

Sir,
Granuloma annulare (GA) is a benign, self-limiting disorder that is characterised by small papules with an annular distribution. Generalised GA (GGA) occurs in about 15% of GA cases and affects the trunk and extremities. It consists of multiple papules with or without an annular arrangement. It is more often associated with systemic disorders (e.g., diabetes mellitus, malignant conditions, and autoimmune thyroiditis) than localised GA.[1,2]
According to Lamm et al.,[3]3% of patients treated with intravesical BCG instillation experience skin rashes. However, there are few case reports of granulomatous reactions, including granulomatous hepatitis and nephritis.[4] We are aware of only one other report of generalised cutaneous granulomatous lesions after intravesical BCG instillation.[5]
Here, we describe a case of GGA induced by intravesical BCG immunotherapy.
A 71-year-old male with bladder cancer was referred to our dermatology department. He presented with a skin rash on the posterior neck and trunk that had appeared one week after his first round of intravesical bacillus Calmette–Guerin (BCG) immunotherapy. He had no complaints of itching or burning sensation. After the transurethral resection of a bladder tumor, he had been receiving additional intravesical BCG immunotherapy as a maintenance treatment every week.
Physical examination found multiple brownish-red papules and slightly elevated plaques of 5-20 mm in diameter on the posterior neck and the torso. Some of the papules were integrated and spread with central hyperpigmentation [Figure 1a and b]. Lab exams, including for angiotensin-converting enzyme, revealed no specific findings. Acid-fast smear, acid-fast bacteria culture, interferon-gamma release assay, and polymerase chain reaction for acid-fast bacteria were all negative. CT scans showed no specific findings. A skin biopsy from the papules revealed epithelioid granulomas consisting of multinucleated giant cells. No caseating necrosis was evident [Figure 1c and d].
Figure 1.
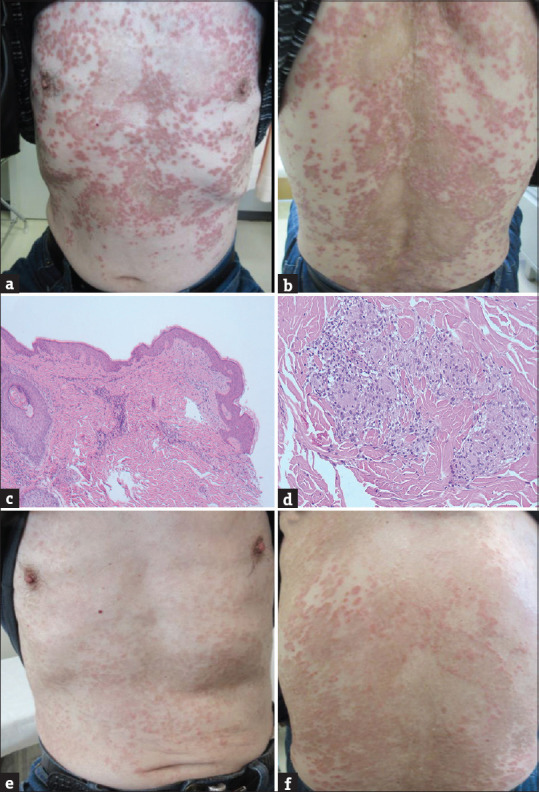
The clinical and histological findings. (a and b) The first visit. Multiple brownish-red papules and slightly elevated plaques are observed on the posterior neck and both sides of the torso. Some of the papules are integrated and confluent. (c and d) Histopathology shows epithelioid granulomas consisting of multinucleated giant cells. Lymphocytic infiltration and interstitial mucin deposition are sparse. There is no finding of caseating necrosis. (hematoxylin and eosin, (c) ×40, (d) ×200). (e and f) The lesion has improved considerably at the completion of intravesical BCG and topical corticosteroids. Because it was challenging for the patient to apply topical corticosteroids sufficiently on the dorsal torso, the improvement is more evident on the ventral side
From the histopathological findings, we suspected interstitial GA. Based on the clinical progress and histopathological findings, we diagnosed GGA induced by intravesical BCG immunotherapy. Strongly suspecting GGA, we started topical corticosteroids. Because it was challenging for the patient to apply topical corticosteroids sufficiently to the dorsal torso, the cutaneous lesions’ improvement was more evident on the ventral side [Figure 1e and f].
A search of PUBMED found nine reports of BCG vaccination-induced GGA from 2001 to 2014, but intravesical BCG immunotherapy-induced GGA had never been reported. In our case, the patient had a medical history of bladder cancer and diabetes mellitus, so it was challenging to exclude cancer- and diabetes-related GGA. However, the cutaneous lesions appeared after the induction of intravesical BCG immunotherapy, so we diagnosed intravesical BCG-induced GGA. In almost all cases of BCG vaccination-induced GGA, the skin lesions improve within one month. Drug-induced GA often regresses spontaneously with discontinuation of the culprit drug; in our case, we chose a topical corticosteroid as a treatment, and the cutaneous lesions visibly improved [Figure 1e and f].
We report a case of GGA induced by intravesical BCG immunotherapy. Although such cases are quite rare, we should consider the possibility of GA when we encounter newly appearing skin eruptions after the introduction of intravesical BCG immunotherapy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kakurai M, Kiyosawa T, Ohtsuki M, Nakagawa H. Multiple lesions of granuloma annulare following BCG vaccination: Case report and literature review. Int J Dermatol. 2001;40:579–81. doi: 10.1046/j.1365-4362.2001.01248-2.x. [DOI] [PubMed] [Google Scholar]
- 2.Nagase K, Koba S, Okawa T, Inoue T, Misago N, Narisawa Y. Generalized granuloma annulare following BCG vaccination, mimicking papular tuberculid. Eur J Dermatol. 2011;21:1001–2. doi: 10.1684/ejd.2011.1512. [DOI] [PubMed] [Google Scholar]
- 3.Lamm DL, van der Meijden PM, Morales A, Brosman SA, Catalona WJ, Herr HW, et al. Incidence and treatment of complications of bacillus Calmette-Guerin intravesical therapy in superficial bladder cancer. J Urol. 1992;147:596–600. doi: 10.1016/s0022-5347(17)37316-0. [DOI] [PubMed] [Google Scholar]
- 4.Green DB, Kawashima A, Menias CO, Tanaka T, Redelman-Sidi G, Bhalla S, et al. Complications of intravesical BCG immunotherapy for bladder cancer. Radiographics. 2019;39:80–94. doi: 10.1148/rg.2019180014. [DOI] [PubMed] [Google Scholar]
- 5.Mahmood F, Elahe S, Leila M. Cutaneous granulomatous reaction post intravesical BCG installation: A case report. Iran J Dermatol. 2012;15:95–8. [Google Scholar]