

Abstract
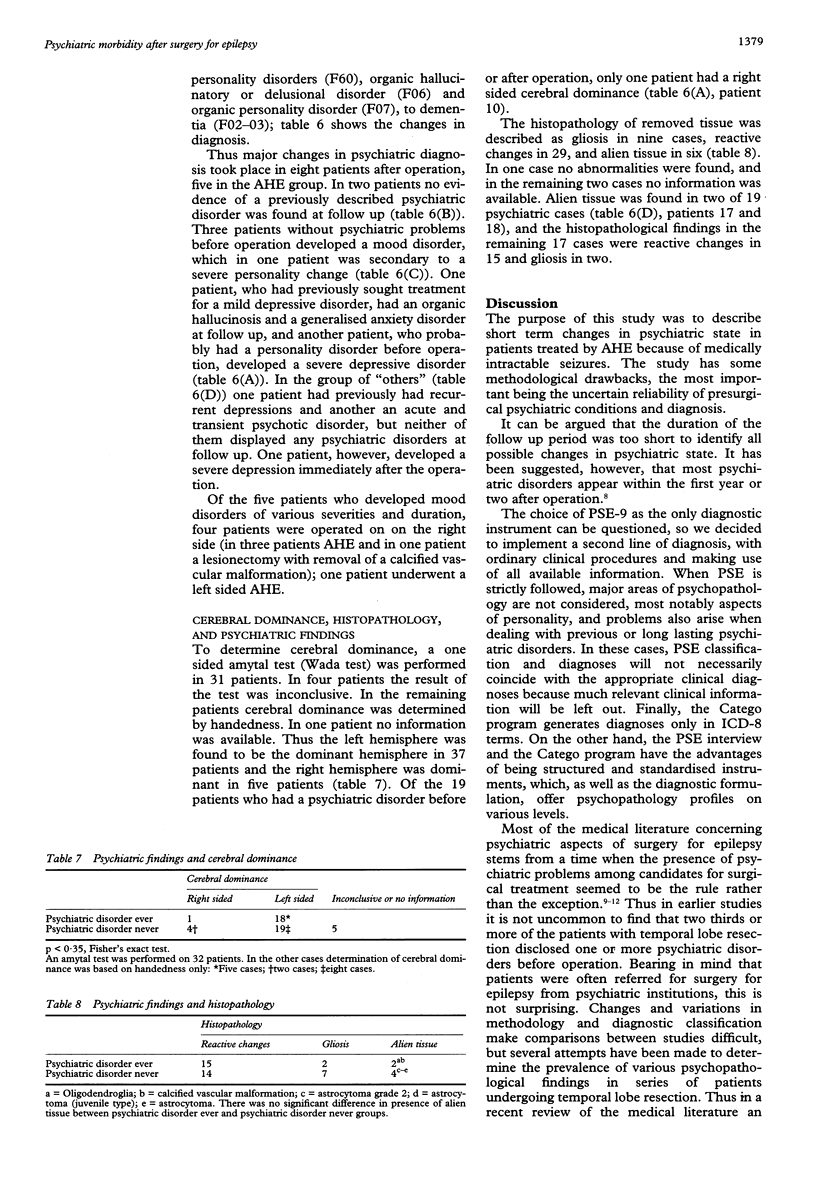
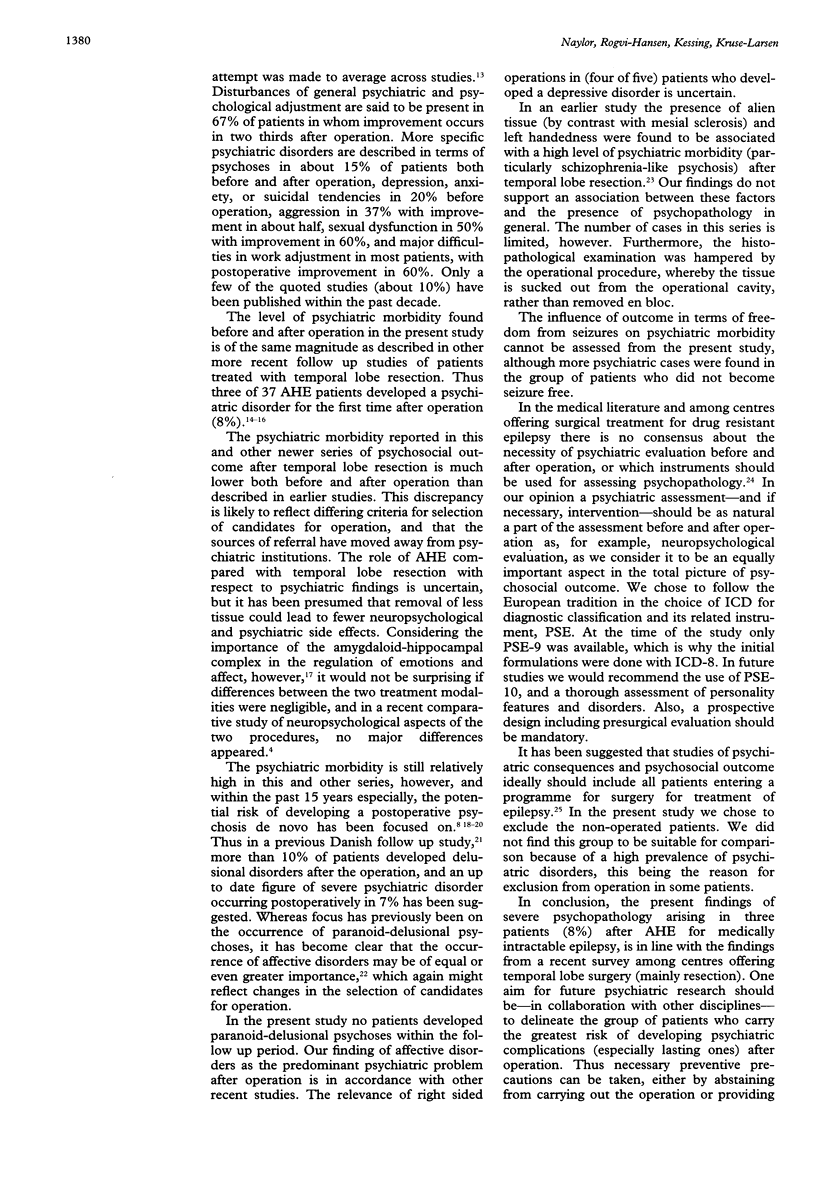
The aim was to assess the occurrence and type of psychiatric disorders of patients with medically intractable epilepsy in relation to surgical treatment, with special reference to amygdalohippocampectomy (AHE). The design was a retrospective psychiatric interview study, including Present State Examination (PSE) and diagnostic classification according to the International Classification of Diseases--8th revision (ICD-8) and ICD-10. Forty seven (94% of total) patients operated on between 1987 and mid-1991 in the Danish epilepsy surgery programme were studied. The main group of interest included 37 patients treated by AHE. The presence of psychiatric disorders before and after operation was assessed by PSE (including the Catego classification) and by ordinary clinical procedures, making use of all available information (hospital case notes and presurgical psychiatric assessments independent of the study). Four patients in the AHE group developed depressive disorders of various durations and severity after operation (in three (8%) patients these occurred de novo). One other patient with AHE with a presumed personality disorder who underwent AHE developed a severe depression, as did one patient after a lesionectomy. No patients developed new paranoid hallucinatory psychoses. No association was found between presence of psychiatric disorders and neither right sided cerebral dominance nor histopathological findings. In conclusion, the postoperative psychiatric morbidity in this sample of patients treated with AHE is of the same magnitude as described in recent series of patients undergoing temporal lobe resection for medically intractable epilepsy. Likewise, affective disorders (depressive conditions) constitute the most prominent psychiatric problem after surgery for epilepsy.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Fenwich P. B., Fenwick P. B. Psychiatric assessment and temporal lobectomy. Acta Neurol Scand Suppl. 1988;117:96–102. doi: 10.1111/j.1600-0404.1988.tb08010.x. [DOI] [PubMed] [Google Scholar]
- Goldstein L. H., Polkey C. E. Short-term cognitive changes after unilateral temporal lobectomy or unilateral amygdalo-hippocampectomy for the relief of temporal lobe epilepsy. J Neurol Neurosurg Psychiatry. 1993 Feb;56(2):135–140. doi: 10.1136/jnnp.56.2.135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jensen I., Larsen J. K. Mental aspects of temporal lobe epilepsy. Follow-up of 74 patients after resection of a temporal lobe. J Neurol Neurosurg Psychiatry. 1979 Mar;42(3):256–265. doi: 10.1136/jnnp.42.3.256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jensen I., Larsen J. K. Psychoses in drug-resistant temporal lobe epilepsy. J Neurol Neurosurg Psychiatry. 1979 Oct;42(10):948–954. doi: 10.1136/jnnp.42.10.948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koch-Weser M., Garron D. C., Gilley D. W., Bergen D., Bleck T. P., Morrell F., Ristanovic R., Whisler W. W., Jr Prevalence of psychologic disorders after surgical treatment of seizures. Arch Neurol. 1988 Dec;45(12):1308–1311. doi: 10.1001/archneur.1988.00520360026006. [DOI] [PubMed] [Google Scholar]
- Mace C. J., Trimble M. R. Psychosis following temporal lobe surgery: a report of six cases. J Neurol Neurosurg Psychiatry. 1991 Jul;54(7):639–644. doi: 10.1136/jnnp.54.7.639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevens J. R. Psychiatric consequences of temporal lobectomy for intractable seizures: a 20-30-year follow-up of 14 cases. Psychol Med. 1990 Aug;20(3):529–545. doi: 10.1017/s0033291700017049. [DOI] [PubMed] [Google Scholar]
- Taylor D. C. Aggression and epilepsy. J Psychosom Res. 1969 Sep;13(3):229–236. doi: 10.1016/0022-3999(69)90040-3. [DOI] [PubMed] [Google Scholar]
- Taylor D. C. Mental state and temporal lobe epilepsy. A correlative account of 100 patients treated surgically. Epilepsia. 1972 Dec;13(6):727–765. doi: 10.1111/j.1528-1157.1972.tb05160.x. [DOI] [PubMed] [Google Scholar]
- Trimble M. R. Behaviour changes following temporal lobectomy, with special reference to psychosis. J Neurol Neurosurg Psychiatry. 1992 Feb;55(2):89–91. doi: 10.1136/jnnp.55.2.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wieser H. G. Selective amygdalo-hippocampectomy for temporal lobe epilepsy. Epilepsia. 1988;29 (Suppl 2):S100–S113. doi: 10.1111/j.1528-1157.1988.tb05793.x. [DOI] [PubMed] [Google Scholar]
- Wieser H. G. Selective amygdalohippocampectomy: indications, investigative technique and results. Adv Tech Stand Neurosurg. 1986;13:39–133. doi: 10.1007/978-3-7091-7010-6_2. [DOI] [PubMed] [Google Scholar]