

Abstract
Background:
Over 10 million robotic surgeries have been performed. However, the cost and benefit of robotic surgery need to be evaluated to help hospitals, surgeons, patients, and payers make proper choices, making a health economic analysis necessary. The authors revealed the bibliometric profile in the field of health economics of robotic surgery to prompt research development and guide future studies.
Materials and methods:
The Web of Science Core Collection scientific database was searched for documents indexed from 2003 to 31 December 2022. Document types, years, authors, countries, institutions, journal sources, references, and keywords were analyzed and visualized using the Bibliometrix package, WPS Office software, Microsoft PowerPoint 2019, VOSviewer software (version 1.6.18), ggplot2, and Scimago Graphica.
Results:
The development of the health economics of robotic surgery can be divided into three phases: slow-growing (2003–2009), developing (2010–2018), and fast-developing (2019–2022). J.C.H. and S.L.C. were the most active and influential authors, respectively. The USA produced the most documents, followed by China, and Italy. Korea had the highest number of citations per document. Surgical Endoscopy and Other Interventional Techniques accepted most documents, whereas Annals of Surgery, European Urology, and Journal of Minimally Invasive Gynecology had the highest number of citations per document. The Journal of Robotic Surgery is promising. The most-cited document in this field is New Technology and Health Care Costs - The Case of Robot-Assisted Surgery in 2010. The proportion of documents on urology is decreasing, while documents in the field of arthrology are emerging and flourishing.
Conclusion:
Research on the health economics of robotic surgery has been unbalanced. Areas awaiting exploration have been identified. Collaboration between scholars and coverage with provisions for evidence development by the government is needed to learn more comprehensively about the health economics of robotic surgery.
Keywords: bibliometrics, healthcare economics and organizations, robotic surgical procedures
Introduction
Highlights
South Korea had the highest number of citations per document. A potential reason for this is discussed in the article.
The main research pattern in the health economics of robotic surgery is cost-effectiveness comparison among robot-assisted surgery, laparoscopic surgery, and open surgery, as well as cost analysis of robotic surgery in certain surgical disciplines, with trial, review, and meta-analysis being the major research methods.
Health economic research on robot-assisted orthopaedic surgery and thoracic surgery is currently a hot topic.
Robot-assisted transplant surgery, ophthalmic surgery, oral surgery, and dermatologic surgery lack health economics research.
Collaboration among institutes and coverage for robotic surgery with provisions for evidence development are suggested to promote an understanding of the health economics of robotic surgery.
By 2023, 7733 robotic surgical systems had been installed worldwide1,2. Over 10 million robotic surgeries have been performed3. These surgeries cover many disciplines, including general surgery4,5, urology6,7, gynaecology8,9, and cardiothoracic surgery10,11. Despite COVID-19, the revenue of Intuitive Surgical companies increased by 28% in 2022 compared with 20212, owing to the benefits of robotic surgery, including high-resolution three-dimensional vision, elimination of hand tremors, and a comfortable operating environment12,13. Some studies have suggested that robotic surgery can lead to lower complication rates, a better short-term quality of life, and better short-term postoperative functional recovery14. However, whether robotic surgery is more cost-effective than conventional surgeries remains controversial15,16. Moreover, the high cost, limited availability, and training opportunities are major obstacles to the adopting of robotic surgery17.
High costs are a long-standing problem. US hospitals paid over 6.22 billion dollars in 2022 for intuitive surgically assisted surgeries2,18. Robotically assisted hysterectomy costs hospitals $2189 more per procedure than laparoscopic hysterectomy8, suggesting that the cost difference for patients may be even higher. To solve this problem, scientists are researching the health economics of robotic surgery. Studies such as Paraiso et al.19, who found that robotic-assisted sacrocolpopexy had longer operating time, increased pain, and cost compared to laparoscopy, and Childers et al.18’s cost benchmarking, and De Rooij et al.20, which compared recovery times and quality of life after minimally invasive and open distal pancreatectomy, can guide adoption decisions21 and inspire cost reduction efforts22,23.
Bibliometric analysis is an effective tool for revealing research trends in specific topics24,25. It has been utilized in robotic surgery to uncover the interdisciplinary nature and topic hotspots26, research trends and patterns of research output27, and publication distributions in this field27,28. However, to the best of our knowledge, no bibliometric study has been performed on the health economics of robotic surgery. This study aims to (1) reveal hotspots and research trends (2), identify underlying issues, and (3) provide guidance to scholars and governments.
Materials and methods
Data source and search criteria
The Web of Science Core Collection (WoSCC) database was selected as the primary database for this study due to its comprehensive coverage of high-quality scholarly literature across various disciplines and its frequent usage by researchers. It was searched from its inception (2003) to 31 December 2022, using our search strategy (Search Strategy, Supplemental Digital Content 1, http://links.lww.com/JS9/B5) containing the search terms “health economic” and “robotic surgery”. There were no restrictions on the language, document type, data category, or document year. Then, a preliminary selection based on the title and abstract of the documents was made. To minimize bias introduced by manual selection, we employed a well-defined selection criteria, taking Gheorghe and colleagues’ research as a reference. Specifically, we included documents that explicitly listed any economic outcome related to health, disease, or disability, including but not limited to cost, cost-effectiveness, patient-reported outcomes, poverty associated with accessing healthcare, provider or health system performance, and health expenditures, in the abstract or title29. The study selection and flow chart of the research framework are shown in Figure 1.
Figure 1.
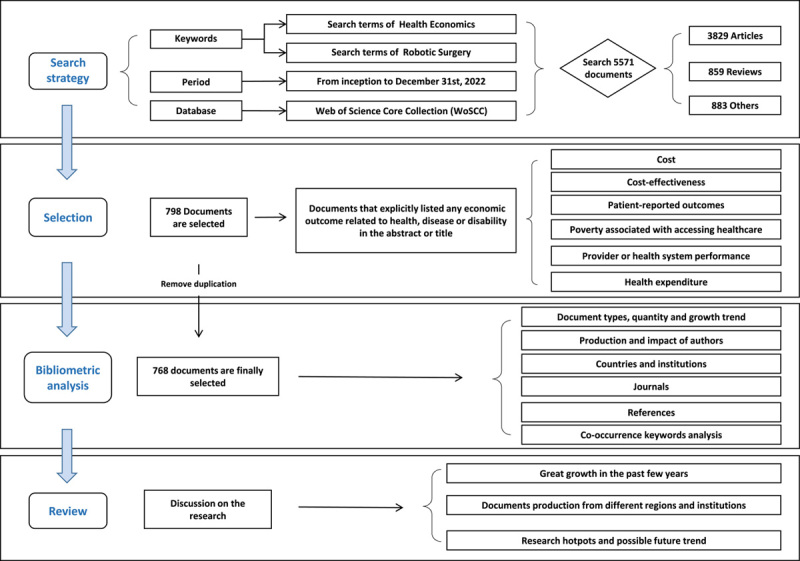
Document selection and flow chart of the research framework.
Analysis method
This study utilized Biblimetrix version 4.030 and VOSviewer software version 1.6.1831 to analyze document types, years, authors, countries, institutions, journal sources, references, and keywords to create social network maps. The number of citations each year was acquired from the Web of Science citation report, and data aggregation and analysis were conducted using WPS Office software. Related figures were drawn using the ggplot2 packages in R (version 4.2.1), Microsoft PowerPoint 2019 and Scimago Graphica32. Notably, when calculating the countries and districts of origin of the indexed documents, documents from China included those from Taiwan, Hong Kong, and Macao, while documents from the UK represented those from England, Northern Ireland, Scotland, and Wales. Social network analysis is the primary method used to analyze co-occurrence33. In bibliometrics, social network analysis is known to reflect research hotspots and trends in a given field in a multidimensional manner. Furthermore, cluster analysis was performed using the VOSviewer software to generate social network maps, which indicated the importance of node size and line thickness34,35. The nodes represent the number or frequency, whereas the lines between the nodes indicate associations, with thicker lines denoting stronger relationships. Thus, the resulting co-word network can visualize trends in health economic studies of robotic surgery. To further understand the research situation of the health economics of robotic surgery in the past 2 years, an additional analysis was performed using the keywords of documents published from 1 January 2021, to 31 December 2022, which will be described in detail later. Manual examination of keywords was conducted to gain a better understanding of the meaning of the keywords and ensure their accurate interpretation.
Results
Document type and quantity
A total of 768 records were identified after the removal of duplicates. Documents were classified into seven types (Fig. 2A). The majority of the documents were articles (72.01%), followed by reviews (15.63%), and proceedings papers (4.17%).
Figure 2.
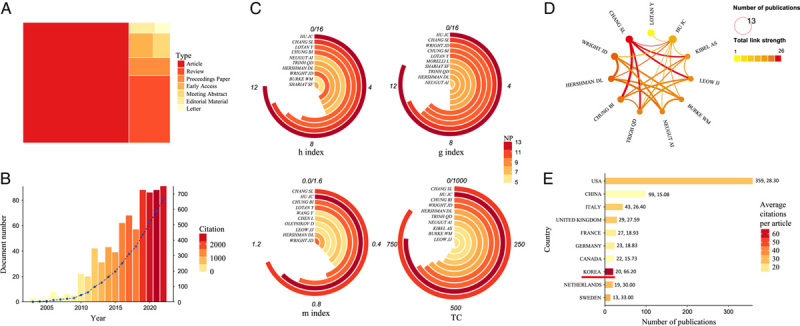
Distribution of document types (A), citations, number of documents accepted per year (B) in the field of health economics of robotic surgery (D) and the social impact (C) of the top 10 most productive authors, along with the collaboration pattern of the 11 authors whose number of publications exceeds 6. the number of indexed documents and average citations per document of the top 10 most productive countries (E). The saturation level of the colour in (B) reflects the citation number each year, while the line indicates the accumulative number of documents. TC, total citations.
Figure 2B shows the number of indexed documents from 2003 to 2022. The number of indexed documents grew slowly, with no more than ten documents per year before 2009. Relevant documents were rarely cited in that period, with fewer than 200 citations each year. However, since 2009, the number of indexed documents per year has outweighed 20 and has generally increased over time. The period from 2019 to 2022 indexed the most documents and received the most attention, with an average of 88 indexed documents, and the number of citations each year outweighed 2000 times.
Active authors, countries, and institutions
A total of 3982 authors were involved in the study of the health economics of robotic surgery. The social impact and production of the top 10 authors are shown in Figure 2C. Among the top 10 most productive authors, eight authors came from the USA. J.C.H. is not only the most productive author in this area but also has the highest h-index and g-index, followed by S.L.C., which has the highest m-index and total citations. Figure 2D displays the collaborative cluster network of authors with a production count exceeding 6. S.L.C. was the most collaborative author, while J.C.H. was ranked medially.
All the documents were obtained from 41 countries. Figure 2E shows the number of documents and average citations per document for the top 10 most productive countries. The USA produced the highest number of documents (359, 46.74%), followed by China (99 documents, 12.89%), and Italy (43 documents, 5.60%). In terms of average citations per document, Korea ranked first with the number of 66.20 citations per document on average. Canada and China ranked low with 15.73, 15.08 citations per document, respectively.
Figure S1 in the Supplemental Digital Content 2, http://links.lww.com/JS9/B6 shows the number of documents and collaborations among the 24 most productive countries. The close linkage between the USA, Germany, the United Kingdom, and Italy is visualized in this figure.
A total of 984 institutions worldwide were found to contribute to research on the health economics of robotic surgery. The top 10 most productive institution is summarized in Figure S2 in the Supplemental Digital Content 2, http://links.lww.com/JS9/B6. The most productive institution is the University of California, Los Angeles with 35 documents accepted. Close collaborative relationships were identified between institutions within each country, as indicated in Figure S3 in the Supplemental Digital Content 2, http://links.lww.com/JS9/B6. The University of California, Los Angeles and University of Michigan are the most collaborative universities, with established collaborative relationships with 38 institutions. The results showed frequent exchanges between Stanford University and Harvard Medical School, as well as among the University of California, Los Angeles, University of Michigan and University of Pittsburgh.
Documents distribution of journals, co-cited journals and co-cited references
These studies were published in 258 journals. The top ten journals were selected based on the number of documents. The numbers of citations and documents, publishing countries, and impact factors (2021) are listed in Table 1. The journal with the most documents was Surgical Endoscopy and Other Interventional Techniques, which accepted 61 documents, accounting for 7.94% of the total number, with 1959 citations. More than half of the top journals are American journals. Surgical Endoscopy and Other Interventional Techniques had the highest h-index, g-index, and m-index. Journal of Robotic Surgery had the second-highest m-index. Annals of Surgery, Journal of Minimally Invasive Gynecology, and European Urology had over 60 citations per document, with Annals of Surgery ranking first with the number of 87.77 citations per document. The impact factors of the top 10 journals are all above 2.000, with European Urology having the highest IF(24.344). Surgical Endoscopy and Other Interventional Techniques is the first journal to publish documents on the health economics of robotic surgery, while Journal of Robotic Surgery is the latest.
Table 1.
The top 10 most productive journals for health economics of robotic surgery researches.
| Journal | No. N (%) | Citation | Citation/N average citation | Country | IF (2021) | h-index | g-index | m-index | PY_start |
|---|---|---|---|---|---|---|---|---|---|
| Surgical Endoscopy and Other Interventional Techniques | 61 (7.9) | 1959 | 32.11 | USA | 3.453 | 28 | 43 | 1.4 | 2004 |
| Journal of Robotic Surgery | 37 (4.8) | 209 | 5.65 | USA | 2.484 | 8 | 13 | 1.14 | 2017 |
| Journal of Endourology | 24 (3.1) | 480 | 20.00 | USA | 2.619 | 15 | 21 | 1 | 2009 |
| Journal of Urology | 18 (2.3) | 642 | 35.67 | USA | 7.641 | 12 | 18 | 0.632 | 2005 |
| BJU International | 17 (2.2) | 768 | 45.18 | UK | 5.969 | 15 | 17 | 1.071 | 2010 |
| International Journal of Medical Robotics and Computer Assisted Surgery | 16 (2.1) | 147 | 9.19 | UK | 2.483 | 7 | 12 | 0.389 | 2006 |
| European Urology | 15 (2.0) | 1039 | 69.27 | Netherlands | 24.344 | 13 | 15 | 0.722 | 2006 |
| World Journal of Urology | 14 (1.8) | 253 | 18.07 | USA | 3.661 | 8 | 14 | 0.727 | 2013 |
| Journal of Minimally Invasive Gynecology | 13 (1.7) | 840 | 64.61 | USA | 4.314 | 13 | 13 | 0.765 | 2007 |
| Annals of Surgery | 13 (1.7) | 1141 | 87.77 | USA | 13.787 | 12 | 13 | 0.667 | 2006 |
N, number of documents; IF, impact factor; PY_start: the first year to accept relevant document.
Table 2 summarizes the top 10 most locally cited references. New technology and health care costs--the case of robot-assisted surgery published by Barbash and colleagues in 2010 was the most-cited reference, with a total of 116 citations. Eight of the most-cited 10 references were from the USA.
Table 2.
The top 10 most locally cited references and globally cited documents for health economics of robotic surgery researches.
| Rank | Reference | Local citations | Country | Doument | Total citations | Country |
|---|---|---|---|---|---|---|
| 1 | New technology and health care costs--the case of robot-assisted surgery | 116 | Israel | New Technology and Health Care Costs - The Case of Robot-Assisted Surgery | 623 | Israel |
| 2 | Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey | 90 | Switzerland | Robotically Assisted vs Laparoscopic Hysterectomy Among Women With Benign Gynecologic Disease | 368 | USA |
| 3 | Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease | 57 | USA | Laparoscopic Compared With Robotic Sacrocolpopexy for Vaginal Prolapse A Randomized Controlled Trial | 289 | USA |
| 4 | Comparative effectiveness of minimally invasive vs open radical prostatectomy | 54 | USA | Comparison of outcomes and cost for endometrial cancer staging via traditional laparotomy, standard laparoscopy and robotic techniques | 274 | USA |
| 5 | Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer | 49 | USA | Minimally Invasive Versus Open Distal Pancreatectomy (LEOPARD) A Multicenter Patient-blinded Randomized Controlled Trial | 240 | Netherlands |
| 6 | The new economics of radical prostatectomy: cost comparison of open, laparoscopic and robot assisted techniques | 46 | USA | Randomized clinical trial of robot-assisted versus standard laparoscopic right colectomy | 232 | South Korea |
| 7 | Local cost structures and the economics of robot assisted radical prostatectomy | 40 | USA | Comparison of robotically performed and traditional laparoscopic colorectal surgery | 228 | USA |
| 8 | Comparison of outcomes and cost for endometrial cancer staging via traditional laparotomy, standard laparoscopy and robotic techniques | 36 | USA | Propensity-Matched Comparison of Morbidity and Costs of Open and Robot-Assisted Radical Cystectomies: A Contemporary Population-Based Analysis in the United States | 168 | USA |
| 9 | Use, costs and comparative effectiveness of robotic assisted, laparoscopic and open urological surgery | 36 | USA | Multicenter Prospective Comparative Study of Robotic Versus Laparoscopic Gastrectomy for Gastric Adenocarcinoma | 167 | South Korea |
| 10 | Cost comparison among robotic, laparoscopic, and open hysterectomy for endometrial cancer | 34 | USA | Conventional laparoscopic and robot-assisted spleen-preserving pancreatectomy: does da Vinci have clinical advantages? | 162 | South Korea |
The top 10 most globally cited documents are listed in Table 2. New technology and health care costs--the case of robot-assisted surgery published by Barbash and colleagues in 2010 is the most-cited documents with a total of 623 citations. Five of the top 10 documents came from the United States, two from Europe, and three from South Korea.
Co-occurrence keywords analysis
The keywords from 768 studies were summarized and counted. Figure 3A shows the density visualization based on the keywords and the intensity of the hotspots with the colour spectrum. The keywords with the highest density in Figure 3A were outcomes, surgery, robotic surgery, laparoscopy, robot, cost, cancer, complications, resection, and minimally invasive surgery. Figure 3B shows the network visualization, which consists of different nodes and wires. The keywords were classified into six different groups marked by different colours. Ten manually selected clusters were marked with circles. Cluster 1, a red circle with nodes of variant colours, contains keywords shared by nine other clusters, including main subjects (robotic, laparoscopic, minimally invasive, and open surgery), measuring indices (risk, cost, perioperative outcomes, quality of life, cost-effectiveness, morbidity, complications, mortality, short-term outcomes, safety, and accuracy), and research methods (clinical trials, cohort studies, and meta-analyses) used in health economics research on robotic surgery.
Figure 3.
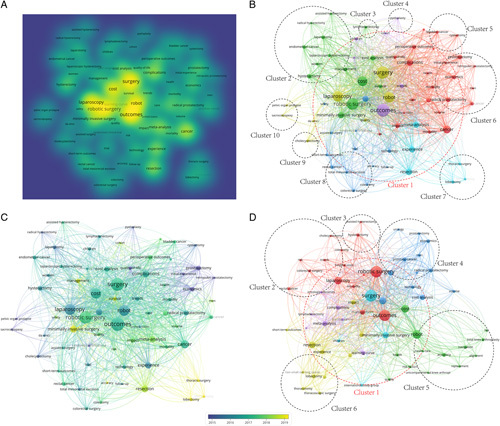
The density visualization map (A), the network map (B), and the overlay visualization map (C) of co-occurrence keywords from 2003 to 2022. The network map of co-occurrence keywords from 1 January 2021 to 31 December 2022 (D). The colours represent the time when the word appeared in (B) while representing different clusters in (C) and (D).
Clusters 2–10 cover health economic research on specific surgical disciplines, including robot-assisted hysterectomy (Cluster 2), lymphadenectomy (Cluster 3), pyeloplasty (Cluster 4), cystectomy (Cluster 5), prostatectomy (Cluster 6), thoracic surgery (Cluster 7), colon and rectum surgery (Cluster 8), cholecystectomy (Cluster 9), and sacrocolpopexy (Cluster 10).
Figure 3C shows an overlay visualization map of keywords from inception (2003) to 2022. Keywords in Cluster 7 in Figure 3B, “survival”, “accuracy”, “management, and “minimally invasive surgery” are novel keywords that emerged after 2019.
Co-occurrence keywords analysis for 2021 and 2022
Figure 3D summarizes the keywords from 2021 to 2022 in health economics studies of robotic surgery. Cluster 1 included subjects, measuring indexes, and research methods, with two novel keywords: “hospital costs” and “oncological outcomes”. Cluster 2 included robot-assisted colorectal surgeries and cholecystectomies. Cluster 3 included hysterectomy. Cluster 4 is about robot-assisted prostatectomy and has decreased in importance compared to Figure 3B). Cluster 5 covers knee arthroplasty, replacement surgery, and alignment surgery, and discusses the navigation system and accuracy. Cluster 6 included robot-assisted thoracotomy and lobectomy.
Discussion
In this paper, we presented a comprehensive bibliometric study of the health economics of robotic surgery. The results of this study shed light on the growing interest in this field, hotspots and research trends, unbalanced situation, and main research pattern, which could potentially enlighten the scholars and policy makers to make proper decisions. Futhermore, to our knowledge, this is the first bibliometric study focusing on robotic surgery health economics (Study in Context, Supplemental Digital Content 3, http://links.lww.com/JS9/B7).
In general, the development of the health economics of robotic surgery can be divided into three phases based on the number of indexed documents and citations: the slow-growing phase (2003–2009), the developing phase (2010–2018), and the fast-developing phase (2019–2022). The increasing number of indexed documents and citations annually reveals a growing interest in the field of robotic surgery health economics. The first robot was used in surgery in 198836. Since then, a plethora of advancements has been made in the field of robotic surgery, and robots have been widely adopted across many specialties after the approval of the Food and Drug Administration37. Many factors facilitate the diffusion of robotic surgery, including marketing38, ergonomic advantages39,40, and competition among hospitals41–43. As the diffusion of robotic systems expands, people start to show concern about whether robotic surgery deserves its high cost and call for more evidence to evaluate the economics of robotic surgery44. Owing to insufficient data, the FDA released a file warning about the use of surgical robots in mastectomy in 2019, which was updated in 202145. Estimated by Barbash et al.21, the additional annual healthcare cost in America brought about by the complete substitution of robotic surgery can reach more than 2.5 billion dollars. The increased attention paid to the health economics of robotic surgery is undoubtedly beneficial in solving this awkward situation. This trend is not only true globally, but is especially true in China. Since the first relevant document was published in 2011, 5 years after China imported its first Davinci surgical system in 2006, China produced 99 documents in total. Of the 99 documents, 67 were published after 2019. This may correspond to the government’s push to encourage research on robotics technology and its applications in 2018.
However, research on the health economics of robotic surgery faces an unbalanced situation. There is a huge gap between developed and developing countries in this field, as indicated by the fact that most productive institutes and authors, along with influential journals, come from developed countries. This may be the result of the insufficient financial viability of hospitals in developing countries when faced with the high price of the surgical robot system. Among the top 10 most productive countries, America is the most productive country with median average citations per document, China is the second most productive country with the lowest average citations per document, and South Korea has the highest number of citations per document, although it produces fewer documents, as indicated by Figure 2E. The US is the largest market for robotic surgery, and as local factors such as insurance and policy heavily influence the health economics of robotic surgery46,48 researchers tend to cite domestic data. This results in the US being the most productive country, with a higher number of average citations. China’s market is expanding, but its average citation number is lower, possibly because most documents are indexed after 2019 and there is a higher proportion of meta-analyses and systematic reviews. Studies in South Korea receive over 100 citations due to their large volume, multicenter nature, or initiative49–51, which raises the average number of citations despite the low total number of indexed documents.
The main research pattern in the health economics of robotic surgery is cost-effectiveness comparison among robot-assisted surgery, laparoscopic surgery, and open surgery, and cost analysis of robotic surgery in certain surgical disciplines, with clinical trials, reviews, and meta-analyses being the major research methods. This is extrapolated by the fact that the nodes in nine clusters labelled from Clusters 2 to 10, which contain the words pertaining to surgery type and some of the measuring indexes, mostly establish linkages with the nodes within its own cluster and Cluster 1, while seldom co-occurring with the nodes of other clusters. The main measuring indices encompassed in the cost-effectiveness comparison, as interpreted from Figure 3B, are cost, Intraoperative and postoperative complications, readmissions, operative time, blood loss, postoperative recovery rates, quality of life, transfusion, reoperation, length of hospital stay, mortality, length of ICU stay, infection rate, rates of positive surgical margins, etc. The dark colours of most nodes in Figure 3C suggest that studies are often repeated to obtain local or contemporary results of higher quality.
This study also identified research hotspots in this field. A comparison between Figure 3B and D shows an increase in the proportion of research on robot-assisted orthopaedic and thoracic surgeries, while the proportion of urological surgery decreases. The terms “accuracy”, “navigation”, “alignment”, and “survivorship” are receiving special attention in research. The appearance of the term “navigation” may indicate that scholars are exploring the relationship between technology and cost-effectiveness of robotic surgery.
The value of robotic surgery has not yet been examined in many areas. By searching the Web of Science core collection database with the searching strategy of “TS=((robot* AND *guid*) AND *surg*) or TS=((robot* AND *assist*) AND *surg*) or TI=(robot*AND *surg*)” and analyzing the Web of Science category, we find that robot-assisted transplant surgery, ophthalmic surgery, oral surgery and dermatologic surgery are lacking health economics researches. Future scholars are encouraged to contribute to these research areas.
Comprehensive health economics analyses, considering societal, governmental, and corporate perspectives, are crucial for understanding the health economic implications of robotic surgery. Currently, most studies on this subject are authored by doctors in the context of hospital applications. However, given the interdisciplinary nature of robotic surgery and its significant societal impact, the roles of government and commercial entities should not be overlooked. More attention should be paid to health economic analyses beyond the hospital setting. Therefore, it is important to place greater emphasis on exploring this topic from the perspectives of society, government, and corporations.
Currently, more highly qualified data are needed to analyze the health economics of robotic surgery. In light of this study, we propose suggestions to facilitate research on the health economics of robotic surgery, and we recommend that institutes in nearby regions collaborate to conduct large-volume, multicenter cohort studies or randomized trials to acquire results of high credence. For the government, it is recommended to provide coverage for robotic surgery with provisions for evidence development, which can promote an understanding of how robotic surgery is being used in real practice52,53.
Our study has several limitations. First, to ensure authenticity, only data from the Web of Science Core Collection were analyzed, which may cause deviations from reality. As the WoSCC encompasses the majority of high-quality studies, this does not significantly impact the overall trend of the results. Second, manual selection is needed to exclude documents that focus on other areas through keywords related to economics, which will bring human false to this study. However, with clear selection criteria, such bias can be effectively mitigated. The inherent limitations of bibliometric studies, such as the fact that the keywords may not accurately reflect the content of literature, cannot be avoided in this study either. In response, we conducted manual examination to better understand the meaning of the keywords and ensure their proper interpretation.
Conclusion
Our global review of publications on the health economics of robotic surgery revealed the shifting focus from the health economics of robot-assisted urological surgery to the health economics of robot-assisted orthopaedic and thoracic surgeries. A significant disparity in this field was also uncovered, highlighted by a substantial gap between developed and developing countries. There is a pressing need for further health economics analysis in the areas of robot-assisted transplant, ophthalmic, oral, and dermatologic surgeries. Moreover, it’s important to conduct health economics analysis of robotic surgery from societal, governmental, and corporate perspectives. As a suggested course of action, fostering collaboration among scholars and implementing government provisions for evidence development is recommended to enhance the understanding of the health economics associated with robotic surgery. Such efforts will contribute academically to advancing knowledge in this domain.
Ethical approval
Not applicable.
Consent
Not applicable.
Sources of funding
This work was supported by the Project of Intelligent Management Software for Multimodal Medical Big Data for New Generation Information Technology of Ministry of Industry and Information Technology of People’s Republic of China (grant No.TC210804V), as well as the Independent Exploration and Innovation Project for Postgraduate Students of Central South University (No.1053320221156).
Author contribution
K.H.: conceptualization, methodology, writing—review and editing, supervision. Y.P.: data curation, methodology, formal analysis, writing—original draft, validation, visualization. Y.L.: data curation, methodology, formal analysis, writing—original draft, validation. S.L., Z.L., L.H., J.D., X.L.: formal analysis, visualization. Y.L.: data curation, formal analysis.
Conflicts of interest disclosure
There are no conflicts of interest.
Research registration unique identifying number (UIN)
Not applicable.
Guarantor
Kai Huang.
Data statement
The data in this study are accessible in the public domain and not of a confidential nature. All the data could be contact with the corresponding author: kaiserhuang@csu.edu.cn with scientific purpose.
Provenance and peer review
Not applicable.
Supplementary Material
Acknowledgements
This work was made possible by the availability and accessibility of bibliometric software tools, Bibliometrix and VOSviewer.
Footnotes
Y.P. and Y.L. contributed equally to this work.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Supplemental Digital Content is available for this article. Direct URL citations are provided in the HTML and PDF versions of this article on the journal's website, www.lww.com/international-journal-of-surgery.
Published online 14 September 2023
Contributor Information
Yihao Peng, Email: yihao2003@csu.edu.cn.
Yuancheng Liu, Email: liuyuancheng@csu.edu.cn.
Sicen Lai, Email: Sicen2101Lai@csu.edu.cn.
Yixin Li, Email: 2204170401@csu.edu.cn.
Zexu Lin, Email: 8301210104@csu.edu.cn.
Lingjia Hao, Email: lisahao@csu.edu.cn.
Jingyi Dong, Email: 8301210102@csu.edu.cn.
Xu Li, Email: 8301210101@csu.edu.cn.
Kai Huang, Email: kaiserhuang@csu.edu.cn.
References
- 1.Calif S. Intuitive announces third quarter earnings [Internet]. 2022 [cited 2023 Jul 1]. https://isrg.intuitive.com/news-releases/news-release-details/intuitive-announces-third-quarter-earnings-2.
- 2.Calif S. Intuitive announces preliminary fourth quarter and full year 2022 results [Internet]. 2023 [cited 2023 Jul 1]. https://isrg.intuitive.com/news-releases/news-release-details/intuitive-announces-preliminary-fourth-quarter-and-full-year-2
- 3.Surgery I. Www.responsibilityreports.com [Internet]. 2022 [cited 2023 Jun30].https://www.responsibilityreports.com/HostedData/ResponsibilityReportArchive/i/NASDAQ_INTC_2021.pdf
- 4.Ji WB, Wang HG, Zhao ZM, et al. Robotic-assisted laparoscopic anatomic hepatectomy in china initial experience. Ann Surg 2011;253:342–348. [DOI] [PubMed] [Google Scholar]
- 5.Nann S, Rana A, Karatassas A, et al. Robot-assisted general surgery is safe during the learning curve: a 5-year Australian experience. J Robot Surg 2023;17:1541–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yaxley JW, Coughlin GD, Chambers SK, et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: early outcomes from a randomised controlled phase 3 study. Lancet 2016;388:1057–66. [DOI] [PubMed] [Google Scholar]
- 7.Haglind E, Carlsson S, Stranne J, et al. Urinary incontinence and erectile dysfunction after robotic versus open radical prostatectomy: a prospective, controlled, nonrandomised trial. Eur Urol 2015;68:216–225. [DOI] [PubMed] [Google Scholar]
- 8.Wright JD, Ananth CV, Lewin SN, et al. Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease. JAMA 2013;309:689–698. [DOI] [PubMed] [Google Scholar]
- 9.Lau S, Vaknin Z, Ramana-Kumar AV, et al. Outcomes and cost comparisons after introducing a robotics program for endometrial cancer surgery. Obstetr Gynecol 2012;119:717–724. [DOI] [PubMed] [Google Scholar]
- 10.Yang HX, Woo KM, Sima CS, et al. Long-term survival based on the surgical approach to lobectomy for clinical stage i nonsmall cell lung cancer comparison of robotic, video-assisted thoracic surgery, and thoracotomy lobectomy. Ann Surg 2017;265:431–437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Paul S, Jalbert J, Isaacs AJ, et al. Comparative effectiveness of robotic-assisted vs thoracoscopic lobectomy. Chest 2014;146:1505–12. [DOI] [PubMed] [Google Scholar]
- 12.Challacombe BJ, Bochner BH, Dasgupta P, et al. The role of laparoscopic and robotic cystectomy in the management of muscle-invasive bladder cancer with special emphasis on cancer control and complications. Eur Urol 2011;60:767–775. [DOI] [PubMed] [Google Scholar]
- 13.Lanfranco AR, Castellanos AE, Desai JP, et al. Robotic surgery—a current perspective. Ann Surg 2004;239:14–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.van der Sluis PC, van der Horst S, May AM, et al. Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer a randomized controlled trial. Ann Surg 2019;269:621–30. [DOI] [PubMed] [Google Scholar]
- 15.Song C, Cheng L, Li YL, et al. Systematic literature review of cost-effectiveness analyses of robotic-assisted radical prostatectomy for localised prostate cancer. BMJ Open 2022;12:e058394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ye LD, Childers CP, de Virgilio M, et al. Clinical outcomes and cost of robotic ventral hernia repair: systematic review. BJS Open 2021;5:zrab098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Krishnan G, Mintz J, Foreman A, et al. The acceptance and adoption of transoral robotic surgery in Australia and New Zealand. J Robot Surg 2019;13:301–307. [DOI] [PubMed] [Google Scholar]
- 18.Childers CP, Maggard-Gibbons M. Estimation of the acquisition and operating costs for robotic surgery. JAMA 2018;320:835–836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Paraiso MFR, Jelovsek JE, Frick A, et al. Laparoscopic compared with robotic sacrocolpopexy for vaginal prolapse a randomized controlled trial. Obstetr Gynecol 2011;118:1005–13. [DOI] [PubMed] [Google Scholar]
- 20.de Rooij T, van Hilst J, van Santvoort H, et al. Minimally invasive versus open distal pancreatectomy (LEOPARD) a multicenter patient-blinded randomized controlled trial. Ann Surg 2019;269:2–9. [DOI] [PubMed] [Google Scholar]
- 21.Barbash GI, Glied SA. New technology and health care costs—the case of robot-assisted surgery. N Engl J Med 2010;363:701–704. [DOI] [PubMed] [Google Scholar]
- 22.Mukherjee UK, Sinha KK. Robot-assisted surgical care delivery at a hospital: Policies for maximizing clinical outcome benefits and minimizing costs. J Operat Manag 2020;66:227–56. [Google Scholar]
- 23.Elliott CS, Hsieh MH, Sokol ER, et al. Robot-assisted versus open sacrocolpopexy: a cost-minimization analysis. J Urol 2012;187:638–643. [DOI] [PubMed] [Google Scholar]
- 24.Donthu N, Kumar S, Pattnaik D, et al. A bibliometric retrospection of marketing from the lens of psychology: insights from Psychology & Marketing. Psychol Market 2021;38:834–865. [Google Scholar]
- 25.Donthu N, Kumar S, Mukherjee D, et al. How to conduct a bibliometric analysis: an overview and guidelines. J Business Res 2021;133:285–96. [Google Scholar]
- 26.Shen LN, Wang SM, Dai W, et al. Detecting the interdisciplinary nature and topic hotspots of robotics in surgery: social network analysis and bibliometric study. J Med Internet Res 2019;21:e12625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Musbahi A, Rao CB, Immanuel A. A bibliometric analysis of robotic surgery from 2001 to 2021. World J Surg 2022;46:1314–1324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Fan GX, Zhou Z, Zhang HL, et al. Global scientific production of robotic surgery in medicine: a 20-year survey of research activities. Int J Surg 2016;30:126–131. [DOI] [PubMed] [Google Scholar]
- 29.Gheorghe A, Gad M, Ismail SA, et al. Capacity for health economics research and practice in Jordan, Lebanon, the occupied Palestinian territories and Turkey: needs assessment and options for development. Health Res Policy Systems 2020;18:99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Aria M, Cuccurullo C. Bibliometrix : An R-tool for comprehensive science mapping analysis. J Informetrics 2017;11:959–75. [Google Scholar]
- 31.van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for Bibliometric mapping. Scientometrics 2009;84:523–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wickham H. GGPLOT2 elegant graphics for data analysis. New York, NY, State of New York: Springer-Verlag New York; 2009. [Google Scholar]
- 33.Mao GZ, Huang N, Chen L, et al. Research on biomass energy and environment from the past to the future: a bibliometric analysis. Sci Total Environ 2018;635:1081–1090. [DOI] [PubMed] [Google Scholar]
- 34.Padilla FM, Gallardo M, Manzano-Agugliaro F. Global trends in nitrate leaching research in the 1960-2017 period. Sci Total Environ 2018;643:400–413. [DOI] [PubMed] [Google Scholar]
- 35.Gao Y, Ge L, Shi SZ, et al. Global trends and future prospects of e-waste research: a bibliometric analysis. Environ Sci Pollut Res 2019;26:17809–17820. [DOI] [PubMed] [Google Scholar]
- 36.Kwoh YS, Hou J, Jonckheere EA, et al. A robot with improved absolute positioning accuracy for CT guided stereotactic brain surgery. IEEE Trans Bio-Med Eng 1988;35:153–160. [DOI] [PubMed] [Google Scholar]
- 37.Shah J, Vyas A, Vyas D. The history of robotics in surgical specialties. Am J Robot Surg 2014;1:12–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Schiavone MB, Kuo EC, Naumann RW, et al. The commercialization of robotic surgery: unsubstantiated marketing of gynecologic surgery by hospitals. Am J Obstetr Gynecol 2012;207:174.e1–174.e1747. [DOI] [PubMed] [Google Scholar]
- 39.Lee MR, Lee GI. Does a robotic surgery approach offer optimal ergonomics to gynecologic surgeons?: a comprehensive ergonomics survey study in gynecologic robotic surgery. J Gynecol Oncol 2017;28:e70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lee EC, Rafiq A, Merrell R, et al. Ergonomics and human factors in endoscopic surgery: a comparison of manual vs telerobotic simulation systems. Surg Endosc Other Intervent Tech 2005;19:1064–1070. [DOI] [PubMed] [Google Scholar]
- 41.Wright JD, Tergas AI, Hou JY, et al. Effect of regional hospital competition and hospital financial status on the use of robotic-assisted surgery. JAMA Surg 2016;151:612–620. [DOI] [PubMed] [Google Scholar]
- 42.Sethi RKV, Henry AJ, Hevelone ND, et al. Impact of hospital market competition on endovascular aneurysm repair adoption and outcomes. J Vasc Surg 2013;58:596–606. [DOI] [PubMed] [Google Scholar]
- 43.Dor A, Koroukian S, Xu F, et al. Pricing of surgeries for colon cancer. Cancer 2012;118:5741–5748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lotan Y. Economics of robotics in urology. Curr Opin Urol 2010;20:92–97. [DOI] [PubMed] [Google Scholar]
- 45.Muhlmann G, Klaus A, Kirchmayr W, et al. DaVinci (R) robotic-assisted laparoscopic bariatric surgery: Is it justified in a routine setting? Obes Surg 2003;13:848–854. [DOI] [PubMed] [Google Scholar]
- 46.Scales CD, Jones PJ, Eisenstein EL, et al. Local cost structures and the economics of robot assisted radical prostatectomy. J Urol 2005;174:2323–2329. [DOI] [PubMed] [Google Scholar]
- 47.Menger RP, Savardekar AR, Farokhi F, et al. A cost-effectiveness analysis of the integration of robotic spine technology in spine surgery. Neurospine 2018;15:216–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Xie Y. Cost-effectiveness of robotic surgery in gynecologic oncology. Curr Opin Obstetr Gynecol 2015;27:73–76. [DOI] [PubMed] [Google Scholar]
- 49.Jeong IG, Khandwala YS, Kim JH, et al. Association of robotic-assisted vs laparoscopic radical nephrectomy with perioperative outcomes and health care costs, 2003 to 2015. JAMA 2017;318:1561–1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Park EJ, Cho MS, Baek SJ, et al. Long-term oncologic outcomes of robotic low anterior resection for rectal cancer a comparative study with laparoscopic surgery. Ann Surg 2015;261:129–137. [DOI] [PubMed] [Google Scholar]
- 51.Aria M, Cuccurullo C, et al. Bibliometrix: An R-tool for comprehensive science mapping analysis. J Informetrics. 2017;11:959–75. [Google Scholar]
- 52.van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for Bibliometric mapping. Scientometrics 2009;84:523–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Wickham H. GGPLOT2 elegant graphics for data analysis. New York, NY, State of New York: Springer-Verlag New York; 2009. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.