

Abstract
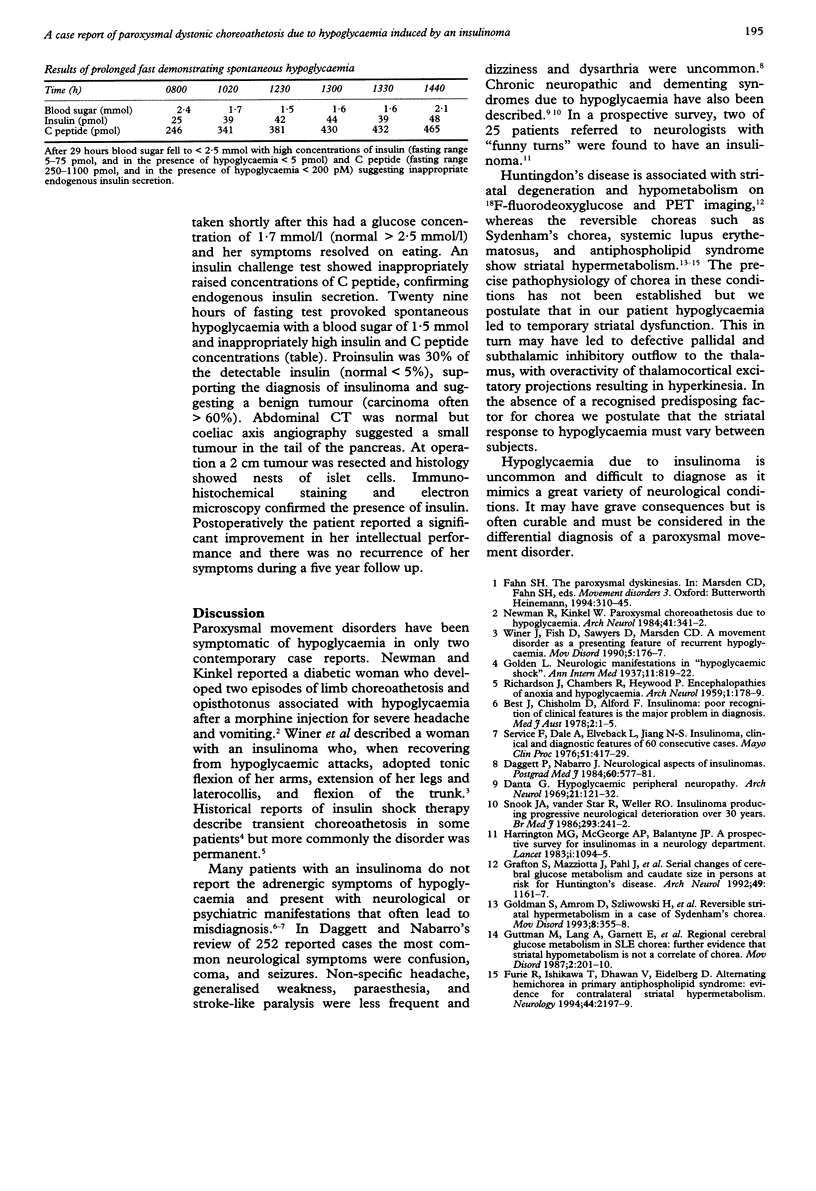
Hypoglycaemia due to an insulinoma can mimic acute disorders of cognition, consciousness, epilepsy, transient ischaemia, or psychosis, and chronic disorders of dementia and neuropathy. Misdiagnosis and delay in treatment are common and prolonged hypoglycaemia can lead to permanent neurological deficit or fatal coma. A 27 year old woman with hypoglycaemia induced by an insulinoma presented with features typical of paroxysmal non-kinesiogenic dystonic choreoathetosis. Striatal dysfunction as a consequence of hypoglycaemia has rarely been described. Insulinoma is a readily treatable condition that should be considered in the differential diagnosis of a paroxysmal movement disorder.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Daggett P., Nabarro J. Neurological aspects of insulinomas. Postgrad Med J. 1984 Sep;60(707):577–581. doi: 10.1136/pgmj.60.707.577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danta G. Hypoglycemic peripheral neuropathy. Arch Neurol. 1969 Aug;21(2):121–132. doi: 10.1001/archneur.1969.00480140021002. [DOI] [PubMed] [Google Scholar]
- Furie R., Ishikawa T., Dhawan V., Eidelberg D. Alternating hemichorea in primary antiphospholipid syndrome: evidence for contralateral striatal hypermetabolism. Neurology. 1994 Nov;44(11):2197–2199. doi: 10.1212/wnl.44.11.2197. [DOI] [PubMed] [Google Scholar]
- Goldman S., Amrom D., Szliwowski H. B., Detemmerman D., Goldman S., Bidaut L. M., Stanus E., Luxen A. Reversible striatal hypermetabolism in a case of Sydenham's chorea. Mov Disord. 1993 Jul;8(3):355–358. doi: 10.1002/mds.870080318. [DOI] [PubMed] [Google Scholar]
- Grafton S. T., Mazziotta J. C., Pahl J. J., St George-Hyslop P., Haines J. L., Gusella J., Hoffman J. M., Baxter L. R., Phelps M. E. Serial changes of cerebral glucose metabolism and caudate size in persons at risk for Huntington's disease. Arch Neurol. 1992 Nov;49(11):1161–1167. doi: 10.1001/archneur.1992.00530350075022. [DOI] [PubMed] [Google Scholar]
- Guttman M., Lang A. E., Garnett E. S., Nahmias C., Firnau G., Tyndel F. J., Gordon A. S. Regional cerebral glucose metabolism in SLE chorea: further evidence that striatal hypometabolism is not a correlate of chorea. Mov Disord. 1987;2(3):201–210. doi: 10.1002/mds.870020307. [DOI] [PubMed] [Google Scholar]
- Harrington M. G., McGeorge A. P., Ballantyne J. P., Beastall G. A prospective survey for insulinomas in a neurology department. Lancet. 1983 May 14;1(8333):1094–1095. doi: 10.1016/s0140-6736(83)91923-2. [DOI] [PubMed] [Google Scholar]
- Newman R. P., Kinkel W. R. Paroxysmal choreoathetosis due to hypoglycemia. Arch Neurol. 1984 Mar;41(3):341–342. doi: 10.1001/archneur.1984.04050150123033. [DOI] [PubMed] [Google Scholar]
- Service F. J., Dale A. J., Elveback L. R., Jiang N. S. Insulinoma: clinical and diagnostic features of 60 consecutive cases. Mayo Clin Proc. 1976 Jul;51(7):417–429. [PubMed] [Google Scholar]
- Snook J. A., vanderStar R., Weller R. O. Insulinoma producing progressive neurological deterioration over 30 years. Br Med J (Clin Res Ed) 1986 Jul 26;293(6541):241–242. doi: 10.1136/bmj.293.6541.241-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winer J. B., Fish D. R., Sawyers D., Marsden C. D. A movement disorder as a presenting feature of recurrent hypoglycaemia. Mov Disord. 1990;5(2):176–177. doi: 10.1002/mds.870050217. [DOI] [PubMed] [Google Scholar]