

Abstract
Introduction
Published global and country-specific deaths associated with population aging are based on decomposition methods that have significant limitations.
Methods
A new decomposition method was developed and its performance was compared with two frequently used methods. The new method was employed to calculate global deaths associated with population aging between 1990 and 2019, using estimates from the Global Burden of Disease Study 2019 (GBD 2019).
Results
Compared to the two frequently-used existing methods, the new decomposition method generated results that are more consistent with logical expectations. Using the new method, the number of global deaths associated with population aging between 1990 and 2019 was 23.3 million. Upper middle-income countries accounted for 43% of global deaths related to population aging. The most deaths associated with population aging occurred from three types of disease: ischemic heart disease (5.0 million), stroke (3.8 million), and chronic obstructive pulmonary disease (2.2 million). China, India, Japan, the United States of America, and Brazil had the largest number of deaths related to population aging. Loss related to population aging was completely or partially counteracted by the reduction in mortality in 195 of the 200 countries and territories experiencing population aging (97.5%).
Conclusions
The new decomposition method achieves more justifiable results associated with population aging than existing methods. Globally, population aging was associated with a substantial increase of deaths between 1990 and 2019, but it was totally or partially offset by the reduction in mortality in 97.5% of countries and territories.
Keywords: Population Aging, Health Impact, Global Health, Decomposition Method
As the population ages steadily in most countries around the world, it has become an increasing research priority to quantify the deaths associated with population aging globally, nationally, and locally. All existing decomposition approaches use changes in age structure to approximate population aging (1–3). This method does not precisely measure deaths associated with population aging and becomes especially problematic in situations where the proportion of old adults increases but the number decreases, such as when conflicts or wars cause more deaths among young and middle-aged adults than among older adults. Recent situations in Iraq and Syria offer examples (1,4-5).
To address gaps in available research evidence caused by methodological limitations in existing decomposition methods, we developed a novel decomposition method. This new method was applied to data from the Global Burden of Disease Study 2019 (GBD 2019) to calculate the worldwide deaths related to population aging between 1990 and 2019. Additionally, we evaluated whether the benefits of improving population health through mortality reduction were greater than the health loss associated with population aging.
METHODS
Unlike previously published decomposition methods that approximate changes in age structure as population aging (1–3), the new method defines the increase in the number of old adults as population aging. Detailed derivation of the new decomposition method and a comparative evaluation of its performance versus two of the most-cited decomposition methods (number-based and rate-based methods) can be found in Supplementary Material (available in https://weekly.chinacdc.cn/). We chose the number-based method developed by Cheng et al. (3) as a comparator because it has clear advantages compared to alternatives. We also selected the widely-used rate-based decomposition method as the other comparator (6). Four countries, which experienced inconsistent changes in the number and proportion of old adults between 1990 and 2019, were selected to create four scenarios for comparing the performance across the three decomposition methods.
All data were derived from online resources of the GBD 2019, which provides estimates for multiple health outcomes across 369 diseases and injuries, and sex-specific population sizes for 204 countries and territories from 1990 to 2019. Detailed estimation methods for GBD 2019 appeared elsewhere (7-8).
Based on World Bank classifications, we categorized the 204 countries and territories into four income groups: low-income countries (LICs), lower middle-income countries (LMICs), upper middle-income countries (UMICs), and high-income countries (HICs). We conducted disease-specific analyses using the level-3 disease categorization (134 subcategories) defined by the GBD 2019. Populations were divided into 20 age groups, ranging from under 5 years to 95 years and older.
We utilized the novel decomposition method to compute global sex-, disease-, and country/territory-specific fatalities linked to population aging from 1990 to 2019. Bar charts and maps were utilized to visually depict subgroup disparities and geographic variances.
We examined the counteracting effect of reducing mortality rates in relation to population aging by using the ratio (denoted as R) of the number of deaths attributed to mortality reduction divided by that associated with population aging based on previous literature (3,9). As the numbers of deaths attributed to population aging and to reduced age-specific mortality are in opposite directions and sum to the net change in total deaths, R has a clear epidemiological interpretation in measuring the relative effect of mortality reduction and population aging. For the 200 out of 204 countries and territories that experienced population aging between 1990 and 2019, “R≤−1”, “−1<R<0” and “R=0” respectively suggest that the benefit achieved due to mortality reduction “clearly exceeded”, “partially balances” or “does not alleviate” the loss associated with population aging. “R>0” indicates that the mortality increase exacerbates the loss associated with population aging.
All data analyses were performed using R4.2.2 (R Foundation, Vienna, Austria), and the package ‘maps’ was used to draw the maps. The study protocol was approved by the Ethics Committee of Xiangya School of Public Health, Central South University on 26 July 2022 (No. XYGW-2022-46).
RESULTS
Global deaths associated with population aging between 1990 and 2019 total approximately 23.3 million, with 12.0 million among men and 11.3 million among women (Figure 1A). UMICs have the largest number of deaths associated with population aging during 1990–2019, with 10.0 million, followed by LMICs (7.0 million), HICs (5.5 million), and LICs (0.8 million) (Figure 1B).
Figure 1.
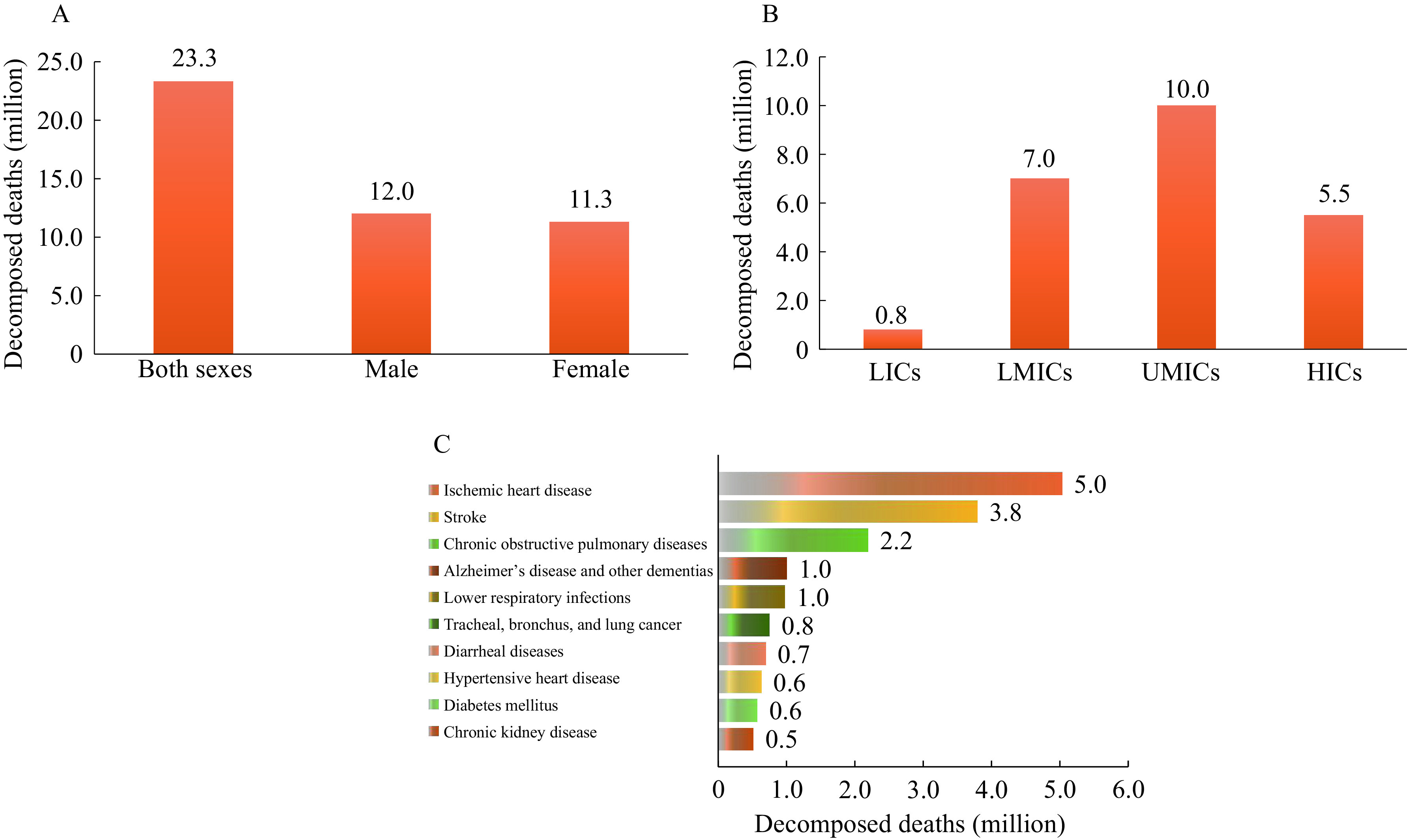
Global deaths related to population aging between 1990 and 2019 by (A) sex; (B) country income; (C) type of dise.
Abbreviation: LICs=low-income countries; LMICs=lower middle-income countries; UMICs=upper middle-income countries; HICs=high-income countries.
The number of deaths associated with population aging vary greatly across different types of diseases between 1990 and 2019 (Figure 1C). The top ten causes of disease accounted for a total of 16.1 million global deaths related to population aging (69.2%); these included ischemic heart disease (5.0 million); stroke (3.8 million); chronic obstructive pulmonary disease (COPD, 2.2 million); Alzheimer’s disease and other dementias (ADOD, 1.0 million); lower respiratory infections (1.0 million); tracheal, bronchus, and lung (TBL) cancer (0.8 million); diarrheal diseases (0.7 million); hypertensive heart disease (0.6 million); diabetes mellitus (0.6 million); and chronic kidney disease (0.5 million).
Of the 200 countries and territories that experienced population aging between 1990 and 2019, the number of deaths associated with population aging varied substantially across countries and territories. China, India, Japan, the United States, and Brazil had the largest number of deaths related to population aging and together accounted for 58.8% of global decomposed deaths. Respective numbers of deaths in those five countries were 6.4 million, 4.4 million, 1.1 million, 1.0 million, and 0.7 million.
Between 1990 and 2019, the number of global deaths averted by reductions in mortality exceeded those associated with population aging (−23.5 million vs. 23.3 million) (Figure 2A). Subgroup analyses show that the decrease in deaths due to mortality reduction completely offsets the increase associated with population aging among males (−12.5 million vs. 12.0 million) and in both LMICs (−8.9 million vs. 7.0 million) and LICs (−3.1 million vs. 0.8 million), but the counteracting effect is only partial in UMICs (−7.8 million vs. 10.0 million) and HICs (−3.6 million vs. 5.5 million) (Figure 2B).
Figure 2.
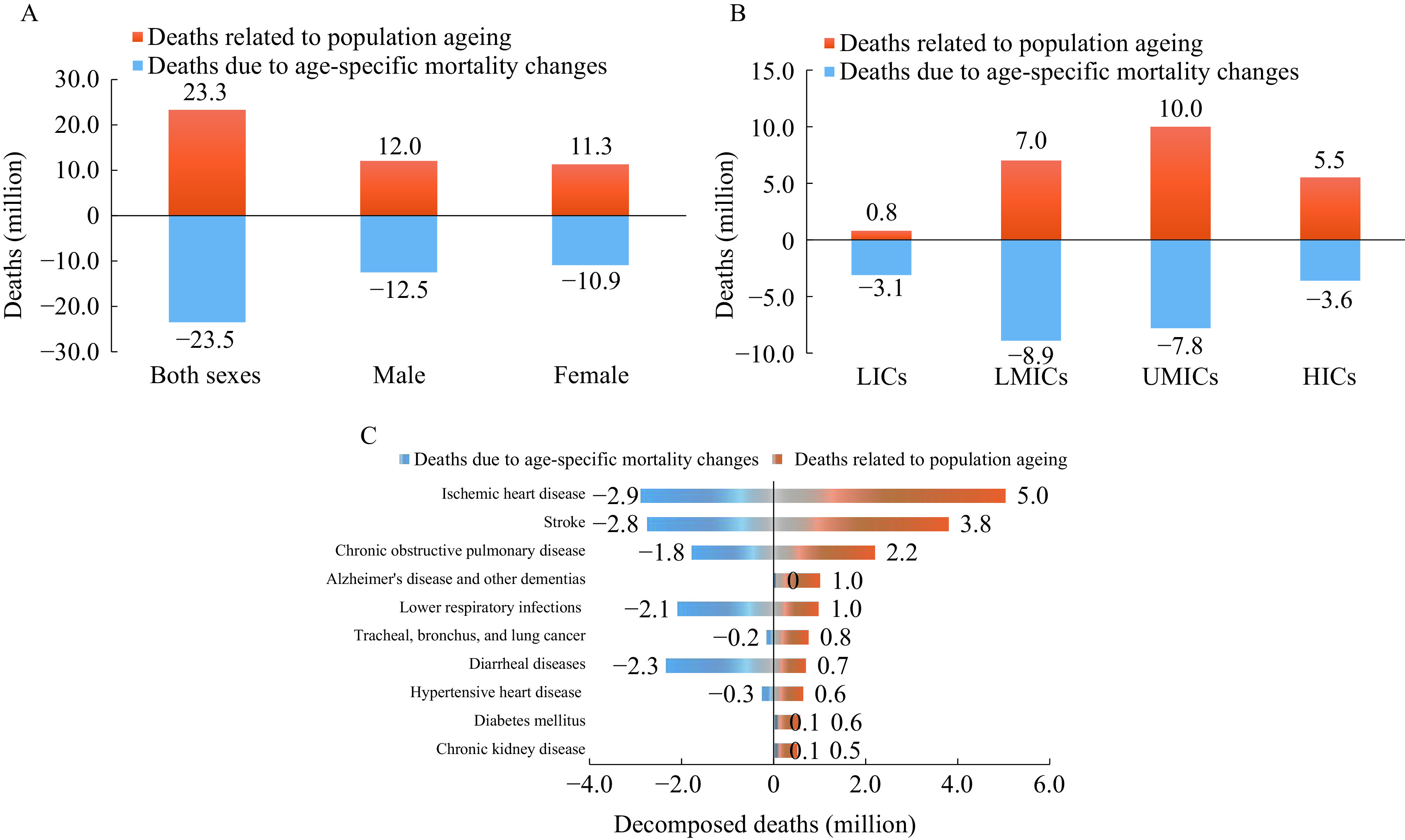
The counteracting effect of mortality reduction against the loss related to population aging between 1990 and 2019. (A) by sex; (B) by country income; (C) by type of disease.
Among the top ten diseases with the highest mortality rates associated with population aging, the counteracting effect of reduced mortality is most pronounced for lower respiratory infections (−2.1 million vs. 0.96 million) and diarrheal diseases (−2.3 million vs. 0.7 million) (Figure 2C). The reduction in mortality was insufficient to counteract the effects of population aging for five disease types: ischemic heart disease (−2.9 million vs. 5.0 million); stroke (−2.8 million vs. 3.8 million); COPD (−1.8 million vs. 2.2 million); TBL cancer (−0.2 million vs. 0.8 million); and hypertensive heart disease (−0.3 million vs. 0.6 million). Importantly, the increase in mortality intensified the impact of population aging on three disease types: ADOD (0.03 million vs. 1.0 million), diabetes mellitus (0.08 million vs. 0.6 million), and chronic kidney disease (0.1 million vs. 0.5 million).
Of the 200 countries and territories that experienced population aging between 1990 and 2019, the health loss associated with population aging was outweighed by the benefits from mortality reduction in 44.0% (88 of 200 countries/territories, R≤−1), and was partially counteracted in 53.5% (107 of 200, −1<R≤0). The most notable counteracting effect occurred in Tajikistan, with an R of −40.8. In contrast, the health loss related to population aging was not offset at all in five countries (5 of 200, R>0): Lesotho, Eswatini, Zimbabwe, Montenegro, and Ukraine.
DISCUSSION
This study presents two main findings. First, the new decomposition method produced decomposed results that align more closely with logical expectations compared to traditional decomposition methods, estimating a total of 23.3 million deaths associated with global population aging. Second, the number of deaths related to population aging was completely or partially offset by the lives saved as a result of mortality reduction in 195 out of the 200 countries and territories with aging population between 1990 and 2019.
The new decomposition method produces more reliable estimates that align with logical expectations compared to the two most cited methods, as supported by both its theoretical foundation and data illustration Supplementary Material and Supplementary Table S1, available in https://weekly.chinacdc.cn/). First, it employs the number of elderly individuals to measure population aging, whereas existing decomposition methods use changes in the age structure as a proxy of population aging. This proxy does not accurately reflect the impact of population aging in certain situations, and it can lead to misleading decomposed results. Second, it equally separates the interaction of age-specific population size and age-specific rate, ensuring the robustness of the results regardless of the decomposition order of these two factors, as outlined in the Supplementary Materials.
A total of 23.3 million deaths associated with population aging reflects the significant impact of population aging on our society. Substantial differences in the number of deaths associated with population aging across sex, country/territory, country income level, and type of disease generally reflect the combined effects of varying demographics and disparities in socio-economic development. The former is related to the steady rise of older adults due to reduced birth rate and prolonged life expectancy in many countries, while the latter country/territory differences are attributed to variations in economic development, migration, education, and healthcare services (10). For instance, the United States accounted for 23.9% of the global gross domestic product (GDP) (11), but only 4.7% of the global deaths associated with population aging.
Despite the alarming 23.3 million global deaths associated with population aging, our findings also demonstrate that the lives saved due to mortality reduction have completely or partially offset the increased deaths associated with population aging between 1990 and 2019 in almost all countries and territories (195 of 200). However, the counteracting effect of mortality reduction varied across subgroups. Specifically, overall mortality increased in five countries (Lesotho, Eswatini, Zimbabwe, Montenegro, and Ukraine) between 1990 and 2019, exacerbating deaths associated with population aging. These findings highlighted the importance and urgency of reducing mortality disparities across countries and territories.
Our findings have at least three important policy implications. First, we recommend the use of the new decomposition method to calculate health outcome counts associated with population aging. Second, our findings highlight the importance and urgency of taking prevention and control actions to curb the large loss of life related to population aging globally and nationally. Field-proven and cost-effective prevention measures, along with medical treatments for high-mortality diseases among the elderly, should be prioritized and implemented worldwide. Third, globally coordinated efforts and investments should be undertaken to reduce disparities in morbidity and mortality associated with population aging across countries and territories.
This study is primarily limited by the availability and quality of estimates from the GBD 2019 public database. In addition, due to the unavailability of complete data on mortality rates, we are unable to provide 95% uncertainty intervals for our estimates. These limitations could be addressed by including high-quality raw data and methodological innovations in future research.
CONCLUSION
The new method we developed is robust and consistent with logical expectations in calculating deaths associated with population aging compared to the two most cited decomposition methods. Therefore, we recommend researchers and policymakers to use the new decomposition method to calculate deaths (and other health losses) associated with population aging. We also call for coordinated global efforts to address the challenge of population aging, which should include prioritization of preventing and treating leading types of disease, implementation of empirically-supported and cost-effective prevention and treatment measures worldwide, and distribution of international aid to support the most affected countries and territories.
Conflicts of interest
No conflicts of interest.
SUPPLEMENTARY MATERIAL
Description of the New Decomposition Method
Suppose that we have collected the following aggregate data for 20 age groups in a given country from the two years over a two-year period: age-specific population size ( ) and age-specific mortality rate (
) and age-specific mortality rate ( ),
),  indexing the year and
indexing the year and  indexing the age groups. The total population sizes and overall mortality rates in the country over the two years are accordingly calculated as
indexing the age groups. The total population sizes and overall mortality rates in the country over the two years are accordingly calculated as  ,
,  ,
,  , and
, and  . D1 and D2 represent the total number of deaths in the given country in years 1 and 2.
. D1 and D2 represent the total number of deaths in the given country in years 1 and 2.
 |
1 |
Where Mn, Mr, and In×r denote the main effect of changes in age-specific population size, age-specific mortality, and their interaction.
With the use of the following formulas, we are able to calculate the number of deaths associated with population aging during a specific time frame.
First, calculate the values of Mn, Mr, and In×r using the following formulas:
 |
2 |
 |
3 |
 |
4 |
Second, separate the main effects and interactions related to older adults from  ,
,  , and
, and  . According to the operational definition of older adults (≥65 years), we can divide each of
. According to the operational definition of older adults (≥65 years), we can divide each of  ,
,  , and
, and  into two parts, for those younger than 65 years old and those ≥65 years old. Let a represent the age group of 65 to 70 years old, and we can rewrite the formulas of Mn, Mr, and In×r as follows:
into two parts, for those younger than 65 years old and those ≥65 years old. Let a represent the age group of 65 to 70 years old, and we can rewrite the formulas of Mn, Mr, and In×r as follows:
 |
5 |
 |
6 |
 |
7 |
Third, calculate the deaths associated with population aging between the two years. We need to first allocate the interaction reasonably and then calculate the health loss associated with population aging.
(a) Justification of interaction allocation
Based on Formulas (2–4), we assume that the proportion of allocating the interaction is Φ in our decomposition method. Therefore, the deaths associated with population aging between years 1 and 2 (PA) are:
 |
8 |
When the reference population is changed from population 1 to population 2, the deaths associated with population aging between years 1 and 2 ( ) is:
) is:
 |
9 |
To ensure the robustness of decomposed results, we restrict  to be equal to -
to be equal to - . Under this restriction, Formulas (8) and (9) lead to:
. Under this restriction, Formulas (8) and (9) lead to:
 |
10 |
which implies Φ= 1/2.
(b) Calculate health loss associated with population aging
Based on the equal allocation of interaction, we use Formula (11) to estimate the health loss associated with population aging (PA):
 |
11 |
Calculation of Subgroup Decomposition Analysis
We demonstrate the application of sex-specific decomposition using the following example. The number of deaths and populations can be aggregated separately for each sex. According to Formula (8), we can compute the number of deaths associated with population aging for the entire population, as well as for males and females, denoted as PAoverall, PAmale, and PAfemale:
 |
12 |
 |
13 |
 |
14 |
Because generally  and
and  ,
,  does not necessarily equal the sum of
does not necessarily equal the sum of  and
and  . This conflicts with the common expectation that the overall decomposed result should equal the sum of subgroup decomposed results for males and females.
. This conflicts with the common expectation that the overall decomposed result should equal the sum of subgroup decomposed results for males and females.
We further investigated under what conditions  ) does hold. Assume
) does hold. Assume  denotes the proportion of males in age group
denotes the proportion of males in age group  at time point
at time point  . We then have
. We then have  . Using Formulas (12–14), we get
. Using Formulas (12–14), we get
 |
Under the assumption that age-specific sex ratios do not change between time points 1 and 2 (i.e.,  , the above expression can be simplified as
, the above expression can be simplified as
 |
That is,  ) holds under this assumption.
) holds under this assumption.
When the age-specific sex ratio changes over time (i.e.,  ), the gap (G) between
), the gap (G) between  and
and  does not necessarily equal zero in all cases. To ensure
does not necessarily equal zero in all cases. To ensure  ) and to maintain the comparative contribution of subgroup decomposed results, we adopt a simple proportional allocation method to distribute the gap (G) between
) and to maintain the comparative contribution of subgroup decomposed results, we adopt a simple proportional allocation method to distribute the gap (G) between  and
and  according to the contributions of subgroup decomposed results.
according to the contributions of subgroup decomposed results.
Specifically, we obtain the adjusted estimates of  and
and  :
:
 |
15 |
 |
16 |
 |
17 |
So that we ensure  = (
= ( +
+  ) in all cases. Similarly, we calculate the adjusted contribution associated with population aging by other variables (i.e., type of disease, country/territory).
) in all cases. Similarly, we calculate the adjusted contribution associated with population aging by other variables (i.e., type of disease, country/territory).
Performance of the New Decomposition Method
All existing decomposition methods can be divided into two categories according to the type of health metric to be decomposed: number-based and rate-based decomposition methods. We selected the number-based method developed by Cheng et al. (1) which was reported to have clear advantages compared to other number-based methods as a comparator, and the only rate-based decomposition method was selected as the other comparator. Compared to the two most cited methods (abbreviated as method I and method Ⅱ) (1-2), we assessed the performance of the new decomposition method (denoted as method Ⅲ). Compared to the two most frequently cited methods (abbreviated as method I and method Ⅱ) (1-2), we assessed the performance of the new decomposition method (denoted as method Ⅲ).
We selected four countries (Afghanistan, China, Nauru, and Niue) with varying changes the number and proportion of older adults between 1990 and 2019 to illustrate the comparative performance of the three methods. We followed a basic principle in comparing the performance of the three decomposition methods, which states that a valid method should reflect the impact of population aging in a reasonable manner. Specifically, a valid decomposition method should increase (decrease) in counts or rates of health outcomes associated with aging as the population ages (gets younger). This is based on the common understanding that older adults generally have higher rates of all-cause mortality and morbidity compared to children and younger adults.
We selected four countries that showed varying changes in the number of older adults and in the proportion of older adults (Supplementary Table S1). In both Afghanistan and China, the number of older adults aged 65 years and older increased between 1990 and 2019. However, the proportion of older adults aged 65 years and older decreased by 2.8% in Afghanistan but increased 7.0% in China. Nauru and Niue, two Pacific Island nations, showed different patterns. In both Nauru and Niue, the number of older adults decreased but the proportion of older adults decreased by 0.2% in Nauru and increased by 2.4% in Niue.
We expect a valid decomposition method to capture the increase of decomposition deaths (mortality) associated with population aging in both China and Afghanistan, as well as the decrease in decomposition deaths (mortality) associated with population aging in Niue and Nauru. As shown in Supplementary Table S1, only method III attained decomposed results associated with population aging in the correct direction for all four countries, with increases for Afghanistan and China, and decreases for Nauru and Niue. Methods I and II generated decomposed results deviating from expectations in Afghanistan, Nauru, and Niue.
Compared to other frequently used decomposition methods (1-2), the new decomposition method has two advantages. First, it generates reasonable decomposition results in all cases, overcoming deficiencies of existing methods such as being sensitive to the decomposition order of factors (3-4). Second, it relies on changes in the number of older adults rather than changes in age structure of the population. In this way, it more rationally captures the health effects of population aging and provides a more helpful basis for evaluating related health policies.
REFERENCES
Cheng XJ, Tan LH, Gao YY, Yang Y, Schwebel DC, Hu GQ. A new method to attribute differences in total deaths between groups to population size, age structure and age-specific mortality rate. PLoS One 2019;14(5):e0216613. http://dx.doi.org/10.1371/journal.pone.0216613.
Yang GH, Wang JF, Wan X, Wang LJ, Chen AP. Quantitative analysis of factors affected mortality trend in Chinese, 2002. Chin J Epidemiol 2005;26(12):934 − 8. http://dx.doi.org/10.3760/j.issn:0254-6450.2005.12.003. (In Chinese).
Li RT, Cheng XJ, Schwebel DC, Yang Y, Ning PS, Cheng PX, et al. Disability-adjusted life years associated with population ageing in China, 1990-2017. BMC Geriatr 2021;21(1):369. http://dx.doi.org/10.1186/s12877-021-02322-7.
Batljan I, Lagergren M, Thorslund M. Population ageing in Sweden: the effect of change in educational composition on the future number of older people suffering severe ill-health. Eur J Ageing 2009;6(3):201 − 11. http://dx.doi.org/10.1007/s10433-009-0120-1.
GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388(10053):1459 − 544. http://dx.doi.org/10.1016/S0140-6736(16)31012-1.
Bashir S, Estève J. Analysing the difference due to risk and demographic factors for incidence or mortality. Int J Epidemiol 2000;29(5):878 − 84. http://dx.doi.org/10.1093/ije/29.5.878.
Table S1. Deaths and mortality associated with population aging between 1990 and 2019 in four selected countries based on the three decomposition methods.*.
| Country | Number of old adults aged ≥65 | Proportion of old adults aged ≥65 (%) | Deaths/mortality related to aging† | ||||||||
| 1990 | 2019 | Change | 1990 | 2019 | Change | Method Ⅰ | Method Ⅱ§ | Method Ⅲ | |||
| * To properly compare three decomposition methods, we followed the basic guideline that a valid method should reflect the impact of population aging in a reasonable direction. Specifically, a valid decomposition method should generate an increase (decrease) in aging-associated health outcome counts or rates as the population ages (gets younger), according to common logic that older adults typically have higher all-cause mortality and morbidity rates than children and younger adults. † Methods Ⅰ and Ⅱ respectively denote the commonly used number-based and rate-based decomposition methods (1,5,6). Method Ⅲ represents the new decomposition method; § Decomposed results of methods Ⅰ and III are reported in the number of deaths, and decomposed results of method II are reported as mortality per 100,000 persons; ¶ The decomposed deaths of method I was 0.18 for Nauru due to the small population size and was therefore rounded to zero. | |||||||||||
| Afghanistan | 560,091 | 784,021 | 223,930 | 4.9 | 2.1 | −2.8 | −77,227 | −315 | 20,800 | ||
| China | 65,625,721 | 178,348,576 | 112,722,855 | 5.5 | 12.5 | 7.0 | 6,529,541 | 504 | 6,429,286 | ||
| Nauru | 188 | 168 | −20 | 1.8 | 1.6 | −0.2 | 0¶ | 2 | −3 | ||
| Niue | 203 | 186 | −17 | 8.7 | 11.1 | 2.4 | 5 | 237 | −2 | ||
References
- 1.GBD 2015 Mortality and Causes of Death Collaborators Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459–544. doi: 10.1016/S0140-6736(16)31012-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bashir S, Estève J Analysing the difference due to risk and demographic factors for incidence or mortality. Int J Epidemiol. 2000;29(5):878–84. doi: 10.1093/ije/29.5.878. [DOI] [PubMed] [Google Scholar]
- 3.Cheng XJ, Tan LH, Gao YY, Yang Y, Schwebel DC, Hu GQ A new method to attribute differences in total deaths between groups to population size, age structure and age-specific mortality rate. PLoS One. 2019;14(5):e0216613. doi: 10.1371/journal.pone.0216613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Roberts L, Lafta R, Garfield R, Khudhairi J, Burnham G Mortality before and after the 2003 invasion of Iraq: cluster sample survey. Lancet. 2004;364(9448):1857–64. doi: 10.1016/S0140-6736(04)17441-2. [DOI] [PubMed] [Google Scholar]
- 5.Amini R, Chee KH, Sen K, Ingman SR Elder care in iran: a case with a unique demographic profile. J Aging Soc Policy. 2021;33(6):611–25. doi: 10.1080/08959420.2020.1722896. [DOI] [PubMed] [Google Scholar]
- 6.Yang GH, Wang JF, Wan X, Wang LJ, Chen AP Quantitative analysis of factors affected mortality trend in Chinese, 2002. Chin J Epidemiol. 2005;26(12):934–8. doi: 10.3760/j.issn:0254-6450.2005.12.003. [DOI] [PubMed] [Google Scholar]
- 7.GBD 2019 Diseases and Injuries Collaborators Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.GBD 2019 Demographics Collaborators Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1160–203. doi: 10.1016/S0140-6736(20)30977-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cheng XJ, Yang Y, Schwebel DC, Liu ZY, Li L, Cheng PX, et al Population ageing and mortality during 1990-2017: a global decomposition analysis. PLoS Med. 2020;17(6):e1003138. doi: 10.1371/journal.pmed.1003138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL Measuring population ageing: an analysis of the Global Burden of Disease Study 2017. Lancet Public Health. 2019;4(3):e159–67. doi: 10.1016/S2468-2667(19)30019-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.World Bank. Gross domestic product ranking table. 2022. https://databankfiles.worldbank.org/public/ddpext_download/GDP.pdf. [2022-11-18].