

Abstract
Jean-Martin Charcot, widely regarded as a leading founder of modern neurology, made substantial contributions to the understanding and characterization of numerous medical conditions. His initial focus was on internal medicine, later expanding to include neuropathology, general neurology, and eventually emerging fields such as neuropsychology and neuropsychiatry. Furthermore, Charcot's intellectual pursuits extended beyond medicine, encompassing research in art history, medical iconography, sociology, religious studies, and the arts, solidifying his status as a polymath.
Keywords: History, Neurology, Neuropathology, Internal Medicine, Psychiatry, Psychology, Polymath
Resumo
Jean-Martin Charcot, amplamente considerado como um proeminente fundador da neurologia moderna, fez contribuições substanciais para a compreensão e a caracterização de várias condições médicas. Seu foco inicial era a medicina interna, expandindo-se posteriormente para incluir a neuropatologia, a neurologia geral e, por fim, campos emergentes como a neuropsicologia e a neuropsiquiatria. Além disso, as buscas intelectuais de Charcot foram além da medicina, abrangendo pesquisas em história da arte, iconografia médica, sociologia, estudos religiosos e artes, solidificando seu status de polímata.
Palavras-chave: História, Neurologia, Neuropatologia, Medicina Interna, Psiquiatria, Psicologia, Polímata
INTRODUCTION
In 2020, Peter Burke, Professor Emeritus of Cultural History at the University of Cambridge, published the book entitled “The Polymath. A cultural history from Leonardo da Vinci to Susan Sontag.” 1 In the introduction to this famous book, the author defined a polymath as “someone who is interested in many subjects and learns many subjects.” Five hundred Western polymaths were presented, including preeminent and controversial physicians such as Erasmus Darwin (1731–1802), Paul Broca (1824–1880), Sigmund Freud (1856–1939) and Oliver Sacks (1933–2015), but interesting omits Jean-Martin Charcot (1825–1893). 1
Apart from being widely considered a leading founder of modern neurology, Charcot's revolutionary ideas about neurological diseases continue to shape the practices of clinicians and scientists to this very day. Furthermore, Charcot's brilliance extended well beyond the realm of neurology, as he was actively engaged in diverse areas of medicine, psychology, arts, politics, diplomacy, religion, and philosophy. 2 3 4 5 This breadth of knowledge and involvement undoubtedly qualifies him as a polymath. 1
The purpose of this article is to briefly present Charcot's main contributions to neurology and beyond.
CHARCOT: A SHORT BIOGRAPHY
Jean-Martin Charcot ( Figure 1 ) was born on November 29, 1825, at 1 rue du Faubourg Poissonnière, 9th arrondissement, Paris, France. His parents were Simon-Pierre Charcot (1798–1863) and Jeanne-Georgette Saussier (1808–1839). He was the eldest of four siblings and was raised in a lower-middle-class artisan family. 2 3 6 7 8 9 Charcot's family background was deeply connected to the manufacture and decoration of carriages, with his father, maternal grandfather, and one of his brothers involved in this trade. 2 3 6 7 8
Figure 1.
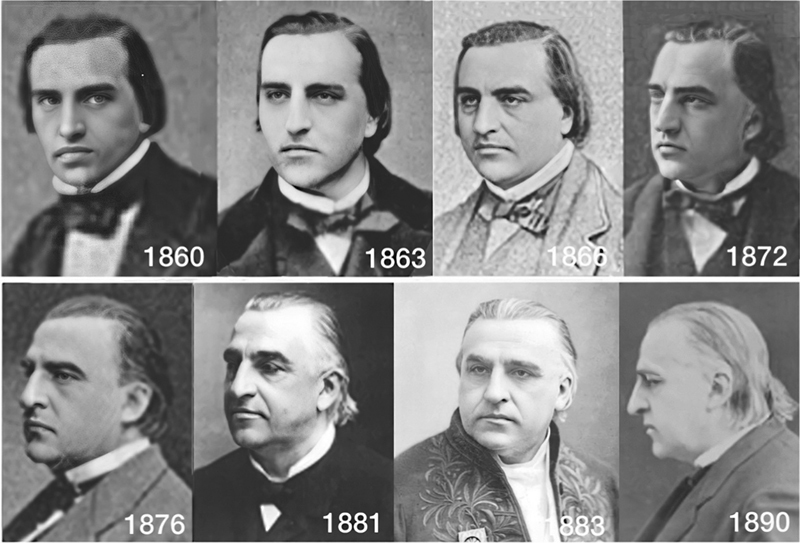
Jean-Martin Charcot (1825–1893). Evolution of Charcot's appearance from his admission to La Salpêtrière (1860) to three years before his death (1890). Public domain ( https://commons.wikimedia.org : 1863, 1872, 1881, 1883) and personal collection (Walusinki: 1860, 1866, 1876, 1890).
During his youth, Charcot was described as a slender individual with long black hair combed back, and he tended to keep to himself, rarely interacting with his peers. 8 At the age of 38, in 1864, Charcot married Augustine-Victoire Laurent (1834–1899), a widow with a 10-year-old daughter named Maria Charlotte Thérèse Durvis (1854–1936). Together, Charcot and Augustine-Victoire had two children: Jeanne Marie Amélie Claudine Charcot (1865–1940) and Jean-Baptiste Charcot (1867–1937). 2 6 7
Charcot pursued his education and graduated in letters before enrolling in the École de Médecine in Paris in 1843. After successfully passing the external competition in December 1845, Charcot was appointed provisional intern in 1847, during which time he earned the admiration and confidence of his mentor, Pierre Rayer (1793–1867). 2 10 Upon Rayer's recommendation, Charcot was appointed as an agrégé (associate professor) at the École de Médecine and introduced to the Societé de Biologie in 1851, which provided him with valuable access to the scientific community. 8
Between 1853 and 1855, Charcot served as a chef de clinique at the Hôpital de la Charité under the leadership of his master Pierre Adolphe Piorry (1794–1879). 8 In May 1856, he was appointed to the Bureau Central of Paris ( médicin des hôpitaux ). 10 In 1857, due to difficulties in expressing himself orally and presenting a controversial thesis on “ De l'expectation en médicine ,” which was deemed insufficient, he failed in his attempt to become an agrégé . Nevertheless, he succeeded in his second attempt in 1860 and assumed the position of agrégé intern of medicine and legal medicine, later being promoted to agrégé in exercise. 8 In 1862, Charcot became the chef de service de La Salpêtrière , and in 1872, he won a public competition for the Chaire d'Anatomie Pathologique . 2 3 6 7 In 1882, he became a clinical professor at the École de Médecine of the University of Paris and assumed the position of Chaire de Clinique des Maladies du Système Nerveux , a role he excelled in until his passing on August 16, 1893. 2 3 6 7
During his tenure, the neurological school at La Salpêtrière gained global recognition as the “Mecca of Neurology.” 2 3 6 7 Charcot's group of pupils included renowned names like Joseph Babiński (1857–1932), and other disciples who also worked in his private practice as secretaries, including Désiré Magloire Bourneville (1840–1909), Charles Féré (1852–1907), Pierre Marie (1853–1940), Paul Richer (1849–1933), Georges Gilles de la Tourette (1857–1904), and Édouard Brissaud (1852–1909). 2 3 11 12 13 14 Additionally, 33 interns were part of Charcot's group at La Salpêtrière between 1862 and 1893, some of whom gained significant prominence in the field of neurology. 11 Many of them are in the world-renowned painting Une Leçon Clinique à La Salpêtriére , from 1887, by André Brouillet (1857–1914) ( Figure 2 ). 12 Internationally acclaimed neurologists sought internships at La Salpêtrière under Charcot's guidance, including James Jackson Putnam (1846–1918), M. Allen Starr (1854–1932), William James (1842–1910), Bernard Sachs (1858–1944), Vladimir M. Bechterew (1857–1927), Liverij O. Darkshevitch (1858–1925), Aleksej Y. Kozhevnikov (1836–1902), Gheorghe Marinescu (1863–1938), and Sigmund Freud. 2 3 4 6 15
Figure 2.
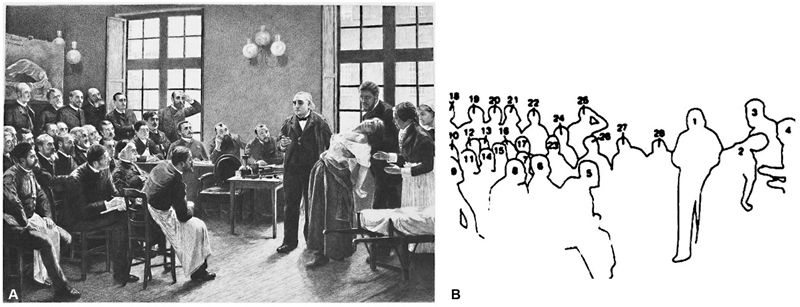
Une Leçon Clinique à La Salpêtriére , from 1887, by André Brouillet. ( A ). A engraved reproduction of Brouillet's painting by Henri Dochy (1851–1915). (Corrêa Neto, personal collection). ( B ). Charcot and other characters of the painting in a drawing with the numbered silhouettes: 1-JM Charcot; 2- Blanche Wittman, the patient; 3- J Babinski; 4- Mlle. Bottard, head nurse; 5- GG de la Tourette; 6- R Vigouroux; 7- H Parinaud; 8- H Berbez; 9- A Londe; 10- G Guinon; 11- L le Bas; 12- A Gombaut; 13- A Arène; 14- J Claretie; 15- A Naquet; 16- Bourneville; 17- G Bellet; 18- V Cornil; 19- P Burty; 20- M Debove; 21- M Durval; 22- JB Charcot; 23- P Berbez; 24- E Brissaud; 25- A Joffroy; 26- P Marie; 27- CS Féré; 28- P Richer.
A noteworthy fact that indirectly underscores Charcot's importance in the Parisian scientific community is his participation as a member of the thesis jury of the École de Médecine in Paris. 16 In the period between 1862 and 1893, a total of 12,500 theses were submitted to the École de Médecine, out of which 3,663 were in the field of neuropsychiatry. 17 Charcot, along with Alfred Vulpian (1826–1887) and Alexandre Axenfeld (1825–1876), were involved in 1,774 of these theses, with Charcot personally participating in 603 of them. 16
The intense scientific production of Charcot, as well as that of his group of disciples at the La Salpêtrière solidified him as the first professor of diseases of the nervous system in the world, as well as the most emblematic neurologist of the 19 th century. 3 4 15 17 18 19 20 Despite not being known for his eloquence, Charcot's lectures were characterized by exceptional clarity and the visual impact of his illustrations. He skillfully engaged his audience, occasionally adding dramatic flair when presenting various classic neurological syndromes. This captivating teaching style was evident both in his Leçons du Mardi (Tuesday lessons), and the scientific meetings held on Thursdays. 2 3 4 15 17 18 19 20
His international fame brought several personalities from Europe, and around the world people to Paris for neurological medical consultations, including the Grand Duke of Russia Vladimir Alexandrovich (1847–1909), the Brazilian Emperor Pedro II (1825–1891), Cardinal Charles Lavigerie (1825–1892), among other political leaders, artists, writers, and philosophers. 2 3 4 5 6 7 21 Furthermore, many of these distinguished personalities frequented Charcot's residence at 217 Boulevard Saint-Germain, especially during winter and spring, where he hosted elegant Tuesday soirées featuring grand receptions and sumptuous dinners. 2 3 4 5 6 7 21
CONTRIBUTIONS TO NEUROLOGY AND NEUROPATHOLOGY
As a professor of pathological anatomy, coupled with his expertise as a neurologist, using the anatomo-clinical method, Charcot made significant contributions to the field of neuropathology. 22 23 24 He was responsible for the original neuropathological descriptions of various neurodegenerative diseases ( Table 1 ). 22 23 24 25 26 27 28 Furthermore, it should be remembered that the coronal section of the brain (“ coupe verticale et transversale du cerveau” ) is known as the “Charcot cut.” 23 29 30
Table 1. Charcot's contributions to neurology, neuropathology, and psychiatry.
| Subject / disease | Partners - year | Contribution | |
|---|---|---|---|
| Neurology and neuropathology | Anatomo-clinical method | Vulpian, Cornil -1862 | Charcot brought new vigor to the clinicopathologic tradition of the Paris school by adding to macroscopic anatomy the new dimension of histology. |
| Charcot-Féré syndrome (ophthalmoplegic migraine) | Féré - 1861 | Charcot, who was a migraineur, and Féré studied eight patients who presented with scintillating scotoma accompanied by changes in ocular motricity. | |
| Tabes dorsalis | Vulpian -1862 | Charcot and Vulpian made a significant breakthrough by establishing a crucial link between specific clinical symptoms and the underlying lesions associated with tabes dorsalis (“ ataxie locomotrice ”). | |
| Parkinson's disease | Vulpian - 1862 | Charcot corrected some of the mistakes in James Parkinson's description, such as the presence of bradykinesia and not paralysis, identified non-motor signs, and with Vulpian coined the term “ Maladie de Parkinson .” | |
| Tremor | Marie - 1862–1893 | He distinguished tremor in degenerative diseases, clinical conditions, intoxication and hysteria. He was the pioneer of treatment with anticholinergics. | |
| Charcot-Bouchard's aneurysms | Bouchard - 1867 | Charcot and Bourchard's study led to the discovery of “aneurysms that developed on intracerebral arterioles” as cause of strokes. | |
| Multiple sclerosis | Vulpian - 1868 | Charcot provided the classic description of “ sclérose en plaques disséminées ” | |
| Amyotrophic lateral sclerosis | 1869–1885 | He described “ sclérose latérale amyotrophique ” (amyotrophic lateral sclerosis), a condition that became known as Charcot's disease | |
| Charcot-Joffroy syndrome | Joffroy -1873 | A rare form of cervical myelopathy known as idiopathic hypertrophic cervical pachymeningitis. It has been described by Charcot and Alix Joffroy in Joffroy's doctoral thesis | |
| Erb-Charcot paralysis | 1876 | A syphilitic myelopathy with sensory and motor symptoms (tabes dorsalis spasmodique). | |
| Charcot cut | 1876 | The coronal section of the brain is known as the “Charcot cut.” | |
| Aphasia | Féré, Marie, Rummo, Bernard, Ballet - 1883 | Charcot created the “bell diagram” describing the circuits of the speech process. | |
| Charcot-Wilbrand syndrome | 1883 | Charcot described a patient with posterior cerebral artery thrombosis who lost the ability to consciously reproduce images from his dreams while awake, although he could still recall dreams of words but not any imagery. | |
| Charcot-Marie-Tooth disease | Marie - 1886 | With Pierre Marie made the initial description of the hereditary sensory-motor peripheral neuropathy. Tooth identified the pathology in the peripheral nerves three months later. | |
| Fugue-poriomania and epilepsies | 1888 | Charcot described a 37-year-old mailman with fugue-poriomania, experiencing three hour-long episodes of wandering around Paris with complete amnesia. This case is now understood as non-convulsive status epilepticus with fugue status, and it significantly contributed to the study of differentiating epilepsy from functional (psychogenic) conditions. | |
| Souques-Charcot geroderma | Jean-Baptist Charcot and Souques - 1891 | The “ géomorphisme cutané ” is a variant of Hutchinson-Gilford progeria, which is characterized by loose, shiny, dry skin, subcutaneous atrophy, eunuchoid habitus, and intellectual deficiency | |
| Psychiatry | Idée fixes | Gille de la Tourette - 1885 | Manifestations of obsessive-compulsive disorder |
| Histeria | Since 1872 | He considered the disease as a result of a dynamic lesion of the brain circuits. Only patients with hysteria could be hypnotized | |
In 1868, Charcot provided the classic description of “ sclérose en plaques disséminées ” (multiple sclerosis), employing the famous anatomo-clinical method, which involves a rigorous semiological evaluation of patients followed by neuropathological studies. He collaborated with his colleague Vulpian on this outstanding description. 26 31 32 33 Similarly, Charcot masterfully described “ sclérose latérale amyotrophique ” (amyotrophic lateral sclerosis) between 1869 and 1885, a condition that became known as Charcot's disease in Europe. 26 34 35 36
In 1886, Charcot and his disciple Pierre Marie made the initial description of the hereditary sensory-motor peripheral neuropathy now recognized as “Charcot-Marie-Tooth disease.” They analyzed five patients and referred to the condition as “ atrophie musculaire progressive ” (progressive muscular atrophy). 27 28 37 Remarkably, three months later, Howard Henry Tooth (1856–1925) presented his thesis for the medical degree in England, entitled “The peroneal type of progressive muscular atrophy,” which clearly identified the pathology in the peripheral nerves. 27 28 38
Charcot played a pivotal role in defining key clinical features of the Parkinson's disease (PD), including bradykinesia and muscle rigidity, which were distinct from the muscle weakness suggested by James Parkinson (1755–1824), another polymath. Charcot's observations also encompassed descriptions of various non-motor symptoms and signs. 33 39 40 41 42 It is essential to recall that Charcot and Vulpian coined the term “ Maladie de Parkinson ,” known earlier as “Shaking Palsy,” in 1862. 39 43 In 1892, Charcot presented a lecture on vibration therapy, discussing his clinical experience with PD using a vibratory chair. The treatment improved sensory symptoms, sleep problems and walking ability, but had limited impact on the tremor associated with PD. Despite Charcot's efforts, the vibrating chair's use for PD was largely disregarded after his passing due to relatively few positive effects observed. 44 45 Furthermore, Charcot's investigations in the study of movement disorders included distinguishing multiple sclerosis tremor from similar manifestations seen in mercury poisoning, and hysteria. Additionally, he was the first to introduce anticholinergic treatment for tremor. 27 39 40 41 42
Charcot conducted extensive research on “aphasia” and delivered lectures at La Salpêtrière , which were later transcribed and published by Charles Féré. 46 47 48 49 50 Gaetano Rummo (1853–1917) translated and transcribed these lectures into Italian, which resulted in the book “ Differenti forme d'aphasia ,” published in 1884. 51 Charcot, known for his ability to make visual representations of complex concepts, received recognition as a “connectionist” or “diagram maker,” including for the remarkable “bell diagram” describing the circuits of the speech process, first presented in Rummo's book ( Figure 3A ). 51 52
Figure 3.
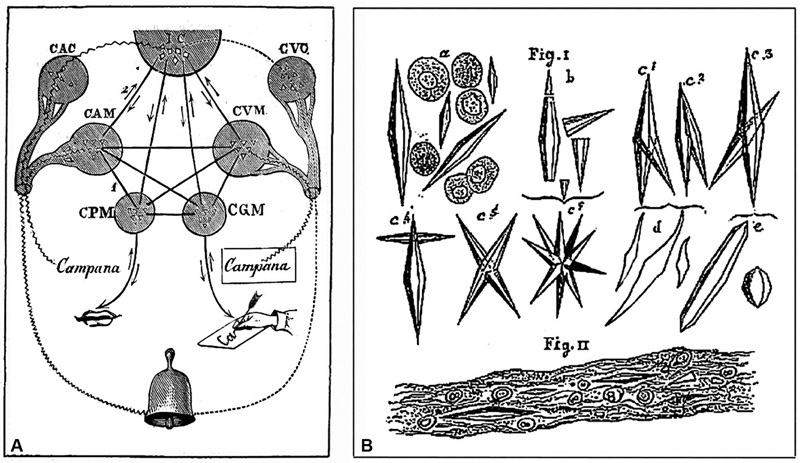
Charcot's drawings for scientific publications. ( A ). Charcot's Bell – Aphasias (Charcot and Rummo, 1884): The bell (campana [cloche]) rings, it is heard and seen. The centers were defined by clinicopathological analysis. Input – auditory input: CAC: center of shared hearing, and CAM: auditory center for words; visual input: CVC: center of shared vision, and CVM: visual center for words. Output – spoken output: CPM: center of articulated language; written output: CGM: center of written language. IC: ideation center. Arrows show the direction of the nervous paths connecting the centers. ( B ). Charcot-Leyden's Crystals (Vulpian and Charcot, 1860).
In collaboration with Charles Joseph Bouchard (1837–1915), Charcot made significant contributions to the understanding of strokes, particularly cerebral hemorrhages. Their study led to the discovery of “aneurysms that developed on intracerebral arterioles.” 53 During the autopsy, Bouchard identified ruptured and intact aneurysms, providing evidence for this pathology, which was later named “Charcot-Bouchard's aneurysms.” 53 54
In addition to his extensive research on various aspects of neurology, Charcot made valuable contributions to the localization of cerebral and spinal cord diseases. 55 He conducted studies on ophthalmoplegic migraine and epilepsies. Charcot's work on ambulatory fugue-poriomania resulted in a classic description of this condition. Charcot-Wilbrand syndrome, identified by a loss of dreaming and visual agnosia, was also a subject of his research. Additionally, he studied Souques-Charcot syndrome, a variant of Hutchinson-Gilford progeria. Charcot also provided a thorough account of Charcot-Joffroy syndrome, a rare form of cervical myelopathy. Furthermore, his investigations led to the characterization of Erb-Charcot paralysis, a condition associated with spinal syphilis that manifests with sensory deficits, spastic paresis, and amyotrophy ( Table 1 ). 2 3 4 15 22 24 55 56 57 58
One of the prominent myelopathies during the 19th century was tabes dorsalis . 3 33 In 1862, during their early collaboration at La Salpêtrière , Charcot and Vulpian made a significant breakthrough by establishing a crucial link between specific clinical symptoms and the underlying lesions associated with tabes dorsalis (“ ataxie locomotrice ”). They observed degeneration or sclerosis of the posterior columns of the spinal cord and atrophy of the posterior spinal roots in affected individuals. 3 59 Around the same time, Lewis A. Sayre (1820–1900) designed a device for suspending patients for scoliosis treatment. Osip Osipovich Motschutkovsky (1845–1903) applied Sayre's method to a scoliosis patient and noticed improvements in tabes dorsalis . 60 Inspired by Motschutkovsky's findings, Charcot assigned Gilles de la Tourette to conduct therapeutic experiments on ataxic patients using suspension therapy. Charcot observed positive results in 14 out of 18 cases, with improvements in walking, balance, pain, and other aspects. 60 61 However, the therapy did not demonstrate objective improvement and had associated risks and fatalities. Despite the uncertainties surrounding its mechanism of action, the treatment remained in use for over a decade due to Charcot's influence before eventually losing popularity. 62
Indeed, Charcot initially believed neurological diseases were hereditary. However, the emergence of the germ theory, championed by Louis Pasteur (1822–1895), in the late 19th century, brought a paradigm shift to French medicine, suggesting microorganisms as disease agents. Charcot was skeptical but not entirely opposed to the new theory, staunchly defending “hereditarianism” for years. 62 In 1882, Jean Alfred Fournier's (1832–1914) association of tabes dorsalis with syphilis marked a turning point, supporting an infectious etiology, contributing to the growing acceptance of the germ theory, including those within Charcot's circle at La Salpêtrière , such as Bouchard and Pierre Marie. 62 63 As a result, Charcot's adherence to hereditarianism and resistance to the new theory led to a certain decline in his political power and influence within French academic circles. 62 64
CONTRIBUTIONS TO NEUROPSYCHOLOGY AND PSYCHIATRY
Charcot's contributions in this area of neuropsychology and psychiatry are numerous, as example, descriptions of the so-called “fixed ideas” (“ idée fixes” ), manifestations of obsessive-compulsive disorder, observed in patients with tics and Tourette's syndrome ( Table 1 ). 2 3 4 15 24 65 66
Charcot's significant contributions to the study of “hysteria” are evident in his research on this clinical condition, now recognized as functional disorders, a term originally coined by Charcot as “neurosis.” 4 15 24 66 67 68 69 Charcot refuted the muscular origin proposed by Pierre Briquet (1796–1881) and disagreed with the traditional “uterine” explanation. Instead, he aligned with the concept of “ovarian hyperaesthesia” suggested by Charles Négrier (1792–1862). 70 71 72 Charcot advocated vigorous compression of the ileo-hypogastric region for the treatment of hysteria and differential diagnosis with epileptic seizures. 70 71 72 73 Nonetheless, neither Charcot nor his disciples formulated any hypotheses explaining the underlying mechanism by which abdominal compression influenced their patients. 70 In the later stages of his life, Charcot underwent a paradigm shift in his understanding of hysteria, conceptualizing the condition as a consequence of dynamic brain circuit lesions. 4 15 24 66 67 68 69
Influenced by Charles Richet's (1850–1935, future Nobel Prize winner in 1913) research on “provoked somnambulism,” Charcot began using hypnosis as a therapeutic tool for hysterics in 1878. 74 75 However, his convictions were not always well accepted by another important research group in this area, the École de Nancy , led by Hippolyte Bernheim (1837–1919). Debates surrounding hypnotism between Charcot's school and the École de Nancy garnered significant public attention, and a well-known crime added to the sensationalistic nature of the discourse. Charcot maintained a viewpoint opposing Bernheim's, asserting that only patients with hysteria could be successfully hypnotized. 74 76 Regrettably, Charcot's approach to discussing hypnosis was combined with pseudoscientific subjects such as clairvoyance and spiritism during his lectures, which drew disapproval from the academic community. 77 78 His research on hysteria and hypnosis at La Salpêtrière influenced Gilles de la Tourette and others, while some of his close disciples, including Féré, Pierre Janet (1859–1947), Alfred Binet (1857–1911), and later Babiński, distanced themselves from the Nancy-Paris controversy. 76 78 79
CHARCOT SEMIOLOGIST
Throughout his career, Charcot presented his cases with rich detail on semiology. He not only described new signs, but also reinterpreted previously described findings. 2 3 6 7 Charcot described what is known as the biliary triad or “Charcot's triad.” 80 The triad is characterized by the presence of recurring abdominal pain in the upper right quadrant associated with fluctuating jaundice and intermittent fever with shivers, and it is associated with the presence of acute cholangitis caused by choledocholithiasis. 80 In patients with sclérose en plaques , the presence of nystagmus, intentional tremor, and dysarthria ( staccato speech) has also become known as “Charcot's triad.” The “Charcot's sign” occurs when there is eyebrow elevation in peripheral facial paralysis. 8 In 1890, Charcot described areas of the body whose compression causes hysteria, the “Charcot's zones.” These areas overlapping fibromyalgia tender points ( Table 2 ). 81
Table 2. Charcot's semiology: signals symptoms and maneuvers.
| Name | Year | Description |
|---|---|---|
| Charcot-Marie's signal | 1883 | Fine, rapid generalized tremor in Basedow-Graves' disease |
| Charcot's vertigo | 1876 | cough-induced dizziness, laryngeal spasm |
| Charcot's signal | ? | Eyebrow elevation in peripheral facial paralysis |
| Charcot's triad I | 1868 | Nystagmus, intentional tremor and dysarthria (“chanted speech”) in multiple sclerosis patients. |
| Charcot's triad II | 1877 | Biliary triad. Presence of recurring abdominal pain in the upper right quadrant associated with fluctuating jaundice and intermittent fever with shivers, and it is associated with the presence of acute cholangitis. |
| Charcot's zones | 1890 | Areas of the body whose compression causes hysteria (Charcot's ovarian point) |
| Clonus | 1862 | “Epileptoid trepidation of the foot” |
| Ear tophaceous | 1860 | Tophaceous deposits in the ear lobes (gout). |
| Charcot's edema | 1892 | Local and very painful edema with a bluish appearance of the extremities, seen in hysterical paralysis. |
| Charcot's intermittent hepatic fever | 1877 | Continuation of Charcot's triad II |
A Charcot's innovation for semiology was the systematic taking of residents' temperatures with a mercury thermometer, rather than simply by hand. His intern for 1868, Bourneville, would make this the subject of his thesis and other subsequent publications. 8 The ocular fundus examination, with an ophthalmoscope, was a new technique invented by Hermann von Helmholtz (1821–1894), in 1851. The importance of fundoscopic examination to the clinical practice of neurology was appreciated by Charcot, who was an early adopter of the ophthalmoscope, and found it useful in some trying differential diagnosis, as in the lecture “ De l'amaurose tabétique” , where he wrote “However, ophthalmoscopy, in this situation, came to bring us a decisive contribution.” 82 83
CONTRIBUTIONS TO INTERNAL MEDICINE
Charcot described many diseases in different areas of internal medicine, causing him to be defined as the “discoverer of diseases” ( Table 3 ). 15
Table 3. Charcot's contributions to internal medicine.
| Subject / disease | Partners - Year | Contribution | |
|---|---|---|---|
| Rheumatology | Gout | Piorry - 1853 | Charcot distinguished gout from chronic rheumatism (rheumatoid arthritis) |
| Garrod- 1867 | Gout in patients with lead poisoning | ||
| Charcot's joint | 1881 | Arthropathy in patients with tabes dorsalis (neurosyphilis) | |
| Charcot's arthopathy | 1868 | Progressive degenerative arthropathy associated with various types of neuropathic diseases, more commonly with diabetes mellitus. “Diabetic Charcot's foot.” | |
| Endocrinology | Basedow-Graves' disease | 1856 | He argued that the cause of the disease was not in the heart, but in the thyroid |
| Hirsch - 1859 | Unlike Trousseau, who coined the eponym Graves' disease, Charcot advocated the eponym Basedow's disease. | ||
| Addison's disease | Vulpian - 1857 | Microscopic findings in the adrenal glands. | |
| Nephrology | Chronic renal insufficiency | 1858 | Retinal damage and thrombosis of the central retinal artery |
| Hematology | Melanemia | 1857 | Charcot recognized this blood change as present in several diseases, such as malaria. It could originate in the spleen, or liver, or kidneys. |
| Charcot-Leyden crystals | Robin -1853 Vulpian -1860 |
Crystals found abundantly in patients with acute leukemia. Later found by Leyden in asthmatic patients. | |
| Angiology | Pulmonary embolism | Ball - 1858 | In a pulmonary embolism case, Charcot described the pathophysiology showed that the clot obstructing the artery was from venous phlebitis of a lower limb. He recognized the elevation of fibrin as a factor promoting clot formation. |
| Intermittent arterial claudication | 1859 | Charcot elucidate the pathophysiological mechanism of ischemia. | |
| Charcot-Weiss-Baker syndrome | 1872 | He described a type of syncope triggered by coughing as well as syncope triggered by compression of the carotid sinus. | |
| Infectiology | Parasitosis | Davaine - 1852 | They presented cases of hydatidosis and echinococcosis. |
| Gangrenous dissecting pneumonia | Ball - 1860 | They envisioned septic emboli before the era of microbiology. | |
| Typhoid fever | Vulpian - 1862 | Description of valvular damage, particularly tricuspid. | |
His doctorate thesis, defended at the University of Paris in 1853, focused on the “ Goutte Asthénique Primitive, Nodosités de Jointures, Rhumatisme Articulaire Chronique” , providing a classical description of progressive chronic rheumatism and differentiating it from cases of gout, under the chairmanship of Piorry. 2 3 4 8 84 His talents as a draftsman are revealed in the plate of hands with deformed fingers illustrating his thesis ( Figure 4 ). 8 Throughout his career, Charcot remained knowledgeable about rheumatic diseases and gout, and in 1863, he reported Alfred Baring Garrod's (1814–1917) observation of the high frequency of gout in those with previous signs of lead intoxication. 8 85 Additionally, Charcot described an arthropathy in patients with tabes dorsalis , known worldwide as “Charcot's joint,” and another articular disease related to diabetic foot arthropathy, referred to as “Charcot's arthropathy” or “diabetic Charcot's foot,” which is associated with various types of neuropathic diseases, but which is undoubtedly much more common in patients with diabetes mellitus. 2 3 4 20 84 This condition predominantly affects the feet, leading to structural deformities and the risk of ulcers and even osteomyelitis. 2 3 4 84 86 87 88
Figure 4.
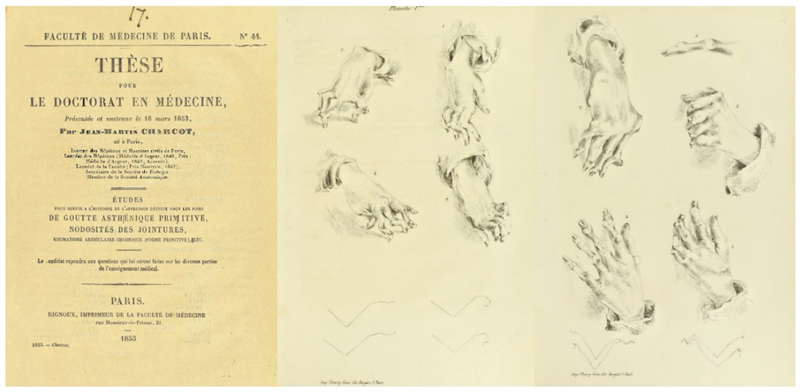
Charcot's thesis, defended at the Faculty of Medicine at the University of Paris in 1853. Charcot drew the joint deformities to illustrate his doctoral thesis. (Charcot, 1853).
In 1835, Robert James Graves (1796–1853) described cases of tachycardia and thyroid enlargement in young women, attributing them to a cardiac lesion and creating the cardio-vascular theory with William Stokes (1804–1878). 89 In 1840, Carl A. von Basedow (1799–1854) associated palpitation of the heart, exophthalmos, and goitre, known as the Merseburg Triad, and suggested a cause related to a “dyscrasia of the blood.” 90 In 1856, Charcot presented a case series of this disease, rejecting the cardiac cause and focusing on structural changes in the thyroid arteries. He proposed increased gland activity due to vasomotor nerve stimulation. In 1859, he reported a case with a fatal meningeal hemorrhage completing the disease's evolution. Charcot also described different tremors in the disease, leading to the term “Charcot-Marie's signal.” 8 Armand Trousseau (1801–1867) admired Graves and Stokes, using the term “Graves' disease” in his clinical lectures. 8 When Graves' textbook was translated into French, Trousseau wrote the foreword in which he commended to readers the work of Graves and indeed first used the term “Graves' disease.” 89 In contrast, Charcot followed the Germanic school and endorsed August Hirsch's (1817–1894) proposal to name the condition “Basedow's disease.” This eponym is still used in non-Anglophone countries to this day. 8
With Vulpian, Charcot presented an observation of Addison's disease to the Société de Biologie in 1857. Macroscopically, the adrenal glands appeared normal, but microscopic observation showed degeneration: “after the ordinary symptoms of Addison's disease, the adrenal capsules would be given as healthy, without having been examined under the microscope or treated with suitable reagents. From the point of view of theory, this should be regarded as untrue.” 8
The use of the microscope, for which Charcot always had great enthusiasm, also contributed to his important discoveries. In 1857, he published an article on “ melanemia ” where he identified colored corpuscles derived from the regressive metamorphosis of red blood cells in certain pathological conditions. He attributed melanemia to the spleen and liver's activity and associated it with nephritis in malarial fever cases. However, Charcot rejected melanemia as the cause of neuropsychic disorders during malaria and wondered whether it should be considered a symptom or a disease, mainly focusing on its relation to fevers. 8
In 1853, Charcot and Charles Philippe Robin (1821–1885) presented a case of acute leukemia to the Société de Biologie . During the autopsy, Robin noted that in the blood of the right ventricle, there was a large quantity of blood crystals, which were very regular in shape and slightly colored yellowish-red. These crystals were also found abundantly in the spleen tissue, forming considerable clusters visible only under the microscope. In 1860, Charcot and Vulpian, referring to another leukemia case, described these crystals as “very elongated octahedrons, very regular in shape and fairly uniform,” measuring 6 to 8 μm ( Figure 3B ). 91 These crystals later became known as Charcot-Leyden crystals in honor of Charcot and Robin's 1853 description, with the addition of the name of Ernst Victor von Leyden (1832–1910), who identified them in the sputum of asthmatics in 1872. 92 Similarly, Charcot-Neumann crystals, which contain phosphate crystals, were described in semen. 4
Intermittent claudication of arterial origin (“ claudication intermitente par oblitération artérielle” ), originally described by Charcot (“Charcot's intermittent claudication ” ), is characterized by the presence of pain, discomfort, weakness, or leg cramps, mainly after physical exercise or walks and disappear after rest. 84 93 94 Charcot described this disease in detail in a soldier who had been injured by a firearm and who developed an aneurysm that formed a thrombus blocking the iliac arteries. 84 93 94 95 96 He based his study on the description, published in an article in 1831 by the Parisian veterinary surgeon, Jean-François Bouley, of claudication in a horse that pulled a carriage through the streets of Paris and had difficulty using its hind feet whenever it had to exercise more strenuously. The animal presented thrombi obstructing the femoral arteries. 95
François-Amilcar Aran (1817–1861) wrote his dissertation in 1853 on the causes of sudden death, including pulmonary embolism, but without specifying its pathophysiology. Benjamin Ball (1833–1893) and Charcot showed in 1858 that the origin of the clot obstructing the pulmonary artery was venous phlebitis of a lower limb. Charcot recognized the elevation of fibrin as a factor favoring clot formation, even though the physiology of hemostasis was still in limbo. He noted the higher frequency of these diseases in young people, especially with a traumatic injury. 8
Another contribution related to the field is Charcot's edema, a painful and bluish edema described in women with hysterical paralysis. 84 93 Charcot gave a detailed description of vasovagal syncope, which is characterized by transitory attacks of significantly reduced heartbeat, reduced arterial pressure, and loss of consciousness. 84 Then, in 1872, he helped clarify a syncope triggered by coughing, by compression of the carotid sinus (carotid sinus hypersensitivity syndrome), described by Johann Nepomuk Czermak (1828–1873) in 1866. Its pathophysiology was comprehensively described by Soma Weiss (1898–1942) and James Porter Baker (1902–1988). 97 This syndrome is also known as the Charcot-Weiss-Baker syndrome. 84 88 Furthermore, Charcot conducted investigations on sore pressure. 98
Charcot made significant contributions to various areas of internal medicine, including nephrology and infectology ( Table 3 ). In his early lessons, he discussed fever, conditions like la gravelle biliaire, pneumonia, and more, without the knowledge of microbiology, which had not yet been established. Charcot and Ball presented a case in 1860 of a woman with heart failure and mitral stenosis who underwent puncture for ascites. Unfortunately, the procedure led to complications, including erysipelas and gangrenous necrotic tissue, resulting in her death. They used the term “gangrenous dissecting pneumonia,” introduced by the German Hermann Lebret (1813–1878) in 1845, envisioning septic emboli before the era of microbiology, suggesting the spread of septic liquids from a primitive focus or blood clots carrying gangrenous fluid. 8
He can also be considered to have pioneered the study of diseases of the elderly, although his contributions in the fields of geriatrics and gerontology are scarce, focusing mainly on gout and chronic rheumatism. 31 99 100 He was also one of the pioneers in establishing rehabilitation clinics with physiotherapy, speech therapy, hydrotherapy, and electrical stimulation of paralyzed muscles. 3
CHARCOT: AN INTELLECTUAL
In his book published in 1988, Paul Johnson, defines intellectuals, presents a series of them, and highlights their moral qualifications, capacity for discernment, and characteristics that qualify them to guide humanity. 101 Charcot had all the basic characteristics for be defined as an intellectual. In parallel with his scientific activities, Charcot had a great appreciation for the arts in general and vast literary and artistic aptitude, and he was also fluent in five languages. 2 3 4 5 6 7 102 103 104 105
He was a man of strong personality and his features emanated a respectable figure. Charcot may be defined as austere, reserved, introvert, taciturn, shy, authoritarian, associated with a competitive temperament, permeated by a skepticism in relation to the treatment of many neurological diseases, and sometimes, with expressions of irony and even sarcasm, in the relationship with other neurologists, and, paradoxically, an intense love for animals. 2 3 105 106 107 108 109 110
Charcot's characteristics regarding the arts, in particular painting and sculpture, were quite eclectic. 2 3 6 7 He had great admiration for the sculpture of ancient Greece, Italian paintings of the Renaissance period, as well as Belgian and Dutch paintings. 2 One of his favorite painters was Delacroix. 2 Although Charcot lacked the ability to play musical instruments, he had an exceptional taste for music. His favorite classical composers were Mozart, Beethoven, Rameau, Gluck, as well as César Franck and Hector Beriloz. 2 3 6 7 In the area of literature, he knew all of Shakespeare's works, of which he was a great admirer and claimed him as his favorite writer. Charcot had a great interest in the area of philosophy, and liked the classic Greek and Latin books, particularly by Plato and Seneca. 2 3 6 7
Even though he was not politically engaged, Charcot had liberal ideas, and even though he was tolerant in religious matters, he was clearly anti-clerical. 3 106 111 Nevertheless, his wake in the chapel of the La Salpêtrière and burial in the Montmartre cemetery were performed within Catholic norms. 2 3 6 7 111 112 Some biography data suggest that Charcot, in the final phase of his life, came to admire Buddhism. 113
CHARCOT: THE ARTIST
Charcot's inherent artistic abilities were a result of his exceptional visual perception and prodigious memory, as documented in various works throughout his career. 2 3 6 7 102 103 104 105 Notably, one of his disciples, Henry Meige (1866–1940), published a book in 1925 titled “ Charcot Artist ,” wherein he showcased a collection of original drawings by Charcot. These drawings encompassed environments, landscapes, family members, colleagues, church sculptures, and several caricatures, some of which exhibited a sense of self-ridicule. 104 The book “ Charcot - Une vie avec l'image ,” published by Catherine Bouchara in 2013, provided substantial insight and a comprehensive perspective. It also presented numerous drawings by Charcot, showcasing his astute observation of patients' postures and neurological signs, always correlated using the renowned anatomo-clinical method. The book featured various drawings of patients with hysteria, family members, in particular his son, Jean-Baptiste and daughter, Jeanna, landscapes from his international travels, and several caricatures. 105
Charcot's own book titled “ Huit jours au Maroc ” (“Charcot in Morocco”) chronicled his trip to Morocco in 1887 and contained numerous drawings, featuring landscapes and local characters, notably from the Jewish community. 102 114 Furthermore, Charcot authored an article later compiled into a book titled “ La foi qui guérit ” (“Faith Healing”). 115 Contrary to his prior skepticism regarding neurological disease treatments, Charcot objectively explored the significance of faith as an auxiliary element in treating patients with neurological ailments. He included conversion pictures related to hysteria, which foreshadowed the later development of psychosomatic medicine. 115
Charcot collaborated with his assistant Paul Richer on the book “ Les Démoniaques dans l'Art ,” published in Paris in 1887. 103 This work, illustrated by Richier, depicted hysterical symptoms in religious and religious art, including Charcot's descriptions of hysteria in religious contexts and his “hysterical saints.” It also explored Charcot's contributions to the field of functional disorders and their implications. 103 116 Another joint publication by Charcot and Paul Richer in 1889 was “ Les Difformes et le Malades dans l'Art ” (“The deformed and diseases in art”), further discussing the intersection of science and art. 117
Moreover, Charcot actively encouraged his disciples, such as Bourneville and Paul-Marie-Léon Regnard (1850–1927), to share the neurological findings of their group at La Salpêtrière through various journals. The “ Iconographie Photographique de la Salpêtrière ,” created in 1876, particularly emphasized hysteria, and later, the “ Nouvelle Iconographie de la Salpêtrière ” covered a wider range of neurological diseases. 3
Charcot Caricaturist
Charcot's relationship with various aspects of art in general, which at first started as a hobby and later became more scientific, also turned toward caricature. 102 104 105 In this area, his works demonstrate significant artistic skills, which are clearly evident in Henry Meige's book entitled “ Charcot Artiste” and the more recent text by Catherine Bouchara entitled “ Charcot - Une vie avec l'image” . 104 105 In 2021, Teive et al. 102 published a historical note to discuss the artistic side of Charcot through his caricatures. This historical note briefly describes eight caricatures during the second half of the nineteenth century in Paris, demonstrating his artistic gifts blended with humor, satire, irony and sarcasm. 102 Figure 5 fully demonstrate these characteristics.
Figure 5.
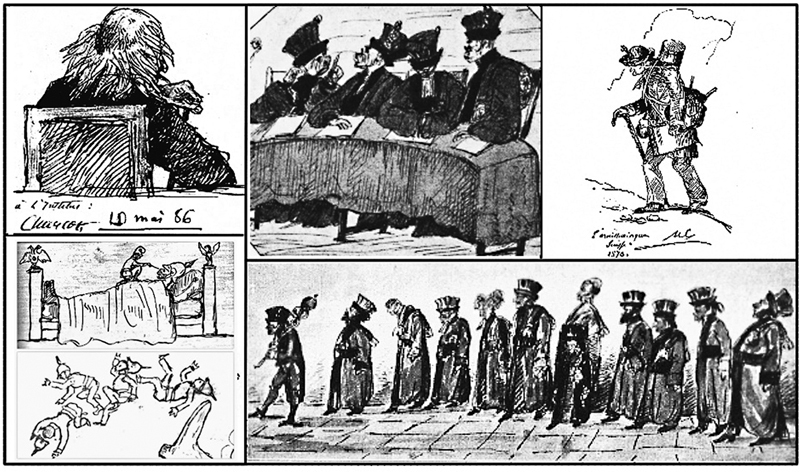
Caricatures by Charcot. Clockwise from top: (1) Professor Michel Eugene Chevreul (1786–1889) during Charcot's visit to a Tuesday session at the Academy of Sciences in Paris around 1885; (2) “The Areopagus,” Charcot drew his medical school colleagues as apes; (3) An old companion from his youth nicknamed “Platypus,” on an excursion in the mountains of Switzerland; (4) Faculty procession: his colleagues at the Paris medical school in pompous costumes during a procession; (5) The final two images portray his indignation during the Franco-Prussian war (1870): the first is untitled, depicting a tiny French soldier atop an enormous, inert Prussian one, and the second he called “ L'Avenir ” (“The Future”). Source: Walusinski, personal collection.
CHARCOT: THE LOVER AND PROTECTOR OF ANIMALS
Charcot was known for his strong sensitivity toward animals and was against hunting and bullfighting due to the unnecessary cruelty inflicted on animals. Charcot's compassionate nature extended to his love for animals, and he treated them with tenderness and care. 6 7 108 109 Guinon 6 reported the scene of Charcot being seen threateningly running behind a duck to catch a frog trapped in its beak.
In his personal life, Charcot had two dogs and a small female monkey named Rosalie, given to him as a gift by Pedro II, the Emperor of Brazil. He developed a close bond with Rosalie, and she would join him at the table during his meals. Charcot would ensure she had enough food and delighted in her playful antics, finding joy when she grabbed nuts or bananas from his plate. The presence of animals, particularly dogs, was a constant in Charcot's home at 217 Boulevard Saint-Germain in Paris. 2 6 7 109 110
Charcot's approach to scientific research was distinct from his contemporaries. He firmly opposed vivisection and experiments involving animals at La Salpêtrière , where most of his neuroanatomical and neuropathological studies were based on human autopsies. 3 6 7 109 110 His stance against animal experimentation was evident in his office, where a sign painted by his wife clearly stated, “You will find no dog laboratory here.” 3 6 7 108 109 This sign symbolized his strong conviction against the use of animals for experimental purposes. Despite his dedication to human autopsies and his contributions to the field of neurology, Charcot's opposition to vivisection received criticism from some members of the scientific community, especially those associated with the École de Médecine . 62
DEATH
Two months following his tiring and counterintuitive journey to England, his wife asked him to rest, as his angina attacks were becoming more frequent. Charcot embarked on a cultural expedition with two of his pupils Isidore Straus (1845–1896) and Maurice Debove (1845–1920) to Vezelay and its basilica, in Burgundy. Tragically, on August 16th, 1893, at three o'clock in the morning, he experienced a severe pulmonary edema as a consequence of cardiac insufficiency secondary to myocardial necrosis. He passed away in a modest guesthouse located by the lake des Settons. Among his co-morbidities were obesity, heavy smoking, and lombalgia. 2 3 With his demise, the world lost the esteemed “ César de la Faculté ,” the renowned “ Napoleon des névroses ,” and the venerable “father of Neurology.” 3 62 118
In conclusion, the celebration of the 200th anniversary of the birth of Jean-Martin Charcot is approaching, and it is scheduled to take place with great dignity in Paris in 2025 during the annual meeting of the International Society for the History of the Neurosciences ( www.charcot2025.fr ). It is important to remember his numerous contributions to internal medicine, neurology, neuropathology, neuropsychology and neuropsychiatry. These accomplishments, in addition to his recognized and expressive artistic production and socio-cultural influence, certainly deserve him the acknowledgment as a polymath.
Conflict of Interest There is no conflict of interest to declare.
Authors' Contributions
CHFC: conceptualization, methodology, project administration, supervision, validation, visualization, writing – original draft, writing – review & editing; LC: validation, visualization, writing – original draft; YCN, EE: conceptualization, supervision, validation, visualization, writing – review & editing; PMF: validation, visualization, writing – review & editing; OW: conceptualization, validation, visualization, writing – review & editing; HAGT: conceptualization, methodology, project administration, supervision, validation, visualization, writing – original draft, writing – review & editing.
References
- 1.Burke P.The polymath: a cultural history from Leonardo da Vinci to Susan Sontag New Haven and London, Yale University Press; 2020, ISBN 9780300250022 [Google Scholar]
- 2.Guillain G JM. New York: Paul B. Heber; 1959. Charcot: his life-his work; pp. 16–29. [Google Scholar]
- 3.Goetz C G, Bonduelle M, Gelfand T. New York: Oxford University Press; 1995. Charcot: Constructing neurology; pp. 268–304. [Google Scholar]
- 4.Poirier J.Jean-Martin Charcot (1825–1893): sa personne, sa personnalité, son personnageNeurologie Libérale 2013; 03–Juillet-août- septembre
- 5.Bogousslavsky J, Boller F. Jean-Martin Charcot and art: relationship of the “founder of neurology” with various aspects of art. Prog Brain Res. 2013;203:185–199. doi: 10.1016/B978-0-444-62730-8.00007-4. [DOI] [PubMed] [Google Scholar]
- 6.Guinon G. Charcot Intime. Paris Med (Paris) 1925;•••:511–516. [Google Scholar]
- 7.Souques A. Charcot Intime. Presse Med. 1925;•••:693–698. [Google Scholar]
- 8.Rodegher A C. Campinas: Universidade Estadual de Campinas, Instituto de Filosofia e Ciências Humanas; 2021. O Olho Clínico: Charcot e a conformação da imagem na produção da Iconografia Fotográfica da Salpêtrière [Dissertation - MSc] [Google Scholar]
- 9.Harris R. London: Tavistock; 1991. Introduction. [Google Scholar]
- 10.Walusinski O. Les facettes peu connues de l'oeuvre de Jean-Martin Charcot (1825–1893) Hist Sci Med. 2022;4:375–390. [Google Scholar]
- 11.Walusinski O. Oscitatio, Brou: 2021. Les 33 internes de Jean-Martin Charcot à la Salpêtrière de 1862 à 1893. [Google Scholar]
- 12.Walusinski O. Oscitatio, Brou: 2021. Une leçon clinique à la Salpêtrière. André Brouillet (1857–1914). Une peinture de la neurologie autour de Charcot. [Google Scholar]
- 13.Walusinski O. Karger, Montreaux: 2011. Jean-Martin Charcot's house officers at la Salpêtrière hospital; pp. 9–35. [DOI] [PubMed] [Google Scholar]
- 14.Teive H AG, Germiniani F MB, Munhoz R P, Walusinski O. Charcot's famous secretaries. Arq Neuropsiquiatr. 2017;75(05):320–323. doi: 10.1590/0004-282X20170034. [DOI] [PubMed] [Google Scholar]
- 15.Lellouch A.[Charcot, discoverer of diseases] Rev Neurol (Paris) 1994150(8-9):506–510. [PubMed] [Google Scholar]
- 16.Walusinski O. Brou: Oscitatio; 2020. Jean-Martin Charcot membre de jurys de thèses à la Faculté de Médicine de Paris (1862–1893) [Google Scholar]
- 17.Gomes MdaM, Engelhardt E. Jean-Martin Charcot, father of modern neurology: an homage 120 years after his death. Arq Neuropsiquiatr. 2013;71(10):815–817. doi: 10.1590/0004-282X20130128. [DOI] [PubMed] [Google Scholar]
- 18.Goetz C G. New York: Raven Press; 1987. Charcot. The Clinician. The Tuesday lessons. [Google Scholar]
- 19.Sigerson G. New York: Hafner Publishing Company; 1962. Lectures on the diseases of the nervous system by J-M Charcot. [Google Scholar]
- 20.Lellouch A. [Charcot's epistemological concept] Hist Sci Med. 1994;28(04):297–305. [PubMed] [Google Scholar]
- 21.Teive H AG, Almeida S M, Arruda W O, Sá D S, Werneck L C.Charcot and Brazil Arq Neuropsiquiatr 200159(2A):295–299. [DOI] [PubMed] [Google Scholar]
- 22.Goetz C G. Chapter 15: Jean-Martin Charcot and the anatomo-clinical method of neurology. Handb Clin Neurol. 2010;95:203–212. doi: 10.1016/S0072-9752(08)02115-5. [DOI] [PubMed] [Google Scholar]
- 23.Bonduelle M.[Charcot, anatomo-pathologist] Arch Anat Cytol Pathol 199442(3-4):171–180. [PubMed] [Google Scholar]
- 24.Jay V. The legacy of Jean-Martin Charcot. Arch Pathol Lab Med. 2000;124(01):10–11. doi: 10.5858/2000-124-0010-TLOJMC. [DOI] [PubMed] [Google Scholar]
- 25.Corcia P, Meininger V. Grey Matter 150th anniversary of Charcot's description of amyotrophic lateral sclerosis. Brain. 2019;142(10):3306–3313. doi: 10.1093/brain/awz280. [DOI] [PubMed] [Google Scholar]
- 26.Zalc B. One hundred and fifty years ago Charcot reported multiple sclerosis as a new neurological disease. Brain. 2018;141(12):3482–3488. doi: 10.1093/brain/awy287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kazamel M, Boes C J. Charcot Marie Tooth disease (CMT): historical perspectives and evolution. J Neurol. 2015;262(04):801–805. doi: 10.1007/s00415-014-7490-9. [DOI] [PubMed] [Google Scholar]
- 28.Sturtz F G, Chazot G, Vandenberghe A J. Charcot-Marie-Tooth disease from first description to genetic localization of mutations. J Hist Neurosci. 1992;1(01):47–58. doi: 10.1080/09647049209525514. [DOI] [PubMed] [Google Scholar]
- 29.Charcot J-M. Paris: Progrès Médical; 1876. Leçons sur les localisations dans les maladies du cerveau et de la moelle épineière. [Google Scholar]
- 30.Gwenaelle I, Plaisant O, Alexis Guédon A. Étude des coupes dites “de Charcot” et “de Flechsig”: des descriptions princeps au recalage dans le BigBrain. Morphologie. 2019;103(342):118. doi: 10.1016/j.morpho.2019.09.027. [DOI] [Google Scholar]
- 31.Charcot J M, Ball B. Paris: Adrien Delahaye; 1874. Leçons Cliniques sur les Maladies des Vieillards et les Maladies Chroniques. [Google Scholar]
- 32.Charcot J M.Des scléroses de la moelle épinière. Histologie de la sclérose em plaques. Gazette des hôpitaux civils et militaires (Lancette française) 186841415–416., 554–555, 557–558, 566–567 [Google Scholar]
- 33.Charcot J M. Paris: Bureaux du Progrès Médical; 1888. Œuvres complètes. Tome I. [Google Scholar]
- 34.Charcot J-M.De la sclérose latérale amyotrophique Prog Med (Paris) 187423325–326., 341–342, 421–423, 453–455 [Google Scholar]
- 35.Charcot J, Joffroy A.Deux cas d'atrophie musculaire progressive avec lésions de la substance grise et des faisceaux antéro-latéraux de la moelle epiniere Arch Physiol Norm Pathol 18692354–367.,629–649,744–769.https://gallica.bnf.fr/ark:/12148/bpt6k432734s# [Google Scholar]
- 36.Charcot J-M, Marie P.Deux nouveaux cas de sclérose latérale amyotrophique suivis d'autopsie Arch Neurol 188510281–35., 168–186 [Google Scholar]
- 37.Charcot J M, Marie P. Sur une forme particulière d'atrophie musculaire progressive: souvent familiale débutant par les pieds et les jambes et atteignant plus tard les mains. Rev Med (São Paulo) 1886;6:97–138. [Google Scholar]
- 38.Tooth H H. Cambridge: University of Cambridge; 1886. The peroneal type of progressive muscular atrophy [Thesis – MD] [Google Scholar]
- 39.Teive H AG. [Charcot's contribution to Parkinson's disease] Arq Neuropsiquiatr. 1998;56(01):141–145. doi: 10.1590/s0004-282x1998000100026. [DOI] [PubMed] [Google Scholar]
- 40.Walusinski O.Jean-Martin Charcot and Parkinson's disease: Teaching and teaching materials Rev Neurol (Paris) 2018174(7-8):491–505. [DOI] [PubMed] [Google Scholar]
- 41.Teive H AG, Munhoz R P. Postural instability in Parkinson's diasese – 120 years after Charcot's death. Arq Neuropsiquiatr. 2014;72(08):636–639. doi: 10.1590/0004-282X20140085. [DOI] [PubMed] [Google Scholar]
- 42.Teive H AG, Zavala J A, Iwamoto F M, Sá D, Carraro H, Jr, Werneck L C.[Contributions of Charcot and Marsden to the development of movement disorders in the 19th and 20th centuries] Arq Neuropsiquiatr 200159(3-A):633–636. [PubMed] [Google Scholar]
- 43.Charcot J M, Vulpian A. Paris: Victor Masson et Fils; 1862. De la paralysie agitante. [Google Scholar]
- 44.Charcot J M. La médicine vibratoire: application des vibrations rapides et continues au traitement de quelques maladies du syste'me nerveux. Prog Med (Paris) 1892;16:149–151. [Google Scholar]
- 45.Goetz C G. Jean-Martin Charcot and his vibratory chair for Parkinson disease. Neurology. 2009;73(06):475–478. doi: 10.1212/WNL.0b013e3181b1640b. [DOI] [PubMed] [Google Scholar]
- 46.Charcot J M. Des différentes formes de l'aphasie. (Leçon recueillie par Ch. Féré) Prog Med (Paris) 1883;11(23):441–444. [Google Scholar]
- 47.Charcot J M. Des différentes formes de l'aphasie. (Leçon recueillie par Ch. Féré) Prog Med (Paris) 1883;11(24):469–471. [Google Scholar]
- 48.Charcot J M. Des différentes formes de l'aphasie. (Leçon recueillie par Ch. Féré) Prog Med (Paris) 1883;11(25):487–488. [Google Scholar]
- 49.Charcot J M. Des différentes formes de l'aphasie. (Leçon recueillie par Ch. Féré) Prog Med (Paris) 1883;11(27):521–523. [Google Scholar]
- 50.Charcot J M. Des différentes formes de l'aphasie. (Leçon recueillie par Ch. Féré) Prog Med (Paris) 1883;11(44):859–861. [Google Scholar]
- 51.Charcot J M, Rummo G. Milano: Vallardi; 1884. Differenti forme d'afasia: lezioni fatte nella Salpetriere nel semestre d'estate dell'anno 1883. (Redatte col consenso dell'autore dal Dr G Rummo) [Google Scholar]
- 52.Engelhardt E, Gomes M M. Charcot and aphasia: contributions of his assistants. Rev Bras Neurol. 2015;51(03):84–88. [Google Scholar]
- 53.Bouchard C J. Paris: F. Savy; 1867. Étude sur quelques points de la pathogénie des hémorrhagies cérébrales. [Google Scholar]
- 54.Akmal S, Jumah F, Ginalis E E, Raju B, Nanda A. Charles Jacques Bouchard (1837-1915) and the Charcot-Bouchard aneurysm. J Neurosurg. 2021;136(05):1470–1474. doi: 10.3171/2021.4.JNS21583. [DOI] [PubMed] [Google Scholar]
- 55.Charcot J M.Leçons sur les localisations dans les maladies du cerveau et de la moelle épinière. Recueillies et publiées par Bourneville D-M et Brissaud E. Progrès Médical Paris: Lecrosnier & Babe; 1876. –1880 [Google Scholar]
- 56.Charcot J M. Contribution à l'étude clinique de la migraine ophthalmoplégique. Rev Neurol (Paris) 1897;5(08):217–222. [Google Scholar]
- 57.Pollola E, Israel A, Gersellas A C. [On an atypical case of recurrent paralysis of the oculomotor nerve (Charcot's ophthalmoplegic migraine)] Arq Bras Oftalmol. 1966;29(04):101–104. [PubMed] [Google Scholar]
- 58.Lapresle J, Desi M. [Painful ophthalmoplegia (author's transl)] Acta Neurol Belg. 1977;77(06):331–350. [PubMed] [Google Scholar]
- 59.Charcot J M, Vulpian A. Sur deux cas de sclérose des cordons postérieurs de la moelle avec atrophie des racines postérieures (Tabes dorsalis, Romberg, ataxie locomotrice progressive, Duchenne de Boulogne) CR Séances Mem Soc Biol. 1862;4:155–173. [Google Scholar]
- 60.Weiner M F, Silver J R.Historical review: suspension therapy for the treatment of tabes dorsalis Eur Neurol 201472(3-4):163–172. 10.1159/000360620 [DOI] [PubMed] [Google Scholar]
- 61.Charcot J M. Paris: Lecrosnier & Babe; 1889. Du Traitement de l'Ataxie Locomotrice par la Suspension suivant la Méthode du Dr Motchoutkowsky. Leçons du Mardi à la Salpétriêre. Leçon du 15 Janvier 1889. Progrès Médical; p. 579. [Google Scholar]
- 62.Brais B. London; University College London; 1990. The making of a famous nineteenth century neurologist Jean-Martin Charcot (1825–1893) [Thesis – PhD] [Google Scholar]
- 63.Fournier A. Paris: Masson; 1882. De l'ataxie locomotrice d'origine syphilitique. Leçons cliniques professées à l'Hôpital Saint-Louis. [Google Scholar]
- 64.Iragui V J. The Charcot-Bouchard controversy. Arch Neurol. 1986;43(03):290–295. doi: 10.1001/archneur.1986.00520030076022. [DOI] [PubMed] [Google Scholar]
- 65.Teive H AG, Chien H F, Munhoz R P, Barbosa E R. Charcot's contribution to the study of Tourette's syndrome. Arq Neuropsiquiatr. 2008;66(04):918–921. doi: 10.1590/s0004-282x2008000600035. [DOI] [PubMed] [Google Scholar]
- 66.Teive H AG, Germiniani F MB, Munhoz R P, Paola Ld. 126 hysterical years - the contribution of Charcot. Arq Neuropsiquiatr. 2014;72(08):636–639. doi: 10.1590/0004-282X20140068. [DOI] [PubMed] [Google Scholar]
- 67.Bogousslavsky J. Jean-Martin Charcot and his legacy. Front Neurol Neurosci. 2014;35(35):44–55. doi: 10.1159/000359991. [DOI] [PubMed] [Google Scholar]
- 68.Widlöcher D, Dantchev N.[Charcot and hysteria] Rev Neurol (Paris) 1994150(8-9):490–497. [PubMed] [Google Scholar]
- 69.White M B. Jean-Martin Charcot's contributions to the interface between neurology and psychiatry. Can J Neurol Sci. 1997;24(03):254–260. doi: 10.1017/s0317167100021909. [DOI] [PubMed] [Google Scholar]
- 70.Walusinski O.Jean-Martin Charcot (1825-1893): A Treatment Approach Gone Astray? Eur Neurol 201778(5-6):296–306. [DOI] [PubMed] [Google Scholar]
- 71.Briquet P. Paris: JB. Baillière; 1859. Traité clinique et thérapeutique de l'hystérie. [Google Scholar]
- 72.Négrier C H. Angers: Imprimerie de Cosnier et Lachèse; 1858. Recueil des faits pour servir à l'histoire des ovaires et des affections hystériques de la femme. [Google Scholar]
- 73.Tourneux J. Paris: Imprimerie Derenne; 1877. Altération de l'ovaire envisagée comme cause de l'hystéro-épilepsie. Thèse Paris no. 350. [Google Scholar]
- 74.Bogousslavsky J, Walusinski O, Veyrunes D. Crime, hysteria and belle époque hypnotism: the path traced by Jean-Martin Charcot and Georges Gilles de la Tourette. Eur Neurol. 2009;62(04):193–199. doi: 10.1159/000228252. [DOI] [PubMed] [Google Scholar]
- 75.Richet C. Le somnambulisme provoqué. J Anat Physiol Norm Pathol. 1875;11:348–378. [Google Scholar]
- 76.Walusinski O, Bogousslavsky J. Charcot, Janet, and French models of psychopathology. Eur Neurol. 2020;83(03):333–340. doi: 10.1159/000508267. [DOI] [PubMed] [Google Scholar]
- 77.Hierons R. Charcot and his visits to Britain. BMJ. 1993;307(6919):1589–1591. doi: 10.1136/bmj.307.6919.1589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Charcot J M. Paris: Lecosnier et Babé; 1890. Seizième leçon: spiritisme et hystérie. Tome III. [Google Scholar]
- 79.Babinski J. Définition de l'hystérie. Rev Neurol (Paris) 1901;9:1074–1080. [Google Scholar]
- 80.Lipsett P A, Pitt H A. Acute cholangitis. Surg Clin North Am. 1990;70(06):1297–1312. doi: 10.1016/s0039-6109(16)45285-0. [DOI] [PubMed] [Google Scholar]
- 81.Teive H A, Germiniani F M, Munhoz R P. Overlap between fibromyalgia tender points and Charcot's hysterical zones: A historical curiosity. Neurology. 2015;84(20):2096–2097. doi: 10.1212/WNL.0000000000001592. [DOI] [PubMed] [Google Scholar]
- 82.Charcot J M. Paris: Lecosnier et Babé; 1894. Œuvres complètes, Tome II. Progrès Médical; pp. 42–58. [Google Scholar]
- 83.Mackay D D, Garza P S, Bruce B B, Newman N J, Biousse V. The demise of direct ophthalmoscopy: A modern clinical challenge. Neurol Clin Pract. 2015;5(02):150–157. doi: 10.1212/CPJ.0000000000000115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Teive H AG, Munhoz R P, Barbosa E R. Little-known scientific contributions of J-M Charcot. Clinics (São Paulo) 2007;62(03):211–214. doi: 10.1590/s1807-59322007000300003. [DOI] [PubMed] [Google Scholar]
- 85.Charcot J M. L'intoxication saturnine exerce-t-elle une influence sur le développement de la goutte? Gazette Hebdomadaire De Médecine Et De Chirurgie. 1863;10:434–439. [Google Scholar]
- 86.Lee L, Blume P A, Sumpio B. Charcot joint disease in diabetes mellitus. Ann Vasc Surg. 2003;17(05):571–580. doi: 10.1007/s10016-003-0039-5. [DOI] [PubMed] [Google Scholar]
- 87.Sanders L J. The Charcot foot: historical perspective 1827-2003. Diabetes Metab Res Rev. 2004;20 01:S4–S8. doi: 10.1002/dmrr.451. [DOI] [PubMed] [Google Scholar]
- 88.Kundu A KR. Charcot in medical eponyms. J Assoc Physicians India. 2004;52:716–718. [PubMed] [Google Scholar]
- 89.Taylor S. London: Royal Society of Medicine Services Ltd.; 1989. Robert Graves: the golden years of Irish Medicine; pp. 1–160. [Google Scholar]
- 90.Basedow C A. Exophthalmos durch Hypertrophie des Zellgewebes in der Augenhöhle. Wochenschrift fur die gesammte Heilkunde (Berlin) 1840;6:197–220. [Google Scholar]
- 91.Charcot J M, Vulpian E A. Note sur les cristaux particulier trouvés dans le sang et les viscères d'un sujet leucémique. Gaz Med. 1860;7:755. [Google Scholar]
- 92.von Leyden E. Zur Kenntnis des Bronchialasthmas. Archiv Path Anat. 1872;54:324. [Google Scholar]
- 93.Lacombe M.[The history of intermittent claudication due to arterial disease] Ann Chir 2005130(6-7):440–444. [DOI] [PubMed] [Google Scholar]
- 94.Charcot J-M.Sur la claudication intermittente observé dans un cas d'oblitération complète des artères iliaques primitivesComptes Rendus des Seances et Mémoires de la Société de Biologie 1859;5(2ème série, 1858):225–238.https://gallica.bnf.fr/ark:/12148/bpt6k6387889t/f437.item#
- 95.Sugar O. Jean-François Bouley (Bouley jeune). Pioneer investigator in intermittent claudication. Spine. 1994;19(03):346–349. doi: 10.1097/00007632-199402000-00016. [DOI] [PubMed] [Google Scholar]
- 96.Bollinger A, Eckert J, Rüttimann B, Becker F. The “galloping” history of intermittent claudication. Vasa. 2000;29(04):295–299. doi: 10.1024/0301-1526.29.4.295. [DOI] [PubMed] [Google Scholar]
- 97.Weiss S, Baker J P. The carotid sinus reflex in health and disease. Its role in the causation of fainting and convulsions. Medicine (Baltimore) 1933;12:297–354. [Google Scholar]
- 98.Levine J M. Historical perspective on pressure ulcers: The decubitous ominosus of Jean-Martin Charcot. J Am Geriatr Soc. 2005;53:124851. doi: 10.1111/j.1532-5415.2005.53358.x. [DOI] [PubMed] [Google Scholar]
- 99.Lellouch A. [J.-M. Charcot: also, pioneer of geriatrics] Rev Prat. 1996;46(01):15–18. [PubMed] [Google Scholar]
- 100.Huard P. [J.M. Charcot's gerontology] Rev Neurol (Paris) 1982;138(12):989–995. [PubMed] [Google Scholar]
- 101.Johnson P. London: Weidenfeld and Nicolson; 1988. Intellectuals. [Google Scholar]
- 102.Teive H AG, Franklin G L, Lima P, Germiniani F MB, Camargo C HF, Walusinski O. The art of Charcot: An outstanding caricaturist. Eur Neurol. 2021;84(01):49–52. doi: 10.1159/000513677. [DOI] [PubMed] [Google Scholar]
- 103.Charcot J M, Richer P. Adrien Delahaye & Émile Lecrosnier (Editors), Paris, France; 1887. Les démoniaques dans l'art. [Google Scholar]
- 104.Meige H. Paris: Masson et Cie.; 1925. Charcot artiste. [Google Scholar]
- 105.Bouchara C. Paris: Philippe Rey; 2013. Charcot. Une vie avec l'image. [Google Scholar]
- 106.Teive H AG, Munhoz R P, Silva G G. Charcot's skepticism. Arq Neuropsiquiatr. 2012;70(11):897–899. doi: 10.1590/s0004-282x2012001100014. [DOI] [PubMed] [Google Scholar]
- 107.Teive H AG, Germiniani F MB, Munhoz R P. Charcot's irony and sarcasm. Arq Neuropsiquiatr. 2017;75(06):402–404. doi: 10.1590/0004-282X20170062. [DOI] [PubMed] [Google Scholar]
- 108.Silva M ME, Meira A T, Walusinski O, Camargo C HF, Teive H AG. Charcot's paradox. Arq Neuropsiquiatr. 2019;77(08):590–593. doi: 10.1590/0004-282X20190037. [DOI] [PubMed] [Google Scholar]
- 109.Nascimento F A, Camargo C HF, Walusinski O, Teive H AG. Charcot and his passion for dogs – a historical note. Eur Neurol. 2020;83(06):636–638. doi: 10.1159/000511573. [DOI] [PubMed] [Google Scholar]
- 110.Teive H A, Arruda W O, Werneck L C.Rosalie: the Brazilian female monkey of Charcot Arq Neuropsiquiatr 200563(3A):707–708. [DOI] [PubMed] [Google Scholar]
- 111.Coutinho L, Walusinski O, Teive H AG. Désiré Bourneville: A socialist in Charcot's inner circle. Eur Neurol. 2022;85(01):79–84. doi: 10.1159/000518846. [DOI] [PubMed] [Google Scholar]
- 112.Teive H AG, Marques P, Germiniani F MB, Walusinski O. Requiem for a neurologist: the funeral rites of Jean-Martin Charcot. Arq Neuropsiquiatr. 2017;75(11):827–829. doi: 10.1590/0004-282X20170144. [DOI] [PubMed] [Google Scholar]
- 113.Teive H AG, Camargo C HF, Walusinski O, Lees A J. Charcot: Buddhist Leanings? Eur Neurol. 2021;84(02):135–138. doi: 10.1159/000514430. [DOI] [PubMed] [Google Scholar]
- 114.Charcot J M. Ottawa: University of Ottawa Press; 2012. Charcot in Morocco. Introduction, notes and translation by Toby Gelfand. [Google Scholar]
- 115.Charcot J-M. La foi qui guérit. Revue Hebdomadaire. 1892;5:112–132. [Google Scholar]
- 116.Coutinho L, Caeira M W, Paola L et al. Les démoniaques dans l'art: Charcot and the “hysterical saints”. Arq Neuropsiquiatr. 2022;80(11):1178–1181. doi: 10.1055/s-0042-1759709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Charcot J M, Richter P. New York: Wentworth Press; 2018. Les Difformes Et Les Malades Dans l'Art. [Google Scholar]
- 118.Goetz C G. The Salpêtrière in the wake of Charcot's death. Arch Neurol. 1988;45(04):444–447. doi: 10.1001/archneur.1988.00520280094023. [DOI] [PubMed] [Google Scholar]