

Abstract
Freiberg’s infarction is the disorder of cartilage degeneration. The second metatarsal head is most vulnerable to Freiberg’s infarction due to its longer length and relative immobility. It is exposed to repetitive stress even during normal activity. The multifactorial etiology of Freiberg’s infarction is mentioned in the literature. It commonly affects the adolescent female with a female-to-male ratio of 5:1. High prevalence in adolescent females is explained in some literature due to wearing high heels, which leads to repetitive forced dorsiflexion injuries to the metatarsal head. Our case is an adolescent female of 20 years who was participating in dancing for 5 months. On examination, there is swelling and tenderness in the bilateral foot, more on the right side. Plain radiography showed the flattening of the head of the right second metatarsal with increased joint space. Mild sclerosis of the underlying bony cortex was seen. A mild deformity with flattening of the lateral surface of the head of the left second metatarsal was also seen.
Keywords: Freiberg, dancer, orthopaedics, radiology
Introduction
Freiberg’s infarction is the osteonecrotic process that was first described in 1914. 1 It predominately affects the second metatarsal head although the third and fourth metatarsal head can also be affected. Incidence is higher in females in their second decade. The exact mechanism is unclear; however, vascular, genetic, and altered biomechanics are possible risk factors. 2 It is a rare disorder with even rarer bilateral involvement. 3 It is usually diagnosed clinically and conventional radiography may be needed for confirmation. Early changes may be diagnosed with the help of magnetic resonance imaging (MRI) showing T1 low signal intensity or photopenic area in bone scans. 2 Conservative management is considered as a first line of treatment to control pain as well as to halt the progression to the advanced stage. Surgical management is used to correct the possible etiology and to address the advanced stage of the disease.4,5
Case report
A 20-year-old female presented in the outpatient department with a 5-month insidious history of right foot pain, located predominately at the second toe. She also complained of mild pain in the left second toe. She described the pain as a constant, dull type that exacerbated on walking. She used to go to the dance class every evening since 8 months. No history of trauma is present. She had no history of any systemic illness. On examination, there is swelling and tenderness in the bilateral foot, more on the right side. Plain radiography showed the flattening of the head of the right second metatarsal with increased joint space (Figure 1(a)–(d)). Mild sclerosis of the underlying bony cortex was seen (Figure 1(a)–(d)). Mild deformity with flattening of the lateral surface of the head of the left 2nd metatarsal was also seen (Figure 1(a)–(d)). No obvious soft tissue swelling was seen. MRI showed high signal intensity in the head of the first metatarsal in dorsal and plantar aspects (Figure 2(a) and (b)). The biochemical profile showed normal serum uric acid levels. Based on that clinical and radiological information, Freiberg’s infarction was diagnosed. The patient was treated conservatively with nonsteroidal anti-inflammatory drugs, rest, and modification of activities. She stopped going to her dance classes. She did not participate in any weight-bearing activities. After 2.5 months of her follow-up, she was symptom-free and could walk on the ground without having any pain and her follow-up X-ray findings were similar to old findings. After another 5 months, she was asked to do a follow-up X-ray for further management but she did not come and we called her through phone but she was not compliant to visit hospital again and had resumed her dancing practice again but with mild pain. She was advised not to practice dance or any other strenuous activities. She was given medication for pain during her discharge.
Figure 1.
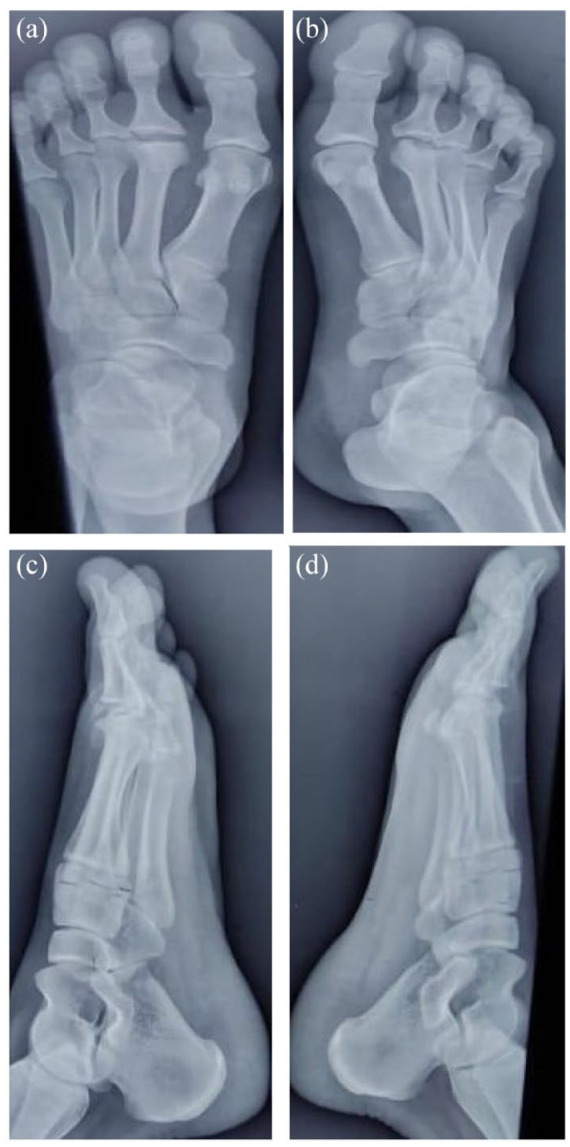
X-ray foot anteroposterior (a and b) and oblique view (c and d) of the bilateral foot shows flattening of the right second metatarsal head with the widening of the joint space. Sclerosis of the articular surface is also noted. No obvious cortical deformity is seen. The rest of the metatarsal and phalangeal bones are normal. There is mild deformity noted in the left metatarsal head with flattening in the lateral surface. Increased joint space is also noted. Sclerosis is noted in the articular surface of the left second metatarsal head.
Figure 2.

(a) Plain T2 fat-sat MRI of right foot showing high signal intensity in the head of first metatarsal in dorsal and plantar aspects (blue arrow). High signal marrow edema is also noted. (b) Plain T2 fat-sat MRI of the left foot showing high signal intensity in the head of first metatarsal in dorsal and plantar aspects (blue arrow).
Discussion
Freiberg’s infarction is the disorder of cartilage degeneration which was first explained in six patients with forefoot pain by Freiberg in 1914. 2 The second metatarsal head is most vulnerable to Freiberg’s infarction due to its longer length and relative immobility. It is exposed to repetitive stress even during normal activity. 4 The multifactorial etiology of Freiberg’s infarction is mentioned in the literature. It commonly affects the adolescent female with a female-to-male ratio of 5:1. High prevalence in adolescent females is explained in some literature due to wearing high heels, which leads to repetitive forced dorsiflexion injury to the metatarsal head. 4 Our case is an adolescent female of 20 years who was participating in dancing for 5 months. Pain in the second metatarsophalangeal joint is the most common symptom of Freiberg’s disease. Other clinical features include swelling, deformity, redness, and difficulty in walking. With the advancement of the disease, it shows malalignment and deformity. 6 Our patient also complained of constant dull aching pain which aggravated on walking. No obvious deformity or malalignment was seen. Radiography is helpful for the confirmation of diagnosis. In radiography, there is a flattening of the metatarsal head with the widening of the joint space. 4 Fragmentation, sclerosis, and cortical thickening can be seen in the advanced stage. 2 In the early stage, MRI is more sensitive than radiography. MRI shows marrow edema, collapse, and hypointensity in the metatarsal head. 4 This case belongs to Stage 2 on Smillie Classification System (Figure 1(a)–(d)). Nonoperative management helps in decreasing foot pressure and unloading the affected metatarsal. According to Smillie, there is the possibility of spontaneous healing at any stage, and restoration of normal function may occur in stages 1–3. As the articular cartilage is nonvascular, it is not affected by the ischemic condition of the underlying bone. 7 Conservative management reduces foot pain and halts the progression to advanced stages. A variable surgical technique is explained for Freiberg’s infarction in literature if conservative management fails. Although all the procedures are associated with a successful outcome, no sufficient evidence is available regarding the superiority of one procedure to the other. 8
Conclusion
We presented our case due to its bilateral involvement which is of a rare type. Only a few cases of bilateral metatarsal head involvement in adolescent females are explained in the literature. Our case is also associated with dancing activities. It also describes use of conservative management especially in a noncompliant patient.
Acknowledgments
None.
Footnotes
Author contribution statement: All authors contributed to the conduct of this research and read and approved the final version of the article. Written informed consent was obtained from the patient party to publish this report in accordance with the journal’s “patient consent policy” on the title page of the article.
Data availability: The data supporting the findings in this case are available upon request to the corresponding author.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval: Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent: Written informed consent was obtained from the patient for anonymized patient information to be published in this article.
ORCID iDs: Shailendra Katwal  https://orcid.org/0000-0001-7903-8789
https://orcid.org/0000-0001-7903-8789
Sarad Katuwal
https://orcid.org/0000-0002-4130-3329
References
- 1. John Donaldson C, Harb Z, Hussain L, et al. Freiberg’s disease of bilateral and adjacent metatarsals. Case Rep Orthop Res 2020; 3: 25–33. [Google Scholar]
- 2. Talusan PG, Diaz-Collado PJ, Reach JS. Freiberg’s infraction: diagnosis and treatment. Foot Ankle Spec 2014; 7(1): 52–56. [DOI] [PubMed] [Google Scholar]
- 3. Maresca G, Adriani E, Falez F, et al. Arthroscopic treatment of bilateral Freiberg’s infraction. Arthroscopy 1996; 12(1): 103–108. [DOI] [PubMed] [Google Scholar]
- 4. Carmont MR, Rees RJ, Blundell CM. Current concepts review: Freiberg’s disease. Foot Ankle Int 2009; 30(2): 167–176. [DOI] [PubMed] [Google Scholar]
- 5. Cerrato RA. Freiberg’s disease. Foot Ankle Clin 2011; 16(4): 647–658. [DOI] [PubMed] [Google Scholar]
- 6. Shane A, Reeves C, Wobst G, et al. Second metatarsophalangeal joint pathology and freiberg disease. Clin Podiatr Med Surg 2013; 30(3): 313–325. [DOI] [PubMed] [Google Scholar]
- 7. Smillie IS. Treatment of Freiberg’s infraction. Proc R Soc Med 1967; 60(1): 29–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Schade VL. Surgical management of Freiberg’s infraction: a systematic review. Foot Ankle Spec 2015; 8(6): 498–519. [DOI] [PubMed] [Google Scholar]