

Abstract
A substudy of ghrelin treatment in a multicenter trial previously revealed that administration of ghrelin improves the exercise capacity of underweight COPD patients. To clarify exertional dyspnea more precisely, exploratory analysis was conducted on data from the substudy. Of 20 underweight COPD patients who were randomized to pulmonary rehabilitation with intravenous ghrelin (2 μg/kg, n = 10) or placebo (n = 10) twice daily for 3 weeks in the substudy, 16 (ghrelin = 9, placebo = 7) could be investigated for dyspnea break-point on the dyspnea-ratio (%) of Δoxygen uptake () (= peak minus resting ) curve. A significant treatment effect of ghrelin on percentage at the dyspnea break-point to Δ (p = 0.049) was achieved. In conclusion, underweight COPD patients benefitted from ghrelin treatment in terms of shifts to the early exercise phase of the dyspnea break-point during a standardized exercise program.
Keywords: Dyspnea, Exercise, Pulmonary rehabilitation, Lactate threshold, Underweight
Introduction
Exertional dyspnea is a major symptom of patients with chronic obstructive pulmonary disease (COPD) [1–3], especially in its advanced stages, characterized by significant systemic deterioration, so-called pulmonary cachexia [4–6]. Ventilatory limitation in conjunction with exertional dyspnea is an important reason COPD patients stop exercise [3, 7–9]. For patients with respiratory diseases we have previously shown that:
dyspnea during exercise reached a break-point at which the level of dyspnea started to increase more steeply; and
the break-point in dyspnea occurred at a similar point to the lactate threshold point [10–13].
Such approaches might provide clues to the physiological mechanisms of exertional dyspnea. However, the development of effective treatments for exertional dyspnea among these patients remains important.
Ghrelin, a 28-amino acid peptide, was first identified in 1999, when it was isolated from rat stomach as an endogenous ligand of the growth hormone (GH) secretagogue receptor (GHSR) [14]. Ghrelin may have many beneficial effects for COPD patients, via GH-dependent and GH-independent mechanisms [15–18]. An open-label pilot study previously showed that ghrelin may improve walking distance and symptoms for underweight COPD patients [19]. These encouraging results prompted us to undertake a multicenter, randomized, double-blind, placebo-controlled trial of ghrelin with 33 COPD patients; this showed that ghrelin administration improved symptoms and respiratory muscle strength [20]. In parallel with the main multicenter trial, to understand the precise mechanism that underlies the improvement of exercise performance or symptoms, a substudy with 20 COPD patients was conducted in a single center (Toneyama National Hospital) as part of the main multicenter trial [21]. The substudy showed that ghrelin administration improved exercise capacity and ventilatory cardiac data, but that endurance time was not increased after administration of ghrelin; in other words, COPD patients treated with ghrelin could exercise more rapidly. Absolute dyspnea level during exercise was not significantly improved compared with placebo [21], however, which suggests a discrepancy between improved physiological findings and measures of direct patient benefit, i.e., exertional dyspnea level. Therefore, after completion of the main multicenter trial, including the substudy, to clarify more precisely the exertional dyspnea pattern after treatment with ghrelin, we examined, for a subpopulation of the substudy (n = 20), whether ghrelin administration affects the break-point in dyspnea during exercise. Sixteen patients could be analyzed for break-point evaluations in an exploratory manner by use of data from the substudy. Preliminary data included in this article have previously been presented in abstract form [22].
Methods
Subjects
The eligibility criteria for the substudy [21] included:
severe to very severe COPD (forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) (= FEV1 %) of less than 70 and %FEV1 of less than 50 %);
underweight (body mass index (BMI) <21 kg/m2);
clinically stable and able to participate in pulmonary rehabilitation (PR);
between 20 and 85 years old; and
signed agreement for participation in this study.
Exclusion criteria for the substudy [21] were:
malignant tumors;
active infection;
severe heart disease;
hepatic dysfunction (serum levels of aspartate aminotransferase and alanine aminotransferase twice, or more, the upper limit of normal);
asthma;
definitely or possibly pregnant;
change in drug regimen within 4 weeks before participation in this study; or
judged to be unable to participate in this study by their physician, in addition to the above exclusion criteria.
Of the patients who completed the substudy, patients who were able:
to tolerate both the pre and post-cardiopulmonary exercise testing (CPET) for at least 4 min (that is, ≥4 measurement points) to ensure adequate dyspnea break-point evaluation; and
to reach the dyspnea break-point determined by using the intersection of two lines on plots of individual dyspnea– curves during exercise in both the pre- and post CPETs
were included in the evaluation.
Study design
The substudy, which led to this exploratory study, was a 3-week, randomized, double-blind, placebo-controlled trial of ghrelin administration during PR conducted at a single center as part of the main multicenter trial between September 1, 2005 and May 14, 2009 [20]. The substudy protocol was approved by the ethics committee of the National Hospital Organization Toneyama National Hospital (approval number 0311) and was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants were fully informed of the risks associated with the study before giving their written informed consent (in Japanese). Eligible participants were randomly assigned in a 1:1 ratio to receive 3-week PR with either ghrelin (2 μg/kg, ghrelin solution with 10 mL saline) or placebo (Fig. 1). The randomization list was generated by a statistician from Hamamatsu University School of Medicine not participating in the study, and it was kept strictly confidential until completion of the study. Randomization was performed in our center, which was involved in the main multicenter study. Neither the investigators nor the patients were unaware of the treatment. The main multicenter study, including the substudy, was registered at https://upload.umin.ac.jp/cgi-open-bin/ctr/ctr.cgi?function=brows&action=brows&type=summary&recptno=R000000103&language=E (number C000000061). Of all the patients (n = 20) who completed the substudy, 16 (ghrelin group, n = 9; placebo group, n = 7) were able to tolerate both pre and post CPETs to ensure adequate analysis for the break-point evaluations, and their data were analyzed for break-point evaluations in an exploratory manner.
Fig. 1.
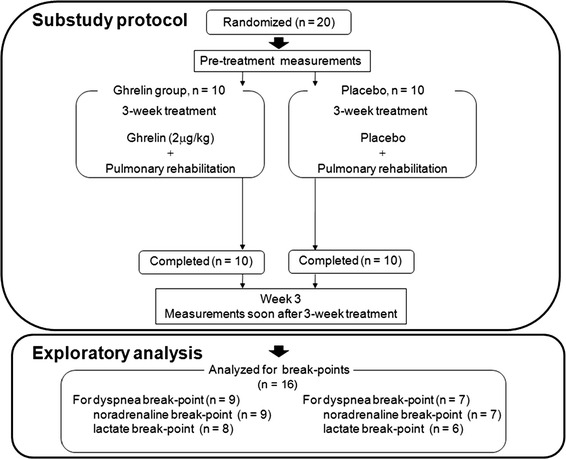
Outline of the study design. The substudy was conducted in a single center (Toneyama National Hospital) as part of the main multicenter trial. In this study, of 20 patients in the substudy, 16 patients could be analyzed the break-point evaluations in an exploratory manner by use of data from the substudy
Preparation of human ghrelin
Human ghrelin was prepared as described elsewhere [19–21]. Administration of ghrelin (2 μg/kg) or placebo was performed intravenously over 30 min and repeated twice a day for 3 weeks in hospital.
Pulmonary rehabilitation (PR)
Exercise training included in the PR program was conducted with high-intensity targets as described elsewhere [21]. The PR program included disease education, breathing control techniques, and exercise training. The exercise training sessions were performed as three sets daily, 5 days a week, for 3 weeks, by use of electromechanically braked cycle ergometers.
Outcome measures
For the exploratory analysis, the outcomes were changes in dyspnea break-point, lactate break-point, and noradrenaline break-point, which were determined from the point of intersection of two lines on plots of individual dyspnea–, lactate (LT)– and noradrenaline (NA)– during exercise.
Procedures
Symptom-limited exercise tests were conducted on an electrically-braked cycle ergometer (CV-1000SS; Lode, Groningen, The Netherlands) with use of a CPET system (Vmaxs-29 C; CareFusion 207, Palm Springs, CA, USA). The incremental testing consisted of 2-min increments to 10 W, the protocol for which was different from that of the main multicenter study. Measurements were collected under room air conditions until subject exhaustion and included: breath-by-breath cardiopulmonary data; intensity of dyspnea (Borg scale); and arterial blood samples. Expired gas data were collected as 30-s averages at rest, during exercise at 2-min intervals, and at the end of the exercise. Dyspnea (Borg scale) and arterial blood were evaluated at rest, during the last 15 s of each exercise stage, and at the end of the exercise. Arterial blood samples for blood gas analysis, plasma noradrenaline, and plasma lactate were obtained and measured as described elsewhere [12].
Food intake
Food intake was evaluated as described elsewhere [20].
Data analysis
Break-point Break-points were determined for each patient who was able to tolerate both the pre and post-CPETs for at least 4 min (that is, ≥4 measurement points) to ensure adequate break-point evaluations. A break-point was determined for each patient by using the intersection of two lines on plots of individual dyspnea–O2 (Fig. 2), lactate (LT)–O2, and noradrenaline (NA)–O2 plots during exercise. The location (%) of each break-point relative to ΔO2 (= peak O2 − resting O2) that occurs during exercise was calculated for each patient by use of the equation 100 × (break-point O2 − resting )/Δ.
Fig. 2.
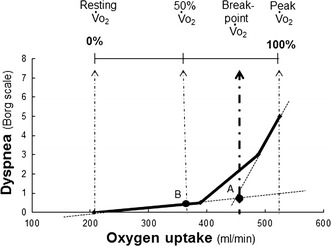
Dyspnea break-point (point A). First, a dyspnea break-point was determined for each patient by using the intersection of two lines on plots of dyspnea as a function of . Second, the location (%) of each resulting dyspnea break-point relative to Δ (= peak − resting ) that occurs during exercise was calculated for each patient by use of the equation 100 × (dyspnea break-point − resting )/Δ. 50 % point (point B). The value at the 50 % point was calculated for each patient by use of the equation resting + (peak − resting )/2. Next, the value of the Borg scale at the 50 % point was calculated for each patient, where the Borg scale on the Y axis corresponded to the 50 % point on the X axis by linear interpolation between adjacent measurement points
50 % point The value at the 50 % point during exercise was calculated for each patient as shown in Fig. 2. Next, each value (for instance, Borg scale) at each 50 % point was calculated by linear interpolation between adjacent measurement points, as described elsewhere [10].
Statistical analysis
Data are presented as means ± standard deviations, except where otherwise indicated. Fisher’s exact tests and Wilcoxon rank sum tests were used to compare baseline characteristics between the groups. Effects were examined once, soon after the 3-week intervention. The results at Week 3 were compared between the two groups by use of unpaired t tests. The significance level had previously been set at p < 0.05. (SAS 9.1.3; SAS Institute, Cary, NC, USA).
Results
Of all the patients (n = 20) who completed the substudy, the data for 16 patients could be analyzed for break-point evaluations (ghrelin group, n = 9; placebo group, n = 7). Break-points were not determined for 3 patients because their endurance times were less than 4 min (i.e., only 3 measurement points were obtained) in one of the pre or post CPETs. The other patient could not reach the break-points because endurance times were very short in CPET, even though 4 measurement points were obtained. There were no significant differences between baseline characteristics in the two groups (Table 1), but it is likely that differences between treatment strategies and cardiopulmonary function at baseline were large.
Table 1.
Patients’ baseline characteristicsa
| Ghrelin, n = 9 | Placebo, n = 7 | |
|---|---|---|
| Age, years | 69.8 (5.9) | 73.6 (4.6) |
| Sex, males/females | 9/0 | 6/1 |
| Height, cm | 161.8 (6.2) | 160.8 (6.0) |
| Weight, Kg | 49.6 (6.3) | 48.1 (8.8) |
| BMI, kg/m2 | 18.9 (2.0) | 18.5 (2.5) |
| Cigarettes, pack-years | 61.5 (29.9) | 62.8 (20.6) |
| Pulmonary function | ||
| FEV1, L | 0.81 (0.21) | 0.85 (0.26) |
| %FEV1, % predicted | 30.7 (9.1) | 35.1 (11.2) |
| FEV1/FVC, % | 41.8 (8.1) | 43.5 (9.1) |
| VC, L | 2.54 (0.44) | 2.74 (0.57) |
| %VC, % | 79.0 (11.4) | 91.2 (15.5) |
| RV, L | 2.80 (0.42) | 3.12 (0.66) |
| RV/TLC, % | 52.5 (7.3) | 53.1 (5.4) |
| IC, L | 1.51 (0.26) | 1.80 (0.34) |
| DLco, % predicted | 61.5 (25.2) | 79.1 (24.5) |
| Exercise capacity in ICPET | ||
| Peak work rate, Watts | 37.8 (13.0) | 37.1 (7.6) |
| Peak , mL/kg/min | 13.5 (3.8) | 14.3 (3.2) |
| Medications | ||
| LAMA | 7 | 3 |
| SAMA | 1 | 1 |
| LABA | 5 | 3 |
| ICS | 3 | 1 |
| Methylxanthines | 4 | 3 |
aThe groups shown represent all patients analyzed for dyspnea break-points both pre-treatment and post-treatment. Medications are not mutually exclusive, and data are presented separately
Data are presented as mean (SD) unless otherwise stated
BMI body mass index, DLco carbon monoxide diffusing capacity, FEV 1 forced expiratory volume in one second, FVC forced vital capacity, IC inspiratory capacity, ICPET incremental cardiopulmonary exercise test, ICS inhaled corticosteroids, LABA long-acting β2-agonist, LAMA long-acting muscarinic antagonist, RV residual volume, SAMA short-acting muscarinic antagonist, TLC total lung capacity, VC vital capacity
Exercise data and break-point in response to ghrelin
In this exploratory study, with incremental exercise, the distribution of reasons for stopping exercise did not differ between the ghrelin and placebo groups at pre-treatment. Most patients stopped primarily because of dyspnea (ghrelin group, 78 % vs. placebo group, 57 %), and fewer patients stopped because of leg discomfort only (ghrelin group, 22 % vs. placebo group, 43 %). The distributions post-treatment were quite similar to those pre-treatment. Peak (mL/kg/min) was significantly different in the ghrelin and placebo groups (mean difference from pre-treatment (ghrelin minus placebo), i.e., treatment effect, +1.2 mL/kg/min, 95 % CI, 0.0 to 2.5; p = 0.048), but there was no significant between-group difference in endurance time, the results for which were similar to those of the substudy [21]. At peak exercise, each mean difference in absolute dyspnea, absolute plasma noradrenaline level, and absolute plasma lactate level in the ghrelin group was similar to that in the placebo group (Fig. 3 and Table 2).
Fig. 3.
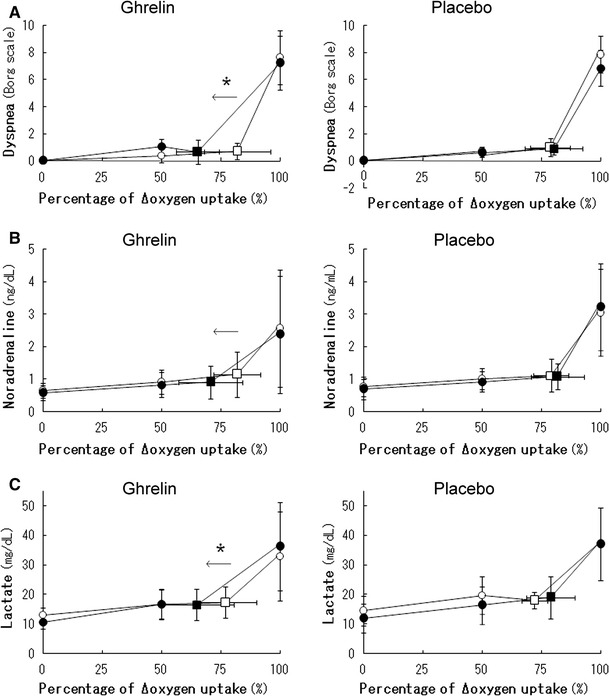
Cardiopulmonary data-ratios (%) from the Δ curves of COPD patients during pulmonary rehabilitation with ghrelin or placebo. Cardiopulmonary responses are plotted against the ratio (%) of Δ that occurs during exercise. Δ, increment in between resting and peak exercise; open symbols, pre-treatment values; solid symbols, post treatment values; square symbols, dyspnea, lactate, or noradrenaline break-point, with SD. Dyspnea, noradrenaline, and lactate break-points with ghrelin were determined for 9, 9, and 8 patients, respectively, and with placebo for 7, 7, and 6 patients, respectively. *P < 0.05, mean differences between pre-treatment and post-treatment were analyzed for the ghrelin and placebo groups by use of unpaired t tests. Treatment effect: mean difference from pre-treatment (ghrelin minus placebo)
Table 2.
Changes in peak incremental exercise data after pulmonary rehabilitation with ghrelin or placebo
| Ghrelin, n = 9 | Placebo, n = 7 | Treatment effect (95 % CI; p valuea) | |
|---|---|---|---|
| , mL/kg/min | 1.4 (0.9) | 0.1 (1.4) | 1.2 (0.0 to 2.5; 0.048) |
| , mL/min | 69.3 (48.6) | 8.4 (69.5) | 60.9 (−2.3 to 124.1; 0.058) |
| Endurance time, s | 56 (98) | 83 (53) | −27 (−115 to 61; 0.523) |
| Dyspnea, Borg | −0.4 (1.3) | −1.0 (1.8) | 0.6 (−1.1 to 2.2; 0.492) |
| Plasma LT, mg/dL | 2.8 (7.9) | 2.4 (12.0) | 0.4 (−10.2 to 11.0; 0.937) |
| Plasma NA, ng/mL | −0.19 (1.32) | 0.03 (0.94) | −0.22 (−1.49 to 1.05; 0.714) |
Data are presented as mean (SD) unless otherwise indicated. LT plasma lactate level, NA plasma noradrenaline level; Treatment effect mean difference from pre-treatment (ghrelin minus placebo); oxygen uptake
a Between-group difference (treatment effect) by unpaired t-test
The break-points for dyspnea, plasma noradrenaline, and lactate were compared by using standardized oxygen uptake. At pre-treatment, the exercise ratio of at each dyspnea, NA, or LT break-point to each Δ (= peak − resting ) occurred at a similar exercise point in the ghrelin and placebo groups (ghrelin group, mean (SD): dyspnea break-point, 82 % (9 %); NA break-point 82 % (10 %), LT break-point 77 % (13 %) vs. placebo group: dyspnea break-point, 79 % (8 %); NA break-point 79 % (7 %), LT break-point 72 % (5 %)). No treatment effect compared with placebo was found for the absolute Borg scale at the dyspnea break-point, for the absolute plasma noradrenaline level at the NA break-point, or for the absolute plasma lactate level at the LT break-point, as shown in Fig. 3. Of note, a significant treatment effect of ghrelin administration on percentage at the dyspnea break-point to Δ (treatment effect −18 %, 95 % CI −35.9 to −0.0, p = 0.049) was obtained, as shown in Fig. 3 and Table 3. However, there was no significant treatment effect of ghrelin administration on the absolute value of at the dyspnea break-point (treatment effect −43 mL/min, 95 % CI −143 to 56, p = 0.366). In addition, in the ghrelin group, the mean difference from pre-treatment in the percentage of at the dyspnea break-point was negatively correlated with the mean difference from pre-treatment in peak (r = −0.696, 95 %CI −0.9 to −0.1, p = 0.035) and positively correlated with the mean difference between pH at peak exercise (r = 0.737, 95 %CI 0.1 to 0.9, p = 0.021) but not with the mean difference between the resting (r = −0.055, 95 %CI −0.7 to 0.6, p = 0.893). Furthermore, the percentage of at the LT break-point to Δ was significantly shifted to the left in Fig. 3, compared with placebo (treatment effect −19 %, 95 % CI −34.1 to −4.2, p = 0.017).
Table 3.
Changes in break-points during pulmonary rehabilitation with ghrelin or placebo
| Ghrelin, % | Placebo, % | Treatment effect (95 % CI; p valuea) | |
|---|---|---|---|
| Dyspnea break-point | −17 (15) | 1 (18) | −18 (−35.9 to −0.0; 0.049) |
| Noradrenaline break-point | −11 (12) | 3 (16) | −14 (−29.1 to 1.0; 0.065) |
| Lactate break-point | −12 (12) | 7 (13) | −19 (−34.1 to −4.2; 0.017) |
Data are presented as mean difference, i.e., ghrelin minus placebo (SD). Dyspnea, noradrenaline, and lactate break-points with ghrelin were determined for 9, 9, and 8 patients, respectively, and with placebo for 7, 7, and 6 patients, respectively
%, ratio of each oxygen uptake () at the break-point to Δ (peak − resting ). Treatment effect: mean difference from pre-treatment (ghrelin minus placebo)
aBetween-group difference (treatment effect) by unpaired t-test
Food intake and body weight
No treatment effect compared with placebo, which was evaluated from pre-treatment, was found for food intake (treatment effect +143 kcal, 95 % CI −183 to 469, p = 0.363) after 3-week treatment, or for weight (treatment effect +0.2 kg, 95 % CI −1.1 to 1.6, p = 0.725) at 4 weeks after the completion of 3-week treatment.
Discussion
In this exploratory analysis of data from a randomized, placebo-controlled trial [22], a significantly higher exercise capacity during CPET was achieved after PR in combination with ghrelin administration, but no significant prolongation of endurance time for exercise or improvement of dyspnea, assessed on the Borg scale, was observed. However, this study showed that the relative location of the dyspnea break-point shifted significantly to an earlier phase of exercise during a standardized exercise program after ghrelin administration.
We have previously shown that:
the dyspnea break-point during exercise occurred similarly among COPD patients at the anaerobic threshold (AT) point, and
the dyspnea break point during exercise occurred in a later exercise phase among COPD patients than among controls [10, 12].
The AT, in other words the lactate threshold, reflects a sustainable and is an objective measure of cardiopulmonary exercise capacity. AT is likely to change significantly with changes in the extent of cardiopulmonary dysfunction [23]. AT becomes progressively larger as the severity of cardiopulmonary dysfunction decreases, but the ratio of at the AT to peak becomes smaller [24, 25]. In this study:
at pre-treatment, the dyspnea break-point also occurred at a similar point to the lactate threshold point, which, in turn, was located in a later exercise phase; and
when treated with ghrelin, the percentage of at the dyspnea break-point to Δ became smaller compared with placebo, but the absolute value of at the dyspnea break-point was unchanged.
The relative change of the dyspnea break-point to an early exercise phase after treatment by ghrelin was associated with an increase in peak rather than a change in resting . This suggests that the relative change of the dyspnea break-point was more strongly associated with improvement in exercise capacity caused by ghrelin treatment, although the percentage of at the dyspnea break-point is calculated using the both values of resting and peak . In general, above the AT point, exertional acidosis develops in COPD patients, which in turn is not compensated by their ventilatory ability to stop exercise immediately [3, 12, 26]. Given the relationship between the change of the dyspnea break-point and the development of acidosis at peak exercise in this study, these findings suggest that after COPD patients treated with ghrelin reached the dyspnea break-point, they had more ability to increase exercise capacity or by using their improved cardiopulmonary function [21], even if severe exertional acidosis was present at peak exercise. As a result, as shown in this study, the exertional dyspnea pattern during a standardized exercise program may be changed. We believe that the cardiopulmonary improvements obtained by ghrelin administration may result in a clinically significant change in the exertional dyspnea pattern, and patients treated with ghrelin may then be able to exercise more rapidly.
This study has some limitations. First, given the exploratory nature of the study, these findings should be regarded as preliminary, Furthermore, although the drug regimen of enrolled patients was not changed within 4 weeks before participation or during the study, and the treatment strategies in the two groups were not significantly different (Table 1), the differences between bronchodilator therapy at baseline were large. In addition, the enrolled patients treated with ghrelin had slightly poorer cardiopulmonary function at baseline. The results obtained in this study might be affected by these biases and must be confirmed in future studies. Second, of 20 patients who completed the substudy, only 16 could be analyzed for break-point evaluations. The number of evaluated participants was small. In addition, it would be important to confirm whether the findings obtained in this study are valid for the whole range of COPD patients. Third, in this study, at week 7, i.e., 4 weeks after completion of the intervention, the sustained effects on the exertional dyspnea pattern of ghrelin treatment should have been evaluated, as in the multicenter trial [20]. Fourth, weight loss is an important risk factor for COPD patients. In this study, the effect of ghrelin on weight was not determined. When the ghrelin and placebo groups were combined in one group, the relative decrease in weight after the 3-week treatment, including the PR program (mean change from pre-treatment (SD), −0.1 (0.9) kg) was followed by an increase 4 weeks after completion of the 3-week treatment (mean change from 3-week treatment (SD), +0.6 (1.1) kg). In this analysis, no such effect of PR was observed in the placebo group. On the basis of the condition of each patient, an appropriate PR program should have been conducted, to checking what intensity and which frequencies are effective. We also need to study which other suitable treatments, for example nutrition therapy are effective in conjunction with ghrelin.
In conclusion, although these findings might be regarded as preliminary and should be confirmed by larger-scale studies, the results of this exploratory analysis revealed that underweight patients with COPD gained a clinically significant benefit from ghrelin treatment with regard to changes in the pattern of exertional dyspnea during a standardized exercise program.
Author Contributions
All the authors participated in the study design, data review, data interpretation, and writing of the report. KM wrote the first draft of the report, and the final version was produced in collaboration with all the authors. All the authors saw and approved the final version of the report. Funders had no role in study design, in data collection and analysis, or in preparation of the report.
Acknowledgments
Funding was received as Research Grants from: the Ministry of Health, Labour and Welfare in Japan; the Program for Promotion of Fundamental Studies in Health Sciences of the National Institute of Biomedical Innovation (NIBIO) of Japan; the Takeda Scientific Foundation in Japan; and Health and Labour Sciences Research Grants, Clinical Research, H20-translational research-general-002. The authors would like to thank Mr K. Tsuguchi (Nihon Ultmarc Inc., Tokyo, Japan) for performing the statistical analysis, Ms Y. Tsuchie (Toneyama National Hospital) for her assistance with this study, and Mr T. Uenishi (Toneyama National Hospital) for obtaining the CPET measurements. They authors would also like to thank the members of the main study that included this substudy at Miyazaki University School of Medicine (Professor M. Nakazato, Dr N. Matsumoto, and Dr Y. Arimura), Nara Medical University (Professor H. Kimura and Dr M. Yoshikawa), and the National Cardiovascular Center Research Institute (Dr K. Yamahara).
Conflict of interest
No conflicts of interest, financial or otherwise are declared by the authors.
Footnotes
Trial Registration
UMIN (University Hospital Medical Information Network in Japan: https://upload.umin.ac.jp/cgi-open-bin/ctr/ctr.cgi?function=brows&action=brows&type=summary&recptno=R000000103&language=E), number C000000061.
References
- 1.ATS Dyspnea. Mechanisms, assessment, and management: a consensus statement. American Thoracic Society. Am J Respir Crit Care Med. 1999;159:321–340. doi: 10.1164/ajrccm.159.1.ats898. [DOI] [PubMed] [Google Scholar]
- 2.Burki NK, Lee LY. Mechanisms of dyspnea. Chest. 2010;138:1196–1201. doi: 10.1378/chest.10-0534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.O’Donnell DE, Ora J, Webb KA, Laveneziana P, Jensen D. Mechanisms of activity-related dyspnea in pulmonary diseases. Respir Physiol Neurobiol. 2009;167:116–132. doi: 10.1016/j.resp.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 4.Gagnon P, Bussieres JS, Ribeiro F, Gagnon SL, Saey D, Gagne N, Provencher S, Maltais F. Influences of spinal anesthesia on exercise tolerance in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:606–615. doi: 10.1164/rccm.201203-0404OC. [DOI] [PubMed] [Google Scholar]
- 5.Landbo C, Prescott E, Lange P, Vestbo J, Almdal TP. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160:1856–1861. doi: 10.1164/ajrccm.160.6.9902115. [DOI] [PubMed] [Google Scholar]
- 6.Wagner PD. Possible mechanisms underlying the development of cachexia in COPD. Eur Respir J. 2008;31:492–501. doi: 10.1183/09031936.00074807. [DOI] [PubMed] [Google Scholar]
- 7.Laveneziana P, Guenette JA, Webb KA, O’Donnell DE. New physiological insights into dyspnea and exercise intolerance in chronic obstructive pulmonary disease patients. Expert Rev Respir Med. 2012;6:651–662. doi: 10.1586/ers.12.70. [DOI] [PubMed] [Google Scholar]
- 8.O’Donnell DE, Bertley JC, Chau LK, Webb KA. Qualitative aspects of exertional breathlessness in chronic airflow limitation: pathophysiologic mechanisms. Am J Respir Crit Care Med. 1997;155:109–115. doi: 10.1164/ajrccm.155.1.9001298. [DOI] [PubMed] [Google Scholar]
- 9.O’Donnell DE, D’Arsigny C, Fitzpatrick M, Webb KA. Exercise hypercapnia in advanced chronic obstructive pulmonary disease: the role of lung hyperinflation. Am J Respir Crit Care Med. 2002;166:663–668. doi: 10.1164/rccm.2201003. [DOI] [PubMed] [Google Scholar]
- 10.Miki K, Maekura R, Hiraga T, Hashimoto H, Kitada S, Miki M, Yoshimura K, Tateishi Y, Fushitani K, Motone M. Acidosis and raised norepinephrine levels are associated with exercise dyspnoea in idiopathic pulmonary fibrosis. Respirology. 2009;14:1020–1026. doi: 10.1111/j.1440-1843.2009.01607.x. [DOI] [PubMed] [Google Scholar]
- 11.Miki K, Maekura R, Hiraga T, Hashimoto H, Kitada S, Miki M, Yoshimura K, Tateishi Y, Sugano T, Motone M. Exertional dyspnea-related acidotic and sympathetic responses in patients with sequelae of pulmonary tuberculosis. J Physiol Sci. 2010;60:187–193. doi: 10.1007/s12576-009-0083-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Miki K, Maekura R, Hiraga T, Kitada S, Miki M, Yoshimura K, Tateishi Y. Effects of oxygen on exertional dyspnoea and exercise performance in patients with chronic obstructive pulmonary disease. Respirology. 2012;17:149–154. doi: 10.1111/j.1440-1843.2011.02086.x. [DOI] [PubMed] [Google Scholar]
- 13.Miki K, Maekura R, Miki M, Kitada S, Yoshimura K, Tateishi Y, Mori M. Exertional acidotic responses in idiopathic pulmonary fibrosis: the mechanisms of exertional dyspnea. Respir Physiol Neurobiol. 2013;185:653–658. doi: 10.1016/j.resp.2012.11.008. [DOI] [PubMed] [Google Scholar]
- 14.Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402:656–660. doi: 10.1038/45230. [DOI] [PubMed] [Google Scholar]
- 15.Matsumura K, Tsuchihashi T, Fujii K, Abe I, Iida M. Central ghrelin modulates sympathetic activity in conscious rabbits. Hypertension. 2002;40:694–699. doi: 10.1161/01.HYP.0000035395.51441.10. [DOI] [PubMed] [Google Scholar]
- 16.Nagaya N, Kojima M, Uematsu M, Yamagishi M, Hosoda H, Oya H, Hayashi Y, Kangawa K. Hemodynamic and hormonal effects of human ghrelin in healthy volunteers. Am J Physiol Regul Integr Comp Physiol. 2001;280:R1483–R1487. doi: 10.1152/ajpregu.2001.280.5.R1483. [DOI] [PubMed] [Google Scholar]
- 17.Nakazato M, Murakami N, Date Y, Kojima M, Matsuo H, Kangawa K, Matsukura S. A role for ghrelin in the central regulation of feeding. Nature. 2001;409:194–198. doi: 10.1038/35051587. [DOI] [PubMed] [Google Scholar]
- 18.Tschop M, Smiley DL, Heiman ML. Ghrelin induces adiposity in rodents. Nature. 2000;407:908–913. doi: 10.1038/35038090. [DOI] [PubMed] [Google Scholar]
- 19.Nagaya N, Itoh T, Murakami S, Oya H, Uematsu M, Miyatake K, Kangawa K. Treatment of cachexia with ghrelin in patients with COPD. Chest. 2005;128:1187–1193. doi: 10.1378/chest.128.3.1187. [DOI] [PubMed] [Google Scholar]
- 20.Miki K, Maekura R, Nagaya N, Nakazato M, Kimura H, Murakami S, Ohnishi S, Hiraga T, Miki M, Kitada S, Yoshimura K, Tateishi Y, Arimura Y, Matsumoto N, Yoshikawa M, Yamahara K, Kangawa K. Ghrelin treatment of cachectic patients with chronic obstructive pulmonary disease: a multicenter, randomized, double-blind, placebo-controlled trial. PLoS ONE. 2012;7:e35708. doi: 10.1371/journal.pone.0035708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Miki K, Maekura R, Nagaya N, Kitada S, Miki M, Yoshimura K, Tateishi Y, Motone M, Hiraga T, Mori M, Kangawa K. Effects of Ghrelin Treatment on Exercise Capacity in Underweight COPD Patients: a substudy of a multicenter, randomized, double-blind, placebo-controlled trial of ghrelin treatment. BMC Pulm Med. 2013;13:37. doi: 10.1186/1471-2466-13-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Miki K, Maekura R, Nagaya N, Kitada S, Miki M, Yoshimura K, Matsui H, Satomi A, Hashimoto H, Mori M, Kangawa K. Effects of ghrelin on the dyspnea pattern in cachectic COPD: Exploratory analysis of a substudy of a multicenter, randomized, double-blind, placebo-controlled trial of ghrelin treatment. Eur Respir J. 2013;42(57 suppl.):517s. [Google Scholar]
- 23.Itoh H, Taniguchi K, Koike A, Doi M. Evaluation of severity of heart failure using ventilatory gas analysis. Circulation. 1990;81:II31–II37. [PubMed] [Google Scholar]
- 24.Kinugawa T, Ogino K, Noguchi N, Mori M, Miyakoda H, Hisatome I, Shigemasa C. Sympathetic nervous response relative to the adenosine triphosphate supply-demand imbalance during exercise is augmented in patients with heart failure. Chest. 1998;114:1295–1300. doi: 10.1378/chest.114.5.1295. [DOI] [PubMed] [Google Scholar]
- 25.Stringer WW, Hansen JE, Wasserman K. Cardiac output estimated noninvasively from oxygen uptake during exercise. J Appl Physiol. 1997;82:908–912. doi: 10.1152/jappl.1997.82.3.908. [DOI] [PubMed] [Google Scholar]
- 26.Wasserman K, Cox TA, Sietsema KE. Ventilatory regulation of arterial H(+) (pH) during exercise. Respir Physiol Neurobiol. 2014;190:142–148. doi: 10.1016/j.resp.2013.10.009. [DOI] [PubMed] [Google Scholar]