

Abstract
Attachment styles may influence interpersonal strategies used to cope with stress. We examined links between attachment style, communicative behaviors, and physical well-being among 166 couples coping with cancer. Results of actor-partner interdependence mediation models indicated that insecure attachment styles were associated with greater self-report of two different and seemingly contradictory communicative behaviors (disclosure and holding back), which in turn were associated with poorer physical well-being. These effects were intrapersonal for both patients and spouses, with the exception of anxious attachment and holding back for spouses. They were also interpersonal in that spouse insecure attachment was associated with poorer patient physical well-being through spouse communication (greater holding back and disclosure). Couple-based communication interventions to support adjustment should consider attachment style.
Keywords: actor–partner interdependence model, attachment, couple’s communication, dyadic coping, physical health
A couple’s ability to cope with the medical and psychosocial challenges of cancer is often linked to perceptions of partner availability and responsiveness (Regan et al., 2015; Traa, De Vries, Bodenmann, & Den Oudsten, 2015; Tsilika, Parpa, Zygogianni, Kouloulias, & Mystakidou, 2015). In the context of couples coping with cancer, several constructs are valuable including attachment, as conceptualized by closeness, intimacy, anxiety or avoidance, and communication conceptualized by disclosure or holding back. These constructs are important to outcomes for both patients and partners, with consequences for physical and mental health. In particular, the extent to which a partner is emotionally available and supportive is highly influenced by her or his attachment style. Conceptualized from Bowlby’s (1969/1982, 1988) attachment theory, attachment style refers to individual differences in seeking closeness to significant others to regulate affect during times of significant psychological need or duress (Bowlby, 1969/1982; Mikulincer & Shaver, 2003; 2016; 2019).
In adult romantic relationships, attachment styles are commonly measured along dimensions of attachment anxiety and avoidance. Individuals with an anxious attachment style tend to be emotionally preoccupied with closeness and engage in excessive expression of concerns, often worrying that their partners will not be sufficiently responsive to their needs (Mikulincer & Shaver, 2019). Individuals with an avoidant attachment style are uncomfortable with intimacy and emotional closeness, avoid asking for help, and are less available to provide effective and sensitive support (Mikulincer & Shaver, 2019). Both anxious and avoidant attachment reflect types of attachment insecurity. By contrast, individuals who are securely attached (low on both dimensions of anxiety and avoidance) are comfortable with intimacy and appropriately seek closeness.
In the last two decades, there has been increased research on the impact of adult attachment styles on health outcomes. Studies have found that couples’ attachment styles are associated with relationship behavior and overall health, including health protective or health damaging behaviors (Feeney, 2000; Pietromonaco, DeVito, Ge, & Lembke, 2015; Pietromonaco, Uchino, & Dunkel- Schetter, 2013). Attachment anxiety and avoidance have been linked with health outcomes such as inflammation and cardiovascular disease as evidenced by changes in cortisol patterns, cardiovascular reactivity, and immune responses (Ehrlich, 2019; Pietromonaco et al., 2013; Pietromonaco & Powers, 2015; Slatcher, & Schoebi, 2017). Attachment styles are thought to influence health outcomes through their shaping of the interpersonal strategies that people use to cope with stress. In turn, these strategies influence relationship behaviors (e.g., provision of support, engaging in joint problem solving) that consequently affect health-related responses and behaviors. These behaviors may serve as important mechanisms in the association between attachment and physical health.
Couples Attachment, Cancer, and Health
Research on attachment among adults coping with serious illness such as cancer has focused on both psychological and symptom burden outcomes. A cancer diagnosis represents a salient threat that triggers attachment behaviors in both patients (due to illness) and their spouses (who may fear losing their partner) (Porter et al., 2012). Several studies have found associations between attachment and outcomes in patients with cancer and their caregiving partners/spouses. For example, among patients with early stage lung cancer and their spouses, avoidant attachment in partners/spouses was associated with poorer functional well-being and increased pain in patients (Porter, Keefe, Davis, et al., 2012). For couples in which both partners reported secure attachment, better adjustment was reported in domains of marital quality, pain, and mood for the patient, and marital quality and mood for the partner/spouse. Similar evidence has been found in the attachment styles of end-stage cancer patients and partner/spousal caregivers. Specifically, patients reported a greater number of cancer symptoms when partners/spouses reported low levels of intimacy and closeness (i.e., analogous to attachment anxiety) (Milbury, Yang, Liao, Tsao, & Bruera, 2018). Patients high in attachment avoidance reported greater symptom burden (e.g., pain, fatigue, nausea, shortness of breath) when their partners/spouses also reported high levels of avoidance (Milbury et al., 2018).
In the context of couples coping with cancer, attachment anxiety and avoidance has also been associated with poorer partner-patient interactions. For example, partners/spouses with either an anxious or avoidant attachment style tended to engage in more compulsive or controlling caregiving behaviors (e.g., were over-involved or overprotective), were more critical of the patient (e.g., minimizing patient symptoms or chastising their efforts for self-care), and provided support that was more self-focused than sensitive to the patient’s needs (Braun et al., 2012). Partners/spouses caring for anxious or avoidantly attached patients often dealt with rejection of the care they offered or had to deal with an overly dependent patient who was dissatisfied with the care received (Braun et al., 2012).
Not only do attachment anxiety and attachment avoidance strongly influence maladaptive patterns of interactions and behaviors that worsen couples’ distress, these interactions can have downstream effects on their physical health (e.g., poor quality of life, lower levels of vitality, chronic pain, and inflammatory bowel disease; De Luca, Dorangricchia, Salerno, Coco, & Cicero, 2017; Pietromonaco & Beck 2019). Despite growing evidence linking attachment and physical well-being (PWB) in couples coping with cancer, the mechanisms by which this association exists are not well-understood and remain a key gap in the attachment and cancer literature. We posit that couple’s communication behaviors, including the degree to which they disclose and hold back from disclosing illness-related concerns, is one such mechanism.
Couple’s Communication in Cancer
Couples may co-regulate their emotions through how and what they communicate to each other, which in turn can influence their physical health (Manne, Ostroff, Winkel, Grana, & Fox, 2005; Manne, Taylor, Dougherty, & Kemeny, 1997). Open communication (e.g., having direct communication, sharing and expressing thoughts and feelings) between patients and their spouses/partners has been shown to buffer the effects of cancer-related stress, influence positive health behaviors (e.g., health check-ups, exercise, diet) and improve marital satisfaction and dyadic coping (Badr & Krebs, 2013; Traa et al., 2015). Conversely, difficulty in communicating about illness-related issues can compromise a couple’s psychological adjustment to cancer and deny both the spouse/partner and patient the ability to provide and receive much needed emotional support. What has not been examined to the same extent is under what conditions direct communication of thoughts and feelings may be more or less helpful or even adaptive for couples.
Undoubtedly, cancer-related discussions can be difficult and can feel threatening and overwhelming. Evidence supports that couples’ open discussion and disclosure of their worries, decisions about cancer treatment, and plans for the future can yield better adaptation to cancer for both the patient and spouse/partner (Manne et al., 2004; Porter, Keefe, Hurwitz, & Faber, 2005). However, cancer patients and their spouses/partners sometimes feel constrained in sharing their concerns, and thus opt to conceal distressing and negative thoughts and feelings that are either directly or indirectly related to their cancer experience. Couples’ tendencies to disclose or conceal thoughts and emotions about cancer has been well-studied in the research literature and greatly expanded our understanding about adaptive and maladaptive communication strategies among patients and spouses/partners in cancer.
Disclosure Dimensions
Disclosure has been operationalized along two dimensions: the extent to which people share and express their emotions and thoughts (emotional disclosure), and the extent to which people hold back from disclosing their thoughts and feelings with each other (holding back). Emotional disclosure is defined as the ability to openly discuss and share information, thoughts, and feelings that are both personal and considered emotionally relevant. In the context of cancer, emotional disclosure may help couples have a clearer understanding about each other’s needs that can improve the quality of support given and received. Moreover, emotional disclosure can enhance couples’ ability to have a ‘shared-experience’ that can increase their sense of closeness and thereby facilitate both individual and relationship adjustment.
Holding back has often been conceptualized as a maladaptive communication behavior, similar to other related constructs such as protective buffering; both have been associated with greater psychological distress and poorer relationship functioning (Langer, Brown, & Syrjala, 2009; Manne et al., 2007, 2010, 2014, 2015; Porter et al., 2005a). Engaging in holding back behaviors compromises how couples cope with cancer as it impedes patients’ and partners’ ability to share their needs to feel supported. Holding back can also make couples feel inauthentic to who they are as individuals and as a couple as they are actively inhibiting how they really feel and think about the cancer experience. Reasons for doing so can be either egoistic (to protect oneself from feeling badly) or prosocial (to protect one’s partner from feeling badly), though prosocial motivations may be stronger, especially among caregivers (Langer et al., 2009). Couples might also hold back feelings and concerns to maintain marital satisfaction, to improve perceptions of closeness, commitment to one another and enhance coordination of cancer care (Badr, 2017). Given the importance of both disclosure and holding back as dimensions of communication in relation to how couples adjust to cancer, we examined their roles as potential mechanisms through which attachment may influence physical health outcomes.
Attachment, Physical Health, and the Mediating Link of Disclosure Dimensions in Couple’s Communication
Researchers suggest that more complex models and testing of mechanisms may be needed when evaluating the links between attachment and physical health (Pietromonaco et al., 2013; Pietromonaco et al., 2015; Pietromonaco & Beck, 2019). We propose that communicative behaviors mediate this link.
Attachment, Disclosure and Holding Back
Attachment theory supports the relevance of attachment principles to patterns of disclosure in couple relationships. As an example, persons who are low in anxiety and low in avoidance (i.e., secure attachment style) view intimate relationships as rewarding and are thus likely to feel comfortable with disclosing their feelings, reflecting comfort with being close and interdependence.
By contrast, those who are avoidantly attached view personal relationships as unrewarding or threatening and thus may maintain interpersonal distance by limiting their discussions about cancer (e.g., holding back). Avoidant individuals may also find it difficult to get others to “open up,” including their partner. Individuals who are anxiously attached may engage in excessive self-disclosure to seek reassurance and feel close to their partner and maintain intimacy.
Few studies have directly examined associations between attachment and disclosure. Of those available, findings indicate that both secure and anxiously attached individuals show greater disclosure compared to those who are avoidantly attached (Mikulincer & Nachshon, 1991). Other studies have shown that anxiously attached individuals tend to score high in disclosure and avoidant individuals tend to score low on measures of disclosure (e.g., Bradford, Feeney & Campbell, 2002; Pietromonaco & Barrett, 1997).
Disclosure, Holding Back, and Physical Well-Being
The theory behind the positive health effects of disclosure asserts that sharing one’s feelings and emotions can create or strengthen relationships, reduce guilt or shame about personal experiences (Murray-Swank, McConnell, & Pargament, 2007), and provide cathartic experiences that in turn reduces distress. Furthermore, it is believed that disclosing thoughts and feelings provides an opportunity for individuals to cognitively process their experiences which may promote healthy perceptions, beliefs, and health-relevant behaviors that positively impact physical well-being (Pennebaker, Kiecolt-Glaser, & Glaser, 1988).
Evidence regarding the impact of disclosure on health comes from studies of written disclosure interventions in which participants write privately about their thoughts and feelings surrounding a stressful or traumatic event. A meta-analysis examining the effects of written disclosure interventions found evidence for positive health effects including (Frisina, Borod, & Lepore, 2004) lower healthcare utilization and improved pain among cancer populations. For example, Stanton and colleagues (2002) found that patients with breast cancer who were randomly assigned to a disclosure condition reported fewer negative physical symptoms and fewer medical appointments after three months as compared to a non-disclosure group.
In a nonintervention study (Porter, Keefe, Lipkus, & Hurwitz, 2005b), ambivalence over emotional expression in patients with gastrointestinal cancer, and their caregivers resulted in greater patient pain and poorer quality of life. In particular, patients who reported being more ambivalent about expressing their emotions engaged in more catastrophizing and reported higher levels of pain behaviors and poorer quality of life. Patients whose caregivers or spouses were high in ambivalence engaged in more catastrophizing, had higher levels of pain and pain behavior, and reported lower emotional well-being.
Taken together, these findings suggest that attachment anxiety and avoidance may influence the degree to which both patients and partners/spouses disclose or hold back their feelings when coping with cancer, which may in turn influence health outcomes. Thus, it is important to examine both intra- and inter-personal effects for patients and partners. To do so, we used the Actor-Partner Interdependence Model (APIM; see Kenny, Kashy, & Cook, 2006) to test the extent to which (a) attachment characteristics of each relationship partner (patient and partner/spouse) influence their own physical well-being outcomes (actor effects), (b) attachment characteristics of one partner influence the other partner’s physical well-being outcomes (partner effects), and (c) the mediating role of communication behavior in the associations between attachment and one’s own and one’s partner’s physical well-being. To our knowledge, this is the first study to examine the link between attachment and physical well-being and the role of mediators (i.e., communication) in the context of couples coping with cancer.
The current study was designed to examine how associations among attachment, emotional disclosure, holding back interrelate and are associated with physical well-being in patients with cancer and their partners/spouses. We hypothesized that (a) patients and partners/spouses high in anxious and avoidant attachment would report poorer physical well-being; (b) anxious attachment in patients and partners/spouses would be positively associated with emotional disclosure (e.g., as anxiously attached individuals might share more of their concerns to elicit reassurance from their partner), and negatively associated with holding back; (c) avoidant attachment in patients and partners/spouses would be positively associated with holding back, and negatively associated with emotional disclosure; and (d) a person’s communication behavior (i.e., emotional disclosure and holding back) would mediate the effect of his or her own attachment on the physical well-being of his or her partner. To address the last hypothesis, we tested the mediating role of communication in the actor and partner effects of attachment on physical well-being.
Prior work suggests that there may be gender differences in emotional expression in persons coping with cancer, with women being more willing to self-disclose and express emotions than men (Baider & Bengel, 2001; Ussher & Perz, 2010). In addition, there may be dispositional differences in emotional expressivity that influence cancer-related communication behaviors (Manne et al., 2014; Reardon & Buck, 1989). Thus, across our models, we accounted for potential effects of gender and emotional expressivity. In the sections that follow, including all tables, figures, and descriptions of results we refer to all non-patient partners as spouses to avoid confusion with partner effects in the statistical sense.
Methods
Study Design and Participants
Participants were enrolled in a larger observational study examining couple’s communication in cancer (R01CA201179; multiple principal investigators: Langer and Porter). Recruitment took place at the Duke Cancer Institute and the Seattle Cancer Care Alliance (the clinical oncology partnership among the University of Washington, Fred Hutchinson Cancer Research Center, and Seattle Children’s Hospital). The Institutional Review Board (IRB) of Arizona State University served as the IRB of record for the Seattle Cancer Care Alliance, with the appropriate authorization agreements for each partner, and the Duke University IRB provided human subjects oversight for the Duke Cancer Institute. All eligible participants gave written informed consent.
Inclusion criteria for patients were: stage II–IV breast, lung, colon, or rectal cancer; within 2 years of diagnosis of current cancer stage; and currently receiving or having received systemic therapy and/or hormone therapy, with a life expectancy of at least 6 months as determined by their oncologist. Patients also needed to be married or in a committed, cohabiting relationship with someone of the same or opposite sex. Both patients and spouses had to be age 18 or older and able to speak and comprehend English. While only baseline patient-reported outcomes are presented here, the full study included audio-video recording of a discussion between the couple, ecological momentary assessment over two weeks after the laboratory session, and a year of follow-up with four additional assessment time points.
Procedures.
Using an IRB-approved HIPAA waiver, eligible participants were identified via review of oncologists’ clinic appointments (at the Duke Cancer Institute) or a listing of recent patient appointments by cancer diagnosis (at the Seattle Cancer Care Alliance). Research staff screened patient eligibility then asked the patients’ oncologists to approve the approach and sign an introductory letter. Research staff followed up via telephone approximately seven days after the letter was mailed. During this initial telephone contact, the study purpose and procedures were reviewed and both patient and partner participation decisions were ascertained. Couples who agreed to participate scheduled the in-person baseline laboratory session which included study questionnaires completed during the visit on a tablet using REDCap software (Harris et al., 2009; Harris et al., 2019).
Measures
Study coordinators at each site abstracted medical record data including diagnosis stage and receipt of cancer treatment. Patients and spouses independently completed measures of their sociodemographic information, attachment, communication, specifically disclosure and holding back, EE, and PWB.
Attachment.
The 18-item Adult Attachment Scale (Revised; Collins & Read, 1990; 1996) asks participants to rate their feelings about romantic relationships on a 5-point Likert-type scale (“Not at all characteristic of me” to “Very characteristic of me”). For this study, participants were asked to respond to items based on their present romantic relationship with their spouse. In this study we computed scores for two attachment dimensions – attachment anxiety (model of self) and attachment avoidance (model of other). Items such as “I often worry that other people don’t really love me” and “I often worry that other people won’t want to stay with me” assess attachment anxiety. Items such as “I find it difficult to allow myself to depend on others” and “I am uncomfortable when anyone gets too emotionally close to me” assess attachment avoidance. Higher scores are indicative of greater attachment insecurity. Both scales showed good internal consistency in this sample (Cronbach’s α = .90 and .87 for patient and spouse attachment anxiety, respectively; α = .84 and .85 for patient and spouse attachment avoidance, respectively).
Communication.
Disclosure and holding back from disclosure of cancer-related thoughts and feelings were assessed using a modified version of the Emotional Disclosure Scale (Pistrang & Barker, 1995). Prior studies have used this modified version to make it more relevant for cancer populations and have found strong psychometric support for it (Porter et al., 2005a, 2009, 2012). For disclosure, participants are asked to rate the extent to which they talked to their spouse in the past week regarding each of 10 concerns (e.g., physical symptoms, emotional well-being, treatment, financial concerns, and fear or worry about disease progression or death), and in a second pass, the extent to which they held back from talking about these concerns to their spouse. Ratings are made on a 0–5 (not at all to a lot) scale. In this sample, Cronbach’s α was .88 and .86 for disclosure among patients and spouses, respectively; and .90 and .84 among patients and spouses, respectively, for holding back).
Emotional Expressivity.
The 17-item Emotional Expressivity scale (EES; Kring, Smith, & Neale, 1994) was used to assess dispositional emotional expressivity or the extent to which participants outwardly display their emotions. Each item is answered on a 6-point Likert-type ranging from 1 (never true) to 6 (always true). Reliability studies demonstrate the EES to be an internally consistent and a stable individual-difference measure. Sample EES items include “I don’t express my emotions to other people” and “Even when I’m experiencing strong feelings, I don’t express them outwardly.” In this sample, α was .91 (α = .91 for patients, α = .92 for spouses).
Physical well-being.
The seven-item Physical Well Being (PWB) subscale of the functional assessment of cancer therapy scale measure (FACT-GP; Cella et al., 1993) was used to measure participants’ self-reported physical well-being over the past week using a five-point response scale ranging from 0 (“not at all”) to 4 (“very much”). PWB items include “I have a lack of energy,” “Because of my physical condition, I have trouble meeting the needs of my family,” “I feel pain,” and “I feel ill” (reverse-scored). Higher scores indicate better well-being. In this sample, α was .85 (α = .85 for patients, α = .75 for spouses).
Analytic Strategy
Actor-Partner interdependence models.
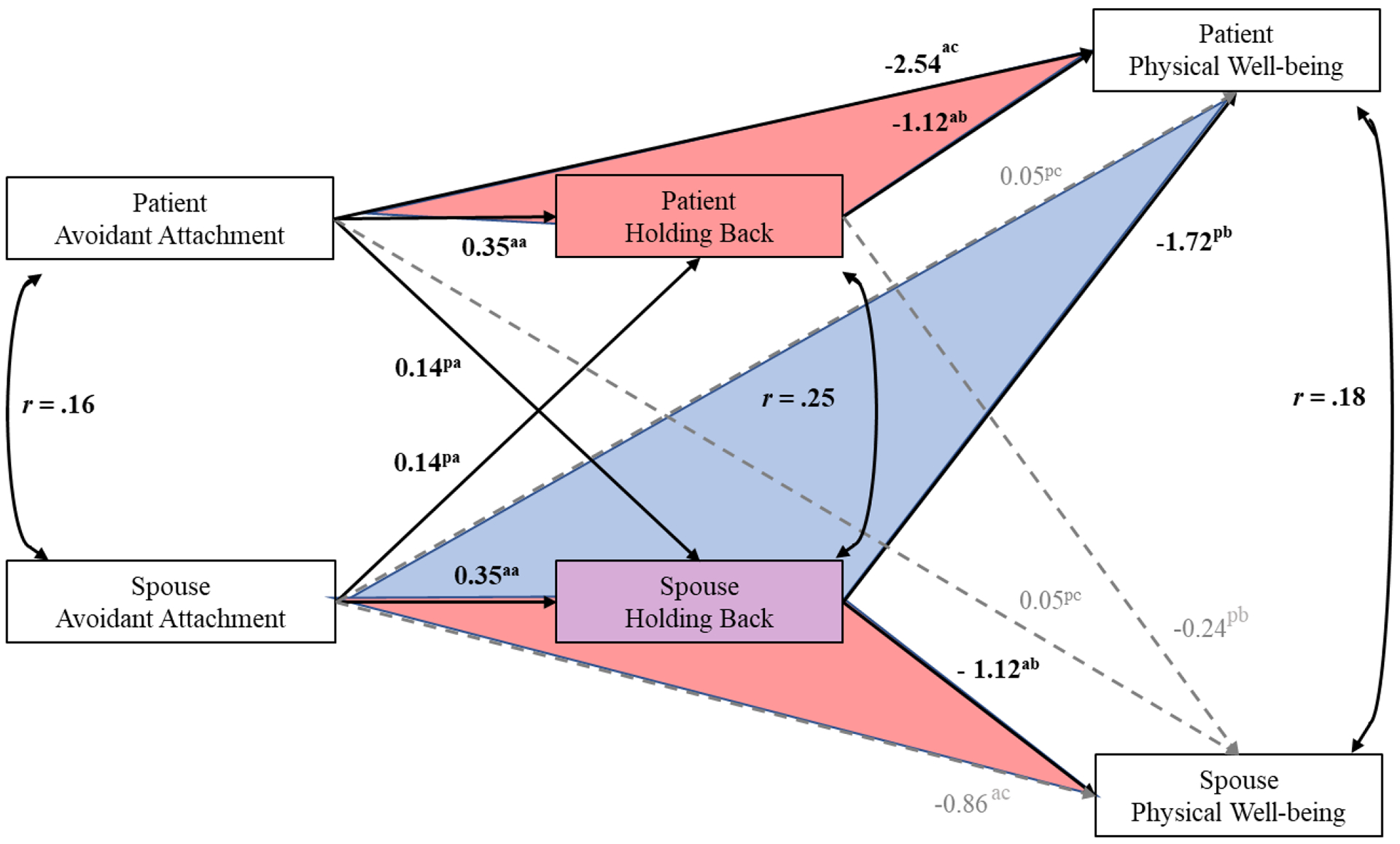
We examined potential indirect associations between a dyad member’s attachment (either anxious or avoidant) and his or her partner’s PWB, as mediated by the dyad member’s own communication behavior (either holding back or disclosing emotions or thoughts) with a separate APIM path analysis for each of the four possible combinations of attachment and communication behavior (see Figure 1 for general structure of APIMs). In each model, associations between attachment and a dyad member’s communication behavior were estimated adjusting for the dyad member’s own gender and EES score; associations with each dyad member’s PWB were estimated adjusting for the dyad member’s own EES score (paths not shown in Figure 1). The unit of analysis in each APIM was the patient-spouse dyad.
Figure 1.
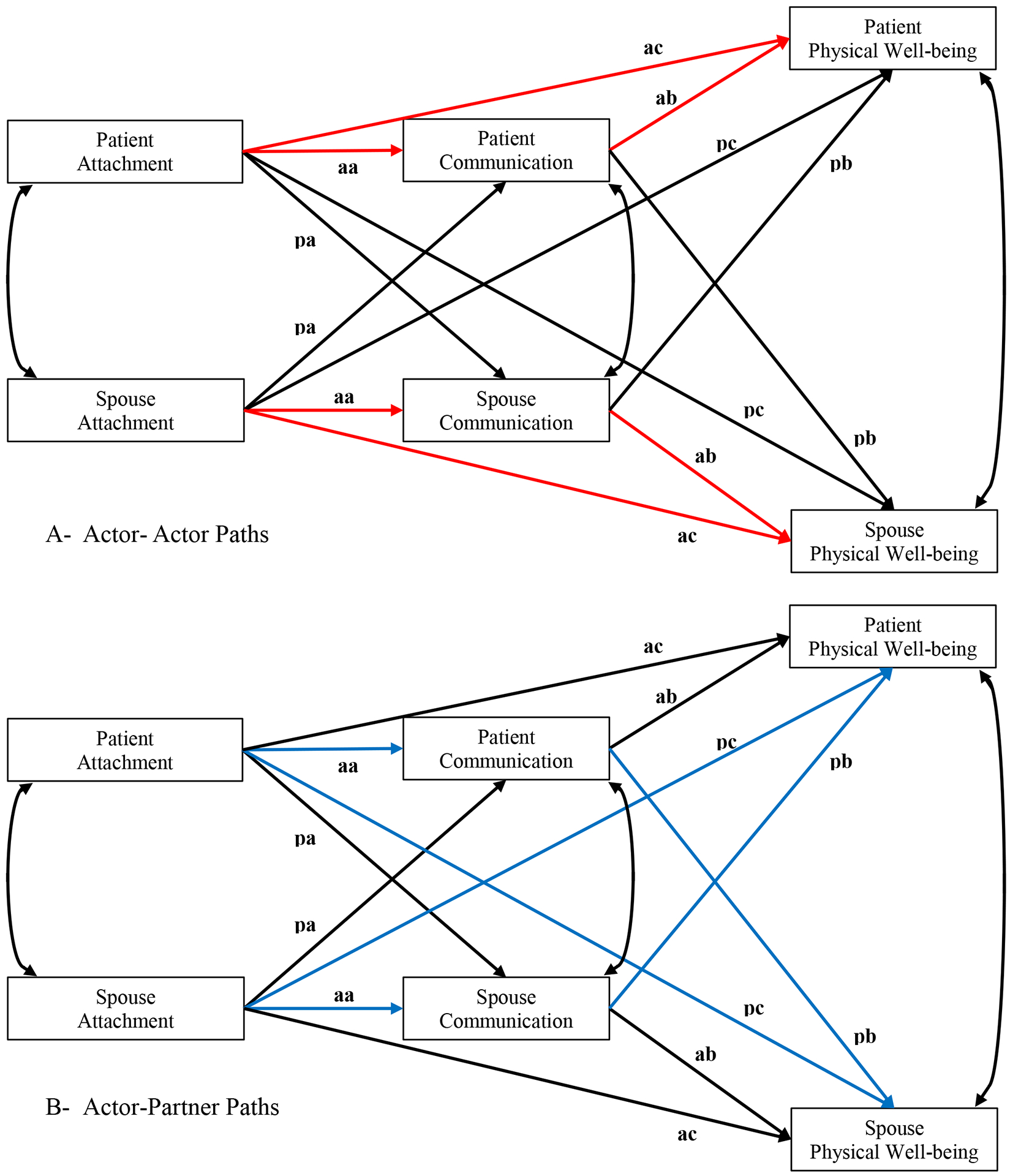
Actor-Partner Interdependence Modeling Path Diagram. In red, A= Actor-Actor Mediation Paths; In blue, B= Actor-Partner Mediation Paths.
First, an APIM with all possible structural, mean, and variance/covariance parameters freely estimated (saturated models) was fit to the data. To arrive at a more parsimonious model, pairwise constraints were specified and tested, one at a time, for pairs of corresponding structural parameters (paths). For example, the first constraint tested was equality of the association between each patient’s attachment measure and his or her own communication behavior (“actor effect” for path a, labeled as “aa” in Figure 1) and the association between the spouse’s attachment measure and his or her own communication behavior (also labeled as “aa” in Figure 1). This constraint was then relaxed and the equality of the ab (“actor effect” for path b) paths was tested. This testing was repeated for all six pairs of corresponding paths.
Next, a model specifying all of the constraints that did not result in significantly worse model fit during the previous steps was fit to the data. The fit of each of these constrained models was then evaluated using a chi-square test (p > .10), RMSEA (p[RMSEA ≤ .05] > .50), and CFI (≥ .95). For the final APIMs, the results of the tests of individual equality constraints are reflected in the models. Models in which the constituent paths of an indirect effect were equal for patients and spouses yielded a single estimate (common to both dyad members) for that indirect effect. We then tested direct and indirect associations using 95% bootstrap confidence intervals (based on 10,000 replications). Indirect associations of primary interest are labeled as “Actor-Partner” effects in Table 2.
Table 2.
Unstandardized parameter estimates and 95% confidence intervals from Actor-Partner Interdependence Modeling
| Effect Type | Effect Description | Estimate | 95% CI |
|---|---|---|---|
| Section 1: APIM for associations among anxious attachment, holding back, and physical well-being | |||
| Direct | −0.87 | (−1.87, 0.10) | |
| Indirect | |||
| Actor-Partner | SP Attachment → SP Holding Back → PT Well-being | −0.45 | (−0.91, −0.11) |
| Direct | −0.42 | (−1.04, 0.13) | |
| Indirect | |||
| Actor-Partner | PT Attachment → PT Holding Back → SP Well-being | −0.04 | (−0.25, 0.17) |
| Model Fit Indices | |||
| χ2(10, n = 166) = 16.63, p = .08 RMSEA = 0.06, p(RMSEA) ≤ .05 = .30 CFI = 0.95 | |||
| Section 2: APIM for associations among anxious attachment, disclosure, and physical well-being | |||
| Direct | −0.65 | (−1.15, −0.20) | |
| Indirect | |||
| Actor-Partner | SP Attachment → SP Disclosure → PT Well-being | −0.37 | (−0.75, −0.12) |
| Direct | −0.65 | (−1.15, −0.20) | |
| Indirect | |||
| Actor-Partner | PT Attachment → PT Disclosure → SP Well-being | 0.06 | (−0.06, 0.19) |
| Model Fit Indices | |||
| χ2(15, n = 166) = 8.53, p = .90 RMSEA = 0.00, p(RMSEA) ≤ .05 = 0.98 CFI = 1.00 | |||
| Section 3: APIM for associations among avoidant attachment, holding back, and physical well-being | |||
| Direct | 0.00 | (−0.59, 0.55) | |
| Indirect | |||
| Actor-Partner | SP Attachment → SP Holding Back → PT Well-being | −0.50 | (−0.94, −0.19) |
| Direct | 0.00 | (−0.59, 0.55) | |
| Indirect | |||
| Actor-Partner | PT Attachment → PT Holding Back → SP Well-being | −0.07 | (−0.28, 0.09) |
| Model Fit Indices | |||
| χ2(14, n = 166) = 15.44, p = .35 RMSEA = 0.02, p(RMSEA) ≤ .05 = .71 CFI = 0.99 | |||
| Section 4: APIM for associations among avoidant attachment, disclosure, and physical well-being | |||
| Direct | −0.18 | (−0.77, 0.35) | |
| Indirect | |||
| Actor-Partner | SP Attachment → SP Disclosure → PT Well-being | −0.29 | (−0.71, −0.03) |
| Direct | −0.18 | (−0.77, 0.35) | |
| Indirect | |||
| Actor-Partner | PT Attachment → PT Disclosure → CG Well-being | 0.00 | (−0.10, 0.10) |
| Model Fit Indices | |||
| χ2(14, n = 166) = 10.97, p = .69 RMSEA = 0.00, p(RMSEA) ≤ .05 = .91 CFI = 1.00 | |||
Note. SP = Spouse; PT = Patient.
Results
Sample characteristics and descriptive statistics
A total of 166 dyads participated in this study. The agreement rate was 44.3% (166 consented/ 374 approached). The primary reasons that patients and/or spouses declined participation were lack of interest in the study (46%) or being too busy (21%). The assessment response rate was 100%.
Patients were 65% female and 86% White with a mean age 52.45 years (SD = 12.5). Forty-four percent of patients had breast cancer; 52% colorectal cancer, and 4% lung cancer. Spouses were 37% female and 87% White with a mean age 53.0 (SD = 13.15). A majority of couples (65.6%) had been married or cohabitating for 16 or more years.
Correlational Findings
Correlations among key study variables are summarized in Table 1. Patients’ anxious and avoidant attachment were negatively correlated with their own PWB and positively correlated with their own holding back. Patients’ anxious attachment was also positively correlated with their own emotional disclosure.
Table 1.
Correlations among Key Study Variables (Patients N = 166 and Spouses, N = 166)
| Variables | Attachment Anxiety | Attachment Avoidance | Disclosure | Holding Back | Physical Well-being | Emotional Expressivity |
|---|---|---|---|---|---|---|
| Attachment anxiety | - | .63** | .28** | .43** | −.26** | −.12 |
| Attachment avoidance | .53** | - | .15 | .33** | −.36** | −.45** |
| Disclosure | .22** | .08 | - | .39** | −.28** | −.05 |
| Holding Back | .37** | .24** | .49** | - | −.42** | −.20* |
| Physical Well-Being | −.29** | −.21** | −.30** | −.28** | - | .04 |
| Emotional Expressivity | −.14 | −.51** | .09 | −.02 | .01 | - |
| Patients Mean (SD) | 2.05 (0.93) | 2.50 (0.67) | 2.35 (0.87) | 2.03 (0.92) | 17.18 (5.00) | 63.77 (14.14) |
| Spouses Mean (SD | 1.88 (0.78) | 2.51 (0.67) | 2.24 (0.83) | 1.94 (0.76) | 20.88 (3.06) | 60.02 (14.54) |
Note
p < .001;
p <. 05;
above the diagonal represents correlations of study variables for patients; below the diagonal represents correlations of study variables for spouses.
Similarly, spouses’ anxious and avoidant attachment were negatively correlated with their own PWB and positively correlated with their own holding back. Spouses’ anxious attachment was also positively correlated with their own emotional disclosure (Table 1).
Avoidant attachment and emotional expressivity were negatively correlated in both patients (r = −.45, p < .001) and spouses (r = −.51, p < .001). No other bivariate correlations between covariates (i.e., gender and emotional expressivity) and the attachment measures were statistically significant.
Actor‐Partner Interdependence Model Findings
Path diagrams representing the results of the final (constrained) APIMs are presented in Figures 2–5, with unstandardized path coefficients and standardized covariances (i.e., correlations). The direct effects shown in each figure represent the effects of attachment anxiety or avoidance on PWB after accounting for disclosure and holding back. Path coefficients sharing a common superscript were constrained to be equal. Fit indices indicated that each of the final models demonstrated good fit (see Table 2). Paths that were significantly different from zero (based on 95% bootstrap CIs) are represented by solid arrows. Paths not significantly different from zero are represented by dashed arrows. Gender and EE were not generally related to mediators or outcomes, accordingly these associations are not represented in the figures. Findings from tests of actor-partner indirect effects (also based on bootstrap confidence intervals) are summarized in Table 2.
Figure 2.
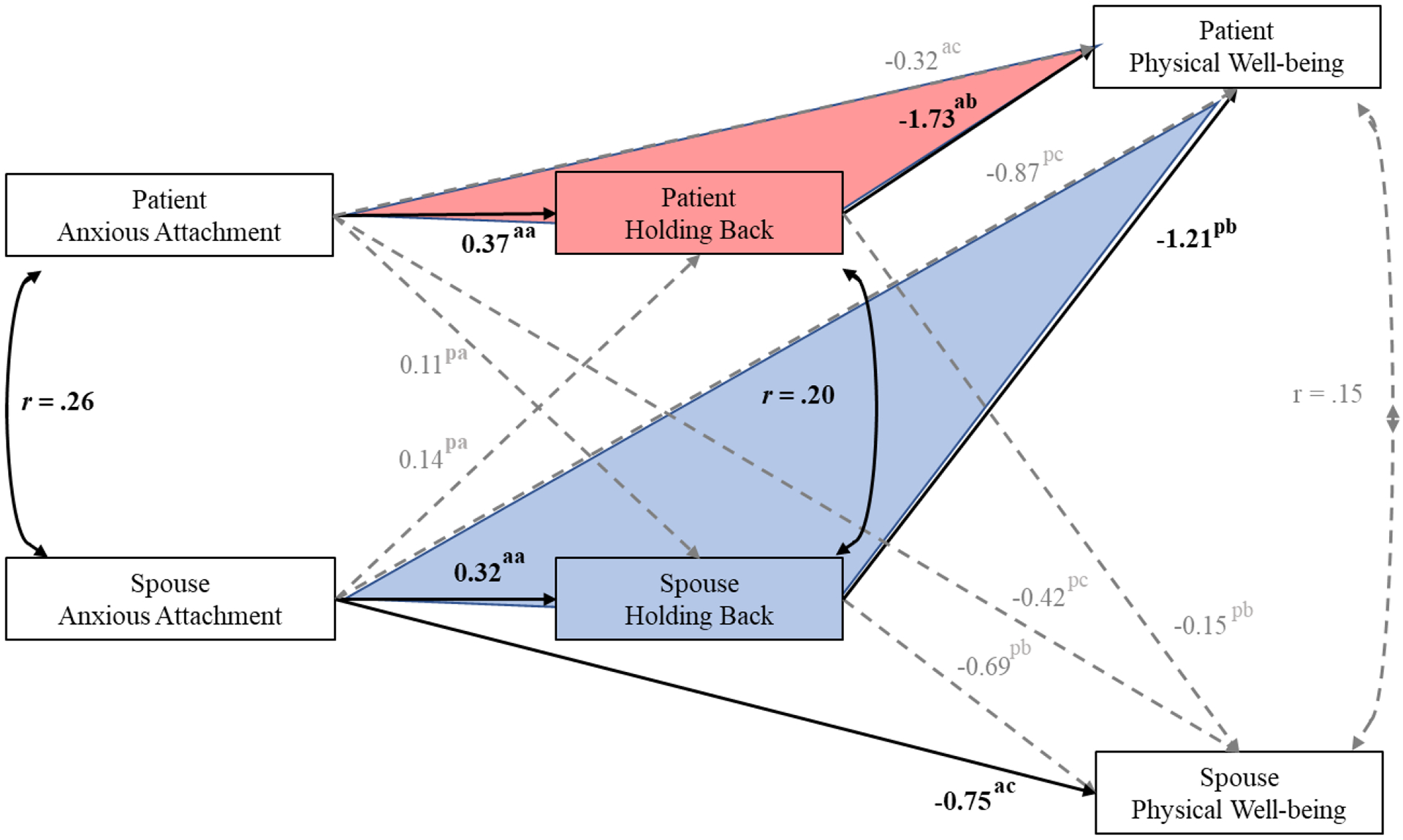
APIM Results: Anxious Attachment, Holding Back, and Physical Well-being. Solid lines denote significant paths; dotted lines, non-significant. Colored triangles denote significant mediation paths.
Figure 5.
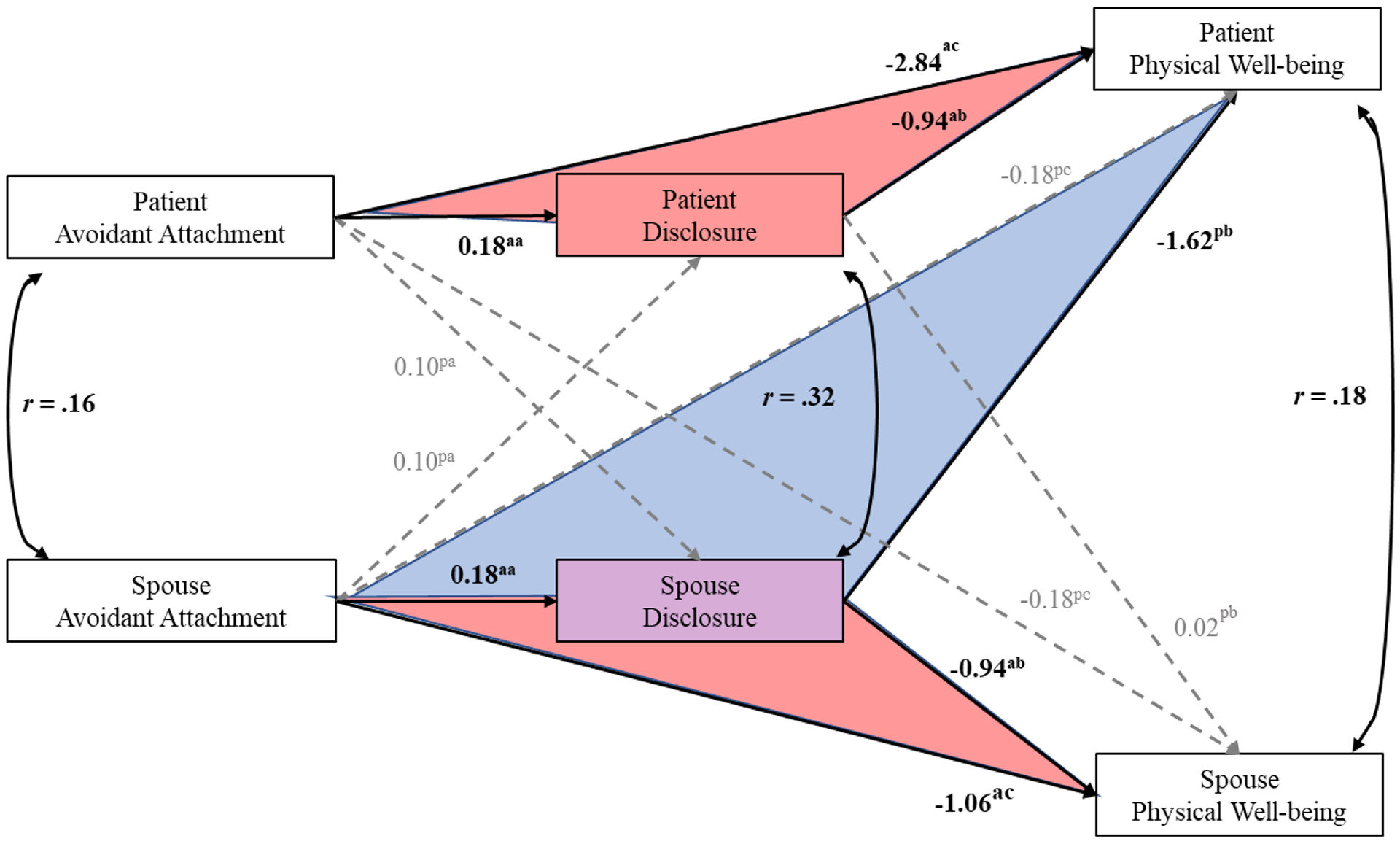
APIM Results: Avoidant Attachment, Disclosure, and Physical Well-Being. Solid lines denote significant paths; dotted lines, non-significant. Colored triangles denote significant mediation paths.
Mediation tests of anxious attachment on PWB through holding back (Figure 2).
Actor effects.
Following the conventions of the APIM framework, the associations between each dyad member’s own attachment and their own PWB are identified as “actor effects” here. For both patients and spouses, anxious attachment was negatively associated with one’s own PWB. This association was mediated by one’s own holding back for patients (IE = −0.64, 95% CI = −1.22, −.0.26) but not for spouses (IE = −0.22, 95% CI = −0.60, .0.004 for spouse). Thus, while for both dyad members higher anxious attachment was associated with greater holding back, only for patients did holding back mediate the relationship with their own PWB (see Figure 2).
Partner effects.
Here also, following the conventions of the APIM framework, the associations between each dyad member’s own attachment and the other member’s PWB (i.e., patient’s attachment with spouse’s PWB and spouse’s attachment with patient’s PWB) are identified as “partner effects.” The indirect association of one’s own anxious attachment with partner PWB via one’s own holding back was significant for spouses (IE = −0.38, 95% CI = −0.89, −0.07; see Table 2 Section 1), but not for patients (IE = −0.06, 95% CI = −0.33, 0.14). Thus, higher anxious attachment on the part of spouses was associated with their own greater holding back, which in turn was associated with poorer patient PWB.
Mediation tests of anxious attachment on PWB through disclosure (see Figure 3).
Figure 3.
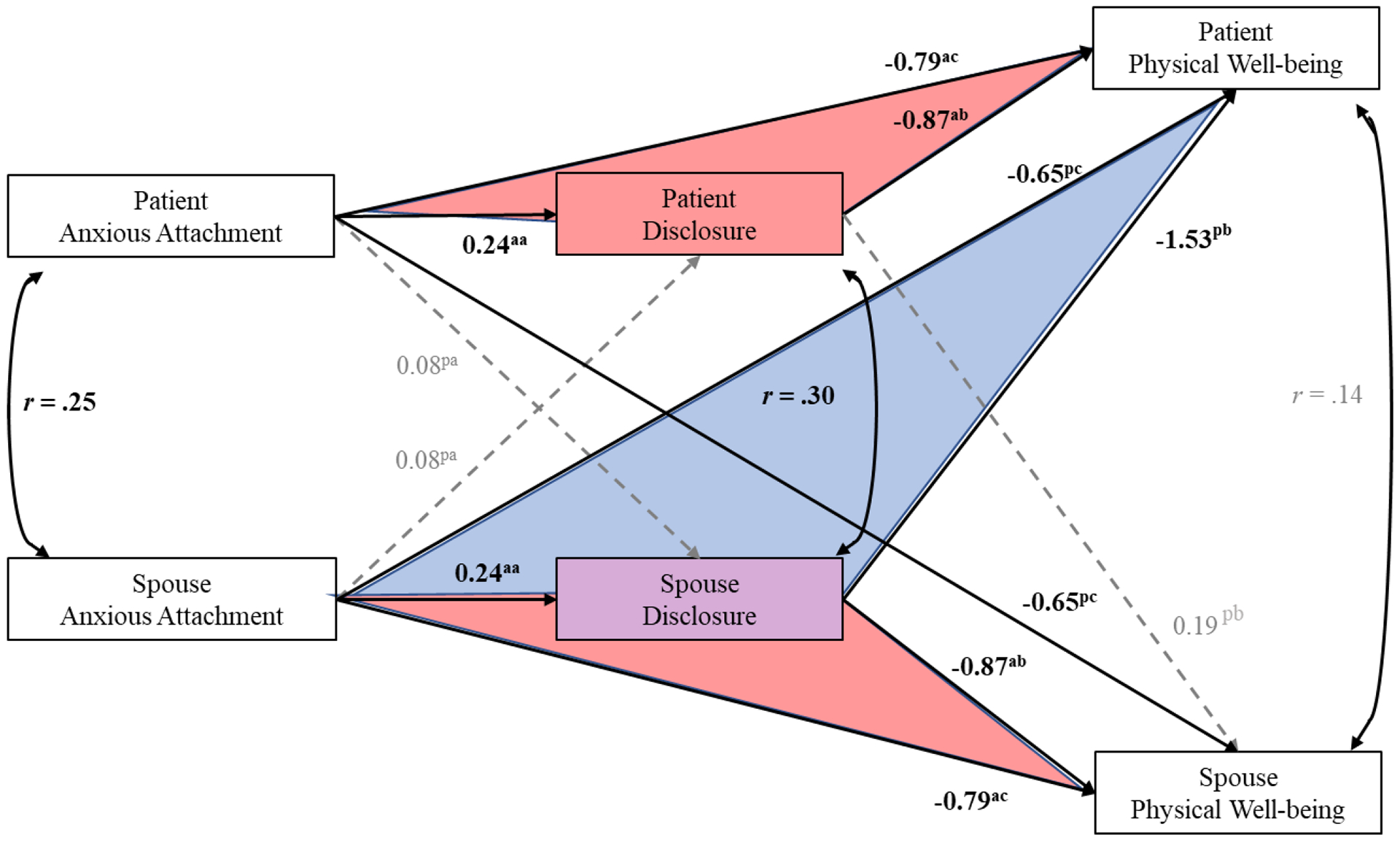
APIM Results: Anxious Attachment, Disclosure, and Physical Well-being. Solid lines denote significant paths; dotted lines, non-significant. Colored triangles denote significant mediation paths.
Actor effects.
For both dyad members, the anxious attachment-PWB link was mediated by disclosure (IE = −.21, 95% CI = −0.40, −0.09) as indicated by positive actor effects between anxious attachment and disclosure, and significant actor effects between disclosure and PWB for both patient and spouse. Thus, the more anxiously attached patients and spouses were, the more they disclosed their feelings, which in turn was associated with their own poorer PWB.
Partner effects.
Spouse anxious attachment was indirectly associated with patient PWB through disclosure (IE = −0.37, 95% CI = −0.75, −0.12; see Table 2 Section 2). The more anxiously attached spouses were, the more they disclosed their feelings, which in turn was associated with poorer PWB for the patient. Other partner effects were not significant.
Mediation tests of avoidant attachment on PWB through holding back (Figure 4).1
Figure 4.
APIM Results: Avoidant Attachment, Holding Back, and Physical Well-Being. Solid lines denote significant paths; dotted lines, non-significant. Colored triangles denote significant mediation paths.
Actor effects.
For patients and spouses both, avoidant attachment was associated with lower PWB, and this association was mediated by one’s own holding back (IE = −.39, 95% CI = −0.76, −0.15).
Partner effects.
Spouse avoidant attachment was associated with patient PWB through spouse holding back (IE = −0.60, 95% CI = −1.13, −0.23; see Table 2 Section 3). The more avoidantly attached spouses were, the more they held back their feelings, which in turn was associated with poorer PWB for the patient. Other partner effects were not significant.
Mediation tests of avoidant attachment on PWB through disclosure (see Figure 5).1
Actor effects.
There were significant positive actor effects between avoidant attachment and disclosure (b = 0.18, 95% CI = 0.01, 0.34 for both members). In addition, for both patients and spouses, there was a significant, negative actor effect between disclosure and PWB (b = −0.94, 95% CI = −1.14, −0.52 for both members). Thus, patients and spouses who reported more avoidant attachment reported more disclosure, and in turn, also reported poorer PWB (IE = −0.17, 95% CI = −0.38, - 0.52; for both members).
Partner effects.
There was a positive actor effect between spouse’s avoidant attachment and spouse’s own disclosure described above (b = 0.18, 95% CI = 0.01, 0.34), and the negative partner effect between spouse’s disclosure and patient’s PWB (b = −1.62, 95% CI = −2.57, −0.74), yielded a significant indirect effect (IE = −0.29, 95% CI = −0.71, −0.03; see Table 2, Section 4). Thus, in couples where spouses reported more avoidant attachment, spouses also reported more disclosure, and in turn, patients reported poorer PWB.
Discussion
Overall, our study findings suggest that anxious attachment in patients and spouses is positively associated with both disclosure and holding back of thoughts and feelings related to cancer and its treatment, and negatively associated with their own PWB. Avoidant attachment in patients and spouses was positively associated with holding back and also negatively associated with their PWB. We also found evidence that disclosure and holding back mediated the relationship between attachment and PWB both at the actor (within person) and partner (across partners) level, with partner effects primarily found for spouse’s attachment being associated with poorer patient physical well-being through spouse disclosure and holding back. Findings from this study extend prior literature on the important role of attachment in the adjustment of patients with cancer and their spouses. To our knowledge, this study is the first to examine communication, in particular disclosure and holding back, as a mechanism underlying the association between attachment and PWB in couples coping with cancer, and to examine both actor and partner effects.
Interestingly, we found a significant positive correlation between disclosure and holding back, and found that both disclosure and holding back were significantly negatively correlated with PWB. These findings suggest that disclosure may not be uniformly positive as a communication strategy. The role of disclosure may be more complex and may require more attention to context, including the attachment of partners and the function of disclosure in couples coping with cancer. We discuss specific findings and their implications in more detail below.
Intrapersonal Associations between Attachment and PWB
Findings indicated that, for both patients and spouses, having an anxious or avoidant attachment style was associated with one’s own poorer PWB, supporting hypothesized associations between insecure attachment and lower PWB. From an attachment perspective, a disease such as cancer may trigger significant stress in anxiously and avoidantly attached patients and spouses, who may have more difficulty making effective use of coping strategies and interpersonal resources due to attachment insecurity. Poorly managed physiological responses to stress (Maunder & Hunter, 2008) in turn may be associated with indices of poorer physical well-being, including greater pain, fatigue, and illness (Feeney, 2000).
Interpersonal Associations between Attachment and PWB
Among both patients and spouses, anxious but not avoidant attachment was negatively associated with the other partner’s PWB. Thus, patients and spouses high in anxious attachment had partners who reported significantly poorer health. To our knowledge, these findings are the first to document in cancer patients and spouses the actor–partner links between attachment in one partner and the PWB of the other. Results also support the promise of dyadic approaches to studying or intervening with couples coping with cancer. Anxiously attached individuals may become so concerned with relational distress and excessive worry about their partner’s responsiveness that this may overwhelm their partner. The lack of significant interpersonal effects for avoidant attachment may be related to the tendency of avoidantly attached individuals to minimize their own concerns and distress in threatening contexts (Bowlby, 1969/1982). As such, when a patient or spouse is avoidantly attached, they may emotionally distance themselves from the partner or downplay their own distress, which may limit its impact on the other’s PWB.
Mediation of Hypothesized Associations
Actor (intrapersonal) effects.
When examining actor (intrapersonal) effects for patients, the anxious attachment-PWB link was mediated by both holding back and disclosure. For spouses, the anxious attachment-PWB link was mediated by disclosure alone. Additionally, for both patients and spouses, the avoidant attachment-PWB link was mediated by holding back and disclosure. Thus, among patients, those high in anxious or avoidant attachment engaged in more disclosure and holding back, which in turn was associated with their own poorer PWB. A similar pattern was evident among spouses, although only avoidant attachment was associated with their own higher holding back.
In the context of threat, individuals who are anxiously attached may seek proximity to others and disclose how they feel in order to seek out reassurance and validation (Bowlby, 1982; Mikulincer & Shaver 2016, 2019). However, in the very process of seeking closeness and intimacy in their relationship, anxiously attached individuals often worry about being rejected or abandoned by their partners (Collins & Read, 1990) for their excessive support-seeking, and thus may resort to holding back behaviors as well. We found this was only the case for patients and not spouses in our study. It may be that for patients, having cancer heightens the fear and threat of being abandoned. In which case, a patient’s anxious disposition may be overly triggered as he or she is feeling challenged by the schemas about how he/she views themselves and their relationship (Mikulincer & Shaver, 2019; Stapleton, Woodcroft-Brown, & Chatwin, 2016).
For avoidantly attached patients and spouses the threat of living and coping with cancer may lead to minimization of distress and greater holding back. One plausible reason for this finding is that avoidant patients and spouses may not be in a psychological space to agree how they respectively feel about living and coping with cancer, and thus are ill-prepared to be emotionally supportive to one another (Dagan et al., 2014; Mikulincer & Shaver, 2019). This finding may also suggest that avoidantly attached individuals may have a different need to express and show their emotions. For example, avoidantly attached people often feel more supported when their partners showed instrumental support, which may be perceived as less emotionally threatening (Simpson Winterheld, Rholes, & Oriña., 2007).
Partner (interpersonal) effects.
When examining interpersonal effects of holding back and disclosure on the link between attachment and PWB, we found significant associations for spouses but not for patients. Specifically, spouses high in anxious attachment were more likely to hold back and to disclose, both of which in turn were associated with poorer patient PWB. Recent literature in caregiving styles and attachment in couples coping with cancer suggests that attachment anxiety is associated with less sensitive and more compulsive caregiving (e.g., the tendency to be overinvolved and over-protective, often engaging in extreme identification with a partner’s difficulties or issues) (Braun et al., 2012). Thus, holding back and disclosure may be driven by the spouse’s need to manage personal distress that overall serves little benefit to the patient. Examples may include spouses over-sharing their worries about cancer to their partner in order to feel validated in their concerns, while at the same time, over-protecting their partner and holding back on cancer topics that they perceive may rupture the relationship. This is consistent with the view of Baston (1991) and others (Feeney & Hohaus, 2001; Tsilika et al., 2015) who suggest that providing care to partners may be motivated by either genuine empathic concern or by personal self-centeredness to reduce one’s own distress (George-Levi et al., 2016).
Lastly, an unexpected finding was that holding back and disclosure were positively correlated. This contrasts with prior studies finding disclosure and holding back to be moderately and negatively correlated (Porter et al., 2005a, 2009), or not significantly correlated (Manne et al., 2010). One potential explanation for this discrepancy is that the correlations of these two constructs may vary as a function of couples’ motives to engage in these behaviors and the context in which these behaviors occur.
These motives may be directly related to one’s attachment style. In fact, there is recent research to support this paradox (Paprocki, & Baucom, 2017). For example, one common strategy for individuals who have relationship-based anxiety is to engage in interpersonal avoidance. This behavior is known as self-silencing (Jack, 1991; Paprocki, & Baucom, 2017). For fear of losing one’s partner’s support, an individual may “self-edit” in such a way that they may become overly agreeable or accommodating to what they believe their partner wants in order to preserve intimacy. At the same time, they might not disclose what they really feel. Thus, they may express what they believe they should share and hold back thoughts and feelings they think may compromise the relationship. It is also possible that they may express thoughts and feelings that they may find “safe” and not ones that may compromise the relationship. Thus, what does get disclosed may not be personally satisfying and thus contribute to poor well-being (as evidenced by the negative association between disclosure and PWB in our study). In essence, a singular motive to preserve the relationship might result in disclosing what the person believes the other wants to hear while holding back on other thoughts and feelings that may seem riskier to disclose.
These findings underscore the importance of communication in context. Holding back and disclosure may not necessarily represent opposite ends of a continuum but rather separate dimensions that can function independently under certain circumstances, such as discussing cancer-related topics. Thus, during cancer-related discussions, spouses and partners may disclose some concerns but may hold back from disclosing others, or may not express the severity of their fears or worries to emotionally protect the other and/or preserve a sense of mutuality (Manne et al., 2010). Attention to the context of cancer and its treatment as well as of attachment helps to make sense of these findings but also raises questions about their generalizability. Our findings may not generalize to more generic or relationally-focused forms of disclosure or holding back unrelated to serious illness like cancer.
Strengths and Limitations
A notable strength of this study was the simultaneous examination of patient and spouse data using actor-partner statistical models to test the interdependence among both partners’ attachment, communication behaviors, and PWB. This strategy provided a unique opportunity to investigate both intrapersonal and interpersonal processes and mechanisms.
Despite these strengths, there are several limitations to note. First, the sample was predominantly Caucasian and well-educated, precluding generalizability to other diverse samples. Our study also focused on one type of medical illness (i.e., cancer) and results may not apply to other serious, life-limiting illnesses. In addition, the study design was cross-sectional and thus the correlational nature of the data precludes causal conclusions. Prospective studies that assess communication and physical well-being over time would allow for a better understanding of the relationship of attachment to health outcomes. Due to the complexity of the analyses and models, we did not investigate how the interaction of patient and spouse attachment dimensions may influence the mediating role of communicative behaviors or the relationship of attachment with PWB. This would be a topic for further study.
In this study, the response rate was 44%, which may seem low. However, this rate is comparable to other studies recruiting patients with cancer and their spouses (Dagan & Hagedoorn, 2014). Lastly, the use of self-report measures may not offer a full picture of attachment dynamics and health in couples. Data from our larger study includes objective measures of communication which may illuminate additional dynamics in how these baseline measures influence other factors over time and in how couples’ attachment and disclosure adapt over time. Future studies could include objective approaches to the assessment of both attachment and communication behaviors (such as behavioral coding of communication during couples’ discussions about cancer) and more comprehensive or objective measures of physical health (e.g., patients’ response to cancer treatments, spouse health care use) to substantiate these results.
Future directions.
Future areas worth exploring include the examination of attachment in the context of relationship satisfaction, communication quality (e.g., is the communication exchange between partners perceived as supportive and sensitive) and well-being in couples. It is possible that levels of relationship satisfaction among couples who are anxious or avoidant may impact how couples communicate and feel about themselves and each other. Another area in need of further study is how the attachment of patients and spouses interact with each other and determine how communication behaviors are expressed and received in couples coping with cancer. Greater or lesser congruence in attachment styles and/or communicative behaviors may influence the role of holding back and disclosure in their relationship.
Furthermore, it may be worth exploring associations between attachment styles and motivations for methods of giving and receiving support that influence communication behaviors in the context of cancer. For example, what is the motivation behind sharing or holding back? As mentioned previously in reference to protective buffering, motivations may be prosocial and/or egoistic, that is, rooted in protecting one’s partner or in protecting oneself (Langer et al., 2009). Do these different motivations manifest differently behaviorally? What is the nature of holding back and disclosure with respect to both content (e.g., what is said) and delivery (e.g., how communication is relayed)? And, under what circumstances during cancer-related discussions are holding back and disclosure adaptive or maladaptive?
If the current findings are replicated in future work, they may have implications for clinical interventions. Emotional disclosure is generally viewed as an adaptive strategy for enhanced communication (Manne et al., 2004; Porter et al., 2005a), but disclosure per se may not be adaptive. It is important to consider what is disclosed (content) is and how it is disclosed (delivery). Spousal disclosure of frustration with a patient’s non-adherence to medications, for example, could be perceived as nagging or controlling by the patient. Clinical interventions designed to improve couple’s communication in cancer may benefit from first exploring patient and partner styles of disclosure and delivery. Additionally, clinicians should consider the effects of the disclosure and how it may be associated with patient and spouse attachment style, and motivations in supporting one another. It may be important to first assess attachment styles in couples, and the degree of match or mismatch, to help guide how communication interventions are presented and delivered. Additionally, given that patients are at particular risk when a spouse is insecurely attached, providing spouses/partners with independent training to improve their communication delivery and enhance their efforts of giving and receiving support may prove beneficial.
Overall, our study findings support the benefit of dyadic analyses and examination of mechanisms to advance the science on attachment in the context of couples coping with serious illnesses such as cancer. Ultimately this work may lead to interventions that can improve the health and well-being of both patients and their caregiving spouses.
Funding:
This study was funded by grant R01CA201179 from the National Cancer Institute, awarded to Multiple Principal Investigators Shelby Langer and Laura S. Porter.
Footnotes
Mediation tests of avoidant attachment on physical well-being through holding back (Fig.4): patient EE was negatively related to patient PWB (b = -0.06, 95% CI = -0.11, -0.02). Mediation tests of avoidant attachment on physical well-being through disclosure (Fig. 5) patient EE was negatively related to patient PWB (b = -0.06, 95% CI = -0.11, -0.01).
References
- Badr H (2017). New frontiers in couple-based interventions in cancer care: Refining the prescription for spousal communication. Acta Oncologica, 56, 139–145. 10.1080/0284186X.2016.1266079 [DOI] [PubMed] [Google Scholar]
- Badr H, & Krebs P (2013). A systematic review and meta‐analysis of psychosocial interventions for couples coping with cancer. Psycho‐Oncology, 22, 1688–1704. 10.1002/pon.3200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baider L, & Bengel J (2001). Cancer and the spouse: Gender-related differences in dealing with health care and illness. Critical Reviews in Oncology/Hematology, 40, 115–123. 10.1016/S1040-8428(01)00137-8 [DOI] [PubMed] [Google Scholar]
- Baston CD (1991). Self‐other merging and the empathy‐altruism hypothesis: reply to Neuberg et al. Journal of Personality and Social Psychology, 73, 517–522. [Google Scholar]
- Bowlby J (1969/1982). Attachment and loss: Vol. 1. Attachment (2nd ed.). New York, NY: Basic Books. [Google Scholar]
- Bowlby J (1988). A secure base: Parent-child attachment and healthy human development. New York, NY: Basic Books. [Google Scholar]
- Bradford SA, Feeney JA, & Campbell L (2002). Links between attachment orientations and dispositional and diary–based measures of disclosure in dating couples: A study of actor and partner effects. Personal Relationships, 9, 491–506. doi: 10.1111/1475-6811.00031 [DOI] [Google Scholar]
- Braun M, Hales S, Gilad L, Mikulicer M, Rydall A, & Rodin G (2012). Caregiving styles and attachment orientations in couples facing advanced cancer. Psycho‐Oncology, 21, 935–943. 10.1002/pon.1988 [DOI] [PubMed] [Google Scholar]
- Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, … & Eckberg, K. (1993). The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. Journal of Clinical Oncology, 11, 570–579. [DOI] [PubMed] [Google Scholar]
- Collins NL, & Read SJ (1990). Adult attachment, working models, and relationship quality in dating couples. Journal of Personality and Social Psychology, 58, 644–663. doi: 10.1037/0022-3514.58.4.644 [DOI] [PubMed] [Google Scholar]
- Collins NL, & Read SJ (1996). Revised adult attachment scale. Unpublished instrument, scoring instructions and reliability information, Department of Psychology, University of California, Santa Barbara. [Google Scholar]
- Dagan M, & Hagedoorn M (2014). Response rates in studies of couples coping with cancer: A systematic review. Health Psychology, 33, 845–852. 10.1037/hea0000013 [DOI] [PubMed] [Google Scholar]
- Dagan M, Sanderman R, Hoff C, Meijerink WJ, Baas PC, van Haastert M, & Hagedoorn M (2014). The interplay between partners’ responsiveness and patients’ need for emotional expression in couples coping with cancer. Journal of Behavioral Medicine, 37, 828–838. doi: 10.1007/s10865-013-9543-4 [DOI] [PubMed] [Google Scholar]
- De Luca R, Dorangricchia P, Salerno L, Coco GL, & Cicero G (2017). The role of couples’ attachment styles in patients’ adjustment to cancer. Oncology, 92, 325–334. 10.1159/000455956 [DOI] [PubMed] [Google Scholar]
- Ehrlich KB (2019). Attachment and psychoneuroimmunology. Current Opinion in Psychology, 25, 96–100. doi: 10.1016/j.copsyc.2018.03.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feeney JA (2000). Implications of attachment style for patterns of health and illness. Child: Care, Health and Development, 26, 277–288. doi: 10.1046/j.1365-2214.2000.00146.x [DOI] [PubMed] [Google Scholar]
- Feeney JA, & Hohaus L (2001). Attachment and spousal caregiving. Personal Relationships, 8, 21–39. 10.1111/j.1475-6811.2001.tb00026.x [DOI] [Google Scholar]
- Frisina PG, Borod JC, & Lepore SJ (2004). A meta-analysis of the effects of written emotional disclosure on the health outcomes of clinical populations. The Journal of Nervous and Mental Disease, 192, 629–634. doi: 10.1097/01.nmd.0000138317.30764.63 [DOI] [PubMed] [Google Scholar]
- George-Levi S, Vilchinsky N, Tolmacz R, Khaskiaa A, Mosseri M, & Hod H (2016). “It takes two to take”: Caregiving style, relational entitlement, and medication adherence. Journal of Family Psychology, 30, 743–751. 10.1037/fam0000203 [DOI] [PubMed] [Google Scholar]
- Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, … & Duda SN (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics, 95, 103208. doi: 10.1016/j.jbi.2019.10320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, & Conde JG (2009). A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42, 377–381. 10.1016/j.jbi.2008.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jack DC (1991). Silencing the self: Women and depression. Harvard University Press. [Google Scholar]
- Kenny DA, Kashy DA, & Cook WL (2006). Dyadic data analysis. New York, NY: The Guilford Press. [Google Scholar]
- Kring AM, Smith DA, & Neale JM (1994). Individual differences in dispositional expressiveness: Development and validation of the Emotional Expressivity Scale. Journal of Personality and Social Psychology, 66, 934–949. 10.1037/0022-3514.66.5.934 [DOI] [PubMed] [Google Scholar]
- Langer SL, Brown JD, & Syrjala KL (2009). Intrapersonal and interpersonal consequences of protective buffering among cancer patients and caregivers. Cancer, 115, 4311–4325. 10.1002/cncr.24586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manne S, Badr H, Zaider T, Nelson C, & Kissane D (2010). Cancer-related communication, relationship intimacy, and psychological distress among couples coping with localized prostate cancer. Journal of Cancer Survivorship, 4, 74–85. doi: 10.1007/s11764-009-0109-y.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manne S, Myers S, Ozga M, Kissane D, Kashy D, Rubin S,… & Rosenblum N (2014). Holding back sharing concerns, dispositional emotional expressivity, perceived unsupportive responses and distress among women newly diagnosed with gynecological cancers. General Hospital Psychiatry, 36, 81–87. 10.1016/j.genhosppsych.2013.10.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manne S, Ostroff J, Rini C, Fox K, Goldstein L, & Grana G (2004). The interpersonal process model of intimacy: The role of self-disclosure, partner disclosure, and partner responsiveness in interactions between breast cancer patients and their partners. Journal of Family Psychology, 18, 589–599. doi: 10.1037/0893-3200.18.4.589 [DOI] [PubMed] [Google Scholar]
- Manne SL, Kissane D, Zaider T, Kashy D, Lee D, Heckman C, & Virtue SM (2015). Holding back, intimacy, and psychological and relationship outcomes among couples coping with prostate cancer. Journal of Family Psychology, 29, 708–719. doi: doi.org/ 10.1037/fam0000096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manne SL, Norton TR, Ostroff JS, Winkel G, Fox K, & Grana G (2007). Protective buffering and psychological distress among couples coping with breast cancer: The moderating role of relationship satisfaction. Journal of Family Psychology, 21, 380–388. 10.1037/0893-3200.21.3.380 [DOI] [PubMed] [Google Scholar]
- Manne SL, Ostroff J, Winkel G, Grana G, & Fox K (2005). Partner unsupportive responses, avoidant coping, and distress among women with early stage breast cancer: Patient and partner perspectives. Health Psychology, 24, 635–641. doi: 10.1037/0278-6133.24.6.635 [DOI] [PubMed] [Google Scholar]
- Manne SL, Taylor KL, Dougherty J, & Kemeny N (1997). Supportive and negative responses in the partner relationship: Their association with psychological adjustment among individuals with cancer. Journal of Behavioral Medicine, 20, 101–125. https://link.springer.com/article/10.1023/A:1025574626454 [DOI] [PubMed] [Google Scholar]
- Maunder RG, & Hunter JJ (2008). Attachment relationships as determinants of physical health. Journal of the American Academy of Psychoanalysis and Dynamic Psychiatry, 36, 11–32. 10.1521/jaap.2008.36.1.11 [DOI] [PubMed] [Google Scholar]
- Mikulincer M, & Nachshon O (1991). Attachment styles and patterns of self-disclosure. Journal of Personality and Social Psychology, 61, 321–331. 10.1037/0022-3514.61.2.321 [DOI] [Google Scholar]
- Mikulincer M, & Shaver PR (2003). The attachment behavioral system in adulthood: Activation, psychodynamics, and interpersonal processes. Advances in Experimental Social Psychology, 35, 56–152. doi: 10.1016/S0065-2601(03)01002-5 [DOI] [Google Scholar]
- Mikulincer M, & Shaver PR (2016). Attachment in adulthood: Structure, dynamics, and change (2nd ed.). New York, NY: Guilford Press. [Google Scholar]
- Mikulincer M, & Shaver PR (2019). Attachment orientations and emotion regulation. Current Opinion in Psychology, 25, 6–10. doi: 10.1016/j.copsyc.2018.02.006 [DOI] [PubMed] [Google Scholar]
- Milbury K, Yang C, Liao ZX, Tsao AS, & Bruera E (2018). Relationship processes and symptom burden in couples coping with metastatic lung cancer. Journal of Clinical Oncology 36, no. 34_suppl 169–169. [Google Scholar]
- Murray-Swank AB, McConnell KM, & Pargament KI (2007). Understanding spiritual confession: A review and theoretical synthesis. Mental Health, Religion and Culture, 10, 275–291. 10.1080/13694670600665628 [DOI] [Google Scholar]
- Paprocki CM, & Baucom DH (2017). Worried About us: Evaluating an Intervention for Relationship‐Based Anxiety. Family Process, 56, 45–58. 10.1111/famp.12175 [DOI] [PubMed] [Google Scholar]
- Pennebaker JW, Kiecolt-Glaser JK, & Glaser R (1988). Disclosure of traumas and immune function: health implications for psychotherapy. Journal of Consulting and Clinical Psychology, 56, 239–245. [DOI] [PubMed] [Google Scholar]
- Pietromonaco PR, & Barrett LF (1997). Working models of attachment and daily social interactions. Journal of Personality and Social Psychology, 73, 1409–1423. 10.1037/0022-3514.73.6.1409 [DOI] [PubMed] [Google Scholar]
- Pietromonaco PR, & Beck LA (2019). Adult attachment and physical health. Current Opinion in Psychology, 25, 115–120. 10.1016/j.copsyc.2018.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pietromonaco PR, DeVito CC, Ge F, & Lembke J (2015). Health and attachment processes. In Simpson JA, & Rholes WS (Eds.), Attachment theory and research: New directions and emerging themes (pp. 287–318). New York, NY: The Guilford Press. [Google Scholar]
- Pietromonaco PR, & Powers SI (2015). Attachment and health-related physiological stress processes. Current Opinion in Psychology, 1, 34–39. doi: 10.1016/j.copsyc.2014.12.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pietromonaco PR, Uchino B, & Dunkel-Schetter C (2013). Close relationship processes and health: Implications of attachment theory for health and disease. Health Psychology, 32, 499–513. doi: 10.1037/a0029349 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pistrang N, & Barker C (1995). The partner relationship in psychological response to breast cancer. Social Science & Medicine, 40, 789–797. 10.1016/0277-9536(94)00136-H [DOI] [PubMed] [Google Scholar]
- Porter LS, Keefe FJ, Baucom DH, Hurwitz H, Moser B, Patterson E, & Kim HJ (2009). Partner‐assisted emotional disclosure for patients with gastrointestinal cancer: results from a randomized controlled trial. Cancer, 115, 4326–4338. 10.1002/cncr.24578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porter LS, Keefe FJ, Baucom DH, Hurwitz H, Moser B, Patterson E, & Kim HJ (2012). Partner-assisted emotional disclosure for patients with GI cancer: 8-week follow-up and processes associated with change. Supportive Care in Cancer, 20, 1755–1762. [DOI] [PubMed] [Google Scholar]
- Porter LS, Keefe FJ, Davis D, Rumble M, Scipio C, & Garst J (2012). Attachment styles in patients with lung cancer and their spouses: associations with patient and spouse adjustment. Supportive Care in Cancer, 20, 2459–2466. https://link.springer.com/article/10.1007/s00520-011-1367-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porter LS, Keefe FJ, Hurwitz H, & Faber M (2005a). Disclosure between patients with gastrointestinal cancer and their spouses. Psycho‐Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer, 14, 1030–1042. 10.1002/pon.915 [DOI] [PubMed] [Google Scholar]
- Porter LS, Keefe FJ, Lipkus I, & Hurwitz H (2005b). Ambivalence over emotional expression in patients with gastrointestinal cancer and their caregivers: Associations with patient pain and quality of life. Pain, 117, 340–348. 10.1016/j.pain.2005.06.021 [DOI] [PubMed] [Google Scholar]
- Reardon KK, & Buck R (1989). Emotion, reason, and communication in coping with cancer. Health Communication, 1, 41–54. 10.1207/s15327027hc0101_6 [DOI] [PubMed] [Google Scholar]
- Regan TW, Lambert SD, Kelly B, Falconier M, Kissane D, & Levesque JV (2015). Couples coping with cancer: exploration of theoretical frameworks from dyadic studies. Psycho‐Oncology, 24, 1605–1617. doi: 10.1002/pon.3854 [DOI] [PubMed] [Google Scholar]
- Simpson JA, Winterheld HA, Rholes WS, & Oriña MM (2007). Working models of attachment and reactions to different forms of caregiving from romantic partners. Journal of Personality and Social Psychology, 93, 466–477. 10.1037/0022-3514.93.3.466 [DOI] [PubMed] [Google Scholar]
- Slatcher RB, & Schoebi D (2017). Protective processes underlying the links between marital quality and physical health. Current Opinion in Psychology, 13, 148–152. doi: 10.1016/j.copsyc.2016.09.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanton AL, & Danoff-Burg S (2002). Emotional expression, expressive writing, and cancer. In Lepore SJ & Smyth JM (Eds.), The writing cure: How expressive writing promotes health and emotional well-being (p. 31–51). American Psychological Association. 10.1037/10451-002 [DOI] [Google Scholar]
- Stapleton P, Woodcroft-Brown A, & Chatwin H (2016). Understanding the relationship between attachment style, relationship satisfaction, illness behaviours, and psychological distress in couples. Journal of Healing and Caring, 16, 1–16. [Google Scholar]
- Traa MJ, De Vries J, Bodenmann G, & Den Oudsten BL (2015). Dyadic coping and relationship functioning in couples coping with cancer: A systematic review. British Journal of Health Psychology, 20, 85–114. doi: 10.1111/bjhp.12094 [DOI] [PubMed] [Google Scholar]
- Tsilika E, Parpa E, Zygogianni A, Kouloulias V, & Mystakidou K (2015). Caregivers’ attachment patterns and their interactions with cancer patients’ patterns. Supportive Care in Cancer, 23, 87–94. doi: 10.1007/s00520-014-2329-6 [DOI] [PubMed] [Google Scholar]
- Ussher JM, & Perz J (2010). Gender differences in self-silencing and psychological distress in informal cancer carers. Psychology of Women Quarterly, 34, 228–242. 10.1111/j.1471-6402.2010.01564.x [DOI] [Google Scholar]