

Abstract
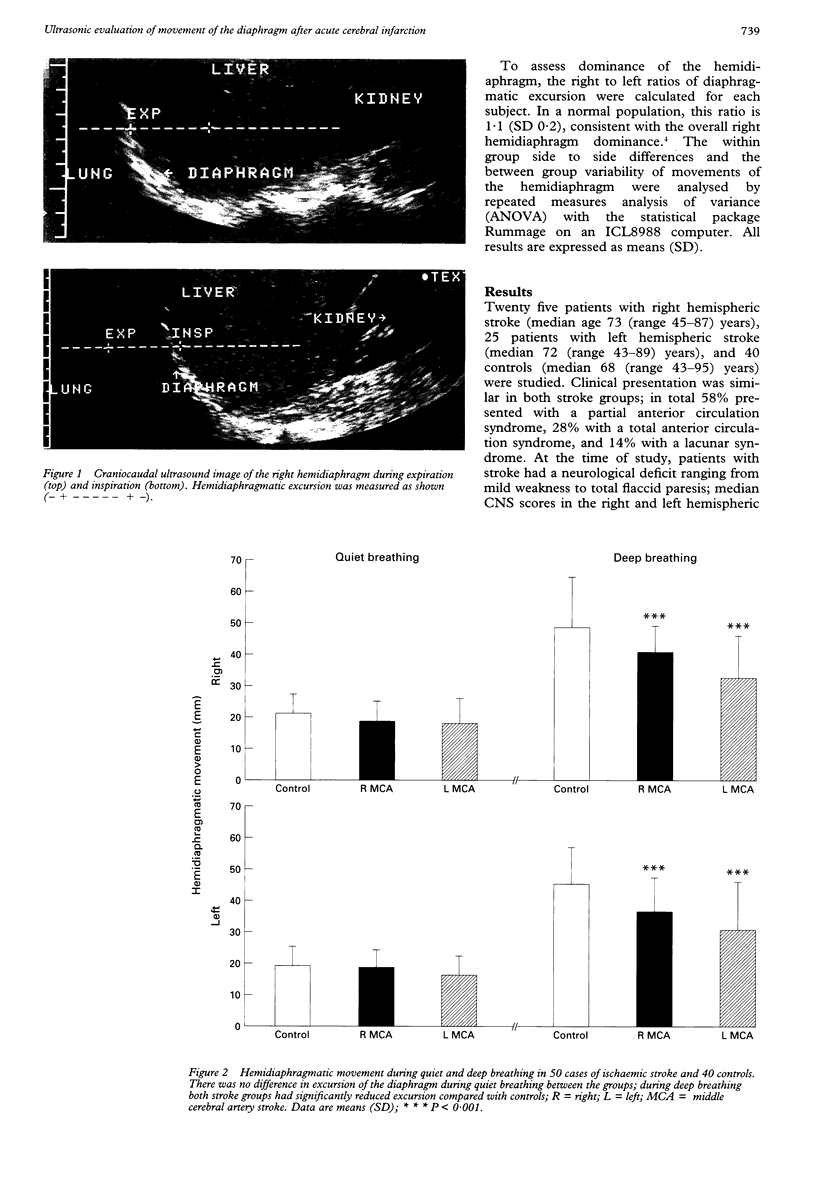
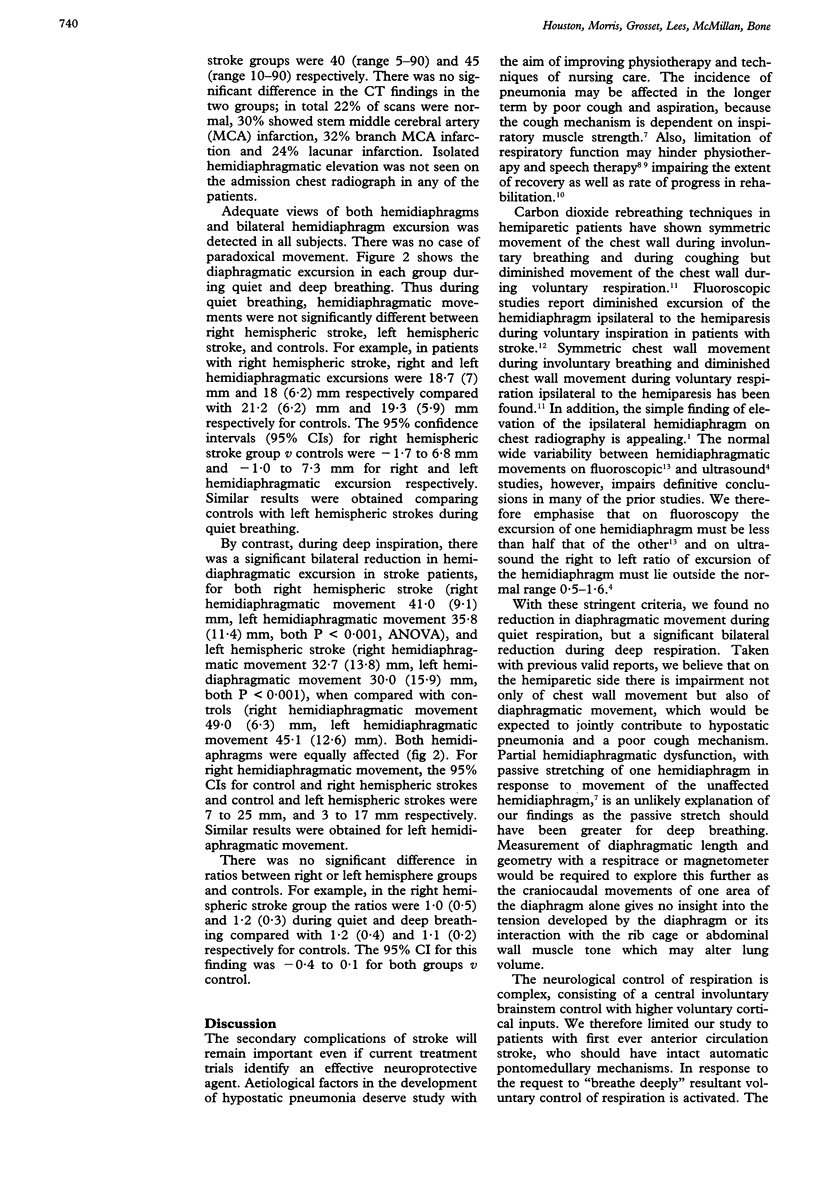
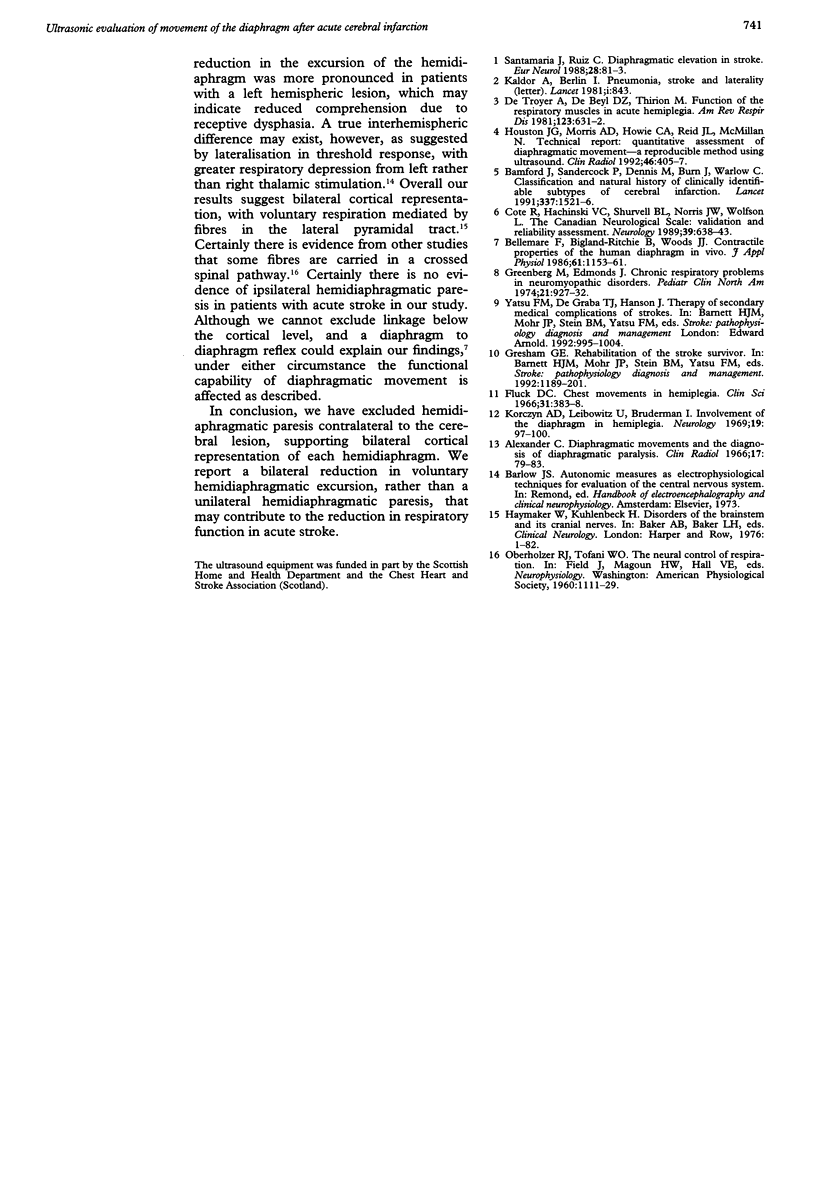
Respiratory dysfunction is an important complication of acute stroke but its mechanisms are poorly understood. Previous indirect assessments suggest that paralysis of the diaphragm occurs contralateral to the cerebral lesion. Diaphragmatic excursion was studied with real time ultrasound during quiet and deep breathing in 50 patients within 72 hours of acute stroke and 40 controls. During quiet breathing, hemidiaphragmatic movements were not significantly different between right hemispheric stroke, left hemispheric stroke, and controls. During deep inspiration, there was a significant bilateral reduction in hemi-diaphragmatic excursion in patients with stroke, for both right hemispheric stroke and left hemispheric stroke when compared with controls (both P < 0.001). Thus isolated hemidiaphragmatic paresis does not occur but maximal excursion of the diaphragm is reduced bilaterally in patients with acute stroke. This is a likely contributor to the respiratory dysfunction after acute stroke.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alexander C. Diaphragm movements and the diagnosis of diaphragmatic paralysis. Clin Radiol. 1966 Jan;17(1):79–83. doi: 10.1016/s0009-9260(66)80128-9. [DOI] [PubMed] [Google Scholar]
- Bamford J., Sandercock P., Dennis M., Burn J., Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. 1991 Jun 22;337(8756):1521–1526. doi: 10.1016/0140-6736(91)93206-o. [DOI] [PubMed] [Google Scholar]
- Bellemare F., Bigland-Ritchie B., Woods J. J. Contractile properties of the human diaphragm in vivo. J Appl Physiol (1985) 1986 Sep;61(3):1153–1161. doi: 10.1152/jappl.1986.61.3.1153. [DOI] [PubMed] [Google Scholar]
- Côté R., Battista R. N., Wolfson C., Boucher J., Adam J., Hachinski V. The Canadian Neurological Scale: validation and reliability assessment. Neurology. 1989 May;39(5):638–643. doi: 10.1212/wnl.39.5.638. [DOI] [PubMed] [Google Scholar]
- De Troyer A., Zegers De Beyl D., Thirion M. Function of the respiratory muscles in acute hemiplegia. Am Rev Respir Dis. 1981 Jun;123(6):631–632. doi: 10.1164/arrd.1981.123.6.631. [DOI] [PubMed] [Google Scholar]
- Fluck D. C. Chest movements in hemiplegia. Clin Sci. 1966 Dec;31(3):383–388. [PubMed] [Google Scholar]
- Greenberg M., Edmonds J. Chronic respiratory problems in neuromyopathic disorders: their nature and management. Pediatr Clin North Am. 1974 Nov;21(4):927–934. doi: 10.1016/s0031-3955(16)33068-1. [DOI] [PubMed] [Google Scholar]
- Houston J. G., Morris A. D., Howie C. A., Reid J. L., McMillan N. Technical report: quantitative assessment of diaphragmatic movement--a reproducible method using ultrasound. Clin Radiol. 1992 Dec;46(6):405–407. doi: 10.1016/s0009-9260(05)80688-9. [DOI] [PubMed] [Google Scholar]
- Kaldor A., Berlin I. Pneumonia, stroke, and laterality. Lancet. 1981 Apr 11;1(8224):843–843. doi: 10.1016/s0140-6736(81)92724-0. [DOI] [PubMed] [Google Scholar]
- Korczyn A. D., Leibowitz U., Bruderman I. Involvement of the diaphragm in hemiplegia. Neurology. 1969 Jan;19(1):97–100. doi: 10.1212/wnl.19.1.97. [DOI] [PubMed] [Google Scholar]
- Santamaria J., Ruiz C. Diaphragmatic elevation in stroke. Eur Neurol. 1988;28(2):81–83. doi: 10.1159/000116235. [DOI] [PubMed] [Google Scholar]