

Abstract
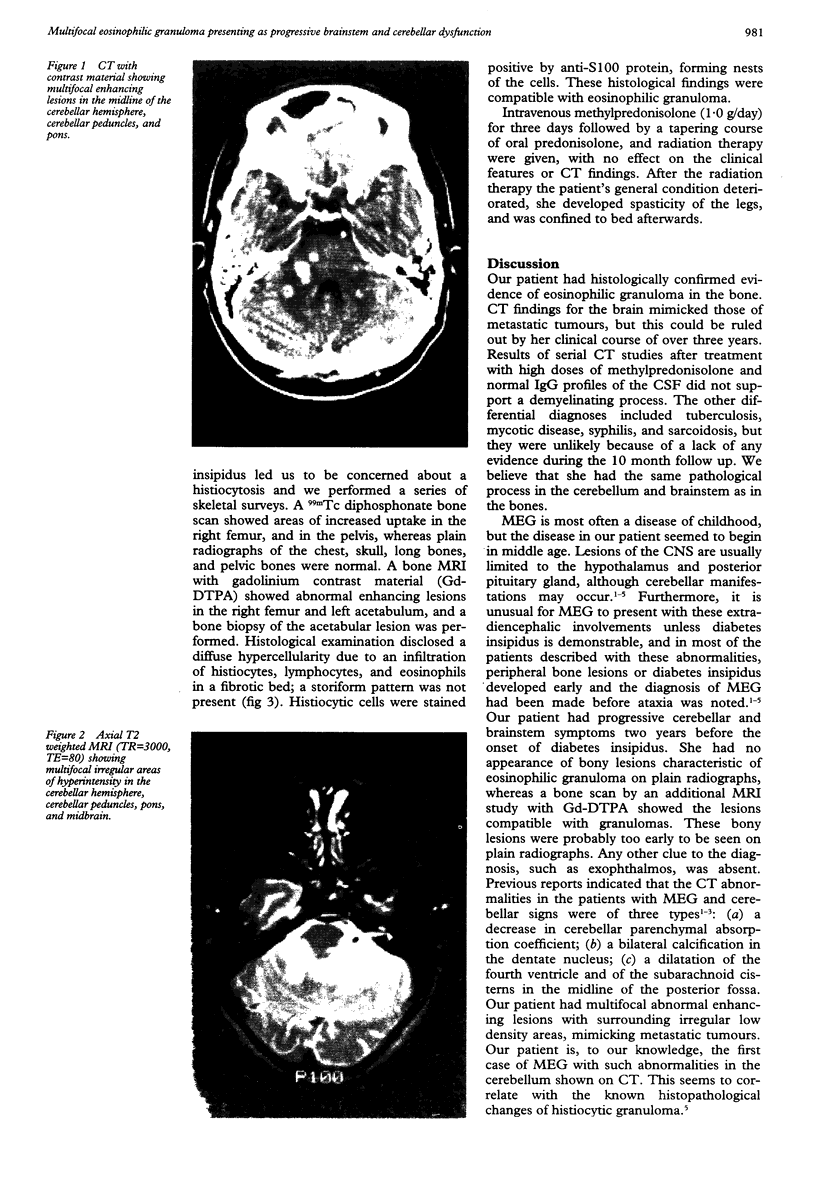
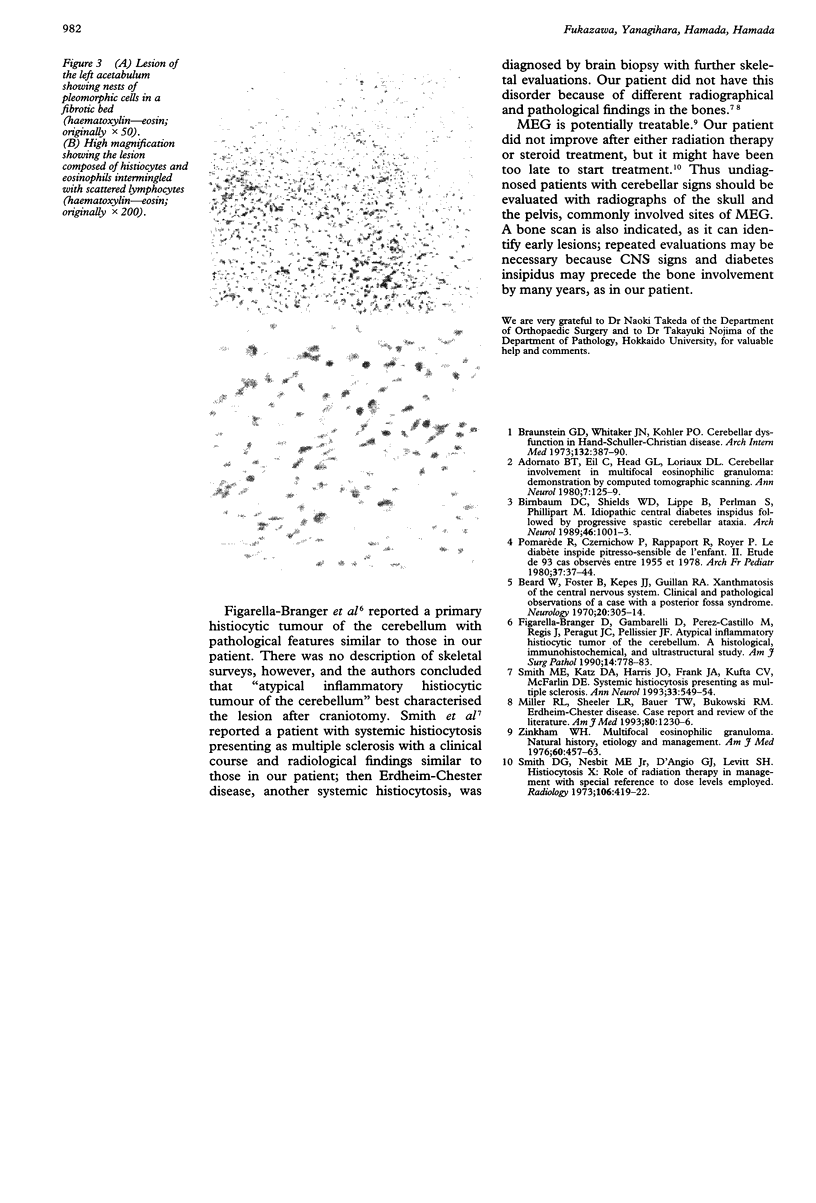
A 55 year old woman with multifocal eosinophilic granuloma (MEG) is described. She developed facial numbness and twitching followed by slowly progressive cerebellar symptoms. Two years later polyuria and polydipsia were noted. A CT of the brain showed multifocal enhancing lesions, and MRI showed areas of hyperintensity on T2 weighted studies in the cerebellar peduncles, pons, and midbrain. Radiographs of the skull, pelvis, and long bones were normal, but a 99mTc diphosphonate bone scan and MRI showed bone lesions compatible with granuloma. The diagnosis of MEG was made by bone biopsy. This is believed to be the first case of MEG with such unusual clinical profiles and radiographical findings. Skeletal surveys are indicated for patients with unexplained focal or multifocal inflammatory changes in the cerebellum.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adornato B. T., Eil C., Head G. L., Loriaux D. L. Cerebellar involvement in multifocal eosinophilic granuloma: demonstration by computerized tomographic scanning. Ann Neurol. 1980 Feb;7(2):125–129. doi: 10.1002/ana.410070206. [DOI] [PubMed] [Google Scholar]
- Beard W., Foster D. B., Kepes J. J., Guillan R. A. Xanthomatosis of the central nervous system. Clinical and pathological observations of a case with a posterior fossa syndrome. Neurology. 1970 Apr;20(4):305–314. doi: 10.1212/wnl.20.4.305. [DOI] [PubMed] [Google Scholar]
- Birnbaum D. C., Shields D., Lippe B., Perlman S., Phillipart M. Idiopathic central diabetes insipidus followed by progressive spastic cerebral ataxia. Report of four cases. Arch Neurol. 1989 Sep;46(9):1001–1003. doi: 10.1001/archneur.1989.00520450071022. [DOI] [PubMed] [Google Scholar]
- Braunstein G. D., Whitaker J. N., Kohler P. O. Cerebellar dysfunction in Hand-Schueller-Christian disease. Arch Intern Med. 1973 Sep;132(3):387–390. [PubMed] [Google Scholar]
- Figarella-Branger D., Gambarelli D., Perez-Castillo M., Regis J., Peragut J. C., Pellissier J. F. Atypical inflammatory histiocytic tumor of the cerebellum. A histological, immunohistochemical, and ultrastructural study. Am J Surg Pathol. 1990 Aug;14(8):778–783. doi: 10.1097/00000478-199008000-00010. [DOI] [PubMed] [Google Scholar]
- Smith D. G., Nesbit M. E., Jr, D'Angio G. J., Levitt S. H. Histiocytosis X: role of radiation therapy in management with special reference to dose levels employed. Radiology. 1973 Feb;106(2):419–422. doi: 10.1148/106.2.419. [DOI] [PubMed] [Google Scholar]
- Smith M. E., Katz D. A., Harris J. O., Frank J. A., Kufta C. V., McFarlin D. E. Systemic histiocytosis presenting as multiple sclerosis. Ann Neurol. 1993 May;33(5):549–554. doi: 10.1002/ana.410330521. [DOI] [PubMed] [Google Scholar]