bovine, caprine and ovine animal populations, in other even‐toed ungulates (Artiodactyla) and in other terrestrial animals. Regular summaries are posted online. CIR (EU) 2020/2002 details compulsory notification and annual reporting requirements from MSs to ADIS.
In accordance with the Zoonoses Directive 2003/99/EC, MSs must report annual surveillance data for bovine brucellosis, and ovine and caprine brucellosis. These data originate from the compulsory national eradication and surveillance programmes that the MSs implement in accordance with EU legislation (AHL). The reports submitted by the MSs are harmonised and can be used for the assessment of the epidemiological situation and analysis of trends in MSs and MS zones.
Article 36 of Regulation (EU) 2016/429 provides for the approval by the European Commission of the disease‐free status of MSs or zones thereof from infection with B. abortus, B. melitensis and B. suis in bovine, and in ovine and caprine animal populations. Because the risk of infection with brucellosis in DFS zones is different from that of non‐disease‐free status (under eradication programme – UEP) zones, these zones have been considered separately in this report.
Regulation (EU) 2016/429 of the European Parliament and of the Council concerns approval of the disease‐free and non‐vaccination status of MSs or zones or compartments. CIR (EU) 2018/1882 35 includes Bos ssp., Bubalus ssp., Bison ssp., Ovis ssp. and Capra ssp. as species for notification, surveillance, prevention, certification and compulsory eradication. CDR 2020/689 36 (Annex IV) describes the conditions required to grant, maintain or suspend the status of free from infection with B. abortus, B. melitensis and B. suis for an establishment keeping bovine animals, and sheep and goats.
Annual surveillance programmes are carried out in DFS zones to confirm the absence of infection with B. abortus, B. melitensis and B. suis in cattle, and in sheep and goats. In UEP zones, control and eradication programmes for brucellosis in cattle, and sheep and goats are in place. These data are comparable across MSs because the monitoring schemes are harmonised, and the data collected and reported to EFSA originate from the census‐as‐sampling framework or a randomised design. These data can be used to carry out trend analyses both at the EU and MS levels, to perform trend watching and produce descriptive summaries, and to assess the impact of control and eradication programmes (Table 1).
Surveillance data for Brucella from food, and animals other than bovine animals, sheep and goats
Monitoring data for Brucella from food, and animals other than bovine animals, and sheep and goats are submitted to EFSA in accordance with Directive 2003/99/EC. Data collected allow for descriptive summaries to be compiled at the EU level, but do not allow for trend watching or trend analyses (Table 1).
In accordance with CIR (EU) 2020/2002, notification to ADIS and surveillance rules apply to other Artiodactyla species (such as camelids or cervids) as susceptible species for brucellosis.
EFSA story map on Brucella
The EFSA story map on Brucella (available here) is a new interactive communication tool developed by EFSA and geared to the general public. This story map provides general information on the pathogen and its epidemiology, including information on where the pathogen can be found, how people and animals get infected, the occurrence of this pathogen in different sources, the disease it causes and how to prevent infection. In addition, this story map also illustrates the monitoring activities implemented in the EU and the role of EFSA with respect to these activities. Users can easily display and explore the content of the different sections in the story map, browsing the dynamic maps, images, text and multimedia features.
EFSA dashboard on Brucella
The EFSA dashboard on Brucella (available here) is a graphical user interface for searching and querying the large amount of data collected each year by EFSA from EU MSs and other reporting countries based on Zoonoses Directive 2003/99/EC. Brucella data and related statistics can be displayed interactively using charts, graphs and maps in the online EFSA dashboard. In this tool, the main statistics can also be viewed and downloaded in tabular format. Detailed information on the use and features of the Brucella dashboard can be found in the user guide that can be downloaded from the online tool. Links to the dashboard are available in the relevant sections of this chapter.
6.3. Results
6.3.1. Overview of key statistics, EU, 2018–2022
Table 40 displays statistics at the EU level on human and animal brucellosis, along with data on detection of Brucella in food, between 2018 and 2022. More detailed descriptions of these statistics are provided in the subsections below and in the chapter on foodborne outbreaks.
TABLE 40.
Summary of Brucella statistics relating to humans, major food categories and animal species (stratified by status of disease of MSs/MS zones), EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 198 | 162 | 132 | 309 | 332 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0.04 | 0.03 | 0.03 | 0.06 | 0.08 | ECDC |
| Number of reporting MSs | 26 | 26 | 26 | 27 | 26 | ECDC |
| Infection acquired in the EU | 64 | 76 | 68 | 126 | 135 | ECDC |
| Infection acquired outside the EU | 38 | 21 | 14 | 50 | 51 | ECDC |
| Unknown travel status or unknown country of infection | 96 | 65 | 50 | 133 | 172 | ECDC |
| Total number of foodborne outbreaks | 0 | 2 | 2 | 2 | 0 | EFSA |
| Number of outbreak‐related cases | 0 | 1 | 1 | 1 | 0 | EFSA |
| Food | ||||||
| Milk and milk products | ||||||
| Number of sampling units | 182 | 320 | 275 | 586 | 1005 | EFSA |
| Number of reporting MSs | 3 | 3 | 3 | 2 | 3 | EFSA |
| Animals | ||||||
| Cattle (bovine animals) | ||||||
| Number of infected herds in disease‐free status zones c | 13 | 8 | 6 | 4 | 3 | EFSA |
| Number of reporting disease‐free status MSs c | 22 | 21 | 20 | 20 | 20 | EFSA |
| Number of positive herds in zones under an eradication programme | 411 | 546 | 603 | 485 | 563 | EFSA |
| Number of reporting MSs with zones under an eradication programme | 5 | 6 | 6 d | 8 | 8 | EFSA |
| Sheep and goats | ||||||
| Number of infected flocks in disease‐free zones d | 2 | 15 | 3 | 1 | 0 | EFSA |
| Number of reporting disease‐free status MSs d | 20 | 20 | 19 | 20 | 20 | EFSA |
| Number of positive herds in zones under an eradication programme | 234 | 331 | 349 | 451 | 620 | EFSA |
| Number of reporting MSs with zones under an eradication programme | 7 e | 6 | 7 f | 8 | 8 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
Data from the United Kingdom (Northern Ireland) were taken into account for 2021–2022. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling also apply to the United Kingdom (Northern Ireland).
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Member States or zones thereof with disease‐free status from infection with Brucella abortus, B. melitensis and B. suis in bovine animal populations. In addition United Kingdom (Northern Ireland) has the disease‐free status from infection with Brucella abortus, B. melitensis and B. suis in bovine animal populations.
Member States or zones thereof with disease‐free status from infection with Brucella abortus, B. melitensis and B. suis in ovine and caprine animal populations. In addition United Kingdom (Northern Ireland) has the disease‐free status from infection with Brucella abortus, B. melitensis and B. suis in ovine and caprine animal populations.
Including France, in which the whole of metropolitan France obtained disease‐free status in 2022 whereas overseas French regions did not have this status.
No data were reported by Bulgaria.
6.3.2. Human brucellosis
In 2022, 198 confirmed cases were reported in the EU, which was a slight increase compared with 2021. The notification rate was 0.04 cases per 100,000 population, which was an increase of 29.2% compared with 2021 (0.03 cases per 100,000 population). In 2022, 26 MSs provided data and information on brucellosis in humans (Table 40). Greece reported the highest notification rate (0.33 per 100,000 population) (Table 41). Nine MSs (Cyprus, Czechia, Estonia, Finland, Hungary, Latvia, Lithuania, Malta and Romania) reported zero cases (Table 41).
TABLE 41.
Reported confirmed human cases of brucellosis and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Status | National coverage c | Data format c | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | |||||||
| Bv a |
Ov, Cp b |
Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | DFS | DFS | Y | C | 7 | 0.08 | 6 | 0.07 | 8 | 0.09 | 6 | 0.07 | 7 | 0.08 |
| Belgium | DFS | DFS | Y | C | 3 | 0.03 | 7 | 0.06 | 4 | 0.03 | 3 | 0.03 | 9 | 0.08 |
| Bulgaria | Y | A | 2 | 0.03 | 0 | 0 | 1 | 0.01 | 0 | 0 | 1 | 0.01 | ||
| Croatia | DFS | Y | C | 2 | 0.05 | 2 | 0.05 | 1 | 0.02 | 3 | 0.07 | 3 | 0.07 | |
| Cyprus | DFS | DFS | Y | C | 0 | 0 | 1 | 0.11 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | DFS | DFS | Y | C | 0 | 0 | 1 | 0.01 | 0 | 0 | 4 | 0.04 | 4 | 0.04 |
| Denmark d | DFS | DFS | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | DFS | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.08 | 1 | 0.08 |
| Finland | DFS | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France e | DFS | Y | C | 37 | 0.05 | 21 | 0.03 | 19 | 0.03 | 34 | 0.05 | 26 | 0.04 | |
| Germany | DFS | DFS | Y | C | 35 | 0.04 | 13 | 0.02 | 19 | 0.02 | 36 | 0.04 | 37 | 0.04 |
| Greece | Y | C | 35 | 0.33 | 24 | 0.22 | 30 | 0.28 | 65 | 0.61 | 97 | 0.90 | ||
| Hungary | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Ireland | DFS | DFS | Y | C | 1 | 0.02 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Italy | Y | C | 20 | 0.03 | 32 | 0.05 | 18 | 0.03 | 49 | 0.08 | 94 | 0.16 | ||
| Latvia | DFS | DFS | Y | C | 0 | 0 | 0 | 0 | 1 | 0.05 | 0 | 0 | 0 | 0 |
| Lithuania | DFS | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | DFS | DFS | Y | C | 1 | 0.15 | 1 | 0.16 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Netherlands | DFS | DFS | Y | C | 5 | 0.03 | 2 | 0.01 | 2 | 0.01 | 7 | 0.04 | 5 | 0.03 |
| Poland | DFS | DFS | Y | C | 1 | < 0.01 | 1 | < 0.01 | 0 | 0 | 2 | 0.01 | 0 | 0 |
| Portugal | Y | C | 13 | 0.13 | 10 | 0.10 | 9 | 0.09 | 33 | 0.32 | 19 | 0.18 | ||
| Romania | DFS | DFS | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 1 | 0.01 |
| Slovakia | DFS | DFS | Y | C | 3 | 0.06 | 6 | 0.11 | 2 | 0.04 | 1 | 0.02 | 0 | 0 |
| Slovenia | DFS | DFS | Y | C | 1 | 0.05 | 0 | 0 | 1 | 0.05 | 6 | 0.29 | 3 | 0.15 |
| Spain f | DFS | DFS | Y | C | 22 | 0.05 | 25 | – | 10 | – | 20 | 0.04 | 40 | 0.09 |
| Sweden | DFS | DFS | Y | C | 10 | 0.10 | 10 | 0.10 | 7 | 0.07 | 14 | 0.14 | 11 | 0.11 |
| EU Total 27 | – | – | 198 | 0.04 | 162 | 0.03 | 132 | 0.03 | 285 | 0.06 | 358 | 0.08 | ||
| United Kingdom g | – | – | – | – | – | – | – | – | – | – | 24 | 0.04 | – | – |
| EU Total | – | – | 198 | 0.04 | 162 | 0.03 | 132 | 0.03 | 309 | 0.06 | 358 | 0.08 | ||
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| Norway | DFS | DFS | Y | C | 1 | 0.02 | 3 | 0.06 | 2 | 0.04 | 4 | 0.08 | 3 | 0.06 |
| Liechtenstein | DFS | DFS | Y | C | 0 | 0 | 0 | 0 | 3 | 0.03 | 7 | 0.08 | 5 | 0.06 |
| Switzerland h | DFS | DFS | Y | C | 6 | 0.07 | 6 | 0.07 | ||||||
Abbreviations: –, Data not reported; DFS, Disease‐free status from infection with B. abortus, B. melitensis and B. suis in bovine animal populations and/or in ovine and caprine animal populations.
Bovine animal populations.
Ovine and caprine animal populations.
Y, yes; N, no; A, aggregated data; C, case‐based data.
No surveillance system.
Metropolitan France obtained disease‐free status in 2022 whereas overseas French regions did not have this status.
Data incomplete for 2020–2021, rate not estimated.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
All zones of the MS have disease‐free status.
Not all zones of the MS have disease‐free status.
No zones of the MS have disease‐free status.
In 2022, the proportion of human infections acquired in the EU was 32.3% (64 out of 198 cases), a decrease compared with 46.9% (76 out of 162) in 2021 and 42.6% (329 out of 773) in 2018–2020. On the other hand, the proportion of infections acquired outside the EU was 19.2% (38 out of 198 cases, most of which were from Iraq), an increase compared with 13.0% (21 out of 162) in 2021 and 14.9% (115 out of 773) in 2018–2020. The proportion of cases with unknown travel status or travel destination was 48.5% (96 out of 198 cases), an increase compared with 40.1% (65 out of 162) in 2021 and 45.9% (355 out of 773) in 2018–2020 (Table 40).
The number of confirmed, domestically acquired brucellosis cases in humans (patients not having been outside the country of notification during the disease incubation period) is overlaid with the national prevalence data on Brucella‐positive cattle herds, and sheep and goat flocks in the EU in 2022 in Figure 14. Greece, Portugal and Spain had the highest number of confirmed domestic cases in humans. Italy, which reported a high number of human brucellosis cases over the years, did not provide information on the origin of infection for 2022. Greece, Portugal and Italy also had the highest prevalence of Brucella‐positive ruminant herds.
FIGURE 14.
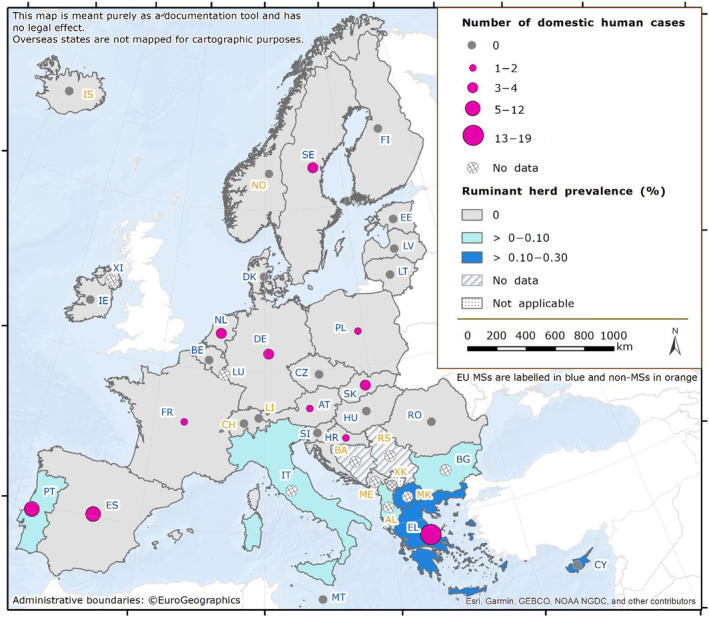
Number of confirmed, domestically acquired brucellosis cases in humans and national prevalence of Brucella‐positive cattle herds, and sheep and goat flocks, in EU MSs and non‐MS countries, 2022.
In 2022, clear seasonality was observed in the number of confirmed brucellosis cases in the EU, with more cases reported from May to September (Figure 13). Over the 2018–2022 period, there was a significantly decreasing trend overall in the EU, and four MSs (Germany, Greece, Italy and Portugal) exhibited a significantly decreasing 5‐year trend from 2018 to 2022. None of the MSs reported an increasing trend.
FIGURE 13.
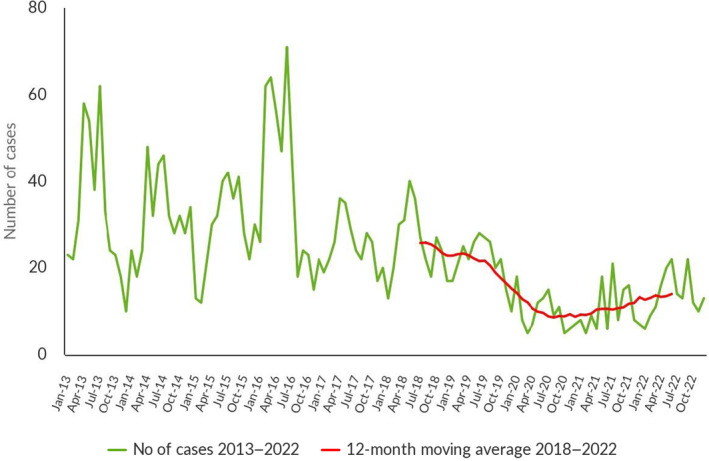
Trend in reported confirmed human cases of brucellosis in the EU, by month, 2018–2022. Source: Austria, Belgium, Cyprus, Czechia, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia and Sweden.
Ten MSs provided information on hospitalisation. Out of 198 human cases, 79 (39.9%) were reported with information on hospitalisation. Among these, 55 (69.6%) were hospitalised. This is an increase of 16.0% compared with the data for 2021 (60.0%). Greece, Portugal and Spain reported the highest number of cases with information about hospitalisation (35, 13 and 12, respectively), most of which required hospital care. No deaths were recorded in 2022, as was the case in 2021.
Out of 198 human cases, 89 (44.9%) were reported with information on the Brucella species by 17 MSs. B. melitensis was reported as the aetiological agent in 84 cases (94.4%); B. abortus was reported in four cases (4.5%); and other (unspecified) Brucella species in one case (1.1%).
The proportion of B. melitensis infections was higher than in 2021 (87.9%). Only 20 (36.4%) out of 55 hospitalised cases were reported with information on the Brucella species. B. melitensis was reported as the aetiological agent in 19 hospitalised cases, and other (unspecified) Brucella species in one hospitalised case.
6.3.3. Brucella in food
Very few monitoring data for Brucella were submitted in 2022, as was the case in previous years. In total, 182 samples of ‘milk’, ‘cheese' and ‘other dairy products’ were collected from processing plants by three MSs (Italy, Portugal and Spain). No positive sample was reported.
6.3.4. Brucella in animals
Surveillance data for bovine brucellosis, and ovine and caprine brucellosis
Cattle
The status of countries for brucellosis in cattle increased to 22 Member States and the United Kingdom (Northern Ireland) having DFS in 2022. Spain, which has not reported any positive herds since 2019, was declared DFS in 2022 for its the whole territory. Out of the five MSs with zones UEP (Bulgaria, Greece, Hungary, Italy and Portugal), only Italy reported increasing numbers of DFS zones. Bulgaria, Greece and Hungary did not have any DFS zone.
Two countries had DFS zones or provinces in cattle:
-
–
Italy: 13 regions and 11 provinces,
-
–
Portugal: one region (Algarve) and 10 districts (from the centre region and from the Azores islands)
Lichtenstein, Norway, Switzerland and the United Kingdom (Northern Ireland) have DFS in accordance with the EU legislation. Iceland, which has no special agreement on animal health (status) with the EU, has never reported any brucellosis cases caused by B. abortus, B. melitensis or B. suis. In 2022, the overall proportion of cattle herds infected in the EU remained low (< 0.001%; 424 out of 1597,251 herds), with 21 MSs and the United Kingdom (Northern Ireland) reporting no cases of brucellosis in cattle. Greece, Italy and Portugal reported the most infected herds.
In 2022, the proportion of cattle herds infected in the DFS MSs remained very low with 13 infected herds (< 0.001%; 13 out of 105,293 herds).
In 2022, the prevalence of brucellosis‐positive cattle herds remained very low in the UEP zones of the five non‐disease‐free MSs, with 411 positive herds (0.39%; 411/1,491,958;), compared with 546 (0.43%) in 2021. The number of positive herds out of all herds reported by Italy in its UEP zones was 346 (453 in 2021), while this number was 21 in Portugal (24 in 2021). Greece reported 42 positive herds (69 in 2021), while Bulgaria reported only two (zero in 2021).
Comparing prevalence data from 2013 to 2022, the overall annual number of cattle herds that were reported positive in UEP zones decreased to 411, while the prevalence of positive cattle herds increased from 0.10% to 0.39% (Figure 15). This is due to a reduction in the number of UEP zones and the resulting drop in the total number of cattle herds of interest.
FIGURE 15.
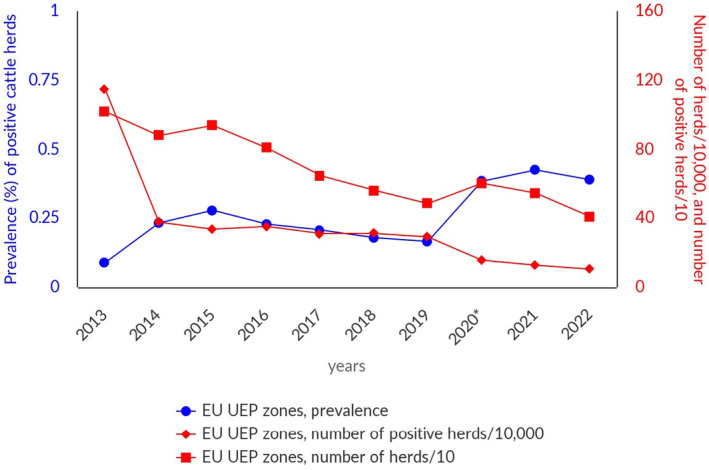
Prevalence of Brucella‐positive cattle herds, in zones under an eradication programme (UEP), EU, 2013–2022. UEP, under an eradication programme.
In 2022, no cases of bovine brucellosis were detected in the four non‐MS countries of Iceland, Liechtenstein, Norway and Switzerland, which are disease‐free. In the Balkans area, the disease is still present in cattle, with seropositive results reported by the EU candidate countries Albania (9 positive herds, 0.008%), Republic of North Macedonia (14 positive herds, 0.103%) and Serbia (7 positive herds, 0.002%) from national monitoring data. Albania reported 31 seropositive results from blood samples (out of 31,724 animals) and nine seropositive farms from milk samples (out of 2359 tests). Republic of North Macedonia reported 214 seropositive animals from 110,090 tested (0.2%), whereas Serbia reported seven positive cattle out of 444,769 (0.002%). Kosovo 37 reported 1.3% positive bovines (78/6000).
For a further interactive look at Brucella monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
Sheep and goats
In 2022, 20 MSs and the United Kingdom (Northern Ireland) were DFS with regards to ovine and caprine brucellosis, while seven MSs had UEP zones (Bulgaria, Croatia, France, Greece, Italy, Malta and Portugal). In 2022, the overall proportion of sheep and goat flocks infected with B. abortus, B. melitensis or B. suis in the EU remained low (0.02%; 236 out of 1023,162 flocks). Out of these seven MSs, three had DFS zones (France, Italy and Portugal), and four MSs had no zones with DFS (Bulgaria, Croatia, Greece and Malta). Italy had increasing numbers of DFS zones. In France, no cases of brucellosis have been reported in small ruminants since 2003, and the whole of metropolitan France obtained DFS in 2022.
Three countries had DFS zones or provinces for sheep and goats:
-
–
France: 13 metropolitan regions,
-
–
Italy: 15 regions and eight provinces,
-
–
Portugal: one region (the autonomous region of the Azores).
In the DFS MSs, prevalence was low, with 20 MSs and the United Kingdom (Northern Ireland) not reporting any case of brucellosis, and Cyprus and Spain reporting one positive flock each (nine reported by Spain in 2021), resulting in an overall prevalence in the DFS zones lower than 0.01% (2 out of 868,229), as was the case in 2021.
In 2022, the seven MSs with UEP zones reported 234 positive flocks (0.15%, 234 out of 154,933 flocks), compared with 331 (0.18%) in 2021 (Figure 16). The number of positive flocks reported by these MSs was 13 in Greece (26 in 2021), 66 in Italy (107 in 2021), 154 in Portugal (196 in 2021) and 1 in Bulgaria (zero in 2021). No positive flocks were reported by Croatia, France or Malta. For the last 3 years, Croatia has reported zero infected herds, indicating that eradication of sheep and goat brucellosis is almost achieved.
FIGURE 16.
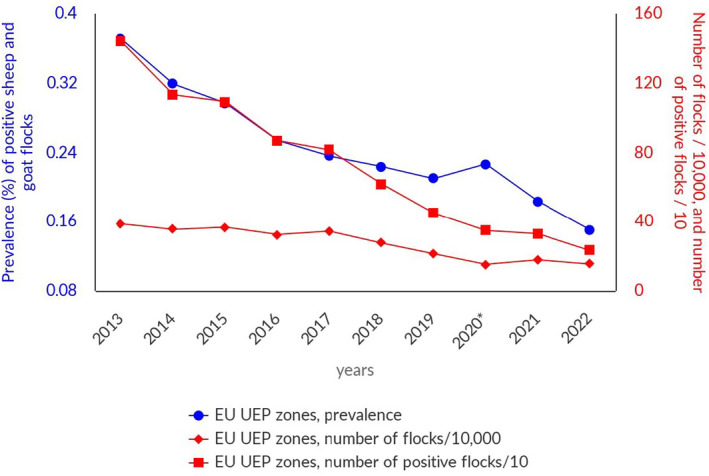
Prevalence of Brucella‐positive sheep and goat flocks, in zones under an eradication programme (UEP), EU, 2013–2022. UEP, under an eradication programme.
From 2013 to 2022, the overall annual number of reported positive sheep and goat flocks in the UEP zones decreased to 234, while the prevalence of positive flocks decreased continuously to 0.15% (Figure 16).
No cases of brucellosis were detected in sheep and goat flocks in 2022 in the following non‐MS countries: Albania, Iceland, Montenegro, Norway, Switzerland and the United Kingdom (Northern Ireland). Republic of North Macedonia reported 24 positive flocks and 437 seropositive small ruminants out of 493,336 (0.09%). Serbia reported only two infected animals out of 1,350,699 (< 0.0002%) from national monitoring data on ovine and caprine brucellosis. Kosovo 38 reported 0.3% positive sheep and goats (5/2000).
For a further interactive look at Brucella monitoring results, several dashboards have been implemented (different filters can be applied to query the data) (here).
Surveillance data for Brucella from animals other than bovine animals, sheep and goats
Similarly to 2021 reports on Brucella from animals other than cattle, and sheep and goats, Brucella species were reported from a wide range of animal species. B. canis was isolated in dogs from four MSs (France, the Netherlands, Sweden and Romania) and Norway. Four MSs reported 92 positive dogs out of 446 tested animals (20.6%). A total of 852 positive microbiological or polymerase chain reaction (PCR) results were reported in pigs and wild boars in eight MSs (Bulgaria, Croatia, France, Germany, Italy, Romania, Slovenia and Spain) and in Switzerland, together with 3927 seropositive results. Surveillance programmes in wildlife are expanding, thus confirming that B. suis biovar 2 is circulating throughout Europe. Unspecified Brucella species were found in dogs, marine mammals, wild deer and wild boars; B. ceti was found in four dolphins in Italy and B. pinnipedialis in two seals in Finland; and two strains of B. microti were isolated from ‘farmed’ frogs in France.
6.4. Discussion
The 5‐year EU trend of confirmed cases of brucellosis in humans declined significantly from 2018 to 2022. However, the EU notification rate in 2022 was higher (0.04 per 100,000 population) than that reported in 2021. Where such information was available, it was clear that human cases were commonly associated with hospitalisation. Human brucellosis remains a persistent public health problem in some MSs, especially in Greece where brucellosis is endemic in sheep and goats. A mean annual notification rate of 0.9/100,000 population was documented in humans in 2005–2020 (Dougas et al., 2022; Kefaloudi et al., 2022). Since the EU‐level brucellosis surveillance started in 2007, Greece has reported a notification rate about 10 times higher than the EU average. However, this trend has been decreasing over the years, and the 5‐year 2018–2022 trend in Greece showed a significant decrease.
In 2022, infections acquired in the EU decreased slightly, which was mainly due to the reduction of cases in Greece. Cases acquired outside the EU increased compared with the previous year. This was likely due to the recovery of international travel and the tourism sectors post‐COVID. Cases were still at a lower level than before the pandemic.
Like in 2021, the highest numbers of domestic human cases were reported in countries that are not free from brucellosis in cattle or in sheep and goats, such as Greece, Spain, Portugal and Italy. Human cases were relating to brucellosis in the ruminant population, since many infected herds or flocks, or both, were identified in these countries. Persons working with farm animals are known to be at increased risk of brucellosis, which remains the predominant occupational disease. Food borne exposure is normally limited to consumption of unpasteurised milk and dairy products or undercooked contaminated meat from countries where brucellosis is endemic in animals. Conversely, human cases in DFS countries, such as France, Germany and Sweden, were largely associated with travel outside the EU. Interestingly, neither Hungary (non‐DFS for cattle) nor Malta (non‐DFS for sheep and goats) reported any cases of human brucellosis.
In 2022, human cases of brucellosis were almost entirely caused by infection with B. melitensis. Furthermore, B. melitensis was the major species involved in cases of hospitalisation where speciation information was provided. This information is very important when optimising risk management to further reduce the disease in humans, considering that B. melitensis is mainly, if not completely, associated with brucellosis in sheep and goats. In contrast to 2021, no human cases were attributed to B. suis. However, this pathogen should be monitored over the coming years to detect any trend for a potentially emerging condition.
In 2021, the regulatory framework for bovine brucellosis, and ovine and caprine brucellosis changed substantially. These infections are currently considered diseases to be controlled in all MSs to eradicate the disease in bovine populations (Bos spp., Bubalus spp. and Bison spp.), and in ovine and caprine populations, throughout the EU, and to be kept under surveillance in other mammals. All MSs are required to have a surveillance or a control and eradication programme in place that is approved by the European Commission. This should lead in the coming years to further improvement in the already very satisfactory epidemiological situation.
Bovine brucellosis, and ovine and caprine brucellosis have been eradicated by most EU MSs. In MSs and DFS zones, very few infected herds or flocks were reported for 2022: 13 infected cattle herds, and two infected sheep and goat flocks.
In 2022 the eradication of brucellosis in bovines has been achieved in Spain. Brucellosis in sheep and goats has been eradicated in metropolitan France. Some MSs were not officially free from bovine brucellosis or from brucellosis in sheep and goats, and both infections were mostly reported in Greece, Italy and Portugal. In Greece, the proportion of tested herds and flocks remained limited, which may affect surveillance precision. The overall number of positive herds and flocks should be interpreted differently between countries, as the proportion of those tested was highly variable between MSs.
Nevertheless, from 2013 to 2022, the overall annual number of reported positive ruminants in the UEP zones decreased, with a decrease in prevalence. In Italy, problems were concentrated in the southern part of the country and Sicily. Moreover, the infection was present in water buffalo from the provinces of Salerno and Caserta, where in the latter province, a drastic increase in the prevalence and incidence of infection in buffaloes has been observed in recent years. About 80% of Campania's buffalo population is found in Caserta. The infection is concentrated in the geographic areas with the highest density of animals and farms per square kilometre (Ottaiano et al., 2022). In UEP zones, non‐foodborne transmission of brucellosis to humans may still occur through direct contact with infected animals. People working with farm animals, including farmers, livestock breeders, butchers, abattoir workers and veterinarians, are known to be at increased risk of brucellosis in endemic countries.
In the Balkans, Albania reported positive results for bovine brucellosis, and Republic of North Macedonia and Serbia reported positive results for brucellosis in bovines, and in sheep and goats.
Attention should also be paid to canine brucellosis cases caused by B. canis, which are also considered zoonotic, even though this infection is not included in the zoonosis directive. In the last 2 years, an increased number of cases was described in Italy (De Massis et al., 2021), France, the Netherlands (van Dijk et al., 2021) and the United Kingdom (England; source APHA). Although zoonotic B. canis infections are rare, the first two human cases of B. canis infection were reported in the Netherlands and in the United Kingdom in dog owners, following recent exposure to B. canis‐infected dogs (Boyden, 2022; Kolwijck et al., 2022).
Consideration should also be given to the recent inclusion of all Ochrobactrum organisms in the genus Brucella by a group of taxonomists, based on recent gene content analysis studies. The adoption of the name Brucella for these organisms has several implications as reported by (Moreno et al., 2022), including possible misidentification and misunderstanding among clinical laboratories and veterinarians, physicians and public health authorities dealing with brucellosis.
In conclusion, although cases of brucellosis in humans and ruminants are declining in the EU, brucellosis is still an animal health concern with public health relevance, especially in southern European countries that are not free from the disease.
7. TRICHINELLA
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
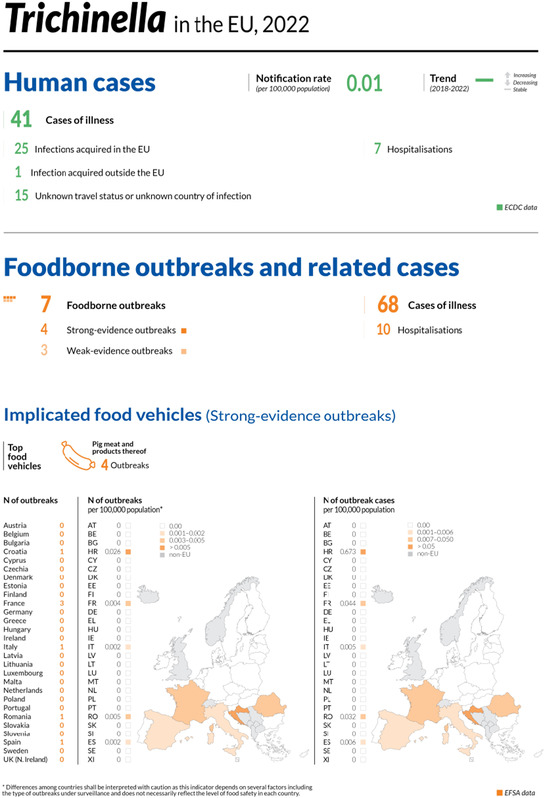
The number of cases and the notification rate include two cases reported erroneously by Finland.
7.1. Key facts
In 2022, there were 41 confirmed cases of human trichinellosis, corresponding to an European Union notification rate of 0.01 cases per 100,000 population 39 and a decrease of 51.9% compared with 2021 (0.02 cases per 100,000 population).
The overall trend for trichinellosis did not show any significant increase or decrease in 2018–2022.
In 2022, no infections with Trichinella were reported in tested fattening pigs (33.7 million) or breeding pigs (0.47 million) raised under controlled housing conditions, recognised by the competent authorities, confirming that farming conditions are a key factor in preventing infection with this zoonosis.
In other domestic pigs, 0.00004% (71 out of 175 million) were positive for Trichinella. Romania accounted for most of the positive pigs (59), followed by Croatia (eight 40 ), Spain (two), Bulgaria (one) and Poland (one).
No Trichinella infections were detected in domestic solipeds in the European Union in 2022, as during 2018–2021.
In 2022, the proportions of Trichinella‐positive hunted wild boar and foxes (indicator animals) were 0.08% and 0.95%, respectively, compared with 0.07% and 1.6% in 2021, respectively.
7.2. Surveillance and monitoring of Trichinella in the EU
7.2.1. Humans
For 2022, 26 EU MSs reported information on trichinellosis in humans. The surveillance of Trichinella infections is mandatory in all reporting MSs, except in Belgium and France, where the surveillance systems are voluntary. Denmark has no surveillance system for trichinellosis, and the disease is not notifiable or reported at the EU level. Twenty‐two MSs used the EU case definition, other case definitions were used by three MSs, and Belgium did not specify the case definition used. The surveillance systems cover the whole population in all MSs reporting trichinellosis data. All countries reported case‐based data except Belgium, Bulgaria and the Netherlands, which reported aggregated data.
7.2.2. Animals
Trichinella monitoring data for domestic pigs (both fattening and breeding animals), farmed wild boar and solipeds
In accordance with Commission Implementing Regulation (EU) 2015/1375, 41 all Trichinella‐susceptible animals intended for human consumption in the EU, i.e. domestic pigs (both fattening and breeding animals), farmed wild boar and solipeds, should be tested for the presence of Trichinella larvae in the muscles unless carcases have undergone a freezing treatment (freezing inactivates the parasite). ISO 18743/2015 or an equivalent method should be used (Commission Implementing Regulation (EU) 2015/1375). Therefore, data on Trichinella infections in these animals are comparable across MSs because the monitoring schemes are harmonised and the data collected and reported to EFSA originate from census sampling (EFSA BIOHAZ Panel, 2013a, 2013b) (Table 42).
TABLE 42.
Summary of Trichinella statistics, relating to humans (2018–2022), domestic pigs (2022) and other main animal species (2018–2022), EU.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 41 c | 77 | 117 | 97 | 66 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0.01 c | 0.02 | 0.03 | 0.02 | 0.01 | ECDC |
| Number of reporting MSs | 26 | 26 | 26 | 27 | 27 | ECDC |
| Infections acquired in the EU | 25 | 29 | 99 | 26 | 18 | ECDC |
| Infections acquired outside the EU | 1 | 2 | 2 | 2 | 1 | ECDC |
| Unknown travel status or unknown country of infection | 15 c | 46 | 16 | 69 | 47 | ECDC |
| Number of outbreak‐related cases | 68 | 2 | 119 | 44 | 114 | EFSA |
| Total number of outbreaks | 7 | 1 | 6 | 5 | 10 | EFSA |
| Animals d | ||||||
| Domestic pigs raised under controlled housing conditions, recognised by the competent authorities | ||||||
| Number of units tested | 34,183,655 | – | – | – | – | EFSA |
| % of positive units | 0 | – | – | – | – | EFSA |
| Number of reporting MSs | 7 | – | – | – | – | EFSA |
| Domestic pigs (other) | ||||||
| Controlled housing conditions not recognised by the competent authorities | ||||||
| Number of units tested | 15,644,310 | – | – | – | – | EFSA |
| % of positive units | 0 | – | – | – | – | EFSA |
| Number of reporting MSs | 8 | – | – | – | – | EFSA |
| Not controlled housing conditions | ||||||
| Number of units tested | 96,748,782 | – | – | – | – | EFSA |
| % of positive units | 0.00007 | – | – | – | – | EFSA |
| Number of reporting MSs | 20 | – | – | – | – | EFSA |
| Other, unspecified | ||||||
| Number of units tested | 63,084,065 | – | – | – | – | EFSA |
| % of positive units | 0 | – | – | – | – | EFSA |
| Number of reporting MSs | 5 | – | – | – | – | EFSA |
| Farmed wild boar | ||||||
| Number of units tested | 5372 | 5755 | 3922 | 7570 | 6343 | EFSA |
| % of positive units | 0 | 0 | 0 | 0 | 0 | EFSA |
| Number of reporting MSs | 8 | 8 | 6 | 7 | 7 | EFSA |
| Hunted wild boar | ||||||
| Number of units tested | 1,514,255 | 1,786,892 | 1470,830 | 1,757,383 | 1,465,788 | EFSA |
| % of positive units | 0.08 | 0.07 | 0.05 | 0.08 | 0.09 | EFSA |
| Number of reporting MSs | 21 | 20 | 21 | 23 | 23 | EFSA |
| Foxes | ||||||
| Number of units tested | 6652 | 6776 | 5764 | 6696 | 6612 | EFSA |
| % of positive units | 0.95 | 1.6 | 0.85 | 1.3 | 1.6 | EFSA |
| Number of reporting MSs | 11 | 11 | 9 | 10 | 10 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States; –, Data not reported.
For 2021, data on animal samples from the United Kingdom (Northern Ireland) were considered. Following the agreement on the withdrawal of the United Kingdom from the EU, particularly with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were considered for 2018–2019 since the United Kingdom was still an EU MS. However, on 1 February 2020, it became a third country.
The number of cases and the number of confirmed cases × 100,000 include two cases reported erroneously by Finland.
Units: animals and/or slaughter animal batches.
Domestic pigs, farmed and hunted wild boar, and other wild animals (e.g. bears) that are not processed to be placed on the EU market (e.g. those intended for own consumption) are exempted from Commission Implementing Regulation (EU) 2015/1375, and their control falls under national legislation. Commission Implementing Regulation (EU) 2015/1375 states that the reporting of data for domestic pigs shall, at least, provide specific information related both to the number of animals tested that were raised under controlled housing conditions and to the number of breeding sows, boar and fattening pigs tested. Furthermore, the regulation states that a negligible risk status for a country or region is no longer recognised.
For the first time, for reporting 2022 Trichinella monitoring results for domestic pigs, MSs had the possibility of specifying whether the pigs were raised under controlled housing conditions officially recognised by the CA (RCHC) or not (Pigs – others). Further voluntary reporting could specify whether these pigs were raised under controlled housing conditions not recognised by the CA (CHC) or whether they were not raised under controlled housing conditions (NCHC). When Trichinella‐positive results were reported, it was mandatory to indicate whether the pigs were raised indoors or outdoors.
Trichinella monitoring data for animals other than domestic pigs, farmed wild boar and solipeds
MSs should monitor the circulation of these nematodes in the main natural reservoir hosts (carnivorous and omnivorous animals) to acquire information on the risk of transmission to domestic animals (and from these to humans) and on the introduction of new Trichinella species from non‐EU countries. However, monitoring data provided by the MSs to EFSA are generated by non‐harmonised monitoring schemes across MSs without mandatory reporting requirements. Wild animals are the main reservoir hosts of Trichinella, and their biology and ecology vary from one MS to another and from one region or habitat in the same MS to another due to the human and environmental impact on ecosystems, resulting in different transmission patterns and prevalence rates of infection. Therefore, data on Trichinella in wild animals are not fully comparable among MSs, as neither harmonised monitoring schemes nor mandatory reporting requirements are in place, and the reported findings must be interpreted with caution. These data allow descriptive summaries to be produced at the EU level but preclude any subsequent data analysis, such as assessing temporal and spatial trends (Table 1).
7.3. Results
7.3.1. Overview of key statistics, EU, 2018–2022
Table 42 summarises EU‐level statistics on human trichinellosis and Trichinella in animals for 2018–2022. More detailed descriptions of these statistics are provided in the subsections below and in the chapter on foodborne outbreaks.
7.3.2. Human trichinellosis
In 2022, 41 confirmed cases 42 of trichinellosis were reported by 26 MSs, which was a decrease compared with 2021 (Table 42). The EU notification rate decreased by 51.9% from 0.02 per 100,000 in 2021 to 0.01 per 100,000 in 2022. This decrease was mainly due to the reduction in the number of confirmed human cases reported in 2022 by Bulgaria (−69%), Croatia (−100%) and Austria (−80%). The number of MSs reporting zero cases in 2022 increased by 11.8% (N = 17).
In 2022, Latvia and Bulgaria had the highest notification rates in the EU (0.16 and 0.13 cases per 100,000, respectively), followed by Estonia (0.08 cases per 100,000) (Table 43).
TABLE 43.
Reported confirmed human cases of trichinellosis and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 2 | 0.02 | 10 | 0.11 | 6 | 0.07 | 1 | 0.01 | 2 | 0.02 |
| Belgium b | Y | A | 0 | – | 0 | – | 0 | – | 0 | – | 0 | – |
| Bulgaria | Y | A | 9 | 0.13 | 29 | 0.42 | 13 | 0.19 | 55 | 0.79 | 45 | 0.64 |
| Croatia | Y | C | 0 | 0 | 17 | 0.42 | 0 | 0 | 3 | 0.07 | 0 | 0 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Denmark c | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | Y | C | 1 | 0.08 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland d | Y | C | 2 | 0.04 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | Y | C | 15 | 0.02 | 2 | < 0.01 | 1 | < 0.01 | 2 | < 0.01 | 0 | 0 |
| Germany | Y | C | 0 | 0 | 2 | < 0.01 | 1 | < 0.01 | 3 | < 0.01 | 0 | 0 |
| Greece | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hungary | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0.02 |
| Ireland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Italy | Y | C | 4 | 0.01 | 0 | 0 | 79 | 0.13 | 10 | 0.02 | 2 | < 0.01 |
| Latvia | Y | C | 3 | 0.16 | 7 | 0.37 | 1 | 0.05 | 1 | 0.05 | 1 | 0.05 |
| Lithuania | Y | C | 0 | 0 | 1 | 0.04 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | Y | A | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 0 | 0 |
| Poland | Y | C | 1 | < 0.01 | 2 | 0.01 | 11 | 0.03 | 2 | 0.01 | 2 | 0.01 |
| Portugal | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 0 | 0 |
| Romania | Y | C | 4 | 0.02 | 6 | 0.03 | 4 | 0.02 | 6 | 0.03 | 10 | 0.05 |
| Slovakia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Slovenia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Spain e | Y | C | 0 | 0 | 1 | – | 1 | – | 12 | 0.03 | 2 | 0 |
| Sweden | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EU Total 27 | 41 d | 0.01 d | 77 | 0.02 | 117 | 0.03 | 97 | 0.02 | 66 | 0.02 | ||
| United Kingdom f | Y | C | – | – | – | – | – | – | 0 | 0 | 0 | 0 |
| EU Total | 41 d | 0.01 d | 77 | 0.02 | 117 | 0.03 | 97 | 0.02 | 66 | 0.01 | ||
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Liechtenstein | Y | C | 0 | 0 | 0 | 0 | 3 | 0.03 | 0 | 0 | 1 | 0.01 |
| Switzerland g | Y | C | 9 | 0.10 | 6 | 0.07 | ||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Sentinel surveillance, notification rate not calculated.
No surveillance system.
The number of cases and confirmed cases*100,000 include two cases reported erroneously by Finland.
Data not complete for 2020–2021. Notification rate not calculated.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Until 2020, Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for 2018–2020.
In 2022, 26 cases (63.4%) of trichinellosis with known travel status and known country of infection were reported as having been acquired in the EU. One MS (Austria) reported one travel‐associated trichinellosis case infected outside the EU. Travel information was not reported for 15 cases4 (36.6%) (Table 42).
The EU trend in confirmed cases of trichinellosis did not show any significant decrease or increase over the period 2018–2022 (Figure 17). Only Italy reported a significantly decreasing trend during the same period, and none of the MSs observed a significant increasing trend. Bulgaria was not included in the EU trend calculations since monthly data were unavailable.
FIGURE 17.
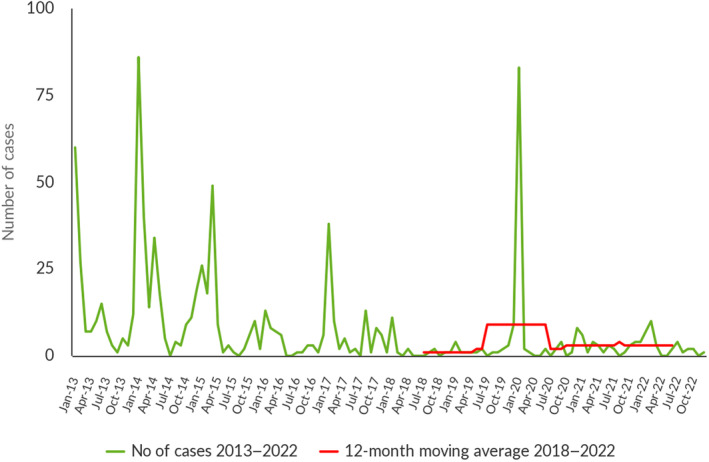
Trend in reported confirmed human cases of trichinellosis in the EU by month, 2018–2022. Sourcea: Austria, Cyprus, Czechia, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Poland, Portugal, Romania, Slovakia, Slovenia and Sweden. aThe case distribution includes two cases reported erroneously by Finland in 2021 and 2022.
Of the nine MSs 43 reporting confirmed cases for 2022, five provided information on hospitalisation (for 11 cases, i.e. 26.8% of all confirmed cases reported in the EU). Of these 11 cases, seven (63.6%) were hospitalised, which was an increase compared with 2021 (38.5%). Five MSs provided information on the outcome of the cases (11 cases, i.e. 26.8% of all confirmed cases); no deaths were reported. T. spiralis and T. britovi were identified as the causative agents of 215 (87.5%) and three (12.5%) confirmed human cases, respectively, reported by four MSs.5
In 2022, 129 FBO‐associated human cases were reported to EFSA. Trichinella was identified in seven FBOs reported by five MSs: Croatia, France, Italy, Romania and Spain. Four out of seven FBOs were reported as strong‐evidence FBOs and affected 40 people, eight of whom needed to be hospitalised. Three FBOs were reported as weak‐evidence FBOs and involved 28 people, two of whom were hospitalised. The FBOs reported as strong‐evidence FBOs by Croatia and Romania were caused by T. spiralis, which was identified in ‘pig meat and products thereof’ and in ‘meat from pig ‐ fresh’, respectively. Two non‐MSs (Bosnia and Herzegovina and Serbia) reported four strong‐evidence FBOs, with 61 human cases of whom four were hospitalised. T. spiralis was the causative agent identified in ‘meat from pig – meat products’ reported by Bosnia and Herzegovina and in ‘meat and meat products’ reported by Serbia.
7.3.3. Trichinella infection in food and animals
No MSs reported monitoring data for food for 2022.
In 2022, 31 countries (27 MSs, the United Kingdom (Northern Ireland), and three non‐MSs) provided information on Trichinella in domestic animals (pigs and/or farmed wild boar). Six MSs and the United Kingdom (Northern Ireland) reported data on breeding and/or fattening pigs RCHC; no positive findings were reported. Eight MSs reported data on breeding and/or fattening pigs raised under CHC; no positive findings were reported. Moreover, eight MSs reported monitoring data in farmed wild boar with no positive results reported (Table 44).
TABLE 44.
Trichinella monitoring results for domestic pigs and farmed wild boar in reporting EU MSs and non‐MS countries, by housing conditions a , 2022.
| Country | N positive/tested (% positive) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Controlled housing conditions, recognised by the competent authorities (RCHC) | Other | ||||||||
| Controlled housing conditions, not recognised by the competent authorities (CHC) | Not controlled housing conditions (NCHC) | Other, unspecified | |||||||
| Fattening pigs | Breeding pigs | Fattening pigs | Breeding pigs | Fattening pigs | Breeding pigs | Farmed wild boar | Fattening pigs | Breeding pigs | |
| Austria | – | – | – | – | 0/4,841,259 (0) | 0/80,315 (0) b | 0/240 (0) | _ | _ |
| Belgium | 0/11,267,485 (0) | – | – | – | 0/39,953 (0) | 0/4,300,265 (0) c | – | _ | _ |
| Bulgaria | – | – | 0/151,270 (0) d | 0/1805 (0) e | 1/24,427 (< 0.01) f | – | – | _ | _ |
| Croatia g | – | – | – | – | 8/− | – | – | _ | _ |
| Cyprus | – | – | – | – | 0/536,462 (0) | 0/12,431 (0) | – | _ | _ |
| Czechia | – | – | 0/2,277,831 (0) | – | – | – | – | _ | _ |
| Denmark | 0/16,449,465 (0) | 0/313,453 (0) c | – | – | 0/681,624 (0) | 0/271,261 (0) c | 0/386 (0) | _ | _ |
| Estonia | – | – | 0/46,123 (0) | – | 0/95,229 (0) | – | – | _ | _ |
| Finland | 0/446 (0) | 0/80 (0) | – | – | – | – | 0/223 (0) | 0/1,835,427 (0) | 0/34,491 (0) |
| France | – | – | 0/132,406 (0) | 0/191,166 (0) c | 0/576,125 (0) | 0/12,853 (0) c | 0/327 (0) | _ | _ |
| Germany | – | – | – | – | – | – | 0/942 (0) | 0/47,254,763 (0) | _ |
| Greece | – | – | – | – | 0/749,273 (0) h | 0/14,926 (0) i | 0/949 (0) | _ | _ |
| Hungary | – | – | – | – | 0/4,198,323 (0) | 0/93,511 (0) | – | _ | _ |
| Ireland | – | – | – | 0/91,189 (0) j | 0/3,545,265 (0) | – | – | _ | _ |
| Italy | 0/3,440,233 (0) | 0/98,030 (0) k | 0/5,622,924 (0) l | 0/61,643 (0) m | 0/50,011 (0) | – | 0/1213 (0) | _ | _ |
| Latvia | 0/502,601 (0) | _ | |||||||
| Lithuania | 0/829,042 (0) | – | – | – | – | – | – | _ | _ |
| Luxembourg | 0/146,037 (0) n | _ | |||||||
| Malta | – | – | – | – | 0/50,280 (0) | 0/931 (0) | – | _ | _ |
| Netherlands | 0/13,310,746 (0) | _ | |||||||
| Poland | – | – | – | – | 1/19,669,063 (< 0.01) o | – | – | _ | _ |
| Portugal | – | – | 0/3,839,997 (0) | 0/31,294 (0) c | 0/136,446 (0) p | 0/3215 (0) q | – | _ | _ |
| Romania | – | – | 0/3,172,631 (0) | 0/24,031 (0) | 56/223,677 (0.03) r | 3/80 (3.8) s | – | _ | _ |
| Slovakia | – | – | – | – | 0/500,253 (0) | 0/85,896 (0) | – | _ | _ |
| Slovenia | – | – | – | – | 0/145,194 (0) t | – | – | _ | _ |
| Spain | – | – | – | – | 2/54,507,190 (< 0.01) u | 0/812,710 (0) v | 0/1092 (0) | _ | _ |
| Sweden | 0/1722,200 (0) | 0/62,016 (0) w | – | – | 0/471,786 (0) | 0/18,540 (0) x | – | _ | _ |
| United Kingdom (Northern Ireland) | 0/1205 (0) t | – | – | – | – | – | – | _ | _ |
| EU Total (27 + XI) | 0/33,710,076 (0) | 0/473,579 (0) | 0/15,243,182 (0) | 0/401,128 (0) | 68/91,041,848 (< 0.01) | 3/5,706,934 (< 0.01) | 0/5372 (0) | 0/63,049,574 (0) | 0/34,491 (0) |
| Iceland | – | – | 0/74,530 (0) | – | – | – | – | _ | _ |
| Norway | – | – | – | – | 0/1,600,000 (0) y | – | – | _ | _ |
| Switzerland | – | – | – | – | 0/2,360,922 (0) | 0/31,096 (0) | – | _ | _ |
|
Total non‐EU Countries |
– | – | 0/74,530 (0) | – | 0/3,960,922 (0) | 0/31,096 (0) | – | 0/63,049,574 (0) | 0/34,491 (0) |
| Total EU (27+ XI) + non‐EU countries | 0/33,710,076 (0) | 0/473,579 (0) | 0/15,317,712 (0) | 0/401,128 (0) | 68/95,002,770 (< 0.01) | 3/5,738,030 (< 0.01) | 0/5372 (0) | 0/63,049,574 (0) | 0/34,491 (0) |
Abbreviation: –, Data not reported.
No pigs reported in 2022 with unspecified housing conditions.
Comprising 1570 boar.
Sows and boar.
Comprising 37,540 piglets.
Sows.
Including 24,310 outdoor pigs with one positive pig.
Croatia reported only positive results, comprising one indoor fattening pig (infected with T. spiralis), six gilts (including four infected with T. spiralis) and one sow (infected with T. spiralis) in indoor mixed herds.
Comprising 229 indoor piglets.
Indoors, comprising 270 boar.
Comprising 697 boar and 100 sows and boar.
Comprising 1709 boar and 1930 gilts.
Comprising 74,950 piglets.
Comprising 1729 boar and 1317 gilts.
Comprising 18,930 piglets and 674 pigs in mixed herds.
Indoor pigs with one positive pig (infected with T. spiralis).
Comprising 53,749 outdoor pigs.
Sows and boar, including 1763 outdoor pigs.
Indoor pigs with 56 positive pigs (including 46 infected with T. spiralis and four with T. britovi).
Indoor sows with three positive sows (infected with T. britovi).
Pigs in mixed herds.
Comprising 1,373,453 indoor pigs, 496,953 outdoor pigs with two positive pigs and 141,413 piglets.
Comprising 610 indoor pigs.
Comprising 489 boar.
Comprising 88 boar.
Indoor pigs.
Five MSs (Bulgaria, Croatia, Poland, Romania and Spain) reported positive findings for domestic pigs NCHC with a total of 71 (0.00004%) positive out of 175 million animals tested in 26 MSs. 44 Croatia reported eight positive indoor fattening pigs,44 Romania reported 56 (78.9%) and three (4.2%) positive indoor fattening and breeding pigs, respectively; Spain and Bulgaria reported two (2.8%) and one (1.4%) positive outdoor fattening pigs, respectively; and Poland reported one (1.4%) positive indoor fattening pig. Species identification was reported for 61 (85.9%) of 71 pigs. T. spiralis was detected in 54 (88.5%) and T. britovi in seven (11.5%) of the 61 pigs for which species identification was reported. As in previous years, these Trichinella infections were found in free‐range and backyard pigs reared in rural EU regions.
As shown in Figure 18, from 2013 to 2019 (7‐year period), Trichinella spp. were not reported in domestic pigs or farmed wild boar in 18 MSs, unlike in the other 10 MSs. In 2020, 2021 and 2022, Trichinella spp. in pigs were reported by seven (Bulgaria, Croatia, France, Greece, Italy, Romania and Spain), six (Croatia, Finland, France, Poland, Romania and Spain) and five (Bulgaria, Croatia, Poland, Romania and Spain) MSs, respectively.
FIGURE 18.
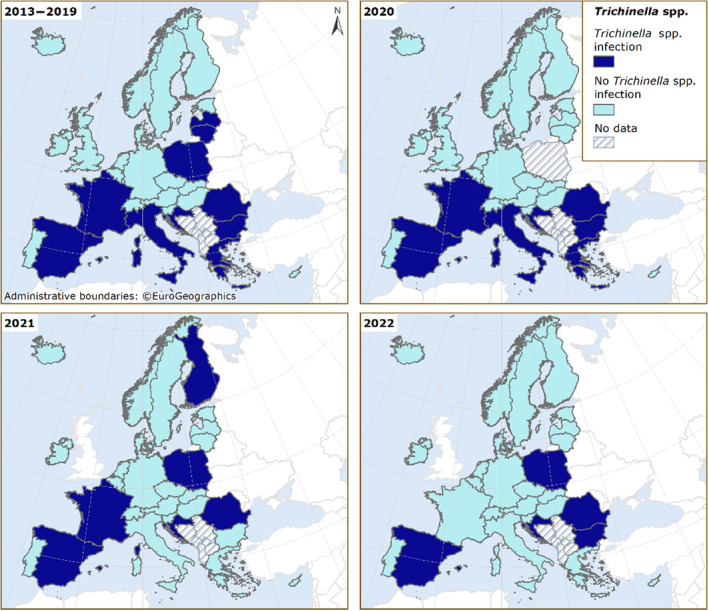
Trichinella spp. in domestic pigs and farmed wild boar in EU MSs and non‐MS countries, 2013–2022. Note: These distribution maps have been built based on data from reports (EFSA and ECDC, 2015a, 2015b, 2016, 2017, 2018, 2019, 2021a, 2021b, 2022).
In 2022, as in the previous five‐year period (2017–2021), positive findings were not reported either in 92,252 domestic solipeds tested in 20 MSs or in 8325 domestic solipeds tested in 2 non‐MSs (Iceland and Switzerland) (Table 45).
TABLE 45.
Trichinella monitoring results for hunted wild boar and wild boar with unspecified habitat, bears, foxes and domestic solipeds, in reporting EU MSs and non‐MS countries, 2022.
| Country | N positive/tested (% positive) | |||
|---|---|---|---|---|
| Hunted or unspecified wild boar | Bears | Foxes | Domestic solipeds | |
| Austria | 0/38,938 (0) | – | 1/214 (0.5) | 0/441 (0) |
| Belgium | 0/17,440 (0) | – | – | 0/6767 (0) |
| Bulgaria | 132/7617 (1.7) | – | – | 0/64 (0) |
| Croatia | 62/994 (6.2) | 2/4 (50.0) | – | – |
| Cyprus | – | – | 0/112 (0) | – |
| Czechia | 3/194,769 (0) | – | 1/2563 (0.04) | 0/59 (0) |
| Denmark | – | – | – | 0/487 (0) |
| Estonia | 7/3013 (0.23) | 6/78 (7.7) | – | 0/5 (0) |
| Finland | 1/1044 (0.10) | 5/110 (4.5) | 45/146 (30.8) | 0/838 (0) |
| France | 1/41,663 (0) | – | – | 0/2408 (0) |
| Germany | 28/418,567 (0.01) | – | 0/767 (0) | 0/3595 (0) |
| Hungary | 1/35,568 (0) | – | – | 0/97 (0) |
| Ireland | – | – | – | 0/1606 (0) |
| Italy | 7/177,744 (0) | 0/2 (0) | 14/2166 (0.65) | 0/24,334 (0) |
| Latvia | 37/10,053 (0.37) | – | – | 0/32 (0) |
| Luxembourg | 0/4240 (0) | – | 0/73 (0) | 0/5 (0) |
| Netherlands | 0/2718 (0) | – | – | 0/1984 (0) |
| Poland | 188/213,525 (0.09) | – | – | – |
| Portugal | 0/622 (0) | – | – | 0/322 (0) |
| Romania | 43/7029 (0.61) | 9/15 (60.0) | – | 0/14,560 (0) |
| Slovakia | 0/9789 (0) | 0/2 (0) | 2/91 (2.2) | – |
| Slovenia | 6/2246 (0.27) | 0/143 (0) | 0/58 (0) | 0/550 (0) |
| Spain | 643/212,873 (0.30) | – | – | 0/32,993 (0) |
| Sweden | 6/113,803 (0.01) | 2/476 (0.4) | 0/162 (0) | 0/1095 (0) |
| United Kingdom (Northern Ireland) | – | – | 0/300 (0) | – |
| EU Total (27 + XI) | 1165/1,514,225 (0.08) | 24/830 (2.9) | 63/6652 (0.95) | 0/92,252 (0) |
| Iceland | – | – | – | 0/7419 (0) |
| Norway | 0/219 (0) | – | – | – |
| Republic of North Macedonia | 42/2570 (1.6) | – | – | – |
| Switzerland | 0/11,582 (0) | – | 0/2 (0) | 0/906 (0) |
|
Total non‐EU countries |
42/14,371 (0.29) | – | 0/2 (0) | 0/8325 (0) |
| Total EU (27+ XI) + non‐EU countries | 1207/1,528,626 (0.08) | 24/830 (2.9) | 63/6654 (0.95) | 0/100,577 (0) |
Abbreviation: –, Data not reported.
Fifteen MSs reported positive findings for hunted wild boar (1165 positive results out of 1,514,225 animals tested [0.08%]). Species identification was provided for 776 wild boar (66.6%), of which 631 (81.3%) were infected with T. spiralis, 145 (18.7%) with T. britovi and one (0.13%) with T. nativa. For 389 (50%) animals, species identification was not reported.
Five MSs (Austria, Czechia, Finland, Italy and Slovakia) reported positive findings for Trichinella in foxes (Vulpes vulpes) with, in total, 63 (0.95%) positive out of 6652 tested animals in 10 MSs and the United Kingdom (Northern Ireland). T. britovi was identified in 10 (90.9%) animals and T. spiralis in 1 (9.1%) out of 11 positive foxes with species identification provided. Five MSs (Croatia, Estonia, Finland, Romania and Sweden) reported positive findings for Trichinella in bears (Ursus arctos), with 24 (2.9%) positive units out of 830 tested in eight MSs (Table 45). T. britovi, T. nativa and T. spiralis were identified in 11 (50.0%), 7 (31.8%) and 4 (18.2%) brown bears, respectively, out of 21 (87.5%) positive bears with species identification provided. Nine MSs and one non‐MS reported data on Trichinella in wild animals other than foxes, brown bears and wild boar. Positive findings were detected for wolves (14.1%), raccoon dogs (29.7%), lynxes (10.4%), birds (0.30%) and other animals (1.4%), as shown in Table 46. In wild animals, T. britovi was identified in three MSs (Italy (28 wolves), Poland (one wolf) and Sweden (one wolf)) and in one non‐MS (Switzerland [seven wolves and six lynxes]). T. pseudospiralis was documented in Finland (one otter). T. nativa was documented in Finland (two lynxes and one jackal) and Sweden (five lynxes and one wolf).
TABLE 46.
Trichinella monitoring results in other wild animals in reporting EU MSs and non‐MS countries, 2022.
| Country | N positive/tested (% positive) | |||||||
|---|---|---|---|---|---|---|---|---|
| Badgers | Wolves | Raccoon dogs | Birds | Lynxes | Raccoons | Martens | Other animals | |
| Austria | 0/31 (0) | – | – | – | – | – | – | 0/2 (0) a |
| Finland | 0/3 (0) | 20/53 (37.7) | 51/154 (33.1) | 1/1 (100) | 9/25 (36) | – | 0/1 (0) | 7/102 (6.9) b |
| Germany | 0/59 (0) | – | – | – | – | 0/158 (0) | 0/178 (0) | 0/211 (0) c |
| Hungary | – | – | – | – | – | – | – | 0/3 (0) d |
| Italy | 0/436 (0) | 36/332 (10.8) | 0/18 (0) | 0/416 (0) | – | – | 0/74 (0) | 0/164 (0) e |
| Latvia | – | – | – | – | – | – | – | 0/9 (0) f |
| Poland | – | 1/1 (100) | – | – | – | – | – | – |
| Slovakia | 0/1 (0) | – | – | – | – | – | – | – |
| Sweden | 0/6 (0) | 2/32 (6.3) | – | – | 5/110 (4.6) | – | – | 0/20 (0) g |
| EU Total (27 + XI) | 0/536 (0) | 59/418 (14.1) | 51/172 (29.7) | 1/417 (0.24) | 14/135 (10.4) | 0/158 (0) | 0/253 (0) | 7/511 (1.4) |
| Switzerland | 0/13 (0) | 7/35 (20.0) | – | – | 6/22 (27.3) | – | – | 0/3 (0) h |
| Total EU (27+ XI) + non‐EU countries | 0/549 (0) | 66/453 (14.6) | 51/172 (29.7) | 1/417 (0.24) | 20/157 (12.7) | 0/158 (0) | 0/253 (0) | 7/514 (1.4) |
Abbreviation: –, Data not reported.
Coypus.
Comprising 1 beaver, 9 corvids, 3 eagles, 17 goshawks, 1 jackal (positive for T. nativa), 1 marine mammal, 2 minks, 1 mustelid, 17 otters (one positive for T. pseudospiralis), 11 owls, 31 white‐tailed eagles (one positive) and 8 wolverines (four positives).
Comprising seven coypus and 204 land game mammals.
Rats.
Comprising 6 crows, 2 deer, 3 falcons, 1 ferret, 33 hedgehogs, 7 jackals, 1 jay, 74 magpies, 1 mouse, 1 otter, 6 polecats, 1 squirrel, 1 weasel and 27 wild cats (Felis silvestris).
Beavers.
Comprising 11 beavers, 1 lion and 8 seals.
Comprising one cat and two deer.
7.4. Discussion
Trichinellosis is a severe but rare human disease reported by nine7 EU MSs in 2022. Forty‐one human cases7 were documented, which was the lowest number of cases reported since the beginning of EU‐level surveillance in 2007. Seventeen of twenty‐six MSs reported zero cases, including three MSs (Cyprus, Luxembourg and Malta) that have never reported any trichinellosis cases to TESSy.
In general, Trichinella infections in humans are often linked to FBOs; therefore, the number and size of FBOs have affected the EU trend for trichinellosis. The EU notification rate was not higher than 0.03 per 100,000 population in the last 5 years, from 2018 to 2022, with the highest rate (0.03) reported in 2020. The lowest rate (0.01) was reported in 2018 and 2022. In 2022, Bulgaria and France accounted for more than half (58.5%) of all confirmed cases in the EU. In 2022, seven FBOs were reported, with 68 associated human cases, by five MSs (Croatia, France, Italy, Romania and Spain) to EFSA's FBO database. As in previous years, the small discrepancies between the FBO‐associated human cases (N = 68) reported to EFSA and the confirmed human cases of trichinellosis (N = 41) reported to TESSy resulted from different case classifications for reporting between the two databases (see Introduction).
Pigs represent the largest livestock category in the EU. More than 209 million pigs were tested for Trichinella in MSs and non‐MSs in 2022, out of more than 246 million pigs reared in the EU (European Commission et al., 2014; European Parliament, 2020), with only 71 positive animals, i.e. about 0.29 per million reared pigs. Only 5 of 27 MSs reported Trichinella in pigs in 2022, with an overall prevalence of 0.000034%. 45 Bulgaria, Croatia, Poland, Romania and Spain documented positive findings in pigs NCHC. Bulgaria and Spain reported one and two positive outdoor pigs, respectively, whereas Croatia, Poland and Romania reported 8, 1 and 59 positive indoor pigs, respectively.
In 2022, 6 out of 27 MSs reported data for pigs RCHC and eight reported data for pigs CHC, with no positive findings, confirming that controlled housing conditions are a key condition for preventing infection with this zoonosis. Most pigs at risk for this infection are backyard or free‐range pigs, usually slaughtered at home, where veterinary control or recording can easily be evaded. In the EU, infected pigs are typically clustered in five MSs (Bulgaria, Croatia, Poland, Romania and Spain) and sporadic infections can be documented in other MSs (Pozio, 2014). EFSA has identified that not raising domestic pigs under controlled housing conditions is a major risk factor for Trichinella infections in animals (EFSA and ECDC, 2011; EFSA BIOHAZ et al, 2011). Identification of Trichinella larvae at the species level in 2022 confirmed that T. spiralis was more prevalent in pigs than T. britovi (88.5% vs. 11.5%) (Pozio et al., 2009). However, T. spiralis was patchily distributed. T. pseudospiralis was identified in zero of 61 pigs for which the Trichinella species was available; these data confirmed the low prevalence of this species in target animals (Pozio, 2016).
Hunted wild boar meat has been a major source of trichinellosis infections in humans since 2015 according to the data reported to TESSy, whereas earlier, pig meat was the main source. Human behaviour can strongly influence sylvatic cycles, both favouring and reducing the transmission of Trichinella spp. For example, carcases of Trichinella‐infected animals left by hunters, or of such animals that have died in road accidents, may be scavenged by other wild animals, thereby contributing to transmission.
No positive findings were reported for solipeds in 2022. Over the last 13 years, only four horses tested positive, out of more than one million tested in 2008, 2010 and 2012 (EFSA and ECDC, 2009, 2010, 2011, 2012, 2013, 2014). This extremely low (< 0.001%) prevalence may have been related to effective control which, according to the EFSA BIOHAZ Panel (EFSA BIOHAZ Panel, 2013b), should be maintained if there is no reliable traceability system in place, especially since meat from solipeds can be eaten raw in some EU countries.
Trichinella spp. circulate among wild animals in large parts of Europe; however, the prevalence of Trichinella infection in these animals can vary among the sampling areas. The reporting of negative findings in MSs could be explained by insufficient surveys, inadequate sample sizes or investigations in regions whose environmental conditions do not favour the transmission of these zoonotic nematodes among wildlife. Some MSs (such as Italy, Switzerland, etc.) tested non‐susceptible wild animals (e.g. deer) for Trichinella infection. Apart from horses, some other herbivores, such as beavers, moose, etc., can be considered accidental hosts of Trichinella spp. (Kärssin et al., 2021). High endemicity for Trichinella in the sylvatic cycles of these countries and/or convenience sampling might justify surveillance in these animals. The large and widespread population of foxes (indicator animals) can be considered as the main natural reservoir of Trichinella in Europe. In 2022, the prevalence of Trichinella infection in this animal species was 0.95%, which was almost half that observed in 2021 (1.6%). In 2022, as in 2021, the proportion of positive samples from wildlife was higher in raccoon dogs (29.7%), wolves (14.1%) and lynxes (10.4%) than in other animals sampled but their population sizes and distributions in Europe are generally limited to a few countries.
In most MSs, there has been increased control at slaughter of pigs NCHC during the last few years. These measures, combined with trichinellosis awareness‐raising and farmers' education activities, may have contributed to a reduction in the parasite biomass in domestic habitats and the probability of acquiring an infection for humans.
Farming practices at risk of transmitting Trichinella spp. (rearing outdoor, backyard or free‐range pigs (Pozio et al., 2021) occur, in general, in disadvantaged and poor areas where veterinary services do not exist or are unable to control many small pig units, or where veterinary supervision can be circumvented (Pozio, 2014). There are examples from the past where countries had suitable controls in place for parasite management in domestic pigs but where changes in pork production affected by socioeconomic conflicts resulted in the re‐emergence of trichinellosis as a severe public health problem (Djordjevic et al., 2003; Cuperlovic et al., 2005). The increasing number of wild boar and foxes and the spread of the raccoon dog population from eastern to western Europe and of the jackal population from south‐eastern to north‐western Europe may increase the prevalence of Trichinella circulating among wild animals (Alban et al., 2011; Széll et al., 2013).
8. ECHINOCOCCUS
The summary data which make up this chapter, and additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases here.
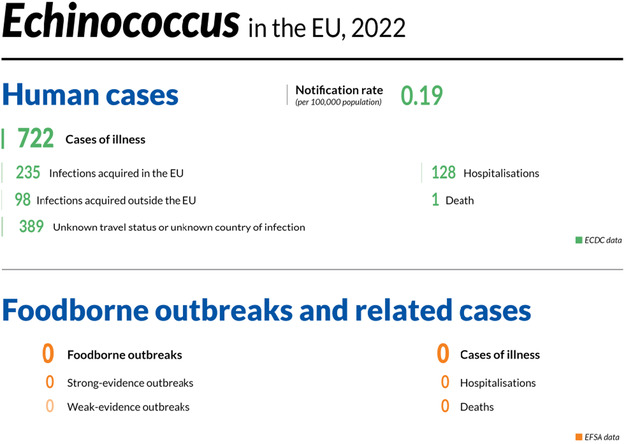
8.1. Key facts
In 2022, there were 722 confirmed cases of human echinococcosis, corresponding to an European Union notification rate of 0.19 per 100,000 population and an increase of 13.8% compared with 2021 (0.17 per 100,000 population).
The overall rate and number of reported echinococcosis cases reached similar levels to the 2018–2019 period, before the COVID‐19 pandemic.
In 2022, Echinococcus granulosus sensu lato, causing cystic echinococcosis, accounted for 62.4% of human cases reported with species information, while E. multilocularis causing alveolar echinococcosis accounted for 37.6% of cases.
In 2022, E. multilocularis was detected by eight Member States and one non‐MS in six different animal categories. Most units that tested positive in the European Union were from foxes (6710), and the proportion of positives was 12.5%. Czechia, Germany, Poland and Slovenia reported the largest proportions of infected foxes among those tested, accounting for 20.5%, 21.6%, 39.4% and 22.7% of positive findings, respectively.
In 2022, E. granulosus sensu lato was detected by 10 Member States and 2 non‐Member States in 13 different animal categories. Most of the units tested in the European Union were from sheep and goats (12,337,176), cattle (7,185,526) and pigs (58,254,973), and the proportion of positives was 0.81%, 0.32% and < 0.01%, respectively. Italy and Spain accounted for the majority of sheep and goats (50.7% and 41.9%), cattle (21.9% and 68.2%) and pigs (6.4% and 91.7%) that tested positive, respectively.
Data from Finland, Ireland, Malta, the United Kingdom (Northern Ireland) and mainland Norway confirmed the free status of these countries for E. multilocularis in 2022 in accordance with Commission Delegated Regulation (EU) 2018/772.
8.2. Surveillance and monitoring of cystic and alveolar echinococcosis in humans and animals in the EU
8.2.1. Humans
For 2022, 25 MSs reported information on echinococcosis infections in humans. Surveillance is mandatory in 22 MSs and voluntary in 3 MSs (Belgium, France and the Netherlands). Two MSs (Denmark and Italy) do not have a surveillance system for echinococcosis. The EU case definition was used by 23 countries; Germany reported using a different case definition, and France did not specify which case definition was used. All MSs except Belgium have comprehensive surveillance systems. The surveillance systems for echinococcosis cover the whole population in all MSs where surveillance systems are in place. All countries reported case‐based data except Bulgaria and the Netherlands, which reported aggregated data.
Alveolar echinococcosis (AE) caused by the tapeworm E. multilocularis and cystic echinococcosis (CE) caused by E. granulosus sensu lato (s.l.) are listed under the common disease name ‘echinococcosis’ in the EU case definition, thus making no distinction between these two diseases. AE and CE can be reported by species and, as of 2019 (2018 data), by clinical presentation of the disease in the ECDC TESSy database.
8.2.2. Animals
Surveillance of E. multilocularis in Europe is usually carried out voluntarily, except in the reporting countries claiming to be free of this parasite per Commission Delegated Regulation (EU) 2018/772 supplementing Regulation (EU) 576/2013. 46 Surveillance is mainly carried out in red foxes, Europe's main definitive host. In 2020, Finland, Ireland, mainland Norway (Svalbard archipelago excluded) and the United Kingdom (Northern Ireland) demonstrated the absence of E. multilocularis through the implementation of an annual surveillance programme in compliance with Regulation (EU) 2018/772 (EFSA, Rusinà, & Zancanaro, 2023 ). In accordance with this regulation, Malta is not required to implement a surveillance programme due to the absence of the definitive host (red fox) on its territory. In all other MSs, data on E. multilocularis depend on whether findings are notifiable, monitoring is in place or studies on E. multilocularis are performed. Data on E. multilocularis in animals vary geographically across and within countries, and over time, depending on the sampling effort and it is therefore challenging to compare reported cases of E. multilocularis within and between countries. According to a meta‐analysis based on studies published between 1900 and 2015, E. multilocularis has been documented in red foxes from 21 countries (Oksanen et al., 2016). Since 2018, this parasite has also been found in golden jackals from Croatia, Hungary, Serbia and Slovenia (Sindičić et al., 2018; Dušek et al., 2020; Balog et al., 2021). Human AE cases have also been detected recently in Croatia and Serbia (Dušek et al., 2020; Lalošević et al., 2023). In accordance with CIR (EU) 2020/2002, disease‐free status EU MSs must notify outbreaks of infection with E. multilocularis in Canidae to the EU ADIS. 47
Surveillance of E. granulosus s.l. is carried out in livestock intermediate hosts during slaughterhouse inspections. In particular, necropsy on sheep liver and lungs is used to detect the presence of parasitic cysts. In contrast, methods based on molecular PCR methods are used to confirm and identify genotype/species belonging to the Echinococcus genus (Siles‐Lucas et al., 2017). Although Regulation (EU) 2018/772 is in force for E. multilocularis, no specific EU regulation is in place for detecting E. granulosus s.l. in animals or humans. Surveillance of the latter parasite, therefore, depends on national regulations. Approximate geographical distribution of E. granulosus s.l. species causing human CE and country‐based incidences in Europe were reported recently (Casulli et al., 2022; Casulli et al., 2023).
8.3. Results
8.3.1. Overview of key statistics, EU, 2018–2022
Table 47 summarises EU‐level statistics aggregated by year for echinococcosis (AE and CE) in humans and E. granulosus s.l. and E. multilocularis in their most relevant definitive and intermediate animal hosts in 2018–2022. More detailed descriptions of these statistics are provided in the subsections below.
TABLE 47.
Summary of echinococcosis statistics caused by Echinococcus multilocularis or Echinococcus granulosus s.l. relating to humans, and the most relevant definitive and intermediate animal hosts, EU, 2018–2022.
| 2022 a | 2021 a | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 722 | 589 | 547 | 779 | 815 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0.19 | 0.17 | 0.16 | 0.17 | 0.18 | ECDC |
| Number of reporting MSs | 25 | 25 | 25 | 26 | 26 | ECDC |
| Infection acquired in the EU | 235 | 127 | 63 | 176 | 149 | ECDC |
| Infection acquired outside the EU | 98 | 83 | 77 | 96 | 83 | ECDC |
| Unknown travel status or unknown country of infection | 389 | 379 | 407 | 507 | 583 | ECDC |
| Animals | ||||||
| Echinococcus multilocularis in foxes | ||||||
| Number of animals tested | 6710 | 6318 | 5506 | 6326 | 6566 | EFSA |
| % positive animals | 12.5 | 17.0 | 16.1 | 13.7 | 18.4 | EFSA |
| Number of reporting MSs | 14 | 14 | 10 | 13 | 13 | EFSA |
| Echinococcus spp. in dogs | ||||||
| Number of animals tested | 2502 | 2942 | 2515 | 2113 | 2605 | EFSA |
| % positive animals | 0.08 | 0.07 | 0.08 | 0.24 | 0.08 | EFSA |
| Number of reporting MSs | 7 | 5 | 5 | 6 | 6 | EFSA |
| Echinococcus granulosus s.l. in cattle (bovine animals) | ||||||
| Number of animals tested | 7,185,526 | 7,065,934 | 7,035,066 | 10,956,688 | 9,920,327 | EFSA |
| % positive animals | 0.32 | 0.21 | 0.21 | 0.17 | 0.23 | EFSA |
| Number of reporting MSs | 16 | 16 | 15 | 16 | 17 | EFSA |
| Echinococcus granulosus s.l. in sheep and goats | ||||||
| Number of animals tested | 12,337,176 | 10,806,419 | 11,089,043 | 36,890,847 | 38,870,491 | EFSA |
| % positive animals | 0.81 | 0.38 | 0.96 | 0.38 | 0.37 | EFSA |
| Number of reporting MSs | 13 | 14 | 12 | 15 | 15 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
For the 2021–2022 period, data on animal samples from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were taken into account for 2018–2019 since the United Kingdom was still an EU MS. However, on 1 February 2020, it became a third country.
8.3.2. Human echinococcosis
In 2022, 722 confirmed echinococcosis cases were recorded by 25 reporting MSs, corresponding to an EU notification rate of 0.19 cases per 100,000 population (Table 48) and an increase of 13.8% compared with 2021 (0.17 per 100,000 population). A mean notification rate of 0.17 per 100,000 population was reported over 2018–2021. In 2022, 23 MSs reported at least one confirmed case, two MSs reported zero cases (Cyprus and Malta) and two MSs did not report any data (Denmark and Italy). In 2022, the highest notification rates were observed in Lithuania and Bulgaria, with 2.6 and 1.3 cases per 100,000 population, respectively, followed by Austria with 0.60 cases per 100,000 population.
TABLE 48.
Reported confirmed human cases of cystic and alveolar echinococcosis and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 54 | 0.60 | 42 | 0.47 | 34 | 0.38 | 36 | 0.41 | 46 | 0.52 |
| Belgium | Y | C | 23 | 0.20 | 17 | 0.15 | 19 | 0.16 | 22 | 0.19 | 15 | 0.13 |
| Bulgaria | Y | A | 89 | 1.3 | 89 | 1.3 | 95 | 1.4 | 193 | 2.8 | 206 | 2.9 |
| Croatia | Y | C | 5 | 0.13 | 3 | 0.07 | 3 | 0.07 | 3 | 0.07 | 4 | 0.10 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 1 | 0.11 | 0 | 0 | 0 | 0 |
| Czechia | Y | C | 10 | 0.10 | 1 | 0.01 | 4 | 0.04 | 1 | 0.01 | 4 | 0.04 |
| Denmark b | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | Y | C | 1 | 0.08 | 4 | 0.30 | 1 | 0.08 | 2 | 0.15 | 0 | 0 |
| Finland c | Y | C | 2 | 0.04 | 6 | 0.11 | 4 | 0.07 | 8 | 0.14 | 1 | 0.02 |
| France | Y | C | 79 | 0.12 | 75 | 0.11 | 55 | 0.08 | 55 | 0.08 | 62 | 0.09 |
| Germany | Y | C | 163 | 0.20 | 160 | 0.19 | 171 | 0.21 | 150 | 0.18 | 176 | 0.21 |
| Greece | Y | C | 5 | 0.05 | 4 | 0.04 | 7 | 0.07 | 7 | 0.07 | 11 | 0.10 |
| Hungary | Y | C | 9 | 0.09 | 7 | 0.07 | 4 | 0.04 | 10 | 0.10 | 9 | 0.09 |
| Ireland c | Y | C | 1 | 0.02 | 1 | 0.02 | 0 | 0 | 0 | 0 | 2 | 0.04 |
| Italy b | – | – | – | – | – | – | – | – | – | – | – | – |
| Latvia | Y | C | 4 | 0.21 | 6 | 0.32 | 5 | 0.26 | 6 | 0.31 | 10 | 0.52 |
| Lithuania | Y | C | 74 | 2.6 | 20 | 0.72 | 37 | 1.3 | 81 | 2.9 | 50 | 1.8 |
| Luxembourg | Y | C | 1 | 0.15 | 1 | 0.16 | 3 | 0.48 | 1 | 0.16 | 0 | 0 |
| Malta c | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | Y | A | 45 | 0.26 | 53 | 0.30 | 48 | 0.28 | 48 | 0.28 | 42 | 0.24 |
| Poland | Y | C | 46 | 0.12 | 26 | 0.07 | 18 | 0.05 | 70 | 0.18 | 51 | 0.13 |
| Portugal | Y | C | 2 | 0.02 | 2 | 0.02 | 1 | 0.01 | 5 | 0.05 | 9 | 0.09 |
| Romania | Y | C | 4 | 0.02 | 1 | 0.01 | 0 | 0 | 1 | 0.01 | 4 | 0.02 |
| Slovakia | Y | C | 6 | 0.11 | 2 | 0.04 | 3 | 0.05 | 11 | 0.20 | 10 | 0.18 |
| Slovenia | Y | C | 5 | 0.24 | 11 | 0.52 | 3 | 0.14 | 6 | 0.29 | 6 | 0.29 |
| Spain d | Y | C | 72 | 0.15 | 33 | – | 8 | – | 34 | 0.07 | 68 | 0.15 |
| Sweden | Y | C | 22 | 0.21 | 25 | 0.24 | 23 | 0.22 | 26 | 0.25 | 29 | 0.29 |
| EU‐27 total | 722 | 0.19 | 589 | 0.17 | 547 | 0.16 | 776 | 0.20 | 815 | 0.21 | ||
| United Kingdom c , e | Y | C | – | – | – | – | – | – | 3 | 0 | 0 | 0 |
| EU total | 722 | 0.19 | 589 | 0.17 | 547 | 0.16 | 779 | 0.17 | 815 | 0.18 | ||
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway c | Y | C | 9 | 0.17 | 11 | 0.20 | 6 | 0.11 | 7 | 0.13 | 7 | 0.13 |
| Liechtenstein b | – | – | – | – | – | – | – | – | – | – | – | – |
| Switzerland b | – | – | – | – | ||||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
No surveillance system.
Finland, Ireland, Malta, the United Kingdom and mainland Norway have been declared free of Echinococcus multilocularis.
Data incomplete for 2020 and 2021, rate not calculated.
Cases reported by the United Kingdom for 2018–2019 were also considered for this estimation (EU‐28). Data for the United Kingdom were collected for 2018–2019 since it was still an EU MS. However, on 1 February 2020, it became a third country.
In 2022, fewer than half of the echinococcosis cases (46.1%; 333/722) were reported with data on importation and probable country of infection; 70.6% (235/333) of cases reported with such information were domestic or related to travel within the EU, while 29.4% (98/333) were associated with travel outside the EU. Compared with the previous period, in 2022, there was an increase in the data on imported cases and probable country of infection, from 30.1% (644/2141 in 2018–2020) to 35.6% (210/589 in 2021) to 46.1% (333/722 in 2022).
In 2022, considering travel associated echinococcosis cases (N = 122), the highest proportions were reported by Germany (100%; 65 vs. 0 non‐travel‐related cases), Sweden (100%; 20 vs. 0 cases), Finland (100%; 2 vs. 0 cases), Belgium (48%; 11 vs. 12 cases) and Czechia (40%; 4 vs. 6 cases). Of the 116 travel‐associated cases for which the probable country of origin of infection was reported, most (84.5%) were reported as originating from outside the EU, mainly from Syria (22.4%), followed by Türkiye (13.3%), Iraq (10.2%), Afghanistan (9.2%) and Ukraine (6.1%). Within the EU, Romania (50%), Bulgaria (38.9%), Croatia (5.6%) and Lithuania (5.6%) were reported as the probable countries of infection in 18 cases.
In 2022, species information was provided for 476 confirmed echinococcosis cases (65.9%) out of 722 confirmed cases reported by 19 MSs (Table 49). In 2022, human infections caused by E. multilocularis accounted for 179 cases (37.6% of cases with known species information), more than in 2018–2021 (31.22%, 31.93%, 26.77%, 27.43%, respectively). France, Germany, Lithuania and Poland reported the highest numbers of human cases caused by E. multilocularis, accounting for 30.2%, 22.9%, 15.6% and 11.7% of all reported AE cases, respectively. Human infections caused by E. granulosus s.l., accounted for 297 cases (62.4%) out of the cases with species information available. Germany, Bulgaria, France and Austria reported the highest numbers of human cases caused by E. granulosus s.l., accounting for 32.3%, 30.0%, 8.4% and 8.1% of all reported CE cases, respectively. In 2022, 15 MSs provided information on hospitalisation, accounting for 16.9% (128/722) of all confirmed cases of echinococcosis in the EU. The overall hospitalisation rate was 46.2%. In 2022, information on case outcomes was provided by 15 MSs for 56.1% of confirmed cases, with one death by E. multilocularis (case fatality rate of 0.2%).
TABLE 49.
Reported human cases of cystic and alveolar echinococcosis in EU MSs and non‐MS countries by country, year and Echinococcus species, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total cases | Eg | Em | Total cases | Eg | Em | Total cases | Eg | Em | Total cases | Eg | Em | Total cases | Eg | Em | |
| Austria | 54 | 24 | 8 | 42 | 24 | 7 | 34 | 18 | 4 | 36 | 16 | 13 | 46 | 29 | 12 |
| Belgium | 23 | 11 | 12 | 17 | 11 | 6 | 19 | 10 | 8 | 22 | 12 | 10 | 15 | 10 | 5 |
| Bulgaria | 89 | 89 | 0 | 89 | 89 | 0 | 95 | 95 | 0 | 193 | 193 | 0 | 206 | 206 | 0 |
| Croatia | 5 | – | 3 | 3 | – | – | 3 | – | – | 3 | – | – | 4 | – | – |
| Cyprus | 0 | 0 | 0 | 0 | 0 | 0 | 1 | – | – | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | 10 | 3 | 4 | 1 | 0 | 1 | 4 | 1 | 2 | 1 | – | – | 4 | 1 | 2 |
| Denmark a | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | 1 | 0 | 1 | 4 | – | – | 1 | 1 | – | 2 | – | – | 0 | 0 | 0 |
| Finland b | 2 | 2 | 0 | 6 | 5 | – | 4 | 3 | – | 8 | 8 | 0 | 1 | 1 | 0 |
| France | 79 | 25 | 54 | 75 | 22 | 53 | 55 | 13 | 42 | 55 | 20 | 35 | 62 | 21 | 41 |
| Germany | 163 | 96 | 41 | 160 | 95 | 42 | 171 | 81 | 54 | 150 | 87 | 41 | 176 | 93 | 59 |
| Greece | 5 | – | – | 4 | – | – | 7 | 7 | 0 | 7 | – | – | 11 | – | – |
| Hungary | 9 | 7 | 1 | 7 | – | – | 4 | 1 | – | 10 | – | – | 9 | – | – |
| Ireland b | 1 | – | – | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | – | – |
| Italy a | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Latvia | 4 | – | – | 6 | 6 | 0 | 5 | 5 | 0 | 6 | 4 | – | 10 | 5 | 1 |
| Lithuania | 74 | 5 | 28 | 20 | 2 | 14 | 37 | – | – | 81 | 30 | 21 | 50 | 11 | 17 |
| Luxembourg | 1 | 1 | 0 | 1 | 0 | – | 3 | 3 | 0 | 1 | 1 | 0 | 0 | 0 | 0 |
| Malta b | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | 45 | – | – | 53 | – | – | 48 | – | – | 48 | – | – | 42 | – | – |
| Poland | 46 | 9 | 21 | 26 | 12 | 11 | 18 | 8 | 6 | 70 | 21 | 25 | 51 | 17 | 19 |
| Portugal | 2 | 1 | – | 2 | 2 | 0 | 1 | 1 | 0 | 5 | 5 | 0 | 9 | 9 | 0 |
| Romania | 4 | – | – | 1 | – | – | 0 | 0 | 0 | 1 | – | – | 4 | – | – |
| Slovakia | 6 | 1 | 4 | 2 | 0 | 2 | 3 | 1 | 2 | 11 | 3 | 8 | 10 | 3 | 3 |
| Slovenia | 5 | 1 | – | 11 | 2 | 2 | 3 | 1 | – | 6 | 1 | – | 6 | 3 | – |
| Spain | 72 | 11 | – | 33 | 1 | – | 8 | 1 | – | 34 | 6 | – | 68 | 12 | – |
| Sweden | 22 | 11 | 2 | 25 | 12 | – | 23 | 8 | 3 | 26 | 17 | 2 | 29 | 5 | 2 |
| EU‐27 total | 722 | 297 | 179 | 589 | 284 | 138 | 547 | 258 | 121 | 776 | 424 | 155 | 815 | 426 | 161 |
| United Kingdom b , c | – | – | – | – | – | – | – | – | – | 3 | 3 | 0 | 0 | 0 | 0 |
| EU total | 722 | 297 | 179 | 589 | 284 | 138 | 547 | 258 | 121 | 779 | 427 | 155 | 815 | 426 | 161 |
| Iceland | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway b | 9 | – | 1 | 11 | 5 | – | 6 | 1 | 1 | 7 | 2 | – | 7 | 5 | 0 |
| Liechtenstein a | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Switzerland a | – | – | – | – | – | – | |||||||||
Abbreviations: Eg, Echinococcus granulosus sensu lato; Em, Echinococcus multilocularis, –, Data not reported.
No surveillance system.
Finland, Ireland, Malta, the United Kingdom and mainland Norway have been declared free of E. multilocularis.
Cases reported by the United Kingdom for 2018–2019 were also considered for this estimation (EU‐28). Data for the United Kingdom were collected for 2018–2019 since it was still an EU MS. However, on 1 February 2020, it became a third country.
8.3.3. Echinococcus spp. in animals and food
Monitoring data for Echinococcus multilocularis
In 2022, 13 MSs, the United Kingdom (Northern Ireland) and two non‐MSs (Norway and Switzerland) reported monitoring data from 6710 and 507 foxes examined for E. multilocularis, respectively (Table 50). Eight MSs (Czechia, France, Germany, Luxembourg, Poland, Slovakia, Slovenia and Sweden) and one non‐MS (Switzerland) reported 11.6% positive samples. Czechia, Germany, Poland and Slovenia reported the largest numbers of infected foxes in Europe, accounting for 20.5%, 21.6%, 39.4% and 22.7% of positive findings, respectively.
TABLE 50.
Echinococcus multilocularis monitoring results in wild and domestic animals in reporting EU MSs and non‐MSs, 2022.
| Country | Presence of Em/ Eg a | N positive/N tested (% positive) | ||||||
|---|---|---|---|---|---|---|---|---|
| Cats | Dogs | Foxes | Pigs | Raccoon dogs | Raccoons | |||
| Czechia | Em/Eg | – | – | 529/2575 (20.5) | – | – | – | |
| Denmark | Em | – | – | 0/21 (0) | 0/17,854,036 (0) | – | – | |
| Estonia | Em/Eg | – | – | – | 0/529,347 (0) | – | – | |
| Finland b | Eg | – | – | 0/166 (0) | – | 0/260 (0) | – | |
| France | Em/Eg | – | 1/1 (100.0) | 7/113 (6.2) | – | – | – | |
| Germany | Em | – | 0/12 (0) | 141/653 (21.6) | 0/2 (0) | – | 0/16 (0) | |
| Hungary | Em/Eg | – | – | – | 0/3 (0) | – | – | |
| Ireland b | Eg | – | – | 0/400 (0) | – | – | – | |
| Italy | Em/Eg | – | 0/13 (0) | 0/181 (0) | 0/5,188,368 (0) | – | – | |
| Latvia | Em/Eg | – | – | – | 0/502,601 (0) | – | – | |
| Luxembourg | Em | – | – | 10/72 (13.9) | 0/146,037 (0) | – | – | |
| Netherlands | Em | – | – | 0/7 (0) | – | 0/2 (0) | – | |
| Poland | Em/Eg | – | 1/90 (1.1) | 134/340 (39.4) | 2/200 (1.0) | – | – | |
| Romania | Em/Eg | – | 0/3 (0) | – | 0/54 (0) | – | – | |
| Slovakia | Em/Eg | 0/815 (0) | 0/2381 (0) | 3/91 (3.3) | 39/585,890 (0.01) c | – | – | |
| Slovenia | Em/Eg | – | – | 5/22 (22.7) | 1/1 (100.0) c | – | – | |
| Sweden | Em/Eg | – | 0/2 (0) | 8/922 (0.87) | 0/2672,400 (0) | – | – | |
| United Kingdom (Northern Ireland) b , d | Eg | – | – | 0/1147 (0) | – | – | – | |
| EU total (27 + XI) | 0/815 (0) | 2/2502 (0.08) | 837/6710 (12.5) | 42/27,478,939 (< 0.01) | 0/262 (0) | 0/16 (0) | ||
| Norway b , e | Eg | – | – | 0/503 (0) | – | – | – | |
| Switzerland | Em | 1/5 (20) | 15/39 (38.5) | 3/4 (75.0) | 4/7 (57.1) | – | – | |
| Total non‐EU countries | 1/5 (20) | 15/39 (38.5) | 3/507 (0.59) | 4/7 (57.1) | – | – | ||
| Total EU (27+ XI) + non‐EU countries | 1/820 (0.12) | 17/2541 (0.67) | 840/7217 (11.6) | 46/27,478,946 (< 0.01) | 0/262 (0) | 0/16 (0) | ||
| Country | Presence of Em/Eg a | N positive/N tested (% positive) | ||||||
| Wild boars | Wild cats (Felis silvestris) | Wolves | Domestic solipeds | Coypu | Squirrel | Voles | ||
| Czechia | Em/Eg | – | – | – | – | – | – | – |
| Denmark | Em | – | – | – | – | – | – | – |
| Estonia | Em/Eg | – | – | – | – | – | – | – |
| Finland b | Eg | – | – | – | – | – | – | 0/946 (0) |
| France | Em/Eg | – | – | – | – | 0/1 (0) | – | – |
| Germany | Em | 3/4 (75.0) | 0/1 (0) | – | – | – | 1/1 (100) | – |
| Hungary | Em/Eg | – | – | – | – | – | – | – |
| Ireland b | Eg | – | – | – | – | – | – | – |
| Italy | Em/Eg | 0/35,645 (0) | – | 0/67 (0) | – | – | – | – |
| Latvia | Em/Eg | – | – | – | – | – | – | – |
| Luxembourg | Em | – | – | – | – | – | – | – |
| Netherlands | Em | – | – | 0/5 (0) | – | – | – | – |
| Poland | Em/Eg | – | – | – | – | – | – | – |
| Romania | Em/Eg | – | – | – | – | – | – | – |
| Slovakia | Em/Eg | – | – | – | – | – | – | – |
| Slovenia | Em/Eg | – | – | – | – | – | – | – |
| Sweden | Em/Eg | 0/13,208 (0) | – | 0/47 (0) | – | – | – | – |
| United Kingdom (Northern Ireland) b , d | Eg | – | – | – | – | – | – | – |
| EU total (27 + XI) | 3/48,857 (0.01) | 0/1 (0) | 0/119 (0) | – | 0/1 (0) | 1/1 (100) | 0/946 (0) | |
| Norway b , e | Eg | – | – | – | – | – | – | – |
| Switzerland | Em | 5/5 (100.0) | – | 1/5 (20.0) | 0/2 (0) | – | – | – |
| Total non‐EU countries | 5/5 (100.0) | – | 1/5 (20.0) | 0/2 (0) | – | – | – | |
| Total EU (27+ XI) + non‐EU countries | 8/48,862 (0.02) | 0/1 (0) | 1/124 (0.81) | 0/2 (0) | 0/1 (0) | 1/1 (100) | 0/946 (0) | |
Abbreviations: –, Data not reported; Em, Echinococcus multilocularis; Eg: Echinococcus granulosus sensu lato.
Presence in the country of Echinococcus multilocularis (Em) and/or Echinococcus granulosus sensu lato (Eg).
Member States listed in the Annex to Commission Implementing Regulation (EU) 2018/878 on applying preventive health measures to control E. multilocularis infection in dogs.
Positive samples from pigs without Echinococcus species information reported were mentioned in the table only for countries with known circulation of both E. multilocularis and E. granulosus sensu lato.
Data on animals from the United Kingdom (Northern Ireland) are considered for 2022. Following the agreement on the withdrawal of the United Kingdom from the EU, particularly with the Northern Ireland protocol, the EU requirements on data sampling are also applicable to Northern Ireland.
Mainland Norway (Svalbard archipelago excluded where E. multilocularis was documented).
In addition to its presence in foxes, Echinococcus spp. has been reported in 1 cat (Switzerland), 17 dogs (France, Poland and Switzerland), 8 wild boars (Germany and Switzerland) and 1 wolf (Switzerland). Moreover, 42 positive pigs were reported by three MSs (Poland, Slovakia and Slovenia) co‐endemic for both Echinococcus species, and four pigs from one non‐MS (Switzerland), endemic only for E. multilocularis. Pigs are good hosts for E. granulosus s.l. while E. multilocularis metacestodes in pigs are abortive, and their presence is often used as a sentinel for the circulation of this parasite in animal hosts. For this reason, the presence of both E. multilocularis and E. granulosus s.l. may be overestimated in co‐endemic countries with unknown species identification. Therefore, positive samples from pigs, dogs and wolves without species identification are only mentioned in Tables 50, 51 for countries with known circulation of both E. granulosus s.l. and E. multilocularis. E. multilocularis was also detected in two sample batches of fresh leaf vegetables and blueberries in France.
TABLE 51.
Echinococcus granulosus sensu lato monitoring results in wild and domestic animals in reporting EU MSs and non‐MSs, 2022.
| Country | Presence of Em/Eg a | N positive/N tested (% positive) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Alpine chamois | Cats | Cattle (bovine animals) | Deer | Dogs | Moose | Mouflons | Mountain goats | Pigs | ||
| Belgium b | Em | – | – | 0/758,282 (0) | – | – | – | – | – | – |
| Bulgaria | Eg | – | – | 1280/36,177 (3.5) | – | – | – | – | – | 0/1200,664 (0) |
| Cyprus | Eg | – | – | – | – | – | – | 1/21 (4.8) | – | – |
| Denmark b | Em | – | – | 0/493,300 (0) | – | – | – | – | – | – |
| Estonia | Em/Eg | – | – | 0/32,702 (0) | – | – | – | – | – | 0/529,347 (0) |
| Finland | Eg | – | – | 0/256,483 (0) | 0/2901 (0) | – | 2/164 (1.2) | – | – | 0/1,871,043 (0) |
| France | Em/Eg | – | – | – | – | 0/0 (0) | – | – | – | – |
| Germany | Em | – | – | 0/10 (0) | – | – | – | – | – | – |
| Greece | Eg | – | – | 991/35,504 (2.8) | – | – | – | – | – | 0/161,960 (0) |
| Hungary | Em/Eg | – | – | – | – | – | – | – | – | 0/3 (0) |
| Italy | Em/Eg | – | – | 5101/2079,861 (0.25) | 0/3 (0) | 0/13 (0) | – | – | – | 133/5,188,501 (< 0.01) |
| Latvia | Em/Eg | – | – | 0/65,826 (0) | – | – | – | – | – | 0/502,601 (0) |
| Luxembourg b | Em | – | – | 0/26,483 (0) | – | – | – | – | – | – |
| Malta | Eg | – | – | – | – | – | – | – | – | – |
| Poland | Em/Eg | – | – | – | – | 0/90 (0) | – | – | – | 0/200 (0) |
| Portugal | Eg | – | – | 6/425,297 (< 0.01) | – | – | – | – | – | 0/5,500,634 (0) |
| Romania | Em/Eg | – | – | 15/16 (93.8) | – | 0/3 (0) | – | – | – | 0/54 (0) |
| Slovakia | Em/Eg | – | 0/815 (0) | 1/32,083 (< 0.01) | – | 0/2381 (0) | – | – | – | 39/585,890 (0.01) c |
| Slovenia | Em/Eg | – | – | 0/8 (0) | – | – | – | – | – | 1/1 (100.0) c |
| Spain | Eg | – | – | 15,891/2,531,404 (0.63) | 1/229,715 (< 0.01) | – | – | 0/8185 (0) | 0/1 (0) | 1910/40,041,675 (< 0.01) |
| Sweden | Em/Eg | – | – | 0/412,090 (0) | 0/7602 (0) | 0/2 (0) | – | – | – | 0/2672,400 (0) |
| EU total (27 + XI) | – | 0/815 (0) | 23,285/7,185,526 (0.32) | 1/240,221 (< 0.01) | 0/2489 (0) | 2/164 (1.2) | 1/8206 (0.01) | 0/1 (0) | 2083/58,254,973 (< 0.01) | |
| Norway | Eg | – | – | 0/300,000 (0) | – | – | 1/1 (100.0) | – | – | 0/1,600,000 (0) |
| Republic of North Macedonia | Eg | – | – | 9/11 (81.8) | – | – | – | – | – | – |
| Switzerland b | Em | 0/1 (0) | – | – | 0/2 (0) | – | – | – | – | – |
|
Total non‐EU countries |
0/1 (0) | – | 9/300,011 (< 0.01) | 0/2 (0) | – | 1/1 (100.0) | – | – | 0/1,600,000 (0) | |
| Total EU (27+ XI) + non‐EU countries | 0/1 (0) | 0/815 (0) | 23,294/7,485,537 (0.31) | 1/240,223 (< 0.01) | 0/2489 (0) | 3/165 (1.8) | 1/8206 (0.01) | 0/1 (0) | 2083/59,854,973 (< 0.01) | |
| Country | Presence of Em/Eg a | N positive/N tested (% positive) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Reindeers | Goats | Sheep | Sheep and goats | Solipeds, domestic | Water buffalos | Wild boars | Wolves | ||
| Belgium b | Em | – | – | – | – | – | – | – | – |
| Bulgaria | Eg | – | – | – | 4271/157,113 (2.7) | – | – | – | – |
| Cyprus | Eg | – | – | – | – | – | – | – | – |
| Denmark b | Em | – | – | – | – | – | – | – | – |
| Estonia | Em/Eg | – | 0/169 (0) | 0/8292 (0) | – | 0/5 (0) | – | – | – |
| Finland | Eg | 10/53,176 (0.02) | 0/908 (0) | 0/56,147 (0) | – | 0/838 (0) | – | 0/174 (0) | 3/53 (5.7) |
| France | Em/Eg | – | – | – | – | – | – | – | – |
| Germany | Em | – | 0/2 (0) | 0/1 (0) | – | – | – | – | – |
| Greece | Eg | 0/12 (0) | 176/185,537 (0.09) | 2312/490,404 (0.47) | – | – | – | – | – |
| Hungary | Em/Eg | – | – | – | – | – | – | – | – |
| Italy | Em/Eg | – | 935/58,059 (1.6) | 49,724/1,337,011 (3.7) | – | 0/6229 (0) | 112/35,240 (0.32) | 8/35,653 (0.02) | 0/67 (0) |
| Latvia | Em/Eg | – | 0/630 (0) | 0/26,344 (0) | – | 0/32 (0) | – | – | – |
| Luxembourg b | Em | – | – | – | – | – | – | – | – |
| Malta | Eg | – | – | 0/6464 (0) | – | – | – | – | – |
| Poland | Em/Eg | – | – | – | – | – | – | – | – |
| Portugal | Eg | – | 0/110,486 (0) | 2/700,197 (< 0.01) | – | – | – | – | – |
| Romania | Em/Eg | – | 0/1 (0) | 0/18 (0) | – | – | – | – | – |
| Slovakia | Em/Eg | – | 0/104 (0) | 698/42,205 (1.7) | – | – | – | – | – |
| Slovenia | Em/Eg | – | – | – | – | – | – | – | – |
| Spain | Eg | – | 4466/1305,809 (0.34) | 37,401/7,623,340 (0.49) | – | 4/6985 (0.06) | – | 8/181,056 (< 0.01) | – |
| Sweden | Em/Eg | 0/40,528 (0) | 0/1025 (0) | 0/226,910 (0) | – | 0/1110 (0) | – | 0/13,208 (0) | 0/47 (0) c |
| EU total (27 + XI) | 10/93,716 (0.01) | 5577/1,662,730 (0.34) | 90,137/10,517,333 (0.86) | 4271/157,113 (2.7) | 4/15,199 (0.03) | 112/35,240 (0.32) | 16/230,091 (0.01) | 3/167 (1.8) | |
| Norway | Eg | – | 0/25,000 (0) | 0/1100,000 (0) | – | – | – | – | – |
| Republic of North Macedonia | Eg | – | – | – | 11/11 (100.0) | – | – | – | – |
| Switzerland b | Em | – | – | 0/3 (0) | – | – | – | – | – |
| Total non‐EU countries | – | 0/25,000 (0) | 0/1100,003 (0) | 11/11 (100.0) | – | – | – | – | |
| Total EU (27+ XI) + non‐EU countries | 10/93,716 (0.01) | 5577/1,687,730 (0.33) | 90,137/11,617,336 (0.78) | 4282/157,124 (2.7) | 4/15,199 (0.03) | 112/35,240 (0.32) | 16/230,091 (0.01) | 3/167 (1.8) | |
Abbreviations: –, Data not reported; EU, European Union; Em, Echinococcus multilocularis; Eg, Echinococcus granulosus sensu lato.
Presence in the country of E. multilocularis (Em) and/or E. granulosus sensu lato (Eg).
Reporting countries with a known circulation of E. multilocularis only, which tested suitable hosts for E. granulosus sensu lato.
Positive samples from wolves and pigs without Echinococcus species information reported were mentioned in the table only for MSs with known circulation of both E. multilocularis and E. granulosus sensu lato.
Monitoring data for Echinococcus granulosus sensu lato
Table 51 summarises the most relevant definitive and intermediate host species tested for E. granulosus s.l. In 2022, 20 MSs, the United Kingdom (Northern Ireland) and 3 non‐MSs (Norway, Republic of North Macedonia and Switzerland) reported monitoring data for E. granulosus s.l. The data reported were from approximately 81 million domestic and wild animals tested for E. granulosus s.l., of which more than 99% were domestic animals (sheep, cattle, goats, pigs, horses, water buffalos, dogs and cats). Most of these data were obtained from domestic livestock during meat inspections at the slaughterhouse. Wild animals tested included Alpine chamois, deer, moose, mouflons, mountain goats, reindeer, wild boars and wolves. A total of 125,502 (0.16%) positive samples were reported by 10 MSs, mainly from domestic animals. These positive samples came primarily from small ruminants (sheep and goats; N = 99,985), accounting for 79.7% of positive results. Positive tests in small ruminants were mainly reported by Italy and Spain, accounting for 50.7% and 41.9% of positive animals, respectively, followed by Bulgaria, Greece and Slovakia. A total of 23,285 cattle tested positive (18.6% of animals positive for E. granulosus s.l.), mainly reported by Spain (68.2%) and Italy (21.9%), followed by Bulgaria and Greece. A total of 2083 pigs tested positive (1.7% of animals positive for E. granulosus s.l.), of which Spain reported 91.7%.
Figures 19 and 20 show the cumulative proportions of positive samples from different intermediate hosts of E. granulosus s.l. and their geographical distribution in EU MSs and other European countries from 2018 to 2022. Small ruminants (sheep and goats) accounted for 77.1% of all positive samples and were reported by a few countries (Italy, Spain, the United Kingdom (Northern Ireland), Greece and Bulgaria) with large animal populations. Greece, Italy and Spain also reported positive results in cattle (13.5%). Positive results in pigs (9.3%) were mainly reported by Poland, followed by Spain. Positive pigs included both E. granulosus s.l. and Echinococcus unspecified. For this reason, positive pigs could potentially be overestimated in co‐endemic countries with E. multilocularis.
FIGURE 19.
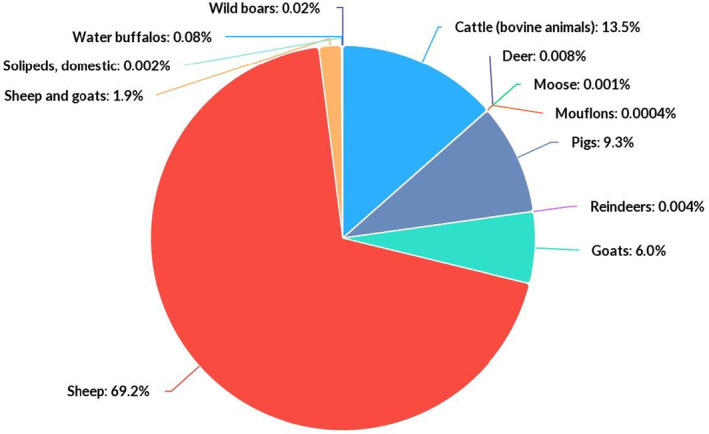
Cumulative proportion (%) of test‐positive animals for Echinococcus granulosus sensu lato, by intermediate host species, in EU MSs and non‐MSs, 2018–2022.
FIGURE 20.
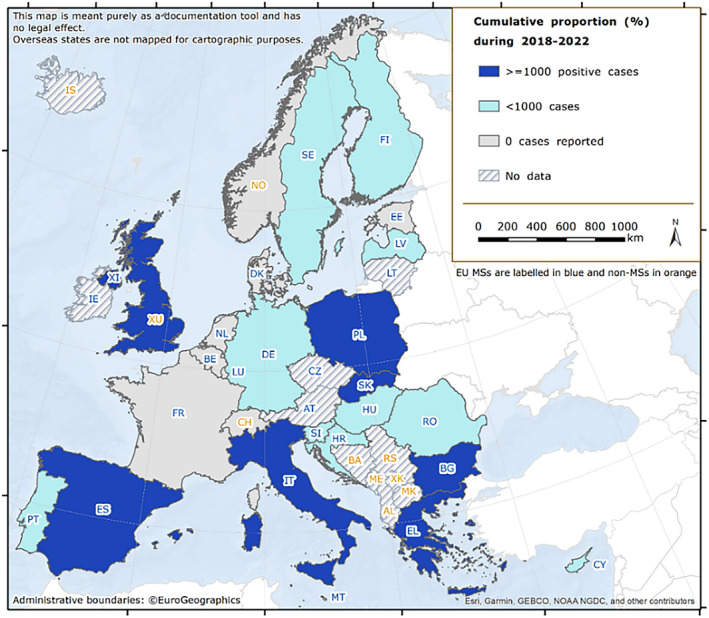
Map of the cumulative proportion (%) of test‐positive animals for Echinococcus granulosus sensu lato in MSs and non‐MSs, by country, 2018–2022. Note: Dark blue ≥ 1000 positive cases; light blue < 1000 cases; grey = 0 cases reported; diagonally shaded = unreported data. Because of the co‐endemicity with Echinococcus multilocularis, positive pigs were excluded from Poland, Romania, Slovakia and Slovenia when Echinococcus species information was not reported. Spain (N = 289,004), Italy (N = 236,474), the United Kingdom (N = 46,937), Greece (N = 45,798), Bulgaria (N = 17,765), Poland (N = 2479) and Slovakia (N = 1654), were the countries with the highest endemicity for E. granulosus s.l. in the EU in 2018–2022.
8.4. Discussion
In 2022, the EU notification rate of confirmed human echinococcosis cases evidenced a progressive resurgence of cases following the COVID‐19 pandemic.
In a few countries, the rise in case numbers over the last 5 years may be explained by increased human surveillance activities and improved notification systems for these diseases. Increased awareness about the diseases among clinicians, as well as immigration from endemic countries, may also have influenced the numbers of CE and AE diagnosed cases in some countries (Richter et al., 2019)the recent discovery of AE in other countries such as Croatia and Serbia points to a geographical spread of the parasite (Balen Topić et al., 2023; Lalošević et al., 2023). It should be emphasised that the true prevalence of these diseases is extremely difficult to estimate due to the long incubation period, high proportion of asymptomatic or paucisymptomatic carriers who never seek medical attention, non‐specific symptoms and under‐reported or misdiagnosed CE and AE cases. The factors mentioned above contribute to the neglected status of these diseases (Casulli, 2020). For these reasons, the patchy data reported by MSs on the number of people with echinococcosis currently represent the ‘tip of the iceberg’ for infections, with asymptomatic carriers and misdiagnosed cases of CE and AE making up the invisible portion. For instance, it has been estimated that the official figures from hospital records should be far higher, with true values 10 and 700 times greater for Bulgaria and Romania in 2015–2016, respectively (Tamarozzi et al., 2018). The prospective, observational, multicentre and online ‘European Register of Cystic Echinococcosis’ (ERCE) (Rossi et al., 2020) seeks to establish a voluntary system to collect harmonised clinical data in the EU. The European (Alveolar) Echinococcosis Registry (Kern et al., 2003) led a similar initiative. More recently, a multicentred retrospective study to lower uncertainty limits on the impact of human CE identified around 65,000 human cases in Europe in 1997–2021 (Casulli et al., 2023). Using different data sources, this study also identified a total number of CE cases fourfold greater than ECDC data in 2017–2019 (Casulli et al., 2023).
In 2022, 24 MSs, the United Kingdom (Northern Ireland), 3 non‐MS (Norway, Republic of North Macedonia and Switzerland) reported monitoring data on E. granulosus s.l. and E. multilocularis in animals. The highest numbers of animals infected with E. granulosus s.l. were reported in Italy and Spain, followed by Bulgaria and Greece. Infections were mainly observed in sheep intermediate hosts and, to a lesser extent, in cattle and goats. Most of the animals (primarily red foxes) infected with E. multilocularis were reported by Czechia, followed by Germany and Poland. The surveillance of E. multilocularis in foxes is important to assess the prevalence of AE in Europe, given that its geographical distribution seems to have widened in recent decades. It is difficult to establish whether the increased geographical distribution of E. multilocularis is due to a growing fox population in Europe (Deplazes et al., 2004; Oksanen et al., 2016) or whether it reflects greater surveillance efforts, as there is a general lack of baseline data and standardised detection methods. One growing source of concern is the detection in recent years of E. multilocularis in golden jackals, which are increasing their geographical range from southern‐eastern to northern‐western Europe, and therefore contributing to the dispersion of this parasite over long distances (Dušek et al., 2020; Balog et al., 2021). In that context, E. multilocularis was detected for the first time in Serbia (in golden jackals and foxes) and in Bosnia and Herzegovina (in foxes) (Miljević et al., 2021; Marinković et al., 2022) (Omeragić et al., 2022).
Moreover, in animals, notification is necessary to obtain reliable data, and information on parasite speciation is essential for risk management efforts since E. granulosus s.l. and E. multilocularis have different epidemiologies and pose different health risks for humans (Possenti et al., 2016; Conraths et al., 2017). For E. granulosus s.l., a notification requirement would ensure that comparable data between MSs are obtained from meat inspections of food‐producing animals. For E. multilocularis, while the need for general notification by all MSs may raise questions, it is nevertheless required in countries free from this parasite, per Regulation (EU) 2018/772.
In general terms, it should be emphasised that animal findings from most endemic countries fluctuated from year to year in 2018–2022. However, positive results in animals and humans were reported in most years. The fluctuations over the last 5 years probably reflect the investigational efforts performed during a particular year rather than a change in the true prevalence of the disease. For instance, Italy reported 49,724 (3.7%) test‐positive sheep in 2022, 1292 (0.12%) in 2021 (EFSA and ECDC, 2022) and 60,608 (6.5%) in 2020 (EFSA and ECDC, 2021b). Moreover, these fluctuations in animal findings can be partially explained by the United Kingdom leaving the EU: in 2019, the United Kingdom accounted for 68.8% and 37.2% of all sheep and goats, and cattle tested in the EU, respectively.
FOODBORNE OUTBREAKS (ACCORDING TO DIRECTIVE 2003/99/EC)
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on foodborne outbreaks reported in the framework of Directive 2003/99/EC are retrievable using the EFSA dashboard on foodborne outbreaks available here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
1 KEY FACTS
In 2022, 27 European Union Member States and the United Kingdom (Northern Ireland) reported 5763 foodborne outbreaks, 48605 cases of illness, 2783 hospitalisations and 64 deaths. A total of 108 foodborne outbreaks, 2166 cases of illness, 186 hospitalisations and one death were reported by seven non‐Member States.
Foodborne outbreaks in the European Union increased by 43.9% in 2022 compared with the previous year (4005 in 2021). Human cases and hospitalisations also increased by 49.4% (32,543 cases in 2021) and 11.5% (2495 hospitalisations in 2021), respectively. The number of deaths increased substantially by 106.5% compared with 2021 (31 deaths in 2021).
In 2022, the foodborne outbreak reporting rate in the European Union was 1.3 per 100,000 population. This represented an increase of 32.8% compared with the mean annual rate for the period 2018–2021 (0.97 outbreaks per 100.000 population). Similarly, the case reporting rate rose to 10.8 cases per 100,000 in 2022, an increase of 35.3% compared with the mean annual rate for the period 2018–2021 (8.0 cases per 100,000).
The number of deaths observed in foodborne outbreaks in 2022 was one of the highest value ever reported to EFSA in the European Union in the last 10 years. Most deaths were caused by Listeria monocytogenes (N = 28; 43.8% of total deaths), confirming the severe health impact associated with L. monocytogenes, especially in vulnerable population groups such as the elderly. The highest case fatality ratio was observed for Streptococcus equi subsp. zooepidemicus, an emerging agent that in 2022 caused a single foodborne outbreak due to consumption of cheese made from unpasteurised milk, leading to 37 cases, of which five deaths.
Salmonella was identified in most foodborne outbreaks in the European Union (N = 1014), making up 17.6% of total outbreaks. This pathogen was also associated with the highest number of hospitalisations (50.5% hospitalisations) and ranked second for the number of cases (13.6% of cases) and deaths (12.5% of deaths). S. Enteritidis was the predominant serovar (N = 395; 77.0% of all Salmonella outbreaks with serovar information available). Salmonella was also responsible for several multi‐country outbreaks in 2022, including a major outbreak caused by monophasic S. Typhimurium, associated with the consumption of chocolate products. Five outbreaks (84 cases and 29 hospitalisations) were caused by S. Typhi.
Norovirus (and other calicivirus) was the agent associated with the highest number of human cases, with an 11.6% increase (N = 7305; 15.0% of outbreak‐associated cases) compared with 2021. This causative agent caused 12 large outbreaks involving more than 100 cases in several Member States and was associated with a large mean outbreak size (22.0 cases).
A total of 487 strong‐evidence outbreaks were reported in 2022 (8.5% of all outbreaks). Among these, foodstuffs belonging to the group ‘composite foods, multi‐ingredient foods and other foods’ were implicated in most outbreaks (29.4%) with an increase of 34.9% over 2021 (106 strong‐evidence outbreaks in 2021), causing most cases (32.4% of all strong‐evidence outbreak‐related cases).
In 2022, for the first time since the start of foodborne outbreaks data collection in the European Union, most strong‐evidence outbreaks and cases identified took place in the setting ‘restaurants, pubs, street vendors, takeaway etc.’ (147 outbreaks; 30.2% of all strong‐evidence outbreaks). In particular, ‘restaurant or cafe or pub or bar or hotel or catering service' were the most frequently reported places of exposure (134 strong‐evidence outbreaks; 27.5%), a rise of 74.0% compared to 2021 (77 strong‐evidence outbreaks).
The number of strong‐evidence outbreaks occurring on domestic premises also increased (145 outbreaks; 19.8% of all strong‐evidence outbreaks) in 2022 in the European Union, albeit to a lesser extent compared with 2021 (121 outbreaks; 34.0% of all strong‐evidence outbreaks).
‘School or kindergarten’ were also places of exposure associated with a high number of cases (1544 cases; 15.7% of all cases in strong‐evidence outbreaks). These findings highlighted the importance of proper implementation of Hazard Analysis and Critical Control Points (HACCP) in public catering as well as the need to improve the awareness of both consumers and food business operators on correct procedures for handling and consuming food.
2 SURVEILLANCE AND MONITORING OF FOODBORNE OUTBREAKS IN THE EU
Every year, EU Member States (MSs) and non‐MSs report to EFSA concerning the foodborne outbreaks (FBOs) occurring in their country, in compliance with Directive 2003/99/EC. The reporting of data is based on the standard set out in the guidance document, published annually by EFSA (EFSA, Amore, Boelaert, et al., 2023; EFSA, Amore, Beloeil, et al., 2023).
EFSA is assigned the task of describing the causative agents and foodstuffs implicated in FBOs, along with their time trends. The aim is to assess the health impact of FBOs in Europe and to characterise the food vehicles most frequently implicated. Outbreaks are categorised as ‘strong‐evidence' or ‘weak‐evidence' based on the strength of evidence implicating a suspected food vehicle as the cause of the outbreak (EFSA, 2014). Data on the place of exposure and contributing factors are also analysed. The analysis takes account of uncertainty around the evidence implicating a given food as the vehicle of the outbreak, by limiting the description of certain findings (i.e. implicated food vehicles, place of exposure and contributory factors) to strong‐evidence outbreaks.
The current data reporting system is known as the European Union Foodborne Reporting System (EU‐FORS). It applies to outbreaks caused by bacteria, viruses, parasites, algae, fungi and their products, such as toxins and biological amines (e.g. histamine), either typical foodborne agents or agents for which foodborne transmission is usually accidental. Outbreaks caused by the ingestion of drinking water are also considered in FBO reporting, since drinking water is defined as a food in Regulation (EC) No 178/2002. 48
FBO data reporting is mandatory for EU MSs and the key findings are summarised in this report.
A description of the national systems in place for outbreak surveillance and reporting can be found in the national zoonoses reports submitted in accordance with Directive 2003/99/EC and published on the EFSA website together with the EU One Health Zoonoses Report, both available online here.
More details on the surveillance and monitoring of foodborne outbreaks in the EU are available on the EFSA story map (here) (see story map sections on ‘what foodborne outbreaks are and how they are classified’, ‘who investigates foodborne outbreaks’ and ‘EU regulatory framework and the role of EFSA’).
3 DATA ANALYSES
Basic indicators used to describe the impact of FBOs on human health include the total number of outbreaks and cases, the number and proportion of cases (%) leading to hospitalisations or deaths, the mean outbreak size (cases per outbreak) and the range of cases per outbreak (minimum and maximum). Outbreak and case reporting rates (per 100,000 population) are used as relative measures of occurrence in the population, allowing a direct comparison among MSs, independently of the size of the population and any variations over time. However, due to the lack of full harmonisation of FBO surveillance among MSs, any direct comparison of findings between countries should be interpreted with caution. Counts of hospitalisations and deaths and the proportion (%) of hospitalisations and deaths among outbreak cases are used as indicators for outbreak severity. However, since the total number of hospitalisations and deaths can be reported as ‘unknown’ by MSs, these values might be underestimated and should be analysed with caution.
The causative agents in FBOs in 2022 have been grouped in accordance with the following criteria:
-
–
‘E. coli other than STEC’ includes any pathogenic E. coli other than ‘Shiga Toxin‐producing E. coli (STEC)’. In 2022, this group included ‘Enteroaggregative E. coli (EAEC)’, ‘Enteroinvasive E. coli’ (EIEC)’, ‘Enteropathogenic Escherichia coli (EPEC)’, ‘Enterotoxigenic E. coli (ETEC)’ and ‘E. coli, unspecified’.
-
–
‘Bacillus cereus toxins’ includes ‘B. cereus’ and ‘B. cereus enterotoxins’.
-
–
‘Staphylococcus aureus toxins’ includes ‘S. aureus', ‘Staphylococcus unspecified’ and ‘staphylococcal enterotoxins'.
-
–
‘Clostridium perfringens toxins’ includes ‘Clostridium, unspecified’ and ‘C. perfringens’.
-
–
‘Norovirus (and other caliciviruses)’ includes ‘calicivirus, unspecified’, ‘norovirus’ and ‘sapovirus’.
Food vehicles have been grouped according to the general criteria set out in the EFSA data catalogues (EFSA, 2023). Places of exposure have been grouped according to the general characteristics and level of risk associated with the setting, as well as the process behind food preparation.
Key statistics at EU level included the United Kingdom for 2019 and previous years since it was a MS. In 2022, in accordance with the Protocol on Ireland/Northern Ireland, FBOs reported by the United Kingdom (Northern Ireland) were included in EU statistics.
Eurostat data on the resident population (on 1 January 2023) were used to calculate reporting rates at national and EU level. Data from the NISRA 49 from 2021 were used for the United Kingdom (Northern Ireland).
Short‐term variations over time were described using the same metrics (annual mean) by comparison with 2021 and 2018–2021. Long‐term variations were also described, taking 2013–2022 as the reference time period. Frequency distributions and trends are shown at EU level. Trends were analysed only at MS level, according to the rationale described in Boelaert et al. (2016) for data quality (Table 1). Time trends were tested for statistical significance over the period 2013–2022 using the Cox‐Stuart sign test, a nonparametric test appropriate for limited numbers of observations. A p‐value of < 0.05 was considered to identify a statistically significant trend, beyond chance. The detection of significant trends at national level should be interpreted with caution, following changes in the reporting specifications for FBOs, introduced in 2014 (EFSA, 2014). MSs with incomplete datasets for the 2013–2022 period were excluded from the analysis.
Key statistics on FBOs for 2021 and previous years may differ from those published in the European Union One Health 2021 Zoonoses Report, as MSs may have updated their data from previous years.
During the last phase of the production of this report, Hungary informed us that the one strong‐evidence outbreak (one case, one hospitalisation and one death) caused by L. monocytogenes, with ‘pig meat and products thereof’ as the implicated food vehicle and ‘others’ as the place of exposure, was reported in error. Footnotes to inform readers of the error have been added to the relevant tables and figures in this report. This error does not affect the FBOs dashboard.
4. RESULTS AND DISCUSSION
4.1 Overview of countries reporting foodborne outbreak data, 2022
During 2022, a total of 5763 foodborne outbreaks (FBOs), 48,605 human cases, 2783 hospitalisations and 64 deaths were reported by 27 MSs and the United Kingdom (Northern Ireland). Among these countries, only Bulgaria reported no foodborne outbreaks detected in 2022. In addition, seven non‐MSs (Bosnia and Herzegovina, Iceland, Montenegro, Norway, Republic of North Macedonia, Serbia and Switzerland) provided information on 108 foodborne outbreaks causing 2166 cases, 186 hospitalisations and 1 death (Table 52).
TABLE 52.
Number of foodborne outbreaks, human cases, hospitalisations and deaths, in reporting EU MSs and non‐MS countries, 2022.
| Country | Outbreaks | Cases | Hospitalised | Deaths | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (strong‐evidence) | % of total | Outbreaks per 100,000 | N | % of total | Mean outbreak size (N) and range (min‐max) | Cases per 100,000 | N | % of total | N | % of total | |||
| N | 2022 a | 2018–2021 a , b | 2022 a | 2018–2021 a , b | |||||||||
| Austria | 28 (8) | 0.49 | 0.31 | 0.40 | 128 | 0.26 | 4.6 (2–30) | 1.4 | 3.3 | 57 | 2.0 | 4 | 6.3 |
| Belgium | 830 (12) | 14.4 | 7.1 | 4.0 | 4222 | 8.7 | 5.1 (2–600) | 36.3 | 17.4 | 124 | 4.5 | 2 | 3.1 |
| Bulgaria | 0 (−) | – | 0 | 0.14 | – | – | – | 0 | 1.8 | – | – | – | – |
| Croatia | 26 (8) | 0.45 | 0.67 | 0.56 | 950 | 2.0 | 36.5 (2–360) | 24.6 | 6.7 | 27 | 0.97 | 0 | 0 |
| Cyprus | 1 (−) | 0.02 | 0.11 | 0.14 | 20 | 0.04 | 20.0 (−) | 2.2 | 2.0 | 3 | 0.11 | 0 | 0 |
| Czechia | 48 (10) | 0.83 | 0.46 | 0.26 | 1582 | 3.3 | 33.0 (2–130) | 15.0 | 10.9 | 31 | 1.1 | 0 | 0 |
| Denmark | 63 (19) | 1.1 | 1.1 | 0.92 | 1286 | 2.6 | 20.4 (2–125) | 21.9 | 27.0 | 51 | 1.8 | 0 | 0 |
| Estonia | 6 (1) | 0.10 | 0.45 | 0.94 | 21 | 0.04 | 3.5 (2–6) | 1.6 | 4.7 | 9 | 0.32 | 0 | 0 |
| Finland | 54 (14) | 0.94 | 0.97 | 0.96 | 620 | 1.3 | 11.5 (2–97) | 11.2 | 22.1 | 51 | 1.8 | 9 | 14.1 |
| France | 1861 (66) | 32.3 | 2.7 | 2.1 | 16,102 | 33.1 | 8.7 (2–383) | 23.7 | 17.9 | 657 | 23.6 | 13 | 20.3 |
| Germany | 211 (17) | 3.7 | 0.25 | 0.36 | 1488 | 3.1 | 7.1 (1–50) | 1.8 | 2.0 | 268 | 9.6 | 8 | 12.5 |
| Greece | 34 (3) | 0.59 | 0.33 | 0.05 | 383 | 0.79 | 11.3 (2–145) | 3.7 | 2.6 | 68 | 2.4 | 3 | 4.7 |
| Hungary c | 15 (3) | 0.26 | 0.15 | 0.27 | 301 | 0.62 | 20.1 (1–93) | 3.1 | 11.6 | 20 | 0.72 | 1 | 1.6 |
| Ireland d | 24 (1) | 0.42 | 0.47 | 0.38 | 113 | 0.23 | 5.4 (2–21) | 2.2 | 1.9 | 10 | 0.36 | 0 | 0 |
| Italy | 175 (32) | 3.0 | 0.30 | 0.18 | 1604 | 3.3 | 9.2 (1–177) | 2.7 | 1.7 | 303 | 10.9 | 15 | 23.4 |
| Latvia | 5 (−) | 0.09 | 0.27 | 1.2 | 155 | 0.32 | 31.0 (22–33.3) | 8.3 | 20.8 | 8 | 0.29 | 0 | 0 |
| Lithuania | 9 (9) | 0.16 | 0.32 | 0.92 | 19 | 0.04 | 2.1 (2–3) | 0.68 | 5.6 | 13 | 0.47 | 0 | 0 |
| Luxembourg | 2 (1) | 0.03 | 0.31 | 0.08 | 63 | 0.13 | 31.5 (2–61) | 9.8 | 0.20 | 1 | 0.04 | 0 | 0 |
| Malta | 29 (−) | 0.50 | 5.6 | 7.2 | 94 | 0.19 | 3.2 (2–5) | 18.0 | 31.8 | 19 | 0.68 | 0 | 0 |
| Netherlands | 1162 (7) | 20.2 | 6.6 | 4.2 | 4463 | 9.2 | 3.8 (2–72) | 25.4 | 16.3 | 59 | 2.1 | 1 | 1.6 |
| Poland | 336 (43) | 5.8 | 0.89 | 0.93 | 3670 | 7.6 | 10.9 (2–122) | 9.7 | 10.5 | 457 | 16.4 | 4 | 6.3 |
| Portugal | 11 (6) | 0.19 | 0.11 | 0.11 | 1634 | 3.4 | 148.5 (16–950) | 15.8 | 4.2 | 27 | 0.97 | 0 | 0 |
| Romania | 9 (6) | 0.16 | 0.05 | 0.05 | 170 | 0.35 | 18.9 (3–60) | 0.89 | 1.4 | 77 | 2.8 | 0 | 0 |
| Slovakia | 137 (9) | 2.4 | 2.5 | 9.1 | 506 | 1.0 | 3.7 (2–24) | 9.3 | 31.2 | 125 | 4.5 | 0 | 0 |
| Slovenia | 5 (2) | 0.09 | 0.24 | 0.02 | 285 | 0.59 | 57.0 (4–138) | 13.5 | 1.2 | 39 | 1.4 | 0 | 0 |
| Spain | 591 (183) | 10.3 | 1.2 | 0.80 | 7136 | 14.7 | 12.1 (2–266) | 15.0 | 8.7 | 233 | 8.4 | 4 | 6.3 |
| Sweden | 89 (26) | 1.5 | 0.85 | 0.58 | 1571 | 3.2 | 17.7 (2–113) | 15.0 | 10.9 | 41 | 1.5 | 0 | 0 |
| United Kingdom (Northern Ireland) | 2 (1) | 0.03 | 0.11 | 0.11 | 19 | 0.04 | 9.5 (1–18) | 1.0 | 0.89 | 5 | 0.18 | 0 | 0 |
| EU Total (27 + XI) c , d | 5763 (487) | 100 | 1.3 | 0.97 | 48,605 | 100 | 8.4 (1–950) | 10.8 | 8.0 | 2783 | 100 | 64 | 100 |
| Bosnia and Herzegovina | 2 (1) | – | 0.06 | 0.06 | 25 | – | 12.5 (6–19) | 0.77 | 1.5 | 4 | – | 0 | – |
| Iceland | 2 (1) | – | 0.53 | 1.0 | 93 | – | 46.5 (46–47) | 24.7 | 17.0 | 0 | – | 0 | – |
| Montenegro | 5 (−) | – | 0.81 | 0.76 | 135 | – | 27.0 (3–98) | 21.9 | 13.8 | 87 | – | 0 | – |
| Norway | 37 (16) | – | 0.68 | 0.65 | 632 | – | 17.1 (1–100) | 11.6 | 21.4 | 23 | – | 0 | – |
| Republic of North Macedonia | 3 (2) | – | 0.16 | 0.20 | 91 | – | 30.3 (7–64) | 5.0 | 6.0 | 2 | – | 0 | – |
| Serbia | 19 (10) | – | 0.28 | 0.40 | 405 | – | 21.3 (3–65) | 6.0 | 4.2 | 26 | – | 0 | – |
| Switzerland e | 40 (9) | – | 0.46 | 0.25 | 785 | – | 20.7 (2–256) | 9.0 | 3.5 | 44 | – | 1 | – |
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
During the last phase of the production of this draft report, Hungary informed us that the one strong‐evidence outbreak (one case, one hospitalisation and one death) was reported in error.
For three outbreaks, information on cases was not available. These outbreaks were excluded from the calculation of the mean outbreak size.
For two outbreaks, information on cases was not available. These outbreaks were excluded from the calculation of the mean outbreak size.
Overall, the total number of outbreaks reported by each MS varied considerably among countries, with a small number of MSs (Belgium, France, the Netherlands and Spain) together accounting for 77.1% (4444 FBOs) of the total number of outbreaks reported in the EU. The same MSs reported almost two‐thirds of the total number of cases in the EU in 2022 (31,923 cases; 65.7% of the total).
As shown in Table 52, the frequency of the reporting of FBOs and cases in 2022 varied considerably among MSs. The outbreak reporting rate ranged from 0.05 (Romania) to 7.1 (Belgium) outbreaks per 100,000 population, and the case reporting rate from 0.68 (Lithuania) to 36.3 (Belgium) cases per 100,000. Considerable variations were also observed among MSs in the mean number of cases per outbreak, described in Table 52 with the ‘mean outbreak size'.
Variations in both the ‘outbreak reporting rate' and ‘case reporting rate' as well as in the ‘mean outbreak size' are influenced by the approach of each MS to outbreak surveillance and its sensitivity. For example, the type of FBOs investigated or reported to EFSA may or may not include household outbreaks (i.e. outbreaks where all the human cases live in a single household), which are usually more frequent than general outbreaks and small in size. Information on the type of outbreak was reported for 3543 FBOs, meaning that for 2220 outbreaks reported by MSs (over a third of FBOs) the type of outbreak was ‘unknown’. In 2022, 17 MSs and two non‐MSs (Serbia, Switzerland) provided information on ‘household’ outbreaks. In Greece, Ireland, Lithuania and Poland, this type of FBO was the predominant type of outbreak reported to EFSA. No ‘household’ outbreaks were reported by Cyprus, Czechia, Denmark, Finland, Hungary, Latvia, Luxembourg, Portugal, Slovenia and the United Kingdom (Northern Ireland). All MSs except Bulgaria and Lithuania notified ‘general’ outbreaks to EFSA (N = 2461 FBOs; 42.7% of the total number of FBOs in the EU). In 2022, ‘general’ outbreaks were more than four times bigger (14.5 cases on average in the EU) than ‘household’ outbreaks (3.4 cases on average in the EU). In general, the MSs with the ‘highest mean outbreak size' and ‘case reporting rate' are those that reported mainly or only ‘general’ outbreaks to EFSA.
Thirteen MSs (Austria, Belgium, Denmark, Estonia, Finland, France, Germany, Ireland, Italy, Luxembourg, the Netherlands, Spain and Sweden) and the United Kingdom (Northern Ireland) reported a total of 808 cases causing 125 hospitalisations as part of multi‐country outbreaks in 2022. Among non‐MSs, Norway and Switzerland reported 60 cases as part of multi‐country outbreaks. Multi‐country outbreaks were caused by Salmonella, Shigella and Cryptosporidium. Being able to link outbreak cases occurring in multiple MSs to the same cross‐border outbreak depends on the capacity of each MS to either investigate the food exposure history of the cases in detail, to trace‐back and trace‐forward distribution chains of contaminated food, or to perform highly discriminatory comparative analyses based on a pheno‐genotypic characterisation of the causative agents in order to assess the level of relatedness among the agents isolated from human cases and/or food. Moreover, rapid exchange information systems such as the Early Warning Response System (EWRS), the EpiPulse and the Rapid Alert System for Food and Feed (RASFF) allow real‐time dissemination of the alert among European countries, which greatly supports the investigation of multi‐country outbreaks. In 2022, these systems were used intensively to support the investigation of multi‐country outbreaks, in particular the outbreak of monophasic S. Typhimurium in chocolate products, which was the largest cross‐border FBO identified in 2022 in Europe (see Section 4.8).
More information on the FBOs and related time trends over the 2018–2022 period can be viewed dynamically on the dashboard (here).
In 2022, the number of FBOs reported by MSs and the United Kingdom (Northern Ireland) increased by 43.9% over the previous year (1758 more FBOs in 2022 than in 2021), as shown in Figure 21. A similar rise was observed in the number of cases and hospitalisations, with 16,062 cases and 288 hospitalisations more than in 2021 (a relative increase of 49.4% and 11.5%, respectively). A comparison between the FBO and case reporting rate in 2022 and the mean annual values observed over the 2018–2021 period, shows that these rates increased by 32.8% and 35.3%, respectively.
FIGURE 21.
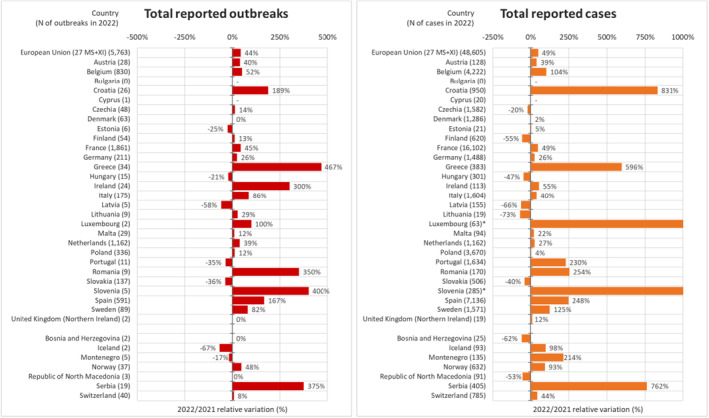
Relative variations (%) in foodborne outbreaks and outbreak‐related cases reported in 2022 compared with 2021, by reporting countries. Note: *2022/2021 relative variation for Luxembourg was 2000% and for Slovenia 9400%. During the last phase of the production of this report, Hungary informed EFSA that one strong‐evidence outbreak (involving one case) was reported in error.
The health impact of FBOs in 2022 was remarkably high, since 64 deaths were reported at EU level, i.e. more than double the number of 2021 (33 more deaths in 2022; a relative increase of 106.5% compared with 2021). Four MSs (Finland, France, Germany and Italy) accounted for 70.3% of all reported deaths. The number of deaths observed in 2022 was the highest ever reported by the EU to EFSA since it first began collecting FBO data in 2004, with the exception of 2011 (84 deaths, mostly due to the single large outbreak of Shiga toxin‐producing E. coli (STEC) O104) (Frank et al., 2011).
In 2022, 487 strong‐evidence FBOs were identified in the EU by 23 MSs (all MSs except Bulgaria, Cyprus, Latvia and Malta) and the United Kingdom (Northern Ireland). This reporting accounted for 8.5% of all FBOs in the EU, a proportion similar to 2021 (8.9%). Altogether, four MSs (France, Italy, Poland and Spain) reported two thirds of all strong‐evidence FBOs in the EU (324 strong‐evidence FBOs; 66.5% of all strong‐evidence FBOs).
Figure 21 shows the relative variations in the number of FBOs and outbreak‐related cases reported in 2022, compared with 2021, at EU and country level. In EU, an increase in the number of FBOs was observed for all countries, except Denmark, Estonia, Hungary, Latvia, Portugal, Slovakia and the United Kingdom (Northern Ireland). A similar pattern, characterised by a higher number of outbreak‐related cases in 2022 than in 2021, can be seen in all countries except Czechia, Finland, Hungary, Latvia, Lithuania and Slovakia. This increase may be explained by the gradual lifting or easing of measures to control COVID‐19 in the third year of the pandemic. Other reasons, including a general improvement in FBO surveillance and its components, were reported by a few MSs and also contributed to this increase.
The distribution of strong‐evidence and weak‐evidence FBOs for the period 2013–2022 and the outbreak reporting rate per 100,000 population is reported in Figure 22. For many MSs and non‐MSs, a resurgence in the number of FBOs to pre‐pandemic levels and a return to the overall trends of occurrence of FBOs over the longer term (2013–2022) could also be clearly seen in 2022.
FIGURE 22.
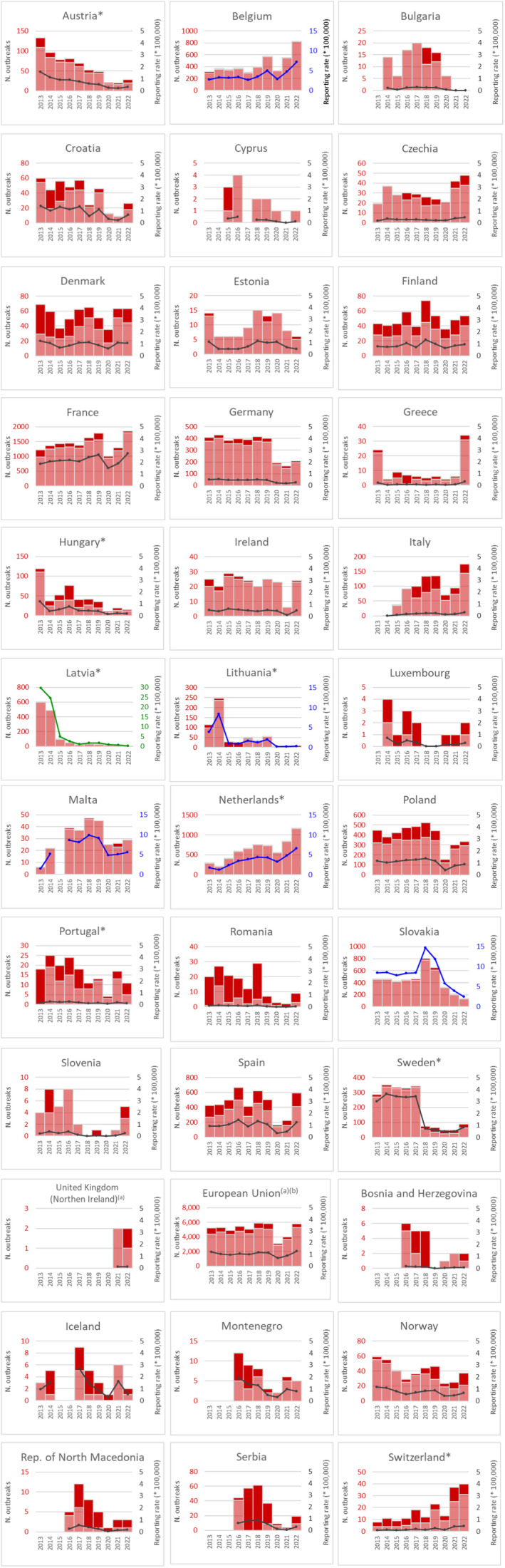
Trends in the number of strong‐evidence and weak‐evidence outbreaks (left axis) and outbreak reporting rate (per 100,000) (right axis) in the EU and reporting EU MS and non‐MS countries, 2013–2022. Note: *Indicates countries with a statistically significant trend (p < 0.05) over the period. During the last phase of the production of this draft report, Hungary informed EFSA that the one strong‐evidence outbreak was reported in error. Dark red and light red show strong‐ and weak‐evidence outbreaks, respectively. Black dots and lines show FBO reporting rates. The dots, lines and secondary Y‐axis in blue or green showing the outbreak reporting rates have been used for Belgium, Latvia, Lithuania, Malta, the Netherlands and Slovakia, in order to draw attention to the reporting rate scale that is different to that of the other countries. aFor the 2021–2022 period, data from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland. bFor the 2013–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Among MSs, a statistically significant decrease in the number of FBOs over the last 10 years was observed for six MSs (Austria, Hungary, Latvia, Lithuania, Portugal and Sweden), while an increasing trend was observed for the Netherlands and Switzerland (Figure 22).
4.2 Overview of causative agents in foodborne outbreaks in 2022
In 2022, a causative agent was identified in 3104 FBOs, accounting for 53.9% of all FBOs reported in the EU. These FBOs resulted in 32,456 human cases, 2475 hospitalisations and 57 deaths. For a high proportion of FBOs, the causative agent was unknown (2659 FBOs; 46.1% of total FBOs).
The agents involved in most outbreaks were bacteria (N = 1444; 25.1% of the total), which also caused the highest number of hospitalisations (N = 1847; 66.4% of the total) and deaths (N = 43; 67.2% of the total). Bacterial toxins were the second group of agents most frequently implicated in FBOs but ranked first as a group for the number of human cases involved (N = 13,902; 28.6% of total human cases). More information is available in Table 53 and can be interactively viewed on the dashboard (here, see page on ‘causative agent’).
TABLE 53.
Number of foodborne outbreaks, human cases, hospitalisations and deaths, by causative agent, in reporting EU MSs, 2022.
| Type of agent | Outbreaks | Cases of illness | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (strong‐evidence) | % of total | Reporting rate per 100,000 | Human cases | Mean outbreak size (cases) and range (min‐max) | Hospitalisations | Deaths | ||||||
| N | 2022 b | 2018‐2021 b , c | N | % of total | N | % of cases d | N | % of cases d | ||||
| Bacteria | Aeromonas | 2 (1) | 0.03 | < 0.01 | < 0.01 | 8 | 0.02 | 4.0 (3–5) | 1 | 12.5 | 0 | 0 |
| Campylobacter | 255 (16) | 4.4 | 0.06 | 0.08 | 1097 | 2.3 | 4.3 (2–32) | 83 | 7.6 | 0 | 0 | |
| Enterococcus | 1 (0) | 0.02 | < 0.01 | < 0.01 | 6 | 0.01 | 6.0 (−) | 1 | 16.7 | 0 | 0 | |
| Escherichia coli other than STEC | 15 (5) | 0.26 | < 0.01 | < 0.01 | 513 | 1.1 | 34.2 (2–123) | 4 | 0.78 | 1 | 0.19 | |
| Listeria monocytogenes e | 35 (17) | 0.61 | 0.01 | < 0.01 | 296 | 0.61 | 8.5 (1–97) | 242 | 81.8 | 28 | 9.5 | |
| Salmonella f | 1014 (200) | 17.6 | 0.23 | 0.22 | 6632 | 13.6 | 6.5 (1–138) | 1406 | 21.2 | 8 | 0.12 | |
| Shiga toxin‐producing E. coli (STEC) g | 71 (1) | 1.2 | 0.02 | 0.01 | 408 | 0.84 | 5.9 (2–45) | 63 | 15.4 | 1 | 0.25 | |
| Shigella | 27 (2) | 0.47 | 0.01 | < 0.01 | 204 | 0.42 | 7.6 (2–47) | 17 | 8.3 | 0 | 0 | |
| Streptococcus equi | 1 (1) | 0.02 | < 0.01 | 0 | 37 | 0.08 | 37.0 (−) | 23 | 62.2 | 5 | 13.5 | |
| Vibrio cholerae (non‐toxigenic) | 1 (1) | 0.02 | < 0.01 | < 0.01 | 4 | 0.01 | 4.0 (−) | 1 | 25.0 | 0 | 0 | |
| Vibrio parahaemolyticus | 8 (2) | 0.14 | < 0.01 | < 0.01 | 113 | 0.23 | 14.1 (2–78) | 2 | 1.8 | 0 | 0 | |
| Yersinia | 14 (0) | 0.24 | < 0.01 | < 0.01 | 96 | 0.20 | 6.9 (2–23) | 4 | 4.2 | 0 | 0 | |
| Subtotal f , g | 1444 (246) | 25.1 | 0.32 | 0.33 | 9414 | 19.4 | 6.5 (1–138) | 1847 | 19.6 | 43 | 0.46 | |
| Bacterial toxins | Bacillus cereus toxins | 306 (15) | 5.3 | 0.07 | 0.02 | 3192 | 6.6 | 10.4 (2–383) | 66 | 2.1 | 2 | 0.06 |
| Clostridium botulinum toxins | 7 (2) | 0.12 | < 0.01 | < 0.01 | 20 | 0.04 | 2.9 (2–5) | 10 | 50.0 | 0 | 0 | |
| Clostridium perfringens toxins | 55 (22) | 0.95 | 0.01 | 0.01 | 2897 | 6.0 | 52.7 (2–950) | 11 | 0.38 | 3 | 0.10 | |
| Staphylococcus aureus toxins | 137 (38) | 2.4 | 0.03 | 0.02 | 2199 | 4.5 | 16.1 (2–119) | 148 | 6.7 | 4 | 0.18 | |
| Bacterial toxins, unspecified | 636 (2) | 11.0 | 0.14 | 0.11 | 5594 | 11.5 | 8.8 (2–139) | 181 | 3.2 | 2 | 0.04 | |
| Subtotal | 1141 (79) | 19.8 | 0.25 | 0.16 | 13,902 | 28.6 | 12.2 (2–950) | 416 | 3.0 | 11 | 0.08 | |
| Viruses | Flavivirus (including Tick‐borne Encephalitis virus) | 3 (3) | 0.05 | < 0.01 | < 0.01 | 8 | 0.02 | 2.7 (2–4) | 8 | 100 | 0 | 0 |
| Hepatitis A | 8 (5) | 0.14 | < 0.01 | < 0.01 | 71 | 0.15 | 8.9 (2–19) | 14 | 19.7 | 0 | 0 | |
| Hepatitis E | 4 (0) | 0.07 | < 0.01 | < 0.01 | 10 | 0.02 | 2.5 (2–4) | 7 | 70.0 | 0 | 0 | |
| Norovirus (and other calicivirus) | 332 (48) | 5.8 | 0.07 | 0.06 | 7305 | 15.0 | 22.0 (2–244) | 97 | 1.3 | 2 | 0.03 | |
| Rotavirus | 2 (1) | 0.03 | < 0.01 | < 0.01 | 28 | 0.06 | 14.0 (2–26) | 2 | 7.1 | 0 | 0 | |
| Other viruses, unspecified | 4 (0) | 0.07 | < 0.01 | 0.01 | 621 | 1.3 | 155.3 (3–600) | 7 | 1.1 | 0 | 0 | |
| Subtotal | 353 (57) | 6.1 | 0.08 | 0.08 | 8043 | 16.5 | 22.8 (2–600) | 135 | 1.7 | 2 | 0.02 | |
| Parasites | Cryptosporidium | 15 (3) | 0.26 | < 0.01 | < 0.01 | 298 | 0.61 | 19.9 (2–107) | 1 | 0.34 | 0 | 0 |
| Giardia h | 3 (0) | 0.05 | < 0.01 | < 0.01 | 7 | 0.01 | 3.5 (3–4) | 0 | 0 | 0 | 0 | |
| Trichinella | 7 (4) | 0.12 | < 0.01 | < 0.01 | 68 | 0.14 | 9.7 (3–26) | 10 | 14.7 | 0 | 0 | |
| Subtotal h | 25 (7) | 0.43 | < 0.01 | < 0.01 | 373 | 0.77 | 15.5 (2–107) | 11 | 2.9 | 0 | 0 | |
| Other causative agents | Histamine and Scombrotoxin | 100 (25) | 1.7 | 0.02 | 0.01 | 513 | 1.1 | 5.1 (2–94) | 44 | 8.6 | 0 | 0 |
| Marine biotoxins | 31 (3) | 0.54 | 0.01 | 0.01 | 82 | 0.17 | 2.6 (2–12) | 8 | 9.8 | 0 | 0 | |
| Mushroom toxins | 7 (3) | 0.12 | < 0.01 | < 0.01 | 25 | 0.05 | 3.6 (2–8) | 11 | 44.0 | 1 | 4.0 | |
| Other agents (incl. unspecified) | 3 (2) | 0.05 | < 0.01 | < 0.01 | 104 | 0.21 | 34.7 (5–74) | 3 | 2.9 | 0 | 0 | |
| Subtotal | 141 (33) | 2.4 | 0.03 | 0.02 | 724 | 1.5 | 5.1 (2–94) | 66 | 9.1 | 1 | 0.14 | |
| Unknown | Unknown / Unspecified | 2659 (65) | 46.1 | 0.59 | 0.37 | 16,149 | 33.2 | 6.1 (2–360) | 308 | 1.9 | 7 | 0.04 |
| EU Total e , i | 5763 (487) | 100 | 1.28 | 0.97 | 48,605 | 100 | 8.4 (1–950) | 2783 | 5.7 | 64 | 0.13 | |
Notes: ‘Escherichia coli other than STEC’ includes Enteroaggregative Escherichia coli (EAEC) (1), Enteroinvasive Escherichia coli (EIEC) (1), Enteropathogenic Escherichia coli (EPEC) (1), Enterotoxigenic Escherichia coli (ETEC) (2) and other unspecified Escherichia coli (10). ‘Marine biotoxins’ includes ciguatoxin (11) and other unspecified toxins (20). ‘Other agents’ includes atropine (1) and lectin (2).
Percentage of the total number of cases reported in the EU.
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Percentage of the total number of cases caused by the causative agent.
During the last phase of the production of this draft report, Hungary informed EFSA that one strong‐evidence outbreak (one case, one hospitalisation and one death) caused by Listeria monocytogenes, was reported in error.
Five outbreaks (84 cases and 29 hospitalisations) were caused by Salmonella Typhi.
For two outbreaks, information on cases was not available. These outbreaks were excluded from the calculation of the mean outbreak size.
For one outbreak, information on cases was not available. This outbreak was excluded from the calculation of the mean outbreak size.
For three outbreaks, information on cases was not available. These outbreaks were excluded from the calculation of the mean outbreak size.
In 2022, the frequency distribution of FBOs per single causative agent was similar to observations in 2021. Salmonella was responsible for by far the highest number of FBOs, followed by ‘bacterial toxins, unspecified’ and ‘norovirus (and other calicivirus)’, which was associated with the highest number of cases. Salmonella also caused the highest number of hospitalisations. L. monocytogenes was responsible for most reported deaths (N = 28; 43.8% of total deaths).
Eight MSs (Belgium, Denmark, Finland, France, Germany, Italy, Spain and Sweden) reported a high number and variety of agents (≥ 10) in FBOs. In contrast, seven MSs (Cyprus, Estonia, Latvia, Lithuania, Luxembourg, Romania and Slovenia) and the United Kingdom (Northern Ireland) reported ≤ three different causative agents in FBOs. These findings suggest a lack of harmonisation in FBO monitoring and reporting across MSs in 2022, as observed in previous years.
For an interactive view of the reporting countries and the number of causative agents reported by each country, see the dashboard on FBOs (here).
4.2.1 Bacteria
FBOs caused by bacteria were reported by all MSs except Bulgaria, by the United Kingdom (Northern Ireland) and by four non‐MSs (Norway, Republic of North Macedonia, Serbia and Switzerland).
Salmonella
Foodborne outbreaks caused by Salmonella were reported by all MSs except Bulgaria and Latvia, and by three non‐MSs (Norway, Serbia and Switzerland). France (N = 236), Spain (N = 225), Poland (N = 191) and Slovakia (N = 113) contributed the most to reporting data. Salmonella was the most frequently reported causative agent in 13 MSs (Austria, Croatia, Cyprus, Estonia, Greece, Hungary, Ireland, Lithuania, Luxembourg, Poland, Slovakia, Slovenia and Spain) and the United Kingdom (Northern Ireland), as well as in one non‐MS (Serbia).
The total number of FBOs caused by Salmonella increased in 2022 compared with 2021 (241 more FBOs, a relative increase of 31.2%), gradually returning to the level of pre‐pandemic years. Key statistics on FBOs caused by Salmonella are available in Table 53.
Among the FBOs reported to EFSA in 2022, Salmonella Typhi was identified as causative agent in five FBOs (one strong‐evidence FBO associated with contaminated water). These FBOs caused 84 cases and 29 hospitalisations and were reported by three MSs (Ireland, the Netherlands and Spain). In previous years, five FBOs caused by the same agent were reported in total, in 2008, 2014, 2016 and 2018.
Information on the serovar was available for half of the FBOs caused by non‐typhoidal Salmonella in the EU (N = 513; 50.6% of all Salmonella FBOs). S. Enteritidis was the main serovar reported (N = 395), followed by S. Typhimurium (N = 57) and monophasic S. Typhimurium (N = 21).
Compared with 2021, FBOs caused by S. Enteritidis increased by 12.9% (45 FBOs more than in 2021), 14.0% for S. Typhimurium (seven FBOs more than in 2021) and 250.0% for monophasic S. Typhimurium (15 FBOs more than in 2021). The huge increase for monophasic S. Typhimurium was mainly due to the reporting of a single multi‐country outbreak associated with chocolate products, with cases reported as single outbreaks by several MSs (Austria, Belgium, Denmark, France, Germany, Ireland, Italy, Luxembourg, the Netherlands, Spain, Sweden) and the United Kingdom (Northern Ireland). More details are available in the section on rapid outbreak assessments (Section 4.8).
The total number of cases and hospitalisations caused by S. Enteritidis and monophasic S. Typhimurium were higher than in 2021. FBO cases concerning S. Typhimurium decreased by 58.3% in 2022 (712 human cases fewer than in 2021). One possible reason for this fall is that in 2021 the number of cases caused by S. Typhimurium was inflated by a single outbreak in Finland involving 750 cases.
The other serovars accounted overall for 7.8% (N = 40) of the total number of Salmonella FBOs with known serovars: S. Agona, S. Ajiobo, S. Ball, S. Bovismorbificans, S. Braenderup, S. Chester, S. Choleraesuis, S. Derby, S. Durham, S. Give, S. Haifa, S. Hessarek, S. Infantis, S. Jukestown, S. Kottbus, S. Mbandaka, S. Mikawasima, S. Minnesota, S. Montevideo, S. Napoli, S. Senftenberg, S. Stanley, S. Strathcona, S. Thompson, S. Virchow. Interestingly, S. Durham, S. Jukestown, S. Minnesota were reported in 2022 for the first time since EFSA began collecting FBO data in 2004.
In 2022 monophasic S. Typhimurium, S. Mbandaka and S. Virchow were reported as causative agents of major multi‐country outbreaks focused by specific Rapid Outbreak Assessment by EFSA and ECDC, (see Section 4.8). Other Salmonella serovars associated with multi‐country outbreaks reported by MSs included S. Agona, S. Ball, S. Enteritidis, S. Jukestown, S. Senftenberg and S. Typhimurium.
Belgium, France, Slovenia and Sweden reported four large FBOs (> 100 cases) caused by S. Enteritidis and S. Typhimurium (one FBO each) and an unknown serovar (two FBOs).
Campylobacter
In 2022, Campylobacter was the fifth most frequently reported agent in FBOs (Table 53). The total number of FBOs and cases did not substantially change compared to figures for 2021 (N = 249). The severity of the disease was milder than in 2021, with a reduction in the number of hospitalisations (51 fewer hospitalisations than in 2021). In 2022, no deaths were reported in Campylobacter outbreaks, representing a remarkable difference compared with 2021 (six deaths).
Overall, 17 MSs (Austria, Belgium, Czechia, Denmark, Finland, France, Germany, Greece, Italy, Latvia, Lithuania, Malta, the Netherlands, Poland, Slovakia, Spain and Sweden) and one non‐MS (Norway) reported FBOs caused by this pathogen. France (N = 72) and Germany (N = 71) were the main contributors (56.1% of all FBOs caused by Campylobacter). In Germany and Malta, Campylobacter was the leading causative agent of FBOs in 2022.
Information on the Campylobacter species implicated in FBOs was available for 106 FBOs (41.6% of FBOs caused by this pathogen). C. jejuni and C. coli were reported in 98 and seven FBOs, respectively.
Listeria monocytogenes
In 2022, the total number of FBOs in the EU caused by L. monocytogenes , involving hospitalisations and deaths, was the highest ever reported to EFSA since it first began collecting FBO data in 2004 (Table 53). This pathogen was identified in a total of 35 FBOs from 11 MSs (Austria, Belgium, Denmark, Finland, France, Germany, Hungary, Italy, the Netherlands, Spain and Sweden). Three FBOs were also reported by two non‐MSs (Norway and Switzerland).
Overall, the health impact of listeriosis FBOs was much higher than in 2021, with a greater number of FBOs (12 more FBOs in 2022; an increase of 52.2%), cases (192 more cases in 2022; an increase of 184.6%), hospitalisations (194 more hospitalisations; an increase of 404.2%) and deaths (16 more deaths; an increase of 133.3%).
Italy reported the majority of human cases (N = 149; 50.3% of total EU cases) and hospitalisations (N = 149; 61.6% of total hospitalisations) and the two largest listeriosis outbreaks. Both were strong‐evidence outbreaks. The first involved 97 human cases (all hospitalised) of which five died. The second involved 43 human cases (all hospitalised) with one death. The implicated food vehicles were ‘broiler meat (Gallus gallus) and products thereof’ and ‘pig meat and products thereof’, respectively. Finland reported two severe strong‐evidence FBOs of listeriosis in vegetables. The first outbreak involved eight cases with six hospitalisations and three deaths. The second was a continuation of an outbreak reported in 2021 linked to pre‐cut vegetables, which in 2022 caused seven cases, seven hospitalisations and two deaths. Four deaths were also reported in a single weak‐evidence FBO in Finland involving 11 cases, with fish as the suspect food.
Shiga toxin‐producing E. coli (STEC)
In 2022, the number of FBOs caused by Shiga toxin‐producing E. coli (STEC) in the EU increased by 129.0% (40 more FBOs than in 2021) (Table 53). This was mainly due to the contribution of France, which provided information on 37 FBOs, accounting alone for more than 50.0% of the total number of STEC FBOs in the EU. Twelve MSs (Austria, Belgium, Denmark, France, Germany, Ireland, Italy, Malta, the Netherlands, Poland, Spain and Sweden) and the United Kingdom (Northern Ireland) as well as one non‐MS (Norway) reported FBOs related to STEC. STEC was the most frequently reported causative agent in FBOs in Ireland and the United Kingdom (Northern Ireland).
Among the FBOs with information on the serogroup (N = 14), serogroup O157 was associated with half of the STEC FBOs and the remaining outbreaks with serogroups O26, O104, O111, O113, O145, O178.
Poland reported 1 weak‐evidence outbreak caused by STEC O104, involving 16 human cases, 5 hospitalisations and 1 death. This is the first time that this STEC serogroup has been reported as the causative agent of an FBO in Europe since 2011, when the large multi‐country outbreak caused by the hybrid enteroaggregative STEC strain O104:H4 caused more than 3000 cases, 50 deaths and 800 cases of haemolytic uremic syndrome. However, no information on the virulence genes of the STEC strain implicated in the Polish outbreak was reported. The FBO occurred in ‘school or kindergarten’ but the implicated food vehicle was not identified.
Other bacteria
In Italy, Streptococcus equi subspecies zooepidemicus caused a severe strong‐evidence outbreak involving a total 37 human cases with 23 hospitalisations and 5 deaths (Table 53). A fresh cheese made from unpasteurised milk was identified as the source of the outbreak (Bosica et al., 2023). This outbreak deserves particular attention for its severity and because S. equi subspecies zooepidemicus has never been reported to EFSA since the collection of FBO data began in 2004.
FBOs caused by Escherichia coli other than STEC were reported by Czechia, Finland, France, Portugal and Spain, including E. coli belonging to the pathogroups enteroaggregative (EAEC), enteroinvasive (EIEC), enteropathogenic (EPEC) and enterotoxigenic (ETEC) and other unspecified E. coli. Two FBOs were also reported by two non‐MSs (Republic of North Macedonia and Switzerland), caused by unspecified E. coli and enteropathogenic E. coli, respectively.
Shigella caused a total of 27 FBOs (16 more FBOs than in 2021) reported by 11 MSs (Austria, Belgium, France, Germany, Greece, Ireland, Malta, the Netherlands, Slovakia, Spain and Sweden). For 13 FBOs no information on the Shigella species was provided. Twelve FBOs were caused by S. sonnei and two by S. flexneri . Norway and Switzerland also reported two FBOs caused by S. sonnei.
FBOs caused by Yersinia in the EU were all weak‐evidence outbreaks (N = 14), and were reported by seven MSs (Belgium, Denmark, Finland, France, Germany, Poland and Spain). Most of the FBOs were caused by Y. enterocolitica (N = 12). For two FBOs, the species was not specified. Three strong‐evidence outbreaks caused by Y. enterocolitica were also reported by one non‐MS (Norway).
Other bacterial agents causing FBOs in 2022 included Aeromonas caviae , Enterococcus spp., non‐toxigenic Vibrio cholerae and Vibrio parahaemolyticus .
4.2.2 Bacterial toxins
In 2022, the reporting rate of FBOs caused by bacterial toxins was 0.25 per 100,000 population. This was a relative increase of 68.2% compared with the rate in 2021, owing mainly to the increased reporting of FBOs associated with Bacillus cereus toxins.
In total, 16 MSs (Belgium, Croatia, Denmark, Finland, France, Germany, Greece, Hungary, Italy, the Netherlands, Poland, Portugal, Romania, Slovenia, Spain and Sweden) and 3 non‐MSs (Republic of North Macedonia, Serbia and Switzerland) reported information on outbreaks caused by bacterial toxin‐producing agents. As in recent years, most of them were notified by France (N = 1020), which alone contributed to 89.4% of all FBOs caused by bacterial toxins in the EU. However, most of the outbreaks reported by France were caused by unspecified bacterial toxins (N = 628).
The intake of bacterial toxins through contaminated food caused 11 deaths in eight FBOs, in 2022 (Table 53). Most of them (N = 9 in six outbreaks) were reported in ‘health care and residential facilities’.
Bacillus cereus toxins ranked first for the number of reported FBOs caused by bacterial toxins and was responsible for two deaths. It was reported by eight MSs (Belgium, Finland, France, Germany, Hungary, Italy, Portugal and Spain) and one non‐MS (Switzerland). In the EU, only 15 FBOs were strong‐evidence FBOs. A considerable increase in the number of FBOs caused by Bacillus cereus toxins was observed in 2022 compared with 2021 (219 more FBOs in 2022, a relative increase of 251.7%). This increase is mainly attributable to France, which alone reported 90.8% of all these FBOs (208 more FBOs than in 2021, a relative increase of 297.1%). Bacillus cereus toxins was identified as the causative agent of five very large (i.e. ≥ 100 cases) FBOs, reported by Spain and France.
Staphylococcus aureus toxins was the second most frequently reported bacterial toxin‐producing agent in FBOs, and first for the number of hospitalisations and deaths, followed by C. perfringens toxins and Clostridium botulinum toxins (Table 53). For these three causative agents, strong‐evidence FBOs accounted for more than 25.0% of total reported FBOs. In Portugal and Romania, S. aureus toxins was the causative agent reported in most FBOs.
Nine MSs (Belgium, Denmark, Finland, France, Italy, Portugal, Slovenia, Spain and Sweden) reported FBOs caused by C. perfringens toxins. In 2022, this pathogen was associated with the largest mean outbreak size (52.7 cases), mainly due to seven very large (i.e. ≥ 100 cases) FBOs causing altogether 1869 cases and mainly occurring in ‘school and kindergarten’ (N = 4). The largest outbreak (950 cases) was reported by Portugal and was linked to the consumption of cooked RTE meat in ‘temporary mass catering (fairs or festivals)’.
4.2.3 Viruses
In 2022, 20 MSs (all MSs except Bulgaria, Cyprus, Estonia, Greece, Lithuania, Malta and Romania) and 4 non‐MSs (Iceland, Montenegro, Norway and Switzerland) reported FBOs caused by viruses (Table 53).
Norovirus (and other calicivirus)
Norovirus (and other calicivirus) was the third most frequently reported causative agent (Table 53), with most cases occurring in France (N = 140; 42.2% of FBOs caused by norovirus (and other calicivirus)). Eighteen MSs and three non‐MSs reported FBOs associated with norovirus (and other calicivirus). In Denmark, Finland, Latvia, Luxembourg and Portugal as well as in Iceland norovirus (and other calicivirus) was the main causative agent of FBOs. The number of FBOs and cases caused by norovirus (and other calicivirus) increased by 32.3% and 11.6% in 2022 (81 more FBOs and 760 more cases than in 2021) respectively, while hospitalisations decreased (59 fewer hospitalisations than in 2021) (Table 53).
Overall in the EU, this causative agent involved the highest number of human cases (N = 7305). Norovirus (and other calicivirus) was associated with a number of very large outbreaks (mean outbreak size of 22.0 on average), mainly reported as general outbreaks (72.6% of all FBOs caused by norovirus (and other calicivirus)). Twelve FBOs reported by seven MSs involved more than 100 human cases each, totalling altogether 1606 cases. They were linked to a large variety of food commodities (i.e. ‘bovine meat’, ‘buffet meals’, ‘cheese and dairy products’, ‘mixed food’, ‘vegetables and juices and other products thereof’, ‘water’), settings (‘canteen or catering at workplace, school etc.’, ‘health care and residential facilities’, ‘multiple places of exposure', ‘restaurants, pubs, street vendors, takeaway etc.’) and contributory factors. However, only five large FBOs were strong‐evidence outbreaks. In addition, Switzerland reported one outbreak involving 100 cases.
Hepatitis A
In 2022, the number of reported FBOs caused by Hepatitis A was lower than in 2021 (five fewer FBOs). Only six MSs (Croatia, Czechia, Hungary, Ireland, Italy and Sweden) and one non‐MS (Montenegro) contributed to the reporting. Three strong‐evidence FBOs were reported by Croatia, all of them linked to the consumption of sandwiches contaminated by infected food handlers. In all FBOs, the place of exposure was ‘school and kindergarten’.
Other viruses
Other reported viruses causing FBOs in the EU in 2022 were Hepatitis E, flavivirus and rotavirus (Table 53). The number of FBOs caused by these agents fell within the same range as in recent years. The number of FBOs and hospitalisations caused by flavivirus decreased progressively from 2018 to 2022. All FBOs caused by flavivirus were strong‐evidence outbreaks caused by tick‐borne encephalitis virus (TBE) reported by Slovakia and linked to the consumption of raw sheep milk and cheese made from sheep milk.
4.2.4 Parasites
FBOs caused by parasites were reported by 12 MSs (Belgium, Croatia, Denmark, Finland, France, Germany, Ireland, Italy, Malta, Romania, Spain and Sweden) and 3 non‐MSs (Bosnia and Herzegovina, Norway and Serbia), in 2022 (Table 53).
Cryptosporidium
Six MSs (Belgium, Denmark, Finland, Germany, Malta and Sweden) reported outbreaks caused by Cryptosporidium (Table 53), which increased by 650.0% (13 more FBOs than in 2021). C. parvum was involved in four FBOs (for the remaining outbreaks, information on the species was not specified). The two largest outbreaks were reported by Sweden and involved 107 and 75 human cases, linked respectively to the consumption of a RTE salad and buffet meals. In addition, three FBOs caused by Cryptosporidium were also reported by one non‐MS (Norway).
Trichinella
A gradual decrease in the number of FBOs caused by Trichinella has been observed since 2017, with the exception of 2022 (N = 11). In the EU, seven FBOs caused by Trichinella (six more than in 2021) were reported by five MSs (Croatia, France, Italy, Romania and Spain) and involved a total of 68 human cases, 10 of whom were hospitalised. No deaths were reported (Table 53). Four FBOs were strong‐evidence outbreaks and caused 40 human cases and 8 hospitalisations.
The species of Trichinella was reported only for two strong‐evidence FBOs by Croatia and Romania, where it was T. spiralis . Croatia reported the largest outbreak caused by T. spiralis, with 26 cases and one hospitalisation, linked to the consumption of pig meat from breeding domesticated pigs. The other strong‐evidence FBO caused by T. spiralis was a household outbreak occurring in a domestic setting, which involved six cases, all hospitalised, after the consumption of fresh pig meat.
In addition, four strong‐evidence FBOs caused by T. spiralis were reported by two non‐MSs (Bosnia and Herzegovina and Serbia), causing a total of 61 human cases and four hospitalisations. The implicated food vehicles were sausages made from pig meat in the FBO occurring in Bosnia and Herzegovina (N = 1) while ‘meat and meat products’, including meat from wild boar and products thereof and homemade dry pig meat, were the food vehicles implicated in the FBOs occurring in Serbia (N = 3).
Giardia
Two MSs (Croatia and Ireland) reported three FBOs associated with Giardia , all weak‐evidence FBOs (Table 53). A suspected vehicle was only reported in the two FBOs in Ireland, where it was ‘water’. Giardia intestinalis was specified in one FBO in Croatia.
4.2.5 Other causative agents
In 2022, FBOs caused by causative agents other than bacteria, bacterial toxins, viruses and parasites, such as histamine and scombrotoxin, marine biotoxins, mushroom toxins or other agents, namely atropine and lectin, were reported by nine MSs (Belgium, Denmark, France, Germany, Italy, Malta, Poland, Spain and Sweden) in the EU (Table 53). For a correct interpretation of the findings, it is important to remember that these causative agents are not regularly covered by national surveillance programmes. The total number of FBOs reported in the EU may therefore be underestimated.
FBOs caused by histamine and scombrotoxin increased by 112.8% compared with 2021 (53 more FBOs in 2022). This increase was mainly related to a higher number of FBOs reported by France (55 FBOs reported in 2022, 22 outbreaks more than in 2021) and Spain (19 FBOs reported in 2022, 18 more outbreaks than in 2021).
Marine biotoxins were responsible for a higher number of FBOs than in 2021 (14 FBOs more; a relative increase of 82.4%). Only two MSs (France and Spain) contributed to the reporting. Among these FBOs, ciguatoxin was identified in 11 outbreaks. Marine biotoxins, in particular ciguatoxins, are considered an emerging threat in Europe and a real reason of concern, owing to the increased presence of toxin‐producing microalgae and fish with ciguatoxins in Europe (Canals et al., 2021).
Mushroom toxins were responsible for seven FBOs reported by three MSs (France, Poland, Spain).
Denmark reported two outbreaks caused by lectin, involving a total of 99 human cases. One was a strong‐evidence outbreak where the place of exposure was ‘school or kindergarten’ and the FBO vehicles were bean soup and green lentils in potato and leek soup. Legumes, like beans, are known to be rich in lectins. Alongside their beneficial effects, these proteins can have health consequences (e.g. nausea, vomiting, diarrhoea, abdominal pain) if legumes are consumed raw or undercooked (He et al., 2018).
4.2.6 Outbreaks caused by unknown/unspecified agents
In 2022, outbreaks caused by unknown agents accounted for 2659 FBOs in the EU (Table 53), an increase of 45.1% compared to 2021. This is the highest number of FBOs with unknown causative agents ever reported to EFSA. More than two‐thirds of these FBOs were notified to EFSA by Belgium (N = 770) and the Netherlands (N = 1139). In these countries, FBOs of unknown origin accounted for the vast majority of reports (92.8% and 98.0%, respectively). Other MSs where most outbreaks were caused by an unknown agent were Czechia, Italy and Sweden. Another 13 MSs (Croatia, Denmark, Finland, France, Germany, Greece, Hungary, Ireland, Lithuania, Poland, Romania, Slovenia and Spain) and five non‐MSs (Bosnia and Herzegovina, Montenegro, Norway, Republic of North Macedonia and Switzerland) contributed to this reporting.
Outbreaks with unknown agents usually occur in confined environments where it is relatively easy to find a link among cases. However, nine FBOs were very large and involved ≥ 100 cases, with eight MSs (Belgium, Croatia, Czechia, France, Greece, Poland, Spain and Sweden) and one non‐MS (Norway), accounting for 1223 and 100 human cases, respectively.
4.3 Overview of food vehicles implicated in foodborne outbreaks
The following sections provide information on the food vehicles implicated in FBOs in 2022 in the EU. Only strong‐evidence outbreaks are considered for this purpose since the body of evidence (i.e. the proof) linking the consumption of a food vehicle and the human cases means that the level of uncertainty around this association is low.
Search interactively for details on food vehicles implicated in strong‐evidence FBOs in MSs and non‐MS countries using the EFSA dashboard (here, page on ‘food vehicles’ for information on FBOs for each implicated food vehicle).
4.3.1 Food vehicles in strong‐evidence outbreaks
Twenty‐three MSs (all except Bulgaria, Cyprus, Latvia and Malta) and the United Kingdom (Northern Ireland) provided information on 487 strong‐evidence FBOs (8.5% of all FBOs reported in the EU), an increase of 36.8% over 2021 (131 more FBOs than in 2021). Spain was the main contributor (37.6% of the total), followed by France (13.6% of the total). Table 54 describes the food vehicles implicated in strong‐evidence FBOs in 2022 in the EU.
TABLE 54.
Frequency distribution of strong‐evidence foodborne outbreaks, by food vehicle, in reporting EU MSs, 2022.
| Type of vehicle | Strong‐evidence outbreaks | Reporting rate per 100,000 | Rank | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outbreaks | Cases | Hospitalisations | Deaths | 2022 | 2018–2021 b | 2022 | 2018–2021 b | |||||
| N | % of total | N | % of total | N | % of total | N | % of total | |||||
| Composite foods, multi‐ingredient foods and other foods | ||||||||||||
| Mixed foods c | 93 | 19.1 | 1960 | 19.9 | 163 | 17.6 | 3 | 9.7 | 0.021 | 0.014 | 2 | 3 |
| Bakery products d | 17 | 3.5 | 262 | 2.7 | 60 | 6.5 | 0 | 0 | 0.004 | 0.005 | 8 | 7 |
| Sweets and chocolate e | 14 | 2.9 | 215 | 2.2 | 56 | 6.0 | 0 | 0 | 0.003 | 0.001 | 10 | 19 |
| Buffet meals | 8 | 1.6 | 246 | 2.5 | 1 | 0.11 | 0 | 0 | 0.002 | 0.002 | 14 | 12 |
| Canned food products f | 1 | 0.21 | 2 | 0.02 | 0 | 0 | 0 | 0 | < 0.001 | < 0.001 | 18 | 23 |
| Other foods | 10 | 2.1 | 512 | 5.2 | 8 | 0.86 | 0 | 0 | 0.002 | 0.004 | 13 | 10 |
| Subtotal | 143 | 29.4 | 3197 | 32.4 | 288 | 31.1 | 3 | 9.7 | 0.032 | 0.027 | ‐ | ‐ |
| Eggs and egg products g | 103 | 21.1 | 919 | 9.3 | 142 | 15.3 | 4 | 12.9 | 0.023 | 0.018 | 1 | 1 |
| Meat and meat products | ||||||||||||
| Pig meat and products thereof h , i | 34 | 7.0 | 730 | 7.4 | 128 | 13.8 | 4 | 12.9 | 0.008 | 0.006 | 4 | 5 |
| Broiler meat (Gallus gallus) and products thereof j | 21 | 4.3 | 386 | 3.9 | 106 | 11.4 | 5 | 16.1 | 0.005 | 0.004 | 6 | 9 |
| Meat and meat products, unspecified | 16 | 3.3 | 456 | 4.6 | 20 | 2.2 | 0 | 0 | 0.004 | 0.004 | 9 | 8 |
| Bovine meat and products thereof k | 11 | 2.3 | 341 | 3.5 | 49 | 5.3 | 0 | 0 | 0.002 | 0.002 | 12 | 14 |
| Turkey meat and products thereof | 1 | 0.21 | 32 | 0.32 | 0 | 0 | 0 | 0 | < 0.001 | < 0.001 | 18 | 21 |
| Sheep meat and products thereof | 1 | 0.21 | 30 | 0.30 | 10 | 1.1 | 0 | 0 | < 0.001 | < 0.001 | 18 | 21 |
| Other or mixed red meat and products thereof l | 10 | 2.1 | 1002 | 10.2 | 11 | 1.2 | 0 | 0 | 0.002 | 0.002 | 13 | 16 |
| Other, mixed or unspecified poultry meat and products thereof m | 6 | 1.2 | 164 | 1.7 | 0 | 0 | 0 | 0 | 0.001 | 0.001 | 15 | 17 |
| Subtotal | 100 | 20.5 | 3141 | 31.8 | 324 | 35.0 | 9 | 29.0 | 0.022 | 0.020 | – | – |
| Fish and fishery products | ||||||||||||
| Fish and fish products n | 49 | 10.1 | 371 | 3.8 | 29 | 3.1 | 2 | 6.5 | 0.011 | 0.007 | 3 | 4 |
| Crustaceans, shellfish, molluscs and products thereof o | 20 | 4.1 | 223 | 2.3 | 8 | 0.9 | 0 | 0 | 0.004 | 0.015 | 7 | 2 |
| Subtotal | 69 | 14.2 | 594 | 6.0 | 37 | 4.0 | 2 | 6.5 | 0.015 | 0.022 | – | – |
| Milk and milk products | ||||||||||||
| Cheese p | 16 | 3.3 | 275 | 2.8 | 33 | 3.6 | 5 | 16.1 | 0.004 | 0.002 | 9 | 12 |
| Dairy products (other than cheeses) q | 10 | 2.1 | 178 | 1.8 | 14 | 1.5 | 2 | 6.5 | 0.002 | 0.001 | 13 | 20 |
| Milk r | 4 | 0.82 | 13 | 0.13 | 5 | 0.5 | 0 | 0 | 0.001 | 0.002 | 16 | 13 |
| Subtotal | 30 | 6.2 | 466 | 4.7 | 52 | 5.6 | 7 | 22.6 | 0.007 | 0.005 | – | – |
| Food of non‐animal origin | ||||||||||||
| Vegetables and juices and products thereof s | 24 | 4.9 | 780 | 7.9 | 41 | 4.4 | 6 | 19.4 | 0.005 | 0.006 | 5 | 6 |
| Cereal products including rice and seeds/pulses t | 2 | 0.41 | 7 | 0.07 | 3 | 0.3 | 0 | 0 | < 0.001 | 0.002 | 17 | 15 |
| Fruit, berries and juices and products thereof u | 2 | 0.41 | 18 | 0.18 | 5 | 0.5 | 0 | 0 | < 0.001 | 0.001 | 17 | 18 |
| Subtotal | 28 | 5.7 | 805 | 8.2 | 49 | 5.3 | 6 | 19.4 | 0.006 | 0.009 | – | – |
| Water v | 13 | 2.7 | 618 | 6.3 | 34 | 3.7 | 0 | 0 | 0.003 | 0.002 | 11 | 14 |
| Drinks, including bottled water | 1 | 0.21 | 123 | 1.2 | 0 | 0 | 0 | 0 | < 0.001 | 0 | 18 | 24 |
| Subtotal | 14 | 2.9 | 741 | 7.5 | 34 | 3.7 | 0 | 0 | 0.003 | 0.002 | – | – |
| EU Total i | 487 | 100 | 9863 | 100 | 926 | 100 | 31 | 100 | 0.109 | 0.105 | – | – |
Notes: Single food items are consolidated into major groups according to their origin. The ‘outbreak reporting rate' columns include the mean outbreak reporting rate per 100,000 for 2022 and for the previous years (2018–2021) for trend watching. The ranking of each food item provides a visual demonstration of the relative importance of the item, among all food vehicles implicated in foodborne outbreaks, for the same year and period.
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
‘Mixed food’ includes ‘mixed food’ (44), ‘other processed food products and prepared dishes – meat based dishes’ (8), ‘other processed food products and prepared dishes – sandwiches’ (7), ‘ready‐to‐eat salads’ (5), ‘other processed food products and prepared dishes’ (5), ‘other processed food products and prepared dishes – rice based dishes’ (4), ‘other processed food products and prepared dishes ‐ pasta based dishes’ (3), ‘other processed food products and prepared dishes – sandwiches – with meat’ (2), ‘other processed food products and prepared dishes – pasta’ (2), ‘other processed food products and prepared dishes – vegetable‐based dishes’ (2), ‘other processed food products and prepared dishes – fish and seafood based dishes’ (2), ‘other processed food products and prepared dishes – pasta – filled pasta’ (2), ‘other processed food products and prepared dishes – mushroom based dishes’ (2), ‘sauce and dressings’ (1), ‘other processed food products and prepared dishes – potato based dishes’ (1), ‘tomato‐containing cooked sauces’ (1), ‘other processed food products and prepared dishes – finger food’ (1), ‘other processed food products and prepared dishes – pizza and pizza‐like dishes’ (1).
‘Bakery products’ includes ‘bakery products – cakes’ (7), ‘bakery products’ (4), ‘bakery products – desserts – containing raw eggs’ (3), ‘bakery products – desserts – containing raw cream’ (2), ‘bakery products – cakes – containing heat‐treated cream’ (1).
‘Sweets and chocolate' includes ‘Chocolate' (9), ‘confectionery products and pastes – soft candy’ (2), ‘sweets and chocolate' (2), ‘confectionery products and pastes – chocolate‐based product’ (1).
‘Canned food products’ includes ‘fish – canned’ (1).
‘Eggs and egg products’ includes ‘eggs and egg products’ (99), ‘eggs’ (4).
‘Pig meat and products thereof’ includes ‘pig meat and products thereof’ (21), ‘meat from pig – meat products – ready‐to‐eat’ (3), ‘meat from pig – meat products – meat specialities’ (2), ‘meat from pig – fresh’ (2), ‘meat from pig – meat products – fresh raw sausages’ (2), ‘cured seasoned pork meat’ (1), ‘meat from pig – minced meat – intended to be eaten raw’ (1), ‘meat from pig – meat products’ (1), ‘meat from pig – meat products – cooked ham’ (1).
During the last phase of the production of this draft report, Hungary informed us that the one strong‐evidence outbreak (one case, one hospitalisation and one death) with ‘pig meat and products thereof’ as the implicated food vehicle was reported in error.
‘Broiler meat (Gallus gallus) and products thereof’ includes ‘broiler meat (Gallus gallus) and products thereof’ (11), ‘meat from broilers (Gallus gallus)’ (7), ‘meat from broilers (Gallus gallus) – meat products’ (1), ‘meat from broilers (Gallus gallus) ‐ meat products – ready‐to‐eat’ (1), ‘meat from broilers (Gallus gallus) – fresh’ (1).
‘Bovine meat and products thereof’ includes ‘bovine meat and products thereof’ (5), ‘meat from bovine animals – meat products – meat specialities’ (3), ‘meat from bovine animals – meat preparation – intended to be eaten raw’ (1), ‘meat from bovine animals – minced meat’ (1), ‘meat from bovine animals – meat products – raw and intended to be eaten raw’ (1).
‘Other or mixed red meat and products thereof’ includes ‘other or mixed red meat and products thereof’ (7), ‘meat, mixed meat – minced meat’ (1), ‘meat from deer (venison) – meat preparation – intended to be eaten cooked’ (1), ‘meat, mixed meat – meat products – ready‐to‐eat’ (1).
‘Other, mixed or unspecified poultry meat and products thereof’ includes ‘other, mixed or unspecified poultry meat and products thereof’ (4), ‘meat from poultry, unspecified’ (1), ‘meat from poultry, unspecified – meat preparation’ (1).
‘Fish and fish products’ includes ‘fish and fish products’ (39), ‘fish – fishery products from fish species associated with a high amount of histidine – not enzyme maturated’ (5), ‘fish’ (3), ‘fish – smoked’ (2).
‘Crustaceans, shellfish, molluscs and products thereof’ includes ‘crustaceans, shellfish, molluscs and products thereof’ (15), ‘live bivalve molluscs – oysters’ (4), ‘snails’ (1).
‘Cheese' includes ‘cheese' (12), ‘cheeses made from sheep's milk – fresh’ (1), ‘cheeses, made from unspecified milk or other animal milk’ (1), ‘cheeses made from cows' milk’ (1), ‘cheeses made from goats' milk’ (1).
‘Dairy products (other than cheeses)’ includes ‘dairy products (other than cheeses)’ (5), ‘dairy products (excluding cheeses) – ice cream’ (3), ‘dairy products (excluding cheeses) – cheese analogue' (1), ‘dairy products (excluding cheeses) – dairy desserts’ (1).
‘Milk’ includes ‘milk, sheep's’ (2), ‘milk’ (2).
‘Vegetables and juices and other products thereof’ includes ‘vegetables and juices and other products thereof’ (15), ‘mushrooms’ (2), ‘vegetables’ (2), ‘vegetables – pre‐cut’ (2), ‘lentil’ (1), ‘rocket, rucola’ (1), ‘spring onion’ (1).
‘Cereal products including rice and seeds/pulses (nuts, almonds)’ includes ‘cereals and meals – flour/meal or finely ground powder’ (1), ‘cereal products including rice and seeds/pulses (nuts, almonds)’ (1).
‘Fruit, berries and juices and other products thereof’ includes ‘fruits – products’ (1), ‘fruit, berries and juices and other products thereof’ (1).
‘Water’ includes ‘tap water, including well water’ (10), ‘water’ (2), ‘water – potable water’ (1).
Composite foods, multi‐ingredient foods and other foods
Foodstuffs belonging to the group ‘composite foods, multi‐ingredient foods and other foods’ ranked first in 2022 among the food vehicles implicated in FBOs and were reported by all but seven MSs (Bulgaria, Cyprus, Estonia, Greece, Latvia, Malta and Slovenia), by the United Kingdom (Northern Ireland) and by three non‐MSs (Iceland, Norway and Switzerland). A total of 143 strong‐evidence FBOs linked to this food group were observed in the EU (Table 54), an increase of 34.9% over 2021 (37 more FBOs in 2022).
The consumption of processed foods is increasing continuously in high‐income countries (Monteiro et al., 2013). This food group includes an extremely wide miscellanea of foods, produced with a combination of multiple ingredients under different processing conditions, either in domestic kitchens or in industrial laboratories and catering facilities, sometimes requiring a high degree of food manipulation and special manufacturing and preservation practices. For this reason, incidents leading to food contamination may be more frequent than in other food groups and may originate from the use of contaminated ingredients, from mechanisms of cross‐contamination among foods, from the processing environment and equipment, and also from food handlers.
‘Mixed food’ was the main food category reported in the EU, causing 17 more outbreaks than in 2021 and the highest number of cases among all food vehicles implicated in strong‐evidence FBOs. A complete description of the food vehicles included in this category is available as a footnote in Table 54. The causative agents responsible for these FBOs included Salmonella (including S. Enteritidis, S. Mbandaka, S. Virchow and Salmonella with unspecified serovar), norovirus, Staphylococcus aureus toxins, C. perfringens, Bacillus cereus, Hepatitis A virus, L. monocytogenes, Cryptosporidium, including Cryptosporidium parvum, Campylobacter, Clostridium botulinum, Vibrio cholerae (non‐toxigenic) and unspecified bacterial toxins. For 19 outbreaks, the causative agent was not identified.
The reporting of outbreaks caused by ‘bakery products’ remained fairly stable in 2022 compared with 2021 (Table 54). Among the FBOs associated with ‘bakery products’, most concerned cakes and desserts containing raw cream or raw eggs. Salmonella, including S. Enteritidis and Salmonella with unspecified serovar, norovirus and C. perfringens were the agents identified in these FBOs.
A total of 14 FBOs linked to the consumption of ‘sweets and chocolate' were reported in 2022, a relative increase of 600.0% compared with the number notified in 2021 (12 more outbreaks in 2022). This increase is mainly attributable to the separate counting of 11 single FBOs reported by MSs, which were part of the same multi‐country outbreak. Overall, the total number of human cases and hospitalisations involved in FBOs associated with ‘sweets and chocolate' increased by 532.4% (181 more human cases in 2022) and 600.0% (48 more hospitalisations in 2022), respectively. More information on the multi‐country outbreak of S. Typhimurium sequence type (ST) 34 linked to chocolate products is available in the section on rapid outbreak assessments (Section 4.8).
Other reported vehicles in this group included ‘buffet meals’, ‘canned food products’ and ‘other foods’ with no substantial variations compared to recent years.
Food of animal origin
The category of foods of animal origin, which includes ‘eggs and egg products’, ‘meat and meat products’, ‘fish and fishery products’ and ‘milk and milk products’, caused a high number of FBOs (N = 302; 62.0% of all strong‐evidence FBOs), human cases (N = 5120; 51.9% of all strong‐evidence FBOs), hospitalisations (N = 555; 59.9% of all strong‐evidence FBOs) and deaths (N = 22; 71.0% of all strong‐evidence FBOs) (Table 54).
In 2022, ‘eggs and egg products’ was the most frequently reported food category among food vehicles, as it was in the FBOs reported in previous years, on average. A total of 103 FBOs were reported by eight MSs (Austria, Belgium, France, Italy, Lithuania, Poland, Slovakia and Spain), an increase of 145.2% over 2021 (61 more FBOs). Cases, hospitalisations and deaths are shown in Table 54. Salmonella was the main agent involved in outbreaks associated with the consumption of this food vehicle (N = 86; 83.5%), including S. Enteritidis (N = 37), S. Typhimurium (N = 4) and other unspecified serovars of Salmonella (N = 45). Six FBOs were also reported by two non‐MSs.
‘Meat and meat products’ was the second most frequently reported food vehicle group of animal origin (N = 100; a 29.9% increase over 2021), causing 3141 human cases, 324 hospitalisations and nine deaths. Various food vehicles belong to this group, as described in Table 54. All MSs reported strong‐evidence FBOs, except Ireland, Luxembourg and Slovakia. Three non‐MSs also reported FBOs caused by ‘meat and meat products’. In the EU, ‘pig meat and products thereof’ and ‘broiler meat (Gallus gallus) and products thereof’ accounted for the highest number of hospitalisations and deaths (Table 54). Most hospitalisations and deaths were caused by L. monocytogenes in both ‘pig meat and products thereof’ (63 hospitalisations and 3 deaths) and ‘broiler meat (Gallus gallus) and products thereof’ (97 hospitalisations and 5 deaths).
‘Other or mixed red meat and products thereof’ was the food of animal origin that caused the highest number of human cases (N = 1002), mainly due to the reporting of three very large strong‐evidence outbreaks caused by C. perfringens toxins, which altogether involved 961 cases. Other causative agents linked with this food vehicle were B. cereus toxins, Salmonella and S. aureus toxins.
A total of 69 FBOs caused by the consumption of food items belonging to the ‘fish and fishery products’ group were reported by 12 MSs (Austria, Croatia, Denmark, Finland, France, Germany, Italy, Lithuania, the Netherlands, Romania, Spain and Sweden). Two more FBOs were reported by two non‐MSs. In the EU, the number of FBOs was higher than in 2021 (14 more FBOs) mainly because of the reporting of a higher number of FBOs linked to ‘fish and fish products’ (19 more FBOs in 2022). In contrast, ‘crustaceans, shellfish, molluscs and products thereof’ were reported in smaller numbers (five fewer FBOs than in 2021). The most frequently reported causative agents in the ‘fish and fishery products’ group were histamine, norovirus, Salmonella including S. Enteritidis, S. Typhimurium and unspecified serovars, L. monocytogenes.
In the ‘milk and milk products’ group, FBOs associated with the consumption of either ‘cheese', ‘dairy products (other than cheeses)’ or ‘milk’ were reported by 10 MSs (Austria, Belgium, Croatia, France, Germany, Italy, Lithuania, Romania, Slovakia and Spain) and one non‐MS in similar numbers to the figures observed in 2021. The causative agents linked to ‘milk and milk products’ were S. aureus toxins, S. Enteritidis and unspecified Salmonella, Tick‐borne Encephalitis virus, norovirus, L. monocytogenes, Campylobacter jejuni, Streptococcus equi, Shigella, Enteropathogenic E. coli. Five persons died in an FBO caused by S. equi subsp. Zooepidemicus (more information is available in Section 4.2.1 on Bacteria).
Foods of non‐animal origin
FBOs linked to foods of non‐animal origin were reported by nine MSs (Denmark, Finland, France, Germany, Hungary, Italy, Poland, Spain and Sweden) and two non‐MSs. The number of strong‐evidence FBOs linked to this type of food decreased by 37.8% in 2022 compared with 2021 (17 fewer FBOs).In seven MSs (Denmark, Finland, France, Germany, Poland, Spain and Sweden) ‘vegetables and juices and other products thereof’ were responsible for most FBOs (24 outbreaks) caused by foods of non‐animal origin (85.7%) in the EU (Table 54), with a decrease of 29.4% compared with 2021 (10 fewer FBOs). Vegetables were implicated also in the two severe outbreaks of listerioses in Finland described above. S. Typhimurium caused a very large strong‐evidence outbreak in Sweden involving 102 human cases and associated with ‘rocket, rucola’. Other causative agents associated with ‘vegetables and juices and other products thereof’ included S. aureus, Salmonella including S. Chester and S. Mbandaka, Bacillus cereus, norovirus, mushroom toxins, lectins, Cryptosporidium parvum and C. botulinum.
Other foods of non‐animal origin implicated in strong‐evidence FBOs were ‘cereal products including rice and seeds/pulses (nuts, almonds)’ (reported by Italy and Spain), ‘fruit, berries and juices and other products thereof’ (reported by Hungary and Poland). S. Typhimurium and atropine and Hepatitis A virus and rotavirus were the identified causative agents in the two groups, respectively.
4.3.2 Suspect food in weak‐evidence outbreaks
In 2022, 5276 weak‐evidence FBOs were reported by 25 MSs (all except Bulgaria and Lithuania) and the United Kingdom (Northern Ireland) in the EU. In line with what was observed in previous years, weak‐evidence FBOs outnumbered those reported as strong‐evidence, accounting for 91.5% of all FBOs in 2022 in the EU. Sixty‐nine weak‐evidence FBOs were also reported by seven non‐MSs (Bosnia and Herzegovina, Iceland, Montenegro, Norway, Republic of North Macedonia, Serbia and Switzerland). France and the Netherlands accounted for most of the reports in the EU (55.9% of all weak‐evidence FBOs), providing information on 1795 and 1155 FBOs, respectively.
Overall, no major discrepancies were observed in the ranking of food types for weak‐evidence outbreaks, compared with strong‐evidence outbreaks. However, ‘eggs and egg products’ were more frequently reported in strong‐evidence FBOs than in weak‐evidence outbreaks (N = 167 corresponding to 5.7% of weak‐evidence FBOs with information on the suspect food available). Among weak‐evidence FBOs associated with ‘mixed food’, the most frequently suspected food was ‘sushi’, followed by ‘mushroom based dishes’, ‘meat based dishes’, ‘sauce and dressings’, ‘sandwiches’, ‘pasta or rice based dishes’, ‘ready‐to‐eat salads’, ‘pizza and pizza‐like dishes’, ‘soups’, ‘legume based dishes’, ‘potato based dishes’, ‘fish and seafood based dishes’. More information is available on the dashboard (here, see page on ‘Food vehicles and causative agents’).
4.3.3 Top‐10 agent/food pairs in strong‐evidence outbreaks associated with the highest impact on health in the EU, 2022
The top‐10 pairs of causative agents and food vehicles in outbreaks involving the highest health impact in 2022 in the EU in terms of all outbreaks, cases, hospitalisations and deaths, are shown in Tables 55, 56, 57 and 58. These tables include also details on the number of MSs reporting FBOs for the relative food/agent pair in 2022, as well as for the period 2018–2021, for trend watching purposes.
TABLE 55.
Top‐10 pathogen/food vehicle pairs causing the highest number of strong‐evidence outbreaks in reporting EU MSs, 2022.
| 2022 | 2018–2021 a,b | Evaluation | ||||||
|---|---|---|---|---|---|---|---|---|
| Rank c | Causative agent | Food vehicle | Outbreaks (N) | Reporting MS (N outbreaks) | Rank c | Outbreaks (N/year) (range) | Reporting MS (N/year) | 2022 versus 2018–2021 d |
| 1 | Salmonella | Eggs and egg products e | 86 | Spain (34), Poland (26), France (14), Slovakia (4), Belgium (3), Austria (2), Lithuania (2), Italy (1) | 1 | 82.3 (37–135) | 8.8 | – |
| 2 | Histamine and Scombrotoxin | Fish and fish products f | 24 | Spain (15), Sweden (5), France (4) | 5 | 18.0 (14–23) | 6.5 | ↑ |
| 2 | Salmonella | Mixed food g | 24 | Spain (16), Slovakia (2), Germany (2), Finland (1), France (1), Romania (1), Hungary (1) | 4 | 19.8 (3–27) | 8.0 | – |
| 3 | Salmonella | Pig meat and products thereof h | 18 | Germany (5), France (5), Italy (3), Greece (2), Spain (1), Lithuania (1), Poland (1) | 6 | 17.0 (11–26) | 6.8 | – |
| 4 | Norovirus (and other calicivirus) | Mixed food i | 16 | Spain (5), Finland (4), Denmark (2), Sweden (2), Poland (1), Belgium (1), Germany (1) | 7 | 9.5 (5–13) | 4.5 | ↑↑ |
| 5 | Salmonella | Sweets and chocolate j | 12 | Austria (1), Belgium (1), Czechia (1), Denmark (1), Germany (1), Ireland (1), Italy (1), Luxembourg (1), Netherlands (1), Spain (1), Sweden (1), United Kingdom (Northern Ireland) (1) | 18 | 4.5 (2–8) | 2.3 | ↑↑ |
| 5 | Staphylococcus aureus toxins | Mixed food k | 12 | Spain (3), Portugal (3), Sweden (2), Croatia (2), Germany (1), Romania (1) | 13 | 6.0 (1–12) | 4.3 | ↑↑ |
| 6 | Salmonella | Bakery products l | 11 | Spain (4), Poland (4), Czechia (1), Italy (1), Romania (1) | 3 | 21.3 (9–32) | 3.8 | ↓ |
| 7 | Norovirus (and other calicivirus) | Crustaceans, shellfish, molluscs and products thereof m | 10 | France (4), Spain (2), Denmark (1), Finland (1), Sweden (1), Netherlands (1) | 2 | 58.5 (19–144) | 6.0 | ↓↓ |
| 8 | Campylobacter | Broiler meat (Gallus gallus) and products thereof n | 9 | Denmark (6), France (2), Spain (1) | 11 | 7.8 (4–10) | 5.5 | – |
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Ranking of the food vehicle based on the number of strong‐evidence FBOs in which the combination (causative agent/food vehicle) was implicated (rank 1 is the highest rank meaning the most commonly implicated). Strong‐evidence outbreaks with unknown causative agents are not included.
A single arrow indicates variations of 25% and 50% in the number of outbreaks; double arrows indicate variations > 50%; a ‘stable' value indicates variations of between −25% and + 25%.
In 2022, ‘Eggs and egg products’ include ‘eggs and egg products’ (82), ‘eggs’ (4).
In 2022, ‘Fish and fish products’ include ‘fish and fish products’ (19), ‘fish – fishery products from fish species associated with a high amount of histidine – not enzyme maturated’ (5).
In 2022, ‘Mixed food’ includes ‘mixed food’ (15), ‘other processed food products and prepared dishes – meat based dishes’ (3), ‘other processed food products and prepared dishes’ (1), ‘other processed food products and prepared dishes – fish and seafood based dishes’ (1), ‘other processed food products and prepared dishes – sandwiches’ (1), ‘other processed food products and prepared dishes – sandwiches – with meat’ (1), ‘ready‐to‐eat salads’ (1), ‘sauce and dressings’ (1).
In 2022, ‘Pig meat and products thereof’ includes ‘pig meat and products thereof’ (11), ‘meat from pig – meat products ‐ meat specialities’ (2), ‘cured seasoned pork meat’ (1), ‘meat from pig – fresh’ (1), ‘meat from pig – meat products – fresh raw sausages’ (1), ‘meat from pig – meat products – ready‐to‐eat’ (1), ‘meat from pig – minced meat – intended to be eaten raw’ (1).
In 2022, ‘Mixed food’ includes ‘mixed food’ (9), ‘other processed food products and prepared dishes – sandwiches’ (3), ‘other processed food products and prepared dishes’ (1), ‘other processed food products and prepared dishes – meat based dishes’ (1), ‘other processed food products and prepared dishes – sandwiches – with meat’ (1), ‘ready‐to‐eat salads’ (1).
In 2022, ‘Sweets and chocolate' includes ‘chocolate' (9), ‘sweets and chocolate' (2), ‘confectionery products and pastes – soft candy’ (1).
In 2022, ‘Mixed food’ includes ‘mixed food’ (3), ‘other processed food products and prepared dishes – pasta’ (2), ‘other processed food products and prepared dishes’ (2), ‘other processed food products and prepared dishes – finger food’ (1), ‘other processed food products and prepared dishes – meat based dishes’ (1), ‘other processed food products and prepared dishes – pasta – filled pasta’ (1), ‘other processed food products and prepared dishes – pizza and pizza‐like dishes’ (1), ‘other processed food products and prepared dishes – rice based dishes’ (1).
In 2022, ‘Bakery products’ include ‘bakery products – cakes’ (4), ‘bakery products – desserts – containing raw eggs’ (3), ‘bakery products’ (2), ‘bakery products – desserts – containing raw cream’ (2).
In 2022, ‘Crustaceans, shellfish, molluscs and products thereof’ includes ‘crustaceans, shellfish, molluscs and products thereof’ (6), ‘live bivalve molluscs – oysters’ (4).
In 2022, ‘Broiler meat (Gallus gallus) and products thereof’ includes ‘meat from broilers (Gallus gallus)’ (6), ‘broiler meat (Gallus gallus) and products thereof’ (3).
TABLE 56.
Top‐10 pathogen/food vehicle pairs causing the highest number of cases in strong‐evidence outbreaks in reporting EU MSs, 2022.
| 2022 | 2018–2021 a,b | Evaluation | ||||||
|---|---|---|---|---|---|---|---|---|
| Rank c | Causative agent | Food vehicle | Cases (N) | Reporting MS (N cases) | Rank c | Cases (N/year) (range) | Reporting MS (N/year) | 2022 versus 2018–2021 d |
| 1 | Clostridium perfringens toxins | Other or mixed red meat and products thereof e | 961 | Portugal (950), Finland (8), France (3) | 34 | 55.8 (28–195) | 0.75 | ↑↑ |
| 2 | Salmonella | Eggs and egg products f | 508 | Spain (265), Poland (80), France (78), Slovakia (39), Belgium (25), Italy (9), Austria (8), Lithuania (4) | 1 | 1000.5 (303–1989) | 8.8 | ↓ |
| 3 | Norovirus (and other calicivirus) | Mixed food g | 476 | Spain (200), Denmark (91), Finland (57), Germany (50), Sweden (48), Poland (24), Belgium (6) | 5 | 419.5 (223–735) | 4.5 | – |
| 4 | Staphylococcus aureus toxins | Mixed food h | 466 | Sweden (160), Portugal (136), Spain (78), Croatia (74), Germany (14), Romania (4) | 16 | 126.3 (3–212) | 4.3 | ↑↑ |
| 5 | Clostridium perfringens toxins | Meat and meat products, unspecified | 368 | Spain (368) | 33 | 56.0 (23–142) | 1.8 | ↑↑ |
| 6 | Norovirus (and other calicivirus) | Water i | 309 | Italy (177), Slovenia (94), Sweden (20), Czechia (18) | 4 | 550.0 (8–1089) | 3.0 | ↓ |
| 7 | Salmonella | Pig meat and products thereof j | 294 | France (135), Germany (83), Greece (35), Italy (35), Lithuania (2), Poland (2), Spain (2) | 13 | 209.0 (69–301) | 6.8 | ↑ |
| 8 | Clostridium perfringens toxins | Other food | 266 | Spain (266) | 27 | 67.8 (13–193) | 1.3 | ↑↑ |
| 9 | Salmonella | Mixed food k | 246 | Finland (97), Spain (71), Slovakia (29), Germany (22), Romania (17), Hungary (7), France (3) | 2 | 796.5 (91–1595) | 8.0 | ↓↓ |
| 10 | Norovirus (and other calicivirus) | Buffet meals | 236 | Sweden (138), Denmark (92), Finland (6) | 10 | 227.0 (121–399) | 3.3 | – |
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Ranking of the food vehicle based on the number of cases of illness in strong‐evidence FBOs in which the combination (causative agent/food vehicle) was implicated (rank 1 is the highest rank meaning the most commonly implicated). Strong‐evidence outbreaks with unknown causative agents are not included.
A single arrow indicates variations of 25% and 50% in the number of outbreaks; double arrows indicate variations > 50%; a ‘stable' value indicates variations of between −25% and + 25%.
:In 2022, ‘Other or mixed red meat and products thereof’ includes ‘meat, mixed meat – meat products – ready‐to‐eat’ (950), ‘meat from deer (venison) – meat preparation – intended to be eaten cooked’ (8), ‘other or mixed red meat and products thereof’ (3).
In 2022, ‘Eggs and egg products’ include ‘eggs and egg products’ (469), ‘eggs’ (39).
In 2022, ‘Mixed food’ includes ‘mixed food’ (246), ‘other processed food products and prepared dishes – sandwiches’ (78), ‘other processed food products and prepared dishes – meat based dishes’ (61), ‘other processed food products and prepared dishes’ (50), ‘ready‐to‐eat salads’ (21), ‘other processed food products and prepared dishes – sandwiches – with meat’ (20).
In 2022, ‘Mixed food’ includes ‘other processed food products and prepared dishes – pasta’ (160), ‘mixed food’ (116), ‘other processed food products and prepared dishes’ (113), ‘other processed food products and prepared dishes – rice based dishes’ (32), ‘other processed food products and prepared dishes – finger food’ (23), ‘other processed food products and prepared dishes – meat based dishes’ (14), ‘other processed food products and prepared dishes – pasta – filled pasta’ (4), ‘other processed food products and prepared dishes – pizza and pizza‐like dishes’ (4).
In 2022, ‘Water’ includes ‘tap water, including well water’ (215), ‘water – potable water’ (94).
In 2022, ‘Pig meat and products thereof’ includes ‘pig meat and products thereof’ (188), ‘meat from pig – meat products – meat specialities’ (36), ‘meat from pig – fresh’ (26), ‘meat from pig – minced meat – intended to be eaten raw’ (19), ‘meat from pig – meat products – ready‐to‐eat’ (15), ‘cured seasoned pork meat’ (8), ‘meat from pig – meat products – fresh raw sausages’ (2).
In 2022, ‘Mixed food’ includes ‘other processed food products and prepared dishes – sandwiches – with meat’ (97), ‘mixed food’ (96), ‘other processed food products and prepared dishes – meat based dishes’ (24), ‘other processed food products and prepared dishes – sandwiches’ (12), ‘ready‐to‐eat salads’ (10), ‘other processed food products and prepared dishes’ (3), ‘other processed food products and prepared dishes – fish and seafood based dishes’ (2), ‘sauce and dressings’ (2).
TABLE 57.
Top‐10 pathogen/food vehicle pairs causing the highest number of hospitalisations in strong‐evidence outbreaks in reporting EU MSs, 2022.
| 2022 a | 2018–2021 a,b | Evaluation | ||||||
|---|---|---|---|---|---|---|---|---|
| Rank c | Causative agent | Food vehicle | Hospitalisations (N) | Reporting MS (N hospitalisations) | Rank c | Hospitalisations (N/year) (range) | Reporting MS (N/year) | 2022 versus 2018–2021 d |
| 1 | Salmonella | Eggs and egg products e | 124 | Poland (43), Spain (32), France (22), Slovakia (12), Belgium (9), Austria (4), Italy (2) | 1 | 215.3 (46–382) | 7.0 | ↓ |
| 2 | Listeria monocytogenes | Broiler meat (Gallus gallus) and products thereof f | 97 | Italy (97) | 31 | 4.3 (1–16) | 0.75 | ↑↑ |
| 3 | Listeria monocytogenes | Pig meat and products thereof g | 63 | Italy (43), Denmark (9), Netherlands (7), Austria (3), Hungary (1) h | 22 | 8.8 (6–29) | 0.50 | ↑↑ |
| 4 | Salmonella | Mixed food i | 61 | Romania (17), Spain (15), Finland (12), Slovakia (8), Germany (6), Hungary (2), France (1) | 2 | 96.3 (11–198) | 6.3 | ↓ |
| 5 | Salmonella | Bakery products j | 60 | Romania (37), Poland (9), Italy (7), Spain (4), Czechia (3) | 4 | 65.5 (21–99) | 3.5 | ‐ |
| 6 | Staphylococcus aureus toxins | Mixed food k | 58 | Sweden (38), Portugal (20) | 7 | 30.3 (21–53) | 2.5 | ↑↑ |
| 7 | Salmonella | Pig meat and products thereof l | 57 | Germany (25), Greece (19), France (5), Italy (5), Lithuania (2), Spain (1) | 6 | 42.0 (22–55) | 5.5 | ↑ |
| 8 | Salmonella | Sweets and chocolate m | 56 | Belgium (28), Germany (11), Austria (5), Czechia (4), Ireland (4), Denmark (1), Luxembourg (1), Italy (1), Netherlands (1) | 16 | 13.8 (8–27) | 2.3 | ↑↑ |
| 9 | Salmonella | Bovine meat and products thereof n | 37 | Slovenia (33), Italy (2), Denmark (2) | 34 | 3.5 (0–8) | 1.5 | ↑↑ |
| 10 | Salmonella | Water o | 32 | Netherlands (25), Greece (7) | 46 | 0.50 (0–2) | 0.25 | ↑↑ |
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Ranking of the food vehicle based on the number of hospitalisations in strong‐evidence FBOs in which the combination (causative agent/food vehicle) was implicated (rank 1 is the highest rank meaning the most commonly implicated). Strong‐evidence outbreaks with unknown causative agents are not included.
A single arrow indicates variations of 25% and 50% in the number of outbreaks; double arrows indicate variations > 50%; a ‘stable' value indicates variations of between −25% and + 25%.
In 2022, ‘Eggs and egg products’ include ‘eggs and egg products’ (112), ‘eggs’ (12).
In 2022, ‘Broiler meat (Gallus gallus) and products thereof’ include ‘meat from broilers (Gallus gallus) – meat products’ (97).
In 2022, ‘Pig meat and products thereof’ includes ‘meat from pig – meat products’ (43), ‘meat from pig – meat products – ready‐to‐eat’ (16), ‘meat from pig – meat products – cooked ham’ (3), ‘pig meat and products thereof’ (1).
During the last phase of the production of this draft report, Hungary informed us that the one strong‐evidence outbreak (one hospitalisation) caused by Listeria monocytogenes, with ‘pig meat and products thereof’ as the implicated food vehicle was reported in error.
In 2022, ‘Mixed food’ includes ‘other processed food products and prepared dishes – meat based dishes’ (20), ‘mixed food’ (18), ‘other processed food products and prepared dishes – sandwiches – with meat’ (12), ‘ready‐to‐eat salads’ (6), ‘other processed food products and prepared dishes – fish and seafood based dishes’ (2), ‘sauce and dressings’ (2), ‘other processed food products and prepared dishes’ (1)
In 2022, ‘Bakery products’ include ‘bakery products – cakes’ (41), ‘bakery products – desserts – containing raw eggs’ (11), ‘bakery products – desserts – containing raw cream’ (5), ‘bakery products’ (3).
In 2022, ‘Mixed food’ includes ‘other processed food products and prepared dishes – pasta’ (38), ‘other processed food products and prepared dishes’ (14), ‘other processed food products and prepared dishes – finger food’ (6).
In 2022, ‘Pig meat and products thereof’ includes ‘pig meat and products thereof’ (30), ‘meat from pig – fresh’ (11), ‘meat from pig – meat products – meat specialities’ (9), ‘meat from pig – minced meat – intended to be eaten raw’ (5), ‘cured seasoned pork meat’ (2).
In 2022, ‘Sweets and chocolate' include ‘sweets and chocolate' (28), ‘chocolate' (24), ‘confectionery products and pastes ‐ soft candy’ (4).
In 2022, ‘Bovine meat and products thereof’ includes ‘meat from bovine animals – meat preparation – intended to be eaten raw’ (33), ‘bovine meat and products thereof’ (2), ‘meat from bovine animals – minced meat’ (2).
In 2022, ‘Water’ includes ‘tap water, including well water’ (32).
TABLE 58.
Top‐10 pathogen/food vehicle pairs causing the highest number of deaths in strong‐evidence outbreaks in reporting EU MSs, 2022.
| 2022 a | 2018–2021 a,b | Evaluation | ||||||
|---|---|---|---|---|---|---|---|---|
| Rank c | Causative agent | Food vehicle | Deaths (N) | Reporting MS (N deaths) | Rank c | Deaths (N/year) (range) | Reporting MS (N/year) | 2022 versus 2018–2021 d |
| 1 | Listeria monocytogenes | Broiler meat (Gallus gallus) and products thereof e | 5 | Italy (5) | 3 | 1.8 (0–7) | 0.25 | ↑↑ |
| 1 | Listeria monocytogenes | Vegetables and juices and other products thereof f | 5 | Finland (5) | 5 | 1.3 (0–5) | 0.50 | ↑↑ |
| 1 | Streptococcus equi | Cheese | 5 | Italy (5) | NA | 0 | 0 | NA |
| 2 | Staphylococcus aureus toxins | Eggs and egg products | 3 | Poland (3) | NA | 0 | 0 | NA |
| 2 | Listeria monocytogenes | Pig meat and products thereof g | 3 | Italy (1), Netherlands (1), Hungary (1) h | 3 | 1.8 (0–5) | 0.50 | ↑↑ |
| 3 | Listeria monocytogenes | Dairy products (other than cheeses) | 2 | Austria (2) | NA | 0 | 0 | NA |
| 3 | Listeria monocytogenes | Fish and fish products i | 2 | Austria (2) | 1 | 3.0 (0–8) | 0.75 | ↓ |
| 4 | Listeria monocytogenes | Mixed food j | 1 | Germany (1) | 6 | 1.0 (0–4) | 0.25 | ‐ |
| 4 | Salmonella | Pig meat and products thereof k | 1 | Germany (1) | 8 | 0.50 (0–2) | 0.25 | ↑↑ |
| 4 | Mushroom toxins | Vegetables and juices and other products thereof | 1 | Spain (1) | NA | 0 | 0 | NA |
Abbreviation: NA, Not Applicable.
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Ranking of the food vehicle based on the number of deaths in strong‐evidence FBOs in which the combination (causative agent/food vehicle) was implicated (rank 1 is the highest rank meaning the most commonly implicated). Strong‐evidence outbreaks with unknown causative agents are not included.
A single arrow indicates variations of 25% and 50% in the number of outbreaks; double arrows indicate variations > 50%; a ‘stable' value indicates variations of between −25% and + 25%.
In 2022, ‘Broiler meat (Gallus gallus) and products thereof’ includes ‘meat from broilers (Gallus gallus) ‐ meat products’ (5).
In 2022, ‘Vegetables and juices and other products thereof’ includes ‘vegetables’, ‘vegetables – pre‐cut’ (5).
In 2022, ‘Pig meat and products thereof’ includes ‘meat from pig – meat products’ (1), ‘meat from pig – meat products ‐ ready‐to‐eat’ (1), ‘pig meat and products thereof’ (1).
During the last phase of the production of this draft report, Hungary informed us that the one strong‐evidence outbreak (one death) caused by Listeria monocytogenes, with ‘pig meat and products thereof’ as the implicated food vehicle was reported in error.
In 2022, ‘Fish and fish products’ includes ‘fish – smoked’ (2).
In 2022, ‘Mixed food’ includes ‘ready‐to‐eat salads’ (1).
In 2022, ‘Pig meat and products thereof’ includes ‘meat from pig – fresh’ (1).
Overall, Salmonella ranked among the top positions in the top‐10 classification, paired with either ‘eggs and egg products’, ‘mixed food’ or ‘pig meat and products thereof’, for the number of FBOs, as well as for human cases and hospitalisations. In 2022, for the first time since EFSA began collecting data on FBOs, Salmonella in water entered the top‐10 pairs for the number of hospitalisations.
Clostridium perfringens toxins was the causative agent involving the highest number of human cases, paired with ‘other or mixed red meat and products thereof’, ‘unspecified meat and meat products’ and ‘other food’ products.
L. monocytogenes was the agent causing the highest number of deaths, paired with a wide variety of food vehicles, as shown in Table 58. This is a matter of concern since L. monocytogenes can be responsible for severe infections in humans (i.e. meningitis, sepsis, abortion, etc.), especially among vulnerable and fragile population groups (Schlech, 2019). The rise of listeriosis events associated with the consumption of foods not traditionally considered as vehicles for the transmission of L. monocytogenes is a reason of concern (Desai et al., 2019).
4.4 Overview of the places of exposure in strong‐evidence outbreaks
Information on the places of exposure for strong‐evidence FBOs in the EU in 2022, is available in Table 59. For further details on the places of exposure, for both strong‐ and weak‐evidence outbreaks, see the dashboard on FBOs (here, see page on ‘Places of exposure' for information on FBOs by place of exposure).
TABLE 59.
Frequency distribution of strong‐evidence foodborne outbreaks by place of exposure (setting), in reporting EU, MS, 2022.
| Type of setting | Strong‐evidence outbreaks | Outbreak reporting rate per 100,000 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Outbreaks | Cases | Hospitalisations | Deaths | 2022a | 2018–2021 a,b | |||||
| N | % of total | N | % of total | N | % of total | N | % of total | |||
| Domestic setting | 145 | 29.8 | 698 | 7.1 | 212 | 22.9 | 2 | 6.5 | 0.032 | 0.042 |
| Restaurant, pub, street vendors, takeaway etc. | ||||||||||
| Restaurant or Cafe or Pub or Bar or Hotel or Catering service | 134 | 27.5 | 1764 | 17.9 | 134 | 14.5 | 0 | 0 | 0.030 | 0.026 |
| Takeaway or fast‐food outlet | 8 | 1.6 | 111 | 1.1 | 6 | 0.65 | 0 | 0 | 0.002 | 0.001 |
| Mobile retailer or market/street vendor | 5 | 1.0 | 20 | 0.20 | 3 | 0.32 | 0 | 0 | 0.001 | 0.001 |
| Canteen or catering at workplace, school etc. | ||||||||||
| School or kindergarten | 28 | 5.7 | 1544 | 15.7 | 14 | 1.5 | 0 | 0 | 0.006 | 0.007 |
| Canteen or workplace catering | 9 | 1.8 | 302 | 3.1 | 16 | 1.7 | 0 | 0 | 0.002 | 0.002 |
| Multiple places of exposure | ||||||||||
| Multiple places of exposure in one country | 24 | 4.9 | 884 | 9.0 | 301 | 32.5 | 20 | 64.5 | 0.005 | 0.004 |
| Multiple places of exposure in more than one country | 9 | 1.8 | 148 | 1.5 | 50 | 5.4 | 0 | 0 | 0.002 | 0.001 |
| Health care and residential facilities | ||||||||||
| Residential institution (nursing home or prison or boarding school) | 24 | 4.9 | 937 | 9.5 | 42 | 4.5 | 2 | 6.5 | 0.005 | 0.005 |
| Hospital and medical care facility | 6 | 1.2 | 327 | 3.3 | 18 | 1.9 | 4 | 12.9 | 0.001 | 0.002 |
| Other place of exposure | ||||||||||
| Others c | 25 | 5.1 | 481 | 4.9 | 27 | 2.9 | 1 | 3.2 | 0.006 | 0.006 |
| Camp or picnic | 10 | 2.1 | 146 | 1.5 | 3 | 0.32 | 0 | 0 | 0.002 | 0.002 |
| Temporary mass catering (fairs or festivals) | 5 | 1.0 | 1088 | 11.0 | 56 | 6.0 | 0 | 0 | 0.001 | < 0.001 |
| Unknown | 55 | 11.3 | 1413 | 14.3 | 44 | 4.8 | 2 | 6.5 | 0.012 | 0.005 |
| EU Total | 487 | 100 | 9863 | 100 | 926 | 100 | 31 | 100 | 0.109 | 0.105 |
For the 2021–2022 period, data on FBOs from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
For the 2018–2019 period, data on FBOs from the United Kingdom were taken into account, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
During the last phase of the production of this draft report, Hungary informed us that the one strong‐evidence outbreak (one case, one hospitalisation and one death) with ‘others’ as the place of exposure was reported in error.
In 2022, for the first time since the collection of FBO data began, the number of strong‐evidence FBOs in ‘restaurants, pubs, street vendors, takeaway etc.’ exceeded that of FBOs in a domestic setting. After two consecutive years of decrease of the proportion of FBOs occurring in this setting during the COVID‐19 pandemic, exposure to contaminated food in ‘restaurants, pubs, street vendors, takeaway etc.’ returned in 2022 and even exceeded the levels observed in pre‐pandemic years, with almost one in three strong‐evidence FBOs taking place in these settings (30.2% of all strong‐evidence FBOs). Strong‐evidence FBOs in ‘restaurants, pubs, street vendors, takeaway etc.’ were reported by 15 MSs (Belgium, Croatia, Denmark, Finland, France, Germany, Hungary, Italy, Lithuania, the Netherlands, Poland, Portugal, Romania, Spain and Sweden) and one non‐MS. In particular, ‘restaurant or cafe or pub or bar or hotel or catering service' was the most frequent place of exposure in this group, involving most human cases (Table 59). The number of strong‐evidence FBOs occurring in ‘restaurant or cafe or pub or bar or hotel or catering service' was higher than in 2021 (57 more strong‐evidence FBOs; an increase of 74.0%).
The second most frequently reported place of exposure in strong‐evidence FBOs was ‘domestic premises’, which was identified in 29.8% of all FBOs by 12 MSs (Austria, Belgium, France, Germany, Greece, Italy, Lithuania, Luxembourg, Poland, Romania, Slovakia and Spain) and three non‐MSs. In the EU, the number of strong‐evidence outbreaks occurring on domestic premises was higher than in 2021 (19.8% more strong‐evidence outbreaks) while the number of cases involved in these outbreaks was lower (13.1% fewer cases than in 2021). However, because FBOs taking place on ‘domestic premises’ are frequently ‘household’ outbreaks, and given that not all MSs report this type of FBO to EFSA (see Section 4.1), the importance of ‘domestic premises’ could be underestimated. This finding highlights the need to continue delivering information to consumers on the importance of the correct handling of food in domestic kitchens. It is crucial to highlight the importance of food labels to help consumers follow the instructions for food preparation, consumption and preservation. The relative importance of ‘domestic premises’, however, fell considerably in 2022 (Table 59) compared with previous years. In 2021 and 2020, the proportion of strong‐evidence FBOs occurring in this setting totalled 34.0% and 39.1% of all strong‐evidence FBOs, respectively. In 2019 and 2018, the figure was even higher than 40.0%. Salmonella was the main causative agent involved in strong‐evidence FBOs in both ‘restaurants, pubs, street vendors, takeaway etc.’ and ‘domestic premises’. Other causative agents in ‘restaurants, pubs, street vendors, takeaway etc.’ included Staphylococcus aureus toxins, histamine and scombrotoxin and norovirus (and other calicivirus).
‘Canteen or catering at workplace, school etc.’ (including ‘school or kindergarten’ and ‘canteen or workplace catering’) and ‘health care and residential facilities’ (including ‘residential institution nursing home or prison or boarding school’ and ‘hospital or medical care facility’) were reported as the place of exposure in 37 and 30 FBOs respectively in the EU. ‘School or kindergarten’ ranked second in 2022 after ‘restaurant or cafe or pub or bar or hotel or catering service’ for the number of human cases involved in FBOs (Table 59). FBOs occurring in ‘canteen or catering at workplace, school etc.’ were reported by 11 MSs (Belgium, Croatia, Denmark, Finland, France, Germany, Italy, Portugal, Slovakia, Spain and Sweden) and three non‐MSs. FBOs were mainly caused by norovirus (and other calicivirus), S. aureus toxins, B. cereus toxins and C. perfringens toxins. Bacterial toxins (C. perfringens toxins, S. aureus toxins, B. cereus toxins) and norovirus (and other calicivirus) were also the main causative agents in strong‐evidence FBOs reported in ‘health care and residential facilities’, which were notified to EFSA by 10 MSs (Belgium, Finland, France, Germany, Hungary, Italy, the Netherlands, Poland, Portugal and Spain).
Strong‐evidence FBOs with ‘multiple places of exposure’ in one or multiple countries were reported by 12 MSs (Austria, Belgium, Denmark, Estonia, Finland, Germany, Ireland, Italy, the Netherlands, Slovenia, Spain and Sweden), by the United Kingdom (Northern Ireland) and by one non‐MS. The causative agents most frequently reported were Salmonella and L. monocytogenes.
4.5 Contributing factors in strong‐evidence foodborne outbreaks
Information on the factors contributing to outbreaks was available for 147 FBOs (30.2% of all strong‐evidence FBOs).
‘Unprocessed contaminated ingredient’ was reported in 41 FBOs caused by Salmonella, histamine and scombrotoxin, Campylobacter, norovirus (and other calicivirus), B. cereus toxins, S. aureus toxins, Trichinella, Cryptosporidium, Shiga toxin‐producing E. coli, Aeromonas, Streptococcus and unknown agents. ‘Inadequate chilling’ and ‘inadequate heat treatment’ (22 FBOs each) were reported in strong‐evidence FBOs mainly caused by Salmonella, Clostridium perfringens, ‘histamine and scombrotoxin’ (only for inadequate chilling) and flavivirus (Tick‐borne Encephalitis virus, only for inadequate chilling). ‘Time storage/temperature abuse’ was reported in 19 strong‐evidence FBOs mainly caused by ‘bacterial toxins’ and ‘Salmonella’. ‘Cross‐contamination’ was reported in 15 strong‐evidence FBOs caused by Salmonella, norovirus (and other calicivirus), S. aureus, L. monocytogenes and Vibrio parahaemolyticus. The main causative agent of strong‐evidence FBOs with the contributing factor of ‘infected food handler’ (N = 41) were ‘norovirus (and other calicivirus)’ and S. aureus toxins. Lastly, ‘water treatment failure’ and ‘untreated drinking water’ were reported in three strong‐evidence waterborne outbreaks. ‘Norovirus (and other calicivirus)’ and ‘E. coli other than STEC’ were the associated causative agents.
See the EFSA story map on FBOs (here), section on ‘How, why and where food contamination may occur’.
4.6 Temporal trends by causative agents
4.6.1 Temporal trends at EU level
Figure 23 describes the number of FBOs reported in the EU over the period 2013–2022, by causative agent. Given that the collection of FBO data is not fully harmonised across the EU, and that changes in the surveillance of FBOs by MSs may have taken place over time, annual variations in the frequency distribution of the causative agents shown in Figure 23 may not necessarily reflect the true epidemiological pattern at EU level.
FIGURE 23.
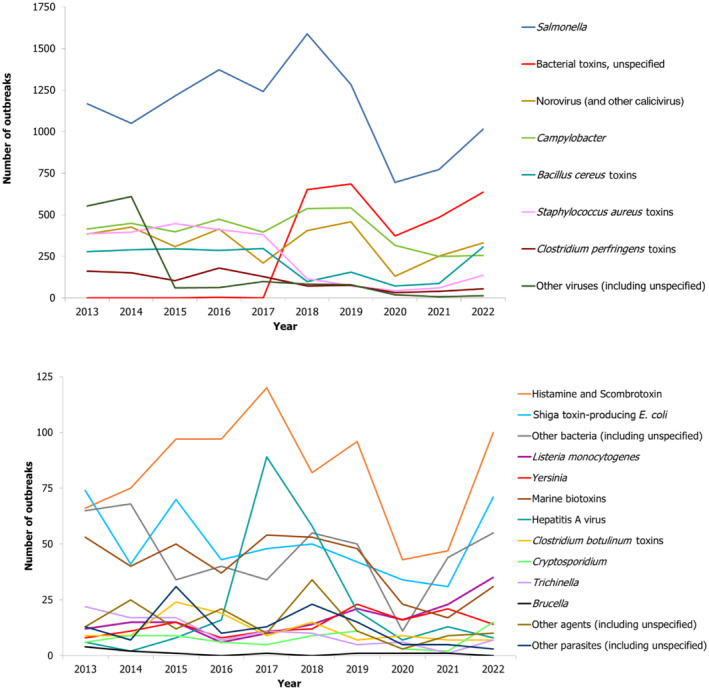
Number of foodborne outbreaks by causative agent, reported to the EU by MSs, 2013–2022. Note: Outbreaks reported by the United Kingdom are included for the 2013–2019 period. However, data from the United Kingdom (Northern Ireland) are taken into account for the 2021–2022 period. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, EU requirements on data sampling are also applicable to Northern Ireland. During the last phase of the production of this draft report, Hungary informed us that the one strong‐evidence outbreak caused by Listeria monocytogenes was reported in error. ‘Marine biotoxins’ include ciguatoxin, muscle‐paralysing toxin, okadaic acid and unspecified marine biotoxins. ‘Norovirus (and other calicivirus)’ include norovirus (Norwalk‐like virus), sapovirus (Sapporo‐like virus) and unspecified calicivirus. ‘Other bacteria (incl. unspecified)’ include Aeromonas, Arcobacter, Cronobacter sakazakii, E. coli other than STEC, Enterococcus, Francisella, Leptospira, Shigella, Streptococcus, Vibrio cholerae (non‐toxigenic), Vibrio parahaemolyticus and other unspecified bacteria. ‘Other parasites (incl. unspecified)’ include Anisakis, Cysticerci, Enterocytozoon bieneusi, Giardia and other unspecified parasites. ‘Other viruses (incl. unspecified)’ include Adenovirus, Enterovirus, Flavivirus (incl. Tick‐borne Encephalitis virus), Hepatitis E virus, unspecified Hepatitis virus, Rotavirus and other unspecified virus. ‘Other agents (incl. unspecified)’ include atropine, chemical agents, lectins, monosodium glutamate, mushroom toxins, mycotoxins, unspecified toxins and wax esters (from fish).
For a further interactive look at FBO data, see the dashboard on FBOs (here), see the dedicated dashboard page on temporal trends.
4.6.2 Temporal country‐specific trends by causative agent, 2013–2022
This paragraph focuses only on statistically significant trends, by causative agent and country. More information can be found on the dashboard (here), see the dedicated dashboard page on temporal trends.
The trend analysis for Salmonella FBOs was carried out for 22 MSs and two non‐MSs with complete data reporting between 2013 and 2022. The statistical test highlighted a significantly decreasing trend in the number of FBOs for six MSs (Austria, Croatia, Czechia, Germany, Latvia and Lithuania), i.e. three more countries than in 2021. For all these MSs, the decrease was mainly attributable to a gradual fall in S. Enteritidis, where the trend was also statistically significant. In Austria, a significant decrease in the number of FBOs caused by S. Typhimurium and monophasic S. Typhimurium also contributed to the generally favourable trend of falling numbers of Salmonella FBOs.
Trend testing on FBOs caused by S. Enteritidis also showed a considerable decrease in Hungary. No statistically significant trends were detected for the other MSs in FBO data reporting between 2013 and 2022 for S. Enteritidis, S. Typhimurium and monophasic S. Typhimurium.
These findings could be due to the successful implementation of National Control Programmes (NCP) for Salmonella in poultry (more information is available in the Section 2.4.4. (Salmonella in animals) of the Salmonella chapter).
Concerning Campylobacter , the temporal trend in FBOs was tested for 14 MSs and one non‐MS. In Austria, FBOs have fallen considerably over the last 10 years, while in France, figures followed an increasing trend over the same period. No other statistically significant trend was observed for FBOs caused by bacterial agents.
In France, a statistically significantly decreasing trend was observed for FBOs caused by C. perfringens toxins and S. aureus toxins, as well as for marine biotoxins.
Concerning parasites, trend in the number of Trichinella FBOs was tested in Romania, and showed a statistically significant fall over the period 2013–2022.
Trends in FBOs caused by norovirus (and other calicivirus) were analysed in 11 MSs and 1 non‐MS with no significant results.
Lastly, a statistically significantly increasing trend in the number of FBOs caused by unknown agents was highlighted for the Netherlands and Switzerland, while for Sweden and Norway a statistically significantly decreasing trend was assessed. Differences among countries relating to increasing or decreasing trends in FBOs caused by unknown agents may be due to changes in the sensitivity of outbreak surveillance, as well as changes in laboratory sample testing and subtyping. More information on the FBOs caused by unknown or unspecified causative agents is available in Section 4.2.6.
4.6.3 Temporal trends by implicated food vehicle, 2013–2022
Only strong‐evidence outbreaks were considered for the trend analysis by implicated food vehicle at country level. Few statistically significantly decreasing trends were detected for food vehicles over the 2013–2022 period while no increasing trends were observed for any food vehicle.
France, Germany and Spain reported a decreasing trend in FBOs associated with the consumption of ‘fish and fish products’. In France, this fall was mainly linked to a statistically significant reduction in the number of FBOs caused by ‘histamine and scombrotoxin’. Other statistically significantly decreasing trends were observed in Portugal and Romania for FBOs implicating ‘mixed food’ and ‘pig meat’, respectively. In both countries, the number of strong‐evidence FBOs associated with these foodstuffs was small (less than 10 per year) as was the range of annual variations.
Information on the number of strong‐evidence outbreaks, by food vehicle, over the period 2016–2022 can be viewed on the dashboard (here). More information on the number of strong‐evidence outbreaks and the outbreak reporting rate (for 100,000 population) by food vehicle is available on the dashboard (here, see page ‘on food vehicle’).
Figures describing statistically significant temporal trends in the number of outbreaks, both by causative agent and MS and by food vehicle and MS, are available as downloadable files from the EFSA knowledge junction at the Zenodo general‐purpose open‐access repository here.
4.7 Waterborne outbreaks
In 2022, 41 waterborne outbreaks were reported by 13 MSs (Austria, Belgium, Croatia, Czechia, France, Greece, Ireland, Italy, the Netherlands, Portugal, Slovenia, Spain and Sweden) and three by two non‐MSs (Norway and Switzerland). In the EU, these outbreaks involved a total of 1958 human cases and 50 hospitalisations. No deaths were reported.
Among the FBOs observed in the EU, 13 were considered strong‐evidence and included outbreaks caused by ‘tap water, including well water’, ‘water’ and ‘potable water’. Interestingly, the reporting of strong‐evidence FBOs in the EU increased by 333.3% in 2022 compared with 2021 (10 more FBOs in 2022). The causative agents involved in these outbreaks were Campylobacter (including C. jejuni and unspecified Campylobacter), C. perfringens, Hepatitis A virus, E. coli other than STEC (including Enteroaggregative E. coli (EAEC), Enterotoxigenic E. coli (ETEC) and unspecified E. coli), norovirus and Salmonella (including S. Bovismorbificans and S. Typhi). Italy reported the largest strong‐evidence outbreak caused by ‘tap water, including well water’. The outbreak was caused by norovirus and involved 177 human cases in multiple places of exposure. No hospitalisations were reported.
Another general waterborne outbreak in Greece occurred in a domestic setting. It was associated with S. Bovismorbificans and involved 33 human cases and seven hospitalisations. The source of the problem was the water distribution system.
In 2022, two MSs (the Netherlands and Ireland) reported FBOs caused by S. Typhi linked with ‘Tap water, including well water’ (one strong‐ and one weak‐evidence outbreak). A total of 74 human cases were involved, mainly due to the large strong‐evidence FBO reported by the Netherlands, which alone caused 72 human cases and 25 hospitalisations. This outbreak occurred in an asylum centre located on a ship and was caused by the consumption of contaminated tap water. The contamination was probably due to a leak of the sewage tank into the water tank, since the two were adjacent.
4.8 ECDC and EFSA rapid outbreak assessment (ROA)
The joint collaboration between EFSA and ECDC led to the publication of different rapid outbreak assessment (ROA) reports of multi‐country foodborne outbreaks occurring in 2022. All assessments concerned multi‐country outbreaks caused by various Salmonella serotypes.
The first ROA and its following update described an outbreak of salmonellosis caused by two distinct strains of monophasic Salmonella Typhimurium sequence type 34. This outbreak evolved rapidly between December 2021 and May 2022, and was characterised by the presence of two clusters involving a total of 324 cases, mainly children ≤ 10 years, in 12 EU/EEA countries (Austria, Belgium, Denmark, France, Germany, Ireland, Italy, Luxembourg, the Netherlands, Norway, Spain, Sweden), the United Kingdom, Switzerland, Canada and the United States. A high hospitalisation rate (around 40.0% of cases) was reported but no deaths. Epidemiological and microbiological investigations identified chocolate products produced by a Belgian factory as the vehicle of the infections. A significant fall in cases was observed following the implementation of rigorous control measures, including the closure of the Belgian processing plant and the global recalls and withdrawals of all chocolate products produced by the Belgian factory (ECDC and EFSA, 2022a, 2022b).
A second outbreak caused by Salmonella Mbandaka ST413 occurred over the period 2021–2022, causing 196 cases in seven EU/EEA countries (Czechia, Estonia, Finland, France, Germany, Ireland, the Netherlands), the United Kingdom and Israel. In addition, 19 hospitalisations and one death were also attributed to this outbreak. Information from the case interviews in Finland and the United Kingdom pointed to ready‐to‐eat chicken products and/or fresh chicken meat as the probable vehicle of infection. Based on the epidemiological data and the whole genome sequencing (WGS) analysis of human isolates, multiple active sources of infection were hypothesised with a likely common source higher up in the chicken supply chain. However, at the date of publication of this ROA, no source(s) of infection could be identified, with a probable risk that the outbreak could have involved new cases of infections (ECDC and EFSA, 2022c).
Salmonella Virchow ST16 was the causative agent responsible for a persistent cross‐border outbreak involving five EU countries (Denmark, France, Germany, Ireland and the Netherlands), the United Kingdom and the United States. Cases were also reported in 2022, although clinical isolates matching the outbreak strain (N = 210) were identified continuously between 2017 and 2023, following the notification of a cluster of 52 cases in the European Surveillance portal of infectious disease (EpiPulse) by France in 2022. No deaths were reported. Information from the case interviews, food traceability investigation and WGS cluster analysis identified kebab products containing chicken meat as the likely source of infection. However, since the batch numbers of the food products implicated in the outbreak and the related microbiological evidence were not available, a common source of infection could not be established (ECDC and EFSA, 2023a).
5 CONCLUSIONS
5.1 Health impact, causative agents and trends
In 2022, the number of FBOs reported at EU level was higher than in 2021 and higher than the mean annual number over the 2018–2021 period. This increase could be explained primarily by a resurgence in the occurrence of outbreaks and cases to the level of pre‐pandemic years in most MSs. A similar increasing pattern was also observed for the number of reported human cases.
During 2022, which was the third year of the COVID‐19 pandemic, many countries still had measures in place to control the spread of the virus, even though these were less restrictive than in the first 2 years of the pandemic. In particular, policies based on individual measures (e.g. vaccination) were gradually put in place and, at the same time, non‐pharmaceutical and restrictive rules (e.g. school closure, suspension of restaurant and catering services) were lifted for the most part. These changes may have favoured a return to the societal and individual lifestyles and behaviours of pre‐pandemic years, with respect to food consumption habits, travelling etc., with possible consequences on human exposure to zoonotic agents, including foodborne pathogens.
One major finding related to the increased health impact of FBOs in 2022, with the rise in the number of hospitalisations and deaths. A total of 64 deaths were reported, one of the highest values reported for the EU in the last 10 years.
As observed in previous years, bacteria again caused the highest number of FBOs, hospitalisations and deaths. In general, the pattern of causative agents implicated in FBOs in 2022 was similar to previous years. Salmonella had by far the biggest direct impact on health, in terms of the number of outbreaks and hospitalisations, despite the increase in the number of MSs reporting statistically decreasing trends in Salmonella FBOs over the 2013–2022 period. Almost all MSs (N = 25), the United Kingdom (Northern Ireland) and three non‐MSs reported outbreaks caused by Salmonella, and for 14 MSs, the United Kingdom (Northern Ireland) and one non‐MS Salmonella was the main causative agent of FBOs. At EU level, S. Enteritidis and S. Typhimurium were the predominant serovars.
For other MSs, the main reported causative agents were different, with either norovirus, unspecified bacterial toxins, Campylobacter, S. aureus toxins or Shiga toxin‐producing E. coli being the most frequently reported causative agents identified in FBOs. These variations may be explained not only by an actual epidemiological difference, but also by differences and peculiarities in the structure, scope and methods of FBO surveillance in place in each country.
Norovirus (and other calicivirus) was the agent with the highest impact in terms of the number of human cases. This finding has also been observed in past years (2012, 2015, 2016, 2019), and is closely related to the specific epidemiology of this viral agent, which is epidemic in nature and liable to cause very large community‐wide outbreaks. In fact, many FBOs caused by norovirus and involving more than 100 human cases were reported by several countries in 2022.
In 2022, one critical finding emerging from the analysis of FBO data related to the high numbers of FBOs, hospitalisations and deaths caused by L. monocytogenes in the EU, the highest ever reported to EFSA since it first began collecting FBO data in 2004. This increase is a matter of concern since this pathogen is associated with a high rate of hospitalisations and deaths, along with severe health consequences for the most vulnerable population subgroups. Septicaemia and cerebral conditions (i.e. meningitis, meningoencephalitis) are life‐threatening conditions occurring mainly in elderly people and immunocompromised individuals, while listeriosis in pregnant women may lead to spontaneous abortion, still birth or foetal death (Doganay, 2003) (Lamont et al., 2011).
Another reason for concern is that the reported listeriosis outbreaks were associated with a wide variety of food vehicles, even some that are not traditionally considered probable vehicles of infection, as has also been observed in the literature. The food vehicles linked with FBOs caused by L. monocytogenes included, among others, meat and meat products, fish and fish products, mixed food and multi‐ingredients foods, dairy products and vegetables (Desai et al., 2019; Koopmans et al., 2023). Buchanan et al. (2017) also stated that despite the success observed in some regions in reducing the prevalence of L. monocytogenes in a few food products, no decrease was observed in the number of invasive listeriosis outbreaks, which even increased in some cases. Some of the reasons behind the increase in the reporting of listeriosis outbreaks may be related to either changes in the food production system (Ercsey‐Ravasz et al., 2012), globalisation or the increased consumption of RTE products (Keto‐Timonen et al., 2007) (Desai et al., 2019). In addition, the widespread implementation of whole genome sequencing (WGS) may have played an important role in this increase. WGS has considerably improved the early detection of listeriosis infections and made it possible to link sporadic cases with different food products and geographical regions (EFSA BIOHAZ Panel et al., 2019). It is crucial to continue raising awareness among food business operators and the most vulnerable population subgroups on the risks associated with foodborne exposure and the negative health consequences of L. monocytogenes, in order to adopt better control measures and reduce the incidence of listeriosis cases.
Lastly, in 2022, a severe strong‐evidence outbreak caused by Streptococcus equi subspecies zooepidemicus was reported to EFSA for the first time since it began collecting data. The FBO was caused by the consumption of unpasteurised cheese made from dairy milk. This event raised attention around the zoonotic potential of this pathogen, which should not be underestimated.
5.2 Food vehicles and places of exposure
In 2022, the food category ‘composite foods, multi‐ingredient foods and other foods’ was reported more frequently than in 2021, and was responsible for the highest number of FBOs. This increase is noteworthy since the production and consumption of processed food is continuously increasing among the population (Monteiro et al., 2013). Within this food category, the consumption of ‘mixed food’ was reported as the cause of the highest number of human cases and hospitalisations in 2022. Since ‘mixed foods’ are usually prepared with multiple ingredients, it may be difficult in outbreak investigations to identify the primary source of contamination.
‘Eggs and egg products’ remained the most frequently implicated vehicle for most strong‐evidence FBOs and, paired with Salmonella, ranked in the top‐10 for the number of FBOs, human cases and hospitalisations. Interestingly, in 2022, the reporting of ‘vegetables and juices and other products thereof’ in strong‐evidence outbreaks decreased compared with 2021. However, pre‐cut vegetables and other items belonging to this food group were responsible for a high number of deaths in two outbreaks, associated with the consumption of vegetables contaminated with L. monocytogenes.
One noteworthy finding observed in 2022 was the frequent reporting of strong‐evidence FBOs in ‘restaurants, pubs, street vendors, takeaway etc.’, which outnumbered those occurring in ‘domestic settings’, for the first time since the collection of FBO data began in 2004. In addition, the number of FBOs occurring in ‘restaurants, pubs, street vendors, takeaway etc.’ in 2022 was not only higher than in 2021, but even higher than in pre‐pandemic years. This finding may be explained by the easing of COVID‐19 control measures, with the gradual reopening of restaurants and catering services. Although the relative importance of ‘domestic premises’ as the place of exposure in strong‐evidence FBOs was lower than during the 2018–2021 period, the number of strong‐evidence FBOs occurring in this setting increased in 2022. These findings highlighted the importance of raising public awareness and perceptions of the risks posed by handling and eating food at home, while also seeking to promote food‐safety education programmes in domestic kitchens, as in the WHO Five Keys campaign. 50
Outbreaks occurring in both ‘canteen or catering at workplace, school etc.’ and ‘health care and residential facilities’ were caused by bacterial toxins, mainly ‘Staphylococcus aureus toxins’ and ‘Clostridium perfringens toxins’, and by viruses, mainly or only ‘norovirus (and other calicivirus)’. The contamination of foods by these pathogens can occur in different phases of the food production chain. While various factors may contribute to the contamination of food with bacterial toxins, mainly incorrect temperatures and storage times, the presence of viruses in food and water is the result of contamination with sewage, poor hygiene or contact with infected food handlers. This finding underlines the importance of strengthening hygiene standards and HACCP protocols in the food production chain, and disseminating knowledge for food handlers.
Interestingly, strong‐evidence FBOs occurring in ‘multiple places of exposure’ in one or more countries were associated with the highest number of deaths, caused mainly by L. monocytogenes and Streptococcus equi subspecies zooepidemicus. Among the FBOs with multiple places of exposure, it is worth mentioning the severe multi‐country outbreak caused by the consumption of chocolate products contaminated with monophasic S. Typhimurium, an outbreak that mainly involved children.
In conclusion, foodborne diseases still represent a public health threat that may raise a number of challenges in relation to the future expansion of vulnerable subgroups in the European population, leading to more severe illness outcomes (European Commission, Eurostat, Corselli‐Nordblad, & Strandell, 2020). In addition, globalisation, population movements and changes in consumption habits may also expose the population to pathogens and lead to foodborne outbreaks (WHO, 2008) (Adinolfi et al., 2016).
ZOONOSES MONITORED ACCORDING THE EPIDEMIOLOGICAL SITUATION (DIRECTIVE 2003/99 LIST B)
1 YERSINIA
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
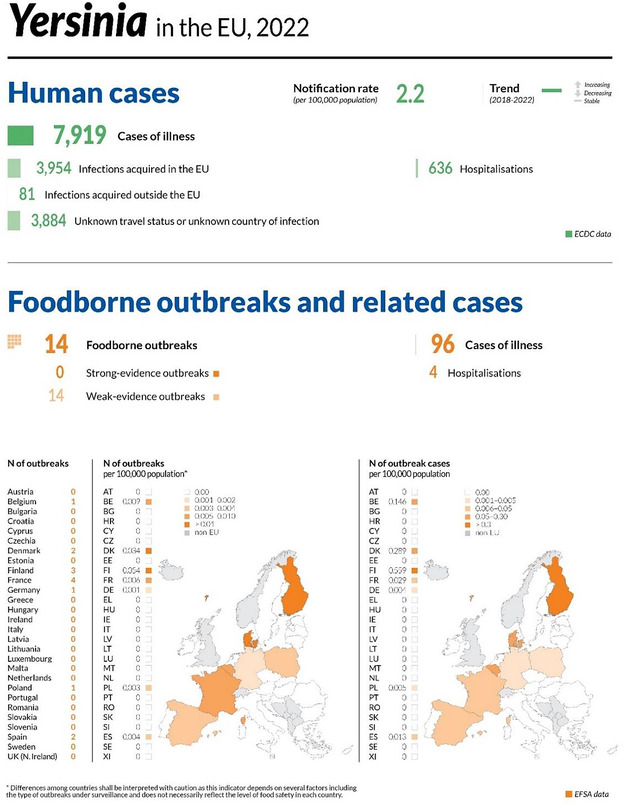
1.1 Key facts
Yersiniosis was the third most commonly reported foodborne gastrointestinal infection in humans in the European Union.
In 2022, there were 7919 confirmed cases of human yersiniosis, corresponding to an European Union notification rate of 2.2 cases per 100,000 population. This was an increase of 16.3% compared with 2021 (1.8 per 100,000 population).
The overall trend for Yersinia infection did not show a statistically significant increase or decrease in the 2018–2022 period.
In 2022, Yersinia enterocolitica was the species reported in the majority (98.7%) of human cases, while Yersinia pseudotuberculosis was notified in only 1.3% of human cases for which the information on Yersinia species was available.
In 2022, none of 328 ‘ready‐to‐eat’ food sampling units reported by four Member States were positive for Yersinia. Of 404 ‘non‐RTE’ ‘non‐ready‐to‐eat’ sampling units reported by three Member States, 3.5% were positive, with the highest level of contamination (3.5%) in ‘meat and meat products’. Yersinia was isolated from some fresh meat categories, with meat from pigs showing the highest percentage of Yersinia‐positive sampling units, 7.8%.
In 2022, Yersinia were detected by five Member States and one non‐Member States in more than eight different animal categories, which overall include more than 30 animal species. The majority of the units tested in the European Union (N = 15,764) were from cattle and the proportion of positives was 0.34% for Y. enterocolitica and 0.32% for Y. pseudotuberculosis. The proportions of positive sampling units from small ruminants, pigs and ‘Pet animals’ were 0.50%, 0.20% and 0.10%, respectively for Y. enterocolitica and 0.29%, 0.00% and 0.31%, respectively for Y. pseudotuberculosis.
1.2 Surveillance and monitoring of Yersinia in the EU
1.2.1 Humans
For 2022, 25 MSs reported information on yersiniosis in humans. Surveillance of yersiniosis is mandatory in 22 MSs. In four MSs (Belgium, France, Greece and Italy) notification is based on a voluntary system. No yersiniosis surveillance system is in place in the Netherlands. The EU case definition was used by 21 MSs, five MSs used a different case definition for reporting (Denmark, France, Germany, Greece and Italy). All MSs, except two (Greece and Italy) had a comprehensive surveillance system. The yersiniosis surveillance system covers the whole population in all MSs except France, Italy and Spain. The estimated coverage of the surveillance system is 91% in Spain. This estimated proportion of population coverage was used in the calculation of notification rates for this MS, whereas for 2018–2020, the rate could not be calculated as no information on coverage was provided. No population coverage estimates were provided for France and Italy, so no notification rates were calculated for these two MSs in any year. All countries reported case‐based data, except Bulgaria and Greece, which reported aggregated data.
1.2.2 Food and animals
Although it is not mandatory to report the presence of Yersinia in food and animals, MSs can report monitoring data on Yersinia to EFSA, in accordance with the Zoonoses Directive (Directive 2003/99/EC). The directive specifies that, in addition to the zoonoses and zoonotic agents for which monitoring is mandatory, zoonoses such as yersiniosis and agents thereof must also be monitored according to the epidemiological situation.
At present, no harmonised Yersinia monitoring plan is in place for food or animals in the EU. Therefore, data on Yersinia in food and animals submitted to EFSA by the MSs are not harmonised. Nevertheless, an EFSA Scientific Opinion recommends the most optimal monitoring methods for Y. enterocolitica and Y. pseudotuberculosis in foodstuffs and animal populations from a public health perspective (EFSA, 2007), whereas harmonised monitoring and reporting criteria for Y. enterocolitica in slaughter pigs were recommended in an EFSA scientific report (EFSA, 2009b).
Monitoring data submitted by MSs for Yersinia in food and animals allow for descriptive summary statistics at the EU level only, and do not support trend analyses and trend watching (Table 1. Consequently, the reported occurrence of Yersinia in major food categories for the year 2022 and for the 4‐year period 2018–2021 was summarised descriptively, making a distinction between ‘ready‐to‐eat' (RTE) and non‐RTE foods. Only results obtained from sampling units collected and tested for Yersinia under an ‘objective sampling’ strategy were considered, in order to limit selection bias. Objective sampling means that MSs collected and tested the samples according to a planned strategy based on a random sampling design representative of the population under study.
1.3 Results
1.3.1 Overview of key statistics, EU, 2018–2022
Table 60 summarises EU‐level statistics on human yersiniosis, and on the occurrence of Yersinia in food and animals, for the period 2018–2022. Although yersiniosis was the third most frequently reported foodborne gastrointestinal infection in humans in the EU in 2022, data on Yersinia in food and animals continue to be reported by few MSs, like in previous years. More detailed descriptions of these statistics are provided in the below subsections and in the chapter on foodborne outbreaks.
TABLE 60.
Summary of Yersinia statistics relating to humans, major food categories and the main animal species, EU, 2018–2022.
| 2022(a) | 2021(a) | 2020 | 2019 b | 2018 b | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 7919 | 7009 | 5737 | 6967 | 7015 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 2.2 | 1.8 | 1.7 | 1.7 | 1.7 | ECDC |
| Number of reporting MSs | 25 | 26 | 26 | 27 | 27 | ECDC |
| Infection acquired in the EU | 3954 | 3548 | 2745 | 3468 | 3446 | ECDC |
| Infection acquired outside the EU | 81 | 18 | 61 | 96 | 106 | ECDC |
| Unknown travel status or unknown country of infection | 3884 | 3443 | 2931 | 3403 | 3463 | ECDC |
| Number of foodborne outbreak‐related cases | 96 | 125 | 236 | 160 | 58 | EFSA |
| Total number of foodborne outbreaks | 14 | 21 | 16 | 23 | 12 | EFSA |
| Food c | ||||||
| Meat and meat products | ||||||
| Number of sampling units | 1640 | 1789 | 1597 | 2304 | 1470 | EFSA |
| Number of reporting MSs | 4 | 6 | 6 | 6 | 6 | EFSA |
| Fruits and vegetable products | ||||||
| Number of sampling units | 69 | 142 | 256 | 17 | 7 | EFSA |
| Number of reporting MSs | 3 | 3 | 4 | 2 | 2 | EFSA |
| Animals d | ||||||
| Cattle (bovine animals) | ||||||
| Number of sampling units | 15,764 | 19,218 | 14,796 | 16,885 | 13,101 | EFSA |
| Number of reporting MSs | 4 | 5 | 5 | 4 | 5 | EFSA |
| Pigs | ||||||
| Number of sampling units | 2010 | 2164 | 2368 | 2591 | 2347 | EFSA |
| Number of reporting MSs | 3 | 5 | 4 | 5 | 6 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
For the 2021–2022 period, data on animal samples from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Number of sampling units was obtained by totalling all sampling units (single, batch and slaughter batch), sampling stages (border control posts, canteen or workplace catering, catering, cutting plant, farm, household, manufacturing, mobile retailer or market/street vendor, processing plant, restaurant or cafe or pub or bar or hotel or catering service, retail, slaughterhouse, unspecified and wholesale), sampling strategies (objective sampling, selective sampling and suspect sampling) and samplers (HACCP and own check and official sampling).
Number of sampling units was obtained by totalling all sampling units (animals and herds), sampling stages at primary production (farm, household, natural habitat, veterinary activities, veterinary clinics and zoo), sampling strategies (convenience sampling, objective sampling and suspect sampling) and samplers (HACCP and own check, industry sampling, official sampling and private sampling).
1.3.2 Human yersiniosis
In 2022, 7919 confirmed cases of yersiniosis were reported by 25 MSs. The notification rate of confirmed yersiniosis cases in the EU was 2.2 cases per 100,000 population. This was an increase of 16.3% compared with 2021 (1.8 per 100,000 population). As in recent years, Germany accounted for the highest number of cases, followed by France (Table 61). Cases reported by these two countries together accounted for 42.6% of all confirmed yersiniosis cases in the EU. As in the previous year, the highest notification rates in 2022 were reported by Denmark (12.7 cases per 100,000 population) and Finland (7.4 cases per 100,000 population). The lowest rates in 2022 were observed in Romania, Greece, Cyprus, Bulgaria, Ireland, Portugal, Poland and Hungary (≤ 0.62 per 100,000) (Table 61).
TABLE 61.
Reported confirmed human cases of yersiniosis and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 131 | 1.5 | 138 | 1.5 | 128 | 1.4 | 112 | 1.3 | 136 | 1.5 |
| Belgium | Y | C | 357 | 3.1 | 329 | 2.8 | 336 | 2.9 | 406 | 3.5 | 392 | 3.4 |
| Bulgaria | Y | A | 8 | 0.12 | 5 | 0.07 | 4 | 0.06 | 11 | 0.16 | 9 | 0.13 |
| Croatia | Y | C | – | – | 12 | 0.30 | 11 | 0.27 | 12 | 0.29 | 20 | 0.49 |
| Cyprus | Y | C | 1 | 0.11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | Y | C | 525 | 5.0 | 456 | 4.3 | 437 | 4.1 | 618 | 5.8 | 622 | 5.9 |
| Denmark | Y | C | 746 | 12.7 | 453 | 7.8 | 413 | 7.1 | 221 | 3.8 | 282 | 4.9 |
| Estonia | Y | C | 53 | 4.0 | 45 | 3.4 | 44 | 3.3 | 42 | 3.2 | 63 | 4.8 |
| Finland | Y | C | 408 | 7.4 | 331 | 6.0 | 386 | 7.0 | 406 | 7.4 | 529 | 9.6 |
| France b | N | C | 1558 | – | 1451 | – | 988 | – | 1135 | – | 929 | – |
| Germany | Y | C | 1814 | 2.2 | 1912 | 2.3 | 1860 | 2.2 | 2164 | 2.6 | 2193 | 2.6 |
| Greece | Y | A | 9 | 0.09 | 7 | 0.07 | 3 | 0.03 | 13 | 0.12 | 21 | 0.20 |
| Hungary | Y | C | 60 | 0.62 | 50 | 0.51 | 25 | 0.26 | 38 | 0.39 | 36 | 0.37 |
| Ireland | Y | C | 17 | 0.34 | 19 | 0.38 | 13 | 0.26 | 9 | 0.18 | 8 | 0.17 |
| Italy b | N | C | 36 | – | 35 | – | 21 | – | 12 | – | 14 | – |
| Latvia | Y | C | 76 | 4.1 | 83 | 4.4 | 88 | 4.6 | 60 | 3.1 | 68 | 3.5 |
| Lithuania | Y | C | 114 | 4.1 | 153 | 5.5 | 123 | 4.4 | 181 | 6.5 | 139 | 4.9 |
| Luxembourg | Y | C | 35 | 5.4 | 12 | 1.9 | 26 | 4.2 | 18 | 2.9 | 16 | 2.7 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands c | – | – | – | – | – | – | – | – | – | – | – | – |
| Poland | Y | C | 180 | 0.48 | 142 | 0.38 | 90 | 0.24 | 196 | 0.52 | 170 | 0.45 |
| Portugal | Y | C | 36 | 0.35 | 34 | 0.33 | 25 | 0.24 | 29 | 0.28 | 30 | 0.29 |
| Romania | Y | C | 14 | 0.07 | 15 | 0.08 | 6 | 0.03 | 36 | 0.19 | 22 | 0.11 |
| Slovakia | Y | C | 287 | 5.3 | 213 | 3.9 | 168 | 3.1 | 255 | 4.7 | 259 | 4.8 |
| Slovenia | Y | C | 54 | 2.6 | 50 | 2.4 | 26 | 1.2 | 28 | 1.3 | 32 | 1.5 |
| Spain d | N | C | 1162 | 2.7 | 754 | 1.7 | 296 | – | 409 | – | 549 | – |
| Sweden | Y | C | 238 | 2.3 | 310 | 3.0 | 220 | 2.1 | 393 | 3.8 | 278 | 2.7 |
| EU Total 27 | – | – | 7919 | 2.2 | 7009 | 1.8 | 5737 | 1.7 | 6804 | 2.1 | 6817 | 2.1 |
| United Kingdom | – | – | – | – | – | – | – | – | 163 | 0.24 | 198 | 0.30 |
| EU Total e | – | – | 7919 | 2.2 | 7009 | 1.8 | 5737 | 1.7 | 6967 | 1.7 | 7015 | 1.7 |
| Iceland | Y | C | 1 | 0.27 | 4 | 1.1 | 3 | 0.82 | 2 | 0.56 | 2 | 0.57 |
| Norway | Y | C | 117 | 2.2 | 85 | 1.6 | 83 | 1.5 | 85 | 1.6 | 105 | 2.0 |
| Liechtenstein c | – | – | – | – | – | – | – | – | – | – | – | – |
| Switzerland c | – | – | – | – | ||||||||
Abbreviations: MSs, Member States; –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Sentinel surveillance; no information on estimated coverage. Notification rate not estimated.
No surveillance system.
Sentinel system; notification rates calculated with an estimated population coverage of 91% in 2021–2022. No information on estimated coverage in 2018–2020, so notification rate cannot be estimated.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
For most (98.0%) of the reported yersiniosis cases of known origin, the infection was acquired in the EU (Table 60) as compared with 99.5% in 2021 and an average of 97.3% in the period 2018–2020. Fifteen countries reported data on imported cases. The proportion of domestic cases with known data was above 90% in all reporting countries, except for five MSs that reported the highest proportion of travel‐associated cases: Luxembourg (53.8%), Finland (39.1%), Ireland (22.2%), Italy (20.0%) and Sweden (14.8%). The proportion of observed travel‐associated cases in 2022 (5.2%) was about twice as high as in 2021 (2.4%). Of the 213 travel‐associated cases with a known country of origin, 132 cases (62.0%) were linked to travel within the EU, with most infections acquired in Spain, Italy, Greece and Croatia (20.5%, 16.7%, 10.6% and 9.8%, respectively). Türkiye and Egypt were the most frequently reported countries of infection outside the EU (23.5% and 12.3%, respectively).
The trend of human yersiniosis cases in the EU for 2018–2022 showed no statistically significant increase or decrease (Figure 24). Germany, Poland, Slovakia and Sweden reported significantly decreasing trends (p < 0.05) during the period 2018–2022. Denmark, France, Ireland, Italy, Latvia, Portugal, Slovenia and Spain reported a significantly increasing trend over the same period.
FIGURE 24.
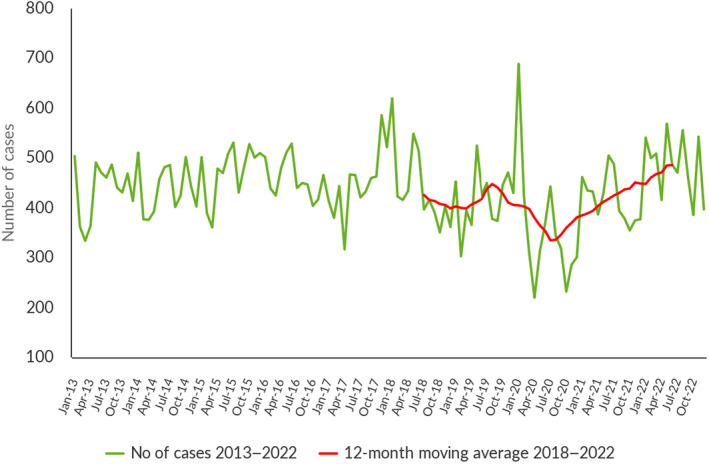
Trends in reported confirmed human cases of yersiniosis in the EU, by month, 2018–2022. Source: Austria, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Hungary, Ireland, Italy, Latvia, Luxembourg, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden.
Yersiniosis cases were reported in all age groups, with the highest proportion of reported cases belonging to the youngest age group from 0 to 14 years (3392 cases: 43.1%) and in particular, in the age group 0–4 (1715 cases: 21.8%).
Information on hospitalisation status was provided for 26.7% (N = 2113) of all yersiniosis cases by 17 MSs. Among these, the proportion of hospitalised cases was 30.1% (N = 636), slightly lower than in 2021. The highest proportions of hospitalised cases were reported by Cyprus and Romania (100% each). However, these MSs reported only a few cases of infection (1 and 14, respectively). Other MSs also reporting high proportions of hospitalised cases were Estonia (71.7%), Lithuania (71.1%), Italy (70.8%) and Latvia (67.1%). Outcomes were reported for 47.5% (N = 3765) of all cases by 17 MSs. As in the previous year, no deaths from yersiniosis were reported in 2022.
Yersinia species information was provided by 22 MSs for 95.5% of confirmed cases reported in the EU, in 2022. Of these cases, 98.7% (N = 7447) were Y. enterocolitica and 1.3% (N = 98) were Y. pseudotuberculosis. Information on Y. enterocolitica bioserotypes was provided for 2191 confirmed cases (27.7%). The most common bioserotypes were 4/O3 (83.2%) and 2/O9 (15.1%).
1.3.3 Yersinia in food
Table 62 summarises the reported occurrence of Yersinia in the main food categories in 2022 and over the 4‐year period of 2018–2022 in the EU. A distinction is made between RTE and non‐RTE food, and fresh meat. The proportions of Yersinia‐positive sampling units in the RTE and non‐RTE categories were 0.0% and 3.5%, respectively. In fresh meat, 7.2% of sampling units were positive.
TABLE 62.
Occurrence of Yersinia in major food categories, EU, 2022 and 2018–2021.
| Food | 2022(a) | 2018–2021 b | ||||
|---|---|---|---|---|---|---|
| N reporting MSs | N sampling units | N positive (%) | N reporting MSs | N sampling units | N positive (%) | |
| RTE food | ||||||
| All | 4 | 328 | 0 (0) | 7 | 2084 | 125 (6) |
| Meat and meat products | 3 | 210 | 0 (0) | 5 | 1915 | 124 (6.5) |
| Meat and meat products from pigs | 3 | 181 | 0 (0) | 3 | 168 | 3 (1.8) |
| Mixed meat and meat products from bovine animals and pigs | 0 | 0 | 0 (0) | 2 | 1553 | 111 (7.2) |
| Mixed meat | 1 | 3 | 0 (0) | 2 | 137 | 10 (7.3) |
| Meat from other animals and raw cured (or seasoned) meat | 2 | 26 | 0 (0) | 3 | 57 | 0 (0) |
| Milk and milk products | 2 | 62 | 0 (0) | 3 | 72 | 0 (0) |
| Fruits and vegetables | 2 | 56 | 0 (0) | 3 | 62 | 0 (0) |
| RTE salads | 0 | 0 | 0 (0) | 1 | 4 | 0 (0) |
| Other processed food products and prepared dishes | 0 | 0 | 0 (0) | 1 | 23 | 1 (4.4) |
| Other food | 0 | 0 | 0 (0) | 1 | 8 | 0 (0) |
| Non‐RTE food | ||||||
| All | 3 | 404 | 14 (3.5) | 9 | 3796 | 257 (6.8) |
| Meat and meat products | 3 | 401 | 14 (3.5) | 7 | 3411 | 228 (6.7) |
| Milk and milk products | 1 | 3 | 0 (0) | 3 | 261 | 29 (11.1) |
| Other food | 0 | 0 | 0 (0) | 5 | 124 | 0 (0) |
| Fresh meat c | ||||||
| All fresh meat | 3 | 166 | 12 (7.2) | 7 | 3805 | 283 (7.4) |
| Fresh meat from pigs | 3 | 128 | 10 (7.8) | 6 | 2200 | 124 (5.6) |
| Fresh meat from bovine animals | 0 | 0 | 0 (0) | 3 | 27 | 1 (3.7) |
| Fresh meat from bovine animals and pigs | 0 | 0 | 0 (0) | 2 | 1401 | 129 (9.2) |
| Other fresh meat | 1 | 38 | 2 (5.3) | 3 | 177 | 29 (16.4) |
Abbreviations: MSs, Member States; RTE, ‘ready‐to‐eat’.
Notes: Fresh meat includes RTE and non‐RTE food. Other RTE food includes: Bakery products, Cereals and nuts – RTE, Chocolate, Other food – RTE. Other non‐RTE food includes: Cereals, dried seeds – non‐RTE, Egg and egg products – non‐RTE, Fish and fishery products – non‐RTE, Fruits, vegetables and juices – non‐RTE, Foodstuffs intended for special nutritional uses – non‐RTE, Other processed food products and prepared dishes – non‐RTE and Seeds, sprouted – non‐RTE.
For the 2021–2022 period, data from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Protocol on Ireland/Northern Ireland, the EU requirements on data sampling are also applicable to Northern Ireland.
Data from the United Kingdom were taken into account for 2018–2019, because the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Fresh meat sampling units are a subset of the two main categories above.
In 2022, most of the 328 RTE food sampling units reported by 4 MSs originated from ‘meat and meat products’ (64.0%) followed by ‘milk and milk products’ (18.9%) and ‘fruit and vegetables’ (17.1%). No Yersinia‐positive sampling units were detected in any RTE food. In contrast, during 2018–2021, 6.0% of RTE food units were positive for Yersinia: 6.5% Yersinia‐positive units of ‘Meat and meat products’, with results for ‘Mixed meat’ and ‘Mixed meat and meat products from bovine animals and pigs’, being 7.3% and 7.2%, respectively. Unlike during 2018–2021, no sampling results were reported for 2022 for the categories ‘RTE salads’ and ‘Other processed food products and prepared dishes’. Despite evidence supporting the need to sample RTE foods, few MSs reported monitoring this type of food for Yersinia to EFSA, even though these foods represent a direct risk to consumers.
Most of the results reported in 2022 by 3 MSs for the 404 non‐RTE sampling units originated from the ‘meat and meat products’ (99.3%) food category. A total of 14 (3.5%) sampling units of ‘meat and meat products’ were positive for Yersinia. During 2018–2021, ‘milk and milk products’ was the most contaminated food category (11.1%), followed by ‘meat and meat products’ (6.7%).
Three MSs reported results for fresh meat categories. The highest percentage of Yersinia‐positive units was for ‘Fresh meat from pigs’ (7.8%), which was 77.1% (N = 128) of all fresh meat sampling units. A decrease in the number of sampling units for non‐RTE food and fresh meat was observed in 2022 compared with 2021. To detect the presence of Yersinia in food, microbiological methods were used for the analysis of 900 sampling units, and molecular methods for 192 sampling units, with Yersinia‐positive rates of 0.78% and 2.1%, respectively.
1.3.4 Yersinia in animals
Table 63 shows the number of sampling units of animals positive for Y. enterocolitica or Y. pseudotuberculosis during 2022, reported by five MSs and one non‐MS. Analyses of the submitted results for 23,705 animals showed the presence of Y. enterocolitica and Y. pseudotuberculosis in a similar percentage of positive sampling units: 0.34% and 0.32%, respectively. In the EU, the reported data were primarily relating to cattle (66.5%, N = 15,764), followed by small ruminants (14.4%, N = 3416) and pigs (8.5%, N = 2010). In these three animal categories, the proportion of positive sampling units for Y. enterocolitica was highest in small ruminants (0.50%), followed by cattle (0.34%) and pigs (0.20%), while for Y. pseudotuberculosis, the highest proportion was in cattle (0.32%), followed by small ruminants (0.29%). ‘Pet animals’ represented 8.3% of all animals sampled, with percentages of Y. enterocolitica‐ and Y. pseudotuberculosis‐positive samples of 0.10% and 0.31%, respectively. For ‘wild animals’, a low to very low proportion of sampling units was positive for Y. enterocolitica (1.3%) and for Y. pseudotuberculosis (0.89%). In order to assess the occurrence of Y. enterocolitica and Y. pseudotuberculosis in animal categories for which this information was available (cattle, deer, leporidae, pigs and small ruminants), microbiological methods were used for the analysis of 21,106 sampling units and molecular methods for 23 sampling units, with Yersinia‐positive rates of 0.72% and 4.3%, respectively.
TABLE 63.
Summary of Yersinia statistics relating to major animal species, reporting EU MSs and non‐MS countries, 2022.
| EU MSs a | Non‐MS countries | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N reporting countries | N tested units b | Yersinia enterocolitica positive sampling units | Yersinia pseudotuberculosis positive sampling units | N reporting countries | N tested units b | Yersinia enterocolitica positive sampling units | Yersinia pseudotuberculosis positive sampling units | |||||
| N | % | N | % | N | % | N | % | |||||
| Cattle (bovine animals) | 3 | 15,764 | 51 | 0.32 | 54 | 0.34 | 1 | 15 | 0 | 0 | 0 | 0 |
| Small ruminants (sheep and goats) | 5 | 3416 | 17 | 0.50 | 10 | 0.29 | 1 | 7 | 0 | 0 | 0 | 0 |
| Pigs | 3 | 2010 | 4 | 0.20 | 0 | 0 | 1 | 6 | 0 | 0 | 0 | 0 |
| Other domestic\farmed animals | 2 | 293 | 0 | 0 | 0 | 0 | 1 | 92 | 0 | 0 | 0 | 0 |
| Pet animals | 3 | 1965 | 2 | 0.10 | 6 | 0.31 | 1 | 1112 | 1 | 0.09 | 2 | 0.18 |
| Wild animals (e.g. deer, wild boar, fallow deer, foxes) | 3 | 224 | 3 | 1.3 | 2 | 0.89 | 1 | 5 | 0 | 0 | 0 | 0 |
| Zoo animals | 1 | 24 | 3 | 12.5 | 2 | 8.3 | 1 | 171 | 0 | 0 | 2 | 1.2 |
| Other (unspecified habitat) | 2 | 9 | 0 | 0 | 3 | 33.3 | 1 | 1 | 0 | 0 | 1 | 100 |
| Total | 5 | 23,705 | 80 | 0.34 | 77 | 0.32 | 1 | 1409 | 1 | 0.07 | 5 | 0.35 |
Abbreviation: MSs, Member States.
For the 2021–2022 period, data on animals from the United Kingdom (Northern Ireland) were taken into account. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, and in particular with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland).
Summary statistics were obtained by summing all sampling units (animals and herds).
1.4 Discussion
In 2022, 25 MSs provided information on yersiniosis, which remains the third most commonly reported foodborne gastrointestinal infection in humans in the EU, as in 2021. An increase in the notification rates and number of confirmed cases of yersiniosis has been reported, with a 16.3% increase of the annual notification rate in 2022 compared with the year 2021. This was the highest number of cases and the highest notification rate reported at the EU level during the last 10 years. The scaling down of national public response measures to COVID‐19 in the EU in 2022, along with the return of social activities such as sports, recreational events and travel, may explain this increase. However, the overall trend for yersiniosis in the 2018–2022, 5‐year period did not show any statistically significant increase or decrease.
The proportion of observed travel‐associated cases in 2022 (5.2%) was about twice as high as in the previous year (2.4%), almost reaching the pre‐pandemic level. Mediterranean countries were the main places of origin for travel‐associated yersiniosis cases.
As in previous years, in 2022, Y. enterocolitica was the species reported in the majority (98.7%) of human cases, while Y. pseudotuberculosis was notified in only 1.3% of human cases for which the information on Yersinia species was available.
In 2022, the most common bioserotypes of Y. enterocolitica in humans were 4/O3 (83.2%) and 2/O9 (15.1%), like in previous years. Information on biotypes is crucial to detect and characterise pathogenic Y. enterocolitica, as reported in an EFSA Opinion (EFSA, 2007). Furthermore, this information would allow for a better understanding of the epidemiology of human Y. enterocolitica infection and better investigation of relevant animal sources. Nevertheless, little information is available on the biotypes and serotypes of Y. enterocolitica isolated from animals and foods.
In 2022, few MSs reported data on Yersinia sampling activities in food and animals. This is probably due to the lack of mandatory monitoring plans for non‐human sources, resulting in significant differences between MSs in their approach to monitoring Yersinia in food and animals. The lack of homogeneity makes statistical analysis and monitoring of trends impossible.
Only four MSs provided data on RTE food for Yersinia, and the number of sampling units (N = 328) was comparable to that of 2021 (N = 355), with a proportion of positives at 0% compared with 0.85% in 2021. Only 56 sampling units of ‘Fruits and vegetables’ were taken, by two MSs. However, it is important to sample more RTE foods, such as RTE vegetables, which are consumed without any treatment, to reduce or eliminate potential Yersinia contamination. Although yersiniosis has usually been associated with consumption of undercooked pork products or unpasteurised milk, the growing trend of RTE vegetables in industrialised countries has been linked to sporadic outbreaks of Y. enterocolitica (Karlsson et al., 2021). Furthermore, two EFSA scientific opinions (EFSA BIOHAZ Panel, 2013c, 2014) have also drawn attention to the Yersinia risk in food of non‐animal origin, such as contamination or cross‐contamination through equipment, water or food handlers. Only three MSs provided data on non‐RTE food for Yersinia, and the number of sampling units was rather low (N = 404) compared with 2021 (N = 736), with a proportion of positive samples of 3.5% compared with 5.2% in 2021.
To investigate the presence of Yersinia in food and animals, mainly conventional microbiological and molecular methods have been used. Although few data are available on the use of molecular methods in animals, these appear to detect Yersinia better in both food and animals. In 2007, an EFSA scientific opinion (EFSA, 2007) indicated that molecular methods, such as PCR, could be a useful strategy for preliminary screening of pathogenic Y. enterocolitica in animal, food or environmental samples, after an enrichment step to increase sensitivity. PCR could be a suitable method to be used in parallel with culture methods for screening of Y. pseudotuberculosis in animal, food or environmental samples. In this context, an ISO method was issued in 2015 (ISO, 2015) and describes horizontal methods based on real‐time PCR for detection of the pathogenic bioserotypes of Y. enterocolitica and for detection of Y. pseudotuberculosis in products for human consumption, animal feeding stuffs and environmental samples. Several scientific papers have reported applications of molecular methods to assess the presence of Y. enterocolitica and Y. pseudotuberculosis in humans, food, animals and the environment (Petsios et al., 2016) (Shoaib et al., 2019) (Bui et al., 2021).
2 TOXOPLASMA GONDII
The summary data which make up this chapter, and additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
2.1 Key facts
This chapter shows the human congenital toxoplasmosis data for 2021 due to two‐year delayed reporting of data from France. As in previous years, France accounted the majority (78.0%) of reported cases of congenital toxoplasmosis in the European Union due to its active screening of pregnant women.
In 2021, there were 150 confirmed cases of human toxoplasmosis in the European Union, corresponding to an European Union notification rate of 5.6 cases per 100,000 live births and an increase of 10.0% compared with 2020 (5.1 cases per 100,000 live births).
Reporting in 2020 and 2021 were partly impacted by the COVID‐19 pandemic and the withdrawal of the United Kingdom from the European Union.
Overall, the number of human cases of congenital toxoplasmosis in the European Union (without the United Kingdom) showed a decrease, although with periodic fluctuations, in the period 2017–2021, mainly mirroring the number of cases reported by a single Member State (France).
In total, 13 Member States and 3 non‐Member States reported 2022 monitoring data on Toxoplasma gondii infections in animals and food. Most animals tested were sheep and goats, which also showed the highest overall prevalence of T. gondii infections in animals (29.0%), as reported by 12 Member States. Most samples with information provided on the sampling context were obtained from clinical investigations. It is impossible to accurately estimate the prevalence of T. gondii infections in animals due to different diagnostic methods, sampling schemes in Member States, and lack of information on the animals’ ages and rearing conditions.
2.2 Surveillance and monitoring of Toxoplasma in the EU
2.2.1 Humans
Twenty MSs reported 2021 congenital toxoplasmosis data to TESSy. Surveillance of toxoplasmosis is compulsory in 20 MSs; in one (France), it is voluntary. Data from France are reported to TESSy with a 2‐year delay. Six MSs (Austria, Belgium, Denmark, Italy, the Netherlands and Sweden) do not have a surveillance system for toxoplasmosis. Twenty MSs used the EU case definition, but one MS (France) reported the use of another case definition. All reporting MSs except one (Spain) had a comprehensive surveillance system with full national coverage. Spain did not have national surveillance or provide an estimate for population coverage, so no notification rate is calculated. All MSs reported case‐based data except Bulgaria, which reported aggregated data.
Regarding congenital toxoplasmosis surveillance only, six countries (Austria, Belgium, France, Greece, Slovakia and Slovenia) have active surveillance of congenital cases with compulsory screening of pregnant women (ECDC, 2023). However, Austria, Belgium and Greece do not report their data to ECDC. Four countries (Bulgaria, Czechia, Germany and Hungary) have voluntary screening of pregnant women. Nine countries have no screening policies and/or surveillance of congenital toxoplasmosis in pregnant women, but three of these countries report their data to ECDC.
2.2.2 Animals and food
There are no EU regulations concerning the surveillance and monitoring of T. gondii in animals and food. Therefore, the available and reported information relies on national legislation and whether the countries have a mandatory reporting system following the detection of T. gondii. As a result, data allow only for descriptive summaries at the EU level (Table 1). The main animal species tested are those intended for human consumption (small ruminants (goats and sheep), cattle and pigs) as well as pet animals (cats and dogs), using samples from aborted animals (ruminants) or clinically suspect animals. Mainly blood samples, but also samples from tissues and organs or faecal samples, are analysed either by direct methods, such as PCR, histology, immunohistochemistry and flotation, or by indirect antibody detection methods, including enzyme‐linked immunosorbent assay, latex agglutination test, direct agglutination and immunofluorescence assay. For food testing, meat is the primary matrix to be analysed by PCR or direct agglutination.
2.3 Results
2.3.1 Human congenital toxoplasmosis
Twenty MSs reported 2021 congenital toxoplasmosis data (Table 64) with 150 confirmed cases. Thirteen MSs reported zero cases (Table 64). As a result of a slightly higher number of cases reported mainly by France, Czechia and Poland for 2021, the notification rate in the EU (5.6 per 100,000 live births) increased by 10.0% compared with 2020 (5.1 per 100,000 live births) (Table 64). Indeed, 2020 was a year for which the COVID‐19 pandemic affected the comparability of data. The highest notification rate was in France (16.9 per 100,000 live births), followed by Poland (3.7), Czechia (3.6), Portugal (2.4) and Germany (1.4) (Table 64).
TABLE 64.
Reported confirmed human cases of congenital toxoplasmosis and notification rates per 100,000 live births in EU MSs and non‐MS countries by country and year, 2017–2021.
| Country | 2021 | 2020 | 2019 | 2018 | 2017 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria b | – | – | – | – | – | – | – | – | – | – | – | – |
| Belgium b | – | – | – | – | – | – | – | – | – | – | – | – |
| Bulgaria | Y | A | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 3.1 |
| Croatia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2.7 | 0 | 0 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | Y | C | 4 | 3.6 | 0 | 0 | 1 | 0.88 | 0 | 0 | 2 | 1.8 |
| Denmark b | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 7.2 | 0 | 0 |
| Finland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | Y | C | 117 | 16.9 | 110 | 15.5 | 134 | 18.8 | 151 | 20.8 | 153 | 20.7 |
| Germany | Y | C | 11 | 1.4 | 14 | 1.8 | 17 | 2.2 | 18 | 2.3 | 8 | 1.0 |
| Greece c | Y | C | – | – | – | – | 0 | 0 | 0 | 0 | 0 | 0 |
| Hungary | Y | C | 1 | 1.1 | 0 | 0 | 1 | 1.1 | 0 | 0 | 0 | 0 |
| Ireland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Italy b | – | – | – | – | – | – | – | – | – | – | – | – |
| Latvia | Y | C | 0 | 0 | 0 | 0 | 1 | 5.2 | 0 | 0 | 0 | 0 |
| Lithuania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands b | – | – | – | – | – | – | – | – | – | – | – | – |
| Poland | Y | C | 13 | 3.7 | 9 | 2.5 | 14 | 3.7 | 25 | 6.3 | 18 | 4.8 |
| Portugal | Y | C | 2 | 2.4 | – | – | – | – | – | – | – | – |
| Romania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.48 | 0 | 0 |
| Slovakia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Slovenia | Y | C | 0 | 0 | 0 | 0 | 1 | 5.1 | 2 | 9.9 | 2 | 9.8 |
| Spain d | N | C | 2 | – | 0 | – | 0 | – | 2 | – | 3 | – |
| Sweden b | – | – | – | – | – | – | – | – | – | – | – | – |
| EU Total 27 | 150 | 5.6 | 133 | 5.1 | 169 | 6.2 | 201 | 7.1 | 188 | 6.6 | ||
| United Kingdom | – | – | – | – | – | – | 7 | 1.0 | 7 | 0.91 | 7 | 0.91 |
| EU Total e | 150 | 5.6 | 133 | 5.1 | 176 | 5.1 | 208 | 5.8 | 195 | 5.4 | ||
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway b | – | – | – | – | – | – | – | – | – | – | – | – |
| Liechtenstein b | – | – | – | – | – | – | – | – | – | – | – | – |
| Switzerland b | – | – | – | – | ||||||||
Abbreviations: MSs, Member States; –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Not notifiable, no surveillance system in place.
No data reported in 2021 and 2020.
Notification rate was not calculated since information on estimated coverage was not available.
Data for the United Kingdom were collected for 2017–2019 since it was still an EU MS. However, on 1 February 2020, it became a third country.
France accounted for 78.0% of all reported cases in the EU, followed by Poland and Germany. France reports the highest number of congenital toxoplasmosis cases in the EU, whereas the other two MSs accounted for 16.0% of the reported cases in 2021.
Between 2017 and 2021, although with fluctuations, an overall decrease in reported cases was observed in France (23.5%) and Germany (38.9%, excluding data from 2017). A similar reduction was not observed in Poland, whereas an increase in the number of reported cases (50%) was observed in Czechia. In 2021, only six MSs (Czechia, Germany, Hungary, Poland, Portugal and Spain) provided information on imported cases of congenital toxoplasmosis, and no imported cases were reported. Data on hospitalisations were reported by four MSs (Czechia, Hungary, Poland and Portugal) on 20 cases, representing 100% of cases reported by these MSs and 13.3% of total cases in the EU, with 15 cases (75.0%) being hospitalised. There were three fatal cases out of 128 (case fatality of 2.3%), for cases with a known outcome. All fatal cases were reported by France. Germany did not report information on outcomes.
2.3.2 Toxoplasma gondii in food and animals
Toxoplasma gondii in food
One MS (Poland) submitted monitoring results for T. gondii in non‐ready‐to‐eat food in 2022. Eight hundred meat samples from bovine animals and pig meat preparation were reported. Forty‐four samples (5.5%) were positive.
Toxoplasma gondii in animals
Monitoring data for 2022 on T. gondii in livestock, pet or zoo animals, and wildlife were provided by 12 MSs and by 3 non‐MSs (Republic of North Macedonia, Norway and Switzerland). Most samples with information provided on the sampling context (programme type) were obtained from clinical investigations.
In small ruminants (sheep and goats), 11 MSs (Austria, Finland, Germany, Greece, Hungary, Ireland, Italy, Latvia, Netherlands, Slovakia and Spain), the United Kingdom (Northern Ireland) and 3 non‐MSs (Republic of North Macedonia, Norway and Switzerland) reported data (Table 65). In total, 4089 animals were tested, and 1180 were found to be positive (28.9%). Moreover, two MSs (Italy and Spain) reported herd/flock data: 191 herds/flocks were tested, and 16 (8.4%) were positive. In cattle, six MSs (Austria, Germany, Ireland, Italy, Latvia and Slovakia), the United Kingdom (Northern Ireland) and one non‐MS (Switzerland) reported data on Toxoplasma. In total, 704 animals were tested, and 30 were found to be positive (4.3%). In pigs, five MSs (Austria, Germany, Italy, Latvia and Slovakia) and the United Kingdom (Northern Ireland) reported monitoring data (Table 65). In addition, one MS (Italy) reported two herd/flock investigations with no positive results. For other livestock (solipeds, alpacas, leporidae, water buffaloes, fowls and ostriches), four MSs (Austria, Germany, Italy and Latvia), the United Kingdom (Northern Ireland) and one non‐MS (Switzerland) reported monitoring data. In total, 944 animals were tested, and seven (0.8%) were positive. In pet animals (cats, dogs, birds, rabbits, guinea pigs and ferrets), seven MSs (Austria, Finland, Germany, Italy, Latvia, the Netherlands and Slovakia) and one non‐MS (Switzerland) tested a total of 4438 animals (2688 cats, 1670 dogs, 37 birds, 22 rabbits, 20 guinea pigs and 1 ferret). There were 547 (12.4%) positive samples, 187 (7.0%) samples from cats, 360 (21.6%) samples from dogs and no positive samples from the other pet animals. Regarding zoo animals, six MSs (Austria, Germany, Ireland, Italy, Latvia and Slovakia) and one non‐MSs (Switzerland) tested in total 298 animals, and 15 (5.0%) were positive. Three MSs (Germany, Italy and Slovakia) and one non‐MS (Switzerland) reported on testing for T. gondii in wildlife. In total, 174 (13.4%) were positive out of a total of 1295 animals, mainly from Italy and Slovakia.
TABLE 65.
Summary of Toxoplasma gondii statistics in the main animal species, EU, 2018–2022.
| Animals a | 2022 b | 2021 b | 2020 | 2019 c | 2018 c | Data source |
|---|---|---|---|---|---|---|
| Small ruminants | ||||||
| Number of tested animals | 4068 | 4525 | 6113 | 12,120 | 6756 | EFSA |
| % of positive animals | 29.0 | 16.8 | 21.3 | 13.5 | 18.3 | EFSA |
| Number of reporting MSs | 11 | 10 | 10 | 11 | 12 | EFSA |
| Bovine animals | ||||||
| Number of tested animals | 703 | 726 | 254 | 664 | 158 | EFSA |
| % of positive animals | 4.3 | 2.5 | 9.8 | 9.2 | 27.8 | EFSA |
| Number of reporting MSs | 6 | 6 | 4 | 6 | 6 | EFSA |
| Pigs | ||||||
| Number of tested animals | 519 | 599 | 948 | 1108 | 263 | EFSA |
| % of positive animals | 11.0 | 5.0 | 9.7 | 11.7 | 22.1 | EFSA |
| Number of reporting MSs | 5 | 4 | 3 | 4 | 4 | EFSA |
| Cats | ||||||
| Number of tested animals | 2361 | 3275 | 1880 | 1525 | 1382 | EFSA |
| % of positive animals | 3.8 | 9.8 | 6.5 | 5.2 | 4.7 | EFSA |
| Number of reporting MSs | 7 | 8 | 6 | 8 | 9 | EFSA |
Abbreviation: MSs, Member States.
Summary statistics referring to MSs were obtained by totalling all samples from single animals (no flocks or herds included), from all sampling stages at primary production (conservation facilities, farm, hunting, natural habitat, retail, slaughterhouse, unspecified, veterinary activities, veterinary clinics and zoo), sampling strategies (convenience sampling, objective sampling, suspect sampling and unspecified) and samplers (HACCP and own check, industry sampling, not applicable, official sampling and private sampling). Indirect and direct diagnostic methods were taken together for the summary statistics to calculate the proportion of positive units.
For the 2021–2022 period, data on animals from the United Kingdom (Northern Ireland) were considered. In accordance with the agreement on the withdrawal of the United Kingdom from the EU, particularly with the Ireland/Northern Ireland protocol, the EU requirements on data sampling are also applicable to the United Kingdom (Northern Ireland). In addition to the MSs, United Kingdom (Northern Ireland) reported data on small ruminants, bovine animals and pigs.
For the 2018–2019 period, data from the United Kingdom were considered because it was still an EU MS. However, on 1 February 2020, it became a third country.
2.4 Discussion
Cases of toxoplasmosis in the EU are strongly biased by high number of cases reported by France, which has accounted for most reported cases since 2009 (ECDC Surveillance Atlas of Infectious Diseases), representing 75.1% to 82.7% of overall EU cases in 2017–2021 (excluding data from the United Kingdom). The high reporting rate for France reflects systematic screening for toxoplasmosis in pregnant women, first established in 1978 and mandatory since 1992. Seronegative women are followed up during pregnancy to detect seroconversion early, and congenital toxoplasmosis cases are laboratory‐confirmed. The constant decrease in cases reported in the EU in 2017–2021 (−20.2%) mirrors the drop in cases reported by France (−23.5%). This decrease was even more evident between 2017 and 2020 (−29.2% in the EU; −28.1% in France), likely as a consequence of the additional effect of the COVID‐19 pandemic on data collection. It is conceivable that data collection at the EU level in 2021 were still impacted by the COVID‐19 pandemic and the control measures adopted in the MSs, including partial or total lockdowns. However, the slight increase in notified cases registered for the year 2021 might reflect the lower impact of the COVID‐19 pandemic compared with the previous year. Independent of a COVID‐19 effect, the decreased reporting of congenital toxoplasmosis in France is the result of a gradual seroprevalence decrease in pregnant women (54% in 1995, 31% in 2016) and the number of seroconversions during pregnancy (from 5.4 per 1000 at risk pregnancies in 1995, to 2.1 in 2010, and expected to be 1.6 by 2020) (Robinson et al., 2021). An educational campaign for pregnant women and reduced exposure to contaminated raw/undercooked meat (e.g. changes in food habits and improved hygiene practices in meat production) or other raw foods at risk of contamination (e.g. fresh produce, molluscs and raw milk) likely contributed to the reduced incidence of T. gondii infection during pregnancy in France, reflecting the lower number of congenital toxoplasmosis cases (Opsteegh et al., 2015; Robinson et al., 2021). By contrast, surveillance for congenital toxoplasmosis in other MSs is highly variable, with countries reporting zero cases or simply not reporting to ECDC or lacking surveillance (Rząd et al., 2023). This can result in abortion, stillbirth, perinatal death or congenital diseases with immediate or late (up to adolescence) manifestations, including ocular diseases, seizures and learning disabilities. All possible strategies for preventing congenital toxoplasmosis, including appropriate information for pregnant women and active screening, should be reinforced.
The 2022 monitoring data from animals reported by MSs show that T. gondii is present in most livestock species across the EU, as well as in pet/zoo animals and wildlife. The limitations of these surveillance data preclude any trend watching or prevalence trend analysis in animals.
The current European surveillance system of T. gondii in animals is strongly affected by several important limitations: (i) the small number of tested animals; (ii) the use of different indirect and direct detection methods, which were in most cases not validated by an independent body; (iii) unknown age of the tested animals; and (iv) no information on the type of husbandry system (housing). Furthermore, there is no relationship between the presence of anti‐T. gondii antibodies and infecting parasites in cattle and horses (Aroussi et al., 2015; Blaga et al., 2019; Opsteegh et al., 2019). For pigs, poultry and small ruminants, serological methods could be useful for the detection of high‐risk animals or herds, but serology is not an indicator of infection in individual animals, as the agreement between direct and indirect methods was estimated to be low to moderate.
The above‐mentioned limitations associated with toxoplasmosis detection and diagnosis, and surveillance rules do not allow for direct comparison of the reported data across MSs.
3 RABIES
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
3.1 Key facts
In 2022, European Union Member States reported no human lyssavirus infections, as in 2021 and in 2020. Human lyssavirus infections were reported in 2019 and 2018, over the past 5 years (2018–2022).
Travel‐associated human rabies cases occurred occasionally in Europe, as reported in recent years. In 2019, four cases were reported from European Union countries, including three travel‐related cases and one EU‐acquired non‐rabies lyssavirus infection caused by European bat lyssavirus 1, while in 2018, one travel‐related case was reported from the UK.
In animals excluding bats, a total of 71 cases of rabies of autochthonous origin were reported by four Member States: 36 cases in Poland (32 foxes, 1 badger, 2 dogs and 1 cat), 28 cases in Romania (15 cows, 7 foxes and 6 dogs), 4 cases in Hungary (three foxes and one dog) and 3 cases in Slovakia (one fox, one badger and one dog). Hungary and Slovakia, countries that had not recorded any cases in 5 and 7 years, respectively, reported cases in 2022. The total number of reported indigenous rabies cases in non‐flying animals in the European Union decreased in 2022 compared with 2021 (118 cases), but was higher than in 2020 (12 cases) and 2019 (5 cases).
Surveillance data on lyssavirus in bats were reported by 16 European Union Member States. Five Member States (France, Germany, the Netherlands, Poland and Spain) reported 26 positive results for lyssavirus, mainly European bat 1 lyssavirus. One non‐Member States country (Switzerland) reported a positive result in a bat for European bat 2 lyssavirus.
A case of rabies was reported by France in an illegally imported dog infected with a rabies virus (RABV) strain.
3.2 Surveillance and monitoring of rabies in the EU
3.2.1 Humans
For 2022, 26 MSs reported data on human lyssavirus infections. Denmark did not report data. Reporting was mandatory in all reporting countries. EU case definitions were used by 23 MSs, although some differences exist for the case definition applied (7, 6 and 10 MSs used the EU‐2008, EU‐2012 and EU‐2018 case definitions, respectively). Two MSs (Germany and Italy) used another case definition and France did not specify the case definition used. Disease surveillance was comprehensive in all reporting MSs. Twenty‐four MSs had passive surveillance, whereas two countries (Czechia and Slovakia) applied active surveillance. For 2022, all reporting countries provided case‐based data.
3.2.2 Animals
The objective of passive rabies surveillance is to detect the presence and assess the geographic distribution of the virus over time, to allow timely dissemination of information for immediate integrated control actions among different sectors, such as the public health and veterinary sectors. For rabies‐free countries, surveillance aims to confirm the absence of the disease. In accordance with Regulation (EU) No 652/2014 51 and Commission Delegated Regulation (EU) No 2020/689, 52 multiannual programmes for eradication of rabies may be co‐financed by the EU. In 2022, 12 MSs had approved elimination, control and surveillance programmes for rabies and oral rabies vaccination (ORV) campaigns were conducted in 10 MSs (Croatia, Estonia, Finland, Greece, Hungary, Latvia, Lithuania, Poland, Romania and Slovakia), as well as in some of the EU‐bordering countries. Surveillance of rabies is carried out by sampling and testing ‘indicator animals’; these are wild or domestic animals (foxes, raccoon dogs, jackals, badgers, dogs, cattle, cats, sheep, equines, goats, etc.) that are found dead (including road‐killed) and/or suspect animals, i.e. animals showing neurological clinical signs or abnormal behaviour compatible with rabies, like biting, licking a wound or scratching a human in the absence of clear neurological signs.
To monitor the efficacy of ORV campaigns, healthy animals of the wild species targeted by oral vaccination, which are foxes, raccoon dogs and golden jackals, are hunted. These animals’ carcases are used to determine rabies immunity and oral vaccine bait uptake. This specific active rabies surveillance is traditionally designated as ‘ORV monitoring’ or ‘monitoring’ and ‘active rabies surveillance’ when rabies diagnosis is performed on such sampling. These hunted animals can indeed also be tested for rabies and very few of them (below 5%) are usually found to be positive for the disease.
Imported or travel‐related companion animals (mainly dogs and cats) from territories and non‐EU countries not included in Annex II of Commission Implementing Regulation (EU) No 577/2013 53 are currently tested for rabies virus neutralising antibodies.
In accordance with Commission Implementing Regulation (EU) 2020/2002, EU MSs must notify outbreaks of infection with rabies virus in non‐flying animals to the EU Animal Disease Information System, ADIS; 54 these are the animal species and groups of species: Carnivora, Bovidae, Suidae, Equidae, Cervidae and Camelidae, but not Chiroptera (bats).
The data reported here include all animals tested for rabies, and those collected for disease surveillance or for ORV monitoring (active surveillance) purposes.
3.3 Results
3.3.1 Overview of key statistics, EU, 2018–2022
A summary of EU‐level rabies statistics in humans and in wild and domestic animals is shown in Table 66 For animals, the total number of samples analysed for passive surveillance from foxes, raccoon dogs, golden jackals, dogs, cats and bats, as well as the number of MSs from which these samples originated, are shown. An increase was observed in the number of tested samples of foxes, which are the main reservoir of the virus in Europe, compared with 2021. The number of tested raccoon dogs and jackals remained stable compared with 2021. In 2022, the number of tested bats increased as compared with 2021. For cats and dogs, the numbers of samples reported increased compared with those of the 2018–2021 period. The number of samples tested from domestic farmed mammals in 2022 was slightly lower than in 2021. Compared with previous years, the number of positive cases in 2022 increased in dogs and farmed animals, while it decreased in cats, red foxes and raccoon dogs.
TABLE 66.
Summary of rabies lyssavirus statistics relating to humans and the main animal reservoirs, EU, 2018–2022.
| 2022 | 2021 | 2020 | 2019(a) | 2018(a) | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 0 | 0 | 0 | 4 | 1 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0 | 0 | 0 | 0 | 0 | ECDC |
| Number of reporting countries | 26 | 26 | 26 | 28 | 28 | ECDC |
| Infection acquired in the EU | 0 | 0 | 0 | 1 | 0 | ECDC |
| Infection acquired outside the EU | 0 | 0 | 0 | 3 | 1 | ECDC |
| Unknown travel status or unknown country of infection | 0 | 0 | 0 | 0 | 0 | ECDC |
| Animals under passive surveillance | ||||||
| Dogs (Canis lupus familiaris) | ||||||
| Number of tested animals | 2174 | 1838 | 1732 | 1901 | 2097 | EFSA |
| Number of positive animals | 11 b | 4 | 4 | 0 | 1 | EFSA |
| Number of reporting MSs | 23 | 21 | 22 | 22 | 23 | EFSA |
| Cats (Felis catus) | ||||||
| Number of tested animals | 2962 | 2335 | 2440 | 2389 | 2661 | EFSA |
| Number of positive animals | 1 | 8 | 2 | 0 | 0 | EFSA |
| Number of reporting MSs | 22 | 20 | 21 | 22 | 21 | EFSA |
| Farmed mammals c | ||||||
| Number of tested animals | 374 | 406 | 392 | 394 | 570 | EFSA |
| Number of positive animals | 15 | 4 | 3 | 1 | 1 | EFSA |
| Number of reporting MSs | 16 | 17 | 17 | 15 | 17 | EFSA |
| Wild animals – Red foxes (Vulpes vulpes) | ||||||
| Number of tested animals | 18,486 | 12,907 | 9805 | 5336 | 5833 | EFSA |
| Number of positive animals | 43 | 97 | 6 | 2 | 6 | EFSA |
| Number of reporting MSs | 18 | 17 | 18 | 16 | 16 | EFSA |
| Wild animals – Raccoon dogs (Nyctereutes procyonoides) | ||||||
| Number of tested animals | 1096 | 1339 | 1214 | 1241 | 1335 | EFSA |
| Number of positive animals | 0 | 2 | 0 | 0 | 0 | EFSA |
| Number of reporting MSs | 7 | 6 | 6 | 7 | 7 | EFSA |
| Wild animals – Jackals (Canis aureus) | ||||||
| Number of tested animals | 241 | 230 | 102 | 42 | 44 | EFSA |
| Number of positive animals | 0 | 0 | 0 | 0 | 0 | EFSA |
| Number of reporting MSs | 7 | 5 | 6 | 5 | 4 | EFSA |
| Wild animals – Bats (order Chiroptera) | ||||||
| Number of tested animals | 1622 | 1316 | 1308 | 2069 | 2278 | EFSA |
| Number of positive animals | 26 | 29 | 31 | 39 | 45 | EFSA |
| Number of reporting MSs | 16 | 16 | 15 | 19 | 18 | EFSA |
| Animals under active surveillance (ORV monitoring) d | ||||||
| Red foxes (Vulpes vulpes) | ||||||
| Number of tested animals | 1896 | 10,581 | 14,416 | 17,805 | 15,737 | EFSA |
| Number of positive animals | 0 | 0 | 0 | 1 | 0 | EFSA |
| Number of reporting MSs | 7 | 9 | 10 | 9 | 9 | EFSA |
| Raccoon dogs (Nyctereutes procyonoides) | ||||||
| Number of tested animals | 322 | 369 | 324 | 301 | 23 | EFSA |
| Number of positive animals | 0 | 0 | 0 | 0 | 0 | EFSA |
| Number of reporting MSs | 4 | 4 | 4 | 3 | 2 | EFSA |
| Jackals (Canis aureus) | ||||||
| Number of tested animals | 1100 | 1499 | 1319 | 1045 | 1304 | EFSA |
| Number of positive animals | 0 | 0 | 0 | 0 | 0 | EFSA |
| Number of reporting MSs | 1 | 3 | 3 | 2 | 3 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States; ORV, oral rabies vaccination.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
One imported case included.
Included cattle (bovine animals), horses, sheep, goats and pigs.
Samples collected in the framework of oral rabies vaccination monitoring (ORV).
Table 66 also displays the active surveillance (ORV monitoring) statistics for ORV target species (foxes, raccoon dogs and golden jackals). In the context of ORV monitoring, the number of tested foxes decreased considerably, about five‐fold, in 2022 compared with 2021, while the number of tested raccoon dogs and golden jackals remained stable. The main reason for the reported decrease is that several countries did not report data from ORV monitoring, as rabies diagnosis in apparently healthy hunted wild animals is no longer included in EU co‐funded eradication programmes. 55
3.3.2 Humans
No human cases were reported between 2020 and 2022. In previous years (2018–2019) four travel‐associated cases were reported, mostly linked to dog exposure from Morocco (N = 2), Tanzania (N = 1) and India (N = 1). France reported an EU‐acquired infection in 2019, due to European bat lyssavirus 1 (EBLV‐1).
3.3.3 Animals
Rabies cases in wildlife
In 2022, 18,486 foxes (Vulpes vulpes) were tested using passive surveillance by 18 MSs. In total, 43 cases of rabies were detected in foxes in the EU: 32 cases in Poland, 7 in Romania, 3 in Hungary and 1 in Slovakia. The geographical distribution and number of cases in foxes per NUTS 3 (Nomenclature of territorial units for statistics), 56 as well as a choropleth map of the total number of foxes sampled per MS for passive surveillance, are shown in Figure 25. Three non‐EU countries (Republic of North Macedonia, Serbia and Switzerland) reported a total of 30 foxes tested under passive surveillance schemes and found none to be positive.
FIGURE 25.
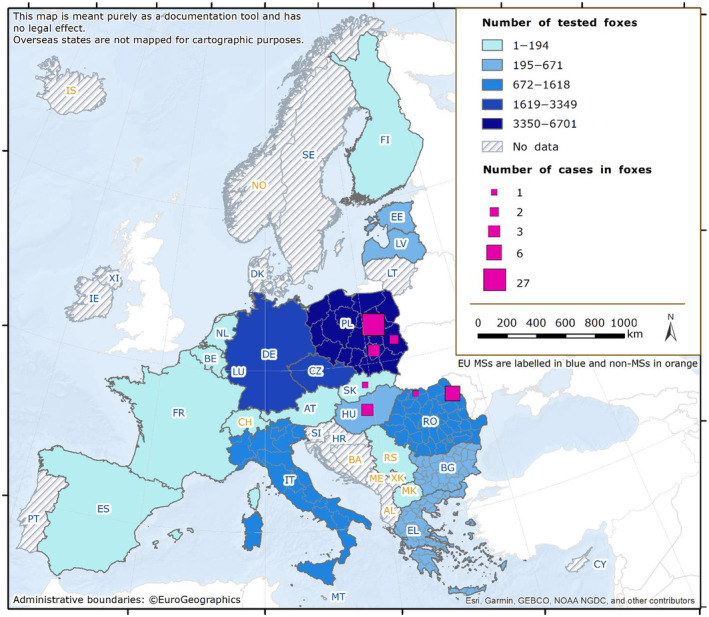
Choropleth map of the number of tested and positive foxes in the framework of passive surveillance, and the geographical distribution of the rabies cases reported in foxes in EU MSs and non‐EU countries, 2022. Note: For Slovakia and Hungary, the geographical distribution of reported cases was not provided.
In 2022, 1096 raccoon dogs (Nyctereutes procyonoides) were tested for rabies by seven MSs (Czechia, Estonia, Finland, Italy, Latvia, Poland and Slovakia) and none were found positive. Most (92.3%) of these samples came from raccoon dogs originating from two MSs (Estonia and Latvia).
Eighteen MSs reported data from passive surveillance for 1578 non‐flying wild animals other than foxes, raccoon dogs or golden jackals. The other most widely tested wild animal species were badgers (N = 597), martens (N = 343), wolves (N = 198), deers, red and roe deers (N = 178) and raccoons (N = 119). Two badgers tested positive for rabies, in Poland and in Slovakia (one case each). Other species tested included mice, lynx, otters, squirrels, hedgehogs, rats, wild boars, bears, ferrets, dormice, wild cats, wolverines, minks, polecats, rodents and moose. All the animals tested negative for rabies. Three non‐MSs (Republic of North Macedonia, Serbia and Switzerland) analysed two wild boars, two wolves, one badger and one marten, and all samples tested negative.
In 2022, 16 MSs and two non‐MSs reported surveillance data on bats. In total, 1622 bats were investigated in the EU (Figure 26). Of these, 26 samples tested positive in five MSs: France (11 EBLV‐1), Germany (6 EBLV‐1), Spain (5 EBLV‐1), Poland (3 unspecified lyssavirus) and the Netherlands (one EBLV‐1). Two non‐MSs, Serbia and Switzerland, analysed 1 bat and 28 bats, respectively and one bat from Switzerland tested positive (European bat 2 lyssavirus (EBLV‐2)).
FIGURE 26.
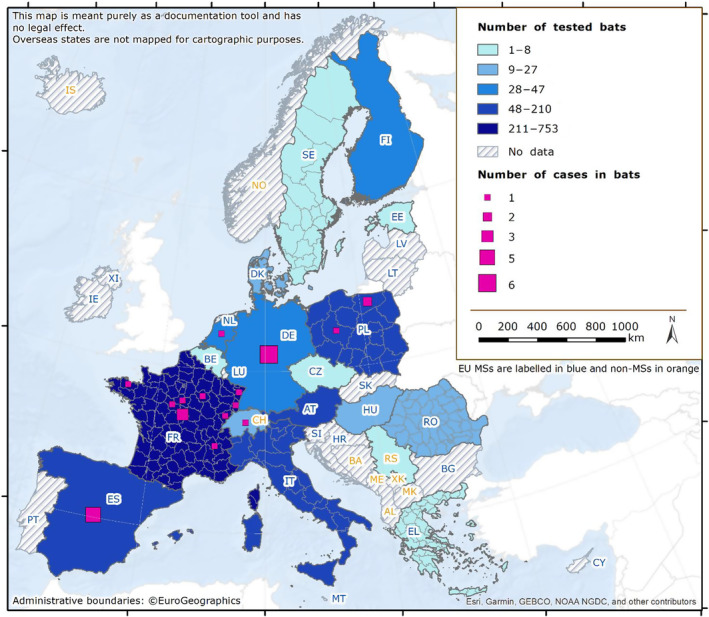
Choropleth map of the number of tested and positive bats, and the geographical distribution of the rabies cases reported in bats in EU MSs and non‐EU countries, 2022. Note: For Germany, Spain and Netherlands, the geographical distribution of reported cases was not provided.
Rabies cases in domestic animals
In 2022, a total of 26 autochthonous domestic animals tested positive for rabies.
Twenty‐one MSs tested in total 5136 samples for dogs and cats: 2174 dogs (from 23 MSs) and 2962 cats (from 22 MSs). A total of 11 pet dogs tested positive: in Romania six cases (RABV), in Poland two cases (unspecified lyssavirus), in Hungary one case (unspecified lyssavirus), in Slovakia one case (RABV) and in France one imported case. This 4‐year‐old dog had been illegally imported from Morocco and then abandoned in a shelter where it stayed for the entire period of rabies contagiousness. Genetic analysis revealed that it was a RABV Cosmopolitan virus strain (ex‐Africa 1), likely originating from Northern Africa. A case in a pet cat (unspecified lyssavirus) was reported by Poland. Four non‐EU countries (Norway, Republic of North Macedonia, Serbia and Switzerland) reported in total results for 52 dogs and 44 cats, with no rabies positives. The geographical distribution and number of tested and reported cases in pets (dogs and cats) are shown in Figure 27.
FIGURE 27.
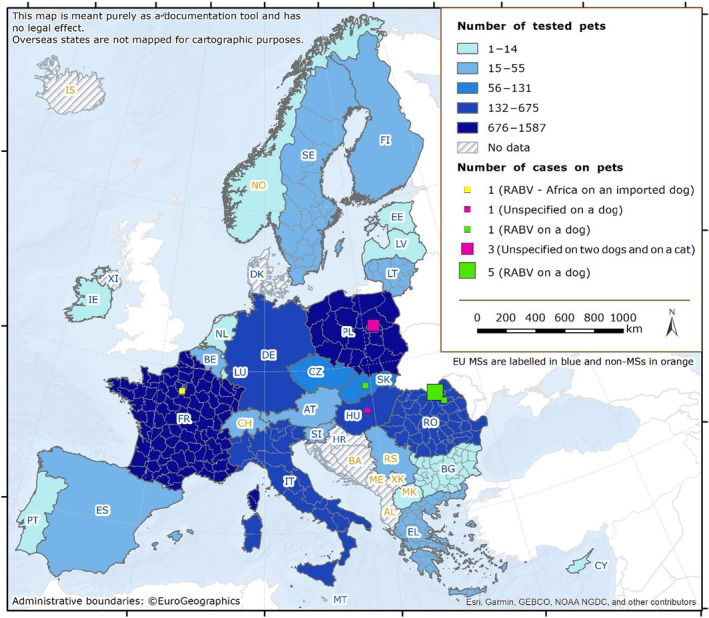
Choropleth map of the number of tested and positive pets, and the geographical distribution of the rabies cases reported in pets in EU MSs and non‐EU countries, 2022. Note: For Slovakia and Hungary, the geographical distribution of reported cases was not provided.
A total of 374 samples from farmed mammals (Figure 28) were tested by 16 MSs (reports included mainly cattle, small ruminants and domestic solipeds). Romania reported 15 cases of rabies (RABV) in cows. Three non‐EU countries reported three samples tested from farmed ruminants (Republic of North Macedonia (one bovine animal), Serbia (one goat) and Switzerland (one cattle); all of them tested negative.
FIGURE 28.
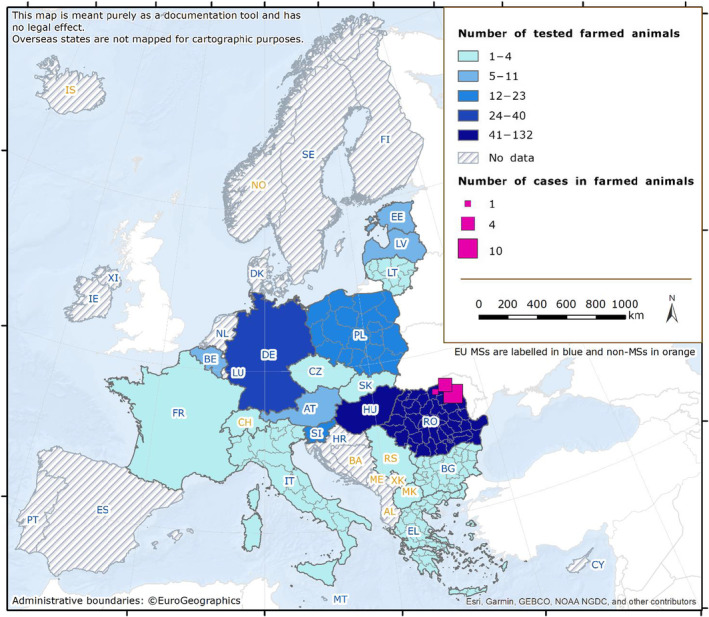
Choropleth map of the number of tested and positive farmed animals, and the geographical distribution of the rabies cases reported in farmed animals in EU MSs and non‐EU countries, 2022.
3.4 Discussion
In Europe, human rabies is a rare disease, with the last autochthonous EU case of RABV human infection dating back to 2012 (Romania). Nowadays, the infection is mainly acquired abroad in countries where dog rabies is endemic, and development of the disease is due to the absence of pre‐exposure prophylaxis or late/inappropriate/incomplete administration of post‐exposure prophylaxis. The illegal import of pets also poses a constant risk of rabies introduction (Klevar et al., 2015). Another rare source of infection is through organ transplantation (Maier et al., 2010). The absence of human rabies deaths since 2020 might be attributable to reduced travel due to the COVID‐19 mitigation measures applied in many MSs. In this regard, recently restored international mobility, combined with reduced rabies control in endemic areas, poses risks in terms of possible travel‐related human cases in the near future (Goel et al., 2023). Although non‐RABV lyssavirus infections are rare, the identification of an EU‐acquired human case due to EBLV‐1 (France, 2019) from an infected bat underlines the need to continue monitoring the occurrence of this fatal encephalitis in humans.
Concerning infections caused by lyssaviruses other than RABV, five human deaths have been reported so far in Europe, more specifically in Ukraine (1977: species not characterised), Russia (1985: EBLV‐1), Finland (1985: EBLV‐2), the United Kingdom (2002: EBLV‐2) and the recent case acquired in France (2019: EBLV‐1) (Fooks et al., 2003; Regnault et al., 2022). All these infections were linked to direct exposure to infected bats; however, indirect exposure to lyssaviruses by contact with infected domestic animals (mainly free‐roaming cats, occasionally infected by a bat lyssavirus) must not be overlooked. In this context, the absence of tools to prevent divergent lyssaviruses from circulating in European bats must be underlined (Echevarría et al., 2019).
The EU programmes for rabies eradication include disease surveillance, oral vaccination campaigns, monitoring of ORV and awareness activities. Results in 2022 show maintenance of the infection in European wildlife reservoirs in Poland (in total 36 cases, including wildlife species and pets) and in Romania (28 cases), and re‐infections of rabies in two rabies‐free MSs, i.e. in Hungary (4 cases) and in Slovakia (3 cases). These latter two MSs had reported the last cases in 2017 and 2015, respectively. The epidemiological data localised these cases close to the borders with Ukraine. In Romania, the markedly increased number of cases, 26 compared with five cases in 2021 (most of them detected in bordering areas with Moldova), is linked with re‐infections in Northern and Eastern areas of the country bordering Ukraine and Moldova, respectively. While the situation seemed to have improved in Poland (113 cases detected in 2021, with 36 cases detected in 2022), the overall situation in the EU shows how fragile the epidemiological situation of a country is, as it is linked to that of neighbouring countries. The cases still being reported over several years in the few remaining MSs with infections, or re‐emergence of rabies, highlight the importance of a sustainable surveillance programme and awareness campaigns for the general public and professionals to ensure the early detection of any potential cases. They also stress the importance of cross‐border collaborations to achieve disease‐free status.
Data relating to rabies passive surveillance in wildlife, mainly in foxes and raccoon dogs, show relative stability in the number of samples tested, and even an increase in the fox sampling effort, due to the surveillance efforts maintained by most rabies‐free and infected MSs for early detection of the virus and for controlling the last foci. Data relating to active surveillance (ORV monitoring) are reported for foxes, raccoon dogs and jackals. This surveillance is conducted by hunting apparently healthy animals and using the animals’ carcases to assess the efficacy of vaccination campaigns in infected and rabies‐free countries involved in eradication programmes. A sample size linked to the area covered by vaccination is recommended. The data show a substantial decrease over the years, and a five‐fold decrease as compared with 2021, in the number of analysed foxes, reflecting the decrease in the size of areas vaccinated in the EU, hence the success of ORV programmes.
Regarding rabies surveillance in bats, the number of tests increased in 2022 compared with 2021 and 2020, despite a lower number of MSs reporting. This increase may be explained by a higher number of tested bats reported by France (753 and 308 in 2022 and 2021, respectively). Positive results obtained in the framework of bat surveillance (26 cases) are in line with the findings of the previous years and confirm that European bats act as reservoirs for lyssaviruses other than rabies virus, reaffirming the public recommendation to handle bats with utmost caution, if at all. The public health hazard of bat lyssaviruses in Europe should not be underestimated.
For 2022, France reported one case of imported rabies in a dog, originating from Evry in the South‐East suburbs of Paris. Imported cases are recurrent in the EU, at a frequency of approximately one imported case per year (EFSA, Alvarez, et al., 2022), and might pose a threat of rabies reintroduction into rabies‐free areas. This also underlines the need to improve public awareness, particularly among travellers, with regard to rabies risks and legislation involving pet movements.
As rabies is still endemic in countries bordering the EU, in areas not far from the borders, several MSs are involved in collaborations with these countries for the implementation of vaccination and testing schemes in buffer zones. The Global Framework for the Progressive Control of Transboundary Animal Diseases (GF‐TADs) created a Standing Group of Experts on Rabies (SGE RAB) in 2019, and the fourth meeting was organised in 2022 with the goal of coordinating rabies control and improving surveillance activities, primarily in the Balkan sub‐region, where a case was detected in a dog in 2020.
Maintaining appropriate surveillance is of paramount importance for all MSs, due to regular resurgence of the disease in rabies‐free areas, and the persistence of active foci in Poland and Romania. Apparent disappearance of the virus has been achieved in most EU territories, and maintaining appropriate surveillance efforts remains the most challenging issue to attaining rabies elimination in the EU.
4 Q FEVER
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
4.1 Key facts
In 2022, there were 719 confirmed cases of human Q fever, corresponding to an European Union notification rate of 0.17 cases per 100,000 population. This was an increase of 56.5% compared with 2021 (0.11 cases per 100,000 population).
The overall trend for human Coxiella burnetii infections did not show any significant increase or decrease in the 2018–2022 period.
In animals, cattle and small ruminants were mostly sampled during clinical investigations and passive monitoring of animals suspected to be infected with C. burnetii. However, in the absence of harmonised reporting data in animals in the European Union, the data reported to EFSA cannot be used to analyse spatial representativeness and trends over the years for Q fever in the European Union or to compare differences among reporting countries.
In total, 18 Member States (17 in 2021) and five non‐Member States (five in 2021) reported 2022 data for C. burnetii in animals. Among the animals tested using direct detection methods (N = 2973), the proportion of positive animals was 3.6% for sheep, 2.1% for goats and 2.7% for cattle. Among the herds tested using direct detection methods (N = 7935), the proportion of positive herds was 4.9% for sheep, 3.5% for goats and 7.7% for cattle. The proportion of seropositive animals was 11.4% for sheep, 17.9% for goats and 2.8% for cattle among the 7697 animals tested in total. The proportion of seropositive herds was 97.7% for sheep and 30.1% for cattle among the 241 herds tested in total, whereas no serological tests were reported for goat herds.
Among the other farmed, domestic or wild animals tested (N = 396 animals, N = 7 herds and N = 6 reporting countries), positivity was reported only in Italy, in birds (13.8%; N = 29), dogs (4.0%; N = 25), water buffalos (1.8%; N = 226) and pigs (N = 1 herd).
4.2 Surveillance and monitoring of Coxiella burnetii in the EU
4.2.1 Humans
For 2022, 25 MSs provided data on Q fever in humans. No surveillance system is in place in Austria. Denmark did not report data for 2020–2022. Surveillance is mandatory in 24 MSs and voluntary in France. The EU case definition was used by 22 countries; three MSs (France, Germany and Italy) reported use of another case definition. Disease surveillance is comprehensive and generally passive except in Czechia and Slovakia. The Q fever surveillance systems cover the whole population in all reporting MSs. All countries reported case‐based data except Belgium and Bulgaria, which provided aggregated data.
4.2.2 Animals
Q fever is a ‘Category E’ disease, for which there is a need for surveillance and annual reporting of confirmed cases by MSs in Bison spp., Bos spp., Bubalus spp., Ovis spp. and Capra spp. (Commission Implementing Regulation CIR (EU) 2018/1882, 57 CIR (EU) 2020/2002 58 ).
However, since neither surveillance nor reporting of animal Q fever has been harmonised in the EU, data may not be representative of the disease situation in each European country and should not be used for tracking or assessing EU‐level temporal and spatial trends.
The main animal categories tested were sheep, goats and cattle. Samples were mostly blood samples, samples from foetuses and stillborn animals, placentas, vaginal swabs from animals suspected of being infected with C. burnetii, as well as bulk milk samples for screening. Samples were tested either using serological methods (antibodies proving past or recent exposure to C. burnetii) or direct detection methods (bacterial material indicating carriage). In most MSs, C. burnetii detection was based on clinical investigation and passive monitoring. A few countries (Belgium, Bulgaria, the Netherlands, Poland) implemented planned surveillance in cattle and small ruminants. Poland (N = 4876) and Belgium (N = 281) used mainly direct detection in herds, whereas Bulgaria (N = 171) mainly ELISA serological tests at the individual animal level. Belgium and the Netherlands carried out regular PCR tests on bulk tank milk from dairy sheep and goats. Some countries reported very low numbers of tests, corresponding to local surveys or selective tests. In addition, samples were taken from other farmed or domestic animals (in particular, water buffalos in Italy) and wild animal species, in zoos or from natural habitats.
4.3 Results
4.3.1 Overview of key statistics, EU, 2018–2022
Table 67 summarises EU‐level statistics on human Q fever, and on the occurrence of C. burnetii in animals, for the period 2018–2022. More detailed descriptions of these statistics are provided in the subsections below.
TABLE 67.
Summary of Coxiella burnetii statistics relating to humans and the main animal species, EU, 2018–2022.
| 2022 | 2021 | 2020 | 2019(a) | 2018(a) | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 719 | 460 | 523 | 951 | 790 | ECDC |
| Total number of confirmed cases/100,000 population (notification rates) | 0.17 | 0.11 | 0.12 | 0.19 | 0.16 | ECDC |
| Number of reporting EU MSs | 25 | 25 | 25 | 27 | 27 | ECDC |
| Infection acquired in the EU | 597 | 359 | 347 | 810 | 629 | ECDC |
| Infection acquired outside the EU | 5 | 3 | 6 | 14 | 12 | ECDC |
| Unknown travel status or unknown country of infection | 117 | 98 | 170 | 127 | 149 | ECDC |
| Animals b | ||||||
| Sheep c | ||||||
| Animals | ||||||
| Serology d | ||||||
| Number of tested animals | 526 | 750 | 911 | 666 | 2986 | EFSA |
| % positive animals | 11.4 | 10.3 | 11.4 | 9.9 | 14.4 | EFSA |
| Number of reporting MSs | 8 | 8 | 8 | 9 | 10 | EFSA |
| Direct detection e | ||||||
| Number of tested animals | 752 | 83 | 347 | 224 | 308 | EFSA |
| % positive animals | 3.6 | 6.0 | 8.9 | 18.3 | 13.6 | EFSA |
| Number of reporting MSs | 7 | 4 | 3 | 4 | 5 | EFSA |
| Other methods/unknown | ||||||
| Number of tested animals | 0 | 523 | 1566 | 2244 | 852 | EFSA |
| % positive animals | – | 0 | 21.5 | 13.3 | 0.59 | EFSA |
| Number of reporting MSs | – | 1 | 2 | 2 | 3 | EFSA |
| Herds | ||||||
| Serology d | ||||||
| Number of tested herds | 128 | 2238 | 17 | 25 | 197 | EFSA |
| % positive herds | 97.7 | 18.9 | 5.9 | 28.0 | 8.6 | EFSA |
| Number of reporting MSs | 1 | 1 | 2 | 1 | 3 | EFSA |
| Direct detection e | ||||||
| Number of tested herds | 2812 | 3130 | 2890 | 2902 | 3480 | EFSA |
| % positive herds | 4.9 | 4.1 | 1.4 | 1.2 | 0.92 | EFSA |
| Number of reporting MSs | 6 | 5 | 4 | 4 | 4 | EFSA |
| Other methods/unknown | ||||||
| Number of tested herds | 0 | 0 | 39 | 53 | 1 | EFSA |
| % positive herds | – | – | 15.4 | 30.2 | 0 | EFSA |
| Number of reporting MSs | – | – | 1 | 1 | 1 | EFSA |
| Goats | ||||||
| Animals | ||||||
| Serology d | ||||||
| Number of tested animals | 140 | 540 | 651 | 656 | 947 | EFSA |
| % positive animals | 17.9 | 24.6 | 25.0 | 18.0 | 20.6 | EFSA |
| Number of reporting MSs | 8 | 6 | 7 | 8 | 9 | EFSA |
| Direct detection e | ||||||
| Number of tested animals | 961 | 200 | 247 | 189 | 179 | EFSA |
| % positive animals | 2.1 | 16.5 | 11.3 | 9.5 | 8.4 | EFSA |
| Number of reporting MSs | 7 | 4 | 3 | 4 | 5 | EFSA |
| Other methods/unknown | ||||||
| Number of tested animals | 0 | 777 | 832 | 845 | 1114 | EFSA |
| % positive animals | – | 0.13 | 0 | 0 | 1.1 | EFSA |
| Number of reporting MSs | – | 1 | 2 | 2 | 3 | EFSA |
| Herds | ||||||
| Serology d | ||||||
| Number of tested herds | 0 | 4 | 141 | 30 | 212 | EFSA |
| % positive herds | – | 50.0 | 78.7 | 73.3 | 25.5 | EFSA |
| Number of reporting MS | – | 1 | 1 | 1 | 3 | EFSA |
| Direct detection e | ||||||
| Number of tested herds | 1189 | 1283 | 1175 | 1167 | 1302 | EFSA |
| % positive herds | 3.5 | 2.0 | 1.2 | 2.8 | 2.8 | EFSA |
| Number of reporting MSs | 5 | 5 | 4 | 4 | 4 | EFSA |
| Other methods/unknown | ||||||
| Number of tested herds | 82 | 0 | 12 | 207 | 27 | EFSA |
| % positive herds | 62.2 | – | 0 | 84.1 | 29.6 | EFSA |
| Number of reporting MSs | 1 | – | 1 | 1 | 1 | EFSA |
| Cattle (bovine animals) | ||||||
| Animals | ||||||
| Serology d | ||||||
| Number of tested animals | 7031 | 3405 | 4664 | 8722 | 14,795 | EFSA |
| % positive animals | 2.8 | 12.2 | 9.6 | 10.5 | 9.8 | EFSA |
| Number of reporting MSs | 9 | 11 | 9 | 11 | 11 | EFSA |
| Direct detection e | ||||||
| Number of tested animals | 1260 | 452 | 832 | 739 | 4665 | EFSA |
| % positive animals | 2.7 | 5.1 | 3.7 | 3.0 | 4.9 | EFSA |
| Number of reporting MSs | 5 | 4 | 5 | 4 | 4 | EFSA |
| Other methods/unknown | ||||||
| Number of tested animals | 0 | 349 | 3870 | 4240 | 4001 | EFSA |
| % positive animals | – | 0.29 | 0.08 | 0.66 | 2.8 | EFSA |
| Number of reporting MSs | – | 1 | 2 | 2 | 4 | EFSA |
| Herds | ||||||
| Serology d | ||||||
| Number of tested herds | 113 | 1201 | 312 | 551 | 2283 | EFSA |
| % positive herds | 30.1 | 15.1 | 14.4 | 30.7 | 10.2 | EFSA |
| Number of reporting MSs | 3 | 1 | 2 | 2 | 4 | EFSA |
| Direct detection e | ||||||
| Number of tested herds | 3934 | 4311 | 3571 | 3673 | 1262 | EFSA |
| % positive herds | 7.7 | 4.8 | 6.7 | 6.3 | 2.6 | EFSA |
| Number of reporting MSs | 6 | 8 | 5 | 5 | 5 | EFSA |
| Other methods/unknown | ||||||
| Number of tested herds | 6 | 0 | 0 | 43 | 132 | EFSA |
| % positive herds | 100 | – | – | 95.3 | 3.8 | EFSA |
| Number of reporting MSs | 1 | – | – | 1 | 1 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
Number of tested animals, and herds were obtained by totalling respectively the animal sampling unit, and the herd or holding sampling units, of all sampling stages (backyard, border control posts, farm, hunting, natural habitat, unspecified, veterinary activities and zoo), sampling strategies (census, convenience sampling, objective sampling selective sampling and suspect sampling) samplers (HACCP and own check, industry sampling, official sampling, not applicable and private sampling) and sampling contexts (clinical investigations, monitoring, outbreak investigation, surveillance, survey and unspecified).
‘Sheep’ also includes the ‘sheep and goats’ category (NB, some countries reported both livestock types together).
Serology includes the complement fixation test (CFT), ELISA, competitive ELISA (C‐ELISA), indirect ELISA (I‐ELISA), IgG ELISA and the immunofluorescence antibody test (IFAT).
Direct detection methods include fluorescent in situ hybridisation (FISH), immunohistochemistry (IHC), microbiological tests, multiplex PCR, PCR, real‐time PCR, real‐time PCR (CEN TC 275/WG 6).
Animal categories
Animal data of interest were classified into three major species categories (sheep, goats and cattle) and aggregated by year to obtain an annual overview of the volume of data submitted. The total number and the proportions of positive animals (individual level) and herds, holdings or flocks (group level) are segregated depending on the type of analytical testing method used (serology or direct detection).
In 2022, compared with year 2021, the total number of (individual) animal samples submitted by EU MSs decreased slightly for sheep (5.8%; N = 1278 in 2022) and for goats (27.4%; N = 1101 in 2022) and increased for cattle (97.1%; N = 8291). Concomitantly, the number of sampled herds remained stable for goats (N = 1271 in 2022) and decreased by 45.2% for sheep (N = 2940 in 2022) and by 26.5% for cattle (N = 4053 in 2022). In comparison to 2021, the total number of submitted samples per year at the animal and herd levels decreased by 37.3% for sheep (N = 4218 in 2022) and by 15.4% for goats (N = 2372 in 2022), but increased by 27.0% for cattle (N = 12,344 in 2022) after 4 years of continuous decrease.
The proportions of positive serological tests varied greatly among years and sampling context. The overall proportions of positive animal samples during 2018–2022 ranged from 9.9% to‐ 14.4% for sheep (11.4% in 2022), from 17.9% to 25.0% for goats (17.9% in 2022) and from 2.8% to 12.2% for cattle (2.8% in 2022). At the herd level, the proportions of positive serological tests ranged from 5.9% to 97.7% for sheep (97.7% in 2022, from N = 128 herds reported by Italy only), from 25.5% to 78.7% for goats (50.0% in 2021, no data reported in 2022) and from 10.2% to 30.7% for cattle (30.1% in 2022).
The range and the proportion of positive direct detection tests were generally lower than those of serological tests, but slightly higher at the herd level than in the four previous years. In particular, data at the animal level reported by the Netherlands were included this year in the following section, because the analytical method was specified in 2022, unlike in previous years. The overall proportions of positive animal samples during 2018–2022 ranged from 3.6 to 18.3% for sheep (3.6% in 2022), from 2.1 to 16.5% for goats (2.1% in 2022) and from 2.7 to 5.1% for cattle (2.7% in 2022). At the herd level, the proportions of positive serological tests ranged from 0.92 to 4.9% for sheep (4.9% in 2022), from 1.2 to 3.5% for goats (3.5% in 2022) and from 2.6 to 7.7% for cattle (7.7% in 2022).
4.3.2 Coxiella burnetii in humans
For 2022, 25 EU MSs reported a total of 719 confirmed cases of Q fever, with a notification rate of 0.17 cases per 100,000 population. This is an increase of 56.5% compared with the rate in 2021 (0.11 per 100,000 population). Hungary had the highest notification rate with 0.69 cases per 100,000 population, followed by Spain and Croatia, with 0.64 and 0.57 cases per 100,000 population, respectively (Table 68).
TABLE 68.
Reported human cases of Q fever and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria b | – | – | – | – | – | – | – | – | – | – | – | – |
| Belgium | Y | A | 6 | 0.05 | 6 | 0.05 | 4 | 0.03 | 10 | 0.09 | 6 | 0.05 |
| Bulgaria | Y | A | 13 | 0.19 | 31 | 0.45 | 103 | 1.5 | 36 | 0.51 | 45 | 0.64 |
| Croatia | Y | C | 22 | 0.57 | 0 | 0 | 2 | 0.05 | 8 | 0.20 | 11 | 0.27 |
| Cyprus | Y | C | 2 | 0.22 | 2 | 0.22 | 1 | 0.11 | 1 | 0.11 | 0 | 0 |
| Czechia | Y | C | 2 | 0.02 | 1 | 0.01 | 1 | 0.01 | 1 | 0.01 | 1 | 0.01 |
| Denmark | Y | C | – | – | – | – | – | – | 0 | 0 | 0 | 0 |
| Estonia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0.04 | 2 | 0.04 |
| France | Y | C | 127 | 0.19 | 92 | 0.14 | 96 | 0.14 | 156 | 0.23 | 172 | 0.26 |
| Germany | Y | C | 65 | 0.08 | 99 | 0.12 | 55 | 0.07 | 148 | 0.18 | 91 | 0.11 |
| Greece | Y | C | 10 | 0.10 | 4 | 0.04 | 4 | 0.04 | 14 | 0.13 | 13 | 0.12 |
| Hungary | Y | C | 67 | 0.69 | 41 | 0.42 | 34 | 0.35 | 47 | 0.48 | 28 | 0.29 |
| Ireland | Y | C | 0 | 0 | 0 | 0 | 2 | 0.04 | 2 | 0.04 | 0 | 0 |
| Italy | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 6 | 0.01 | 1 | < 0.01 |
| Latvia | Y | C | 2 | 0.11 | 0 | 0 | 1 | 0.05 | 0 | 0 | 0 | 0 |
| Lithuania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | Y | C | 3 | 0.46 | 0 | 0 | 2 | 0.32 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 2 | 0.38 | 1 | 0.19 | 0 | 0 | 1 | 0.20 | 2 | 0.42 |
| Netherlands | Y | C | 12 | 0.07 | 6 | 0.03 | 7 | 0.04 | 16 | 0.09 | 18 | 0.10 |
| Poland | Y | C | 2 | 0.01 | 0 | 0 | 0 | 0 | 4 | 0.01 | 0 | 0 |
| Portugal | Y | C | 25 | 0.24 | 18 | 0.17 | 22 | 0.21 | 32 | 0.31 | 36 | 0.35 |
| Romania | Y | C | 49 | 0.26 | 5 | 0.03 | 12 | 0.06 | 109 | 0.56 | 22 | 0.11 |
| Slovakia | Y | C | 0 | 0 | 2 | 0.04 | 5 | 0.09 | 1 | 0.02 | 2 | 0.04 |
| Slovenia | Y | C | 1 | 0.05 | 0 | 0 | 1 | 0.05 | 6 | 0.29 | 1 | 0.05 |
| Spain | Y | C | 303 | 0.64 | 149 | 0.31 | 170 | 0.36 | 332 | 0.71 | 313 | 0.67 |
| Sweden | Y | C | 6 | 0.06 | 3 | 0.03 | 1 | 0.01 | 10 | 0.10 | 7 | 0.07 |
| EU Total 27 | 719 | 0.17 | 460 | 0.11 | 523 | 0.12 | 942 | 0.22 | 771 | 0.18 | ||
| United Kingdom | – | – | – | – | – | – | 9 | 0.01 | 19 | 0.03 | 9 | 0.01 |
| EU Total c | 719 | 0.17 | 460 | 0.11 | 523 | 0.12 | 951 | 0.19 | 790 | 0.16 | ||
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway | Y | C | 4 | 0.07 | 4 | 0.07 | 5 | 0.09 | 8 | 0.15 | 5 | 0.09 |
| Liechtenstein | Y | C | 0 | 0 | 0 | 0 | 53 | 0.61 | 102 | 1.2 | 51 | 0.60 |
| Switzerland d | Y | C | 89 | 1.0 | 111 | 1.3 | ||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Not notifiable, no surveillance system exists.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years from 2018 to 2020.
Most Q fever cases (83.0%; N = 597) were reported to have been acquired in the EU, representing an increase compared with 2021 (78%), 2020 (66.3%) and 2018 (79.6%), but in line with 2019 (85.2%). France, Germany, Hungary, the Netherlands, Slovenia and Sweden reported travel‐associated cases. Five cases (0.70%) were imported from outside the EU, namely from Angola, Bosnia and Herzegovina, the Democratic Republic of the Congo, The Gambia and Iraq. For 117 cases (16.3%), there were no data on travel or the country of infection (Table 67).
In 2022, cases occurred year‐round. Most Q fever cases occurred from April to August, in line with the spring/summer seasonal pattern (Figure 29).
FIGURE 29.
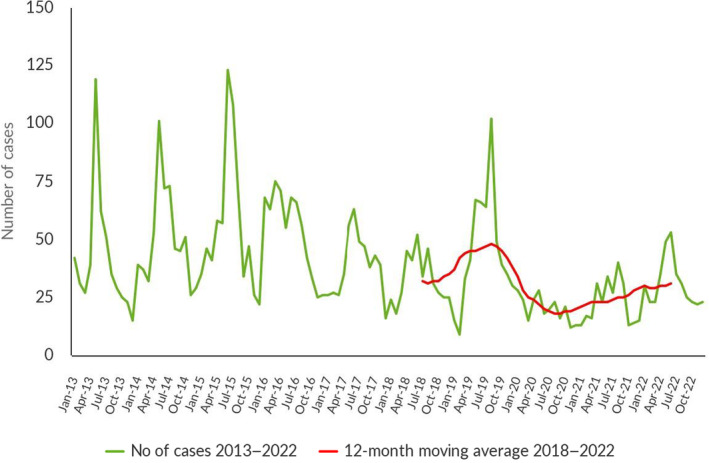
Trend in reported confirmed human cases of Q fever in the EU by month, 2018–2022. Source: Cyprus, Czechia, Estonia, Finland, France, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia and Sweden.
The number of Q fever cases increased compared with 2021. However, the overall Q fever trend in 2018–2022 did not show a significant increase or decrease in the EU. At the country level, a significantly decreasing trend was observed in Portugal (p < 0.05).
In 2022, 14 MSs reported outcomes for 445 cases (61.9%; N = 445), an increase compared with 2021 (58.7%). The highest number of outcomes were reported from Spain (208), Hungary (67) and Germany (63). A total of four deaths were reported from Portugal (1) and Spain (3) and were recorded in patients from 35 to 70 years old, resulting in an EU case fatality of 0.90% – a decrease compared with 2021 (1.5%).
4.3.3 Coxiella burnetii in animals
Sheep
Thirteen MSs and three non‐MSs (Republic of North Macedonia, Serbia and Switzerland) reported results for a total of 1647 animals and 2940 flocks. At the animal level, direct detection tests (N = 1015; 6.8% positive) were used more frequently than serological tests (N = 632; 10.6% positive). The Netherlands reported nearly half of the direct detection tests (N = 492; 0.0% positive). At the herd level, serological tests were only reported by Italy (N = 128, 97.7% positive). Most direct detection tests were reported by Poland (N = 2320; 0.34% positive), Belgium (N = 182; 12.6% positive), Italy (N = 151; 43.7% positive) and Spain (N = 150; 26.7% positive).
Goats
Ten MSs and one non‐MS (Switzerland) reported results for a total of 1249 animals and 1271 herds. At the animal level, direct detection tests (N = 1109; 2.8% positive) were more frequently used than serological tests (N = 140; 17.9% positive). The Netherlands and Switzerland reported most direct detection tests (N = 826; 0.0% positive and N = 148; 7.4% positive, respectively). Serological tests at the animal level were mainly reported by Italy (N = 55, 7.3% positive) and Slovakia (N = 34, 0.0% positive). At the herd level, almost all tests were direct detection tests, mostly carried out by Poland (N = 878; 0.0% positive), Belgium (N = 252; 7.9% positive), Italy (N = 28; 10.7% positive) and Spain (N = 27; 70.4% positive).
Cattle
Sixteen MSs and five non‐MSs (Iceland, Norway, Republic of North Macedonia, Serbia and Switzerland) provided data. In total, 11,855 animals and 4134 herds were tested. At the animal level, direct detection tests were less often employed (N = 4589; 8.5% positive) than serological tests (N = 7146; 2.8% positive). Italy (N = 3156; 0.91% positive), Austria (N = 1580; 5.8% positive), Slovakia (N = 1147; 2.1% positive) and Ireland (N = 649; 2.9% positive) provided 89.7% of the serological tests, whereas Switzerland tested 3322 animals using direct detection tests, resulting in 10.5% positivity. At the herd level, most tests involved direct detection methods. Results were mainly reported by Belgium (N = 2012; 7.5% positive) and Poland (N = 1815; 6.8% positive). Bulgaria and Iceland reported most of the herd‐level data obtained using serological methods (N = 91; 31.9% positive and N = 81; 0.0% positive, respectively).
Other animal species
Four MSs (Austria, Ireland, Italy and Slovakia) and two non‐MSs (Norway and Switzerland) reported data on animals other than sheep, goats and cattle. In total, seven herds and 396 animals were tested from various domestic and wild animal species, such as other ruminant species (water buffalo, alpaca, etc.), pigs, pets (dogs), birds and diverse other species. Positivity was reported only in Italy, mainly in wild birds (13.8% positive samples out of 29 tested with direct detection methods), dogs (5.9% positive samples out of 17 tested with serological methods, and none positive out of 8 tested with direct detection methods), water buffalos (1.8% positive out of 226 animals tested with serological methods, and six herds found negative with direct detection methods) and pigs (one herd tested, which resulted positive with serological methods, and two animals tested and found negative with direct detection methods).
4.4 Discussion
Q fever, caused by C. burnetii, affects humans and animals. Due to its microbial characteristics that include high virulence, environmental resistance and aerosol dissemination, it is classified as a potential biological weapon. Humans mainly acquire the infection through environmental contamination arising from bacterial shedding in infected animals, but also possibly through tick‐borne transmission and a foodborne route (Basanisi et al., 2022). In Europe, the majority of clinical cases are sporadic. However, several outbreaks among humans have been reported. Up to 2016, France and Germany reported most of the confirmed cases. In 2017, two outbreaks were reported from Bulgaria in the Gabrovo and Blagoevgrad regions (Genova‐Kalou et al., 2019). Year 2021 saw the lowest number of human Q fever cases in the EU; Germany and Spain accounted for more than 50% of the overall number of cases (ProMED‐mail, 2021; Hurtado et al., 2023). Since 2017, Spain has reported the highest number of cases annually. The increase in the number of human cases reported by Spain is most likely explained by a change in their reporting system from voluntary to mandatory (Christodoulou et al., 2023).
In 2022, the number of human Q fever cases increased compared with the 2020–2021 pandemic years but was similar to that reported during the pre‐pandemic period. France, Germany, Hungary and Spain accounted for about 78.2% of cases. An outbreak of Q fever (20 confirmed cases), through airborne transmission, was recorded in Croatia and was linked to non‐occupational exposure in a semi‐urban area in Čavle, due to environmental contamination on three farms (Tomljenovic et al., 2023). However, the Q fever trend for the 2018–2022 period did not show a significant increase or decrease in the EU. In 2022, the percentage of case fatality showed a reduction (0.90%) compared with 2021 (1.5%).
The results obtained from animals – mainly from small ruminants and cattle – are insufficient for analysing trends for Q fever at the EU level. The start of annual EU reporting in 2021 (Q fever is a ‘Category E' disease in the new EU Animal Health Law) has had little impact on reporting data harmonisation among countries. The results submitted by different MSs and non‐MSs are not directly comparable, mainly due to differences in sampling strategy (sample types, testing methods, coverage of the monitoring), data completeness and sensitivity of the surveillance method. Progress has been made in acquainting reporting countries with analytical methods, but agreement among EU MSs on case definitions at the animal and herd levels is still lacking to obtain a proper appraisal of the Q fever situation in domestic ruminants. Animal species other than farmed ruminants (such as pets or wild animals) may be considered as potential reservoirs of C. burnetii and can be included in epidemiological investigations if needed (Georgiev et al., 2013). For example, in 2022, a clinical investigation in Italy reported noteworthy positivity in tissue samples from ‘wild birds’ living in their natural habitat. In the coming years, it is of utmost importance to investigate and identify the source of C. burnetii infection and the persistence of environmental contamination (Carrié et al., 2019; Hurtado et al., 2023). The major challenge is to reduce human exposure to this zoonosis through a preventive ‘One Health’ approach.
5 WEST NILE VIRUS
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
5.1 Key facts
In 2022, there were 1133 confirmed and probable cases of human West Nile virus infection, corresponding to an European Union notification rate of 0.26 cases per 100,000 population. This represented an increase of 631.8% in locally acquired cases, compared with 2021.
During the past 5 years, two unusually intense transmission seasons were documented in 2018 and 2022, but the overall trend for human West Nile virus infections showed no significant increase or decrease during the 2018–2022 period.
In 2022, 431 birds and 166 equines tested positive for West Nile virus, as reported to EFSA. This represent an increase of 195.2% and 245.8% respectively compared with 2021. West Nile virus extended its geographical area, affecting birds and equines, and emerged during 2022 on the Atlantic coast in France. Its incidence increased in the North of Germany and in the South of Italy. In 2022, 364 outbreaks in animals were reported to the European Union Animal Diseases Information System by nine Member States, with the number of avian outbreaks (263) reported for 2022 being the highest since 2018. Italy, Germany, Spain, Austria and Hungary all reported outbreaks in birds to the European Union Animal Diseases Information System, with Italy and Germany reporting the highest numbers (76.1% and 19.4% respectively).
Nine Member States reported outbreaks in equids to the European Union Animal Diseases Information System, with the highest proportion in Italy, Germany and Greece, accounting for 46.5%, 15.8% and 8.9% of the total number of outbreaks, respectively.
5.2 Surveillance and monitoring of West Nile virus in the EU
5.2.1 Humans
In 2022, 26 MSs reported data on WNV infection in humans. Surveillance is mandatory in 24 MSs, in France it is voluntary, and Germany did not specify their surveillance system. No surveillance system is in place in Denmark. The EU case definition was used by 24 MSs, France reported another case definition, and Germany did not specify the case definition used. All countries except Germany had a comprehensive surveillance system. The WNV surveillance systems cover the whole population in all MSs and all countries reported case‐based data.
For the human disease due to West Nile virus, ECDC uses term WNV infection in line with WHO ICD‐11. That includes the febrile form (West Nile Fever (WNF)) and the neurological form (WNND), as well as asymptomatic infections. About 80% of WNV infections in humans are asymptomatic.
5.2.2 Animals
From a veterinary standpoint, WNV is the causative agent of WNF, a disease that develops into asymptomatic forms, benign forms (flu‐like syndrome) and neuro‐invasive forms (WOAH, 2023) in line with the World Organisation for Animal Health (WOAH) terminology. WWNV surveillance in animals involves mostly passive surveillance, including surveillance based on the diagnosis of neuro‐invasive cases in equids, but some countries implement active surveillance of equids and/or captive birds and/or wild birds. Alongside EU MSs, Serbia and Switzerland submit reports to EFSA on animal surveillance and monitoring activities in animals. Two sources of information are used to complete this report. Firstly, data are submitted to EFSA by EU MSs, Serbia and Switzerland from annual surveillance and monitoring activities in accordance with Directive 2003/99/EC. 59 WNV is listed in Annex I, Part B (viruses transmitted by arthropods) as a virus to be monitored, according to the epidemiological situation in a MS, in compliance with Article 4.1 of the same Directive. Secondly, it is mandatory for MSs to notify outbreaks of equine and avian WNV to ADIS, 60 in accordance with CIR (EU) 2020/2002. 61
5.3 Results
5.3.1 Overview of key statistics, EU, 2018–2022
In 2022, WNV cases were reported in humans, equids and birds. Over the past 5 years, the number of countries reporting surveillance data in animals and humans has been relatively stable (Table 69).
TABLE 69.
Summary of WNV infection statistics relating to humans, birds and equids EU, 2018–2022.
| 2022 | 2021 | 2020 | 2019(a) | 2018(a) | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed and probable cases | 1133 | 158 | 333 | 442 | 1612 | ECDC |
| Total number of confirmed and probable cases/100,000 population (notification rates) | 0.26 | 0.04 | 0.08 | 0.09 | 0.32 | ECDC |
| Number of reporting MSs | 26 | 26 | 26 | 27 | 27 | ECDC |
| Infection acquired in the EU | 1124 | 153 b | 331 | 435 | 1573 | ECDC |
| Infection acquired outside the EU | 6 | 5 | 2 | 5 | 29 | ECDC |
| Unknown travel status or unknown country of infection | 3 | 0 | 0 | 2 | 10 | ECDC |
| Animals | ||||||
| Birds | ||||||
| Number of animals tested c | 18,882 | 19,640 | 11,141 | 14,932 | 13,970 | EFSA |
| Number of positive animals by PCR‐based methods | 431 | 146 | 165 | 104 | 425 | EFSA |
| Number of MSs reporting surveillance/monitoring data to EFSA | 14 | 13 | 11 | 13 | 11 | EFSA |
| Number of outbreaks notified to ADIS | 263 | 8 | 2 | 53 | 22 | ADIS |
| Number of MSs notifying outbreaks to ADIS | 5 | 2 | 1 | 2 | 6 | ADIS |
| Equids | ||||||
| Number of animals tested | 4336 | 6114 | 6749 | 5563 | 13,785 | EFSA |
| Number of positive animals by PCR d ‐based methods | 0 | 1 | 1 | 4 | 7 | EFSA |
| Number of animals positive for IgM by ELISA | 166 | 47 | 209 | 74 | 393 | EFSA |
| Number of MSs reporting surveillance/monitoring data to EFSA | 13 | 14 | 14 | 14 | 12 | EFSA |
| Number of outbreaks notified to ADIS | 101 | 45 | 189 | 100 | 292 | ADIS |
| Number of MSs notifying outbreaks to ADIS | 9 | 7 | 9 | 8 | 10 | ADIS |
Abbreviations: ADIS, Animal Disease Information System; ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; ELISA, enzyme‐linked immunosorbent assay; MSs, Member States; PCR, polymerase chain reaction.
Data from the United Kingdom are taken into account for 2017–2019, because the United Kingdom was an EU MS, but it became a third country on 1 February 2020.
One case reported from the EU was later found to have originated in Mayotte.
Samples tested using an unspecified analytical method are not included.
PCR: polymerase chain reaction.
The number of probable and confirmed human cases of (WNV) infection reported in 2022 was 1133, corresponding to an EU notification rate of 0.26 per 100,000 population. This was the second highest notification rate reported, after 2018.
While the number of tested equids appears to have remained stable since 2019, there has been an overall increase in the number of tested birds since 2020, reflecting an intensification of the surveillance system in place.
More detailed descriptions of these statistics are provided in the subsections below.
5.3.2 West Nile virus infections in humans
In 2022, 1133 confirmed and probable cases of WNV infections in humans were reported (including 987 confirmed infections), corresponding to an EU notification rate of 0.26 per 100,000 population. This was the second highest notification rate reported during the period 2018–2022 (Table 69).
Among all reported confirmed and probable WNV infections, 1124 (99.2%) were acquired in the EU (Table 69), six cases (0.53%) were acquired outside the EU (Israel, Morocco, Serbia, Senegal, United States) and in three cases the travel status or country of infection is unknown (Table 69).
Among the 1124 cases acquired in the EU, 1111 were locally acquired, i.e. within the reporting MS (Table 70), thirteen were imported from another EU country. The EU notification rate of locally acquired cases increased by 631.8% compared with 2021 (Table 70).
TABLE 70.
Locally acquired human West Nile virus (WNV) infection cases (confirmed and probable) and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format(a) | Confirmed cases | Total cases and rate | Total cases and rate | Total cases and rate | Total cases and rate | Total cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | ||||
| Austria | Y | C | 6 | 6 | 0.07 | 3 | 0.03 | 0 | 0 | 4 | 0.05 | 21 | 0.24 |
| Belgium | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Bulgaria | Y | C | 1 | 1 | 0.01 | 0 | 0 | 1 | 0.01 | 5 | 0.07 | 15 | 0.21 |
| Croatia | Y | C | 5 | 5 | 0.13 | 0 | 0 | 0 | 0 | 0 | 0 | 58 | 1.4 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 23 | 2.6 | 1 | 0.12 |
| Czechia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 5 | 0.05 |
| Denmark b | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | Y | C | 3 | 6 | 0.01 | 1 | < 0.01 | 0 | 0 | 2 | < 0.01 | 27 | 0.04 |
| Germany | Y | C | 17 | 17 | 0.02 | 4 | < 0.01 | 22 | 0.03 | 5 | 0.01 | 1 | < 0.01 |
| Greece | Y | C | 172 | 286 | 2.7 | 59 | 0.55 | 144 | 1.3 | 227 | 2.1 | 315 | 2.9 |
| Hungary | Y | C | 9 | 14 | 0.14 | 7 | 0.07 | 3 | 0.03 | 36 | 0.37 | 215 | 2.2 |
| Ireland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Italy | Y | C | 723 | 723 | 1.2 | 65 | 0.11 | 69 | 0.12 | 54 | 0.09 | 610 | 1.0 |
| Latvia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Lithuania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | Y | C | 0 | 0 | 0 | 0 | 0 | 8 | 0.05 | 0 | 0 | 0 | 0 |
| Poland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Portugal | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Romania | Y | C | 47 | 48 | 0.25 | 7 | 0.04 | 6 | 0.03 | 67 | 0.35 | 277 | 1.4 |
| Slovakia | Y | C | 0 | 1 | 0.02 | 0 | 0 | 0 | 0 | 1 | 0.02 | 0 | 0 |
| Slovenia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0.19 |
| Spain | Y | C | 4 | 4 | 0.01 | 6 | 0.01 | 77 | 0.16 | 0 | 0 | 0 | 0 |
| Sweden | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EU Total 27 | – | – | 987 | 1111 | 0.25 | 152 | 0.03 | 330 | 0.07 | 425 | 0.10 | 1549 | 0.35 |
| United Kingdom c | – | – | – | – | – | – | – | – | – | 0 | 0 | 0 | 0 |
| EU Total | – | – | 987 | 1111 | 0.25 | 152 | 0.03 | 330 | 0.07 | 425 | 0.08 | 1549 | 0.31 |
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Liechtenstein | Y | C | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 1 | 0.01 | 0 | 0 |
| Switzerland d | Y | C | 0 | 0 | 0 | 0 | 0 | ||||||
Abbreviation: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Not notifiable, no surveillance system exists.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
Eleven EU MSs (Austria, Bulgaria, Croatia, France, Germany, Greece, Hungary, Italy, Romania, Slovakia, Spain) reported at least one locally acquired confirmed or probable human case of WNV infection in 2022. Most of the locally acquired infections were reported by Italy and Greece, accounting respectively for 65.1% and 25.7% of the total number of probable/confirmed cases in the EU.
Of the 1111 cases of probable/confirmed human infection that were locally acquired in 2022, 710 involved males (64.0%), and over 81.5% of cases occurred in people aged 50 or older.
Eight EU MSs reported locally acquired infections in humans and provided data on the hospitalisation status of their cases. Of the cases with known hospitalisation status (366 cases, 32.9% of total infections) in 2022, 86.9% (N = 318) were hospitalised.
Clinical manifestations were reported for 1109 locally acquired cases (99.8%), while 10.1% (N = 112) were asymptomatic. Among the humans with symptoms, 53.3% (N = 591) of infections were neuro‐invasive (Table 71). This compares with 63.2% (N = 96) neuro‐invasive and 16.4% (N = 25) asymptomatic infections in 2021.
TABLE 71.
Locally acquired human West Nile neuro‐invasive disease (WNND) cases (confirmed and probable) and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases | Total cases and rate | Total cases and rate | Total cases and rate | Total cases and rate | Total cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | ||||
| Austria | Y | C | 1 | 1 | 0.01 | 1 | 0.01 | 0 | 0 | 1 | 0.01 | 4 | 0.05 |
| Belgium | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Bulgaria | Y | C | 1 | 1 | 0.01 | 0 | 0 | 1 | 0.01 | 4 | 0.06 | 13 | 0.18 |
| Croatia | Y | C | 3 | 3 | 0.08 | 0 | 0 | 0 | 0 | 0 | 0 | 47 | 1.1 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 20 | 2.3 | 1 | 0.12 |
| Czechia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.01 | 3 | 0.03 |
| Denmark b | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Finland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| France | Y | C | 2 | 3 | 0 | 0 | 0 | 0 | 0 | 1 | < 0.01 | 7 | 0.01 |
| Germany | Y | C | 7 | 7 | 0.01 | 2 | < 0.01 | 7 | 0.01 | 3 | < 0.01 | 0 | 0 |
| Greece | Y | C | 135 | 184 | 1.7 | 38 | 0.36 | 116 | 1.1 | 140 | 1.3 | 241 | 2.2 |
| Hungary | Y | C | 8 | 11 | 0.11 | 7 | 0.07 | 1 | 0.01 | 23 | 0.24 | 152 | 1.6 |
| Ireland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Italy | Y | C | 330 | 330 | 0.56 | 35 | 0.06 | 46 | 0.08 | 24 | 0.04 | 243 | 0.40 |
| Latvia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Lithuania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Luxembourg | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | Y | C | 0 | 0 | 0 | 0 | 0 | 6 | 0.03 | 0 | 0 | 0 | 0 |
| Poland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Portugal | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Romania | Y | C | 46 | 47 | 0.25 | 7 | 0.04 | 6 | 0.03 | 65 | 0.33 | 277 | 1.4 |
| Slovakia | Y | C | 0 | 1 | 0.02 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Slovenia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 0.19 |
| Spain | Y | C | 3 | 3 | 0.01 | 6 | 0.01 | 72 | 0.15 | 0 | 0 | 0 | 0 |
| Sweden | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EU Total 27 | – | – | 536 | 591 | 0.13 | 96 | 0.02 | 255 | 0.06 | 282 | 0.06 | 992 | 0.23 |
| United Kingdom c | – | – | – | – | – | – | – | – | – | 0 | 0 | 0 | 0 |
| EU Total | – | – | 536 | 591 | 0.13 | 96 | 0.02 | 255 | 0.06 | 282 | 0.06 | 992 | 0.20 |
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Liechtenstein | Y | C | 0 | 0 | 0 | 0 | 0 | – | – | – | – | – | – |
| Switzerland d | Y | C | 0 | – | – | – | – | ||||||
Abbreviations: WNND, West Nile Neuro‐invasive Disease; –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
Not notifiable, no surveillance system exists.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
In 2022, the remaining 406 cases (36.6%) were symptomatic with non‐neurological symptoms. This compares with 31 cases (20.4%) in 2021.
Data on the outcome of infections were reported for all of the 1111 locally acquired cases. In 2022, 92 deaths were reported among cases with WNV infections, compared with 11 in 2021. The case fatality rate was 8.3% (7.2% in 2021) among all locally acquired WNV infections and 15.6% (10.4% in 2021) among locally acquired WNV infections with WNND.
5.3.3 West Nile virus infections in animals
In 2022, 18 EU MSs, Serbia and Switzerland submitted WNV monitoring and surveillance data from birds and/or equids to EFSA. Nine MSs notified outbreaks in birds or in equids to ADIS. Italy and Germany notified the highest numbers of outbreaks in birds (76.1% and 19.4%, respectively), whereas Italy notified 46.5% of the total number of equine outbreaks. Some countries did not submit WNV data to either ADIS or EFSA in 2022.
Table 72 displays 2022 summary data from both data sources, for birds and equids, by reporting country. In some cases, the comparison may show discrepancies, so the following points should be taken into consideration for interpreting the data. Firstly, the reported number of animals tested based on surveillance activities submitted to EFSA includes the following registered methods: detection of IgG and IgM antibodies, seroneutralisation and the detection of flavivirus or WNV genomes using a PCR‐based method. Samples tested using an unspecified analytical method are not included. Secondly, some countries did not report confirmed outbreaks among birds to ADIS, while nevertheless including them in their national reports submitted to EFSA. Thirdly, an outbreak notified to ADIS can refer to more than one infected animal if they constitute a single epidemiological unit and/or are from the same location. Lastly, the number of positive animals includes cases for which the disease was confirmed clinically and/or in a laboratory, either by the detection of IgM‐specific antibodies indicating a recent infection by WNV (available for equids only), or by the detection of the WNV genome using a PCR‐based method indicating an ongoing infection (for both birds and equids). Results of serum neutralisation testing and IgG ELISA, including observation of seroconversion in avian or equid sentinel animals by detecting specific neutralising antibodies, are not included because it is not possible to determine when the infection occurred.
TABLE 72.
Summary of WNV surveillance/monitoring results in animals reported to EFSA, and WNV outbreaks notified to ADIS, by EU MSs and non‐MS countries, 2022.
| Country (EU MSs, non‐EU country) a | Birds | Equids | |||||
|---|---|---|---|---|---|---|---|
| Data on surveillance activities submitted to EFSA | N (%) outbreaks in ADIS | Data on surveillance activities submitted to EFSA | N (%) outbreaks in ADIS | ||||
| N (%) animals tested | N (%) animals positive using PCR‐based methods b | N (%) animals tested | N (%) animals positive using ELISA‐IgM(c) | N (%) animals positive using PCR‐based methods b | |||
| Austria | 171 (0.91) | 3 (0.70) | 2 (0.76) | 16 (0.37) | 1 (0.60) | 0 (0) | 1 (0.99) |
| Bulgaria | 64 (0.34) | 0 (0) | NR | NR | NR | NR | NR |
| Croatia | NR | NR | NR | NR | NR | NR | 8 (7.9) |
| Cyprus | 472 (2.5) | – | NR | 122 (2.8) | 0 (0) | – | NR |
| Czechia | NR | NR | NR | 853 (19.7) | 33 (19.9) | – | NR |
| Denmark | 390 (2.1) | 0 (0) | NR | NR | NR | NR | NR |
| Finland | 4 (0.02) | 0 (0) | NR | NR | NR | NR | NR |
| France | 152 (0.80) | 0 (0) | NR | 38 (0.88) | 9 (5.4) | 0 (0) | 6 (5.9) |
| Germany | 1896 (10.0) | 54 (12.5) | 51 (19.4) | 101 (2.3) | 17 (10.2) | – | 16 (15.8) |
| Greece | 41 (0.22) | 0 (0) | NR | 1341 (30.9) | 12 (7.2) | 0 (0) | 9 (8.9) |
| Hungary | 6 (0.03) | 0 (0) | 1 (0.38) | 25 (0.58) | ‐ | 0 (0) | 3 (3.0) |
| Italy | 12,102 (64.1) | 365 (84.7) | 200 (76.1) | 1155 (26.6) | 82 (49.4) | – | 47 (46.5) |
| Portugal | NR | NR | NR | 3 (0.07) | 3 (1.8) | – | 3 (3.0) |
| Romania | 53 (0.28) | – | NR | NR | NR | NR | NR |
| Slovakia | NR | NR | NR | 52 (1.2) | 0 (0) | – | NR |
| Slovenia | 48 (0.25) | 0 (0) | NR | 1 (0.02) | – | 0 (0) | NR |
| Spain | 3325 (17.6) | 9 (2.1) | 9 (3.4) | 628 (14.5) | 9 (5.4) | 0 (0) | 8 (7.9) |
| Sweden | 158 (0.84) | 0 (0) | NR | 1 (0.02) | 0 (0) | – | NR |
| EU Total (27 + XI) | 18,882 (100) | 431 (100) | 263 (100) | 4336 (100) | 166 (100) | 0 (0) | 101 (100) |
| Serbia | 431 | 25 | NR | 1853 | 25 | – | NR |
| Switzerland | NR | NR | NR | 18 | – | 0 | NR |
Abbreviations: ADIS, Animal Disease Information System; MSs, Member States. NR: No reporting by the relevant Member State. –: Analytical method specified in the column header not used.
: Analytical method in the column header used with negative results.
Samples tested with an unspecified analytical method are not included.
PCR: polymerase chain reaction (for identification of the virus genome).
ELISA: enzyme‐linked immunosorbent assay.
Figure 30 displays the geographical distribution of outbreaks in animals (ADIS data) together with the geographical distribution of locally acquired West Nile virus infections among humans.
FIGURE 30.
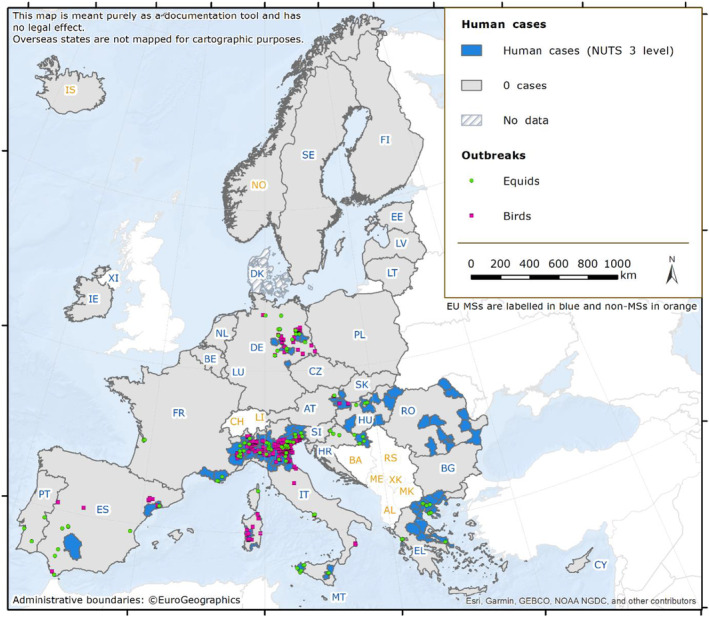
Geographical distribution of locally acquired West Nile virus infections among humans (NUTS 3 level*) and outbreaks notified to ADIS among equids and birds (X,Y coordinates) across the EU, 2022 transmission season. *The NUTS (Nomenclature of territorial units for statistics) are a hierarchical system divided into three levels. NUTS 1: major socio‐economic regions, NUTS 2: basic regions for the application of regional policies, NUTS 3: small regions for specific diagnoses (https://ec.europa.eu/eurostat/web/gisco/geodata/reference‐data/administrative‐units‐statistical‐units/nuts)
In birds, 14 MSs reported a total of 18,882 analysed samples as part of their surveillance and monitoring activities (Tables 69, 72). Italy and Spain submitted 64.1% and 17.6% of these data respectively, while a total of 431 infected birds were reported to EFSA by Austria, Germany, Italy and Spain (Table 72). This represents a relative increase of 195.2% compared with 2021. WNV infections occurred in crows, doves, goshawks, jays, magpies, owls, Passeriformes, pheasants, pigeons and starlings. The same four MSs plus Hungary reported avian outbreaks to ADIS. Serbia, a non‐EU country, reported 431 analyses with 25 PCR‐positive animals to EFSA.
In equids, 13 MSs reported a total of 4336 analysed samples to EFSA as part of their surveillance and monitoring activities (Tables 69, 72). Eight MSs reported a total of 166 equid cases that were confirmed by ELISA IgM (Table 72) which represents a relative increase of 245.8% compared with 2021. Czechia reported 33 ELISA IgM positive animals, accounting for 19.9% of the total number of WNV‐positive animals reported to EFSA. Two non‐EU countries, Serbia and Switzerland, reported 1853 and 18 analyses with respectively 25 and no ELISA‐IgM confirmed positives. Nine MSs (Austria, Croatia, France, Germany, Greece, Hungary, Italy, Portugal and Spain) reported a total of 101 equid outbreaks to ADIS. The highest number of outbreaks were reported by Italy, Germany and Greece, accounting for 46.5%, 15.8%, 8.9% of the total number of outbreaks respectively, amounting to 71% of all notified outbreaks. Serbia and Switzerland did not report outbreaks in equids to ADIS.
Moreover, Serbia and Denmark reported a total of 1740 tested cattle samples and 18 bat samples to EFSA, as part of their surveillance and monitoring activities. Serbia reported 140 PCR‐positive animals to EFSA. No bats were found to be infected by West Nile virus.
5.3.4 Joint analysis of trends and seasonality
WNV is endemic in several EU countries and both animal and human cases of WNV infections are reported every year (Figure 31). Infections in Europe occur seasonally, with most cases being reported between July and September (Figure 32). During the past 5 years, two unusually intense transmission seasons were documented in 2018 and 2022, with no significant trend (p = 0.77) in the overall 5‐year period (Figure 31). In 2022, the number of reported cases of locally acquired WNV human infections (total = 1111; Table 69, Figure 32) and of WNV outbreaks in animals (total = 364; Table 69; Figure 33) were the highest since 2018.
FIGURE 31.
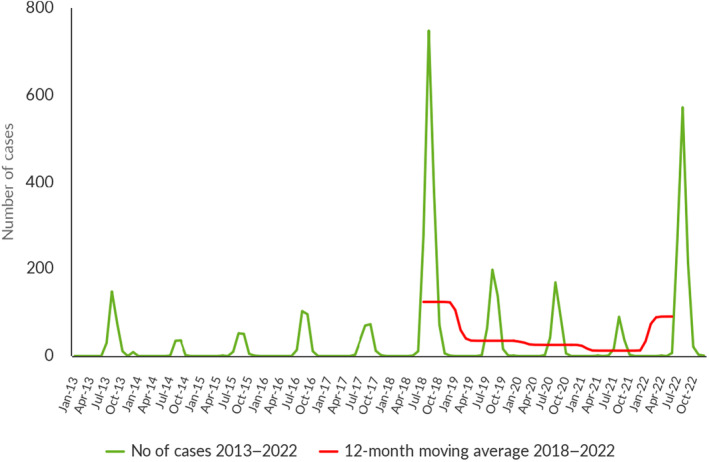
Trend in locally acquired human WNV infections reported in EU MSs, by month, 2018–2022. Source: Austria, Belgium, Bulgaria, Cyprus, Czechia, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden.
FIGURE 32.
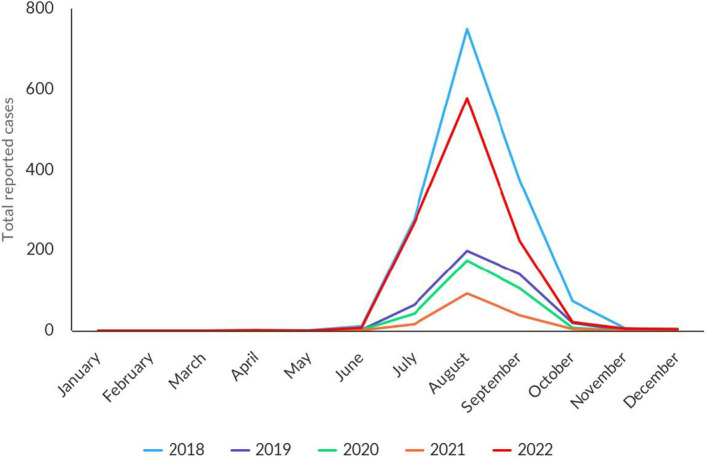
Reported human cases of West Nile virus infection in EU MSs, by month, 2018–2022. Note: The data set includes only locally acquired WNF cases and only countries that consistently reported cases (or reported zero cases) over the whole reporting period (last 5 years) and to the level of detail required for trend analysis (not aggregated).
FIGURE 33.
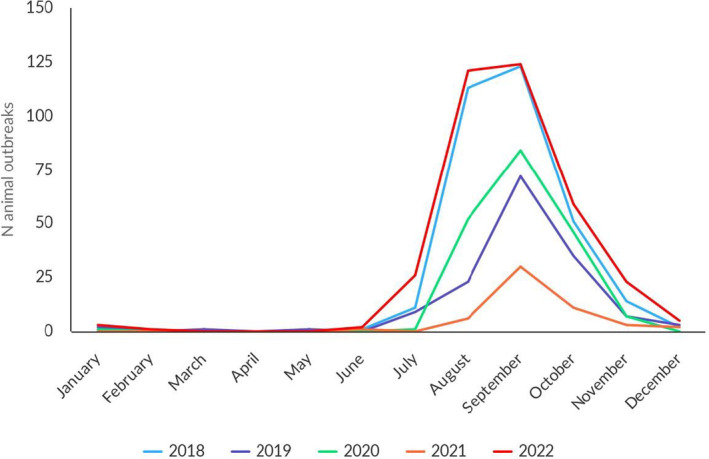
Outbreaks of West Nile infection in birds and equids in EU MSs, by month, 2018–2022. Data source: ADIS for animal outbreaks.
As in 2018, the 2022 WNV transmission season started earlier than in non‐epidemic years, with the first locally acquired human case 62 and the first animal outbreak reported within Europe in June, with cases peaking in August among humans, as in previous years, (Figure 32) and among animals in early August–September (101 outbreaks, Figure 33). The trend of WNV outbreaks detection in birds and equids is similar to the one observed in 2018.
5.4 Discussion
Human cases of WNV infection are reported every year in some EU MSs, while in others WNV is only diagnosed in people who have travelled in endemic areas. The number of EU MSs reporting local WNV transmission has increased in recent years (Hubálek and Halouzka, 1999; Sikkema et al., 2020; Young et al., 2021). In 2022, all the countries that reported locally acquired cases of WNV infection in humans had also reported locally acquired cases in the past. The majority of EU MSs reported cases in birds and equids to either EFSA or ADIS. Nevertheless, some countries did not submit monitoring and surveillance data this year.
WNV circulation is influenced by environmental conditions, such as low precipitation in winter and high spring temperatures (Marini et al., 2021; Farooq et al., 2022). These conditions can contribute to the spread and density of Culex mosquitoes, consequently enhancing virus replication in the vector (Reisen et al., 2006; Fornasiero et al., 2020). During the period 2018–2022, two unusually intense levels of transmission were documented in 2018 and 2022.
In 2022, the number of reported human cases and reported animal outbreaks was the highest since 2018, and the WNV transmission season started earlier than in non‐epidemic years. Most human and animal infections were reported in Italy (Riccardo et al., 2022), where reported human cases were even higher than in 2018, and in Greece (Pervanidou et al., 2023). However, both countries experienced more localised WNV transmission in 2022 than in 2018, the most severely affected areas being north‐eastern Italy and northern and central Greece.
This unusually high localised level of transmission was also driven, in Italy, by the re‐emergence of WNV lineage 1, following several years of low‐level circulation, with increased transmission in humans and birds (Barzon et al., 2022). The increase was not associated in 2022 with any substantial changes in the surveillance system that could have increased its sensitivity, compared with previous years. The surveillance of WNV in Italy is currently regulated by a national plan in place since 2020 (Italian Ministry of Health, 2019).
Noteworthily, the emergence of WNV (three positive equine cases) was notified in southwestern France, in the Nouvelle Aquitaine region, close to Bordeaux. The distribution of WNV extended to the north of Germany, with equine and avian cases reported. Moreover, for the first time, avian cases were detected in southern Italy.
The number of avian cases reported to EFSA was the highest for the past 4 years, once again reaching the level of 2018. The number of outbreaks in birds notified to ADIS was the highest ever.
Although the number of tested equines reported to EFSA was the lowest since 2018, the number of positive animals was the highest. The two major lineages of WNV (lineage 1 and lineage 2) are considered endemic in Europe. They are derived from a limited number of independent introductions from Africa, followed by local spread and evolution. Lineage 2 has become the dominant lineage over the past few years and has been associated with significant human epidemics (Papa et al., 2011; Hernández‐Triana et al., 2014; Beck et al., 2020; Pacenti et al., 2020). During the 2021 transmission season, the re‐introduction of WNV lineage 1 was confirmed in Italy. In 2022, the circulation of WNV lineage 1 increased notably in humans and birds in north‐eastern Italy (Barzon et al., 2022), while Greece documented the circulation of WNV lineage 2 (Pervanidou et al., 2020).
The epidemic year of 2018 was marked by a dry winter and warm spring, favouring WNV replication and transmission by mosquitoes (Haussig et al., 2018; Riccardo et al., 2018; Pervanidou et al., 2020). The climatic anomalies of 2022 were different, with higher‐than‐average temperatures and persistent lower‐than‐average rainfall in May/June, followed by severe thunderstorms and flooding from the beginning of July (Riccardo et al., 2022).
With almost 600 reported cases of neuro‐invasive disease and 92 related deaths in 2022, the impact of WNV on human health in EU MSs remains relevant in terms of hospitalisation and death. As in prior years, neuro‐invasive infections continued to be the most frequently reported clinical presentation in 2022. Nevertheless, substantial under‐detection/under‐reporting of clinically asymptomatic and/or mildly symptomatic WNV infections exists and should be considered when reading the data presented. Similarly, most EU countries limit screening of WNV in animals to suspected symptomatic cases.
The ECDC Technical report ‘Surveillance, prevention and control of West Nile virus and Usutu virus infections in the EU/EEA’, published in September 2023 (ECDC and EFSA, 2023b), gave an overview of the WNV epidemiological situation in the EU/EAA. It described the laboratory diagnosis, surveillance systems and preventive measures applied to ensure the safety of substances of human origin, as well as pinpointing the gaps that need to be addressed for a better understanding of the changing epidemiology of WNV in Europe. The Integrated ‘One Health approach’ remains pivotal to acquiring a full picture of WNV monitoring/surveillance and preventing future emergencies.
Integrated One Health active surveillance provides a concrete advantage in the rapid detection and characterisation of WNV circulation across the human–animal interface and can effectively guide action to ensure the safety of substances of human origin (e.g. blood and organs) and improve risk communication (Riccardo et al., 2020). Active surveillance, with planned sampling in sentinels or wild animals, and possibly mosquito screening, allows earlier detection of cases and is useful to indicate when and where to start the screening of blood/organ donors. WNV burden for public and veterinary health must guide policy‐makers in implementing effective monitoring strategies in line with the local context and temporality.
6 TULARAEMIA
The summary data which make up this chapter, as well as additional information on related projects and internet sources, are published for this report on the EFSA Knowledge Junction at Zenodo here. Summary statistics on human surveillance data with downloadable files are retrievable using the ECDC Surveillance Atlas of Infectious Diseases available here.
6.1 Key facts
In 2022, there were 620 confirmed cases of human tularaemia, corresponding to an European Union notification rate of 0.14 cases per 100,000 population. This was a decrease of 29.5% compared with the rate in 2021 (0.20 per 100,000 population).
The overall trend for human Francisella tularensis infections did not show any significant increase or decrease in the 2018–2022 period.
In 2022, F. tularensis was detected by three Member States in five different animal categories. The majority of sampled animals in the European Union (N = 363) were hares with 9.9% positive samples. Other results from animals in the European Union were reported from monkeys, dogs, squirrels, moles, rabbits, other rodents and hares, with extremely small sample sizes, and a few samples were found to be positive.
6.2 Surveillance and monitoring of tularaemia in the EU
6.2.1 Humans
For 2022, 26 EU MSs provided data on tularaemia in humans. There is no surveillance system in place for tularaemia in Denmark. Surveillance is mandatory in all reporting MSs, and is mostly passive, except in Czechia and Slovakia, where surveillance is active. Surveillance systems are comprehensive with full national coverage in all reporting countries. The EU case definition was used by 25 MSs, while Germany and Italy reported using other case definitions. All countries reported case‐based data except Belgium and Bulgaria, which reported aggregated data.
6.2.2 Animals
Tularaemia in animals is an internationally reportable disease (with reporting to WOAH); therefore, at European level, each country receives communications from its veterinary services. In some countries, notification is mandatory under national law. Animal monitoring data on F. tularensis are submitted to EFSA on a voluntary basis by EU MSs and non‐MS countries. Notably, for 2022, three EU MSs (Austria, Finland and Sweden) and one non‐MS (Switzerland) reported these data to EFSA. Surveillance was mostly passive.
6.3 Results
6.3.1 Overview of key statistics, EU, 2018–2022
Table 73 summarises EU‐level statistics on tularaemia in humans and in major animal species, respectively, for 2018–2022. The number of samples and number of animal species tested were higher than in 2021. More detailed descriptions of these statistics are provided in the subsections below.
TABLE 73.
Summary of Francisella tularensis statistics relating to humans and the main animal species, EU, 2018–2022.
| 2022 | 2021 | 2020 | 2019 | 2018 | Data source | |
|---|---|---|---|---|---|---|
| Humans | ||||||
| Total number of confirmed cases | 620 | 881 | 678 | 1319 | 392 | ECDC |
| Total number of confirmed cases/100,000 population (notification rate) | 0.14 | 0.20 | 0.15 | 0.26 | 0.08 | ECDC |
| Number of reporting MSs | 26 | 26 | 26 | 27 | 27 | ECDC |
| Infection acquired in the EU | 475 | 719 | 498 | 1203 | 353 | ECDC |
| Infection acquired outside the EU | 1 | 2 | 2 | 3 | 3 | ECDC |
| Unknown travel status or unknown country of infection | 144 | 160 | 178 | 113 | 36 | ECDC |
| Number of foodborne outbreak‐related cases | 0 | 0 | 0 | 0 | 0 | EFSA |
| Total number of foodborne outbreaks | 0 | 0 | 0 | 0 | 0 | EFSA |
| Animals b | ||||||
| Hares | ||||||
| Number of sampled animals | 363 | 317 | 222 | 211 | 112 | EFSA |
| Number of positive animals | 36 | 70 | 81 | 67 | 20 | EFSA |
| % of positive animals | 9.9 | 22.1 | 36.5 | 31.8 | 17.9 | EFSA |
| Number of reporting MSs | 3 | 3 | 3 | 2 | 2 | EFSA |
| Animals other than hares | ||||||
| Number of sampled animals | 107 | 18 | 5 | 152 | 0 | EFSA |
| Number of positive animals | 8 | 5 | 1 | 8 | 0 | EFSA |
| % of positive animals | 7.5 | 27.8 | 20.0 | 5.3 | – | EFSA |
| Number of reporting MSs | 3 | 3 | 1 | 1 | 0 | EFSA |
Abbreviations: ECDC, European Centre for Disease Prevention and Control; EFSA, European Food Safety Authority; MSs, Member States; –, Data not reported.
Data from the United Kingdom were taken into account for the 2018–2019 period, since the United Kingdom was still an EU MS at that time. However, on 1 February 2020 it became a third country.
The number of sampled animals was obtained by totalling all animal‐level results, sampling stages (natural habitat, unspecified, veterinary activities, veterinary clinics and zoo), sampling strategies (convenience sampling, selective sampling and suspect sampling) and samplers (industry sampling, not applicable and official sampling).
6.3.2 Tularaemia in humans
For 2022, 26 EU MSs reported a total of 620 confirmed cases of tularaemia, with a notification rate of 0.14 cases per 100,000 population. This was a decrease of 29.5% compared with the rate in 2021 (0.20 per 100,000 population). More than 70.0% of cases were reported by Finland, France, Germany and Sweden. In 2022, Sweden had the highest notification rate with 2.1 per 100,000 population, followed by Finland, Slovenia and Lithuania, with 1.7, 0.57 and 0.53 per 100,000 population, respectively (Table 74). A total of 475 tularaemia cases (76.6%) were reported to have been acquired in the EU, which was a decrease compared with 2021 (81.6%) and with 2018 and 2019 (90.1% and 91.2%, respectively). Austria, France, Germany, Poland and Sweden reported travel‐associated cases. Only one case (0.2%) was imported from outside the EU (from Egypt), whereas for 144 cases (23.2%), there were no data on travel or the country of infection (Table 73).
TABLE 74.
Reported confirmed human cases of tularaemia and notification rates per 100,000 population in EU MSs and non‐MS countries, by country and by year, 2018–2022.
| Country | 2022 | 2021 | 2020 | 2019 | 2018 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| National coverage a | Data format a | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | Confirmed cases and rate | ||||||
| Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | Cases | Rate | |||
| Austria | Y | C | 35 | 0.39 | 58 | 0.65 | 33 | 0.37 | 20 | 0.23 | 7 | 0.08 |
| Belgium | Y | A | 7 | 0.06 | 9 | 0.08 | 1 | 0.01 | 4 | 0.03 | 0 | 0 |
| Bulgaria | Y | A | 1 | 0.01 | 0 | 0 | 2 | 0.03 | 1 | 0.01 | 1 | 0.01 |
| Croatia | Y | C | 1 | 0.03 | 0 | 0 | 0 | 0 | 1 | 0.02 | 0 | 0 |
| Cyprus | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Czechia | Y | C | 46 | 0.44 | 50 | 0.47 | 67 | 0.63 | 102 | 0.96 | 32 | 0.30 |
| Denmark b | – | – | – | – | – | – | – | – | – | – | – | – |
| Estonia | Y | C | 3 | 0.23 | 1 | 0.08 | 1 | 0.08 | 2 | 0.15 | 1 | 0.08 |
| Finland | Y | C | 93 | 1.7 | 86 | 1.6 | 143 | 2.6 | 48 | 0.87 | 7 | 0.13 |
| France | Y | C | 63 | 0.09 | 146 | 0.22 | 82 | 0.12 | 85 | 0.13 | 133 | 0.20 |
| Germany | Y | C | 68 | 0.08 | 113 | 0.14 | 59 | 0.07 | 70 | 0.08 | 52 | 0.06 |
| Greece | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hungary | Y | C | 9 | 0.09 | 7 | 0.07 | 20 | 0.20 | 22 | 0.23 | 17 | 0.17 |
| Ireland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Italy | Y | C | 3 | 0.01 | 3 | 0.01 | 0 | 0 | 1 | < 0.01 | 0 | 0 |
| Latvia | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0.10 | 0 | 0 |
| Lithuania | Y | C | 15 | 0.53 | 7 | 0.25 | 2 | 0.07 | 4 | 0.14 | 5 | 0.18 |
| Luxembourg | Y | C | 0 | 0 | 3 | 0.47 | 0 | 0 | 0 | 0 | 0 | 0 |
| Malta | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Netherlands | Y | C | 1 | 0.01 | 5 | 0.03 | 1 | 0.01 | 3 | 0.02 | 2 | 0.01 |
| Poland | Y | C | 33 | 0.09 | 43 | 0.11 | 5 | 0.01 | 21 | 0.06 | 16 | 0.04 |
| Portugal | Y | C | 0 | 0 | 0 | 0 | 1 | 0.01 | 1 | 0.01 | 2 | 0.02 |
| Romania | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Slovakia | Y | C | 4 | 0.07 | 0 | 0 | 12 | 0.22 | 20 | 0.37 | 6 | 0.11 |
| Slovenia | Y | C | 12 | 0.57 | 54 | 2.6 | 1 | 0.05 | 7 | 0.34 | 4 | 0.19 |
| Spain | Y | C | 6 | 0.01 | 4 | 0.01 | 1 | < 0.01 | 88 | 0.19 | 4 | 0.01 |
| Sweden | Y | C | 220 | 2.1 | 292 | 2.8 | 247 | 2.4 | 817 | 8.0 | 102 | 1.0 |
| EU Total 27 | – | – | 620 | 0.14 | 881 | 0.20 | 678 | 0.15 | 1319 | 0.30 | 391 | 0.09 |
| United Kingdom c | – | – | – | – | – | – | – | – | 0 | 0.00 | 1 | 0.00 |
| EU Total | – | – | 620 | 0.14 | 881 | 0.20 | 678 | 0.15 | 1319 | 0.26 | 392 | 0.08 |
| Iceland | Y | C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Norway | Y | C | 58 | 1.1 | 95 | 1.8 | 99 | 1.8 | 183 | 3.4 | 58 | 1.1 |
| Liechtenstein | Y | C | 1 | 2.5 | 2 | 5.1 | 130 | 1.5 | 153 | 1.8 | 113 | 1.3 |
| Switzerland d | Y | C | 114 | 1.3 | 226 | 2.6 | ||||||
Abbreviations: –, Data not reported.
Y, yes; N, no; A, aggregated data; C, case‐based data.
No surveillance system.
Cases reported by the United Kingdom for the period 2018–2019 were also taken into account for this estimation (EU‐28). Data for the United Kingdom were collected for the 2018–2019 period, since it was still an EU MS at that time. However, on 1 February 2020, it became a third country.
Switzerland provided data directly to EFSA. The human data for Switzerland include data from Liechtenstein for the years 2018–2020.
Tularaemia cases mainly occurred from July to November, but cases were observed all throughout the year. In 2022, infections peaked in the end‐of‐summer and early autumn months, in line with the seasonal pattern (Figure 34).
FIGURE 34.
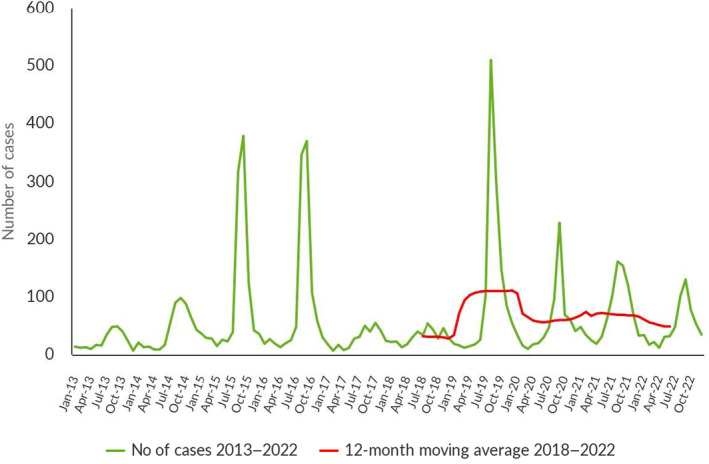
Trends in reported confirmed human cases of tularaemia in the EU, by month and year, 2018–2022. Source: Austria, Cyprus, Czechia, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Luxembourg, Malta, the Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain and Sweden.
In 2022, the number of tularaemia cases decreased compared with 2021. However, the overall tularaemia trend in the 2018–2022 period did not show a statistically significant decrease in the EU (p > 0.01). At the country level, a statistically significantly increasing trend was observed in Austria, Finland and Germany (p < 0.05). The proportion of male cases was higher, with a male‐to‐female ratio of 1.6:1. Children under 14 years of age accounted for 51 cases (8.3%). The number of cases increased with age up to 60 years and slowly decreased after 60 years. The highest number of cases was for the 50–75‐year age group (47.5%).
Data on hospitalisation status were provided by 10 MSs for 151 (24.4%) confirmed cases. A total of 91 hospitalisations were reported by 10 MSs (Austria, Czechia, Estonia, Hungary, Lithuania, the Netherlands, Poland, Slovakia, Slovenia and Spain), corresponding to 60.3% of confirmed cases with reported hospitalisation status; this was an increase compared with 2021 (50.7%). A proportion of 30.8% of hospitalisations were counted in the 45–60‐year age group. The highest hospitalisation rates were reported in Poland (84.4%), Slovakia (75.0%), Austria (74.2%) and Czechia (68%). In 2022, 11 MSs reported outcomes for 227 cases (36.6%), with two deaths recorded in the 80‐85‐year age group and with an EU case fatality rate of 0.88%, which was a decrease compared with 2021 (0.59%).
6.3.3 Tularaemia in animals
For 2022, overall, three EU MSs (Austria, Finland and Sweden) reported sampling results, which are summarised in Table 75. Thirty‐six hares, four squirrels, three dogs and one monkey were found positive for tularaemia. The non‐MS Switzerland reported eight positive hares.
TABLE 75.
Francisella tularensis monitoring results for animals, by species in reporting EU MSs and non‐MS countries, 2022.
| Country | N positive/N tested (% positive) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Domestic animals | Wild animals | Zoo animals | |||||||||
| Dogs | Rabbits | Hares | Beavers | Foxes | Squirrels | Moles | Rabbits | Other rodents | Hares | Monkeys | |
| Austria | 0/1 (0) | – | 16/201 (8.0) | – | – | – | 0/1 (0) | 0/1 (0) | 0/36 (0) | – | 1/1 (100) |
| Finland | – | – | 12/134 (9.0) | – | – | 1/56 (1.8) | – | – | – | – | – |
| Sweden | 3/8 (37.5) | – | 8/28 (28.6) | – | – | 3/3 (100) | – | – | – | – | – |
| EU Total (27 + XI) | 3/9 (33.3) | – | 36/363 (9.9) | – | – | 4/59 (6.8) | 0/1 (0) | 0/1 (0) | 0/36 (0) | – | 1/1 (100) |
| Switzerland | – | 0/3 (0) | 8/14 (57.1) | 0/1 (0) | 0/3 (0) | – | – | – | – | 0/1 (0) | 0/2 (0) |
| Total EU (27+ XI) + non‐EU countries | 3/9 (33.3) | 0/3 (0) | 44/377 (11.7) | 0/1 (0) | 0/3 (0) | 4/59 (6.8) | 0/1 (0) | 0/1 (0) | 0/36 (0) | 0/1 (0) | 1/3 (33.3) |
Abbreviation: –, Data not reported.
6.4 Discussion
Tularaemia, caused by F. tularensis, affects humans and animals. Because of its low infectious dose and high virulence, and since it can spread via aerosols, it is classified as a biological threat. Humans can acquire the disease through several routes. In particular, the pathogen can be transmitted from animals, vectors (mosquitoes and ticks), contaminated environment, food and water (Maurin and Gyuranecz, 2016). The disease shows a seasonal pattern in humans (Hestvik et al., 2015), consistent with a higher likelihood of exposure in summer and autumn months due to recreational outdoor activities (notably hunting), exposure to contaminated water (Hennebique et al., 2019) and vector bites. Tularaemia is widely distributed throughout most of Europe, and in endemic regions within Scandinavian countries, it is typically transmitted through mosquito bites (Kenney et al., 2017). Notification rates for tularaemia vary among MSs and over time. Sweden has reported cases of tularaemia since 1931 and recorded two major outbreaks in 2015 and 2019 (Dryselius et al., 2019), whereas in 2016, Finland had the highest notification rate. In 2018, an outbreak occurred in France, whereas in 2019, Norway and Sweden reported the highest number of cases.
The number of human cases reported for the EU was lower than the numbers reported for 2019–2021. More precisely, tularaemia cases decreased compared with the 2020–2021 pandemic years, and also fell to less than half of the number observed in 2019. The majority of cases were reported by Finland, France, Germany and Sweden. Moreover, France recorded 50.0% fewer cases compared with 2021, despite having adopted the new EU case definition in 2021, which is less restrictive for confirmed cases. In 2022, Bulgaria changed its reporting data from case‐based to aggregated, but this aspect was not remarkable due to the few cases generally reported over the years. From 2018 to 2022, at the country level, Austria, Finland and Germany reported an increase in the trend for confirmed cases. Overall, the tularaemia trend in the 2018–2022 period did not show a statistically significant increase or decrease in the EU.
Wildlife continues to play a role in maintaining F. tularensis in the ecological cycle, and also in the occurrence of human cases. F. tularensis is present in wild animals (such as hares) and in vectors (e.g. ticks and mosquitoes), which can be sources of infections for humans (WHO, 2007; Maurin and Gyuranecz, 2016). The vector role of mosquitoes for F. tularensis was considered in a recent review in which it was found that there is no conclusive evidence that mosquitoes can transmit F. tularensis during blood feeding. Most likely, mosquitoes act as mechanical vectors (Jonckers Nieboer et al., 2023).
The circulation of F. tularensis among wild animals has been reported in numerous countries in north‐central Europe, where it is considered endemic (Hestvik et al., 2015; Faber et al., 2018; Seiwald et al., 2020), as well as in Spain (Mínguez‐González et al., 2021).
In the last 5 years, among the reporting MSs, the number of hares tested has increased (from 112 to 363) and the annual proportion of positive samples has decreased from 17.9% to 9.9%. The reporting of positive dogs (3/9) is interesting because dogs live in close contact with humans and can therefore share exposure to F. tularensis (Kwit et al., 2020). As tularaemia monitoring is very often passive, they do not reflect the status of the entire population, so it is difficult to paint an accurate picture of the spread of the disease among animals. For example, the positivity rate reported in dogs in 2022 is not indicative of the spread of the disease in this population.
It should be highlighted that risks of exposure and/or new outbreaks in humans are often preceded by the appearance of the disease in animals, which means that wildlife monitoring (hares are good indicators) is crucial. Tularaemia is a disease with a variety of complex characteristics; it is therefore difficult to control. Cooperation among both the veterinarian and human sectors is crucial for extensive and timely epidemiological, laboratory and clinical investigations, especially with regard to early tularaemia events. This approach is key to preventing further human exposure to the pathogen and to adopting actions for the control of tularaemia outbreaks. Good communication between these two sectors is essential because both serve as alerts for each other. In fact, it is not uncommon for disease in humans to be an indicator of F. tularensis circulation in wild animals or in the environment.
7 OTHER ZOONOSES AND ZOONOTIC AGENTS
The summary data which make up this chapter are published as supporting information for this report on the EFSA Knowledge Junction at Zenodo here.
In 2022, data on Bacillus, Chlamydia, Clostridium, Cronobacter, Klebsiella, non‐pathogenic Enterococcus, non‐pathogenic Escherichia coli, Proteus, Staphylococcus, Streptococcus, Vibrio, caliciviruses, flaviviruses other than West Nile virus, hepatitis virus, Cysticercus, Leptospira and Sarcocystis were reported to EFSA.
7.1 Bacillus spp.
Greece and Luxembourg submitted data on Bacillus cereus in various foods collected at hospitals or medical care facilities, schools or kindergartens, canteens or workplace catering establishments, retail, mobile food retailers, collective catering establishments (restaurant or cafe or pub or bar, or hotel or catering service) and manufacturing plants. Out of 3415 single samples, only 95 (2.8%) were reported positive. The positive food categories were primarily ‘other processed food products and prepared dishes’, ‘vegetable‐based sauces’, ‘mushroom‐cooked sauces’ and ‘RTE salads’.
Greece reported three B. anthracis‐positive bovine animals, as well as two goats and one sheep also positive for B. anthracis (75%) out of a total of eight samples collected at the farm level during clinical investigations. Greece moreover reported data on Bacillus spp. from buffalos, sheep and wild boars, finding no positives out of 13 collected samples.
7.2 Caliciviruses (including norovirus)
Five MSs (Bulgaria, Croatia, France, Portugal and Romania) reported data on caliciviruses for a total of eight batches and 133 single samples. No positive samples were found.
7.3 Chlamydia spp.
Two MSs (Austria and Denmark) and one non‐MS (Republic of North Macedonia) reported data on Chlamydia spp. in various animal species. Austria reported 95 (8.3%) positives out of 1143 samples, Denmark reported 16 (25.4%) positives out of 63 samples and Republic of North Macedonia reported 35 (54.7%) positives out of 64 samples.
7.4 Clostridium spp.
Romania and one non‐MS (Republic of North Macedonia) provided data on Clostridium spp. in foods for a total of 80 tested samples. No positive samples were detected.
Greece and one non‐MS (Republic of North Macedonia) reported data on Clostridium spp. from various ruminant species for a total of 64 samples collected during clinical investigations. Greece detected 31 (56.4%) positives out of 55 animal samples, and Republic of North Macedonia detected three (33.3%) positives out of nine samples.
7.5 Hepatitis virus
Three MSs (Bulgaria, France and Romania) provided data on hepatitis virus in pre‐cut and non‐pre‐cut fruits and leaf vegetables collected at the primary production, manufacturing and distribution (wholesale and retail) levels. Five (5.6%) out of ninety tested samples were positive.
7.6 Proteus spp.
Greece tested for the presence of Proteus spp. A total of, 161 samples of milk collected from dairy cows, goats and sheep during clinical investigations, obtaining 22 (13.7%) positives.
7.7 Staphylococcus spp. and staphylococcal enterotoxins
Five MSs (Croatia, Germany, Greece, Italy and Spain) provided data on Staphylococcus spp. (reported as Staphylococcus, Staphylococcus spp. unspecified, S. aureus or S. intermedius) in various food matrices (N = 7494) and animals (N = 13,832). Overall, 8.3% of foods and 12.6% of animals were reported positive. ‘Other processed food products and prepared dishes’, ‘meat products – ready‐to‐eat’ and ‘cheeses soft and semi‐soft’ were the food categories with the highest numbers of positive results.
7.8 Cysticercus spp.
Eight MSs (Belgium, Finland, Luxembourg, Malta, Slovakia, Slovenia, Spain and Sweden) submitted data on Cysticercus spp. in various animal species. Belgium collected 758,282 bovine carcases from slaughterhouses and found 700 (0.09%) positive samples. None of the 2,127,700 carcases from bovine animals, pigs or farmed wild boars collected by Finland were positive. Luxembourg detected 63 (0.24%) positive bovine carcases out of 26,483 collected samples. None of the 62,922 bovine, pig, sheep or goat carcases collected by Malta were positive. Slovakia detected no positive bovine carcases out of 32,083, a single positive pig carcase out of 585,890 and 228 (4.8%) positive sheep carcases out of 4782 samples collected at slaughterhouses. Slovenia provided results on 23 bovine carcases collected at slaughterhouses, detecting 1 (4.3%) positive sample. Spain provided data on Cysticercus spp. in various animal species: 89 (< 0.01%) out of 2,586,042 bovine animals, 163,913 (2.49%) out of 6,586,572 sheep, 17,790 (2.04%) out of 871,084 goats, 2630 (0.01%) out of 40,115,220 pigs, 20 (0.52%) out of 3874 domestic solipeds, 76 (0.06%) of 129,614 hunted wild boars, 5 (< 0.01%) out of 141,570 deer and 2 (0.02%) out of 8378 mouflons were positive. Sweden detected no positive samples out of 412,090 bovine and 2672,400 pig carcases collected at slaughterhouses.
7.9 Leishmania
Greece and one non‐MS (Republic of North Macedonia) provided data on Leishmania collected on 6241 blood samples from dogs, detecting 598 (9.6%) positive samples.
7.10 Sarcocystis spp.
Belgium reported data from 758,282 bovine animals collected at the slaughterhouse, finding 97 (0.01%) positive samples for Sarcocystis spp.
7.11 Other
Bulgaria provided data on non‐pathogenic Enterococcus spp. collected from drinking water during quality control monitoring at production plants. None tested positive out of the 240 tested samples.
Five MSs (Bulgaria, Greece, Luxembourg, Malta and Latvia) and two non‐MSs (Iceland and Republic of North Macedonia) provided data on E. coli and non‐pathogenic E. coli in various food matrices and animals. Ten (0.75%) out of 1340 food samples and 393 (77.8%) out of 505 animal samples tested positive.
Six MSs (Cyprus, Denmark, Italy, the Netherlands, Romania and Slovakia) and two non‐MSs (Serbia and Switzerland) reported data to verify the presence of flaviviruses other than West Nile virus in various animal species. Cyprus detected 26 (21.3%) positives out of 122 domestic solipeds and 15 (3.2%) positives out of 472 birds. No positive samples were found by Denmark, which collected 91 samples from poultry. Italy tested 166 wild birds and five domestic solipeds with no positives. The Netherlands found a single positive out of 15,497 wild birds tested. Romania obtained 35 (66.0%) positives out of 53 poultry samples tested. Slovakia found no positives out of 52 horses tested. Among non‐MSs, Serbia found 140 (8.0%) positives out of 1740 bovine animals tested and Switzerland obtained no positives out of 18 domestic solipeds.
Greece reported data on Klebsiella spp. in milk collected from various ruminants (dairy cows, goats, sheep), obtaining 2 (1.2%) positives out of 163 tested samples.
Greece provided data on Streptococcus spp. in milk collected from cattle and small ruminants, obtaining 43 (22.9%) positives out of 188 tested samples.
The Netherlands tested 185 single samples and 327 batches of raw fish and crustaceans – shrimp, collected at border control posts to verify the presence of Vibrio spp. Vi cholerae was detected in 11 batches, and V. parahaemolyticus was detected 18 single samples and in 1 batch, for a total of 30 (5.9%) positives.
Two MSs (Bulgaria and Slovenia) provided data on Leptospira in various animal species. Bulgaria detected no positives out of 7263 tested samples, and Slovenia detected 7 (7.3%) positives out of 96 tested samples.
MICROBIOLOGICAL CONTAMINANTS SUBJECT TO FOOD SAFETY CRITERIA (REGULATION (EC) NO 2073/2005 63 )
This chapter summarises the 2022 information and data provided by reporting countries on microbiological contaminants in food for which food safety criteria (FSC) have been set down in EU legislation (Regulation (EC) No 2073/2005): histamine, staphylococcal enterotoxins and C. sakazakii. Requirements from the Official Controls Regulation (EU) 2017/625 64 (OCR) have been implemented for the first time. In contrast with previous legislation, competent authorities (CAs) must use methods complying with relevant internationally recognised rules or protocols, including those accepted by the CEN. This condition is met by the use of EN ISO methods, which are ISO methods recognised by CEN. Consequently, and unlike in previous legislation, CAs cannot use the alternative methods mentioned in Commission Regulation (EC) No 2073/2005 when they carry out official controls to verify the correct implementation of the provisions of this Regulation by FBOs. The implementation of this change in legislative testing requirements may have impacted the results of 2022 official food control samples taken as part of Commission Regulation (EC) No 2073/2005, compared with the results of similar samples in 2021 and before, when OCR requirements were not yet implemented by EFSA in collecting zoonosis data. For this reason, the above‐mentioned results should be interpreted with caution.
1 HISTAMINE
1.1 Histamine data in the context of Regulation (EC) No 2073/2005
Histamine is a thermostable biogenic amine occurring naturally in the human body, and which is involved in key human physiological functions. However, its ingestion at high concentrations through food is associated with the onset of health disorders such as scombroid poisoning.
Regulation (EC) No 2073/2005 on microbiological criteria for foodstuffs defines FSC for histamine in food in three categories at the retail level: ‘fishery products from fish species associated with a high amount of histidine' (food category 1.26), ‘fishery products which have undergone enzyme maturation treatment in brine, manufactured from fish species associated with a high amount of histidine' (food category 1.27) and ‘fish sauce produced by fermentation of fishery products’ (food category 1.27a). Information was also obtained at manufacturing level, indicating the correct application of GMP (good manufacturing practices) and the proper maintenance of the cold chain, which is essential to avoid the development or increase of histamine in fish and fish products.
Histamine data were reported by 12 MSs (Bulgaria, Czechia, Denmark, Estonia, France, Germany, Italy, Luxembourg, Romania, Slovakia, Slovenia and Spain).
In official control samples (N = 6061) for histamine in food category 1.26 at the distribution level (wholesale establishments, retail establishments, border control posts, catering and restaurants), 0.3% had a histamine content higher than 200 mg/kg, 0.2% a histamine content of between 100 and 200 mg/kg, 17.6% a histamine content above the limit of detection, but less than or equal to 100 mg/kg. Of the total number of samples, 52% were of EU origin (Denmark, Estonia, European Union, Italy, Latvia, Romania, Spain) and 18% of non‐EU origin (Colombia, El Salvador, Ghana, Greenland, Maldives, Mauritius, Philippines, Seychelles, Thailand, Türkiye, United Kingdom, Vietnam, non‐EU countries), while for 30%, no information was available. Of the total number of samples, 21% came from canned fish and 4% from raw fish, while for 75% no information was provided.
At the manufacturing level (processing plants), 609 official control samples were collected and the results were as follows: 0.7% had a histamine content higher than 200 mg/kg, and 3.8% a histamine content higher than the limit of detection, but less than or equal to 100 mg/kg. Of the total number of samples, 97% were of EU origin (Italy, Slovakia), while 3% were of non‐EU origin. Of the total number of control samples, 8% came from canned fish and 24% from raw fish, while for 68% no information was reported.
For food category 1.27, 1227 and 11 official control samples were collected at the distribution and manufacturing levels, respectively. At the distribution level, 15.8% of samples had a histamine concentration less than or equal to 200 mg/kg, 0.2% a histamine content between 200 and 400 mg/kg and 0.7% a histamine content higher than 400 mg/kg. Of the total number of samples, 51% were of EU origin (Denmark, Italy Romania, EU countries) and 10% of non‐EU origin, while for 39% no information was available. A total 25% of the control samples came from canned fish.
At the manufacturing level, all samples taken (N = 11) were negative and were of EU origin (Italy).
For food category 1.27a at the distribution level, 10 official control samples were reported: 80% of samples had a histamine content less than or equal to 400 mg/kg but above the limit of detection, and none had a histamine content above 400 mg/kg. Of the total number of control samples, 10% were of EU origin (Italy).
1.2 Other surveillance data for histamine
MSs also collected and analysed fishery products for surveillance purposes, outside the context of Regulation (EC) 2073/2005 on microbiological criteria for foodstuffs.
A total of 1930 samples and 306 batches were collected as part of the Surveillance activity; data were reported by 11 MSs (Belgium, Croatia, Estonia, Germany, Greece, Italy, Latvia, Portugal, Romania, Slovakia and Spain) and 2 non‐MSs (Serbia and Iceland).
A total of 809 single samples and 108 batches at the distribution level, and 1121 sampling units and 198 batches at the manufacturing level were collected, respectively.
At the distribution level , 76%, 23% and 1% of the collected sampling units (N = 809) were classified in categories 1.26, 1.27 and 1.27a, respectively. Ten per cent of the samples falling into category 1.26 had a histamine content higher than 200 mg/kg and 20% of the samples in category 1.27a had a histamine concentration higher than 400 mg/kg.
A total 55%, 26%, 11% and 8% of sampling units were taken from retail, border control posts, wholesale and catering, respectively. Of the total number of sampling units, 46% were of EU origin (Estonia, Germany, Italy, Latvia, Spain, EU countries), and 26% of non‐EU origin (Cape Verde, China, Ecuador, Mauritius, Morocco, Mozambique, Sri Lanka, Thailand), while for 28% no information was available.
All the batches (N = 108) taken at Border Control Posts were classified in categories 1.26. All batches were negative and were of non‐EU origin (Ecuador, Morocco, Philippines, the United Kingdom, Thailand, Türkiye).
At the manufacturing level , all sampling units (N = 1121) were taken at processing plants; 87% and 13% of the samples were classified in categories 1.26 and 1.27, respectively. Just 0.4% of the samples falling into category 1.26 had a histamine content higher than 200 mg/kg.
Of the total sampling units, 82% were of EU origin (Estonia, Italy, Latvia, Portugal, Romania, Sweden, EU countries) and 10.5% of non‐EU origin (Iceland, non‐EU countries), while for 7.5%, no information was available.
All the batches (N = 198) taken at processing plants were classified in category 1.26 and were of EU origin (Greece). Of the total number of batches, 59% had a histamine content higher than the limit of detection, but less than or equal to 100 mg/kg.
2 STAPHYLOCOCCAL ENTEROTOXINS
2.1 Staphylococcal enterotoxins data in the context of Regulation (EC) No 2073/2005
Data on staphylococcal enterotoxins were reported by four MSs (Bulgaria, Italy, Slovakia and Spain). At the distribution level, a total of 2294 official control samples were tested with seven (0.3%) positives, detected by Italy (N = 5) and Spain (N = 2). ‘Cheeses made from cows’ milk, unspecified’ collected at the retail level and ‘cheeses made from cows' milk ‐ soft and semi‐soft’ collected at the wholesale level were the positive food categories. None of the total 870 official control samples collected by Italy, Slovakia and Romania at the manufacturing level were positive.
2.2 Other surveillance data for Staphylococcal enterotoxins
Ten MSs (Bulgaria, Cyprus, Czechia, Germany, Greece, Italy, Portugal, Romania, Slovakia and Spain) reported data on staphylococcal enterotoxins collected in contexts other than those stipulated in Regulation (EC) No 2073/2005. Twenty‐seven (0.42%) out of 6437 tested samples were positive. ‘Other processed food products and prepared dishes’ and ‘cheeses made from cows’ milk – soft and semi‐soft’, mainly collected at the distribution and manufacturing levels, were the food categories found positive for staphylococcal enterotoxins.
3 CRONOBACTER SAKAZAKII
3.1 Cronobacter sakazakii data in the context of Regulation (EC) No 2073/2005
The results of 714 official control samples concerning C. sakazakii in ‘infant formulae' and ‘foodstuffs intended for special nutritional uses – dried dietary foods for special medical purposes intended for infants below six months’ collected at the distribution level (retail and wholesale) were reported by five MSs (Cyprus, Hungary, Slovenia, Slovakia and Spain). Two positives (0.3%) were detected by Slovakia in dried infant formulae, out of 452 collected samples.
Estonia and Spain collected official control samples from food at processing plants, obtaining no positives out of 126 tested samples.
3.2 Other surveillance data for Cronobacter sakazakii
Eleven MSs reported data on Cronobacter spp. collected in contexts other than those stipulated in Regulation (EC) No 2073/2005. ‘Infant formulae', ‘foodstuffs intended for special nutritional uses’ and ‘dairy products, excluding cheeses’ were collected at the retail, processing plant and wholesale levels or at hospital or medical care facilities for surveillance or monitoring purposes. A total of 600 single samples and 190 batches were collected. Ten single samples (1.7%) and three batches (1.6%) tested positive.
ABBREVIATIONS
- ADIS
Animal Disease Information System
- AE
alveolar echinococcosis
- AHAW
Animal Health and Welfare
- AHL
Animal Health Law
- APHA
Animal and Plant Health Agency (APHA)
- ATLAS
Surveillance Atlas of Infectious Diseases
- BIOHAZ
Panel Scientific Panel on biological hazards
- CA
Competent Authority
- CE
cystic echinococcosis
- CEN
European Committee for Standardization
- CFU
colony forming unit
- CgMLST
core genome multi‐locus sequence typing
- CHC
raised under controlled housing conditions not recognised by the CA
- CI
confidence Interval
- CIR (EU)
Commission Implementing Regulation (EU)
- CSF
Cerebrospinal Fluid
- DCF
EFSA's Data Collection Framework
- DSF
disease‐free status
- EAEC
Enteroaggregative E. coli
- EBLV
European bat lyssavirus
- ECDC
European Centre for Disease Prevention and Control
- EEA
European Economic Area
- EFTA
European Free Trade Association
- EIEC
Enteroinvasive E. coli
- ELISA
enzyme‐linked immunosorbent assay
- EPEC
enteropathogenic E. coli
- ERCE
European Register of Cystic Echinococcosis'
- ETEC
Enterotoxigenic E. coli
- EU‐FORS
European Union Foodborne Reporting System
- EUOHZ
The European Union One Health Zoonoses Report
- EURL
European Union Reference Laboratory
- EVD
Emerging and Vector borne Diseases
- EWRS
Early Warning Response System
- FAO
Food and Agriculture Organization of the United Nations
- FBO
foodborne outbreak
- FBOp
food business operator
- FSC
food safety criteria
- FWD
Food and Waterborne Diseases and Zoonoses
- GAP
Good Agricultural Practices
- GF‐TADs
The Global Framework for the Progressive Control of Transboundary Animal Diseases
- GMP
Good Manufacturing Practices
- HACCP
Hazard Analysis and Critical Control Point
- HUS
haemolytic uremic syndrome
- IgG
immunoglobulin G
- IgM
immunoglobulin M
- ISO
International Organization for Standardization
- JEMRA
Joint FAO/WHO expert meetings on microbial risk assessment
- MALDITOF MS
Matrix‐assisted laser desorption ionisation time‐of‐flight mass spectrometry
- MDR
multi‐drug resistant
- MS
Member State
- MSM
mechanically separated meat
- MTBC
Mycobacterium tuberculosis complex
- NCHC
not raised under controlled housing conditions
- NCP
National Control Programme
- NS
not significant
- NUTS
Nomenclature of territorial units for statistics
- OCR
Official Controls Regulation
- ORV
oral rabies vaccination
- PCR
polymerase chain reaction
- PFGE
pulsed‐field gel electrophoresis
- PHC
process hygiene criteria
- RABV
Rabies virus
- RASFF
rapid alert system for food and feed
- RCHC
raised under controlled housing conditions recognised by the Competent Authority
- ROA
rapid outbreak assessment
- ROC curve
receiver operating characteristic curve
- RTE
ready‐to‐eat
- SGE RAB
Standing Group of Experts on Rabies
- STEC
Shiga toxin‐producing Escherichia coli
- TB
tuberculosis
- TBE
tick‐borne Encephalitis virus (TBE)
- TESSy
The European Surveillance System
- UEP
under eradication programme
- WGS
whole genome sequencing
- WHO
World Health Organization
- WNF
West Nile fever
- WNND
West Nile neuro‐invasive disease
- WNV
West Nile virus
- WOAH
World Organisation for Animal Health
- XDR
extensively drug‐resistant
- ZOE
Zoonoses under a One Health perspective in the EU
COUNTRY CODES
- Austria
AT
- Belgium
BE
- Bulgaria
BG
- Croatia
HR
- Cyprus
CY
- Czechia
CZ
- Denmark
DK
- Estonia
EE
- France
FR
- Greece
GR
- Hungary
HU
- Italy
IT
- Latvia
LV
- Malta
MT
- Poland
PL
- Romania
RO
- Slovakia
SK
- Slovenia
SI
- Spain
ES
- United Kingdom (Northern Ireland)
XI
CONFLICT OF INTEREST
If you wish to access the declaration of interests of any expert contributing to an EFSA scientific assessment, please contactinterestmanagement@efsa.europa.eu.
REQUESTOR
European Commission
QUESTION NUMBER
EFSA‐Q‐2021‐00763
COPYRIGHT FOR NON‐EFSA CONTENT
EFSA may include images or other content for which it does not hold copyright. In such cases, EFSA indicates the copyright holder and users should seek permission to reproduce the content from the original source.
MAP DISCLAIMER
The designations employed and the presentation of material on any maps included in this scientific output do not imply the expression of any opinion whatsoever on the part of the European Food Safety Authority concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
ACKNOWLEDGEMENTS
EFSA and the ECDC wish to thank the members of the EFSA Scientific Network for Zoonoses Monitoring Data and of the ECDC Food and Waterborne Diseases and Zoonoses Network, the ECDC Emerging and Vector‐borne Diseases Network and the ECDC Tuberculosis Network, who provided the data and reviewed the report; the members of the Scientific Network for Zoonoses Monitoring Data for their endorsement of this scientific report; the EFSA staff members (Frank Boelaert, Giusi Amore, Valentina Rizzi, Anca Stoicescu, Kateryna Chuzhakina, Maria Teresa Da Silva Felício, Sandra Luisa De Almeida Florentino Correia, Michaela Hempen, Winy Messens, Sotiria‐Eleni Antoniou, Francesca Baldinelli, Alessandro Broglia, Lisa Kohnle and Lina Mur), the ECDC staff members (Taina Niskanen, Mohammed Afzal, Tamas Bakonyi and Veronica Cristea) and the EFSA and ECDC contractor: Istituto Superiore di Sanità (Gaia Scavia, Ilaria Altieri, Fabrizio Anniballi, Pierfrancesco Barbariol, Antonino Bella, Simone Cacciò, Adriano Casulli, Alessandra Ciervo, Elisabetta Delibato, Maria Grazia Dente, Michele Luca D'Errico, Aurora Garcia Fernandez, Federico Giannoni, Maria Angeles Gomez Morales, Francesca Iacoponi, Arnold Knijn, Marco Lalle, Claudia Lucarelli, Cinzia Marianelli, Stefano Morabito, Marco Francesco Ortoffi, Flavia Riccardo, Elisabetta Suffredini, Rosangela Tozzoli, Eleonora Ventola and Laura Villa); Istituto Zooprofilattico delle Venezie (Giorgia Angeloni, Lisa Barco, Grazia Manca, Aurora Boscolo, Katia Capello, Giulia Cento, Laura Ciot, Paola De Benedictis, Laura Gagliazzo, Annie Ishebabi, Elena Lazzaro, Monica Lorenzetto, Marzia Mancin, Claudio Mantovani, Angelo Sardella, Martina Simonato and Marica Toson); Istituto Zooprofilattico Sperimentale dell'Abruzzo e del Molise ‘G. Caporale' (Paolo Calistri, Marta Cresci, Enrico De Albentiis, Giuliano Garofolo, Diana Palma, Fabrizio De Massis, Francesco Pomilio, Americo Bonanni, Susanna Tora, Alessio Di Lorenzo, Mauro Ferella, Andrea De Ruvo, Raffaella Lucchini and Annamaria Conte); Istituto Zooprofilattico Sperimentale della Lombardia ed Emilia Romagna 'B. Ubertini’ (Maria Beatrice Boniotti, Nadia Vicari, Silvia Bellini, Gabriele Casadei); the French Agency for Food, Environmental and Occupational Health & Safety (Adrien Asséré, Christophe Cordevant, Aurélie Couesnon, Radu Blaga, Florence Cliquet, Corinne Danan, Nolwenn Dheilly, Luca Freddi, Gaëlle Gonzalez, Claire Ponsart, Dana Pottratz, Emmanuelle Robardet, Elodie Rousset and Isabelle Vallée) for the support provided to this scientific report.
EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) , (2023). The European Union One Health 2022 Zoonoses Report. EFSA Journal, 21(12), e8442. 10.2903/j.efsa.2023.8442
Approved: 8 November 2023
Note: A plain language summary of this scientific report is available at https://efsa.onlinelibrary.wiley.com/doi/10.2903/j.efsa.2023.p211202
Notes
Directive 2003/99/EC of the European Parliament and of the Council of 17 November 2003 on the monitoring of zoonoses and zoonotic agents, amending Council Decision 90/424/EEC and repealing Council Directive 92/117/EEC. OJ L 325, 12.12.2003, p. 31–40.
See mandate M‐2015‐0231 in Open EFSA Questions: https://open.efsa.europa.eu/questions/EFSA‐Q‐2020‐00787.
Decision No 1082/2013/EU of the European Parliament and of the Council of 22 October 2013 on serious cross‐border threats to health and repealing Decision No 2119/98/EC. OJ L 293, 5.11.2013, p. 1–15.
Commission Implementing Decision 2018/945/EU on the communicable diseases and related special health issues to be covered by epidemiological surveillance as well as relevant case definitions. OJ L 170, 6.7.2018, p. 1–74.
Agreement on the withdrawal of the United Kingdom of Great Britain and Northern Ireland from the European Union and the European Atomic Energy Community. OJ L 29, 31.1.2020, p. 7 (‘Withdrawal Agreement’).
For the collection of data, EFSA aligned with the guidelines of the Commission concerning customs registration that lays down abbreviations and terminology, and which are available at https://taxation‐customs.ec.europa.eu/system/files/2020‐11/use_of_gb_and_xi_codes_guidance.pdf
Definitions adopted by TESSy for surveillance systems and summarised in the EUOHZ 2022: Legal character; ‘Compulsory’ (Co): the surveillance system has a legal basis (at the national administrative level or other) under which reporting of cases of the disease(s) under surveillance is compulsory, ‘Voluntary’ (V): the surveillance system is based on a voluntary agreement (at the national level or other) by which reporting of cases of the disease(s) under surveillance is voluntary, ‘Other’ (O): any system that does not fall under one of the above descriptions, ‘Unknown’: not specified/unknown, Comprehensiveness; ‘Comprehensive’ (Cp): reporting is based on cases occurring within the whole population of the geographical area where the surveillance system is set up (national, regional, etc.), ‘Sentinel’ (Se): reporting is based on a selected group of physicians/hospitals/laboratories, or other institutions' notifications, and/or cases occurring within a selected population defined by age group, gender, exposure or other selection criteria, ‘Other’ (O): reporting is based on a part of the population or group of physicians (or other institutions) which is not specified, for example reporting from laboratories with no selection criteria, ‘Unknown’: not specified/unknown, Active/Passive; ‘Active’ (A): the surveillance system is based on the public health officials' initiative to contact the physicians, laboratory or hospital staff, or other relevant sources to report data, ‘Passive’ (P): the surveillance system relies on the physicians, laboratory or hospital staff, or other relevant sources to take the initiative to report data to the health department, ‘Unknown’: not specified/unknown, National coverage; Defined as covering the entire population of the country, or a part of it. May be unknown when not specified.
Based on the customs union treaty of the Principality of Liechtenstein with Switzerland, Liechtenstein is part of the Swiss customs territory. Due to the strong connection between the veterinary authorities of Liechtenstein and Switzerland, and Liechtenstein's integration into the Swiss system in the veterinary field, in principal, all legislation, rules and data on contagious diseases are identical for both Switzerland and Liechtenstein. If not mentioned otherwise, the Swiss data also include the data from Liechtenstein.
This designation is without prejudice to positions on status, and is in line with UNSCR 1244/1999 and the ICJ Opinion on the Kosovo declaration of independence.
This designation is without prejudice to positions on status, and is in line with UNSCR 1244/1999 and the ICJ Opinion on the Kosovo declaration of independence.
Commission Regulation (EC) No 2073/2005 of 15 November 2005 on microbiological criteria for foodstuffs OJ L 338, 22.12.2005, p. 1–26.
Commission Implementing Regulation (EU) 2019/627 of 15 March 2019, laying down uniform practical arrangements for the performance of official controls on products of animal origin intended for human consumption in accordance with Regulation (EU) 2017/625 of the European Parliament and of the Council and amending Commission Regulation (EC) No 2074/2005 regarding official controls. OJ L 131, 17.5.2019, p. 51–100.
This means official sampling using the same method and sampling area as food business operators. At least 49 random samples shall be taken in each slaughterhouse each year. The number of samples may be reduced in small slaughterhouses and based on a risk evaluation.
Directive 2003/99/EC of the European Parliament and of the Council of 17 November 2003 on the monitoring of zoonoses and zoonotic agents, amending Council Decision 90/424/EEC and repealing Council Directive 92/117/EEC. OJ L 325, 12.12.2003, p. 31–40.
Commission Implementing Decision (EU) 2020/1729 of 17 November 2020 on the monitoring and reporting of antimicrobial resistance in zoonotic and commensal bacteria.
Commission Regulation (EC) No 2073/2005 of 15 November 2005 on microbiological criteria for foodstuffs.
Regulation (EC) No 852/2004 of the European Parliament and of the Council of 29 April 2004 on the hygiene of foodstuffs. OJ L 139, 30.4.2004, p. 1–54.
Commission Regulation (EU) No 1086/2011 of 27 October 2011 amending Annex II to Regulation (EC) No 2160/2003 of the European Parliament and of the Council and Annex I to Commission Regulation (EC) No 2073/2005 as regards salmonella in fresh poultry meat Text with EEA relevance. OJ L 281, 28.10.2011, p. 7–11.
Commission Implementing Regulation (EU) 2019/627 of 15 March 2019 laying down uniform practical arrangements for the performance of official controls on products of animal origin intended for human consumption in accordance with Regulation (EU) 2017/625 of the European Parliament and of the Council and amending Commission Regulation (EC) No 2074/2005 as regards official controls. OJ L 131, 17.5.2019, p. 51–100.
Regulation (EC) No 2160/2003 of the European Parliament and of the Council of 17 November 2003 on the control of salmonella and other specified food‐borne zoonotic agents. OJ L 325, 12.12.2003, p. 1–15.
Regulation (EC) No 853/2004 of the European Parliament and of the Council of 29 April 2004 laying down specific hygiene rules for food of animal origin.
COMMISSION REGULATION (EU) No 200/2012 of 8 March 2012 concerning a Union target for the reduction of Salmonella Enteritidis and Salmonella Typhimurium in flocks of broilers, as provided for in Regulation (EC) No 2160/2003 of the European Parliament and of the Council.
Commission Regulation (EU) No 1190/2012 of 12 December 2012 concerning a Union target for the reduction of Salmonella Enteritidis and Salmonella Typhimurium in flocks of turkeys, as provided for in Regulation (EC) No 2160/2003 of the European Parliament and of the Council.
Commission Regulation (EC) No 2073/2005 of 15 November 2005 on microbiological criteria for foodstuffs.
Commission Regulation (EC) No 2073/2005 of 15 November 2005 on microbiological criteria for foodstuffs.
Directive 2003/99/EC of the European Parliament and of the Council of 17 November 2003 on the monitoring of zoonoses and zoonotic agents, amending Council Decision 90/424/EEC and repealing Council Directive 92/117/EEC.
Regulation (EU) 2017/625 of the European Parliament and of the Council of 15 March 2017 on official controls and other official activities performed to ensure the application of food and feed law, rules on animal health and welfare, plant health and plant protection products (…).
Commission Implementing Regulation (EU) 2020/2002 of 7 December 2020 laying down rules for the application of Regulation (EU) 2016/429 of the European Parliament and of the Council with regard to Union notification and Union reporting of listed diseases, to formats and procedures for submission and reporting of Union surveillance programmes and of eradication programmes and for application for recognition of disease‐free status, and to the computerised information system, OJ L 412, 8.12.2020, p. 1–28.
EU Animal Diseases Information System (ADIS). More information is available at: https://food.ec.europa.eu/animals/animal‐diseases/animal‐disease‐information‐system‐adis_en
This designation is without prejudice to positions on status, and is in line with UNSCR 1244/1999 and the ICJ Opinion on the Kosovo declaration of independence.
Regulation (EU) 2016/429 of the European Parliament and of the Council of 9 March 2016 on transmissible animal diseases and amending and repealing certain acts in the area of animal health (‘Animal Health Law’).
Directive 2003/99/EC of the European Parliament and of the Council of 17 November 2003 on the monitoring of zoonoses and zoonotic agents, amending Council Decision 90/424/EEC and repealing Council Directive 92/117/EEC.
Commission Implementing Regulation (EU) 2020/2002 of 7 December 2020 laying down rules for the application of Regulation (EU) 2016/429 of the European Parliament and of the Council with regard to Union notification and Union reporting of listed diseases, to formats and procedures for submission and reporting of Union surveillance programmes and of eradication programmes and for application for recognition of disease‐free status, and to the computerised information system, OJ L 412, 8.12.2020, p. 1–28.
EU Animal Diseases Information System (ADIS). More information is available at: https://food.ec.europa.eu/animals/animal‐diseases/animal‐disease‐information‐system‐adis_en
Commission Implementing Regulation (EU) 2018/1882 of 3 December 2018 on the application of certain disease prevention and control rules to categories of listed diseases and establishing a list of species and groups of species posing a considerable risk for the spread of those listed diseases.
Commission Delegated Regulation (EU) 2020/689 of 17 December 2019 supplementing Regulation (EU) 2016/429 of the European Parliament and of the Council as regards rules for surveillance, eradication programmes and disease‐free status for certain listed and emerging diseases.
This designation is without prejudice to positions on status and is in line with UNSCR 1244/1999 and the ICJ Opinion on the Kosovo declaration of independence.
This designation is without prejudice to positions on status and is in line with UNSCR 1244/1999 and the ICJ Opinion on the Kosovo declaration of independence.
The number of cases and the number of confirmed cases × 100,000 include two cases reported erroneously by Finland.
Croatia reported only positive results.
Commission Implementing Regulation (EU) 2015/1375 of 10 August 2015 laying down specific rules on official controls for Trichinella in meat (text with EEA relevance). OJ L 212, 11.8.2015, pp. 7–34.
The number of cases and the number of confirmed cases*100,000 include two cases reported erroneously by Finland.
The number of cases and the number of confirmed cases*100,000 include two cases reported erroneously by Finland.
Croatia reported only positive results.
Croatia reported only positive results.
Commission Delegated Regulation (EU) 2018/772 of 21 November 2017 supplementing Regulation (EU) 576/2013 of the European Parliament and of the Council with regard to preventive health measures for the control of Echinococcus multilocularis infection in dogs and repealing Delegated Regulation (EU) 1152/2011 C/2017/7619 OJ L 130, 28.5.2018, pp. 1–10.
EU Animal Diseases Information System (ADIS). More information is available at: https://food.ec.europa.eu/animals/animal‐diseases/animal‐disease‐information‐system‐adis_en
Regulation (EC) No 178/2002 of the European Parliament and of the Council of 28 January 2002 laying down the general principles and requirements of food law, establishing the European Food Safety Authority and laying down procedures in matters of food safety.
Northern Ireland Statistics and Research Agency (NISRA) https://www.nisra.gov.uk/
The core messages of the WHO Five Keys campaign is: keep clean; separate raw and cooked; cook thoroughly; keep food at safe temperatures; and use safe water and raw materials.
Regulation (EU) No 652/2014 of the European Parliament and of the Council of 15 May 2014 laying down provisions for the management of expenditure relating to the food chain, animal health and animal welfare, and relating to plant health and plant reproductive material, amending Council Directives 98/56/EC, 2000/29/EC and 2008/90/EC, Regulations (EC) No 178/2002, (EC) No 882/2004 and (EC) No 396/2005 of the European Parliament and of the Council, Directive 2009/128/EC of the European Parliament and of the Council and Regulation (EC) No 1107/2009 of the European Parliament and of the Council and repealing Council Decisions 66/399/EEC, 76/894/EEC and 2009/470/EC. OJ L 189, 27.6.2014, pp. 1–32.
Commission Delegated Regulation (EU) 2020/689 of 17 December 2019 supplementing Regulation (EU) 2016/429 of the European Parliament and of the Council as regards rules for surveillance, eradication programmes and disease‐free status for certain listed and emerging diseases.
Commission Implementing Regulation (EU) No 577/2013 of 28 June 2013 on the model identification documents for the non‐commercial movement of dogs, cats and ferrets, the establishment of lists of territories and third countries and the format, layout and language requirements of the declarations attesting compliance with certain conditions provided for in Regulation (EU) No. 576/2013 of the European Parliament and of the Council. OJ L 178, 28.6.2013, pp. 109–148.
EU Animal Diseases Information System (ADIS). More information is available at: https://food.ec.europa.eu/animals/animal‐diseases/animal‐disease‐information‐system‐adis_en
Guidelines for the Union co‐funded programmes of eradication, control and surveillance of animal diseases and zoonoses for the years 2021–2022, available online at https://food.ec.europa.eu/system/files/2021‐06/cff_animal_vet‐progs_guidance_progs_erad_wd‐2021‐10502.pdf
The NUTS are a hierarchical system divided into three levels. NUTS 1: major socio‐economic regions, NUTS 2: basic regions for the application of regional policies, NUTS 3: small regions for specific diagnoses. (https://ec.europa.eu/eurostat/web/gisco/geodata/reference‐data/administrative‐units‐statistical‐units/nuts)
Commission Implementing Regulation (EU) 2018/1882 of 3 December 2018 on the application of certain disease prevention and control rules to categories of listed diseases and establishing a list of species and groups of species posing a considerable risk for the spread of those listed diseases. OJ L 308, 4.12.2018, p. 21–29.
Commission Implementing Regulation (EU) 2020/2002 of 7 December 2020 laying down rules for the application of Regulation (EU) 2016/429 of the European Parliament and of the Council with regard to Union notification and Union reporting of listed diseases, to formats and procedures for submission and reporting of Union surveillance programmes and of eradication programmes and for application for recognition of disease‐free status, and to the computerised information system. OJ L 412, 8.12.2020, p. 1–28.
Directive 2003/99/EC of the European Parliament and of the Council of 17 November 2003 on the monitoring of zoonoses and zoonotic agents.
EU Animal Diseases Information System (ADIS). More information is available at: https://food.ec.europa.eu/animals/animal‐diseases/animal‐disease‐information‐system‐adis_en
COMMISSION IMPLEMENTING REGULATION (EU) 2020/2002 of 7 December 2020 laying down rules for the application of Regulation (EU) 2016/429 of the European Parliament and of the Council with regard to Union notification and Union reporting of listed diseases, to formats and procedures for submission and reporting of Union surveillance programmes and of eradication programmes and for application for recognition of disease‐free status, and to the computerised information system.
The earliest case reported in April was in the Island of Mayotte, France, which does not inform on the EU transmission season.
Commission Regulation (EC) No 2073/2005 of 15 November 2005 on microbiological criteria for foodstuffs.
Regulation (EU) 2017/625 of the European Parliament and of the Council of 15 March 2017 on official controls and other official activities performed to ensure the application of food and feed law, rules on animal health and welfare, plant health and plant protection products.
REFERENCES
- Adinolfi, F. , Di Pasquale, J. , & Capitanio, F. (2016). Economic issues on food safety. Italian Journal of Food Safety, 5(1). 10.4081/ijfs.2016.5580 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alba, P. , Carfora, V. , Feltrin, F. , Diaconu, E. L. , Sorbara, L. , Dell'Aira, E. , Cerci, T. , Ianzano, A. , Donati, V. , Franco, A. , & Battisti, A. (2023). Evidence of structural rearrangements in ESBL‐positive pESI(like) megaplasmids of S. Infantis . FEMS Microbiology Letters, 370, 1–8. 10.1093/femsle/fnad014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alban, L. , Pozio, E. , Boes, J. , Boireau, P. , Boué, F. , Claes, M. , Cook, A. J. , Dorny, P. , Enemark, H. L. , van der Giessen, J. , Hunt, K. R. , Howell, M. , Kirjusina, M. , Nöckler, K. , Rossi, P. , Smith, G. C. , Snow, L. , Taylor, M. A. , Theodoropoulos, G. , … Zimmer, I. A. (2011). Towards a standardised surveillance for Trichinella in the European Union. Preventive Veterinary Medicine, 99(2–4), 148–160. 10.1016/j.prevetmed.2011.02.008 [DOI] [PubMed] [Google Scholar]
- Aroussi, A. , Vignoles, P. , Dalmay, F. , Wimel, L. , Dardé, M. L. , Mercier, A. , & Ajzenberg, D. (2015). Detection of toxoplasma gondii DNA in horse meat from supermarkets in France and performance evaluation of two serological tests. Parasite, 22, 14. 10.1051/parasite/2015014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balen Topić, M. , Papić, N. , Višković, K. , Sviben, M. , Filipec Kanižaj, T. , Jadrijević, S. , Jurković, D. , & Beck, R. (2023). Emergence of Echinococcus multilocularis in central continental Croatia: A human case series and update on prevalence in foxes. Life (Basel), 13(6), 1402. 10.3390/life13061402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balog, T. , Nagy, G. , Halász, T. , Csányi, E. , Zomborszky, Z. , & Csivincsik, Á. (2021). The occurrence of Echinococcus spp. in golden jackal (Canis aureus) in southwestern Hungary: Should we need to rethink its expansion? Parasitology International, 80, 102214. 10.1016/j.parint.2020.102214 [DOI] [PubMed] [Google Scholar]
- Barzon, L. , Montarsi, F. , Quaranta, E. , Monne, I. , Pacenti, M. , Michelutti, A. , Toniolo, F. , Danesi, P. , Marchetti, G. , Gobbo, F. , Sinigaglia, A. , Riccetti, S. , Dal Molin, E. , Favero, L. , Russo, F. , & Capelli, G. (2022). Early start of seasonal transmission and co‐circulation of West Nile virus lineage 2 and a newly introduced lineage 1 strain, northern Italy, June 2022. Euro Surveillance, 27(29). 10.2807/1560-7917.Es.2022.27.29.2200548 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barzon, L. , Pacenti, M. , Montarsi, F. , Fornasiero, D. , Gobbo, F. , Quaranta, E. , Monne, I. , Fusaro, A. , Volpe, A. , Sinigaglia, A. , Riccetti, S. , Molin, E. D. , Satto, S. , Lisi, V. , Gobbi, F. , Galante, S. , Feltrin, G. , Valeriano, V. , Favero, L. , … Capelli, G. (2022). Rapid spread of a new West Nile virus lineage 1 associated with increased risk of neuroinvasive disease during a large outbreak in northern Italy, 2022: One health analysis. Journal of Travel Medicine, taac125, 1–11. 10.1093/jtm/taac125 [DOI] [PubMed] [Google Scholar]
- Basanisi, M. G. , La Bella, G. , Nobili, G. , Raele, D. A. , Cafiero, M. A. , Coppola, R. , Damato, A. M. , Fraccalvieri, R. , Sottili, R. , & La Salandra, G. (2022). Detection of Coxiella burnetii DNA in sheep and goat milk and dairy products by droplet digital PCR in South Italy. International Journal of Food Microbiology, 366, 109583. 10.1016/j.ijfoodmicro.2022.109583 [DOI] [PubMed] [Google Scholar]
- Beck, C. , Leparc Goffart, I. , Franke, F. , Gonzalez, G. , Dumarest, M. , Lowenski, S. , Blanchard, Y. , Lucas, P. , Lamballerie, X. , Grard, G. , Durand, G. A. , Zientara, S. , Tapprest, J. , L'Ambert, G. , Durand, B. , Desvaux, S. , & Lecollinet, S. (2020). Contrasted epidemiological patterns of West Nile virus lineages 1 and 2 infections in France from 2015 to 2019. Pathogens, 9(11). 10.3390/pathogens9110908 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blaga, R. , Aubert, D. , Thébault, A. , Perret, C. , Geers, R. , Thomas, M. , Alliot, A. , Djokic, V. , Ortis, N. , Halos, L. , Durand, B. , Mercier, A. , Villena, I. , & Boireau, P. (2019). Toxoplasma gondii in beef consumed in France: Regional variation in seroprevalence and parasite isolation. Parasite, 26, 77. 10.1051/parasite/2019076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bless, P. J. , Schmutz, C. , & Mäusezahl, D. (2017). The recurrent campylobacteriosis epidemic over Christmas and new year in European countries, 2006–2014. BMC Research Notes, 10(1), 266. 10.1186/s13104-017-2587-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boelaert, F. , Amore, G. , Van der Stede, Y. , & Hugas, M. (2016). EU‐wide monitoring of biological hazards along the foodchain: Achievements, challenges and EFSA vision for the future. Current Opinion in Food Science, 12, 52–62. 10.1016/j.cofs.2016.08.004 [DOI] [Google Scholar]
- Bosica, S. , Chiaverini, A. , De Angelis, M. E. , Petrini, A. , Averaimo, D. , Martino, M. , Rulli, M. , Saletti, M. A. , Cantelmi, M. C. , Ruggeri, F. , Lodi, F. , Calistri, P. , Cito, F. , Cammà, C. , Di Domenico, M. , Rinaldi, A. , Fazii, P. , Cedrone, F. , Di Martino, G. , … Savini, G. (2023). Severe Streptococcus equi subspecies zooepidemicus outbreak from unpasteurized dairy product consumption, Italy. Emerging Infectious Diseases, 29(5), 1020–1024. 10.3201/eid2905.221338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyden, P. (2022). Should we be doing more about Brucella canis? Veterinary Record, 191(2), 82. 10.1002/vetr.2060 [DOI] [PubMed] [Google Scholar]
- Buchanan, R. L. , Gorris, L. G. M. , Hayman, M. M. , Jackson, T. C. , & Whiting, R. C. (2017). A review of listeria monocytogenes: An update on outbreaks, virulence, dose‐response, ecology, and risk assessments. Food Control, 75, 1–13. 10.1016/j.foodcont.2016.12.016 [DOI] [Google Scholar]
- Bui, T. H. , Ikeuchi, S. , O'Brien, Y. S. , Niwa, T. , Hara‐Kudo, Y. , Taniguchi, T. , & Hayashidani, H. (2021). Multiplex PCR method for differentiating highly pathogenic Yersinia enterocolitica and low pathogenic Yersinia enterocolitica, and Yersinia pseudotuberculosis . Journal of Veterinary Medical Science, 83(12), 1982–1987. 10.1292/jvms.21-0358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byrne, A. W. , Barrett, D. , Breslin, P. , O'Keeffe, J. , Murphy, K. J. , Conteddu, K. , Morera‐Pujol, V. , Ryan, E. , & Ciuti, S. (2022). Disturbance ecology meets bovine tuberculosis (bTB) epidemiology: A before‐and‐after study on the association between Forest Clearfelling and bTB herd risk in cattle herds. Pathogens, 11(7). 10.3390/pathogens11070807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canals, A. , Martínez, C. V. , Diogène, J. , Gago‐Martínez, A. , Cebadera‐Miranda, L. , de Vasconcelos, F. M. , Gómez, I. L. , Sánchez, E. V. M. , Alférez, R. C. , Núñez, D. , Friedemann, M. , Oleastro, M. , Boziaris, I. , Rambla, M. , Campàs, M. , Fernández, M. , Andree, K. , Tudó, A. , Rey, M. , … Sibat, M. (2021). Risk characterisation of ciguatera poisoning in Europe. EFSA Supporting Publications, 18(5), 86. 10.2903/sp.efsa.2021.EN-6647 [DOI] [Google Scholar]
- Carrié, P. , Barry, S. , Rousset, E. , de Crémoux, R. , Sala, C. , Calavas, D. , Perrin, J.‐B. , Bronner, A. , Gasqui, P. , Gilot‐Fromont, E. , Becker, C. A. M. , Gache, K. , & Jourdain, E. (2019). Swab cloths as a tool for revealing environmental contamination by Q fever in ruminant farms. Transboundary and Emerging Diseases, 66, 1202–1209. 10.1111/tbed.13137 [DOI] [PubMed] [Google Scholar]
- Casulli, A. (2020). Recognising the substantial burden of neglected pandemics cystic and alveolar echinococcosis. The Lancet Global Health, 8(4), e470–e471. 10.1016/s2214-109x(20)30066-8 [DOI] [PubMed] [Google Scholar]
- Casulli, A. , Abela‐Ridder, B. , Petrone, D. , Fabiani, M. , Bobić, B. , Carmena, D. , Šoba, B. , Zerem, E. , Gargaté, M. J. , Kuzmanovska, G. , Calomfirescu, C. , Rainova, I. , Sotiraki, S. , Lungu, V. , Dezsényi, B. , Herrador, Z. , Karamon, J. , Maksimov, P. , Oksanen, A. , … Santolamazza, F. (2023). Unveiling the incidences and trends of the neglected zoonosis cystic echinococcosis in Europe: A systematic review from the MEmE project. The Lancet Infectious Diseases, 23, e95–e107. 10.1016/s1473-3099(22)00638-7 [DOI] [PubMed] [Google Scholar]
- Casulli, A. , Massolo, A. , Saarma, U. , Umhang, G. , Santolamazza, F. , & Santoro, A. (2022). Species and genotypes belonging to Echinococcus granulosus sensu lato complex causing human cystic echinococcosis in Europe (2000–2021): A systematic review. Parasites & Vectors, 15(1), 109. 10.1186/s13071-022-05197-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chousalkar, K. K. , & Willson, N. L. (2022). Nontyphoidal salmonella infections acquired from poultry. Current Opinion in Infectious Diseases, 35(5), 431–435. 10.1097/qco.0000000000000876 [DOI] [PubMed] [Google Scholar]
- Christodoulou, M. , Malli, F. , Tsaras, K. , Billinis, C. , & Papagiannis, D. (2023). A narrative review of Q fever in Europe. Cureus, 15(4), e38031. 10.7759/cureus.38031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clayton, D. , & Hills, M. (2013). Chapter 11.2: Log likelihood ratios and p‐values. In Statistical models in epidemiology (p. 384). OUP Oxford. [Google Scholar]
- Conraths, F. J. , Probst, C. , Possenti, A. , Boufana, B. , Saulle, R. , La Torre, G. , Busani, L. , & Casulli, A. (2017). Potential risk factors associated with human alveolar echinococcosis: Systematic review and meta‐analysis. PLoS Neglected Tropical Diseases, 11(7). 10.1371/journal.pntd.0005801 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuperlovic, K. , Djordjevic, M. , & Pavlovic, S. (2005). Re‐emergence of trichinellosis in southeastern Europe due to political and economic changes. Veterinary Parasitology, 132(1–2), 159–166. 10.1016/j.vetpar.2005.05.047 [DOI] [PubMed] [Google Scholar]
- de la Cruz, M. L. , Pozo, P. , Grau, A. , Nacar, J. , Bezos, J. , Perez, A. , Dominguez, L. , Saez, J. L. , Minguez, O. , de Juan, L. , & Alvarez, J. (2019). Assessment of the sensitivity of the bovine tuberculosis eradication program in a high prevalence region of Spain using scenario tree modeling. Preventive Veterinary Medicine, 173, 104800. 10.1016/j.prevetmed.2019.104800 [DOI] [PubMed] [Google Scholar]
- De Massis, F. , Sacchini, F. , Averaimo, D. , Garofolo, G. , Lecchini, P. , Ruocco, L. , Lomolino, R. , Santucci, U. , Sgariglia, E. , Crotti, S. , Petrini, A. , Migliorati, G. , D'Alterio, N. , Gavaudan, S. , & Tittarelli, M. (2021). First isolation of Brucella canis from a breeding kennel in Italy. Veterinaria Italiana, 57, 3. 10.12834/VetIt.2497.15848.1 [DOI] [PubMed] [Google Scholar]
- Deplazes, P. , Hegglin, D. , Gloor, S. , & Romig, T. (2004). Wilderness in the city: The urbanization of Echinococcus multilocularis. Trends in Parasitology, 20(2), 77–84. 10.1016/j.pt.2003.11.011 [DOI] [PubMed] [Google Scholar]
- Desai, A. N. , Anyoha, A. , Madoff, L. C. , & Lassmann, B. (2019). Changing epidemiology of listeria monocytogenes outbreaks, sporadic cases, and recalls globally: A review of ProMED reports from 1996 to 2018. International Journal of Infectious Diseases, 84, 48–53. 10.1016/j.ijid.2019.04.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DIN (Deutsches Institut Fur Normung E.V. ‐ German National Standard‐) . (2004). DIN 10167:2004 DE. Nachweis von Escherichia coli O157 in Fleisch und Fleischerzeugnissen. Detection of Escherichia coli O157 in meat and meat products .
- Djordjevic, M. , Bacic, M. , Petricevic, M. , Cuperlovic, K. , Malakauskas, A. , Kapel, C. M. , & Murrell, K. D. (2003). Social, political, and economic factors responsible for the reemergence of trichinellosis in Serbia: A case study. The Journal of Parasitology, 89(2), 226–231. 10.1645/0022-3395(2003)089[0226:Spaefr]2.0.Co;2 [DOI] [PubMed] [Google Scholar]
- Doganay, M. (2003). Listeriosis: Clinical presentation. FEMS Immunology & Medical Microbiology, 35(3), 173–175. 10.1016/S0928-8244(02)00467-4 [DOI] [PubMed] [Google Scholar]
- Dougas, G. , Katsiolis, A. , Linou, M. , Kostoulas, P. , & Billinis, C. (2022). Modelling human brucellosis based on infection rate and vaccination coverage of sheep and goats. Pathogens, 11(2), 167. 10.3390/pathogens11020167 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dryselius, R. , Hjertqvist, M. , Mäkitalo, S. , Lindblom, A. , Lilja, T. , Eklöf, D. , & Lindström, A. (2019). Large outbreak of tularaemia, Central Sweden, July to September 2019. Euro Surveillance, 24(42). 10.2807/1560-7917.Es.2019.24.42.1900603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dušek, D. , Vince, A. , Kurelac, I. , Papić, N. , Višković, K. , Deplazes, P. , & Beck, R. (2020). Human alveolar echinococcosis, Croatia. Emerging Infectious Diseases., 26(2), 364–366. 10.3201/eid2602.181826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- ECDC (European Centre for Disease Prevention and Control) . (2019). ECDC strategic framework for the integration of molecular and genomic typing into European surveillance and multi‐country outbreak investigations – 2019–2021 . 10.2900/805317 [DOI]
- ECDC (European Centre for Disease Prevention and Control) . (2023). Congenital toxoplasmosis. In: ECDC. Annual epidemiological report for 2020. Stockholm: ECDC . https://www.ecdc.europa.eu/en/publications‐data/congenital‐toxoplasmosis‐annual‐epidemiological‐report‐2020
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2018a). Multi‐country outbreak of listeria monocytogenes serogroup IVb, multi‐locus sequence type 6, infections probably linked to frozen corn. EFSA Supporting Publications, 15(3), 18. 10.2903/sp.efsa.2018.EN-1402 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2018b). Multi‐country outbreak of listeria monocytogenes sequence type 8 infections linked to consumption of salmon products. EFSA Supporting Publications, 15(10). 10.2903/sp.efsa.2018.EN-1496 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2019). Multi‐country outbreak of Listeria monocytogenes sequence type 6 infections linked to ready‐to‐eat meat products. 16 (12). 10.2903/sp.efsa.2019.EN-1745 [DOI]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2022a). Multi‐country outbreak of monophasic salmonella Typhimurium sequence type 34 linked to chocolate products – First update – 18 may 2022. EFSA Supporting Publications, 19(6), 25. 10.2903/sp.efsa.2022.EN-7352 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2022b). Multi‐country outbreak of monophasic salmonella Typhimurium sequence type (ST) 34 linked to chocolate products – 12 April 2022. EFSA Supporting Publications, 19(4), 15. 10.2903/sp.efsa.2022.EN-7318 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2022c). Multi‐country outbreak of salmonella Mbandaka ST413, possibly linked to consumption of chicken meat in the EU/EEA, Israel and the UK. EFSA Supporting Publications, 19(12), 13. 10.2903/sp.efsa.2022.EN-7707 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2023a). Multi‐country outbreak of salmonella Virchow ST16 infections linked to the consumption of meat products containing chicken meat. EFSA Supporting Publications, 20(4), 16. 10.2903/sp.efsa.2023.EN-7983 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2023b). Surveillance, prevention and control of West Nile virus and Usutu virus infections in the EU/EEA. EFSA Supporting Publications, 20(9), 8242E. 10.2903/sp.efsa.2023.EN-8242 [DOI] [Google Scholar]
- ECDC and EFSA (European Centre for Disease Prevention and Control and European Food Safety Authority) . (2023c). Three clusters of salmonella Enteritidis ST11 infections linked to chicken meat and chicken meat products. EFSA Supporting Publications, 20(11), 34. 10.2903/sp.efsa.2023.EN-8388 [DOI] [Google Scholar]
- ECDC, EFSA and ANSES (European Centre for Disease Prevention and Control, European Food Safety Authority and French Agency for Food Environmental and Occupational Health and Safety) . (2021). European Listeria typing exercise (ELiTE) . 10.2900/314391 [DOI]
- Echevarría, J. E. , Banyard, A. C. , McElhinney, L. M. , & Fooks, A. R. (2019). Current rabies vaccines do not confer protective immunity against divergent lyssaviruses circulating in Europe. Viruses, 11(10). 10.3390/v11100892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA (European Food Safety Authority) . (2007). Monitoring and identification of human enteropathogenic Yersinia spp. ‐ scientific opinion of the panel on biological hazards. EFSA Journal, 5(12), 30. 10.2903/j.efsa.2007.595 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2009a). Statistical analysis of temporal and spatial trends of zoonotic agents in animals and food part I: Critical review of the statistical analysis carried out on the community summary report 2006 data. EFSA Journal, 7(5), 253r. 10.2903/j.efsa.2009.253r [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2009b). Technical specifications for harmonised national surveys on Yersinia enterocolitica in slaughter pigs. EFSA Journal, 7(11), 23. 10.2903/j.efsa.2009.1374 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2011). Statistical analysis of temporal and spatial trends of zoonotic agents in animals and food part II: Applications of spatial analysis and further developments of temporal analysis. EFSA Journal, 9(8), 2331. 10.2903/j.efsa.2011.2331 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2014). Update of the technical specifications for harmonised reporting of food‐borne outbreaks through the European Union reporting system in accordance with directive 2003/99/EC. EFSA Journal, 12(3), 25. 10.2903/j.efsa.2014.3598 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) . (2023). The EFSA catalogues applied for the 2022 zoonoses data reporting. [Data Set]. Zenodo. 10.5281/zenodo.7560225 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) , Alvarez, J. , Nielsen, S. S. , Robardet, E. , Stegeman, A. , Van Gucht, S. , Vuta, V. , Antoniou, S. E. , Aznar, I. , & Papanikolaou, A. (2022). Risks related to a possible reduction of the waiting period for dogs after rabies antibody titration to 30 days compared with 90 days of the current EU legislative regime. EFSA Journal, 20(6), e07350. 10.2903/j.efsa.2022.7350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA (European Food Safety Authority) , Amore, G. , Beloeil, P. A. , Boelaert, F. , Fierro, R. G. , Papanikolaou, A. , Rizzi, V. , & Stoicescu, A. V. (2023). Zoonoses, foodborne outbreaks and antimicrobial resistance guidance for reporting 2022 data. EFSA Supporting Publications, 20(1), 153. 10.2903/sp.efsa.2023.EN-7827 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) , Amore, G. , Boelaert, F. , Papanikolaou, A. , Rizzi, V. , & Stoicescu, A. V. (2023). Manual for reporting on zoonoses and zoonotic agents, within the framework of directive 2003/99/EC, and on some other pathogenic microbiological agents for information derived from the year 2022. EFSA Supporting Publications., 20(1), 81. 10.2903/sp.efsa.2023.EN-7825 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) , Costa, G. , Di Piazza, G. , Koevoets, P. , Iacono, G. , Liebana, E. , Pasinato, L. , Rizzi, V. , & Rossi, M. (2022). Guidelines for reporting whole genome sequencing‐based typing data through the EFSA one health WGS system. EFSA Supporting Publications. 10.2903/sp.efsa.2022.EN-7413 [DOI] [Google Scholar]
- EFSA (European Food Safety Authority) , Rusinà, A. , & Zancanaro, G. (2023). Annual assessment of Echinococcus multilocularis surveillance reports submitted in 2023 in the context of commission delegated regulation (EU) 2018/772. EFSA Journal, 21(8), e08204. 10.2903/j.efsa.2023.8204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA AHAW Panel (EFSA Panel on Animal Health and Welfare) . (2014). Statement on a conceptual framework for bovine tuberculosis. EFSA Journal, 12(5), 59. 10.2903/j.efsa.2014.3711 [DOI] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2017). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2016. EFSA Journal, 15(12), 5077. 10.2903/j.efsa.2017.5077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2021b). The European Union one health 2020 Zoonoses report. EFSA Journal, 19(12), 324. 10.2903/j.efsa.2021.6971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2009). The community summary report on trends and sources of Zoonoses and zoonotic agents in the European Union in 2007. EFSA Journal, 7(1), 223r. 10.2903/j.efsa.2009.223r [DOI] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2010). The community summary report on trends and sources of Zoonoses, zoonotic agents and food‐borne outbreaks in the European Union in 2008. EFSA Journal, 8(1), 1496. 10.2903/j.efsa.2010.1496 [DOI] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2011). The European Union summary report on trends and sources of Zoonoses, zoonotic agents and food‐borne outbreaks in 2009. EFSA Journal, 9(3), 2090. 10.2903/j.efsa.2011.2090 [DOI] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2012). The European Union summary report on trends and sources of Zoonoses, zoonotic agents and food‐borne outbreaks in 2010. EFSA Journal, 10(3), 2597. 10.2903/j.efsa.2012.2597 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2013). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2011. EFSA Journal, 11(4), 3129. 10.2903/j.efsa.2013.3129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2014). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2012. EFSA Journal, 12(2), 3547. 10.2903/j.efsa.2014.3547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2015a). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2013. EFSA Journal, 13(1), 3991. 10.2903/j.efsa.2015.3991 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2015b). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2014. EFSA Journal, 13(12), 4329. 10.2903/j.efsa.2015.4329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2016). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2015. EFSA Journal, 14(12), e04634. 10.2903/j.efsa.2016.4634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2018). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food‐borne outbreaks in 2017. EFSA Journal, 16(12), 262. 10.2903/j.efsa.2018.5500 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2019). The European Union one health 2018 Zoonoses report. EFSA Journal, 17(12), 276. 10.2903/j.efsa.2019.5926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2021a). The European Union one health 2019 Zoonoses report. EFSA Journal, 19(2), 286. 10.2903/j.efsa.2021.6406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA and ECDC (European Food Safety Authority and European Centre for Disease Prevention and Control) . (2022). The European Union one health 2021 Zoonoses report. EFSA Journal, 20(12), 273. 10.2903/j.efsa.2022.7666 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) . (2013a). Scientific opinion on the public health hazards to be covered by inspection of meat (solipeds). EFSA Journal, 11(6), 161. 10.2903/j.efsa.2013.3263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) . (2013b). Scientific opinion on the public health hazards to be covered by inspection of meat from farmed game. EFSA Journal, 11(6), 181. 10.2903/j.efsa.2013.3264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) . (2013c). Scientific opinion on the risk posed by pathogens in food of non‐animal origin. Part 1 (outbreak data analysis and risk ranking of food/pathogen combinations). EFSA Journal, 11(1), 138. 10.2903/j.efsa.2013.3025 [DOI] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) . (2014). Scientific opinion on the risk posed by pathogens in food of non‐animal origin. Part 2 (salmonella, Yersinia, Shigella and norovirus in bulb and stem vegetables, and carrots). EFSA Journal, 12(12), 91. 10.2903/j.efsa.2014.3937 [DOI] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) , Koutsoumanis, K. , Allende, A. , Alvarez‐Ordóñez, A. , Bolton, D. , Bover‐Cid, S. , Chemaly, M. , Davies, R. , De Cesare, A. , Hilbert, F. , Lindqvist, R. , Nauta, M. , Peixe, L. , Ru, G. , Simmons, M. , Skandamis, P. , Suffredini, E. , Jenkins, C. , Malorny, B. , … Herman, L. (2019). Whole genome sequencing and metagenomics for outbreak investigation, source attribution and risk assessment of food‐borne microorganisms. EFSA Journal, 17(12), 78. 10.2903/j.efsa.2019.5898 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) , Koutsoumanis, K. , Allende, A. , Alvarez‐Ordóñez, A. , Bolton, D. , Bover‐Cid, S. , Chemaly, M. , De Cesare, A. , Herman, L. , Hilbert, F. , Lindqvist, R. , Nauta, M. , Peixe, L. , Ru, G. , Simmons, M. , Skandamis, P. , Suffredini, E. , Dewulf, J. , Hald, T. , … Davies, R. (2019). Salmonella control in poultry flocks and its public health impact. EFSA Journal, 17(2). 10.2903/j.efsa.2019.5596 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) , Koutsoumanis, K. , Allende, A. , Alvarez‐Ordonez, A. , Bolton, D. , Bover‐Cid, S. , Davies, R. , De Cesare, A. , Herman, L. , Hilbert, F. , Lindqvist, R. , Nauta, M. , Peixe, L. , Ru, G. , Simmons, M. , Skandamis, P. , Suffredini, E. , Alter, T. , Crotta, M. , … Chemaly, M. (2020). Update and review of control options for campylobacter in broilers at primary production. EFSA Journal, 18(4), e06090. 10.2903/j.efsa.2020.6090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) , Koutsoumanis, K. , Allende, A. , Alvarez‐Ordóñez, A. , Bover‐Cid, S. , Chemaly, M. , Davies, R. , De Cesare, A. , Herman, L. , Hilbert, F. , Lindqvist, R. , Nauta, M. , Peixe, L. , Ru, G. , Simmons, M. , Skandamis, P. , Suffredini, E. , Jenkins, C. , Monteiro Pires, S. , … Bolton, D. (2020). Pathogenicity assessment of Shiga toxin‐producing Escherichia coli (STEC) and the public health risk posed by contamination of food with STEC. EFSA Journal, 18(1), 105. 10.2903/j.efsa.2020.5967 [DOI] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) , Koutsoumanis, K. , Alvarez‐Ordóñez, A. , Bolton, D. , Bover‐Cid, S. , Chemaly, M. , Davies, R. , De Cesare, A. , Herman, L. , Hilbert, F. , Lindqvist, R. , Nauta, M. , Peixe, L. , Ru, G. , Simmons, M. , Skandamis, P. , Suffredini, E. , Jordan, K. , Sampers, I. , … Allende, A. (2020). The public health risk posed by listeria monocytogenes in frozen fruit and vegetables including herbs, blanched during processing. EFSA Journal, 18(4), 102. 10.2903/j.efsa.2020.6092 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards) , Ricci, A. , Allende, A. , Bolton, D. , Chemaly, M. , Davies, R. , Fernández Escámez, P. S. , Girones, R. , Herman, L. , Koutsoumanis, K. , Nørrung, B. , Robertson, L. , Ru, G. , Sanaa, M. , Simmons, M. , Skandamis, P. , Snary, E. , Speybroeck, N. , Ter Kuile, B. , … Lindqvist, M. W. (2018). Scientific opinion on the listeria monocytogenes contamination of ready‐to‐eat foods and the risk for human health in the EU. EFSA Journal, 16(2), 173. 10.2903/j.efsa.2018.5134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- EFSA BIOHAZ Panel, EFSA CONTAM Panel and EFSA AHAW Panel (EFSA Panel on Biological Hazards, EFSA Panel on Contaminants in the Food Chain and EFSA Panel on Animal Health and Welfare) . (2011). Scientific opinion on the public health hazards to be covered by inspection of meat (swine). EFSA Journal, 9(10). 10.2903/j.efsa.2011.2351 [DOI] [Google Scholar]
- EFSA BIOHAZ Panel, EFSA CONTAM Panel and EFSA AHAW Panel (EFSA Panel on Biological Hazards, EFSA Panel on Contaminants in the Food Chain and EFSA Panel on Animal Health and Welfare) . (2012). Scientific opinion on the public health hazards to be covered by inspection of meat (poultry). EFSA Journal, 10(6), 179. 10.2903/j.efsa.2012.2741 [DOI] [Google Scholar]
- Ercsey‐Ravasz, M. , Toroczkai, Z. , Lakner, Z. , & Baranyi, J. (2012). Complexity of the international agro‐food trade network and its impact on food safety. PLoS One, 7(5), e37810. 10.1371/journal.pone.0037810 [DOI] [PMC free article] [PubMed] [Google Scholar]
- European Commission, Eurostat , Corselli‐Nordblad, L. , & Strandell, H. (2020). Ageing Europe – Looking at the lives of older people in the EU – 2020 edition . 10.2785/628105 [DOI]
- European Commission , Eurostat, M. P. , Rabade, T. , & Forti, R. (2014). Pig farming in the European Union: considerable variations from one Member State to another. Pig farming sector ‐ statistical portrait 2014. Statistics in focus 15/2014 . https://op.europa.eu/en/publication‐detail/‐/publication/51424486‐e017‐48ea‐90f6‐aa89c570e59b
- European Parliament , 2020. The EU pig meat sector. https://www.europarl.europa.eu/RegData/etudes/BRIE/2020/652044/EPRS_BRI(2020)652044_EN.pdf [Google Scholar]
- Eurostat (European Commission . (2022). Population structure and ageing . https://ec.europa.eu/eurostat/statistics‐explained/index.php?title=Population_structure_and_ageing
- Faber, M. , Heuner, K. , Jacob, D. , & Grunow, R. (2018). Tularemia in Germany‐a Re‐emerging zoonosis. Frontiers in Cellular and Infection Microbiology, 8, 40. 10.3389/fcimb.2018.00040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- FAO and WHO (Food and Agriculture Organization of the United Nations and World Health Organization) . (2018). Shiga toxin‐producing Escherichia Coli (STEC) and food: Attribution, Characterization and Monitoring. edn .
- FAO and WHO (Food and Agriculture Organization of the United Nations and World Health Organization) Food and Agriculture Organization of the United Nations and World Health Organization . (2022). Listeria monocytogenes in ready‐to‐eat (RTE) foods: attribution, characterization and monitoring ‐ Meeting report. Microbiological Risk Assessment Series No. 38. Rome . 10.4060/cc2400en [DOI]
- Farooq, Z. , Rocklöv, J. , Wallin, J. , Abiri, N. , Sewe, M. O. , Sjödin, H. , & Semenza, J. C. (2022). Artificial intelligence to predict West Nile virus outbreaks with eco‐climatic drivers. Lancet Reg Health Eur, 17, 100370. 10.1016/j.lanepe.2022.100370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernández‐Martínez, N. F. , Ruiz‐Montero, R. , Briones, E. , Baños, E. , García San Miguel Rodríguez‐Alarcón, L. , Chaves, J. A. , Abad, R. , Varela, C. , team, o. b. o. t. L , & Lorusso, N. (2022). Listeriosis outbreak caused by contaminated stuffed pork, Andalusia, Spain, July to October 2019. Eurosurveillance, 27(43), 2200279. 10.2807/1560-7917.ES.2022.27.43.2200279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fooks, A. R. , Johnson, N. , Brookes, S. M. , Parsons, G. , & McElhinney, L. M. (2003). Risk factors associated with travel to rabies endemic countries. Journal of Applied Microbiology, 94(Suppl), 31s–36s. 10.1046/j.1365-2672.94.s1.4.x [DOI] [PubMed] [Google Scholar]
- Fornasiero, D. , Mazzucato, M. , Barbujani, M. , Montarsi, F. , Capelli, G. , & Mulatti, P. (2020). Inter‐annual variability of the effects of intrinsic and extrinsic drivers affecting West Nile virus vector Culex pipiens population dynamics in northeastern Italy. Parasites & Vectors, 13(1), 271. 10.1186/s13071-020-04143-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frank, C. , Werber, D. , Cramer, J. P. , Askar, M. , Faber, M. , an der Heiden, M. , Bernard, H. , Fruth, A. , Prager, R. , Spode, A. , Wadl, M. , Zoufaly, A. , Jordan, S. , Kemper, M. J. , Follin, P. , Müller, L. , King, L. A. , Rosner, B. , Buchholz, U. , … Krause, G. (2011). Epidemic profile of Shiga‐toxin‐producing Escherichia coli O104:H4 outbreak in Germany. The New England Journal of Medicine., 365(19), 1771–1780. 10.1056/NEJMoa1106483 [DOI] [PubMed] [Google Scholar]
- Fujiwara, P. I. , & Olea‐Popelka, F. (2016). Editorial commentary: Why it is important to distinguish Mycobacterium bovis as a causal agent of human tuberculosis. Clinical Infectious Diseases, 63(5), 602–603. 10.1093/cid/ciw374 [DOI] [PubMed] [Google Scholar]
- Genova‐Kalou, P. , Vladimirova, N. , Stoitsova, S. , Krumova, S. , Kurchatova, A. , & Kantardjiev, T. (2019). Q fever in Bulgaria: Laboratory and epidemiological findings on human cases and outbreaks, 2011 to 2017. Euro Surveillance, 24, 37. 10.2807/1560-7917.Es.2019.24.37.1900119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Georgiev, M. , Afonso, A. , Neubauer, H. , Needham, H. , Thiéry, R. , Rodolakis, A. , Roest, H. J. , Stärk, K. D. , Stegeman, J. A. , Vellema, P. , van der Hoek, W. , & More, S. J. (2013). Q fever in humans and farm animals in four European countries, 1982 to 2010. Eurosurveillance, 18. 10.2807/ese.18.08.20407-en [DOI] [PubMed] [Google Scholar]
- Goel, K. , Sen, A. , Satapathy, P. , Kumar, P. , Aggarwal, A. K. , Sah, R. , & Padhi, B. K. (2023). Human rabies control in the era of post‐COVID‐19: A call for action. Journal of Travel Medicine, 1–4. 10.1093/jtm/taad009 [DOI] [PubMed] [Google Scholar]
- Gormley, E. , O'Keeffe, J. , Murphy, D. , Aldwell, F. E. , Fitzsimons, T. , Stanley, P. , Tratalos, J. A. , McGrath, G. , Fogarty, N. , Kenny, K. , More, S. J. , Messam, L. L. , & Corner, L. A. (2017). Oral vaccination of free‐living badgers (Meles meles) with Bacille Calmette Guérin (BCG) vaccine confers protection against tuberculosis. PLoS One, 12(1), e0168851. 10.1371/journal.pone.0168851 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halbedel, S. , Sperle, I. , Lachmann, R. , Kleta, S. , Fischer, M. A. , Wamp, S. , Holzer, A. , Lüth, S. , Murr, L. , Freitag, C. , Espenhain, L. , Stephan, R. , Pietzka, A. , Schjørring, S. , Bloemberg, G. , Wenning, M. , Dahouk, S. A. , Wilking, H. , & Flieger, A. (2023). Large multicountry outbreak of invasive Listeriosis by a listeria monocytogenes ST394 clone linked to smoked rainbow trout, 2020 to 2021. Microbiology Spectrum, 11(3), e03520–e03522. 10.1128/spectrum.03520-22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haussig, J. M. , Young, J. J. , Gossner, C. M. , Mezei, E. , Bella, A. , Sirbu, A. , Pervanidou, D. , Drakulovic, M. B. , & Sudre, B. (2018). Early start of the West Nile fever transmission season 2018 in Europe. Euro Surveillance, 23(32). 10.2807/1560-7917.Es.2018.23.32.1800428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- He, S. , Simpson, B. K. , Sun, H. , Ngadi, M. O. , Ma, Y. , & Huang, T. (2018). Phaseolus vulgaris lectins: A systematic review of characteristics and health implications. Critical Reviews in Food Science and Nutrition, 58(1), 70–83. 10.1080/10408398.2015.1096234 [DOI] [PubMed] [Google Scholar]
- Hennebique, A. , Boisset, S. , & Maurin, M. (2019). Tularemia as a waterborne disease: A review. Emerging Microbes Infections, 8(1), 1027–1042. 10.1080/22221751.2019.1638734 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hernández‐Triana, L. M. , Jeffries, C. L. , Mansfield, K. L. , Carnell, G. , Fooks, A. R. , & Johnson, N. (2014). Emergence of west nile virus lineage 2 in europe: A review on the introduction and spread of a mosquito‐borne disease. Frontiers in Public Health, 2, 271. 10.3389/fpubh.2014.00271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hestvik, G. , Warns‐Petit, E. , Smith, L. A. , Fox, N. J. , Uhlhorn, H. , Artois, M. , Hannant, D. , Hutchings, M. R. , Mattsson, R. , Yon, L. , & Gavier‐Widen, D. (2015). The status of tularemia in Europe in a one‐health context: A review. Epidemiology and Infection, 143(10), 2137–2160. 10.1017/s0950268814002398 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubálek, Z. , & Halouzka, J. (1999). West Nile fever–a reemerging mosquito‐borne viral disease in Europe. Emerging Infectious Diseases, 5(5), 643–650. 10.3201/eid0505.990505 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurtado, A. , Zendoia, I. I. , Alonso, E. , Beraza, X. , Bidaurrazaga, J. , Ocabo, B. , Arrazola, I. , Cevidanes, A. , Barandika, J. F. , & García‐Pérez, A. L. (2023). A Q fever outbreak among visitors to a natural cave, Bizkaia, Spain, December 2020 to October 2021. Eurosurveillance, 28(28), 2200824. 10.2807/1560-7917.ES.2023.28.28.2200824 [DOI] [PMC free article] [PubMed] [Google Scholar]
- IMH (Italian Ministry of Health) . (2019). Piano Nazionale di prevenzione, sorveglianza e risposta alle Arbovirosi (PNA) 2020–2025 . https://www.salute.gov.it/imgs/C_17_pubblicazioni_2947_allegato.pdf
- ISO (International Organization for Standardization) . (2001). ISO 16654:2001. Microbiology of Food and Animal Feeding Stuffs – Horizontal Method for the Detection of Escherichia Coli O157 . [DOI] [PubMed]
- ISO (International Organization for Standardization) . (2012). ISO TS 13136:2012. Microbiology of food and animal feed – Real‐time polymerase chain reaction (PCR)‐based method for the detection of food‐borne pathogens – Horizontal method for the detection of Shiga toxin‐producing Escherichia coli (STEC) and the determination of O157, O111, O26, O103 and O145 serogroups .
- ISO (International Organization for Standardization) . (2015). ISO/TS 18867:2015, microbiology of the food chain polymerase chain reaction (PCR) for the detection of food‐borne pathogens. Detection of pathogenic Yersinia enterocolitica and Yersinia pseudotuberculosis .
- Jonckers Nieboer, L. F. W. , Fischer, E. A. J. , & Braks, M. A. H. (2023). Available evidence for mosquito‐borne Francisella tularensis transmission is inconclusive. Frontiers in Tropical Diseases, 4. 10.3389/fitd.2023.1230903 [DOI] [Google Scholar]
- Karlsson, P. A. , Tano, E. , Jernberg, C. , Hickman, R. A. , Guy, L. , Järhult, J. D. , & Wang, H. (2021). Molecular characterization of multidrug‐resistant Yersinia enterocolitica from foodborne outbreaks in Sweden. Frontiers in Microbiology, 12, 664665. 10.3389/fmicb.2021.664665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kärssin, A. , Remes, N. , Korge, K. , Viigipuu, M. , Stensvold, C. R. , Gómez‐Morales, M. A. , Ludovisi, A. , Jokelainen, P. , & Lassen, B. (2021). Herbivores as accidental hosts for trichinella: Search for evidence of trichinella infection and exposure in free‐ranging moose (alces alces) in a highly endemic setting. Journal of Wildlife Diseases, 57(1), 116–124. 10.7589/jwd-d-19-00011 [DOI] [PubMed] [Google Scholar]
- Kefaloudi, C. , Mellou, K. , Dougas, G. , Vorou, R. , Mitrou, K. , & Kontopidou, F. (2022). Human brucellosis in Greece, 2005‐2020: A persistent public health problem. Vector‐Borne and Zoonotic Diseases, 22(3), 163–169. 10.1089/vbz.2021.0050 [DOI] [PubMed] [Google Scholar]
- Kenney, A. , Cusick, A. , Payne, J. , Gaughenbaugh, A. , Renshaw, A. , Wright, J. , Seeber, R. , Barnes, R. , Florjanczyk, A. , & Horzempa, J. (2017). The potential for flower nectar to allow mosquito to mosquito transmission of Francisella tularensis. PLoS One, 12(5), e0175157. 10.1371/journal.pone.0175157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kern, P. , Bardonnet, K. , Renner, E. , Auer, H. , Pawlowski, Z. , Ammann, R. W. , Vuitton, D. A. , & Kern, P. (2003). European echinococcosis registry: Human alveolar echinococcosis, Europe, 1982–2000. Emerging Infectious Diseases, 9(3), 343–349. 10.3201/eid0903.020341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keto‐Timonen, R. , Tolvanen, R. , Lundén, J. , & Korkeala, H. (2007). An 8‐year surveillance of the diversity and persistence of listeria monocytogenes in a chilled food processing plant analyzed by amplified fragment length polymorphism. Journal of Food Protection, 70(8), 1866–1873. 10.4315/0362-028X-70.8.1866 [DOI] [PubMed] [Google Scholar]
- Klevar, S. , Høgåsen, H. R. , Davidson, R. K. , Hamnes, I. S. , Treiberg Berndtsson, L. , & Lund, A. (2015). Cross‐border transport of rescue dogs may spread rabies in Europe. The Veterinary Record, 176(26), 672. 10.1136/vr.102909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kolwijck, E. , Lutgens, S. P. M. , Visser, V. X. N. , van Apeldoorn, M. J. , Graham, H. , Koets, A. P. , Schrauwen, M. M. W. P. , Reubsaet, F. A. G. , Broens, E. M. , & Kortbeek, L. M. (2022). First case of human Brucella canis infection in The Netherlands. Clinical Infectious Diseases, 75(12), 2250–2252. 10.1093/cid/ciac425 [DOI] [PubMed] [Google Scholar]
- Koopmans, M. M. , Brouwer, M. C. , Vázquez‐Boland, J. A. , & van de Beek, D. (2023). Human Listeriosis. Clinical Microbiology Reviews, 36(1), e0006019. 10.1128/cmr.00060-19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuhn, K. G. , Nygård, K. M. , Guzman‐Herrador, B. , Sunde, L. S. , Rimhanen‐Finne, R. , Trönnberg, L. , Jepsen, M. R. , Ruuhela, R. , Wong, W. K. , & Ethelberg, S. (2020). Campylobacter infections expected to increase due to climate change in northern Europe. Scientific Reports, 10(1), 13874. 10.1038/s41598-020-70593-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwit, N. A. , Middaugh, N. A. , VinHatton, E. S. , Melman, S. D. , Onischuk, L. , Aragon, A. S. , Nelson, C. A. , Mead, P. S. , & Ettestad, P. J. (2020). Francisella tularensis infection in dogs: 88 cases (2014–2016). Journal of the American Veterinary Medical Association, 256(2), 220–225. 10.2460/javma.256.2.220 [DOI] [PubMed] [Google Scholar]
- Lake, I. R. , Colón‐González, F. J. , Takkinen, J. , Rossi, M. , Sudre, B. , Dias, J. G. , Tavoschi, L. , Joshi, A. , Semenza, J. C. , & Nichols, G. (2019). Exploring campylobacter seasonality across Europe using the European surveillance system (TESSy), 2008 to 2016. Euro Surveillance, 24(13). 10.2807/1560-7917.Es.2019.24.13.180028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lalošević, D. , Živojinov, M. , Isaković, V. , Ivanov, D. , Trivunović, V. , & Ružić, M. (2023). The first human case of multilocular echinococcosis recognized in Serbia. Serbian Archives of Medicine, 151(7–8), 453–456. 10.2298/SARH230112060L [DOI] [Google Scholar]
- Lamont, R. F. , Sobel, J. , Mazaki‐Tovi, S. , Kusanovic, J. P. , Vaisbuch, E. , Kim, S. K. , Uldbjerg, N. , & Romero, R. (2011). Listeriosis in human pregnancy: A systematic review. Journal of Perinatal Medicine, 39(3), 227–236. 10.1515/jpm.2011.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langkabel, N. , Meemken, D. , Li, T.‐T. , Sotiraki, S. , Anastasiadou, S. , Nesbakken, T. , & Langforth, S. (2023). Use of harmonised epidemiological indicators (HEIs) for broilers in Europe. Food Control, 154, 110020. 10.1016/j.foodcont.2023.110020 [DOI] [Google Scholar]
- Maier, T. , Schwarting, A. , Mauer, D. , Ross, R. S. , Martens, A. , Kliem, V. , Wahl, J. , Panning, M. , Baumgarte, S. , Müller, T. , Pfefferle, S. , Ebel, H. , Schmidt, J. , Tenner‐Racz, K. , Racz, P. , Schmid, M. , Strüber, M. , Wolters, B. , Gotthardt, D. , … Drosten, C. (2010). Management and outcomes after multiple corneal and solid organ transplantations from a donor infected with rabies virus. Clinical Infectious Diseases, 50(8), 1112–1119. 10.1086/651267 [DOI] [PubMed] [Google Scholar]
- Marini, G. , Manica, M. , Delucchi, L. , Pugliese, A. , & Rosà, R. (2021). Spring temperature shapes West Nile virus transmission in Europe. Acta Tropica, 215, 105796. 10.1016/j.actatropica.2020.105796 [DOI] [PubMed] [Google Scholar]
- Marinković, D. , Gavrilović, P. , Vidanović, D. , Ćirović, D. , Kuručki, M. , Vasković, N. , & Aničić, M. (2022). First report of alveolar hydatid disease (Echinococcus multilocularis) in a Golden jackal (Canis aureus). Acta Parasitologica, 67(3), 1401–1406. 10.1007/s11686-022-00556-y [DOI] [PubMed] [Google Scholar]
- Maurin, M. , & Gyuranecz, M. (2016). Tularaemia: Clinical aspects in Europe. The Lancet Infectious Diseases, 16(1), 113–124. 10.1016/S1473-3099(15)00355-2 [DOI] [PubMed] [Google Scholar]
- Miljević, M. , Lalošević, D. , Simin, V. , Blagojević, J. , Čabrilo, B. , & Čabrilo, O. B. (2021). Intestinal helminth infections in the golden jackal (Canis aureus L.) from Vojvodina: Hotspot area of multilocular echinococcosis in Serbia. Acta Veterinaria Hungarica, 69(3), 274–281. 10.1556/004.2021.00030 [DOI] [PubMed] [Google Scholar]
- Mínguez‐González, O. , Gutiérrez‐Martín, C. B. , Martínez‐Nistal, M. D. C. , Esquivel‐García, M. D. R. , Gómez‐Campillo, J. I. , Collazos‐Martínez, J. , Fernández‐Calle, L. M. , Ruiz‐Sopeña, C. , Tamames‐Gómez, S. , Martínez‐Martínez, S. , Caminero‐Saldaña, C. , Hernández, M. , Rodríguez‐Lázaro, D. , & Rodríguez‐Ferri, E. F. (2021). Tularemia outbreaks in Spain from 2007 to 2020 in humans and domestic and wild animals. Pathogens, 10(7). 10.3390/pathogens10070892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monteiro, C. A. , Moubarac, J. C. , Cannon, G. , Ng, S. W. , & Popkin, B. (2013). Ultra‐processed products are becoming dominant in the global food system. Obesity Reviews, 14(S2), 21–28. 10.1111/obr.12107 [DOI] [PubMed] [Google Scholar]
- Montoro‐Dasi, L. , Lorenzo‐Rebenaque, L. , Marco‐Fuertes, A. , Vega, S. , & Marin, C. (2023). Holistic strategies to control salmonella Infantis: An emerging challenge in the European broiler sector. Microorganisms, 11(7), 1765. 10.3390/microorganisms11071765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moreno, E. , Blasco, J. M. , Letesson, J. J. , Gorvel, J. P. , & Moriyón, I. (2022). Pathogenicity and its implications in taxonomy: The Brucella and Ochrobactrum case. Pathogens, 11(3). 10.3390/pathogens11030377 [DOI] [PMC free article] [PubMed] [Google Scholar]
- NACMCF (National Advisory Committee on Microbiological Criteria for Foods) . (2019). Response to questions posed by the Food and Drug Administration regarding virulence factors and attributes that define foodborne Shiga toxin‐producing Escherichia coli (STEC) as severe human pathogens. Journal of Food Protection, 82(5), 724–767. 10.4315/0362-028x.Jfp-18-479 [DOI] [PubMed] [Google Scholar]
- NMKL (Nordisk Metodikkomité for Næringsmidler ‐ Nordic Committee on Food Analysis) . (2005). Escherichia coli O157. Detection in food and feeding stuffs. NMKL No. 164, 2 . http://www.nmkl.org/index.php?option=com_zoo&task=item&item_id=337&Itemid=319&lang=en
- Oksanen, A. , Siles‐Lucas, M. , Karamon, J. , Possenti, A. , Conraths, F. J. , Romig, T. , Wysocki, P. , Mannocci, A. , Mipatrini, D. , La Torre, G. , Boufana, B. , & Casulli, A. (2016). The geographical distribution and prevalence of Echinococcus multilocularis in animals in the European Union and adjacent countries: A systematic review and meta‐analysis. Parasites & Vectors, 9(1), 519. 10.1186/s13071-016-1746-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omeragić, J. , Goletić, T. , Softić, A. , Goletić, Š. , Kapo, N. , Soldo, D. K. , Šupić, J. , Škapur, V. , Čerkez, G. , Ademović, E. , Semren, O. , & Alić, A. (2022). First detection of Echinococcus multilocularis in Bosnia and Herzegovina. International Journal for Parasitology: Parasites and Wildlife, 19, 269–272. 10.1016/j.ijppaw.2022.11.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Opsteegh, M. , Kortbeek, T. M. , Havelaar, A. H. , & van der Giessen, J. W. (2015). Intervention strategies to reduce human toxoplasma gondii disease burden. Clinical Infectious Diseases, 60(1), 101–107. 10.1093/cid/ciu721 [DOI] [PubMed] [Google Scholar]
- Opsteegh, M. , Spano, F. , Aubert, D. , Balea, A. , Burrells, A. , Cherchi, S. , Cornelissen, J. B. W. J. , Dam‐Deisz, C. , Guitian, J. , Györke, A. , Innes, E. A. , Katzer, F. , Limon, G. , Possenti, A. , Pozio, E. , Schares, G. , Villena, I. , Wisselink, H. J. , & van der Giessen, J. W. B. (2019). The relationship between the presence of antibodies and direct detection of toxoplasma gondii in slaughtered calves and cattle in four European countries. International Journal for Parasitology, 49(7), 515–522. 10.1016/j.ijpara.2019.01.005 [DOI] [PubMed] [Google Scholar]
- Ottaiano, M. , Brunetti, R. , Calistri, P. , Di Lorenzo, A. , Di Sabatino, D. , Cito, F. , Chiodini, P. , Baldi, L. , & De Carlo, E. (2022). Risk factors for the persistence and spread of Brucellosis in buffaloes in the province of Caserta (2015–2020) . https://brucellosis2022.izs.it/wp‐content/uploads/2022/09/Conference_Proceedings_Brucellosis2022.pdf
- Pacenti, M. , Sinigaglia, A. , Franchin, E. , Pagni, S. , Lavezzo, E. , Montarsi, F. , Capelli, G. , & Barzon, L. (2020). Human West Nile virus lineage 2 infection: Epidemiological, clinical, and Virological findings. Viruses, 12(4). 10.3390/v12040458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Papa, A. , Xanthopoulou, K. , Gewehr, S. , & Mourelatos, S. (2011). Detection of West Nile virus lineage 2 in mosquitoes during a human outbreak in Greece. Clinical Microbiology and Infection, 17(8), 1176–1180. 10.1111/j.1469-0691.2010.03438.x [DOI] [PubMed] [Google Scholar]
- Persad, A. K. , & LeJeune, J. T. (2014). Animal reservoirs of Shiga toxin‐producing Escherichia coli. Microbiology Spectrum, 2(4), Ehec‐0027‐2014. 10.1128/microbiolspec.EHEC-0027-2014 [DOI] [PubMed] [Google Scholar]
- Pervanidou, D. , Kefaloudi, C. N. , Vakali, A. , Tsakalidou, O. , Karatheodorou, M. , Tsioka, K. , Evangelidou, M. , Mellou, K. , Pappa, S. , Stoikou, K. , Bakaloudi, V. , Koliopoulos, G. , Stamoulis, K. , Patsoula, E. , Politis, C. , Hadjichristodoulou, C. , & Papa, A. (2023). The 2022 West Nile virus season in Greece; a quite intense season. Viruses, 15(7). 10.3390/v15071481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pervanidou, D. , Vakali, A. , Georgakopoulou, T. , Panagiotopoulos, T. , Patsoula, E. , Koliopoulos, G. , Politis, C. , Stamoulis, K. , Gavana, E. , Pappa, S. , Mavrouli, M. , Emmanouil, M. , Sourvinos, G. , Mentis, A. , Tsakris, A. , Hadjichristodoulou, C. , Tsiodras, S. , & Papa, A. (2020). West Nile virus in humans, Greece, 2018: The largest seasonal number of cases, 9 years after its emergence in the country. Eurosurveillance, 25(32), 1900543. 10.2807/1560-7917.ES.2020.25.32.1900543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pessoa, J. , Rodrigues da Costa, M. , Nesbakken, T. , Meemken, D. , & RIBMINS Cost Action . (2021). Assessment of the effectiveness of pre‐harvest meat safety interventions to control foodborne pathogens in broilers: A systematic review. Current Clinical Microbiology Reports, 8(2), 21–30. 10.1007/s40588-021-00161-z [DOI] [Google Scholar]
- Petrin, S. , Wijnands, L. , Benincà, E. , Mughini‐Gras, L. , Delfgou‐van Asch, E. H. M. , Villa, L. , Orsini, M. , Losasso, C. , Olsen, J. E. , & Barco, L. (2023). Assessing phenotypic virulence of salmonella enterica across serovars and sources. Frontiers in Microbiology, 14. 10.3389/fmicb.2023.1184387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petsios, S. , Fredriksson‐Ahomaa, M. , Sakkas, H. , & Papadopoulou, C. (2016). Conventional and molecular methods used in the detection and subtyping of Yersinia enterocolitica in food. International Journal of Food Microbiology, 237, 55–72. 10.1016/j.ijfoodmicro.2016.08.015 [DOI] [PubMed] [Google Scholar]
- Possenti, A. , Manzano‐Román, R. , Sánchez‐Ovejero, C. , Boufana, B. , La Torre, G. , Siles‐Lucas, M. , & Casulli, A. (2016). Potential risk factors associated with human cystic echinococcosis: Systematic review and meta‐analysis. PLoS Neglected Tropical Diseases, 10, e0005114. 10.1371/journal.pntd.0005114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pozio, E. (2014). Searching for Trichinella: Not all pigs are created equal. Trends in Parasitology, 30(1), 4–11. 10.1016/j.pt.2013.11.001 [DOI] [PubMed] [Google Scholar]
- Pozio, E. (2016). Trichinella pseudospiralis an elusive nematode. Veterinary Parasitology, 231, 97–101. 10.1016/j.vetpar.2016.03.021 [DOI] [PubMed] [Google Scholar]
- Pozio, E. , Celli, M. , Ludovisi, A. , Interisano, M. , Amati, M. , & Gómez‐Morales, M. A. (2021). Animal welfare and zoonosis risk: Anti‐Trichinella antibodies in breeding pigs farmed under controlled housing conditions. Parasites and Vectors, 14(1), 417. 10.1186/s13071-021-04920-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pozio, E. , Rinaldi, L. , Marucci, G. , Musella, V. , Galati, F. , Cringoli, G. , Boireau, P. , & La Rosa, G. (2009). Hosts and habitats of Trichinella spiralis and Trichinella britovi in Europe. International Journal for Parasitology, 39(1), 71–79. 10.1016/j.ijpara.2008.06.006 [DOI] [PubMed] [Google Scholar]
- ProMED‐mail . (2021). Q fever‐Germany: (Berlin) sheep, human, laboratory staff, RFI. 26 September: 20210926.8698730 . https://www.promedmail.org
- Quereda, J. J. , Morón‐García, A. , Palacios‐Gorba, C. , Dessaux, C. , García‐Del Portillo, F. , Pucciarelli, M. G. , & Ortega, A. D. (2021). Pathogenicity and virulence of listeria monocytogenes: A trip from environmental to medical microbiology. Virulence, 12(1), 2509–2545. 10.1080/21505594.2021.1975526 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radoshevich, L. , & Cossart, P. (2018). Listeria monocytogenes: Towards a complete picture of its physiology and pathogenesis. Nature Reviews. Microbiology, 16(1), 32–46. 10.1038/nrmicro.2017.126 [DOI] [PubMed] [Google Scholar]
- Regnault, B. , Evrard, B. , Plu, I. , Dacheux, L. , Troadec, E. , Cozette, P. , Chrétien, D. , Duchesne, M. , Vallat, J. M. , Jamet, A. , Leruez, M. , Pérot, P. , Bourhy, H. , Eloit, M. , & Seilhean, D. (2022). First case of lethal encephalitis in Western Europe due to European bat lyssavirus type 1. Clinical Infectious Diseases, 74(3), 461–466. 10.1093/cid/ciab443 [DOI] [PubMed] [Google Scholar]
- Reisen, W. K. , Fang, Y. , & Martinez, V. M. (2006). Effects of temperature on the transmission of west nile virus by Culex tarsalis (Diptera: Culicidae). Journal of Medical Entomology, 43(2), 309–317. 10.1603/0022-2585(2006)043[0309:Eotott]2.0.Co;2 [DOI] [PubMed] [Google Scholar]
- Riccardo, F. , Bella, A. , Monaco, F. , Ferraro, F. , Petrone, D. , Mateo‐Urdiales, A. , Andrianou, X. D. , Del Manso, M. , Venturi, G. , Fortuna, C. , Di Luca, M. , Severini, F. , Caporali, M. G. , Morelli, D. , Iapaolo, F. , Pati, I. , Lombardini, L. , Bakonyi, T. , Alexandra, O. , … Palamara, A. T. (2022). Rapid increase in neuroinvasive West Nile virus infections in humans, Italy, July 2022. Eurosurveillance, 27(36). 10.2807/1560-7917.Es.2022.27.36.2200653 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riccardo, F. , Bolici, F. , Fafangel, M. , Jovanovic, V. , Socan, M. , Klepac, P. , Plavsa, D. , Vasic, M. , Bella, A. , Diana, G. , Rosi, L. , Pezzotti, P. , Andrianou, X. D. , Di Luca, M. , Venturi, G. , Maraglino, F. , Pervanidou, D. , Cenciarelli, O. , Baka, A. , … Suk, J. E. (2020). West Nile virus in Europe: After action reviews of preparedness and response to the 2018 transmission season in Italy, Slovenia, Serbia and Greece. Global Health, 16(1), 47. 10.1186/s12992-020-00568-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riccardo, F. , Monaco, F. , Bella, A. , Savini, G. , Russo, F. , Cagarelli, R. , Dottori, M. , Rizzo, C. , Venturi, G. , Di Luca, M. , Pupella, S. , Lombardini, L. , Pezzotti, P. , Parodi, P. , Maraglino, F. , Costa, A. N. , Liumbruno, G. M. , & Rezza, G. (2018). An early start of West Nile virus seasonal transmission: The added value of one heath surveillance in detecting early circulation and triggering timely response in Italy, June to July 2018. Euro Surveillance, 23(32). 10.2807/1560-7917.Es.2018.23.32.1800427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richter, J. , Esmann, L. , Lindner, A. K. , Trebesch, I. , Equihua‐Martinez, G. , Niebank, M. , Georgi, S. , Schürmann, D. , Pfäfflin, F. , Pasić, M. , & Gertler, M. (2019). Cystic echinococcosis in unaccompanied minor refugees from Afghanistan and the Middle East to Germany, July 2016 through June 2017. European Journal of Epidemiology, 34(6), 611–612. 10.1007/s10654-019-00492-8 [DOI] [PubMed] [Google Scholar]
- Robinson, E. , de Valk, H. , Villena, I. , Le Strat, Y. , & Tourdjman, M. (2021). National perinatal survey demonstrates a decreasing seroprevalence of toxoplasma gondii infection among pregnant women in France, 1995 to 2016: Impact for screening policy. Euro Surveillance, 26(5). 10.2807/1560-7917.Es.2021.26.5.1900710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosner, B. M. , Gassowski, M. , Albrecht, S. , & Stark, K. (2021). Investigating the campylobacter enteritis winter peak in Germany, 2018/2019. Scientific Reports, 11(1), 22902. 10.1038/s41598-021-02423-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rossi, P. , Tamarozzi, F. , Galati, F. , Akhan, O. , Cretu, C. M. , Vutova, K. , Siles‐Lucas, M. , Brunetti, E. , & Casulli, A. (2020). The European register of cystic echinococcosis, ERCE: State‐of‐the‐art five years after its launch. Parasites & Vectors, 13(1), 236. 10.1186/s13071-020-04101-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rząd, M. , Kanecki, K. , Lewtak, K. , Goryński, P. , Tyszko, P. , Lewandowska‐Andruszuk, I. , & Nitsch‐Osuch, A. (2023). Congenital toxoplasmosis among hospitalized infants in Poland in the years 2007–2021: Study based on the national hospital registry. Scientific Reports, 13(1), 11060. 10.1038/s41598-023-38270-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salines, M. , Lazou, T. , Gomez‐Luengo, J. , Holthe, J. , Nastasijevic, I. , Bouwknegt, M. , Dadios, N. , Houf, K. , Blagojevic, B. , & Antic, D. (2023). Risk categorisation of abattoirs in Europe: Current state of play. Food Control, 152, 109863. 10.1016/j.foodcont.2023.109863 [DOI] [Google Scholar]
- Samper‐Cativiela, C. , Diéguez‐Roda, B. , Trigo da Roza, F. , Ugarte‐Ruiz, M. , Elnekave, E. , Lim, S. , Hernández, M. , Abad, D. , Collado, S. , Sáez, J. L. , de Frutos, C. , Agüero, M. , Moreno, M. , Escudero, J. A. , & Álvarez, J. (2022). Genomic characterization of multidrug‐resistant salmonella serovar Kentucky ST198 isolated in poultry flocks in Spain (2011–2017). Microbial Genomics, 8(3), 000773. 10.1099/mgen.0.000773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sapountzis, P. , Segura, A. , Desvaux, M. , & Forano, E. (2020). An overview of the elusive passenger in the gastrointestinal tract of cattle: The Shiga toxin producing Escherichia coli . Microorganisms, 8(6), 877. 10.3390/microorganisms8060877 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schlech, W. F. (2019). Epidemiology and Clinical Manifestations of Listeria monocytogenes Infection. In: (ed.)^(eds.) Gram‐Positive Pathogens: Vol. Wiley Online Books, 793–802 10.1128/9781683670131.ch50 [DOI] [PMC free article] [PubMed]
- Scorpio, A. , & Zhang, Y. (1996). Mutations in pncA, a gene encoding pyrazinamidase/nicotinamidase, cause resistance to the antituberculous drug pyrazinamide in tubercle bacillus. Nature Medicine, 2(6), 662–667. 10.1038/nm0696-662 [DOI] [PubMed] [Google Scholar]
- Seiwald, S. , Simeon, A. , Hofer, E. , Weiss, G. , & Bellmann‐Weiler, R. (2020). Tularemia goes west: Epidemiology of an emerging infection in Austria. Microorganisms, 8(10), 1597. 10.3390/microorganisms8101597 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shoaib, M. , Shehzad, A. , Raza, H. , Niazi, S. , Khan, I. M. , Akhtar, W. , Safdar, W. , & Wang, Z. (2019). A comprehensive review on the prevalence, pathogenesis and detection of Yersinia enterocolitica . RSC Advanced, 9(70), 41010–41021. 10.1039/c9ra06988g [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sikkema, R. S. , Schrama, M. , van den Berg, T. , Morren, J. , Munger, E. , Krol, L. , van der Beek, J. G. , Blom, R. , Chestakova, I. , van der Linden, A. , Boter, M. , van Mastrigt, T. , Molenkamp, R. , Koenraadt, C. J. , van den Brand, J. M. , Oude Munnink, B. B. , Koopmans, M. P. , & van der Jeugd, H. (2020). Detection of West Nile virus in a common whitethroat (Curruca communis) and Culex mosquitoes in The Netherlands, 2020. Euro Surveillance, 25(40). 10.2807/1560-7917.Es.2020.25.40.2001704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siles‐Lucas, M. , Casulli, A. , Conraths, F. J. , & Müller, N. (2017). Laboratory diagnosis of Echinococcus spp. in human patients and infected animals. Advances in Parasitology, 96, 159–257. 10.1016/bs.apar.2016.09.003 [DOI] [PubMed] [Google Scholar]
- Sindičić, M. , Bujanić, M. , Štimac, I. , Martinković, F. , Tuškan, N. , Špehar, M. , & Konjević, D. (2018). First identification of Echinococcus multilocularis in golden jackals in Croatia. Acta Parasitologica, 63(3), 654–656. 10.1515/ap-2018-0076 [DOI] [PubMed] [Google Scholar]
- Széll, Z. , Marucci, G. , Pozio, E. , & Sréter, T. (2013). Echinococcus multilocularis and Trichinella spiralis in golden jackals (Canis aureus) of Hungary. Veterinary Parasitology, 197(1), 393–396. 10.1016/j.vetpar.2013.04.032 [DOI] [PubMed] [Google Scholar]
- Tamarozzi, F. , Akhan, O. , Cretu, C. M. , Vutova, K. , Akinci, D. , Chipeva, R. , Ciftci, T. , Constantin, C. M. , Fabiani, M. , Golemanov, B. , Janta, D. , Mihailescu, P. , Muhtarov, M. , Orsten, S. , Petrutescu, M. , Pezzotti, P. , Popa, A. C. , Popa, L. G. , Popa, M. I. , … Casulli, A. (2018). Prevalence of abdominal cystic echinococcosis in rural Bulgaria, Romania, and Turkey: A cross‐sectional, ultrasound‐based, population study from the HERACLES project. The Lancet Infectious Diseases, 18(7), 769–778. 10.1016/s1473-3099(18)30221-4 [DOI] [PubMed] [Google Scholar]
- Teunis, P. , Havelaar, A. , Vliegenthart, J. , & Roessink, G. (1997). Risk assessment of campylobacter species in shellfish: Identifying the unknown. Water Science and Technology, 35(11–12), 29–34. 10.2166/wst.1997.0705 [DOI] [Google Scholar]
- Teunis, P. F. , Falkenhorst, G. , Ang, C. W. , Strid, M. A. , De Valk, H. , Sadkowska‐Todys, M. , Zota, L. , Kuusi, M. , Rota, M. C. , Simonsen, J. B. , Mølbak, K. , Van Duynhoven, Y. T. , & Van Pelt, W. (2013). Campylobacter seroconversion rates in selected countries in the European Union. Epidemiology and Infection, 141(10), 2051–2057. 10.1017/s0950268812002774 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomljenovic, M. , Lakošeljac, D. , Knežević, L. , Bubonja‐Šonje, M. , Abram, M. , Špičić, S. , Zdelar‐Tuk, M. , Duvnjak, S. , Reil, I. , Valjin, O. , Kramarić, M. , Miškić, T. , Janković, I. L. , & Rončević, D. (2023). Coxiella burnetii (Q‐fever) outbreak associated with non‐occupational exposure in a semi‐urban area of western Croatia in 2022. Zoonoses and Public Health, 70(4), 285–293. 10.1111/zph.13022 [DOI] [PubMed] [Google Scholar]
- van Dijk, M. A. M. , Engelsma, M. , Visser, V. X. N. , Keur, I. , Holtslag, M. , Willems, N. , Meij, B. , Willemsen, P. T. J. , Wagenaar, J. , Roest, H. I. J. , & Broens, E. (2021). Transboundary spread of Brucella canis through import of infected dogs, The Netherlands, November 2016–December 2018. Emerging Infectious Disease Journal, 27(7), 1783–1788. 10.3201/eid2707.201238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Walle, I. , Björkman, J. T. , Cormican, M. , Dallman, T. , Mossong, J. , Moura, A. , Pietzka, A. , Ruppitsch, W. , & Takkinen, J. (2018). Retrospective validation of whole genome sequencing‐enhanced surveillance of listeriosis in Europe, 2010 to 2015. Euro Surveillance, 23(33). 10.2807/1560-7917.Es.2018.23.33.1700798 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wagenaar, J. A. , French, N. P. , & Havelaar, A. H. (2013). Preventing campylobacter at the source: Why is it so difficult? Clinical Infectious Diseases, 57(11), 1600–1606. 10.1093/cid/cit555 [DOI] [PubMed] [Google Scholar]
- WHO (World Health Organization) . (2007). WHO Guidelines on tularaemia . https://apps.who.int/iris/handle/10665/43793
- WHO (World Health Organization) . (2008). Foodborne disease outbreaks: Guidelines for investigation and control. World Health Organization, 162 pp . https://www.who.int/publications/i/item/9789241547222
- WHO (World Health Organization) . (2022). Global tuberculosis report. edn. Geneva, 68 pp. Licence: CC BY‐NC‐SA 3.0 IGO . https://www.who.int/publications/i/item/9789240061729
- WOAH (World Organisation for Animal Health) , 2023. Manual of diagnostic tests and vaccines for terrestrial animals, twelfth edition 2023. https://www.woah.org/en/what‐we‐do/standards/codes‐and‐manuals/terrestrial‐manual‐online‐access/. [Google Scholar]
- Young, J. J. , Haussig, J. M. , Aberle, S. W. , Pervanidou, D. , Riccardo, F. , Sekulić, N. , Bakonyi, T. , & Gossner, C. M. (2021). Epidemiology of human West Nile virus infections in the European Union and European Union enlargement countries, 2010 to 2018. Euro Surveillance, 26(19). 10.2807/1560-7917.Es.2021.26.19.2001095 [DOI] [PMC free article] [PubMed] [Google Scholar]