

Abstract
A young man presented with acute stabbing chest pain. A 12-lead electrocardiogram revealed electrical alternans with phasic variation of the QRS amplitude in all leads. Lung auscultation revealed absent left hemithorax breath sounds. Chest radiography confirmed a left-sided tension pneumothorax. Tension pneumothorax is a very rare cause for electrical alternans. (Level of Difficulty: Intermediate.)
Key Words: acute chest pain, electrical alternans, pneumothorax
Central Illustration
A 29-year-old male patient presented to the emergency department with acute-onset stabbing chest pain with irradiation to the back and worsening with inspiration. He had no other complaints, including dyspnea, orthopnea, syncope, or palpitations, and he was an ex-smoker. On examination, he was in moderate distress with significant pain. His blood pressure was 137/86 mm Hg, heart rate was 73 beats/min, respiratory rate was 22 breaths/min, oxygen saturation was 97% in room air, and temperature was 36.5 ºC. Breath sounds were globally decreased without wheezing or rales and were absent in the left hemithorax. The extremities were well perfused with strong and symmetric pulses. No edema or jugular venous distention was appreciated. A 12-lead electrocardiogram (ECG) was immediately performed (Figure 1).
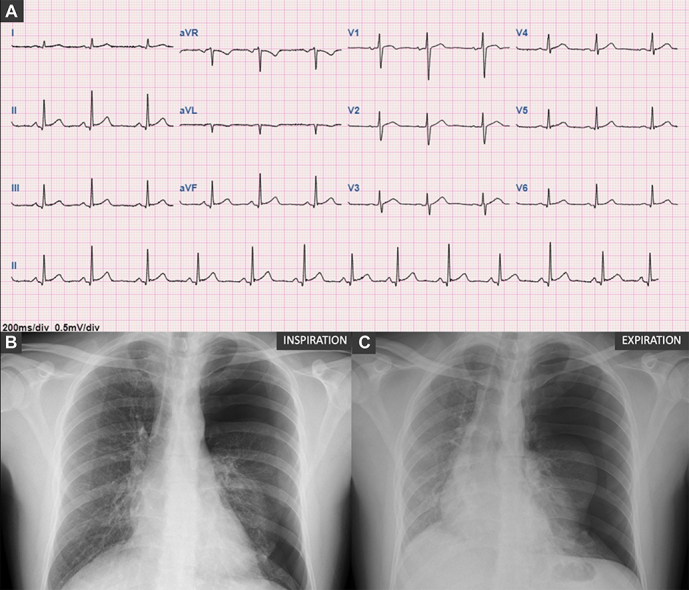
Figure 1.

12-Lead Electrocardiogram and Chest Radiography at Presentation
(A) 12-lead electrocardiogram: sinus rhythm of 76 beats/min, normal P-wave amplitude and duration, normal QRS axis and duration, and phasic variation of the QRS amplitude in all leads. Chest radiography showing (B) a large left pneumothorax in inspiration with (C) deviation to the right mediastinum in expiration.
What is the probable cause for the ECG changes:
-
1.
Pericardial effusion
-
2.
Acute coronary syndrome
-
3.
Hypertensive pneumothorax
-
4.
Interstitial lung disease
Discussion/Rationale
ECG revealed sinus rhythm, normal P-wave amplitude and duration, and normal QRS axis and duration with phasic variation of the QRS amplitude in all leads (Figure 1A). A chest radiography revealed a large left-side pneumothorax with collapse of the left lung and deviation to the right mediastinum with expiration (Figures 1B and 1C). Arterial blood gas and blood analyses were unremarkable. Analgesic medication was administered, and an urgent 18-F chest tube was placed in the fifth left intercostal space with immediate improvement of the symptoms. Control chest radiographs revealed complete re-expansion of the left lung, and 5 days later the drain was removed. An ECG after re-expansion of the lung showed normalization of the QRS voltage.
Electrical alternans is defined as variation in the QRS amplitude in any lead without additional changes in the conduction system of the heart and is caused by motion and rotation of the heart that causes variation and oscillation in the amplitude sign detected by the electrodes.1 This phenomenon is usually associated with cardiac pathologies, mainly those cursing with pericardial effusion and tamponade, or less frequently can be related to electrophysiological pathologies and digoxin medication.1 Pulmonary causes for electrical alternans are very rare, but severe cases of asthma and pleural effusion and rare cases of pneumothorax have been reported.1, 2, 3
Tension pneumothorax is a life-threatening condition that occurs when the air in the pleural space is not able to escape during expiration, increasing the pressure in the ipsilateral side and compressing the mediastinum. In severe cases, this mechanism can compress the heart and the vasculature with a reduction in cardiac output and venous return.3 The mechanism of electrical alternans in pneumothorax has been proposed to be related to the changes in the position of the heart and oscillation with respiration, and hemodynamic changes may coexist in severe cases.3 Other ECG-reported manifestations of pneumothorax, such as sinus tachycardia, high-amplitude P waves, P-wave inversion, inversion of precordial T waves, or low-amplitude QRS voltage, were not present in this case. The normalization of the ECG after re-expansion of the lung corroborates the pneumothorax as the cause of electrical alternans.
Funding Support and Author Disclosure
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Footnotes
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center.
References
- 1.Ingram D., Strecker-McGraw M.K. StatPearls; 2022. Electrical Alternans. [Google Scholar]
- 2.Schmidt D.C., Andersson C., Schultz H.H. ECG with alternating electric axis in relation to left-sided tension pneumothorax: a case report and review of the literature. Eur Clin Respir J. 2018;5(1) doi: 10.1080/20018525.2018.1495982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kuritzky P., Goldfarb A.L. Unusual electrocardiographic changes in spontaneous pneumothorax. Chest. 1976;70(4):535–537. doi: 10.1378/chest.70.4.535. [DOI] [PubMed] [Google Scholar]