

Abstract
Background:
Athletes in the Winter Olympic Games are subject to high injury rates given the physical demands of sports. Comprehensive data regarding injury characteristics in these athletes are limited.
Purpose:
To summarize and analyze data regarding the incidence and characteristics of sports injuries occurring in the Winter Olympic Games.
Study Design:
Scoping review; Level of evidence, 4.
Methods:
A systematic review of the PubMed, EMBASE, Web of Science, and China National Knowledge Infrastructure databases was conducted. Included were studies reporting the incidence of sports injuries during the Winter Olympics Games from 1995 through 2021. From 168 studies initially retrieved, 4 studies (8824 athletes, 1057 injured athletes) were included. A single-group meta-analysis of sports injury characteristics was performed, with subgroup analysis performed according to the different sports, injury locations, and injury types. Injury severity (time lost from sport) and mechanism were also assessed.
Result:
The overall injury incidence rate (IIR) during the Winter Olympic Games was 9.6% (95% CI, 4.1%-19.8%). Snow sports were associated with the highest IIR (11.3%), with the top 3 events being the snowboard cross event in snowboarding (31.4%), the aerials event in freestyle skiing (28.6%), and the slopestyle event in snowboarding (27.7%). The most common injury locations were the knee (IIR = 20.0%; 95% CI 17.9%-22.0%), head (IIR = 10.6%; 95% CI, 9.4%-11.9%), and ankle (IIR = 8.2%; 95% CI 7.8%-8.7%). The most common injury types were contusion/hematoma/bruise (IIR = 29.9%; 95% CI 29.7%-30.0%), sprain (dislocation, subluxation, instability, ligamentous, rupture) (IIR = 21.9%; 95% CI 21.4%-22.3%), and strain (muscle rupture, tear, tendon rupture) (IIR = 11.3%; 95% CI 11.0%-11.6%). Regarding injury severity, most athletes had no time lost from sport (64.5%); 24.0% lost fewer than 7 days, and 11.5% lost more than 7 days. The most common injury mechanism was noncontact-related injury (63.3%).
Conclusion:
In Winter Olympics sports, snow-sport injuries were more common than those associated with other sports, and the most common injury location was the knee. Most injuries did not require time loss, and the most were noncontact-related injuries.
Keywords: injury prevention, sports injury, systematic review, Winter Olympic Games
The modern Olympics Games are considered the pinnacle of all sporting events. 29 With the rise in the number of participants, an increasing risk of musculoskeletal disorders, sports injuries, and chronic diseases may be observed in elite athletes during their careers.10,37 Because the winter Olympics sports are characterized by greater speed, higher height, and more intense competition than those associated with the summer Olympics sports, the rate of sports injuries in the Winter Olympic Games is higher than that in the Summer Olympic Games.24,32 Moreover, once injured, it is difficult for elite athletes to return to their preinjury levels, and many are forced to retire.14,34 Consequently, it is important for the International Olympic Committee (IOC) to protect athlete health and prevent sport injuries. With the increasing recognition of the characteristics of sports injuries in the Winter Olympic Games, a more reliable understanding of the injury patterns during the Olympic Games has been gained, leading to the better prevention of sport injuries in these elite athletes.18,25
We therefore believe it important to describe the trends in injury incidence, body location, injury type and severity, and mechanism to build a foundation for injury prevention and protection of athlete health. The purpose of this research was to summarize and analyze the incidence and characteristics of sports injuries occurring in the Winter Olympic Games. We hypothesized that the injury rate of snow sports would be higher and that the most common injury location would be in the lower extremity, with these injury types being contusions/hematomas/bruising with minimal time lost from sport.
Methods
Search Strategy
The current systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO), and the format and reporting of this review adhered to the reporting Meta-analyses Of Observational Studies in Epidemiology (MOOSE) guidelines. 33 A comprehensive search of the PubMed, EMBASE, Web of Science, and China National Knowledge Infrastructure databases was conducted. The search strategy included the combination of the following terms to identify relevant articles: (1) “Winter Olympic Games” OR “Olympic Winter Games” OR “Winter Olympics”, (2) “injur*” OR “pain*”, (3) “epidemiology” OR “epidemiologic” OR “epidemiological” OR “survey” OR “statistics” OR “incidence” OR “incidences”, (4) (1 AND 2 AND 3).
After removing duplicates and reprints, titles and abstracts were screened for suitability. Full-text articles were retrieved to determine inclusion or exclusion and reduce selection and recall biases. Thus, review articles, retrospective studies, single or multiple case reports, and case series were excluded.
Selection Criteria
The studies that met the following criteria were included in this review9,28,29,36:
Reported injury epidemiology in an observed sample.
Reported the rate of sports injuries in a sample investigated during the Winter Olympics, or provided sufficient data from which these figures could be calculated. No restrictions were placed on athlete age, sex, or competitive level.
Any studies that met the following criteria were excluded:
Investigated injuries in non-Winter Olympics events, such as the youth Olympics, summer Olympics, or Paralympic Games.
Conference papers, dissertation papers, review papers, case papers, and nonfull-text articles.
Reported about social science, public health, or medical services.
Included spectator and workforce injury/illness information.
Covered other games in addition to the Winter Olympic Games.
Not in English or Chinese.
The full text of articles that were eligible were retrieved and evaluated by 2 reviewers (Y.Wu and R.D.), both with a master’s degree in sports rehabilitation. Any disagreements between the reviewers were resolved by a third reviewer (Y.Wenqiang), who holds a master’s degree in sports medicine.
Assessment of Study Quality
The Critical Appraisal Skills Programme (CASP) was used to assess study quality. 42 The CASP includes 12 questions and is commonly used to assess the quality of observational studies (case-control, cohort studies, and case series). For case series, questions 7, 8, and 12, which pertain specifically to the incidence rates reported in each study, were excluded.
Data Extraction
The data extracted included study characteristics (eg, author, published year, and number of sample) and injury characteristics (eg, sport, number of sports injuries, incidence of injury, injury location, injury types, injury severity, and mechanism of injury). The reported injury rates were extracted and converted to an injury incidence rate (IIR; reported as a percentage) per 100 player-athletes using the following formula7,40:
All data were extracted using Microsoft Excel (Version 2310; Build 16.0.16924.20054). In case of any unclear or missing data, the authors of that study were contacted by email for clarification.
Statistical Analysis
Both qualitative and quantitative analyses were performed. Appropriate tables, diagrams, and effects models were constructed to analyze the Winter Olympics injury data using Review Manager Version 5.3 software (The Cochrane Collaboration), adopting single-group meta-analysis, and calculating the combined odds ratio and the 95% confidence interval. Subgroups analysis was performed according to the different sports, injury locations, and injury types.
Heterogeneity was assessed using the I2 test, which quantifies the proportion of the observed variance attributable to the variance in true effects rather than to sampling error. 4 When the I2 was <50%, heterogeneity was considered low, and the fixed-effects model was used for the meta-analysis. When the I2 was ≥50%, heterogeneity was considered high, and the random-effects model was used. If the IIR was too low, a logarithmic transformation was performed on the injury rate.
Results
Overall, 168 articles were identified using the search strategy outlined in Figure 1. After removal of duplicates and exclusion of articles based on the full-text review, 4 studies were included in the meta-analysis (Table 1).11,13,30,31
Figure 1.
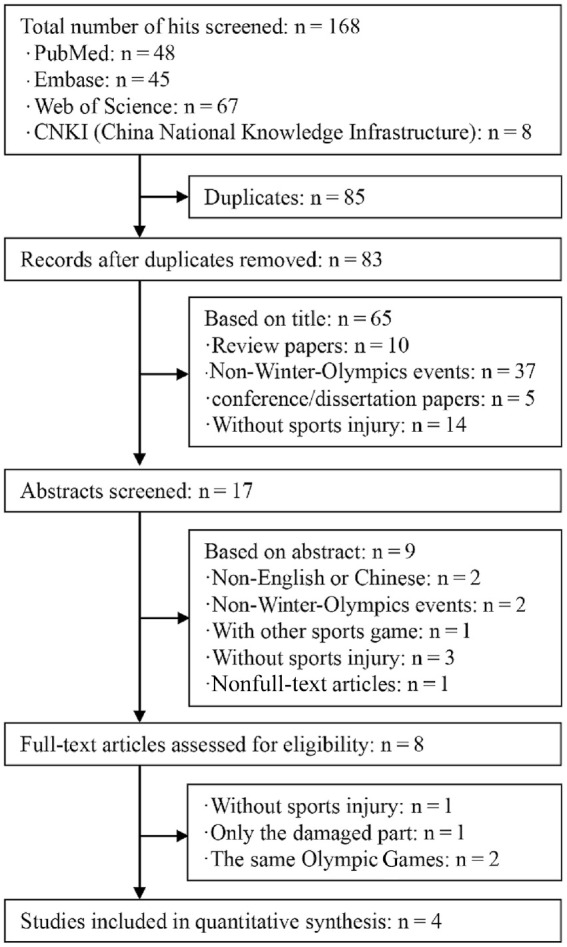
Flowchart of the process and rationale illustrating the inclusion and exclusion criteria used in the systematic review.
Table 1.
Study Characteristics
| Lead Author (Year Published) | Olympic Venue; Year | Sample Size | No. of injuries |
|---|---|---|---|
| Soligard (2019) 30 | Pyeongchang, South Korea; 2018 | 2914 | 376 |
| Soligard (2015) 31 | Sochi, Russia; 2014 | 2788 | 391 |
| Engebretsen (2010) 13 | Vancouver, Canada; 2010 | 2567 | 287 |
| Ekeland (1996) 11 | Lillehammer, Norway; 1994 | 555 | 3 |
| Total | - | 8824 | 1057 |
CASP Assessment
The results of the CASP assessment are presented in Table 2. The findings exclude questions 7, 8 and 12, which pertain specifically to the incidence rates reported in each study. The quality of the included studies was high.
Table 2.
Results of CASP Checklist for Cohort Studies a
| Study | CASP Questions b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5(A) | Q5(B) | Q6(A) | Q6(B) | Q9 | Q10 | Q11 | |
| Soligard 30 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Soligard 31 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Engebretsen 13 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ekeland 11 | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
CASP, Critical Appraisal Skills Programme.
CASP questions: Q1, Did the study address a clearly focused issue? Q2, Was the cohort recruited in an acceptable way? Q3, Was the exposure accurately measured to minimize bias? Q4, Was the outcome accurately measured to minimize bias? Q5, (A) Have the authors identified all important confounding factors? (B) Have they taken account of the confounding factors in the design and/or analysis? Q6, (A) Was the follow-up of subjects complete enough? (B) Was the follow-up of subjects long enough? Q7, What are the results of this study? Q8, How precise are the results? Q9, Do you believe the results? Q10, Can the results be applied to the local population? Q11, Do the results of this study fit with other available evidence? Q12, What are the implications of this study for practice?
Injury Incidence
The 4 included studies comprised 8824 athletes, 1057 of whom had injuries. The overall IIR in the Winter Olympics was 9.6% (95% CI, 0.82%-18.37%; I2 = 99%).
IIR According to Sport
The Winter Olympics sports were divided into ice sports (bobsled, skating, ice hockey, and curling) and snow sports (alpine skiing, freestyle skiing, snowboarding, and Nordic events); IIRs by sport are listed in Table 3. Only 1 study reported the injury rate for alpine skiing. 11 In total, the IIRs of ice sports and snow sports were 12.6% and 11.3%, respectively. The IIR for ice sports was higher than that for snow sports, although this difference was not statistically significant (P > .05). In addition, the 3 sports with the highest IIRs were snow sports: snowboard-cross in snowboarding (31.4%), aerials in freestyle skiing (28.6%), and slopestyle in snowboarding (27.7%).
Table 3.
IIR According to Sport a
| Sport | Soligard 30 | Soligard 31 | Engebretsen 13 | Ekeland 11 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Athl, n | Inj, n | Athl, n | Inj, n | Athl, n | Inj, n | Athl, n | Inj, n | Athl, n | Inj, n | IIR, % | |
| Ice sports | 1380 | 188 | 1324 | 146 | 1289 | 169 | NR | NR | 3993 | 503 | 12.6 |
| Bobsled | 323 | 45 | 326 | 45 | 314 | 37 | NR | NR | 963 | 127 | 13.2 |
| Bobsled | 163 | 28 | 171 | 31 | 159 | 32 | NR | NR | 493 | 91 | 18.5 |
| Luge | 110 | 13 | 108 | 9 | 108 | 2 | NR | NR | 326 | 24 | 7.4 |
| Skeleton | 50 | 4 | 47 | 5 | 47 | 3 | NR | NR | 144 | 12 | 8.3 |
| Skating | 450 | 55 | 432 | 37 | 431 | 46 | NR | NR | 1313 | 138 | 10.5 |
| Figure skating | 153 | 15 | 149 | 20 | 146 | 21 | NR | NR | 448 | 56 | 12.5 |
| Short-track | 113 | 17 | 106 | 9 | 109 | 20 | NR | NR | 328 | 46 | 14.0 |
| Speed skating | 184 | 23 | 177 | 8 | 176 | 5 | NR | NR | 537 | 36 | 6.7 |
| Ice hockey | 495 | 79 | 466 | 52 | 444 | 82 | NR | NR | 1405 | 213 | 15.2 |
| Curling | 112 | 9 | 100 | 12 | 100 | 4 | NR | NR | 312 | 25 | 8.0 |
| Snow sports | 1601 | 190 | 1464 | 242 | 1278 | 118 | 555 | 3 | 4898 | 553 | 11.3 |
| Alpine skiing | 322 | 57 | 314 | 65 | 308 | 46 | 555 | 3 | 1499 | 171 | 11.4 |
| Freestyle skiing | 272 | 50 | 262 | 72 | 172 | 23 | NR | NR | 706 | 145 | 20.5 |
| Aerials | 50 | 10 | 43 | 21 | 47 | 9 | NR | NR | 140 | 40 | 28.6 |
| Halfpipe | 51 | 14 | 51 | 13 | NR | NR | NR | NR | 102 | 27 | 26.5 |
| Moguls | 60 | 3 | 57 | 14 | 57 | 1 | NR | NR | 174 | 18 | 10.3 |
| Ski cross | 57 | 14 | 59 | 8 | 68 | 13 | NR | NR | 184 | 35 | 19.0 |
| Slopestyle | 54 | 9 | 52 | 16 | NR | NR | NR | NR | 106 | 25 | 23.6 |
| Snowboarding | 321 | 51 | 237 | 59 | 185 | 33 | NR | NR | 743 | 143 | 19.3 |
| Halfpipe | 54 | 8 | 66 | 12 | 69 | 9 | NR | NR | 189 | 29 | 15.3 |
| Slopestyle | 66 | 14 | 46 | 17 | NR | NR | NR | NR | 112 | 31 | 27.7 |
| Snowboard cross | 70 | 18 | 61 | 21 | 57 | 20 | NR | NR | 188 | 59 | 31.4 |
| Parallel slalom | 62 | 3 | 64 | 9 | 59 | 4 | NR | NR | 185 | 16 | 8.7 |
| Big air | 69 | 8 | NR | NR | NR | NR | NR | NR | 69 | 8 | 11.6 |
| Nordic events | 686 | 32 | 651 | 46 | 613 | 16 | NR | NR | 1950 | 94 | 4.8 |
| Biathlon | 219 | 6 | 204 | 14 | 202 | 3 | NR | NR | 625 | 23 | 3.7 |
| Cross-country | 311 | 18 | 297 | 23 | 292 | 9 | NR | NR | 900 | 50 | 5.6 |
| Nordic combined | 55 | 1 | 54 | 2 | 52 | 1 | NR | NR | 161 | 4 | 2.5 |
| Ski jumping | 101 | 7 | 96 | 7 | 67 | 3 | NR | NR | 264 | 17 | 6.4 |
| Total | 2914 | 376 | 2788 | 391 | 2567 | 287 | 555 | 3 | 8824 | 1057 | 12.0 |
Athl, athletes; Inj, injuries; IIR, injury incidence rate; NR, not reported.
IIR According to Injury Location
Among the 4 studies included, 1 reported the injury location data on just 65 athletes with severe injuries, 13 and 1 reported the injury location of only 3 athletes. 11
The total IIR for all locations in the body was 7.1% (95% CI, 2.3%-11.9%; I2 = 0%). The lower limb (IIR = 44.0%; 95% CI, 43.6%-44.3%) was the most frequently injured location. The knee was the most commonly injured part (IIR = 20.0%; 95% CI, 17.9%-22.0%). This was followed by the head (IIR = 10.6%; 95% CI, 9.4%-11.9%). The third was the ankle (IIR = 8.2%; 95% CI 7.8%-8.7%). Table 4 lists the pooled IIRs by location.
Table 4.
IIR According to Injury Location a
| Location | Soligard 30 | Soligard 31 | Engebretsen 13 | Ekeland 11 | Total IIR (95% CI) |
|---|---|---|---|---|---|
| Head and neck | 16.0 | 19.7 | 20.7 | 33.3 | 18.6 (18.2-19.1) |
| Face (including eyes, ears, nose) | 5.7 | 1.6 | 4.5 | NR | 5.3 (5.1-5.5) |
| Head | 6.3 | 18.0 | 10.5 | 33.3 | 10.6 (9.4-11.9) |
| Cervical spine/neck | 4.1 | NR | 5.6 | NR | 4.8 (4.5-5.1) |
| Trunk | 17.4 | 14.8 | 16.5 | NR | 17.0 (16.9-17.1) |
| Thoracic spine/upper back | 3.3 | 1.6 | 3.5 | NR | 3.3 (3.3-3.4) |
| Lumbar spine/lower back | 7.3 | 8.2 | 5.6 | NR | 6.8 (6.6-7.1) |
| Chest/ribs | 1.6 | 3.3 | 1.8 | NR | 1.7 (1.6-1.8) |
| Abdomen | 0.3 | NR | 1.8 | NR | 1.5 (0.7-2.2) |
| Pelvis/sacrum/buttock | 4.9 | 1.6 | 3.9 | NR | 4.5 (4.4-4.7) |
| Upper limbs | 22.0 | 16.4 | 21.4 | NR | 21.7 (21.7-21.8) |
| Shoulder/clavicle | 7.1 | 4.9 | 5.3 | NR | 6.5 (6.2-6.7) |
| Upper arm | 1.6 | NR | 1.1 | NR | 1.5 (1.3-1.7) |
| Elbow | 3.3 | 3.3 | 3.2 | NR | 3.2 (3.2-3.2) |
| Forearm | 1.6 | 1.6 | 1.1 | NR | 1.5 (1.3-1.7) |
| Wrist | NR | 3.3 | 4.9 | NR | 4.9 (4.8-4.9) |
| Hand/finger | 8.4 | 3.3 | 6.0 | NR | 7.7 (7.3-8.0) |
| Lower limbs | 44.6 | 49.2 | 41.4 | 66.7 | 44.0 (43.6-44.3) |
| Hip/groin | 6.5 | 1.6 | 4.9 | NR | 6.0 (5.8-6.2) |
| Knee | 14.4 | 41.0 | 13.7 | 33.3 | 20.0 (17.9-22.0) |
| Thigh | 4.6 | 1.6 | 7.0 | NR | 5.7 (5.3-6.1) |
| Lower leg | 3.3 | NR | 6.3 | NR | 4.9 (4.3-5.5) |
| Achilles tendon | 1.4 | 1.6 | 1.1 | NR | 1.3 (1.2-1.4) |
| Ankle | 9.2 | 1.6 | 5.6 | NR | 8.2 (7.8-8.7) |
| Foot/toe | 5.2 | 1.6 | 2.8 | 33.3 | 5.4 (3.3-7.5) |
| Total | 7.1 | 20.2 | 6.7 | 4.8 | 7.1 (2.3-11.9) |
Data are reported in percentages. IIR, injury incidence rate; NR, not reported.
IIR According to Injury Type
Two studies reported the type of injury,30,31 1 recording the injury type data on just 65 athletes with severe injuries, 13 and 1 recording nothing about the injury type. 11 Of all the injury types, contusion/hematoma/bruising was the most common (IIR = 29.9%; 95% CI, 29.7%-30.0%), followed by sprains (dislocation, subluxation, instability, ligamentous, rupture) (IIR = 21.9%, 95% CI, 21.4%-22.3%) and strains (muscle rupture, tear, tendon rupture) (IIR = 11.3%, 95% CI, 11.0%-11.6%) (Table 5).
Table 5.
IIR According to Injury Type a
| Injury Type | Soligard 30 | Soligard 31 | Engebretsen 13 | Ekeland 11 | Total IIR (95% CI) |
|---|---|---|---|---|---|
| Concussion | 4.4 | 15.9 | 7.1 | 33.3 | 6.5 (5.8-7.1) |
| Fracture (trauma, stress, other bone injuries) | 7.0 | 21.7 | 6.7 | 33.3 | 7.9 (7.3-8.5) |
| Sprain (dislocation, subluxation, instability, ligamentous, rupture) | 22.7 | 39.1 | 18.1 | 33.3 | 21.9 (21.4-22.3) |
| Strain (muscle rupture, tear, tendon rupture) | 10.2 | 5.8 | 12.8 | NR | 11.3 (11.0-11.6) |
| Meniscus, cartilage | 2.0 | NR | 1.4 | NR | 1.8 (1.6-2.0) |
| Contusion, hematoma, bruise | 31.1 | 8.7 | 28.4 | NR | 29.9 (29.7-30.0) |
| Tendinosis, tendinopathy | 0.3 | 1.4 | 5.7 | NR | 5.2 (4.4-6.0) |
| Arthritis, synovitis, bursitis | 1.2 | NR | 1.1 | NR | 1.1 (1.1-1.2) |
| Impingement | 1.7 | NR | 1.1 | NR | 1.5 (1.3-1.8) |
| Laceration, abrasion, skin lesion | 10.8 | NR | 8.9 | NR | 10.1 (9.9-10.3) |
| Dental injury, broken tooth | 1.2 | NR | 1.1 | NR | 1.1 (1.1-1.2) |
| Muscle cramps, spasm | 3.8 | 2.9 | 2.8 | NR | 3.5 (3.3-3.6) |
| Other (including nerve, spinal cord, fasciitis) | 3.8 | 4.3 | 5.0 | NR | 4.3 (4.1-4.6) |
Data are reported in percentages. IIR, injury incidence rate; NR, not reported.
Injury Severity
Injury severity was reported in 3 studies,13,30,31 while the remaining study did not explicitly describe severity. 11 The severity of injury, as per the statement, ranged from slight (no time loss from sport), minimal (1-3 days absence), mild (4-7 days absence), moderate (8-28 days absence), and severe (more than 28 days absence). 42 In this analysis, 64.5% of athletes had no time loss from sport after injury, 24.0% lost <7 days, and 11.5% lost >7 days.
Three studies reported time-loss data in different sports.13,30,31 Among the athletes with time lost to injury, the relationship between injury severity and injury rate according to sport is given in Table 6. The rate of time loss after injury in snow sports was higher than that in ice sports (65.4% vs 30.5%, P < .05), and the top 3 sports with the highest injury time loss were snowboarding (20.5%), freestyle skiing (18.9%), and alpine skiing (17.3%).
Table 6.
Injury Severity (Time Loss) According to Sport a
| Sport | Soligard 30 | Soligard 31 | Engebretsen 13 | |||
|---|---|---|---|---|---|---|
| ≥1 day | >7 days | ≥1 day | >7 days | Time Loss | Total Time Loss | |
| Ice sports | 29.0 | 4.8 | 27.2 | 13.2 | 35.4 | 30.5 |
| Bobsled | 7.3 | 1.6 | 4.0 | 1.3 | 6.2 | 5.8 |
| Bobsled | 4.8 | NR | 3.3 | 1.3 | 4.6 | 4.2 |
| Luge | 1.6 | 1.6 | 0.7 | NR | NR | 0.8 |
| Skeleton | 0.8 | NR | NR | NR | 1.5 | 0.8 |
| Skating | 10.5 | 1.6 | 6.0 | 1.3 | 4.6 | 7.0 |
| Figure skating | 1.5 | NR | 1.3 | 0.7 | NR | 0.9 |
| Short-track | 3.0 | 0.8 | 2.6 | 0.7 | 3.1 | 2.9 |
| Speed skating | 5.3 | 0.8 | 2.0 | NR | 1.5 | 2.9 |
| Ice hockey | 11.3 | 1.6 | 11.6 | 9.9 | 24.6 | 15.8 |
| Curling | NR | NR | 0.7 | 0.7 | NR | 0.2 |
| Snow sports | 71.0 | 33.9 | 71.5 | 40.4 | 53.8 | 65.4 |
| Alpine skiing | 14.3 | 6.0 | 19.2 | 7.9 | 18.5 | 17.3 |
| Freestyle skiing | 25.0 | 12.9 | 22.5 | 15.2 | 9.2 | 18.9 |
| Aerials | 1.5 | NR | 4.0 | 2.6 | 3.1 | 2.9 |
| Halfpipe | 6.5 | 3.2 | 4.0 | 2.6 | NR | 3.5 |
| Moguls | 8.1 | 4.0 | 6.6 | 3.3 | 1.5 | 5.4 |
| Ski cross | 6.5 | 4.8 | 4.0 | 4.0 | 4.6 | 5.0 |
| Slopestyle | 2.4 | 0.8 | 4.0 | 2.6 | NR | 2.1 |
| Snowboarding | 25.0 | 14.5 | 17.9 | 11.3 | 18.5 | 20.5 |
| Halfpipe | 2.4 | 0.8 | 2.0 | 1.3 | 3.1 | 2.5 |
| Slopestyle | 7.3 | 4.8 | 7.9 | 3.3 | NR | 5.1 |
| Snowboard cross | 9.7 | 7.3 | 6.6 | 5.3 | 12.3 | 9.5 |
| Parallel slalom | 1.6 | NR | 1.3 | 1.3 | 3.1 | 2.0 |
| Big air | 4.0 | 1.6 | NR | NR | NR | 1.3 |
| Nordic events | 5.6 | NR | 11.9 | 6.0 | 7.7 | 8.4 |
| Biathlon | 0.8 | NR | 3.3 | 1.3 | 1.5 | 1.9 |
| Cross-country | 2.4 | NR | 4.6 | 2.0 | 3.1 | 3.4 |
| Nordic combined | NR | NR | 1.3 | 1.3 | NR | 0.4 |
| Ski jumping | 2.4 | NR | 2.6 | 1.3 | 3.1 | 2.7 |
Data are reported in percentages. NR, not reported.
Injury Mechanism
Three studies described the injury mechanism,13,30,31 classified as contact or noncontact. One study described only contact and noncontact injury rates. 11 The most common reported injury mechanism was noncontact injury (IIR = 63.6%; 95% CI, 62.9%-64.4%).
Discussion
The principal findings were that the overall incidence of injury during the Winter Olympic Games was 9.6%; the top 3 injury incidences were snowboard cross of snowboarding (31.4%), aerials of freestyle skiing (28.6%), and slopestyle of snowboarding (27.7%); the most common injury locations were the knees (20.0%); the most injuries were slight without time loss (64.5%); and the most were noncontact-related injuries (63.3%). This is the first systematic review to evaluate the characteristics of sports injuries of Winter Olympic Games athletes. This systematic review and meta-analysis aimed to investigate the prevalence, incidence, and profile of injuries, including sports with the highest number of injuries, as well as the body location, type of injury, severity of injury, and mechanism of injury in athletes.
Injury Incidence
Our findings showed that the incidence of injury in Winter Olympic Games athletes was 9.6%. The overall injury rate throughout the Summer and Winter Olympic Games has remained fairly constant. The injury rates in Tokyo 2020, Rio de Janeiro 2016, London 2012, and Beijing 2008 were 9.1, 9.8, 11, and 9.6 per 100 athletes, respectively.12,19,32 The rates in the recent Paralympic Winter Olympic Games were higher than those at the Winter Olympic games, at 19.8 and 23.8 per 100 athletes in Pyeongchang 2018 and Vancouver 2010.7,28,39 This might have been due to a number of reasons. First, Olympic sports have the characteristics of requiring greater speeds, greater heights, and more intense competition than recreational sports. Second, the Olympic Games require higher physical fitness, and Paralympians find it more difficult to complete the sport and are more susceptible to injury. Third, the injury incidence may experience incidental variation as a result of factors such as the events included in the Olympic Games (eg, any new sports added), environmental factors, venue or track design, competition rules or changes in equipment, the manner of information recording, athlete awareness of injury protection, and the capability of medical services of transportation and treatment for injured athletes.5,20,38
Injury Rates in Different Sports
Our hypothesis, that the injury rate of snow sports would be higher, was partially supported. Our results showed that the difference in IIR in ice-sports and snow sports was not significant, and the top 3 sports in terms of injury rates were snow sports, snowboard cross of snowboarding, aerials of freestyle skiing, and slopestyle of snowboarding. Some studies have identified a large variation among these different sports. The IOC Medical Commission had defined freestyle skiing and snowboard, super-G, speed skating, short-track, and ice hockey as high-risk sporting events. 3 Moreover, the International Ski Federation (FIS) World Cup reported snowboard cross and halfpipe, aerial and halfpipe skiing, and ski cross as having higher rates of injury.15,35 The main reason for this high injury rate is that the sports involve more extreme performance and snow constructions. 35 Furthermore, the combination of speed and jumps seen in freestyle skiing and snowboarding may promote a risk-taking attitude for participants to stay at the top of their sport performance. In particular, jumping is the essence of the sport, and the judging criteria reward height and rotation.16,21 Previous studies reported that the injury risk was lower among Nordic skiing athletes than that among alpine, freestyle, and snowboard athletes, as they are not exposed to icy surfaces, high speed, or spectacular jumps.16,17,41 However, some studies have reported that athletes in every sport have the same risk of injury.1,18
Injury Location
Our hypothesis that the most common injury location would be the lower extremity was largely supported. Our study showed that the knee, head, and ankle were the body parts injured most frequently among Winter Olympics athletes. Winter Olympics sports involve jumping and rotating movements at high speed. Especially when snow-sports athletes perform aerial maneuvers, they risk damaging their knee joints. Studies have shown that jumping promotes knee injuries in professional snowboarders.2,22 Like ours, several studies have identified the knee as the most common site of injury.26,27 Head injuries are reportedly frequent, while some studies have also identified head injuries as the second-most common injury location.6,41 Although the FIS International Competition rules state that a helmet should be worn specifically for snowboarding or ski racing, the rate of injury to the head is high, especially during training.8,35 The ankle is another area with a high injury rate.19,23 Ankle sprain was a common prevalent diagnosis in sports injury 19 ; this may be related to the jumping and lower limb stabilizing movements. This predisposes the ankle to injury. In many cases, knee, head, and ankle injuries result in long absence from training and competition. Thus, it is important for athletes to prevent sports injury.
Injury Type, Severity, and Mechanism
Our hypothesis that contusion/hematoma/bruising would be the more common injury types was supported. Our findings indicated that the most common injury type was contusion/hematoma/bruising, sprain (dislocation, subluxation, instability, ligamentous, rupture), and strain (muscle rupture, tear, tendon rupture). This may be related to the movements performed during these sports, many of which involve torsional and shear force at high speed. Moreover, injury rate is influenced by factors such as the field conditions, weather, and temperature.
Our hypothesis that most injuries would be associated with minimal time lost from sport was not supported. Our results indicated that the most common injury severity was slight. Our findings also indicated that most athletes would not lose time from sports after injury. However, all injuries, even those of minor severity without time loss, have the potential to be both participation-limiting and performance-inhibiting, and thus prevent athletes from possibly fulfilling their potential performance. The injury mechanism can affect the type and severity of the injury. Our study showed that most of the injuries were noncontact. This may because many athletes sustain chronic injury and are at a higher risk of injury. However, the type, severity, and mechanism of injuries in competition differed between different sports. Information regarding the injury severity, type, and mechanism are essential for setting targets for preventive, therapeutic, and rehabilitative strategies.
Limitations
This study has several limitations. First, the low number of studies included in the meta-analytic review limits the generalizability of our results. The varying injury definitions, duration of data collection, and methodological, language differences as well as the same Olympic games in different studies resulted in only 4 studies being suitable. Furthermore, some included studies did not provide all of the detailed information used to calculate these figures, such as the number of injuries and exposures by sex, the injury location and type in different sports, or the injury severity in different periods. At the same time, these injuries may be under-reported, because the athlete may not want to reveal injury for fear of being not cleared to compete. Finally, there was no subgroup of injury characteristics by sex and sport.
Suggestions and Future Directions
We hope that the results of this study can help to provide data required for the development, application, and assessment of injury causation and prevention models. The IOC, National Olympic Committee, and International Sports Federation should strengthen the monitoring and protection of athletes to reduce the incidence of injuries. For example, researching the precise biomechanical factors involved in the injury mechanism and movement technology in large-scale competitions can help provide evidence-based injury prevention measures to every athlete. The comprehensive capacity of medical services needs to be enhanced to improve the professional quality of medical personnel, intervene with early rehabilitation, promote mental health, and improve the level of services. Future research should be combined with virtual simulation technology to explore whether adding virtual simulation training can reduce the injury incidence in difficult movements. At the same time, such advancements could also be adopted to benefit the general population.
Conclusion
Snow-sports injuries were the most common in the Winter Olympic Games, and the 3 sports with the highest IIRs were snowboard cross of snowboarding, aerials of freestyle skiing, and slopestyle of snowboarding. The most common injury locations were the knee, head, and ankle. The most common injury types were contusion/hematoma/bruising, sprain, and strain. Most injuries were slight without time loss from sport, and the most were noncontact-related injuries. Our results can inform both the planning and provision of health care, prevention, treatment, and rehabilitation for athletes in Winter Olympics sports.
Footnotes
Final revision submitted May 17, 2023; accepted June 2, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: this study was granted by the research fund of the National Science and Technology Winter Olympics Special Project (21110006D), and Tianjin Research Innovation Project for Postgraduate Student (2021YJSB376). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
- 1. Bere T, Florenes TW, Nordsletten L, Bahr R. Sex differences in the risk of injury in World Cup alpine skiers: a 6-year cohort study. Br J Sports Med. 2014;48(1):36-40. [DOI] [PubMed] [Google Scholar]
- 2. Bladin C, McCrory P. Snowboarding injuries. An overview. Sports Med. 1995;19(5):358-364. [DOI] [PubMed] [Google Scholar]
- 3. Blank C, Schamasch P, Engebretsen L, et al. Medical services at the first Winter Youth Olympic Games 2012 in Innsbruck/Austria. Br J Sports Med. 2012;46(15):1048-1054. [DOI] [PubMed] [Google Scholar]
- 4. Borenstein M. Research Note: In a meta-analysis, the I2 index does not tell us how much the effect size varies across studies. J Physiother. 2020;66(2):135-139. [DOI] [PubMed] [Google Scholar]
- 5. Brennan RJ, Keim ME, Sharp TW, et al. Medical and public health services at the 1996 Atlanta Olympic Games: an overview. Med J Aust. 1997;167(11-12):595-598. [DOI] [PubMed] [Google Scholar]
- 6. Chaze B, McDonald P. Head injuries in winter sports: downhill skiing, snowboarding, sledding, snowmobiling, ice skating and ice hockey. Neurol Clin. 2008;26(1):325-332; xii-xiii. [DOI] [PubMed] [Google Scholar]
- 7. Derman W, Runciman P, Jordaan E, et al. High incidence of injuries at the Pyeongchang 2018 Paralympic Winter Games: a prospective cohort study of 6804 athlete days. Br J Sports Med. 2020;54(1):38-43. [DOI] [PubMed] [Google Scholar]
- 8. Dickson TJ, Terwiel FA. Head injury and helmet usage trends for alpine skiers and snowboarders in western Canada during the decade 2008-9 to 2017-18. J Sci Med Sport. 2021;24(10):1004-1009. [DOI] [PubMed] [Google Scholar]
- 9. Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44(1):123-140. [DOI] [PubMed] [Google Scholar]
- 10. Drawer S, Fuller CW. Evaluating the level of injury in English professional football using a risk based assessment process. Br J Sports Med. 2002;36(6):446-451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Ekeland A, Dimmen S, Lystad H, Aune AK. Completion rates and injuries in alpine races during the 1994 Olympic Winter Games. Scand J Med Sci Sports. 1996;6(5):287-290. [DOI] [PubMed] [Google Scholar]
- 12. Engebretsen L, Soligard T, Steffen K, et al. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br J Sports Med. 2013;47(7):407-414. [DOI] [PubMed] [Google Scholar]
- 13. Engebretsen L, Steffen K, Alonso JM, et al. Sports injuries and illnesses during the Winter Olympic Games 2010. Br J Sports Med. 2010;44(11):772-780. [DOI] [PubMed] [Google Scholar]
- 14. Fjellman-Wiklund A, Söderman K, Lundqvist M, Häger CK. Retrospective experiences of individuals two decades after anterior cruciate ligament injury - a process of re-orientation towards acceptance. Disabil Rehabil. 2022;44(21):6267-6276. [DOI] [PubMed] [Google Scholar]
- 15. Florenes TW, Heir S, Nordsletten L, Bahr R. Injuries among World Cup freestyle skiers. Br J Sports Med. 2010;44(11):803-808. [DOI] [PubMed] [Google Scholar]
- 16. Florenes TW, Nordsletten L, Heir S, Bahr R. Injuries among World Cup ski and snowboard athletes. Scand J Med Sci Sports. 2012;22(1):58-66. [DOI] [PubMed] [Google Scholar]
- 17. Frick B, Moser K. Are women really less competitive than men? Career duration in Nordic and alpine skiing. Front Sociol. 2020;5:539766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Junge A, Engebretsen L, Alonso JM, et al. Injury surveillance in multi-sport events: the International Olympic Committee approach. Br J Sports Med. 2008;42(6):413-421. [DOI] [PubMed] [Google Scholar]
- 19. Junge A, Engebretsen L, Mountjoy ML, et al. Sports injuries during the Summer Olympic Games 2008. Am J Sports Med. 2009;37(11):2165-2172. [DOI] [PubMed] [Google Scholar]
- 20. Kennedy MI, Moatshe G, Engebretsen L. Global forum: orthopaedic physicians in the Winter and Summer Olympic Games. J Bone Joint Surg Am. 2020;102(11):e52. [DOI] [PubMed] [Google Scholar]
- 21. Machold W, Kwasny O, Gässler P, et al. Risk of injury through snowboarding. J Trauma. 2000;48(6):1109-1114. [DOI] [PubMed] [Google Scholar]
- 22. Matsumoto K, Miyamoto K, Sumi H, Sumi Y, Shimizu K. Upper extremity injuries in snowboarding and skiing: a comparative study. Clin J Sport Med. 2002;12(6):354-359. [DOI] [PubMed] [Google Scholar]
- 23. Nabhan D, Walden T, Street J, Linden H, Moreau B. Sports injury and illness epidemiology during the 2014 Youth Olympic Games: United States Olympic team surveillance. Br J Sports Med. 2016;50(11):688-693. [DOI] [PubMed] [Google Scholar]
- 24. Nabhan D, Windt J, Taylor D, Moreau W. Close encounters of the US kind: illness and injury among US athletes at the PyeongChang 2018 Winter Olympic Games. Br J Sports Med. 2020;54(16):997-1002. [DOI] [PubMed] [Google Scholar]
- 25. Palmer-Green D, Elliott N. Sports injury and illness epidemiology: Great Britain Olympic Team (TeamGB) surveillance during the Sochi 2014 Winter Olympic Games. Br J Sports Med. 2015;49(1):25-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Palmer D, Cooper DJ, Emery C, et al. Self-reported sports injuries and later-life health status in 3357 retired Olympians from 131 countries: a cross-sectional survey among those competing in the games between London 1948 and PyeongChang 2018. Br J Sports Med. 2021;55(1):46-53. [DOI] [PubMed] [Google Scholar]
- 27. Palmer D, Engebretsen L, Carrard J, et al. Sports injuries and illnesses at the Lausanne 2020 Youth Olympic Winter Games: a prospective study of 1783 athletes from 79 countries. Br J Sports Med. 2021;55(17):968-974. [DOI] [PubMed] [Google Scholar]
- 28. Pinheiro LSP, Ocarino JM, Madaleno FO, et al. Prevalence and incidence of injuries in para athletes: a systematic review with meta-analysis and GRADE recommendations. Br J Sports Med. 2021;55(23):1357-1365. [DOI] [PubMed] [Google Scholar]
- 29. Sharma S, Dhillon MS, Kumar P, Rajnish RK. Patterns and trends of foot and ankle injuries in Olympic athletes: a systematic review and meta-analysis. Indian J Orthop. 2020;54(3):294-307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Soligard T, Palmer D, Steffen K, et al. Sports injury and illness incidence in the PyeongChang 2018 Olympic Winter Games: a prospective study of 2914 athletes from 92 countries. Br J Sports Med. 2019;53(17):1085-1092. [DOI] [PubMed] [Google Scholar]
- 31. Soligard T, Steffen K, Palmer-Green D, et al. Sports injuries and illnesses in the Sochi 2014 Olympic Winter Games. Br J Sports Med. 2015;49(7):441-447. [DOI] [PubMed] [Google Scholar]
- 32. Soligard T, Steffen K, Palmer D, et al. Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic Summer Games: a prospective study of 11274 athletes from 207 countries. Br J Sports Med. 2017;51(17):1265-1271. [DOI] [PubMed] [Google Scholar]
- 33. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008-2012. [DOI] [PubMed] [Google Scholar]
- 34. Tito N, Porter E, Castonguay T, Dover G. Longitudinal validation of a specific measure of fear avoidance in athletes: predicting time from injury to return to sports competition. J Pain Res. 2023;16:1103-1114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Torjussen J, Bahr R. Injuries among elite snowboarders (FIS Snowboard World Cup). Br J Sports Med. 2006;40(3):230-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Vaishya R, Kambhampati SBS, Vaish A. Meniscal injuries in the Olympic and elite athletes. Indian J Orthop. 2020;54(3):281-293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: a study of radiographic and patient relevant outcomes. Ann Rheum Dis. 2004;63(3):269-273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Watanabe K, Akama T, Asakawa S, et al. Medical services at the 2017 Sapporo Asian winter games: injury and illness epidemiology at a 34-nation multisport event. Br J Sports Med. 2019;53(1):32-36. [DOI] [PubMed] [Google Scholar]
- 39. Webborn N WS, Emery CA. The injury experience at the 2010 Winter Paralympic Games. Clin J Sport Med. 2012;22(1):3-9. [DOI] [PubMed] [Google Scholar]
- 40. Williams S, Trewartha G, Kemp S, Stokes K. A meta-analysis of injuries in senior men’s professional Rugby Union. Sports Med. 2013;43(10):1043-1055. [DOI] [PubMed] [Google Scholar]
- 41. Xu Y, Yang C, Yang Y, et al. A narrative review of injury incidence, location, and injury factor of elite athletes in snowsport events. Front Physiol. 2020;11:589983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Yeomans C, Kenny IC, Cahalan R, et al. The incidence of injury in amateur male Rugby Union: a systematic review and meta-analysis. Sports Med. 2018;48(4):837-848. [DOI] [PMC free article] [PubMed] [Google Scholar]