

Abstract
Objectives A 1-year prospective human intervention study was performed to examine the anticaries, anti-inflammatory, antiproteolytic, and antimicrobial effects of fermented lingonberry juice (FLJ), used as a mouthwash for a period of 6 months, followed by a 6-month washout period.
Materials and Methods Twenty-five adults were recruited from private dental clinics in Helsinki and Joensuu (Finland). Standard oral examinations and sample gatherings were performed at base level, 6 months, and 1 year for oral Streptococcus mutans (S. mutans) , Candida , and Lactobacilli levels, and active matrix metalloprotease-8 (aMMP-8) levels, and for decayed, missing, filled teeth (DMFT), decayed, missing filled surfaces (DMFS) and decayed surfaces (DS) indexes, and probing pocket depths (PPDs), bleeding on probing (BOP), and visible plaque index (VPI). FLJ was used by the participants once daily for 30 seconds for 6 months. FLJ contains 0.212% (w/v) polyphenols, 3% (w/ v) sugars, and contains no excipients. Ten milliliters of FLJ were equal to 1 dL of lingonberry juice.
Statistical Analysis Statistical analyses were performed with nonparametric Friedman's test and pairwise post-hoc analysis with Dunn-Bonferroni test, SPSS (version 27; IBM) and p < 0.05 was considered as statistically significant.
Results The levels of S. mutans and Candida counts, DS, BOP, and VPI decreased significantly ( p < 0.05) during the FLJ period. Lactobacilli counts increased significantly, while there was also significant difference in aMMP-8 levels, DMFT, and DMFS between the three measurement points. PPDs were not affected.
Conclusions The specially formulated FLJ may have a positive decreasing effect on S. mutans , and Candida counts as well as decrease low-grade inflammation and proteolytic burden in the oral mucosa and periodontal tissues. The beneficial effects to the oral cavity of FLJ mouthwash may be useful among patients with oral diseases, such as dental caries, periodontitis and candidosis.
Keywords: fermented lingonberry juice, caries, periodontitis, candidosis, antimicrobial, inflammation
Introduction
Dental caries and periodontal disease, two major oral infections and inflammatory diseases, affect most of the population. 1 2 In the past years, the concept that Streptococcus mutans ( S. mutans ) and Lactobacilli act as the keystone bacteria in caries development is under doubt, and recently a more multispecies infectious etiology has received support, 3 4 although the issue is controversial. 5 The oral normal biofilm consists of hundreds of species 6 and, e.g., the subgingival plaque related to periodontal disease has been studied to contain approximately five hundred bacterial species. The interaction of these species with each other 7 and the host have been revealed piece by piece in caries, 8 and in periodontal disease, 9 10 and that Candida species may have role in these diseases. 11 The idea of using Lactobacilli in prevention of oral microbiome dysbiosis has been suggested. 12 Studies on multispecies, and even more importantly, in vivo human studies revealing these interactions are still quite scarce.
To prevent dental, gingival, and mucosal infections and inflammation, additional mouthwash preparations of natural origin have been proposed. Lingonberries are low-bush wild berries, which grow in the northern hemisphere and several in vitro studies have shown that their phenolic substances have anti-inflammatory, 13 antimicrobial, 14 and antioxidative effects. 15 Our previous studies with fermented lingonberry juice (FLJ) specially designed for safe oral use 16 showed that it has beneficial oral antimicrobial and anti-inflammatory effects in a 2-week in vivo human pilot study. 17 Active matrix metalloprotease-8 (aMMP-8) chair-side point-of-care mouthrinse test has proven to be suitable to measure periodontal inflammation levels, and implemented as a biomarker in the new staging- and grading-classification of periodontal disease. 18 19 20
In this study, we aimed to evaluate the effects of 6 months use of FLJ on levels of typical oral microbes ( Candida , S. mutans , and Lactobacilli ), and the in vivo effects on hypothesized prevention of caries, inflammation, and periodontal disease.
Materials and Methods
Twenty-five adults (aged between 28 and 91 years, mean age 64 years; M/F ratio was 10/15) were recruited randomly from private dental practices in Helsinki and Joensuu (Finland). Patients were excluded if they were pregnant, had received antibiotic medications, or if they had used chlorhexidine mouthwash during the study.
Standard oral examinations and sample gatherings were performed at the beginning of the study, and after 6 months and 1 year. The patients were instructed not to eat, drink, or brush teeth for 1 hour prior to the examinations. A saline rinse (10 mL for 30 seconds) was collected to evaluate effects on oral S. mutans , Candida , and Lactobacilli levels, reflecting caries and candidosis risk. Second, a chairside mouthrinse test was performed (PerioSafe, Dentognostics, Jena, Germany) according to the manufacturer's instructions to measure matrix metalloprotease-8 (aMMP-8) levels, which reflect inflammation and proteolytic periodontal destruction activity. 19 20 21 Dental decayed, missing, filled teeth (DMFT), decayed, missing, filled surfaces (DMFS) and decayed surfaces (DS) indexes were calculated and probing pocket depths (PPDs), bleeding on probing (BOP %) and visible plaque index (VPI) scale (0–3) were recorded. Saline rinse samples were cultivated by serial dilutions on Mitis salivarius (Merck, Darmstadt, Germany) bacitracin (0.2 U/mL) 20% saccharose, Sabouraud dextrose (LabM, Bury, UK) and DeMan Rogosa and Sharpe (Merck, Darmstadt, Germany) agars, and colony counts of S. mutans , Candida, and Lactobacilli were calculated. S. mutans counts were evaluated by light microscopy. CHROMagar Candida medium (CHROMagar, Paris, France) and latex agglutination test (Bichro-Dubli FumouzeR, Fumouze Diagnostics, Levallois-Perret, France) were used to identify Candida species. Scaling and root planning were performed after each sampling and oral examination time point. The participants used 10 mL of FLJ 16 (Lingora®, Vantaa, Finland) as a mouthwash for 30 second daily in addition to their normal oral homecare routines. FLJ is all natural, pasteurized, and manufactured by a patented method and contains no excipients. Naturally occurring sugars in lingonberry juice are reduced to 3g/100 mL and its polyphenol concentration is 212 mg/100 mL. Thus, the antimicrobial and anti-inflammatory effects are induced solely by the specific composition achieved by the fermentation process of lingonberry juice.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Stockholm Community, Sweden (2016–08–24/2016/1:8 and 2016–1-24) and the Helsinki University Central Hospital, Finland (360/13/03/00/13 and 51/13/02/2009). Informed consent was obtained from all subjects involved in the study.
Statistical analyses were performed with non-parametric Friedman's test and pairwise post-hoc analysis with Dunn-Bonferroni test (SPSS, version 27; IBM, Armonk, NY, United States), and p < 0.05 was considered as statistically significant. Initial correlations between the variables were calculated with Spearman's and the effects of FLJ mouthrinse with the repeated measures correlation (the rmcorr package, version 0.4.1 in R statistical software version 3.6.3). 22
Results
A total of 21 of the 25 recruited participants used the mouthwash according to instructions (10 mL/once a day) and were included in the analyses. One patient used 5 mL/once a day, two used 10 mL irregularly, and one used 20 mL/once a day. Diseases, medications, and smoking habits are shown in Table 1 . Analysis of the microbial cultivations revealed that most of the patients' yeast species (23/25) were identified as Candida albicans , only two as C. dubliniensis . Four patients had a mixed C. albicans /non- C. albicans (nd) growth.
Table 1. Patient characteristics ( n = 21) .
| Age (mean ± standard deviation) | 65.29 ± 16.23 years |
| Sex (female/ male, %) | 61.9/38.1% |
| Smoking (yes %) | 19.0% |
| Diseases (mean, range) 8. Medications (mean, range) |
1.76, 0–4 2.95, 0–9 |
| Medications causing xerostomia (mean, range) | 1.33, 0–4 |
The effects of FLJ on the 11 parameters studied are shown in Fig. 1 . During the FLJ mouthwash period, there was a significant difference between at least two measurement points in the levels of VPI, BOP, aMMP-8, DMFT, DMFS, DS, Candida , S. mutans , and Lactobacilli ( p < 0.05). VPI ( Fig. 1A ), BOP ( Fig. 1B ), DS ( Fig. 1H ) Candida ( Fig. 1I ), and S. mutans ( Fig. 1J ) decreased significantly and Lactobacilli ( Fig. 1K ) increased significantly between 0 and 6 months ( p = 0.001, p = 0.033, p = 0.033, p = 0.002, p = 0.021, respectively). Furthermore, S. mutans ( Fig. 1J ) increased significantly between 6 and 12 months and Lactobacilli ( Fig. 1K ) increased significantly between 0 and 12 months ( p = 0.006 and p < 0.001, respectively). Finally, both aMMP-8 ( Fig. 1C ) and BOP ( Fig. 1B ) levels were smaller at 12 months compared with the beginning of FLJ (0 months), but the difference did not reach statistical significance. There were no significant differences in PD more than or equal to 4mm ( Fig. 1D ) and PD more than or equal to 6 mm ( Fig. 1E ).
Fig. 1.
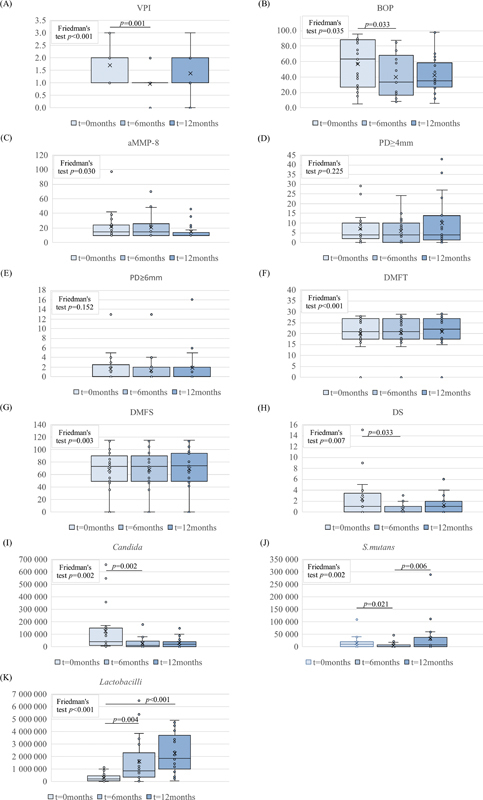
Boxplots of variables included in this study. Time points of recordings (0, 6 months, 1 year) are marked with separate colors on the x-axis. ( A ) Visible plaque index (VPI); ( B ) bleeding on probing (BOP); ( C ) active matrix metalloprotease (aMMP-8); ( D ) periodontal probing depth (PD) more than or equal to 4mm; ( E ) periodontal probing depth (PD) more than or equal to 6mm; ( F ) decayed, missing, filled teeth (DMFT); ( G ) decayed, missing, filled surfaces (DMFS); ( H ) decayed surfaces (DS); ( I ) Candida counts; ( J ) Streptococcus mutans counts; ( K ) lactobacilli counts. Microbial counts are reported as colony forming units/mL on the vertical axis. p -Values are indicated as bars above the boxplots, p < 0.05 was considered significant.
Statistically significant ( p < 0.05) positive correlations at the beginning of the study were found between VPI versus BOP (rho = 0.700), VPI versus PD ≥ 6mm (rho = 0.491), VPI vs S. mutans (rho = 0.423), BOP vs PD≥ 6mm (rho = 0.418), aMMP-8 versus Candida counts (rho = 0.502), aMMP-8 vs Lactobacilli counts (rho = 0.397), DMFT versus DMFS (rho = 0.818), PD≥ 4 versus PD ≥ 6mm (rho = 0.461), PD ≥ 6mm versus Candida counts (rho = 0.413), Candida versus Lactobacilli counts (rho = 0.570), and S. mutans versus Lactobacilli counts (rho = 0.399). During the FLJ mouthwash period, significant repeated measures correlations ( p < 0.05) were found between Candida counts versus DS (rmcorr = 0.572), Lactobacilli counts versus VPI (rmcorr = -0.380), and BOP versus VPI (rmcorr = 0.383). Importantly, nearly significant correlations were found between Lactobacilli versus DMFT (rmcorr = 0.241; p = 0.120), Lactobacilli counts versus BOP (rmcorr = -0.291, p = 0.058), and Lactobacilli versus Candida (rmcorr = 0.287; p = 0.062).
Discussion
The search for the pathogen(s) causing caries has been ongoing for decades and most studies indicate that this multifactorial disease incidence increases due to high carbohydrate diet frequency and the presence of acidogenic microbes (not necessarily S. mutans ), failing of salivary protective properties, vulnerable tooth anatomy, or insufficient manual cleaning of the teeth, resulting in enamel and dentin decay. The main aim is to prevent disease initiation and eventual progress by aiding host defensive mechanisms. The protection of teeth with fluoride has been the most effective established preventive measure against caries. In symbiotic conditions, microbial balance is maintained by host–microbial and microbial–microbial interactions, and even opportunistic pathogens exist side by side. When this balance is disturbed depending on, for example, host immune deficiencies, local excess of carbohydrates, mechanical trauma, or deepened gingival probing depths, increased anaerobic conditions create optimal environments for the dysbiotic and opportunistic pathogen proliferation or activation of specific destructive enzymatic production and cascades. 4 20 23 24 25 The basic building blocks of dentin and periodontium are proteins, and collagens are found in both structures. Minute protein structural difference and the specificity of each microbial proteolytic enzyme may be the determinant by which species will flourish. Several oral microbes, such as Candida , S. mutans , and Porphyromonas gingivalis , possess collagenolytic or basement membrane degrading proteolytic enzymes or have proteins that interact with the host to enhance adhesion and subsequent invasion. 26 On the species level, it is about survival of the fittest, a continuous race for nutrients, living space and beat the host defense mechanisms. According to the current understanding, a symbiotic oral microbiota to maintain or restore oral health is prevalent. 27
In this study, FLJ juice caused statistically significant reductions in Candida and S. mutans levels, and Candida levels remained at a lower level at the 1-year time point. Also, caries incidence (DS) decreased significantly during the mouthwash period and slowly reverted to near study onset level. May Candida yeasts play a more pivotal role in caries? They are also acidogenic and some evidence points to that direction. 28 The caries indexes DMFT/DMFS/DS gave a dissimilar picture of the caries incidence. This is due to the fact that secondary caries findings are concealed if they occur on the same tooth surface as missing or filled surfaces; the same surface is counted only once. Therefore, the authors state that DS gives a more accurate picture of caries incidence. High S. mutans levels have also been found to be coassociated with severe untreated periodontitis. 29 Lactobacilli counts rose significantly in this study during the FLJ period. Lactobacilli are associated and found from carious lesions, and they are acidogenic, but according to this study, no significant correlation was found with caries incidence (DS) and surprisingly, negative correlation with VPI. Lactobacilli has not shown significant upregulation of gene expressions of collagenolytic enzymes in root caries. 30 The advantage in increasing the patient's own Lactobacilli counts is that the effect remained even after the washout period, compared with commercial probiotic Lactobacilli preparations whose colonization is only very short-term. Lactobacilli are proposed to inhibit Candida by competing with niches and adhesion, production of lactic or organic acids, inhibiting inflammation or altering gene expression, 31 and may be beneficial in chemotherapy-related mucositis. 32 Candida and streptococci may have mutualistic interactions in the oral cavity increasing binding or increase drug resistance, as opposed to antagonistic effects of Lactobacilli against Candida . 7
BOP and VPI decreased significantly by FLJ. At the same time, aMMP-8 levels were decreasing that may be indicative of diminished inflammatory and tissue destructive proteolytic burden. The basic metabolism of gingival tissue is based on continuous tissue component remodeling of proteins, but excessive proteolytic and collagenolytic inflammation eventually may cause irreversible tissue damage. Candida yeasts have been proven to be gelatinolytic and Candida glabrata cell wall proteases are able to convert pro-MMP-8 to its active forms in vitro , and this activation was inhibited by FLJ. 21 The chair-side point-of-care aMMP-8 test is a valuable tool to diagnose and follow treatment efficacy and is more precise than BOP in staging and grading of periodontal disease. 19 20 As the key pathogens in periodontitis are not known, scaling and root planning and oral homecare instructing have been the best treatment options. Additional chlorhexidine is applied as adjunctive therapy in difficult cases. Chlorhexidine is a broad-spectrum antiseptic but has multiple side effects and cannot be used for prolonged periods, 33 and there is inconclusive evidence of its effect on lowering S. mutans levels. 34 35 By contrast FLJ does not inhibit the growth of Lactobacilli in vitro or in vivo , and none of the participants in the current and previous studies 16 17 reported any side effects. Lingonberries are known to have antimicrobial, anti-inflammatory, and antioxidant effects. 36 Clinical human trials have shown beneficial effects of FLJ on salivary parameters and reducing xerostomia, 37 and potential inhibition of plaque levels, bleeding on probing, and inflammation in dental implants. 38
Conclusions
This is the first in vivo prospective study to our knowledge of the effects of lingonberries in the oral environment. FLJ seems to offer a safe addition to oral homecare, potentially decreasing visible plaque, BOP, Candida , and S. mutans levels, caries risk as well as periodontal low-grade inflammation and proteolytic tissue destructive aMMP-8 burden in vivo without side effects. The search for identifying culprit microbes causing these diseases is still the ultimate target, and further randomized double-blinded placebo-controlled in vivo studies are required to verify these results.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Stockholm Community, Sweden (2016–08–24/2016/1:8 and 2016–1-24) and the Helsinki University Central Hospital, Finland (360/13/03/00/13 and 51/13/02/2009).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results can be obtained from the authors on request.
References
- 1.Chapple I L, Bouchard P, Cagetti M G et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol. 2017;44 18:S39–S51. doi: 10.1111/jcpe.12685. [DOI] [PubMed] [Google Scholar]
- 2.Peres M A, Macpherson L MD, Weyant R Jet al. Oral diseases: a global public health challenge. [published correction appears in Lancet. 2019 Sep 21;394(10203):1010] Lancet 2019394(10194):249–260. [DOI] [PubMed] [Google Scholar]
- 3.Kleinberg I. A mixed-bacteria ecological approach to understanding the role of the oral bacteria in dental caries causation: an alternative to Streptococcus mutans and the specific-plaque hypothesis. Crit Rev Oral Biol Med. 2002;13(02):108–125. doi: 10.1177/154411130201300202. [DOI] [PubMed] [Google Scholar]
- 4.Tanner A CR, Kressirer C A, Rothmiller S, Johansson I, Chalmers N I. The caries microbiome: implications for reversing dysbiosis. Adv Dent Res. 2018;29(01):78–85. doi: 10.1177/0022034517736496. [DOI] [PubMed] [Google Scholar]
- 5.Banas J A, Drake D R. Are the mutans streptococci still considered relevant to understanding the microbial etiology of dental caries? BMC Oral Health. 2018;18(01):129. doi: 10.1186/s12903-018-0595-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aas J A, Paster B J, Stokes L N, Olsen I, Dewhirst F E. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol. 2005;43(11):5721–5732. doi: 10.1128/JCM.43.11.5721-5732.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Förster T M, Mogavero S, Dräger A et al. Enemies and brothers in arms: Candida albicans and gram-positive bacteria. Cell Microbiol. 2016;18(12):1709–1715. doi: 10.1111/cmi.12657. [DOI] [PubMed] [Google Scholar]
- 8.Gross E L, Beall C J, Kutsch S R, Firestone N D, Leys E J, Griffen A L. Beyond Streptococcus mutans: dental caries onset linked to multiple species by 16S rRNA community analysis. PLoS One. 2012;7(10):e47722. doi: 10.1371/journal.pone.0047722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Paster B J, Boches S K, Galvin J L et al. Bacterial diversity in human subgingival plaque. J Bacteriol. 2001;183(12):3770–3783. doi: 10.1128/JB.183.12.3770-3783.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chen L J, Tsai H T, Chen W J et al. In vitro antagonistic growth effects of Lactobacillus fermentum and lactobacillus salivarius and their fermentative broth on periodontal pathogens. Braz J Microbiol. 2012;43(04):1376–1384. doi: 10.1590/S1517-838220120004000019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Xiao J, Huang X, Alkhers Net al. Candida albicans and early childhood caries: a systematic review and meta-analysis Caries Res 201852(1-2):102–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rosier B T, Marsh P D, Mira A. Resilience of the oral microbiota in health: mechanisms that prevent dysbiosis. J Dent Res. 2018;97(04):371–380. doi: 10.1177/0022034517742139. [DOI] [PubMed] [Google Scholar]
- 13.Ryyti R, Hämäläinen M, Peltola R, Moilanen E. Beneficial effects of lingonberry (Vaccinium vitis-idaea L.) supplementation on metabolic and inflammatory adverse effects induced by high-fat diet in a mouse model of obesity. PLoS One. 2020;15(05):e0232605. doi: 10.1371/journal.pone.0232605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kylli P, Nohynek L, Puupponen-Pimiä R et al. Lingonberry (Vaccinium vitis-idaea) and European cranberry (Vaccinium microcarpon) proanthocyanidins: isolation, identification, and bioactivities. J Agric Food Chem. 2011;59(07):3373–3384. doi: 10.1021/jf104621e. [DOI] [PubMed] [Google Scholar]
- 15.Dróżdż P, Šėžienė V, Pyrzynska K. Phytochemical properties and antioxidant activities of extracts from wild blueberries and lingonberries. Plant Foods Hum Nutr. 2017;72(04):360–364. doi: 10.1007/s11130-017-0640-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pärnänen P.A preparation for balancing the composition of the oral microbial flora. EuroPatent2 585 087 Bl2017 [Google Scholar]
- 17.Pärnänen P, Nikula-Ijäs P, Sorsa T. Antimicrobial and anti-inflammatory lingonberry mouthwash - a clinical pilot study in the oral cavity. Microorganisms. 2019;7(09):331. doi: 10.3390/microorganisms7090331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Alassiri S, Parnanen P, Rathnayake N et al. The ability of quantitative, specific, and sensitive point-of-care/chair-side oral fluid immunotests for aMMP-8 to detect periodontal and peri-implant diseases. Dis Markers. 2018;2018:1.306396E6. doi: 10.1155/2018/1306396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sorsa T, Alassiri S, Grigoriadis A et al. Active MMP-8 (aMMP-8) as a grading and staging biomarker in the periodontitis classification. Diagnostics (Basel) 2020;10(02):61. doi: 10.3390/diagnostics10020061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sorsa T, Sahni V, Buduneli N et al. Active matrix metalloproteinase-8 (aMMP-8) point-of-care test (POCT) in the COVID-19 pandemic. Expert Rev Proteomics. 2021;18(08):707–717. doi: 10.1080/14789450.2021.1976151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pärnänen P, Sorsa T, Tervahartiala T, Nikula-Ijäs P. Isolation, characterization and regulation of moonlighting proteases from Candida glabrata cell wall. Microb Pathog. 2020;149:104547. doi: 10.1016/j.micpath.2020.104547. [DOI] [PubMed] [Google Scholar]
- 22.Bakdash J Z, Marusich L R. Repeated measures correlation. Front Psychol. 2017;8:456. doi: 10.3389/fpsyg.2017.00456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Alfakry H, Malle E, Koyani C N, Pussinen P J, Sorsa T. Neutrophil proteolytic activation cascades: a possible mechanistic link between chronic periodontitis and coronary heart disease. Innate Immun. 2016;22(01):85–99. doi: 10.1177/1753425915617521. [DOI] [PubMed] [Google Scholar]
- 24.Tanner A C. Anaerobic culture to detect periodontal and caries pathogens. J Oral Biosci. 2015;57(01):18–26. doi: 10.1016/j.job.2014.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rosa E, Rymovicz A, Rached R, Grégio A, Silva W, Samaranayake L. Anaerobic enhancement of protease secretion by periodontal Candida albicans strains. Arch Oral Res. 2013;9(02):177–184. [Google Scholar]
- 26.Singh B, Fleury C, Jalalvand F, Riesbeck K. Human pathogens utilize host extracellular matrix proteins laminin and collagen for adhesion and invasion of the host. FEMS Microbiol Rev. 2012;36(06):1122–1180. doi: 10.1111/j.1574-6976.2012.00340.x. [DOI] [PubMed] [Google Scholar]
- 27.Kilian M, Chapple I L, Hannig M et al. The oral microbiome - an update for oral healthcare professionals. Br Dent J. 2016;221(10):657–666. doi: 10.1038/sj.bdj.2016.865. [DOI] [PubMed] [Google Scholar]
- 28.Fakhruddin K S, Perera Samaranayake L, Egusa H, Ngo H C, Pesee S. Profuse diversity and acidogenicity of the candida -biome of deep carious lesions of severe early childhood caries (S-ECC) . J Oral Microbiol. 2021;13(01):1.964277E6. doi: 10.1080/20002297.2021.1964277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Contardo M S, Díaz N, Lobos O, Padilla C, Giacaman R A. Oral colonization by Streptococcus mutans and its association with the severity of periodontal disease in adults. Rev Clín Periodoncia Implantol Rehabil Oral. 2011;4:9–12. [Google Scholar]
- 30.Damé-Teixeira N, Parolo C CF, Maltz M, Rup A G, Devine D A, Do T. Gene expression of bacterial collagenolytic proteases in root caries. J Oral Microbiol. 2018;10(01):1.424475E6. doi: 10.1080/20002297.2018.1424475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zangl I, Pap I J, Aspöck C, Schüller C. The role of Lactobacillus species in the control of Candida via biotrophic interactions. Microb Cell. 2019;7(01):1–14. doi: 10.15698/mic2020.01.702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cereda E, Caraccia M, Caccialanza R. Probiotics and mucositis. Curr Opin Clin Nutr Metab Care. 2018;21(05):399–404. doi: 10.1097/MCO.0000000000000487. [DOI] [PubMed] [Google Scholar]
- 33.Karpiński T M, Szkaradkiewicz A K. Chlorhexidine–pharmaco-biological activity and application. Eur Rev Med Pharmacol Sci. 2015;19(07):1321–1326. [PubMed] [Google Scholar]
- 34.James P, Parnell C, Whelton H. The caries-preventive effect of chlorhexidine varnish in children and adolescents: a systematic review. Caries Res. 2010;44(04):333–340. doi: 10.1159/000315346. [DOI] [PubMed] [Google Scholar]
- 35.Coelho A SEC, Paula A BP, Carrilho T MP, da Silva M JRF, Botelho M FRR, Carrilho E VVF. Chlorhexidine mouthwash as an anticaries agent: a systematic review. Quintessence Int. 2017;48(07):585–591. doi: 10.3290/j.qi.a38353. [DOI] [PubMed] [Google Scholar]
- 36.Pärnänen P, Lähteenmäki H, Tervahartiala T, Räisänen I T, Sorsa T. Lingonberries-general and oral effects on the microbiome and inflammation. Nutrients. 2021;13(11):3738. doi: 10.3390/nu13113738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pärnänen P, Lomu S, Räisänen I T, Tervahartiala T, Sorsa T. Effects of fermented lingonberry juice mouthwash on salivary parameters-a one-year prospective human intervention study. Dent J (Basel) 2022;10(04):69. doi: 10.3390/dj10040069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lähteenmäki H, Tervahartiala T, Räisänen I T, Pärnänen P, Sorsa T. Fermented lingonberry juice's effects on active MMP-8 (aMMP-8), bleeding on probing (BOP), and visible plaque index (VPI) in dental implants-A clinical pilot mouthwash study. Clin Exp Dent Res. 2022;8(06):1322–1330. doi: 10.1002/cre2.638. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data supporting reported results can be obtained from the authors on request.