

A 47-year-old man was transferred to our hospital with methicillin-resistant Staphylococcus aureus (MRSA) bacteremia. On admission, the patient had multiple 1–3-cm-sized black dotlike erythematous lesions throughout the body (Figure 1A). In addition, he had multiple patchy consolidations in both lung fields (Figure 1B) and multifocal dots scattered in both fronto-parieto-temporal lobes (Figure 1C). On the 2nd day of admission, transthoracic echocardiography revealed a 2.25×1.5-cm-sized friable mass in the tricuspid septal leaflet (Figure 1D, Supplementary Videos 1 and 2). MRSA was isolated from the patient’s blood and skin lesions. Unexpectedly, no intracardiac shunt was shown on transthoracic and transesophageal echocardiography. Tricuspid septal leaflet repair and mass debridement had been performed in the referring hospital. MRSA was isolated from the debrided mass from the tricuspid valve.
Figure 1.
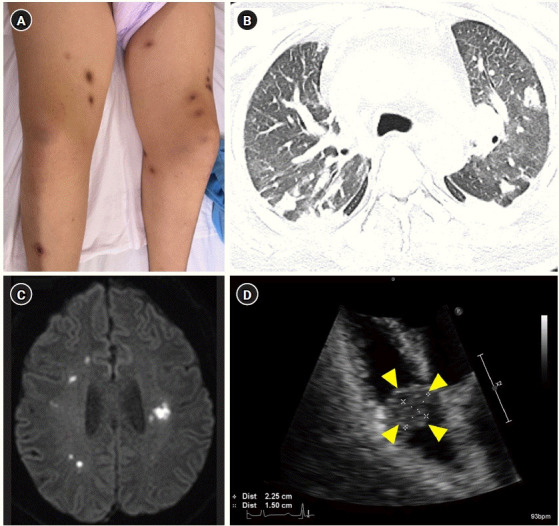
(A) Multiple dot-like black erythematous lesions measuring 1–3 cm throughout the body. (B) Chest computed tomography revealing multiple nodules in both lungs. (C) Diffusion-weighted brain magnetic resonance imaging of lesions with high signal intensity, appearing as multiple scattered dots, in both fronto-parieto-temporal lobes. (D) Apical view of the four chambers on transthoracic echocardiography showing vegetation in the tricuspid valve indicated by yellow arrowheads.
In this case, atypical features were noted. Infective endocarditis occurred on a normal tricuspid valve, and a large vegetation was present, caused by MRSA. He also exhibited clinical signs of systemic embolization, despite the absence of congenital heart disease, central venous catheter use, and drug use, making this case particularly unique and challenging to diagnose and treat [1,2].
Acknowledgments
This study was approved by the Institutional Review Board at Jeju National University Hospital (No. 2023-07-006). The patient provided informed consent for publication of the report.
Footnotes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: JRY. Data curation: JRY, KYB. Formal analysis: JRY. Methodology: JRY, MK. Project administration: JRY. Visualization: JRY. Writing–original draft: MK. Writing–review & editing: JRY.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.4266/acc.2023.01228.
Transthoracic echocardiogram, apical four-chamber view. A 47-year-old man without prior cardiac abnormalities was admitted with multiple septic embolic lesions and methicillin-resistant Staphylococcus aureus bacteremia. A transthoracic echocardiogram demonstrated a tricuspid septal leaflet with a 2.25×1.5-cm-sized friable vegetative lesion.
Transthoracic echocardiogram, paralong axis view.
REFERENCES
- 1.Shmueli H, Thomas F, Flint N, Setia G, Janjic A, Siegel RJ. Right-sided infective endocarditis 2020: challenges and updates in diagnosis and treatment. J Am Heart Assoc. 2020;9:e017293. doi: 10.1161/JAHA.120.017293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. ESC Scientific Document Group 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur Heart J. 2015;36:3075–128. doi: 10.1093/eurheartj/ehv319. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Transthoracic echocardiogram, apical four-chamber view. A 47-year-old man without prior cardiac abnormalities was admitted with multiple septic embolic lesions and methicillin-resistant Staphylococcus aureus bacteremia. A transthoracic echocardiogram demonstrated a tricuspid septal leaflet with a 2.25×1.5-cm-sized friable vegetative lesion.
Transthoracic echocardiogram, paralong axis view.